old woman with severe coronary heart disase and … · abdome: liver palpable painful two...
TRANSCRIPT
OLD WOMAN WITH SEVERE CORONARY HEART DISASE AND LEFT BUNDLE BRANCH BLOCK
MULHER IDOSA COM DOENÇA CORONARIANA SEVERA E BLOQUEIO COMPLETO DE RAMO
ESQUERDO
MUJER DE EDAD AVANZADA CON ENFERMEDAD CORONARIA SEVERA Y BLOQUEO COMPLETO DE
RAMA IZQUIERDA
Case of Andrés Ricardo Pérez-Riera MD PhDChief of electrovectorcardiogram sector – Cardiology Discipline - ABC Medicine Faculty – Santo André - São Paulo Brazil.Contact [email protected] phone: (011) 84693388

Feminine, Caucasian, 74 yo, retired, severe coronary artery disease, (two clinical episodes of myocardial infarctions at past), essential hypertension, type 2 diabetes mellitus, hyperlipoproteinemia type IIb(increased blood levels of low density lipoproteins LDL and apoprotein B (ApoB) and centripetal obesity android fat distribution. Absolute waist circumference 105cm and waist–hip ratio>0.85. (body mass index >30 kg/m2 ).BP 165/90, General: Breathless, moderately obese woman in acute distress sitting upright complaining "I am going to die. Please help me."Normocephalic. Eyes, ears, and throat normal.Neck: Whit the patient positioned under 45° distended neck veins with visible large 'a' waves, The jugular venous pressure JVP to 12cm. Sistolic bruit on left carotid reflecting turbulence of flow .Chest: the point of maximal impulse (ictus cordis) palpated in the 6th intercostal space just al axilar line and exceed a quarter size (24.26 mm). No thrill. Normal HR, regular. Grade 3/6 systolic murmur at LSB, S3 gallop noted. Lung: bilateral rales one third lower bases.Abdome: Liver palpable painful two centimeters below right costal margin. HJR+ Non-tender to palpation, +Bowel sounds 4 quadrants. Genitalia: Exam deferred.Extremities: minimal pitting edema of lower extremities to the knees. Nail beds acyanotic, no clubbing. Pedis and posterior tibial pulse in retromalleolar decreased. Elevation of the left foot to 30º for 30 seconds caused pallor. (Buerger’s test). Neurologic: No localized or sensory deficits. Mental status intact.
Which is the ECG/VCG diagnosis and why?--------------------------------------------------------------------------------------------------------------------------
Paciente del sexo femenino, 74 años, jubilada, sabidamente portadora de severa enfermedad coronaria(antecedente de dos episodios clinicos previos de infarto de miocardio). hipertensa esencial, diabética tipo 2, dislipémica tipo IIb (aumento de LDL y Apo B) y obesa centrípeta (índice de masa corporal > 30) distribuición androide: circunferencia abdominal 105cm y relación cintura/cadera >0.85 Indice de masacorporal >30kg/m2. PA 165/90, respiración dificultosa, obesa, sentada y diciendo que estaba por morir. “Porfabor me ayude”.Cabeza: nada digno de notaCuello: con la paciente 45 grados se observa distensión de las yuguares con ondas “a” aumentadas. Soplo sistólico en carótida izquierda refejando turbulencia al flujo sanguineo.Tórax: choque de la punta palpable en el 6to espacio intercostal izquierdo en la linea axilar anterior y no se cubre con una pulpa digital. Ausencia de frémito catário.RCR, soplo sistólico 3/6 el el borde izquierdo del esternón y tercer ruido con cadencia de galopePulmones rales crepitantes bilaterales en el tercio inferior de ambos pulmones.Abdomen: hígado palpable doloroso a dos centímetros del reborde costal derecho. Ruidos hidroaereos pesentes en los cuatro cuadrantesGenitales: no realizado.Extremidades; fobea en la región maleolar de las extremidades inferiores, Lecho ungeal acianótico y sin baqueteamiento digital. Pulso pedio y tibial posterior en la región retro-maleolar interna disminuido a la izquierda. La maniobra de elevación del pie izquierdo a 30º por 30 segundos causó palidez del pie( test de Buerger)Neurológico: sin déficit neurologicos. Buen contacto.
Preguntas: Cual es el diagnóstico ECG/VCG y porque?
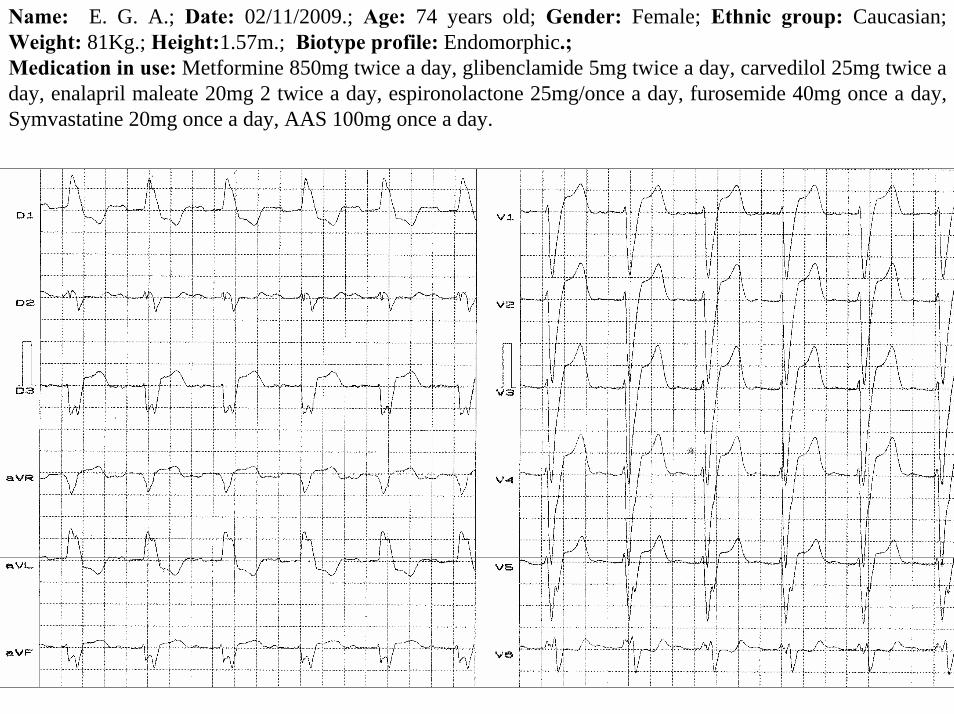
Name: E. G. A.; Date: 02/11/2009.; Age: 74 years old; Gender: Female; Ethnic group: Caucasian; Weight: 81Kg.; Height:1.57m.; Biotype profile: Endomorphic.; Medication in use: Metformine 850mg twice a day, glibenclamide 5mg twice a day, carvedilol 25mg twice a day, enalapril maleate 20mg 2 twice a day, espironolactone 25mg/once a day, furosemide 40mg once a day, Symvastatine 20mg once a day, AAS 100mg once a day.

Y
X I
IIIII
aVF
aVR aVL
T
X
Z
V6
V1
V4
V5
V2
V3
T
Y
Z
aVF
T
V2

COLLEAGES OPINION
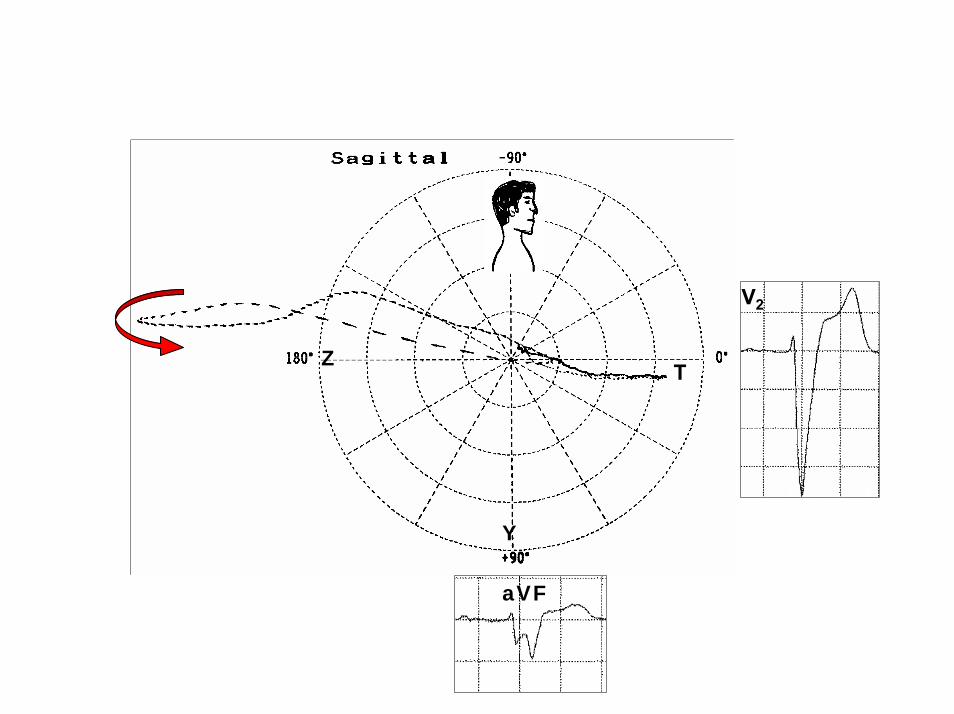
Caro Andrés:O caso é realmente muito interessante. O diagnóstico eletrocardiográfico é de um BRE mais BDAS. Ocorre que o supradesnivelamento do segmento ST está presente de V1 a V5 o que não é habitual em presença de BRE isolado. O Vectocardiograma revela área eletricamente inativa em face anterior.Podemos concluir a partir destes dados, que houve uma obstrução da artéria descendente anterior e poderíamos até elucubrar que durante a ocorrência do infarto que a anamnese já havia revelado, tivesse se instalado o BRE (apenas elucubração, não nenhuma certeza). Por outro lado, tratando-se de paciente diabética, com síndrome metabólica, não surpreenderia se a cinecoronariografiarevela-se uma coronariopatia difusa, com comprometimento das demais artérias coronárias.Um grande abraço do Hélio Germiniani que o felicita pela sua linda Tese.Prof. Hélio Germiniani Professor livre-docente de Cardiologia da UFPr.Professor Adjunto IV de Farmacologia da UFPr.Coordenador do Curso de Pós-Graduação Mestrado em Cardiologia daU.F.PrChefe do Serviço de Eletrocardiografia do Hospital de Clínicas da U.F.Pr.Ex-presidente da Sociedade Brasileira de Cardiologia e da Sociedade Paranaense de Cardiologia. Dear Andrés,The case is really very interesting. The electrocardiographic diagnosis is of LBBB plusLSFB. It so happens that ST segment elevation is present fromV1 through V5, which is not usual in the presence of isolated LBBB. The Vectorcadiogram reveals an electrically inactive area in the anterior wall. We can conclude from these data, that there was an obstruction of the ADA, and we mayeven present the hypothesis that during the infarction that the anamnesis had alreadyrevealed that the LBBB had installed (just a hypothesis, with no certainty). On the otherhand, since this is a diabetic patient, with metabolic syndrome, I would not be surprised ifcoronary angiography revealed a diffuse CAD, with involvement of the other coronaryarteries. Warm regards from Hélio Germiniani, and congratulations for your great thesis.
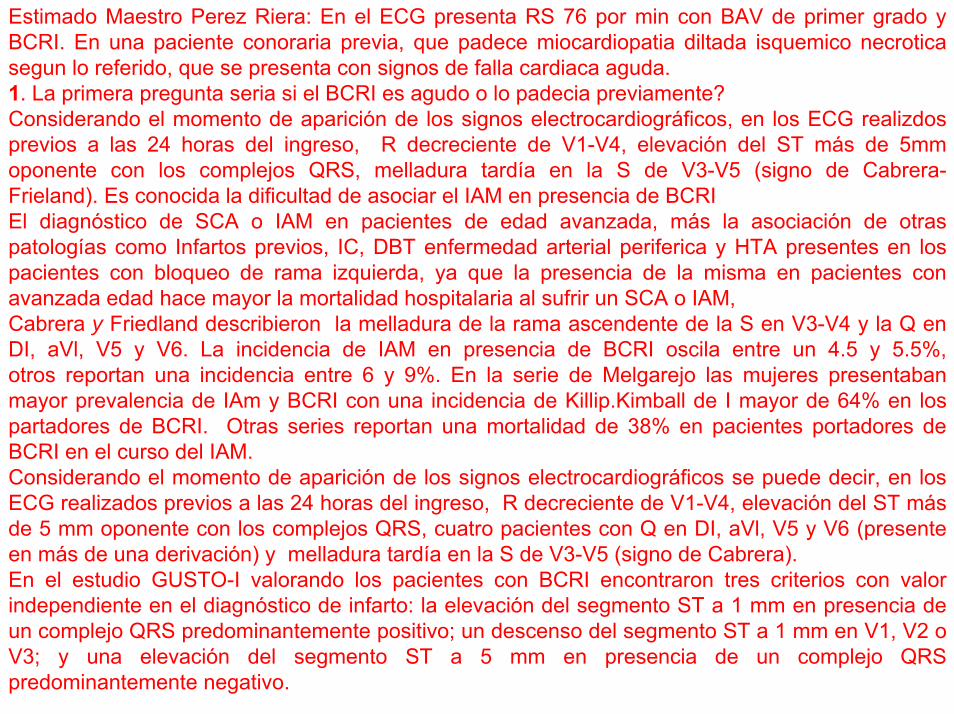
Estimado Maestro Perez Riera: En el ECG presenta RS 76 por min con BAV de primer grado y BCRI. En una paciente conoraria previa, que padece miocardiopatia diltada isquemico necroticasegun lo referido, que se presenta con signos de falla cardiaca aguda.1. La primera pregunta seria si el BCRI es agudo o lo padecia previamente?Considerando el momento de aparición de los signos electrocardiográficos, en los ECG realizdosprevios a las 24 horas del ingreso, R decreciente de V1-V4, elevación del ST más de 5mm oponente con los complejos QRS, melladura tardía en la S de V3-V5 (signo de Cabrera-Frieland). Es conocida la dificultad de asociar el IAM en presencia de BCRIEl diagnóstico de SCA o IAM en pacientes de edad avanzada, más la asociación de otraspatologías como Infartos previos, IC, DBT enfermedad arterial periferica y HTA presentes en lospacientes con bloqueo de rama izquierda, ya que la presencia de la misma en pacientes con avanzada edad hace mayor la mortalidad hospitalaria al sufrir un SCA o IAM,Cabrera y Friedland describieron la melladura de la rama ascendente de la S en V3-V4 y la Q en DI, aVl, V5 y V6. La incidencia de IAM en presencia de BCRI oscila entre un 4.5 y 5.5%, otros reportan una incidencia entre 6 y 9%. En la serie de Melgarejo las mujeres presentabanmayor prevalencia de IAm y BCRI con una incidencia de Killip.Kimball de I mayor de 64% en lospartadores de BCRI. Otras series reportan una mortalidad de 38% en pacientes portadores de BCRI en el curso del IAM.Considerando el momento de aparición de los signos electrocardiográficos se puede decir, en losECG realizados previos a las 24 horas del ingreso, R decreciente de V1-V4, elevación del ST másde 5 mm oponente con los complejos QRS, cuatro pacientes con Q en DI, aVl, V5 y V6 (presenteen más de una derivación) y melladura tardía en la S de V3-V5 (signo de Cabrera). En el estudio GUSTO-I valorando los pacientes con BCRI encontraron tres criterios con valor independiente en el diagnóstico de infarto: la elevación del segmento ST a 1 mm en presencia de un complejo QRS predominantemente positivo; un descenso del segmento ST a 1 mm en V1, V2 o V3; y una elevación del segmento ST a 5 mm en presencia de un complejo QRS predominantemente negativo.
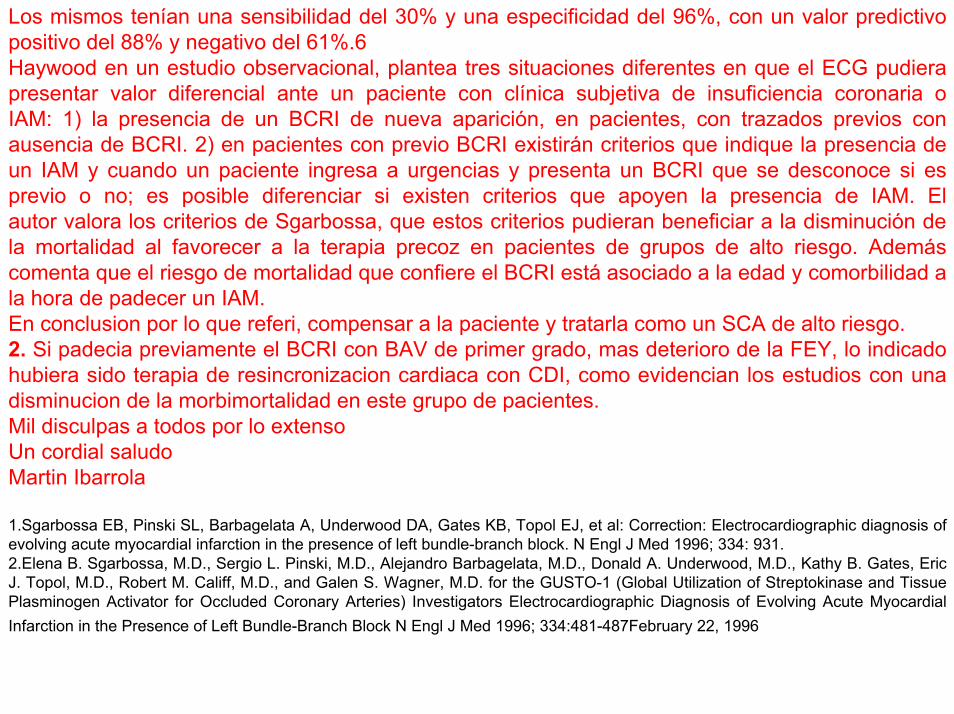
Los mismos tenían una sensibilidad del 30% y una especificidad del 96%, con un valor predictivopositivo del 88% y negativo del 61%.6 Haywood en un estudio observacional, plantea tres situaciones diferentes en que el ECG pudierapresentar valor diferencial ante un paciente con clínica subjetiva de insuficiencia coronaria o IAM: 1) la presencia de un BCRI de nueva aparición, en pacientes, con trazados previos con ausencia de BCRI. 2) en pacientes con previo BCRI existirán criterios que indique la presencia de un IAM y cuando un paciente ingresa a urgencias y presenta un BCRI que se desconoce si es previo o no; es posible diferenciar si existen criterios que apoyen la presencia de IAM. El autor valora los criterios de Sgarbossa, que estos criterios pudieran beneficiar a la disminución de la mortalidad al favorecer a la terapia precoz en pacientes de grupos de alto riesgo. Ademáscomenta que el riesgo de mortalidad que confiere el BCRI está asociado a la edad y comorbilidad a la hora de padecer un IAM.En conclusion por lo que referi, compensar a la paciente y tratarla como un SCA de alto riesgo.2. Si padecia previamente el BCRI con BAV de primer grado, mas deterioro de la FEY, lo indicadohubiera sido terapia de resincronizacion cardiaca con CDI, como evidencian los estudios con unadisminucion de la morbimortalidad en este grupo de pacientes.Mil disculpas a todos por lo extensoUn cordial saludoMartin Ibarrola
1.Sgarbossa EB, Pinski SL, Barbagelata A, Underwood DA, Gates KB, Topol EJ, et al: Correction: Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. N Engl J Med 1996; 334: 931. 2.Elena B. Sgarbossa, M.D., Sergio L. Pinski, M.D., Alejandro Barbagelata, M.D., Donald A. Underwood, M.D., Kathy B. Gates, Eric J. Topol, M.D., Robert M. Califf, M.D., and Galen S. Wagner, M.D. for the GUSTO-1 (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries) Investigators Electrocardiographic Diagnosis of Evolving Acute Myocardial Infarction in the Presence of Left Bundle-Branch Block N Engl J Med 1996; 334:481-487February 22, 1996

Discutire el caso de bloqueo de rama izquierda ,enviado por nuestro maestro Profesor Andrés Ricardo Pérez Riera MD PhD: este es un caso gravisimo, muy probable, bloqueo bilateral LBBB + bloqueo AV de primer grado. El BCRI es muy ancho (casi 200 ms), sugeriendo dilatación del VI muy probablemente como evolución de una HVI asociada a isquemia severa. Las ondas S,s muy profundas en las precordiales indican predominancia de los potenciales posteriores por remodelación de un infarto anterior y SVI sistólica y diastólica La separacion en aVL, entre R1 y R2 de alrededor de 80 ms, sugiere fibrosis severa del septo ventricular (normalmente R1-R2 del LBBB sin patologia es de ≤40ms)El potencial que aparece como primer vector en II antecede al QRS en I y aVL, sugeriendo depolarizacion muy lenta del VD, probablemente por infarto de esta cámara, que origina los signos de insuficiencia ventricular derecha y alta presion auticular. La falta de progresion de las R hasta V6 que es muy infrecuente en BCRI , muy probablemente sea consecuencia de infarto anteroseptal muy extenso (los bloqueos Q/S hasta V6 se ven en marcapasos derechos o en infartos anteriores muy extensos ). En conclusion este ECG indica dilatación de ambos ventriculos, por infartos muy extenso anterior izquierdo y de VD, talvez con insuficiencia tricuspidea o mitral. En los. datos clinicos falta la irradiacion del soplo, y si el higado late. Debo agregar que este BCRI es troncular (frecuente en mujeres post-menopáusicas generalmente se acompaña de calcificación del anillo valvular izquierdo) no relacionado al cuadro isquemico Probablemente el bloqueo de primer grado tiene relacion con el infarto de VD. Estos ECGs son bastante frecuentes actualmente debido a los tratamientos médicos mas eficaces o by-pass aorto coronario. Una chance probable de mejorar en algo el sufrimiento de esta pobre mujer es cateterizarla y tratar de abrir cualquier arteria que aun pueda suplir este miocardio Un fraternal abrazo Samuel Sclarovsky
I will tried to report a very severe case in a 74 year old female with CLBBB, presented our good friend Professor Dr Andrés Ricardo Pérez Riera MD PhD: From the electrical conduction point of view, it is a case of CLBBB + first-degree A-V block suggesting a bilateral bundle branch block. From the morphological point of view this is a very wide LBBB (near 200ms) suggesting severe left ventricular dilatation. The S,s waves in the V2 ,V3 are very deep, suggesting that the prevalent electrotonic ventricular forces are shifted to the posterior wall, indicating posterior remodeling due to extensive transmural anterior wall infarction or LVH due diastolic and systolic overloading as well The space between the first R and the second one in aVL is 80 ms , suggesting a severe delay in the anterior wall of left ventricular , due to a repair fibrosis after extensive infarction ( in patient with CLBBB without structural heart disease RR´ is 40 ms )The positive vector witch appears in II and V6, precede the left vectors expressed in aVL and I, indicated most probably very slow depolarization of right ventricle, suggesting a RV fibrosis due to an old infarction.The lack of R progression in CLBBB is not a frequent finding, The lack of R progression of CLBBB
pattern is found in right ventricle pacemaker excitation or in very extensive anterior wall MI with left axis deviation
The clinics parameters indicate a severe mitral insufficiency with a tricuspide one ,tooIn conclusion this patient in according to the electrical morphology suffers from a severe biventricular dilatation, most probably the right ventricular dysfunction and tricuspide insuffiency relief the overflow to the left one. This is a troncular CLBBB, no related to the the ischemic process, but very frequent in post menopausal female, frequently accompanied with annulus calcification of the left valves. The left conduction delay due to posterior and anterior infarction, is seen as atypical LBBB, due to a down regulation of the conexin 43 due to severe anterior and posterior ischemia in this pattern mimicking LBBB is complete different fron the troncular. My opinion is this patient ,must be undergone a hemodinamic study and try to open every artery possible , because in this severe cases still leaving , are many hibernated areas in the heart, and same time it is possible to get positive results. This cases were very seldom in the past ( I survive 52 years as cardiologist ) but in the modern era , this cases are more frequent due to the modern medical treatment ,aortic -coronary bypass and angioplasty My best regard Samuel Sclarovsky
Estimados amigos del Foro: en primer lugar quiero agradecer las conceptuosas palabras de AB y del Profesor Pérez Riera hacia mi persona.Con respecto al caso, obviamente tenemos un infarto de pared anterior y de pared libre del ventrículo izquierdo porque no hay crecimiento de la onda R en las precordiales y en el plano horizontal la porción final cruza el eje de Z hacia la derecha, lo que motiva las "S" profundas en precordiales izquierdas. Ademas el plano frontal es sugestivo la concomitancia de necrosis inferior.El cuadro parece ser agudo porque la repolarización ventricular el bucle QRS no cierra en 0 sinó que deja un importante vector ST responsable por el desnivel de este segmento. Sia eso le agregamos el del bucle de T es redondeado, podemos sospechar que el proceso es isquémico. Cabe destacar el septum está indemne, porque el nacimiento del bucle QRS en el PH está dirigido hacia delante y a izquierda, es decir preservado.Saludos a todosCarlos Lavergne NeuquénDear Friends Forum: First of all I want to thank the glowing words of AB and Professor Pérez-Riera related myself Regarding the case, we obviously have an anterior and left ventricular free wall MI because there is no growth of the R wave in the horizontal plane and the end of QRS loop crosses the orthognal Z axis to the right, what motivates the final "S" deep waves in left precordial leads.Besides the frontal plane is suggestive of inferior necrosis in association.The picture seems to be acute because the QRS ventricular repolarization loop does not close to 0 but leaves an important ST segment elevation. Additionally, the loop T is round, suggestive of ischemic T-loop.Notably the septum is intact, because the initial 10ms QRS loop in the PH is preserved because it is directed forward and left.Greetings to all. Carlos Lavergne MD Neuquén
Dear Andrés: This woman with severe ischemic cardiomyopathy and LBBB has ECG findings compatible with several old myocardial infarctions. From the ECG perspective she is in sinus rhythm with a first degree AV block (PR ~ 280 ms) and a very wide QRS (~180 ms) suggestive of left ventricular hypertrophy. The QRS axis is left at approximately -30 degrees. The ST-T wave findings are typical of the secondary ST-T changes seen with LBBB with the general direction of the ST-T in the opposite direction from the QRS direction. I do not see primary (ischemic) ST-T abnormalities. In lead V3 the take-off of the ST wave is ~5 mm above the baseline, but I think thisis unlikely to be primary ischemia. Several findings in the QRS complex suggest old myocardial infarctions. In lead V5 the prominent notch in the upstroke of the S wave is the "sign of Cabrera" and represents myocardial scar late in the left ventricular activation sequence (LV lateral wall). The prominent S wave in lead V6, assuming accurate lead placement, is also likely a Q-wave equivalent and an electrically silent area of myocardium in the basal-lateral wall of the LV. Also, in lead V6 as well as lead II there is an "bite" taken out of the initial r-wave (? sign of Chapman) which also is a Q-wave equivalent of old myocardial scar from an area of LV that is activated early in the LV activation sequence.I'm interested in other ideas from colleagues especially with regard to the VCG findings.Best regards,Yanowitz, Frank MDProfessor of MedicineUniversity of Utah School of MedicineMedical Director, ECG DepartmentLDS Hospital Salt Lake City, Utah 8th Ave. and C StreetSalt Lake City, Utah 84143 [email protected]; [email protected]

Querido Andrés: Esta mujer con cardiomiopatia isquémica severa y BCRI tiene hayazgoscompatibles con varios infartos antiguos.El ECG muestra ritmo sinusal, bloqueo AV de primer grado (PR ≈ 280 ms) QRS muyancho(~180 ms) sugestivo de SVI. El eje del QRS se encuentra ≈ en -30º. El ST/T tiene características secundárias observadas en los BRCI no complicados con dirección totalmente opuesta a la del QRS. Yo no veo anormalidades primárias en el ST/T. En la derivación V3 el supradesnivel del ST se encuentra ≈ 5mm arriba de la linea de base, no obstante no pienso que esto sea alteración primarias de repolarización.Vários hallazgos en el complejo QRS sugieren infartos antiguos de miocardio. En la derivación V5 se observa una escotadura en la rampa ascendente de la S conocida comosigno de Cabrera y representa cicatrices que afectan la secuencia de la activación del VI en la pared lateral.La onda S profunda de V6 asumiendo que el electrodo esté en posición correcta, es también un equivalente de una Q de necrosis y una area silente de miocardio en la regiónbasal-lateral del VI( signo de Chapman) el cual también es un equivalente de una Q de cicatriz antigua en la secuencia de activación ventricular. Estoy interesado en otras ideas de colegas especialmente en relación a los hayazgosvectocardiográficos.
Estimados amigos: el analisis del ECG/VCG en contexto de la clinica "orientadora " se trata de :BAV de 1er gradoBloqueo De Rama Izquierda Disfrazado Precordial Con R En V1(por Necrosis AnterolateralExtensa ) y fuerzas en cuadrante Ne Por Necrosis InferiorAlteracion de R.V por discinecia anterior y apical
Todo esto explica el compromiso clinico y hemodinamico de la paciente choque punta difusoondas a en pulso venoso por dilatacion de VD mas htps soplo de insuficiencia tricuspideahepatomegalia tercer ruido galope POR DILATACION MAS DISF SIST.V.I mas ANEUR.hipoperfusionlecho ungueal palido
Posiblemente encontremos en el eco las alteraciones descriptas con una fraccion de eyeccionseveramente disminuida ( menor de 30 %) y disfuncion diastolica por alteracion de la distensibilidad (patron tipo 3-4 ) y citerios de disincronia A-V ,inter e intra ventricular ,criterios quesumados a falla tratamiento full para ICBCRIPotencial indicacion de terapia eléctrica de resincronizacion
Abrazos a todos
Juan José Sirena
OUR DIAGNOSIS AND FINAL COMMENTS
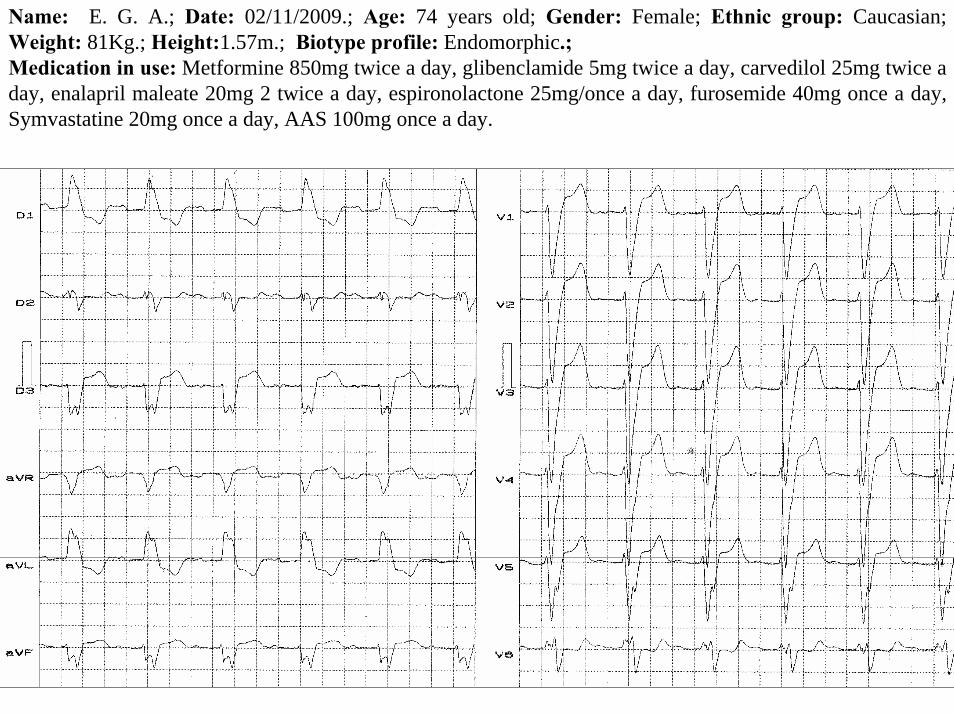
Name: E. G. A.; Date: 02/11/2009.; Age: 74 years old; Gender: Female; Ethnic group: Caucasian; Weight: 81Kg.; Height:1.57m.; Biotype profile: Endomorphic.; Medication in use: Metformine 850mg twice a day, glibenclamide 5mg twice a day, carvedilol 25mg twice a day, enalapril maleate 20mg 2 twice a day, espironolactone 25mg/once a day, furosemide 40mg once a day, Symvastatine 20mg once a day, AAS 100mg once a day.
Y
X I
IIIII
aVF
aVR aVL
T
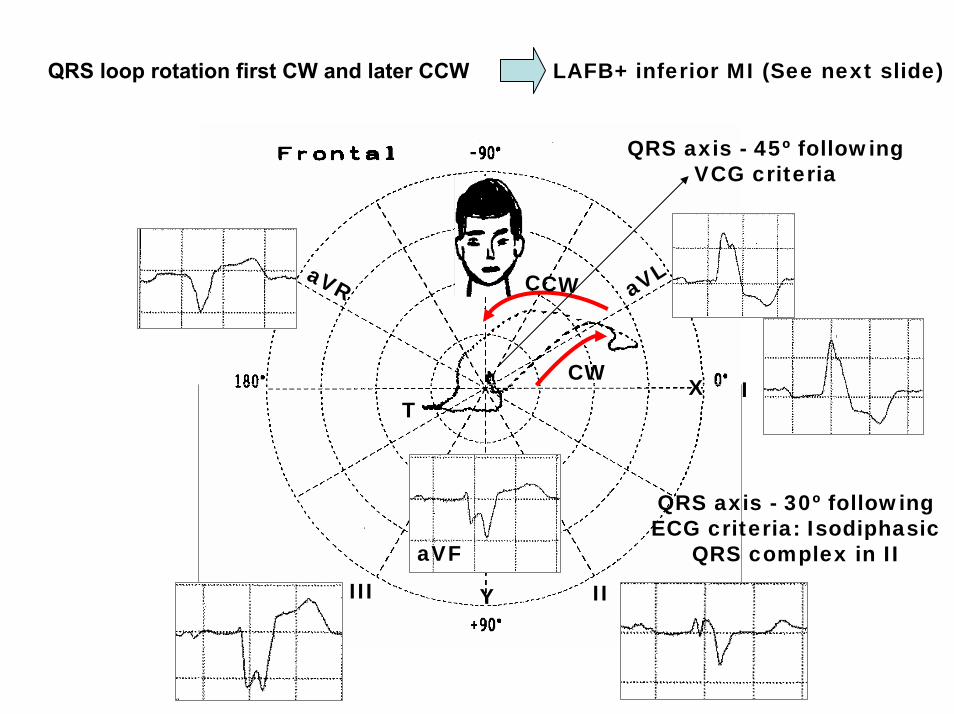
QRS axis - 45º following VCG criteria
QRS axis - 30º following ECG criteria: Isodiphasic
QRS complex in II
QRS loop rotation first CW and later CCW LAFB+ inferior MI (See next slide)
CCW
CW
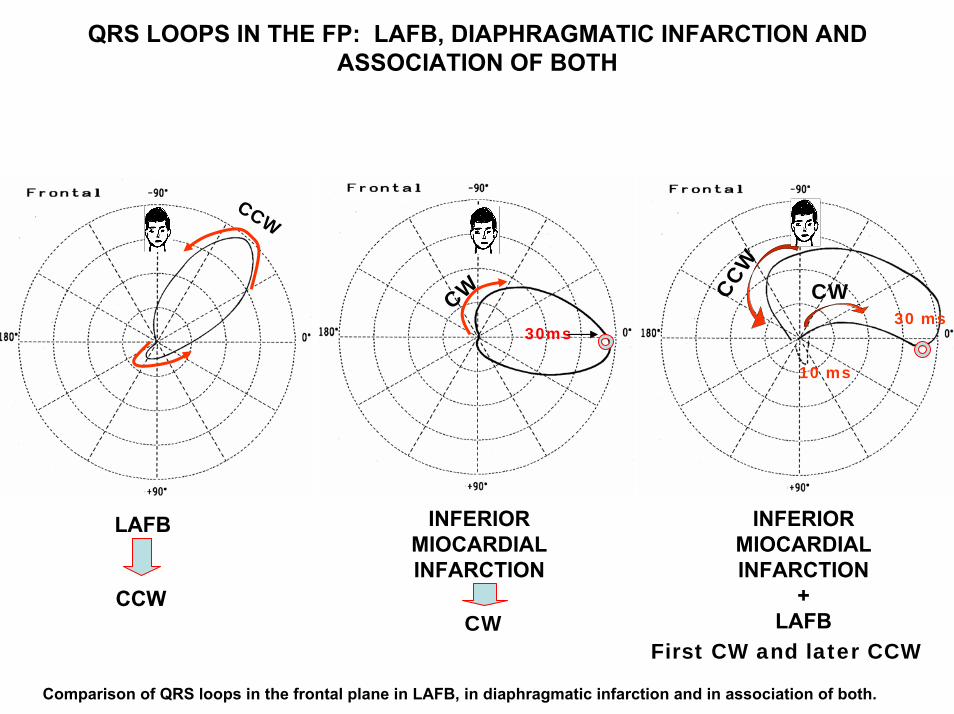
QRS LOOPS IN THE FP: LAFB, DIAPHRAGMATIC INFARCTION AND ASSOCIATION OF BOTH
LAFB
30 ms
10 ms
30ms
INFERIORMIOCARDIALINFARCTION
CCW
CW CWCCW
INFERIORMIOCARDIALINFARCTION
+LAFB
CCWCW
First CW and later CCW
Comparison of QRS loops in the frontal plane in LAFB, in diaphragmatic infarction and in association of both.
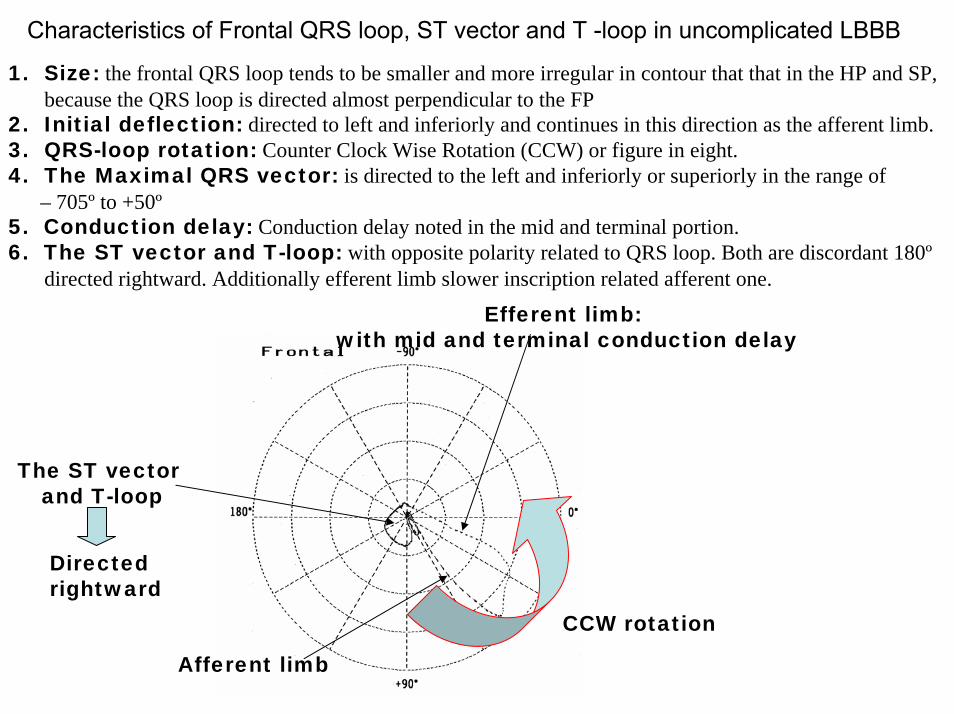
Characteristics of Frontal QRS loop, ST vector and T -loop in uncomplicated LBBB
1. Size: the frontal QRS loop tends to be smaller and more irregular in contour that that in the HP and SP, because the QRS loop is directed almost perpendicular to the FP
2. Initial deflection: directed to left and inferiorly and continues in this direction as the afferent limb.3. QRS-loop rotation: Counter Clock Wise Rotation (CCW) or figure in eight.4. The Maximal QRS vector: is directed to the left and inferiorly or superiorly in the range of
– 705º to +50º5. Conduction delay: Conduction delay noted in the mid and terminal portion.6. The ST vector and T-loop: with opposite polarity related to QRS loop. Both are discordant 180º
directed rightward. Additionally efferent limb slower inscription related afferent one.
Afferent limb
CCW rotation
The ST vector and T-loop
Efferent limb: with mid and terminal conduction delay
Directed rightward
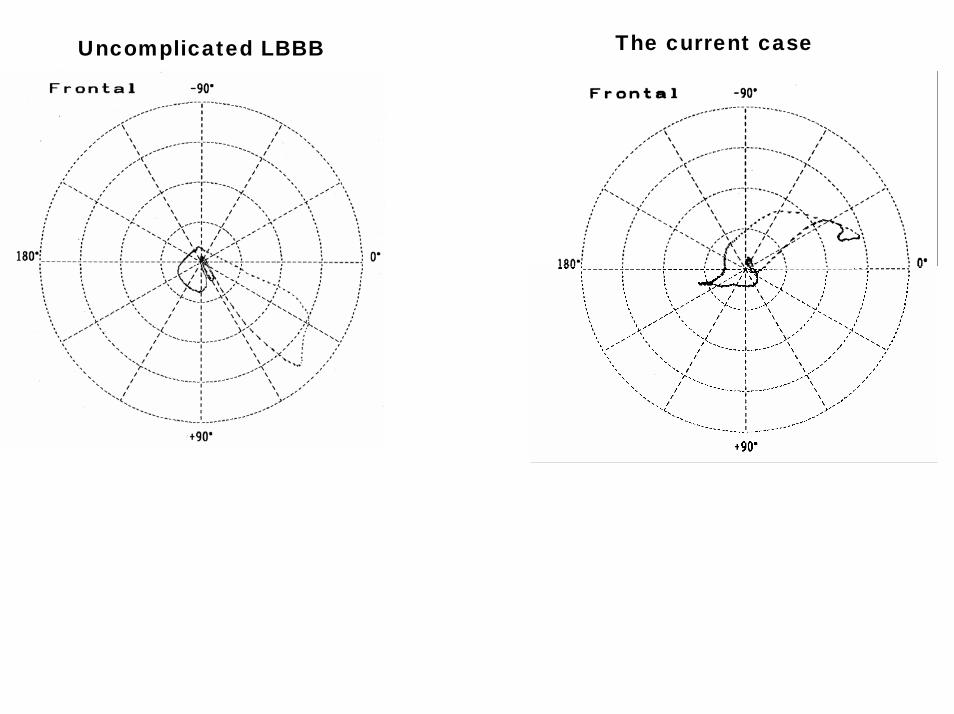
The current caseUncomplicated LBBB
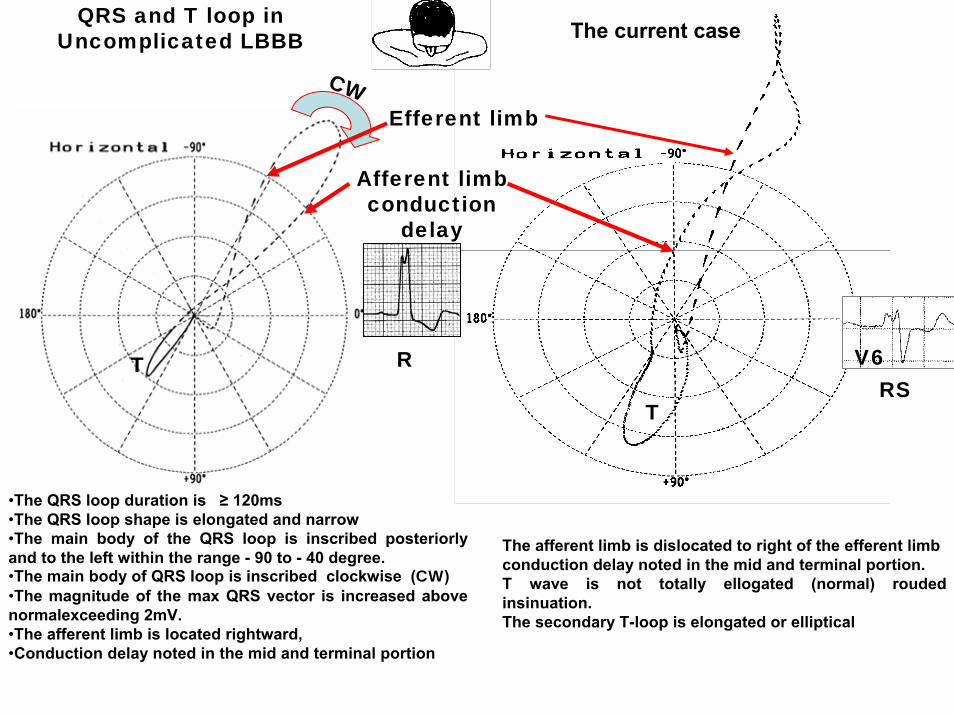
QRS and T loop inUncomplicated LBBB The current case
TRS
T V6
CW
Afferent limbconduction
delay
Efferent limb
R
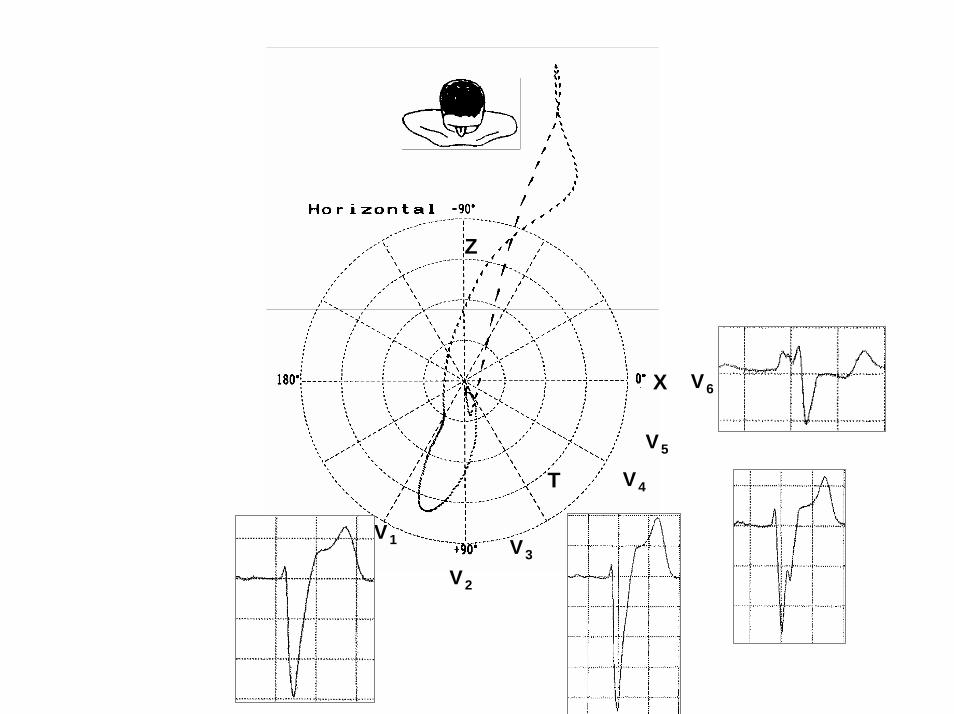
•The QRS loop duration is ≥ 120ms•The QRS loop shape is elongated and narrow•The main body of the QRS loop is inscribed posteriorlyand to the left within the range - 90 to - 40 degree.•The main body of QRS loop is inscribed clockwise (CW)•The magnitude of the max QRS vector is increased above normalexceeding 2mV.•The afferent limb is located rightward,•Conduction delay noted in the mid and terminal portion
The afferent limb is dislocated to right of the efferent limbconduction delay noted in the mid and terminal portion.T wave is not totally ellogated (normal) rouded insinuation.The secondary T-loop is elongated or elliptical
X
Z
V6
V1
V4
V5
V2
V3
Cabrera’s sign
Notch
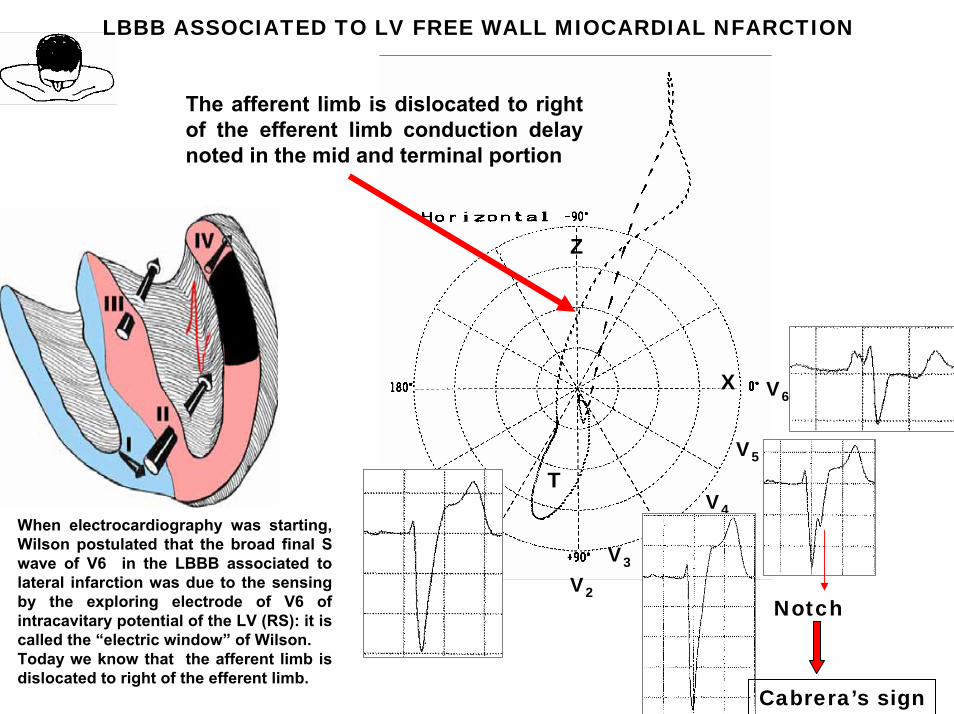
LBBB ASSOCIATED TO LV FREE WALL MIOCARDIAL NFARCTION
The afferent limb is dislocated to right of the efferent limb conduction delay noted in the mid and terminal portion
When electrocardiography was starting, Wilson postulated that the broad final S wave of V6 in the LBBB associated to lateral infarction was due to the sensing by the exploring electrode of V6 of intracavitary potential of the LV (RS): it is called the “electric window” of Wilson.Today we know that the afferent limb is dislocated to right of the efferent limb.
T
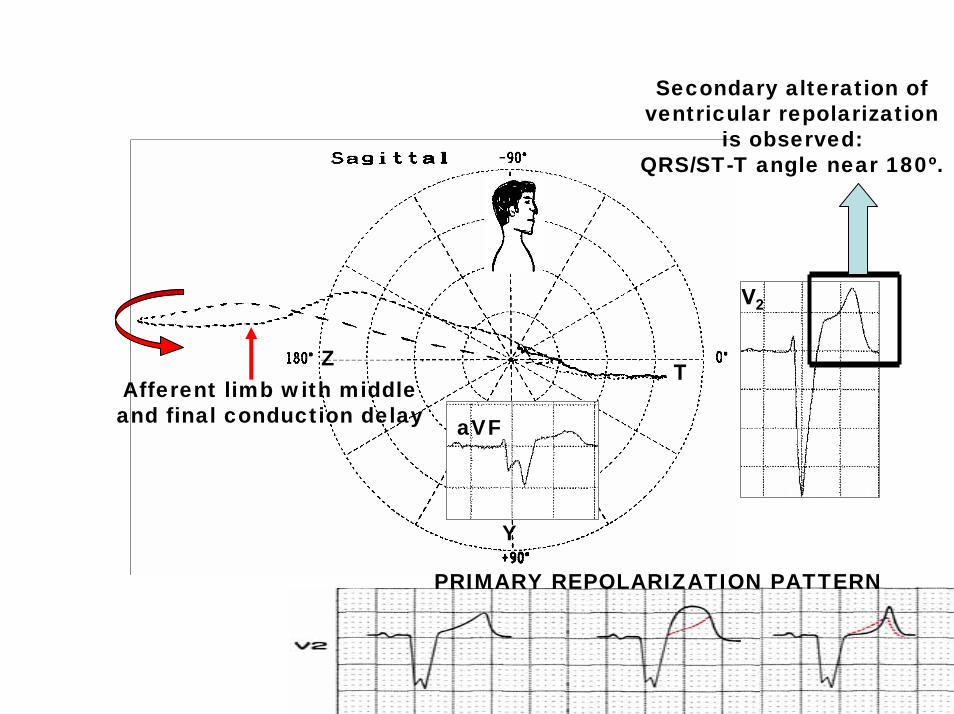
Y
Z
aVF
Afferent limb with middle and final conduction delay
T
V2
Secondary alteration of ventricular repolarization
is observed: QRS/ST-T angle near 180º.
PRIMARY REPOLARIZATION PATTERN
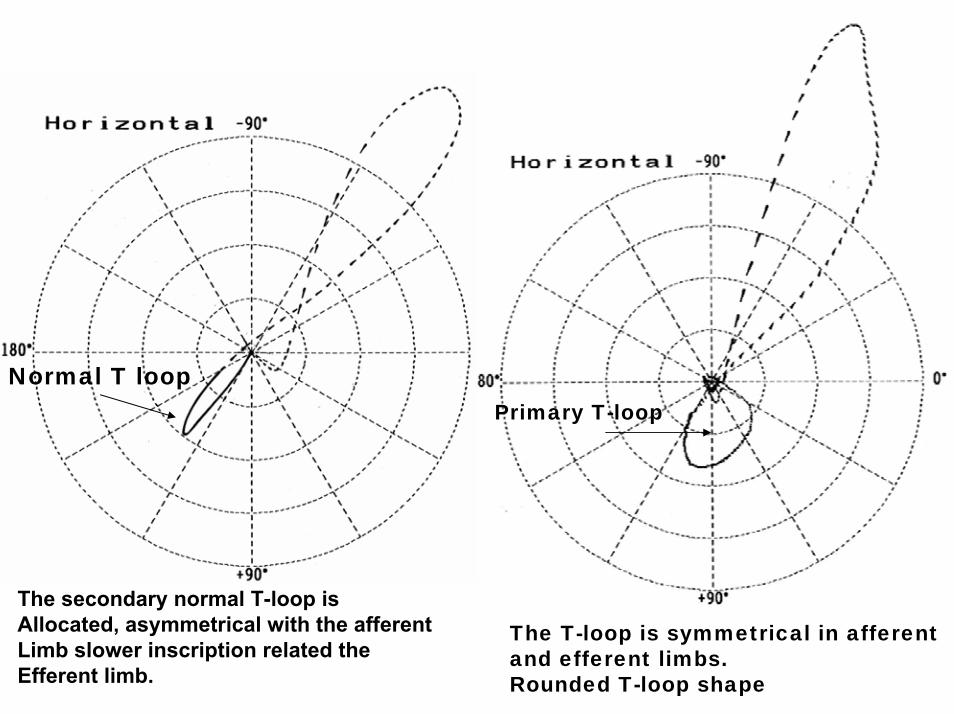
The T-loop is symmetrical in afferent and efferent limbs.Rounded T-loop shape
Normal T loopPrimary T-loop
The secondary normal T-loop isAllocated, asymmetrical with the afferentLimb slower inscription related theEfferent limb.

Very wide QRS duration = 180ms suggesting severe LV enlargement
Prolonged PR interval
The mean patient age at LBBB diagnosis was relatively elderly, and the LBBB incidence increased progressively with advancing age. Hypertension, coronary artery disease, left ventricular hypertrophy, ST-T abnormalities, and an increased cardiothoracic ratio were associated with LBBB. LBBB predicted for mortality from heart failure but not for all-cause mortality, independent of age, gender, and underlying disease1.
1. Imanishi R, Seto S, Ichimaru S, et al. Prognostic significance of incident complete left bundle branch block observed over a 40-year period. Am J Cardiol. 2006; 98: 644-648.
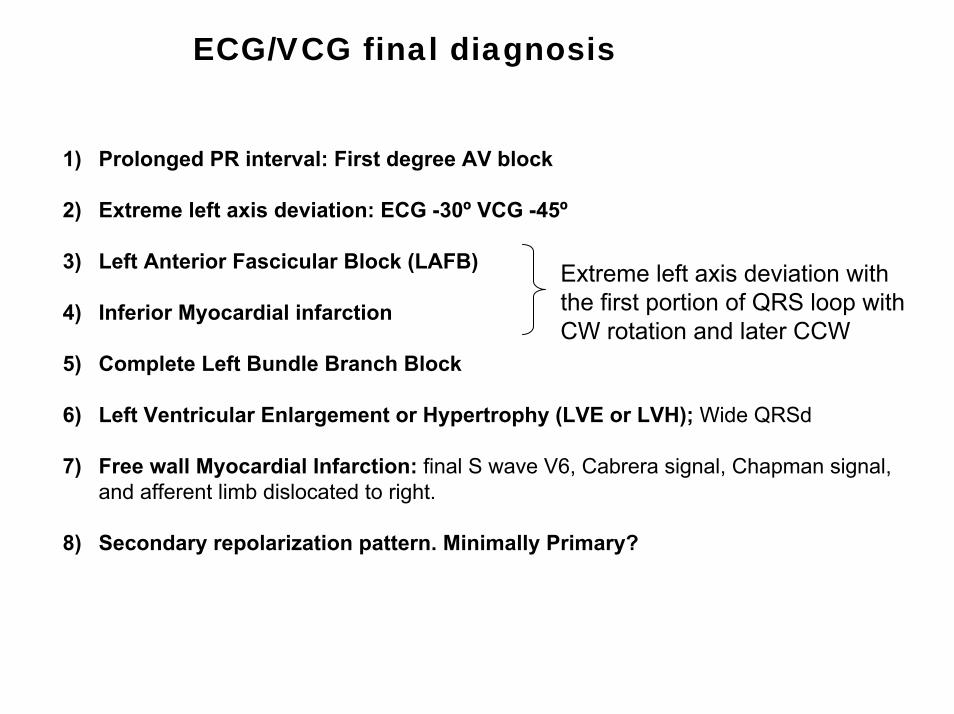
ECG/VCG final diagnosis
1) Prolonged PR interval: First degree AV block
2) Extreme left axis deviation: ECG -30º VCG -45º
3) Left Anterior Fascicular Block (LAFB)
4) Inferior Myocardial infarction
5) Complete Left Bundle Branch Block
6) Left Ventricular Enlargement or Hypertrophy (LVE or LVH); Wide QRSd
7) Free wall Myocardial Infarction: final S wave V6, Cabrera signal, Chapman signal, and afferent limb dislocated to right.
8) Secondary repolarization pattern. Minimally Primary?
Extreme left axis deviation with the first portion of QRS loop with CW rotation and later CCW

Elderly patients (aged 60-85 years) with chronic heart failure (NYHA class II-IV CHF) and LBBB had statistically significant increases of end diastolic and systolic dimensions, end diastolic and systolic volumes, sphericity index, long axis, decreases of relative thickness of the left ventricle, interventricular septum, and left low ventricular ejection fraction. Pronounced mitral regurgitation also was more frequent in patients with LBBB. During follow up 14/34 patients (41.2%) with LBBB and 19/74 patients (25.7%) without LBBB died. There were 10 and 9 sudden deaths among patients with and without LBBB, respectively1.
The reports in the literature indicate a large increase in mortality when LBBB develops in patients over 44 years of age2.
1. Larina VN, Bart BIa.Structural-functional peculiarities of the heart and survival of elderly patients with chronic heart failure and left bundle branch block Kardiologiia. 2009;49:16-21.
2. Deharo JC.Left bundle branch block. Electrocardiographic and prognostic aspectsArch Mal Coeur Vaiss. 2000 Apr;93:31-37.

Patients with LBBB and concomitant coronary artery disease (CAD) have a worse prognosis than those with LBBB without CAD. In addition, subjects with CAD and concomitant LBBB have a higher cardiovascular mortality than those with a similar extent of CAD but without LBBB. Because the presence of LBBB makes the noninvasive identification of CAD problematic, patients with LBBB often are referred for coronary angiography to assess the presence and severity of CAD. Those with CAD were likely to be older, Caucasian, and men; they were more likely to have angina pectoris, MI, and diabetes mellitus; and they were more likely to have a left ventricular ejection fraction (LVEF) <0.50. In contrast, patients with heart failure (HF) were less likely to have CAD1.
In survivors of myocardial infarction (MI), new LBBB is associated with adverse outcomes, In post-MI survivors with left ventricular (LV) systolic dysfunction and/or heart failure (HF), new LBBB was an independent predictor of all major adverse cardiovascular outcomes during long-term follow-up. This readily available ECG marker should be considered a major risk factor for long-term cardiovascular complications in high-risk patients after MI2.
The presence of LBBB on admission ECG in patients who have AMI is an independent predictor of in-hospital mortality. Because 85% of deaths in patients who have LBBB occur within the first week, these patients should be recognized early and receive prompt and aggressive treatment (thrombolysis)3.
1. Abrol R, Trost JC, Nguyen K,et al. Predictors of coronary artery disease in patients with left bundle branch block undergoing coronary angiography. Am J Cardiol. 2006;98:1307-1310.
2. Stephenson K, Skali H, McMurray JJ, et al. Long-term outcomes of left bundle branch block in high-risk survivors of acute myocardial infarction: the VALIANT experience. Heart Rhythm. 2007; 4:308-313.
3. Guerrero M, Harjai K, Stone GW, et al. Comparison of the prognostic effect of left versus right versus no bundle branch block on presenting electrocardiogram in acute myocardial infarction patients treated with primary angioplasty in the primary angioplasty in myocardial infarction trials. Am J Cardiol. 2005; 96: 482-488
In case of AMI and a BBB major diagnostic and prognostic issues should be addressed with different considerations, depending on the presence of a LBBB or a RBBB, distinguishing new or presumably new BBB, considering the possibility that the BBB masks ECG features of MI with ST-segment elevation. Wong et al. analysis of HERO-2 trial demonstrates that in the setting of an anterior STEMI, the presence of an RBBB, whatever its onset, is associated with a higher risk of death. The same analysis shows as RBBB associated with an inferior infarction does not portend a worse prognosis independently of its onset. Patients with LBBB already present at randomization were found to have worse pre-infarction characteristics, responsible, by itself, for the worst prognosis. However, the occurrence of an LBBB after randomization indicates a 'true' ischaemic conduction damage, thus carrying an independent negative prognostic value due to the large percentage of myocardium involved. HERO-2 trial, showing prognostic differences between different clinical presentations, underlines the importance to be familiar with the mechanisms related to BBBs and with the prognostic implications of BBBs in the setting of an AMI.Patients with LBBB, RBBB, or indeterminate ventricular conduction disturbances show longer repolarization duration than patients without these conduction disturbances, and QT (RR,QRS) and JT(RR) intervals reflect better than QTc repolarization duration in patients with conduction disturbances. QT(RR) and JT(RR) intervals significantly and independently predict mortality in patients after MI with conduction disturbances1.
1. Piotrowicz K, Zareba W, McNitt S, et al. Repolarization duration in patients with conduction disturbances after myocardial infarction. Am J Cardiol. 2007; 99:163-168.
The prognostic implications in HF with preserved systolic function (HF-PSF) are less well understood. The simple clinical finding of BBB is a powerful independent predictor of worse clinical outcomes in patients with HF and reduced LVEF. It is less frequent, with a more modest predictive effect, in patients with preserved systolic function1.Criteria of cardiac resynchronization therapy (CRT) from American College of Cardiology and American Heart Association guidelines are:LVEF ≤ 0.35;]
Functional class III or IV(NYHA). Patients with class III or IV HF are candidates for CDT regardless of underlying etiology if cardiac recompensation to class III is at least temporarily successful. CRT has a beneficial effect on clinical symptoms, exercise capacity, and systolic LV performance in patients with HF. HF in functional state NYHA II should be regarded as a CRT indication is currently being investigated in the randomized RAFT and MADIT-CRT trials.QRS interval > 130 ms particularly if LBBB is present. Patients with CLBBB and a QRS duration of 120-130 ms seem to benefit if echocardiographic criteria demonstrate ventricular dyssynchrony. Since a multiplicity of echocardiographic criteria of ventricular dyssynchrony exists which is neither standardized nor evaluated in large-scale randomized trials, ventricular dyssynchrony on echocardiography alone cannot be regarded as an established indication for CRT without a QRS complex ≥120 ms. whether Sinus rhythm. In addition, available data also suggest an indication for CRT in patients with atrial fibrillation if the other criteria listed above are met.
1. Hawkins NM, Wang D, McMurray JJ, et al. Prevalence and prognostic impact of bundle branch block in patients with heart failure: evidence from the CHARM programme. Eur J Heart Fail. 2007; 9:510-517.
CRT is possible using biventricular pacing or ICD systems has to be highly differentiated to optimize the proportion of patients who derive significant symptomatic benefit from this therapy, on the one hand, and to avoid this invasive treatment in patients with a low probability of clinical success of CRT, on the other hand.In patients with nonischaemic cardiomyopathy, the LVEF was improved from 28% to 37%, and in patients with ischaemic cardiomyopathy, the LVEF was improved from 30% to 36%. No significant difference of the improvement was found between the two groups. CRT could significantly improve cardiac function in patients with chronic HF regardless of the underlying heart disease1.ECG abnormalities that were associated with postoperative MI were a RBBB and a LBBB. Similar results were found for all-cause mortality. Bundle branch blocks identified on the preoperative ECG were related to prediction of postoperative MI and death but did not improve prediction beyond risk factors identified on patient history2. Cardiac resynchronization therapy (CRT) provides a therapeutic option for patients with CHF NYHA class III or IV, sinus rhythm, and LBBB with QRS ≥120ms( CLBBB). Some authors do not consider QRS pattern. Studies show that only patients with LBBB benefit form CRT, and not patients with RBBB or nonspecific intraventricular conduction delay. Additionally, approximately 30% diagnosed with LBBB by ECG criteria may not have true complete LBBB , but likely have a combination of LVH and LAFB. Stricter criteria for CRT for Complete LBBB must include QRS duration ≥ 140ms for men and ≥ 130ms for women and with mid-QRS notching or slurring in ≥2mm contiguous leads.
1. Hua W, Niu HX, Wang FZ, et al. Short-term effect of cardiac resynchronization therapy in patients with ischaemic or nonischaemic cardiomyopathy. Chin Med J (Engl). 2006; 119:1507-1510.
2. van Klei WA, Bryson GL, Yang H,et al. The value of routine preoperative electrocardiography in predicting myocardial infarction after noncardiac surgery. Ann Surg. 2007;246:165-170.
3. Strauss, DG, Selvester RH, Galen S, et al. Defining Left Bundle Branch Block in the Era of Cardiac Resynchronization Therapy. Am J Cardiol 2011; 107: 927-934.
The results of MADIT-CRT, as well as the extended follow-up of the REVERSE substudy of the European patient cohort, have shown that prevention of HF progression can be well accomplished with CRT and implantable cardioverter-defibrillator (ICD) backup (CRT-D). HF events and death occurred significantly less often in patients with CRT-D than in those with an ICD only. A clinically important reversal of ventricular remodeling with reduced ventricular volumes and increased LVEF was found in the CRT-D-treated patients. CRT in asymptomatic or mildly symptomatic HF patients.( NYHA class I or II HF) the most benefit was demonstrated in patients showing a "classic" LBBB ECG pattern and in female patients1.
Structural myocardial remodelling due to CRT has been described extensively. CRT results in an electrical remodelling with a reduction of the intrinsic QRS duration. A significant decrease in intrinsic QRS duration was observed in responders, only a slight decrease was seen in non-responders2.
In hyper responder patients (they fulfilled concurrently the two following criteria: functional recovery (NYHA class I or II) and normalization of LV ejection fraction (LVEF).), "normalization" of LV function after CRT persists as long as pacing is maintained with an excellent survival3.
1. Klein HU. Cardiac resynchronization therapy in asymptomatic or mildly symptomatic heart failure patients. Curr Treat Options Cardiovasc Med. 2010 Oct;12(5):431-42.
2. Mischke K, Knackstedt C, Fache K, et al.. Electrical remodelling in cardiac resynchronization therapy: decrease in intrinsic QRS duration. Acta Cardiol. 2011 Apr;66(2):175-80.
3. Castellant P, Orhan E, Bertault-Valls V, Is "hyper response" to cardiac resynchronization therapy in patients with nonischemic cardiomyopathy a recovery, a remission, or a control? Ann Noninvasive Electrocardiol. 2010 Oct;15(4):321-7.