new ischemic stroke and outcomes with vorapaxar versus placebo · new ischemic stroke and outcomes...
TRANSCRIPT

J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y VO L . 6 4 , N O . 2 2 , 2 0 1 4
ª 2 0 1 4 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R I N C . h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 4 . 0 7 . 9 9 7
New Ischemic Stroke and OutcomesWith Vorapaxar Versus Placebo
Results From the TRA 2�P-TIMI 50 TrialMarc P. Bonaca, MD, MPH,* Benjamin M. Scirica, MD, MPH,* Eugene Braunwald, MD,* Stephen D. Wiviott, MD,*Shinya Goto, MD,y Dennis W. Nilsen, MD,zx Vernon Bonarjee, MD,zx Sabina A. Murphy, MPH,*David A. Morrow, MD, MPH*
ABSTRACT
Fro
Me
Me
xDpo
As
Sm
Ro
Ca
Ro
Wo
Gil
Fo
Up
Me
rec
BACKGROUND Vorapaxar, a novel antiplatelet therapy, reduces thrombotic events in patients with a history of
myocardial infarction (MI) or peripheral artery disease (PAD); however, because of an increased risk of intracranial
hemorrhage, it is contraindicated in patients with a history of stroke.
OBJECTIVES The aim of this study was to investigate the incidence of new ischemic stroke and subsequent death or
intracerebral hemorrhage in patients with MI or PAD and no cerebrovascular disease (CVD) treated with vorapaxar.
METHODS The TRA 2�P-TIMI 50 (Trial to Assess the Effects of Vorapaxar in Preventing Heart Attack and Stroke in
Patients With Atherosclerosis-Thrombolysis In Myocardial Infarction 50) was a randomized, double-blind, placebo-
controlled trial of vorapaxar 2.5 mg daily in 26,449 patients with atherosclerosis, stratified by qualifying disease (MI,
PAD, or CVD). A total of 20,170 patients with MI/PAD, but no CVD, were enrolled.
RESULTS In patients with MI/PAD and no prior stroke or transient ischemic attack, vorapaxar reduced first ischemic
stroke (hazard ratio [HR]: 0.57, 95% confidence interval [CI]: 0.43 to 0.75; p < 0.001). The risk of hemorrhagic con-
version after stroke (HR: 1.19, 95% CI: 0.49 to 2.91; p ¼ 0.70) or death (HR: 1.09, 95% CI: 0.57 to 2.07; p ¼ 0.79) during
follow-up was not significantly increased with vorapaxar in patients who had a new ischemic stroke (n ¼ 204). Although
hemorrhagic stroke was increased (HR: 2.79, 95% CI: 1.00 to 7.73; p ¼ 0.049), overall stroke was significantly reduced
(HR: 0.67, 95% CI: 0.52 to 0.87; p ¼ 0.002).
CONCLUSIONS Vorapaxar reduces ischemic stroke in patients with MI or PAD and no known CVD. There does not
appear to be a significant increase in the risk of hemorrhagic conversion or death in patients who experienced a first
ischemic stroke on vorapaxar. Although primary hemorrhagic stroke is increased, vorapaxar reduces the total incidence of
stroke. (Trial to Assess the Effects of Vorapaxar (SCH 530348; MK-5348) in Preventing Heart Attack and Stroke in
Patients With Atherosclerosis [TRA 2�P-TIMI 50]; NCT00526474) (J Am Coll Cardiol 2014;64:2318–26) © 2014 by the
American College of Cardiology Foundation.
m the *TIMI Study Group, Cardiovascular Division, Department of Medicine, Brigham and Women’s Hospital and Harvard
dical School, Boston, Massachusetts; yDepartment of Medicine (Cardiology), Tokai University School of Medicine, Institute of
dical Science, Isehara, Japan; zDepartment of Cardiology, Stavanger University Hospital, Stavanger, Norway; and the
epartment of Clinical Science, Faculty of Medicine and Dentistry, University of Bergen, Bergen, Norway. This study was sup-
rted by a grant fromMerck & Co. The TIMI Study Group has received significant research grant support from Accumetrics, Amgen,
traZeneca, Beckman Coulter, Bristol-Myers Squibb, CV Therapeutics, Daiichi-Sankyo Co. Ltd., Eli Lilly and Company, Glaxo-
ithKline, Integrated Therapeutics, Merck & Co., Nanosphere, Novartis Pharmaceuticals, Nuvelo, Ortho-Clinical Diagnostics, Pfizer,
che Diagnostics, Sanofi, Sanofi-Synthelabo, Siemens Medical Solutions, and Singulex. Dr. Bonaca was supported by a Research
reerDevelopmentAward (K12HL083786) from theNational Heart, Lung, and Blood Institute; andhas received consulting fees from
che Diagnostics, Merck & Co., AstraZeneca, and Bayer. Dr. Scirica has received research grants via the TIMI Study and Brigham and
men’s Hospital from AstraZeneca, Bristol-Myers Squibb, Daiichi-Sankyo, GlaxoSmithKline, Johnson & Johnson, Bayer Healthcare,
ead, Eisai, andMerck & Co.; and consulting fees fromAstraZeneca, GEHealthcare, Gilead, Lexicon, Arena, Eisai, St. Jude’sMedical,
rest Pharmaceuticals, Bristol-Myers Squibb, BostonClinical Research Institute, Covance, University ofCalgary, andElsevierPractice
date Cardiology. Dr. Braunwald has received research grants (institutional) from Daiichi-Sankyo, Duke University, AstraZeneca,
rck & Co., and GlaxoSmithKline; has received fees for lectures from Daiichi-Sankyo, Menarini International, and Medscape; has
eived fees as a consultant forTheMedicinesCompanyandSanofi; andhasbeen anunpaid consultant andhas givenunpaid lectures

AB BR E V I A T I O N S
AND ACRONYM S
CI = confidence interval
CVD = cerebrovascular disease
DAPT = dual antiplatelet
therapy
HR = hazard ratio
J A C C V O L . 6 4 , N O . 2 2 , 2 0 1 4 Bonaca et al.D E C E M B E R 9 , 2 0 1 4 : 2 3 1 8 – 2 6 Vorapaxar and New Stroke
2319
V orapaxar is a novel thrombin receptor antag-onist that has potent antiplatelet effectsand reduces atherothrombotic events in
patients with stable atherosclerotic vascular disease(1). This benefit is balanced against an increasedrisk of bleeding, including a risk of intracranial hem-orrhage that is highest in patients with a prior strokeor transient ischemic attack (TIA) (1,2). A similar
SEE PAGE 2327
MI = myocardial infarction
MRS = modified Rankin Scale
PAD = peripheral
artery disease
TIA = transient ischemic attack
heterogeneous response by symptomatic vascularterritory was observed with other potent antiplateletagents and is reflected in current guidelines forpatients with cerebrovascular disease (CVD) (3–8).Vorapaxar was recommended for approval for clinicaluse in the United States in patients with priormyocardial infarction (MI) or peripheral artery dis-ease (PAD), but no prior stroke or TIA (9). Becausethis population is at a heightened risk of a firstischemic stroke, and any such event occurring on vor-apaxar could expose a patient to an increased riskof harm, understanding the incidence of stroke andsubsequent outcomes with vorapaxar in this popula-tion will be important to clinicians (5,10,11).
The TRA 2�P-TIMI 50 (Trial to Assess the Effects ofVorapaxar in Preventing Heart Attack and Stroke inPatients With Atherosclerosis-Thrombolysis InMyocardial Infarction 50) studied vorapaxar for sec-ondary prevention of atherothrombosis in patientswith stable atherosclerosis, including prior MI,symptomatic PAD, or ischemic stroke (1,12). We pre-viously characterized the risks of intracranial hem-orrhage and total stroke in the overall population andin the key subgroup of patients who qualified for thetrial with prior MI, including those with a concomi-tant history of CVD (13).
The present report is, therefore, focused on the keyclinical issue of the incidence of first stroke andassociated outcomes in patients with history of MI orPAD, and no history of CVD, who are treated withvorapaxar in addition to standard antiplatelet
for Merck & Co. Dr. Wiviott has received research grants from Merck & Co., A
Eli Lilly and Company, AstraZeneca, Johnson & Johnson, Arena, St. Jude
Squibb. Dr. Goto has received honoraria from Eisai, Sanofi, Otsuka, Bayer,
Japan, Tanabe-Mitsubishi, Takeda, Daiichi-Sankyo, Mochida, and MSD; an
ringer Ingelheim, Otsuka, and Daiichi-Sankyo. Dr. Morrow has received resea
Beckman Coulter, BG Medicine, BRAHMS, Bristol-Myers Squibb, Critical Diag
Lilly and Company, GlaxoSmithKline, Johnson & Johnson, Merck & Co., Nova
Singulex; and has received consulting fees from Abbott Laboratories, BG Med
Instrumentation Laboratory, Johnson & Johnson, Konica Minolta, Merck & Co
authors have reported that they have no relationships relevant to the conte
Listen to this manuscript’s audio summary by JACC Editor-in-Chief Dr. Vale
You can also listen to this issue’s audio summary by JACC Editor-in-Chief D
Manuscript received April 8, 2014; revised manuscript received June 23, 201
therapy. Because antiplatelet therapy hasdirectionally opposite effects on ischemicstroke versus primary hemorrhagic stroke, wenow discriminate between the occurrences ofthese forms of stroke and provide an analysisof their functional severity.
METHODS
STUDY POPULATION AND PROCEDURES. TRA2�P-TIMI 50 (Trial to Assess the Effects ofVorapaxar in Preventing Heart Attack andStroke in Patients With Atherosclerosis) was
a multinational, randomized, double-blind, placebo-controlled trial among 26,449 subjects with stableatherosclerotic vascular disease manifest by priorMI, PAD, or ischemic stroke (12). Details of the trialdesign were previously reported (1,12). Participantsentering the trial with a prior MI or PAD and withouta history of prior CVD, defined as prior stroke or TIA,are the basis for the present study. Patients with MIqualified on the basis of a history of spontaneous MIoccurring 2 weeks to 12 months before randomiza-tion (1). Patients with PAD qualified by a history ofintermittent claudication in conjunction with anankle-brachial index <0.85 or previous revasculari-zation for limb ischemia. Randomization was strati-fied according to the qualifying diagnosis (12).Patients were ineligible if they had a plannedrevascularization, a history of a bleeding diathesis,were receiving vitamin K antagonist therapy, or hada history of intracranial bleeding (12).Eligible patients were randomized in a 1:1 fashion toreceive vorapaxar 2.5 mg daily or matching placebo.After the data safety monitoring board’s recommen-dation, the protocol was amended to discontinue thestudy drug in patients with a history of stroke orat the time of an occurrence of a new stroke during thetrial (1,12). Randomization was stratified both byqualifying disease state and by the pre-randomizationvariable of planned thienopyridine use (12).
straZeneca, and Eisai; and has been a consultant for
Medical, Icon Medical Imaging, and Bristol-Myers
Novartis, AstraZeneca, Asteras, Pfizer, Medtronics-
d has received research grants from Sanofi, Boeh-
rch grant support from Abbott, Amgen, AstraZeneca,
nostics, CV Therapeutics, Daiichi-Sankyo Co. Ltd., Eli
rtis Pharmaceuticals, Roche Diagnostics, Sanofi, and
icine, Daiichi-Sankyo, Eli Lilly and Company, Gilead,
., Novartis, Roche Diagnostics, and Servier. All other
nts of this paper to disclose.
ntin Fuster.
r. Valentin Fuster.
4, accepted July 15, 2014.

TABLE 1 Baseline Characteristics (Randomized Treatment Allocation)
Vorapaxar(n ¼ 10,080)
Placebo(n ¼ 10,090) p Value
Demographics
Age 60 (52–67) 60 (52–67) 0.90
Female 2,204 (22) 2,165 (21) 0.48
White race 8,939 (89) 8,924 (88) 0.54
Weight <60 kg 597 (6) 580 (6) 0.61
Clinical characteristics
Diabetes mellitus 2,385 (24) 2,377 (24) 0.86
Hypertension 6,520 (65) 6,564 (65) 0.57
Hyperlipidemia 8,554 (85) 8,573 (85) 0.85
Current smoker 2,143 (21) 2,214 (22) 0.24
Any coronary artery disease 9,341 (93) 9,377 (93) 0.44
Peripheral artery disease 2,313 (23) 2,364 (23) 0.42
CrCl at baseline <60 ml/min 1,186 (12) 1,131 (11) 0.21
Carotid revascularization 191 (2) 169 (2) 0.24
Coronary revascularization 7,953 (79) 7,954 (79) 0.91
Peripheral arterial revascularization 1,171 (12) 1,199 (12) 0.56
Baseline medical therapy
No antiplatelet therapy 77 (1) 102 (1) 0.061
Aspirin 9,746 (97) 9,756 (97) 0.99
Thienopyridine 7,177 (71) 7,215 (72) 0.63
Aspirin and thienopyridine therapy 6,920 (69) 6,983 (69) 0.39
ACE inhibitor or ARB 7,584 (75) 7,713 (76) 0.046
Values are median (interquartile range) or n (%).
ACE ¼ angiotensin-converting enzyme inhibitor; ARB ¼ angiotensin receptor blocker;CrCl ¼ creatinine clearance.
CENTRAL ILLUSTRATION Thrombin Activation of PAR-1 and Ischemic Stroke
Bonaca, M.P. et al. J Am Coll Cardiol. 2014; 64(22):2318–26.
Protease-activated receptor 1 (PAR-1) is expressed on platelets, endothelial and vascular smooth muscle cells and is activated by thrombin.
Vorapaxar is a PAR-1 antagonist, which blocks thrombin mediated platelet activation and reduces ischemic stroke.
Bonaca et al. J A C C V O L . 6 4 , N O . 2 2 , 2 0 1 4
Vorapaxar and New Stroke D E C E M B E R 9 , 2 0 1 4 : 2 3 1 8 – 2 6
2320
ENDPOINTS. The primary efficacy and safety defini-tions, as well as the main trial results, were previ-ously described (1). Stroke was a pre-specifiedcomponent of the overall trial primary endpoint.A stroke endpoint was defined as the new onset offocal neurological symptoms lasting more than 24 h orevidence of new infarct on brain imaging, even ifsymptoms were <24 h in duration (12). Strokeevents were further classified as ischemic or pri-mary hemorrhagic. Ischemic strokes associated withhemorrhagic conversion were also identified. Non-hemorrhagic infarction with hemorrhagic conversionwas defined as evidence of cerebral infarction, withblood felt to represent hemorrhagic conversion, andnot a primary hemorrhage, on the basis of location andimaging characteristics. Microhemorrhage evidenton magnetic resonance imaging, whether in the cortexor deep brain structures, was not considered to meetthe definition of hemorrhagic conversion. All poten-tial stroke events were adjudicated by a clinical eventscommittee comprised of neurology specialists blin-ded to treatment allocation (12).
CLINICAL ASSESSMENT. Site investigators weretrained in the assessment of disability after stroke us-ing the modified Rankin Scale (MRS). Investigatorswere instructed to complete an assessment at baseline,

FIGURE 1 Kaplan-Meier Curves for Any Stroke During Follow-Up by
Treatment Allocation
1.8% Placebo Vorapaxar
1.6%
1.4%
1.2%
1.0%
0.8%
0.6%
0.4%
0.2%
0.0%0 180 360 540
Any
Stro
ke (%
)
Days
720 900
1.65%
HR 0.6795% CI 0.52, 0.87,
P=0.002
1.20%
1080
Stroke during follow-up with vorapaxar versus placebo is shown. Stroke events include
ischemic stroke, ischemic stroke with hemorrhagic conversion, and hemorrhagic stroke.
Outcomes out to 1,080 days (3 years) are shown. CI ¼ confidence interval;
HR ¼ hazard ratio.
FIGURE 2 Kaplan-Meier Curves for Ischemic Stroke During Follow-Up by
Treatment Allocation
1.6% VorapaxarPlacebo
1.4%
1.2%
1.0%
0.8%
0.6%
0.4%
0.2%
0.0%0 180 360 540
Days
Isch
emic
Str
oke
(%)
720
1.47%HR 0.57
95% CI 0.43 – 0.75
P<0.001
0.88%
900 1080
Ischemic stroke during follow-up with vorapaxar versus placebo is shown. Stroke events
include ischemic stroke. Outcomes out to 1,080 days (3 years) are shown. Abbreviations
as in Figure 1.
J A C C V O L . 6 4 , N O . 2 2 , 2 0 1 4 Bonaca et al.D E C E M B E R 9 , 2 0 1 4 : 2 3 1 8 – 2 6 Vorapaxar and New Stroke
2321
at stroke presentation, at discharge from stroke hos-pitalization, and for the remainder of follow-up. Scoreson the MRS increase with greater disability and rangefrom 0 (no symptoms) to a maximum of 6 (death), witha score of 3 indicating moderate disability (14).
STATISTICAL METHODS. Baseline characteristics werecompared using the chi-square test for categoricalvariables and the Wilcoxon rank sum test for contin-uous variables. The efficacy analyses were performedusing a Cox proportional hazards model, with theinvestigational treatment allocation, qualifyingatherosclerosis (MI or PAD), and planned use of athienopyridine as covariates. The Kaplan-Meiermethod was used to calculate cumulative eventrates at 3 years. Efficacy data were analyzed on anintention-to-treat basis. Safety analyses were per-formed among patients who received 1 or more dosesof study drug, and included events through 60 daysafter premature cessation of study therapy, or 30 daysafter a final visit at the conclusion of the trial.Outcomes of interest for this analysis after a firstischemic stroke were death and hemorrhagic con-version. Analyses were performed using Stata version12.1 (Stata Corp., College Station, Texas).
RESULTS
BASELINE CHARACTERISTICS. A total of 20,170patients qualified for the trial with MI or PAD and hadno history of CVD (Online Figure 1). Median follow-up in this cohort was 31 months, representing over52,000 patient-years of observation. Their baselinecharacteristics are shown in Table 1. Backgroundtreatment included aspirin in 97%, thienopyridine in71%, and dual antiplatelet therapy (DAPT) in 69%.Experimental treatment allocation was well balanced(Table 1). Therewas frequent use of statin therapy (93%in those on vorapaxar and 94% in those on placebo)and angiotensin-converting enzyme inhibitor orangiotensin receptor blocker therapy (76% overall).
VORAPAXAR AND TOTAL STROKE (ISCHEMIC AND
HEMORRHAGIC). During follow-up, there were 243new strokes occurring at a median of 507 daysfollowing randomization. Median follow-up was 358days after a first stroke occurring during participationin the trial. The majority of new strokes wereischemic strokes without hemorrhagic conversion(n ¼ 187). Ischemic stroke with hemorrhagic conver-sion occurred in 20 patients, primary hemorrhagicstroke in 19 patients, and nonclassified stroke in 23patients. Compared with placebo, vorapaxar led to asignificant reduction in new stroke in patients withMI or PAD and no prior stroke or TIA (1.20% vs. 1.65%,
hazard ratio [HR]: 0.67, 95% confidence interval [CI]:0.52 to 0.87; p ¼ 0.002) (Figure 1).
ISCHEMIC STROKE. Vorapaxar reduced ischemicstroke (74 vs. 130, 0.88% vs. 1.47%, HR: 0.57, 95% CI:

TABLE 2 Efficacy and Bleeding Endpoints
EndpointVorapaxar
(n ¼ 10,080)Placebo
(n ¼ 10,090) HR (95% CI) p Value
Overall efficacy
CVD/MI/stroke 688 (7.9) 851 (9.5) 0.80 (0.73–0.89) <0.001
CVD/MI/stroke/urgent coronaryrevascularization
896 (10.1) 1,073 (11.8) 0.83 (0.76–0.90) <0.001
Stroke endpoints*
Any stroke 98 (1.2) 145 (1.6) 0.67 (0.52–0.87) 0.002
All ischemic stroke 74 (0.9) 130 (1.5) 0.57 (0.43–0.75) <0.001
Ischemic stroke withouthemorrhagic conversion
69 (0.8) 118 (1.3) 0.58 (0.43–0.78) <0.001
Ischemic stroke withhemorrhagic conversion
8 (0.1) 12 (0.1) 0.67 (0.27–1.63) 0.38
Primary hemorrhagic stroke 14 (0.2) 5 (0.1) 2.79 (1.00–7.74) 0.049
Transient ischemic attack 48 (0.5) 55 (0.7) 0.88 (0.59–1.29) 0.50
Bleeding
GUSTO moderate/severe bleed† 312 (3.8) 202 (2.5) 1.57 (1.32–1.88) <0.001
GUSTO severe bleed† 105 (1.3) 87 (1.1) 1.22 (0.92–1.62) 0.16
Fatal bleed 17 (0.3) 14 (0.2) 1.23 (0.60–2.49) 0.57
Values are n (%) except as indicated. *Any stroke includes 23 strokes of unknown subtype. †Includes fatalbleeding.
CI ¼ confidence interval; CVD ¼ cardiovascular disease; GUSTO ¼ Global Utilization Of Streptokinase and tPAfor Occluded arteries; HR ¼ hazard ratio; MI ¼ myocardial infarction.
FIGURE 3 First Strokes Occurring During Follow-Up by
Stroke Type and Treatment Allocation
160
Ischemic Stroke (no hemorrhagic conversion)
Ischemic stroke (with hemorrhagic conversion)Primary Hemorrhagic stroke
140
120
100
80
60
40
20
PlaceboN=10,090 N=10,080
N=20,170P<0.0014
12
66
12
118
Patie
nts (
N)
Vorapaxar0
7
First strokes occurring during follow-up are shown by stroke type
for patients randomized to vorapaxar or placebo.
Bonaca et al. J A C C V O L . 6 4 , N O . 2 2 , 2 0 1 4
Vorapaxar and New Stroke D E C E M B E R 9 , 2 0 1 4 : 2 3 1 8 – 2 6
2322
0.43 to 0.75; p < 0.001) (Figure 2, Table 2), includingischemic stroke without hemorrhagic conversion(0.83% vs. 1.33%, HR: 0.58, 95% CI: 0.43 to 0.78;p < 0.001), with a consistent trend for ischemic strokewith hemorrhagic conversion (0.10% vs. 0.14%, HR:0.67, 95% CI: 0.27 to 1.63; p ¼ 0.38) (Figure 3, Table 2).New transient ischemia was numerically lower inpatients randomized to vorapaxar compared withplacebo (0.53% vs. 0.65%, HR: 0.88; 95% CI: 0.59 to0.1.29; p ¼ 0.50) (Table 2).
These findings with respect to new ischemicstroke were similar among patients who entered thetrial on the basis of MI or PAD (Table 3). In particular,among patients who qualified with prior MI, vor-apaxar reduced the risk of any stroke by 38% and ofischemic stroke by 49% (Table 3). In patientsenrolled with MI who we previously identified as atparticularly low risk for bleeding complications(age <75 years, weight $60 kg, no history of stroke orTIA; n ¼ 14,909) (10), vorapaxar reduced the occur-rence of any stroke by 40% and ischemic stroke by53% (Online Table 1).
OUTCOMES AFTER ISCHEMIC STROKE. In thosepatients who experienced a first ischemic strokeduring the trial, there was no significant increase inthe hazard of hemorrhagic conversion with vorapaxarcompared with placebo (8 of 66 with vorapaxar vs.12 of 118 with placebo, HR: 1.19, 95% CI: 0.49 to 2.91;p ¼ 0.70). Moreover, there was no statistically sig-nificant interaction between planned thienopyridine
therapy and the effect of vorapaxar on the develop-ment of ischemic stroke with hemorrhagic conversion(p for interaction ¼ 0.56). In addition, there was nodetectable increase in the hazard of death duringfollow-up after a first ischemic stroke with vorapaxarcompared with placebo (HR: 1.09, 95% CI: 0.57 to2.07; p ¼ 0.79) (Figure 4).
At the time of a first ischemic stroke, 72% (53 of 74)of patients randomized to vorapaxar and 70% (91 of130) of patients randomized to placebo were on studytreatment. When restricting the analysis to thosepatients taking study treatment at the time of theirfirst ischemic stroke, there was no increase in subse-quent hemorrhagic conversion with vorapaxar com-pared with placebo, whether or not the study drugwas stopped within 30 days after the stroke (3 of 20with vorapaxar vs. 5 of 39 on placebo) or continuedfor 30 days or longer (3 of 33 with vorapaxar vs. 3 of 52on placebo).
HEMORRHAGIC STROKE. When considering allpatients with MI or PAD and no prior stroke or TIA,the rate of ischemic stroke with hemorrhagic con-version was similar with vorapaxar compared withplacebo (0.10% with vorapaxar vs. 0.14% withplacebo, HR: 0.67, 95% CI: 0.27 to 1.63; p ¼ 0.38)(Table 2, Figure 3). Primary hemorrhagic stroke wasincreased with vorapaxar (0.17% vs. 0.06%, HR: 2.79;95% CI: 1.00 to 7.74; p ¼ 0.049) (Table 2, Figure 3).Rates of fatal bleeding of any kind (0.3% vs. 0.2%;p ¼ 0.57) were similar with vorapaxar compared withplacebo (Table 2).

TABLE 3 Vorapaxar Compared With Placebo for Stroke by Qualifying Disease State
EndpointMI
(n ¼ 16,897)PAD
(n ¼ 3,273) p Interaction
Any stroke 0.62 (0.45–0.85) 0.80 (0.51–1.25) 0.35
All ischemic stroke 0.51 (0.36–0.72) 0.71 (0.44–1.14) 0.28
Ischemic stroke withouthemorrhagic conversion
0.51 (0.35–0.74) 0.76 (0.46–1.25) 0.21
Ischemic stroke withhemorrhagic conversion
0.75 (0.26–2.16) 0.51 (0.093–2.76) 0.70
Values are HR (95% CI).
HR ¼ hazard ratio; PAD ¼ peripheral artery disease; other abbreviations in Table 2.
FIGURE 4 Kaplan-Meier Curves for Death Occurring After Ischemic Stroke
by Treatment Allocation
20%
18%
16%
14%
12%
Deat
h (%
)
Days from Ischemic Stroke
10%
8%
6%
4%
2%
0%0 30 60 90 120 150 180
13.8%
Placebo Vorapaxar N=130 N=74
p=0.79
HR 1.0995% CI 0.57 - 2.07
13.4%
This figure shows all deaths occurring after ischemic stroke through 180 days.
Abbreviations as in Figure 1.
J A C C V O L . 6 4 , N O . 2 2 , 2 0 1 4 Bonaca et al.D E C E M B E R 9 , 2 0 1 4 : 2 3 1 8 – 2 6 Vorapaxar and New Stroke
2323
MRS AFTER STROKE WITH VORAPAXAR. In patientswho experienced an ischemic stroke during trialfollow-up, there was no difference in the meanMRS after stroke (90 days or last observation carriedforward) with vorapaxar versus placebo (2.7 vs. 2.3;p ¼ 0.21). The overall reduction in ischemic strokewas similar across all MRS categories (Figure 5A), andwas consistent for ischemic stroke with and withouthemorrhagic conversion (Online Figures 2 and 3). Thehazard of a moderate-to-severely disabling ischemicstroke of any kind was reduced with vorapaxar, bothfor nonfatal events (MRS 3 to 5, HR: 0.51 95% CI: 0.30to 0.87; p ¼ 0.013) and for all events, including fatalstrokes (MRS 3 to 6, HR: 0.55 95% CI: 0.35 to 0.87;p ¼ 0.011) (Online Figure 4). Hemorrhagic stroke wasincreased with vorapaxar across MRS, including thosethat were fatal (score of 6) (Online Figure 5).
When evaluating all strokes (ischemic and hemor-rhagic), vorapaxar reduced stroke across MRS cate-gories, with the exception of a greater number of fatalstrokes (MRS 6) with vorapaxar (20 vs. 15) (Figure 5B).The hazard of a moderately to severely disablingnonfatal stroke was reduced with vorapaxar (MRS 3to 5, HR: 0.51 95% CI: 0.30 to 0.87; p ¼ 0.013),with a consistent trend when including fatal events(MRS 3 to 6, HR: 0.73 95% CI: 0.50 to 1.08; p ¼ 0.11)(Online Figure 5).
INFLUENCE OF BACKGROUND THIENOPYRIDINE
THERAPY. The majority of patients receiving athienopyridine were also administered aspirin asDAPT (Table 1). The reduction in a new stroke of anykind with vorapaxar compared with placebo wassimilar in both patients planned for thienopyridinetherapy (n ¼ 13,452, HR: 0.65, 95% CI: 0.46 to 0.93;p ¼ 0.018), as well as those not planned for thieno-pyridine therapy (n ¼ 6,718, HR: 0.70, 95% CI: 0.48 to1.01; p ¼ 0.022; p for interaction ¼ 0.79) (Figure 6).Findings were similar for new ischemic stroke (plan-ned thienopyridine therapy HR: 0.54, 95% CI: 0.37 to0.80; p ¼ 0.002 vs. no planned thienopyridinetherapy HR: 0.60, 95% CI: 0.39 to 0.91; p ¼ 0.016;p for interaction ¼ 0.75) (Figure 6). Vorapaxarwas associated with increased rates of hemorrhagicstroke, regardless of background thienopyridine(Online Figure 4).
DISCUSSION
Vorapaxar significantly reduced the risk of stroke inpatients with a history of MI or PAD and no priorhistory of stroke or TIA, the patient group approvedfor use by the U.S. Food and Drug Administration(Central Illustration). This benefit with vorapaxar
was mediated through a significant reduction inischemic stroke, which represented the majority ofnew strokes occurring in this cohort (84%). Vor-apaxar increased the risk of primary hemorrhagicstroke; however, due to the infrequency of thisevent relative to ischemic stroke, the overall inci-dence of stroke was reduced. Importantly, inpatients who experienced a first ischemic strokewhile taking vorapaxar, there was no significantincrease in the risk of hemorrhagic conversion ordeath during follow-up. The reduction in ischemicstroke was consistent across MRS, includingseverely disabling and fatal events.
ANTIPLATELET THERAPY AND STROKE. New treat-ments that prevent stroke are needed (15). Stroke isthe leading cause of long-term disability in theUnited States, with about a quarter of patients who
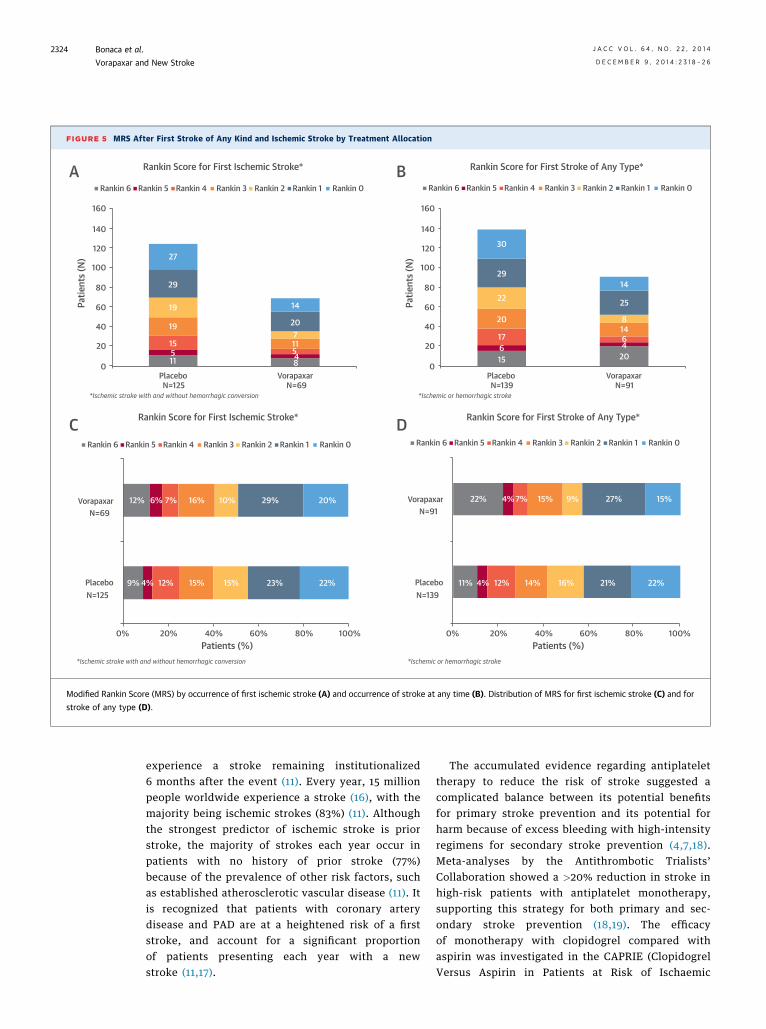
FIGURE 5 MRS After First Stroke of Any Kind and Ischemic Stroke by Treatment Allocation
Rankin Score for First Ischemic Stroke*A B
C D
2730
14
25
8
64
20
14
29
22
20
17615
14
207
548
11
29
19
19
15
12%
9% 4% 12% 15% 15% 23%
22% 4% 7% 15% 9% 27% 15%
11% 4% 12% 14% 16% 21% 22%22%
6% 7% 16% 10% 29% 20%
511
Rankin 6 Rankin 5 Rankin 4
Placebo
160
140
120
Patie
nts (
N)
Patie
nts (
N)100
80
60
40
20
0Vorapaxar
Patients (%) Patients (%)
Placebo
Vorapaxar
N=125
N=69
N=125
0% 20% 40% 60% 80% 100% 0% 20% 40% 60% 80% 100%
Placebo
VorapaxarN=91
N=139
*Ischemic stroke with and without hemorrhagic conversion
*Ischemic stroke with and without hemorrhagic conversion
*Ischemic or hemorrhagic stroke
*Ischemic or hemorrhagic stroke
N=69Placebo VorapaxarN=139 N=91
Rankin 3 Rankin 2 Rankin 1 Rankin 0
Rankin Score for First Ischemic Stroke*
Rankin Score for First Stroke of Any Type*
Rankin Score for First Stroke of Any Type*
160
140
120
100
80
60
40
20
0
Rankin 6 Rankin 5 Rankin 4 Rankin 3 Rankin 2 Rankin 1 Rankin 0 Rankin 6 Rankin 5 Rankin 4 Rankin 3 Rankin 2 Rankin 1 Rankin 0
Rankin 6 Rankin 5 Rankin 4 Rankin 3 Rankin 2 Rankin 1 Rankin 0
Modified Rankin Score (MRS) by occurrence of first ischemic stroke (A) and occurrence of stroke at any time (B). Distribution of MRS for first ischemic stroke (C) and for
stroke of any type (D).
Bonaca et al. J A C C V O L . 6 4 , N O . 2 2 , 2 0 1 4
Vorapaxar and New Stroke D E C E M B E R 9 , 2 0 1 4 : 2 3 1 8 – 2 6
2324
experience a stroke remaining institutionalized6 months after the event (11). Every year, 15 millionpeople worldwide experience a stroke (16), with themajority being ischemic strokes (83%) (11). Althoughthe strongest predictor of ischemic stroke is priorstroke, the majority of strokes each year occur inpatients with no history of prior stroke (77%)because of the prevalence of other risk factors, suchas established atherosclerotic vascular disease (11). Itis recognized that patients with coronary arterydisease and PAD are at a heightened risk of a firststroke, and account for a significant proportionof patients presenting each year with a newstroke (11,17).
The accumulated evidence regarding antiplatelettherapy to reduce the risk of stroke suggested acomplicated balance between its potential benefitsfor primary stroke prevention and its potential forharm because of excess bleeding with high-intensityregimens for secondary stroke prevention (4,7,18).Meta-analyses by the Antithrombotic Trialists’Collaboration showed a >20% reduction in stroke inhigh-risk patients with antiplatelet monotherapy,supporting this strategy for both primary and sec-ondary stroke prevention (18,19). The efficacyof monotherapy with clopidogrel compared withaspirin was investigated in the CAPRIE (ClopidogrelVersus Aspirin in Patients at Risk of Ischaemic

FIGURE 6 Effect of Vorapaxar on Stroke Subtype Stratified by
Background Thienopyridine Therapy
All Ischemic Stroke
Ischemic Stroke with Hemorrhagic Conversion
Ischemic Stroke without Hemorrhagic Conversion
Favors Vorapaxar Favors Placebo
Hazard Ratio p-value
0.002
0.29
0.99
0.016
0.008
0.018
0.057
0.018
0.54
0.57
0.65
0.70
0.59
0.56
1.00
0.60
p-interaction
0.75
0.56
0.91
0.79
All Stroke
+ thienopyridine
– thienopyridine
+ thienopyridine
– thienopyridine
+ thienopyridine
– thienopyridine
+ thienopyridine
– thienopyridine
0.1 1.0 10
This figure shows the hazard of each stroke type with vorapaxar stratified by
background thienopyridine therapy.
J A C C V O L . 6 4 , N O . 2 2 , 2 0 1 4 Bonaca et al.D E C E M B E R 9 , 2 0 1 4 : 2 3 1 8 – 2 6 Vorapaxar and New Stroke
2325
Events) trial, which showed a numeric, but not sta-tistically significant, reduction in ischemic strokewith clopidogrel, primarily in those patients whoqualified for the trial with stroke, rather than withMI or PAD (20). Although DAPT with aspirin andclopidogrel appeared potentially effective for thereduction of all stroke and ischemic stroke in a post-hoc analysis of the CHARISMA (Clopidogrel for HighAtherothrombotic Risk, Ischemic Stabilization, Man-agement, and Avoidance) trial, in several largededicated trials of long-term secondary stroke pre-vention, DAPT showed either lack of benefit oroverall harm in multiple well-powered studies(2–4,7,8).
This complicated balance may stem from theheterogeneous etiologies of stroke events (e.g.,cardioembolic, lacunar, hemorrhagic, or athero-thrombotic) and whether all causes of ischemicstroke are equally modifiable with antiplatelettherapy. Indeed, outcomes with intensive anti-platelet therapy appear to differ among subsets ofstroke patients, including harm in patients enrolledin a trial with entry criteria of lacunar stroke, andbenefit in a trial of patients enrolled with minoracute ischemic stroke (8,21). It is plausible thatantiplatelet therapy would carry the greatest benefitin preventing atherothrombotic strokes, and thoseat the greatest risk of this stroke subtype arethose with established atherosclerotic vasculardisease (15).
FINDINGS WITH VORAPAXAR. The main results fromthe TRA 2�P-TIMI 50 trial show a significant reductionin overall ischemic events with vorapaxar whenadded to background antiplatelet therapy (2) (CentralIllustration). On the basis of these results, vorapaxarwas recommended for approval in patients with priorMI or symptomatic PAD (9), but because of an excessrisk of intracranial hemorrhage, it should not beadministered to patients with a history of stroke orTIA.
In the present analysis, we described the inci-dence and subtypes of first stroke in this popula-tion, and demonstrated a significant 33% reductionin strokes of any kind and a 43% reduction inischemic stroke with vorapaxar. This benefit ofvorapaxar was on the background of aspirin therapy,and was observed whether or not a thienopyridinewas also used. The reduction in ischemic stroke wasalso consistent at all levels of severity, as measuredby MRS. At the same time, vorapaxar increased therisk of primary hemorrhagic stroke, but the fre-quency was significantly lower than the ischemicstroke frequency, resulting in a significant reduction
in all strokes. In addition, we found an overalldecreased risk of ischemic stroke with hemorrhagicconversion with vorapaxar compared with placebo,which was due to a significant reduction in ischemicstroke. Importantly, we did not find a significantincrease in the risk of hemorrhagic conversion ordeath in patients who had an ischemic stroke onvorapaxar.
STUDY LIMITATIONS. In TRA 2�P-TIMI 50, vorapaxarwas studied in addition to background antiplatelettherapy and, therefore, the efficacy and safety ofvorapaxar as monotherapy for stroke preventioncannot be evaluated.
CONCLUSIONS
In stable patients with atherosclerotic vascular dis-ease and no history of stroke or TIA, chronic therapywith vorapaxar reduces the risk of ischemic stroke.Although primary hemorrhagic stroke was increasedwith vorapaxar, stroke of any kind was significantlyreduced. This benefit of vorapaxar is consistent whengiven with aspirin or aspirin and a thienopyridine.Patients who suffer a first ischemic stroke on vor-apaxar were not at a detectable increased risk ofsubsequent intracranial hemorrhage or death whenvorapaxar was discontinued.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Marc P. Bonaca, TIMI Study Group, CardiovascularDivision, Brigham and Women’s Hospital, 75 FrancisStreet, Boston, Massachusetts 02115. E-mail:[email protected].

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: The risk of first
ischemic stroke and subsequent outcomes in patients with
stable atherosclerotic vascular disease (history of myocardial
infarction or symptomatic peripheral artery disease) and no
history of stroke or transient ischemic attack treated with the
recently approved novel PAR-1 antagonist vorapaxar are un-
known. The objectives were to investigate both whether PAR-1
antagonism modifies the risk of ischemic stroke and whether
patients who experience a first ischemic stroke on vorapaxar are
at increased risk of hemorrhagic conversion or death. PAR-1
antagonism with vorapaxar significantly reduced all strokes in
this population by 33% and ischemic stroke by 43%. No statis-
tically significant increase in the risk of hemorrhagic conversion
or death was observed with vorapaxar when the agent was
stopped after a first ischemic stroke.
TRANSLATIONAL OUTLOOK: PAR-1 antagonism reduces
the risk of stroke overall and ischemic stroke, and is not asso-
ciated with increased risk of hemorrhagic conversion or death
after stroke when therapy is stopped after first ischemic stroke.
Bonaca et al. J A C C V O L . 6 4 , N O . 2 2 , 2 0 1 4
Vorapaxar and New Stroke D E C E M B E R 9 , 2 0 1 4 : 2 3 1 8 – 2 6
2326
RE F E RENCE S
1. Morrow DA, Braunwald E, Bonaca MP, et al.,TRA 2P-TIMI 50 Steering Committee andInvestigators. Vorapaxar in the secondary pre-vention of atherothrombotic events. N Engl J Med2012;366:1404–13.
2. Morrow DA, Alberts MJ, Mohr JP, et al.,Thrombin Receptor Antagonist in Secondary Pre-vention of Atherothrombotic Ischemic Events–TIMI 50 Steering Committee and Investigators.Efficacy and safety of vorapaxar in patients withprior ischemic stroke. Stroke 2013;44:691–8.
3. Wiviott SD, Braunwald E, McCabe CH, et al.,TRITON-TIMI 38 Investigators. Prasugrel versusclopidogrel in patients with acute coronarysyndromes. N Engl J Med 2007;357:2001–15.
4. Sacco RL, Diener HC, Yusuf S, et al., PRoFESSStudy Group. Aspirin and extended-release dipyr-idamole versus clopidogrel for recurrent stroke.N Engl J Med 2008;359:1238–51.
5. SaccoRL,AdamsR,AlbersG, etal., AmericanHeartAssociation/American Stroke Association Council onStroke; Council on Cardiovascular Radiology andIntervention: American Academy of Neurology.Guidelines for prevention of stroke in patients withischemic stroke or transient ischemic attack: a state-ment for healthcare professionals from the AmericanHeart Association/American Stroke AssociationCouncil on Stroke: Co-sponsored by the Council onCardiovascular Radiology and Intervention: TheAmerican Academy ofNeurology affirms the value ofthis guideline. Circulation 2006;113:e409–49.
6. SPS3 Investigators, Benavente OR, Hart RG,McClure LA, et al. Effects of clopidogrel added toaspirin in patients with recent lacunar stroke.N Engl J Med 2012;367:817–25.
7. Diener HC, Bogousslavsky J, Brass LM, et al.Aspirin and clopidogrel compared with clopidogrelalone after recent ischaemic stroke or transientischaemic attack in high-risk patients (MATCH):
randomised, double-blind, placebo-controlledtrial. Lancet 2004;364:331–7.
8. Diener HC, Weber R. Clopidogrel added toaspirin adds no benefit but bleeding risk in patientswith recent lacunar stroke. Stroke 2013;44:861–3.
9. United States Food and Drug Administration.FDA cardiovascular and renal drugs advisorycommittee proceedings NDA 204886. January 15,2014. Silver Spring, MD: FDA.
10. Rich DQ, Gaziano JM, Kurth T. Geographicpatterns in overall and specific cardiovasculardisease incidence in apparently healthy men in theUnited States. Stroke 2007;38:2221–7.
11. RogerVL,GoAS, Lloyd-JonesDM,etal.,AmericanHeart Association Statistics Committee and StrokeStatistics Subcommittee. Heart disease and strokestatistics—2012 update: a report from the AmericanHeart Association. Circulation 2012;125:e2–220.
12. Morrow DA, Scirica BM, Fox KA, et al., TRA2�P-TIMI 50 Investigators. Evaluation of a novelantiplatelet agent for secondary prevention inpatients with a history of atherosclerotic disease:design and rationale for the thrombin-receptorantagonist in secondary prevention of athero-thrombotic ischemic events (TRA 2�P)-TIMI 50trial. Am Heart J 2009;158:335–41.e3.
13. Scirica BM, Bonaca MP, Braunwald E, et al., TRA2�P-TIMI 50 Steering Committee Investigators.Vorapaxar for secondary prevention of thromboticevents for patients with previous myocardialinfarction: a prespecified subgroup analysis of theTRA 2�P-TIMI 50 trial. Lancet 2012;380:1317–24.
14. van Swieten JC, Koudstaal PJ, Visser MC, et al.Interobserver agreement for the assessment ofhandicap in stroke patients. Stroke 1988;19:604–7.
15. Adams RJ, Albers G, Alberts MJ, et al.,American Heart Association; American StrokeAssociation. Update to the AHA/ASA recommen-dations for the prevention of stroke in patients
with stroke and transient ischemic attack. Stroke2008;39:1647–52.
16. McIntosh J, Mensah G. The Atlas of HeartDisease and Stroke. Geneva, Switzerland: WorldHealth Organization, 2004.
17. O’Donnell MJ, Xavier D, Liu L, et al., INTER-STROKE Investigators. Risk factors for ischaemicand intracerebral haemorrhagic stroke in 22 coun-tries (the INTERSTROKE study): a case-controlstudy. Lancet 2010;376:112–23.
18. Antithrombotic Trialists’ Collaboration. Col-laborative meta-analysis of randomised trialsof antiplatelet therapy for prevention of death,myocardial infarction, and stroke in high riskpatients. BMJ 2002;324:71–86.
19. Antithrombotic Trialists’ (ATT) Collaboration,Baigent C, Blackwell L, Collins R, et al. Aspirin inthe primary and secondary prevention of vasculardisease: collaborative meta-analysis of individualparticipant data from randomised trials. Lancet2009;373:1849–60.
20. CAPRIE Steering Committee. A randomised,blinded, trial of clopidogrel versus aspirin inpatients at risk of ischaemic events (CAPRIE).Lancet 1996;348:1329–39.
21. Wang Y, Wang Y, Zhao X, et al., CHANCEInvestigators. Clopidogrel with aspirin in acuteminor stroke or transient ischemic attack. N Engl JMed 2013;369:11–9.
KEY WORDS antiplatelet therapy,intracranial hemorrhage, PAR-1, plateletaggregation inhibitors, secondaryprevention, thrombin receptor
APPENDIX For a supplemental table andfigures, please see the online version ofthis article.