musculoskeltal ii module
TRANSCRIPT
2021-2022
MUSCULOSKELTAL II MODULE
BY HEADS OF DEPARTMENTS
Faculty of Medicine
MTI

2
Anatomy
BY
PROF. DR. HODA ELAASAR
Musculoskeletal II moduleMUS II 215
PROFESSOR & HEAD OF ANATOMY DEPARTMENT FACULTY OF MEDICINE - MTI
PROFESSOR OF ANATOMYFACULTY OF MEDICINE - CAIRO UNIVERSITY
3

4
Musculoskeletal II
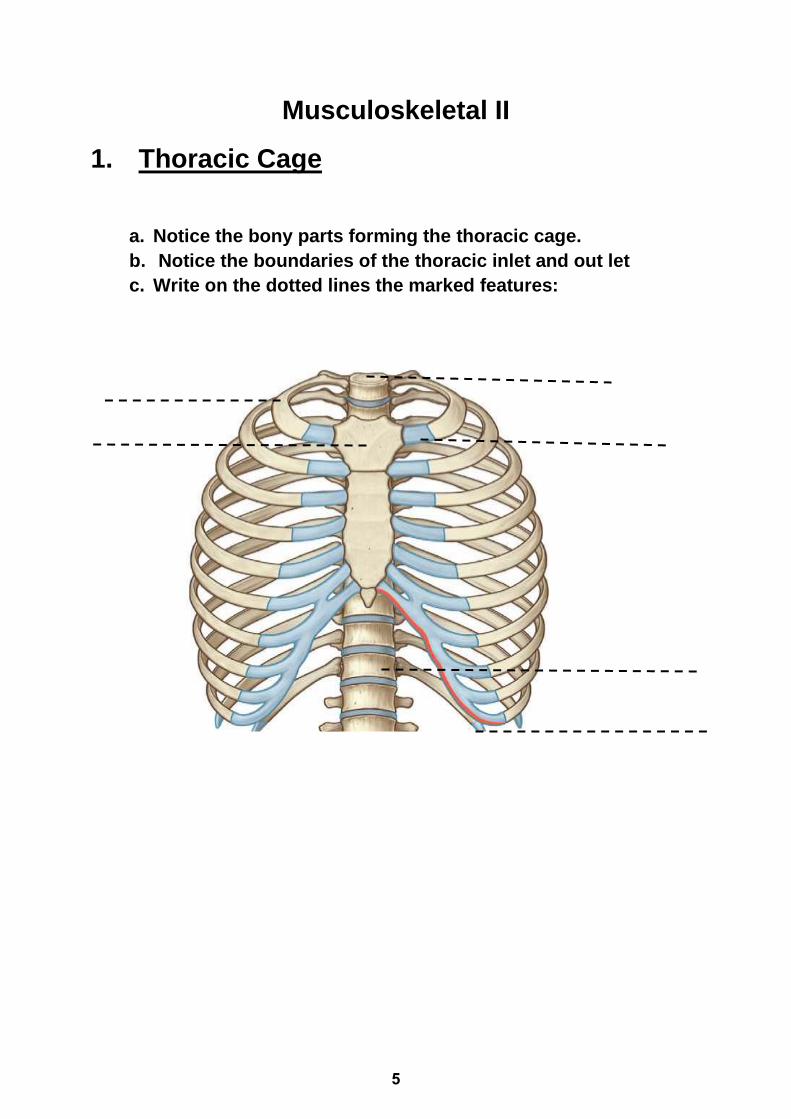
1. Thoracic Cage
a. Notice the bony parts forming the thoracic cage.
b. Notice the boundaries of the thoracic inlet and out let
c. Write on the dotted lines the marked features:
5
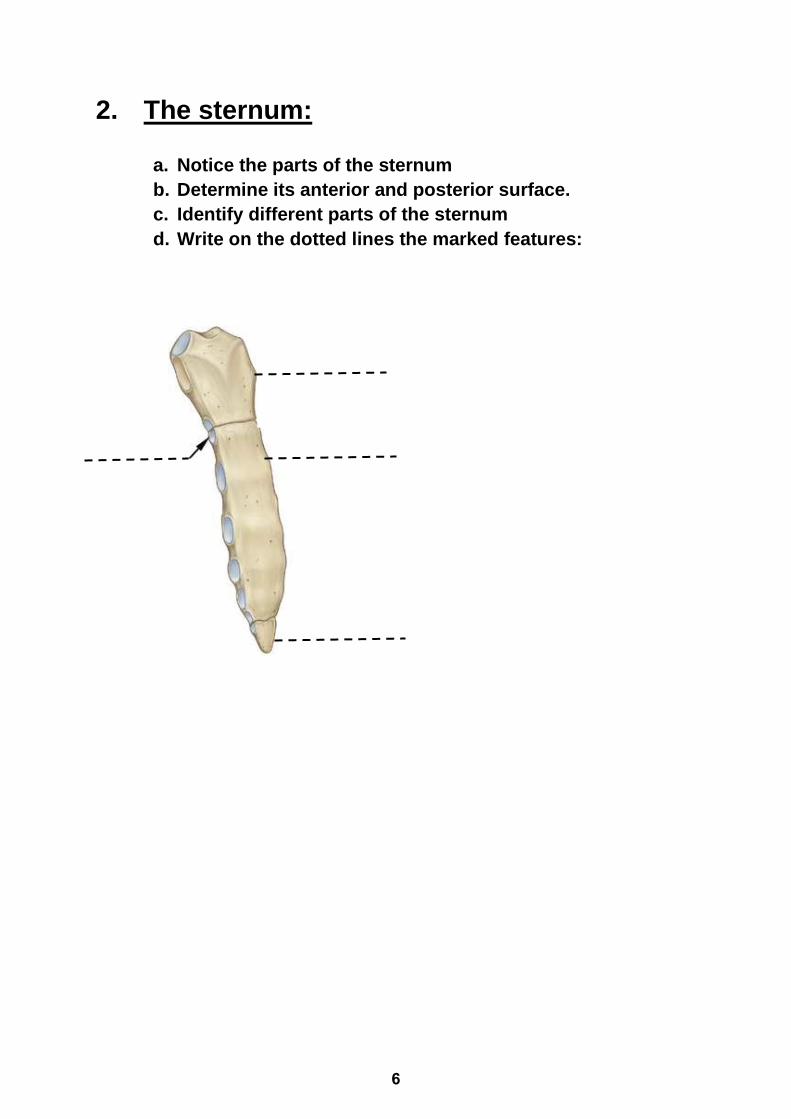
2. The sternum:
a. Notice the parts of the sternum
b. Determine its anterior and posterior surface.
c. Identify different parts of the sternum
d. Write on the dotted lines the marked features:
6
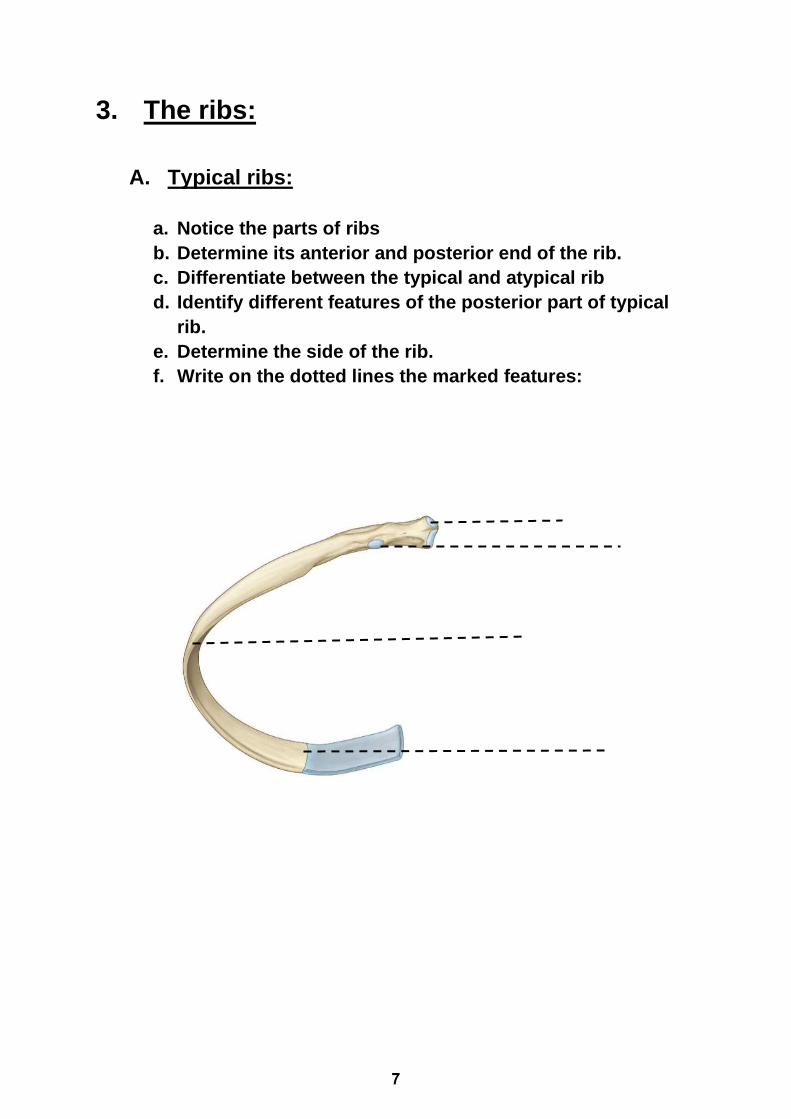
3. The ribs:
A. Typical ribs:
a. Notice the parts of ribs
b. Determine its anterior and posterior end of the rib.
c. Differentiate between the typical and atypical rib
d. Identify different features of the posterior part of typical
rib.
e. Determine the side of the rib.
f. Write on the dotted lines the marked features:
7
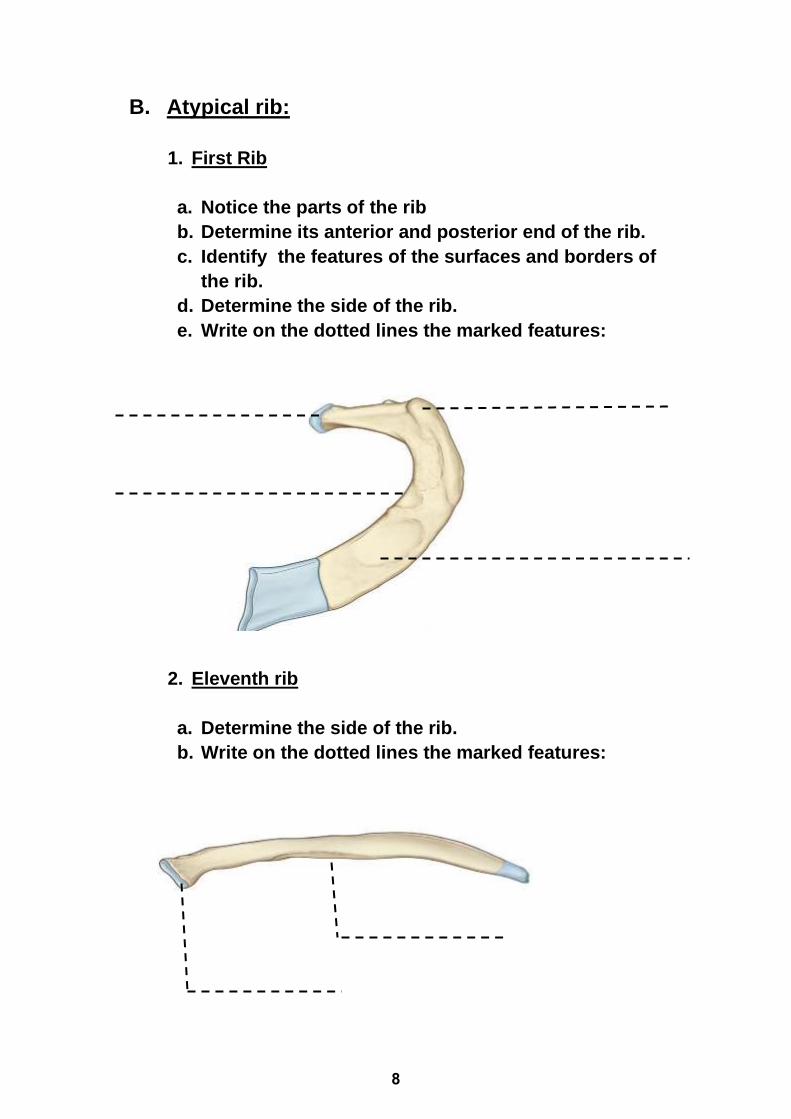
B. Atypical rib:
1. First Rib
a. Notice the parts of the rib
b. Determine its anterior and posterior end of the rib.
c. Identify the features of the surfaces and borders of
the rib.
d. Determine the side of the rib.
e. Write on the dotted lines the marked features:
2. Eleventh rib
a. Determine the side of the rib.
b. Write on the dotted lines the marked features:
8
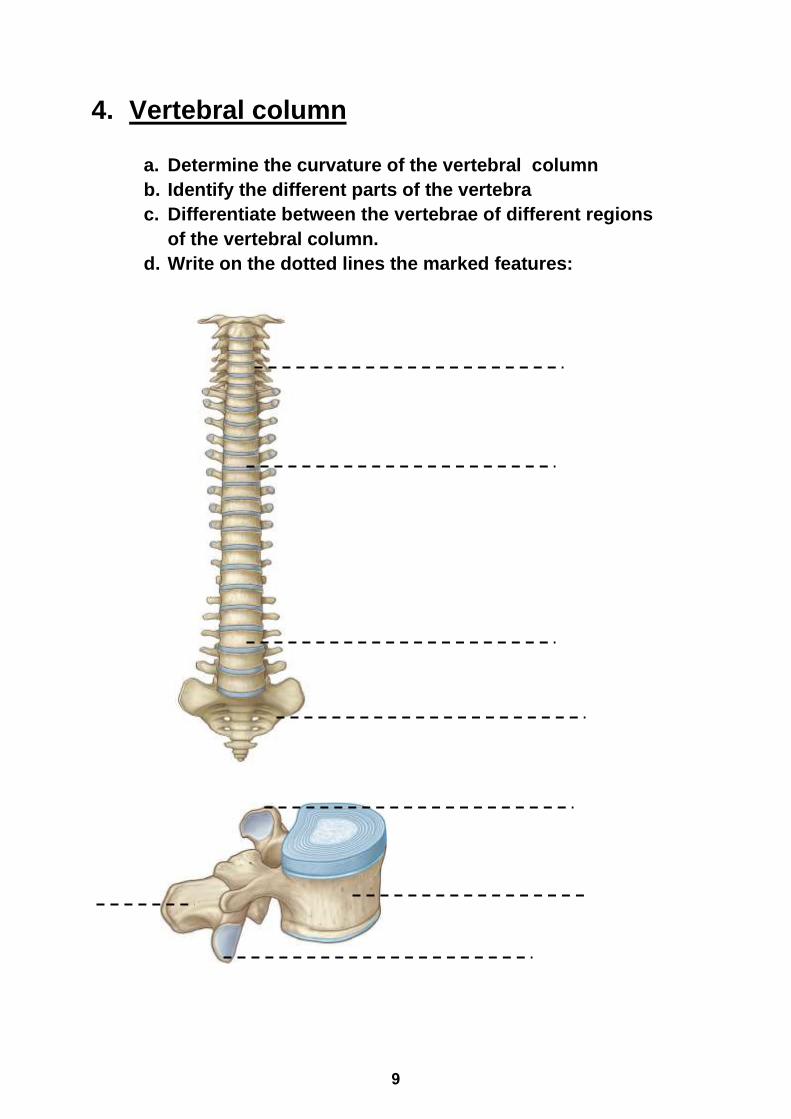
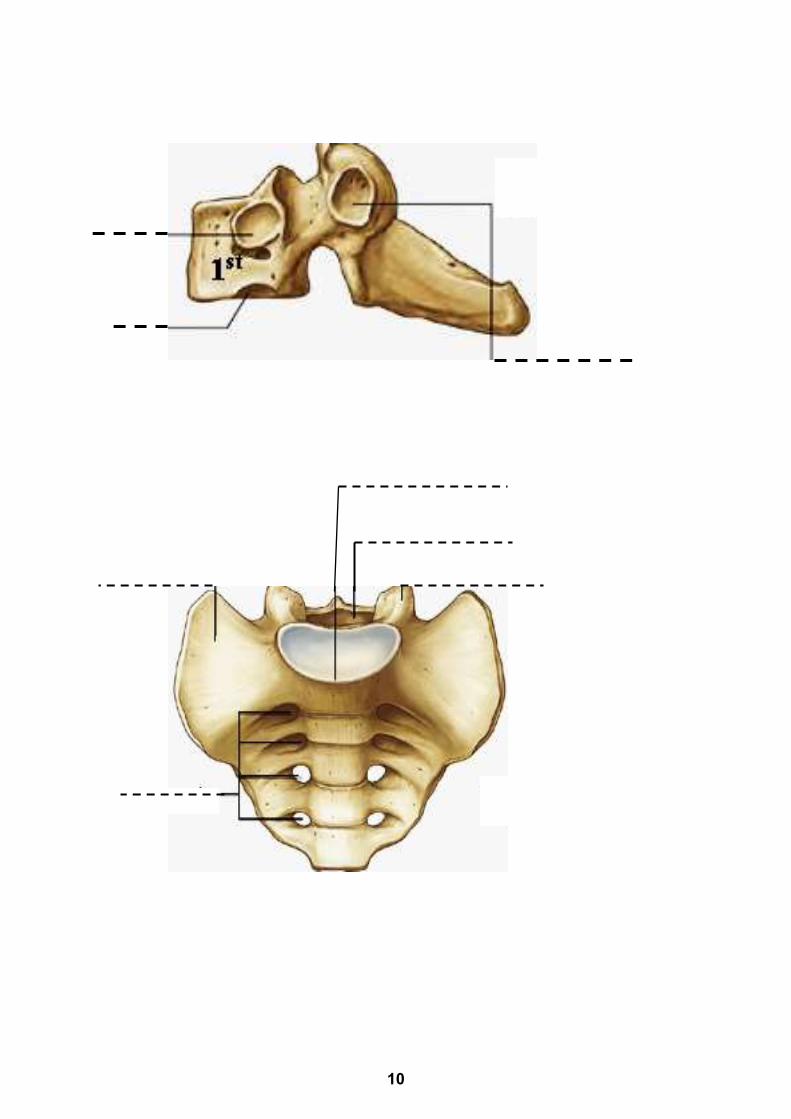
4. Vertebral column
a. Determine the curvature of the vertebral column
b. Identify the different parts of the vertebra
c. Differentiate between the vertebrae of different regions
of the vertebral column.
d. Write on the dotted lines the marked features:
9
10
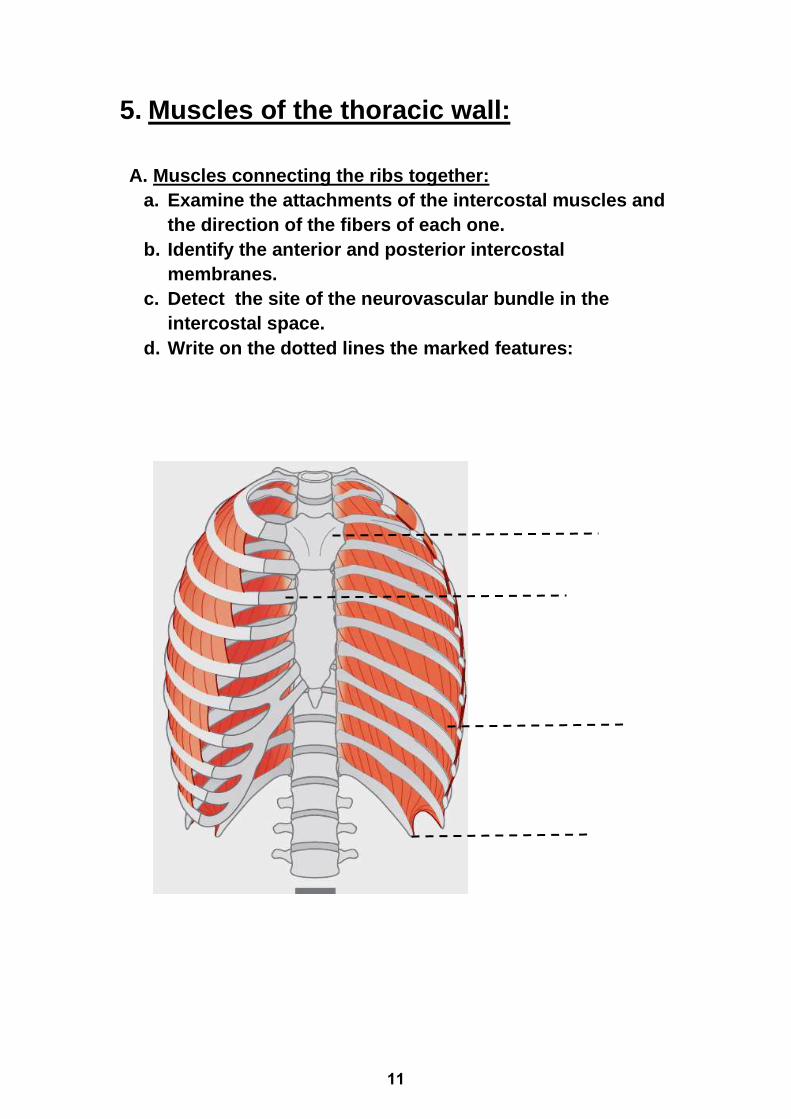
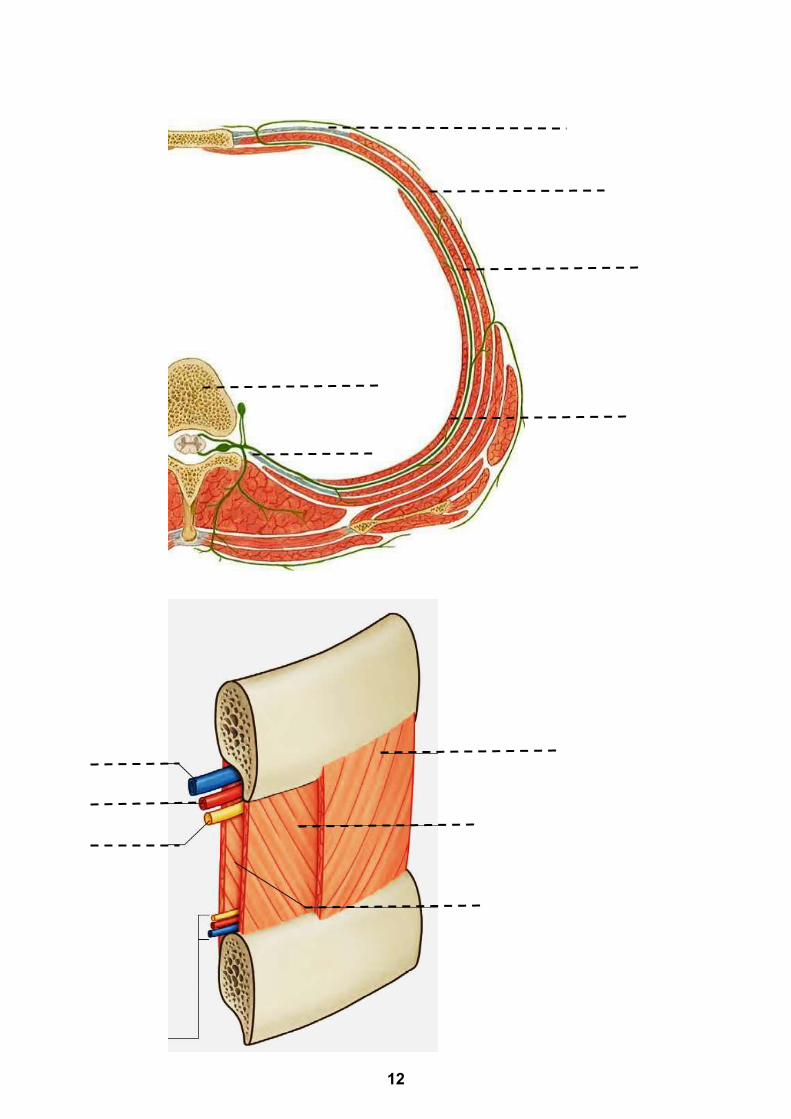
5. Muscles of the thoracic wall:
A. Muscles connecting the ribs together:
a. Examine the attachments of the intercostal muscles and
the direction of the fibers of each one.
b. Identify the anterior and posterior intercostal
membranes.
c. Detect the site of the neurovascular bundle in the
intercostal space.
d. Write on the dotted lines the marked features:
11
12
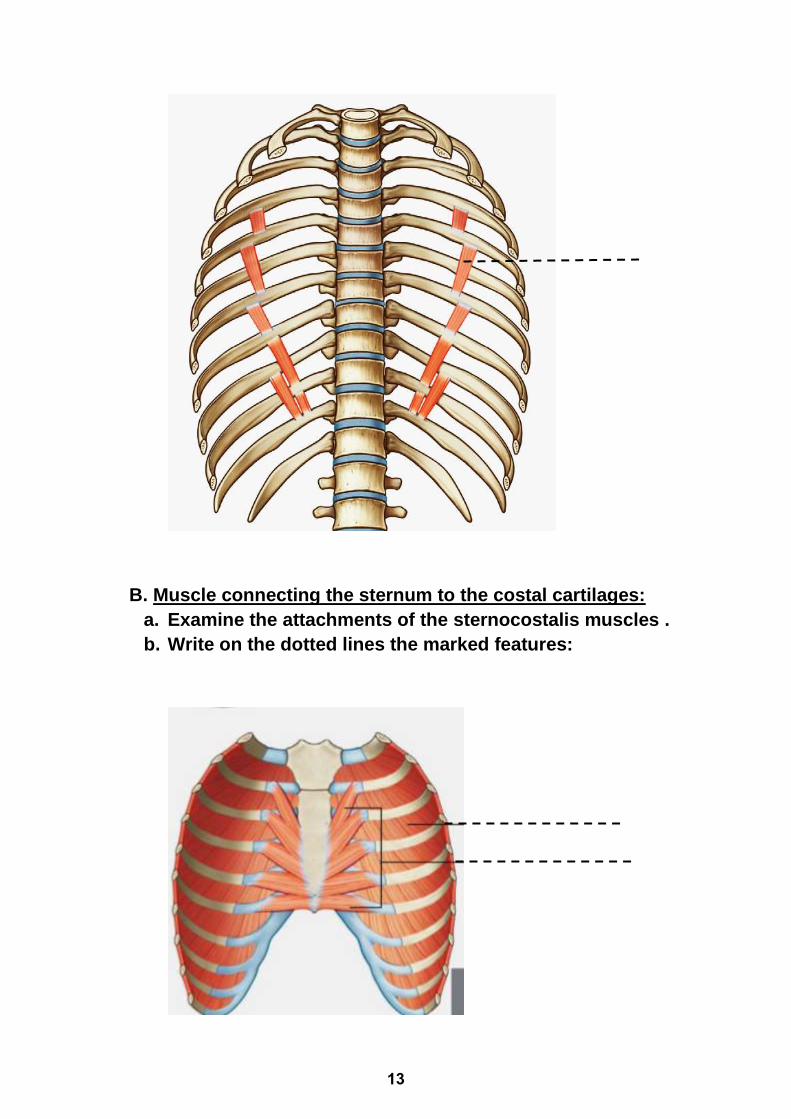
B. Muscle connecting the sternum to the costal cartilages:
a. Examine the attachments of the sternocostalis muscles .
b. Write on the dotted lines the marked features:
13
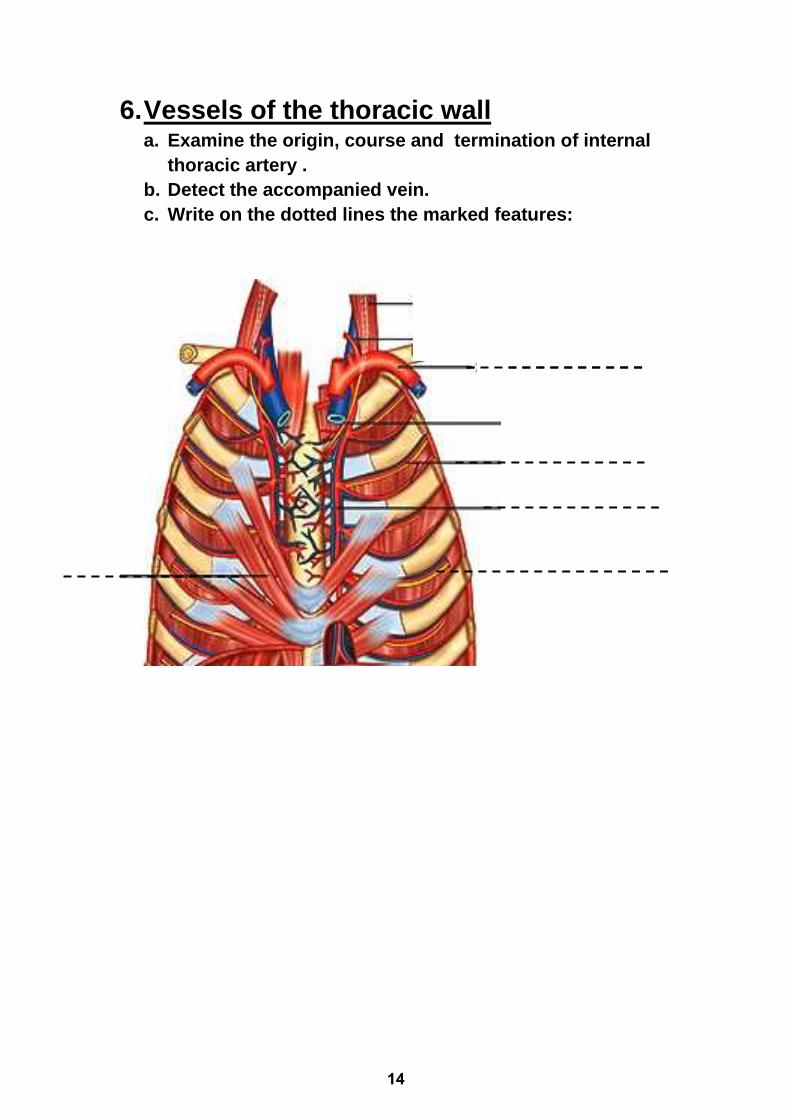
6. Vessels of the thoracic wall a. Examine the origin, course and termination of internal
thoracic artery .
b. Detect the accompanied vein.
c. Write on the dotted lines the marked features:
14
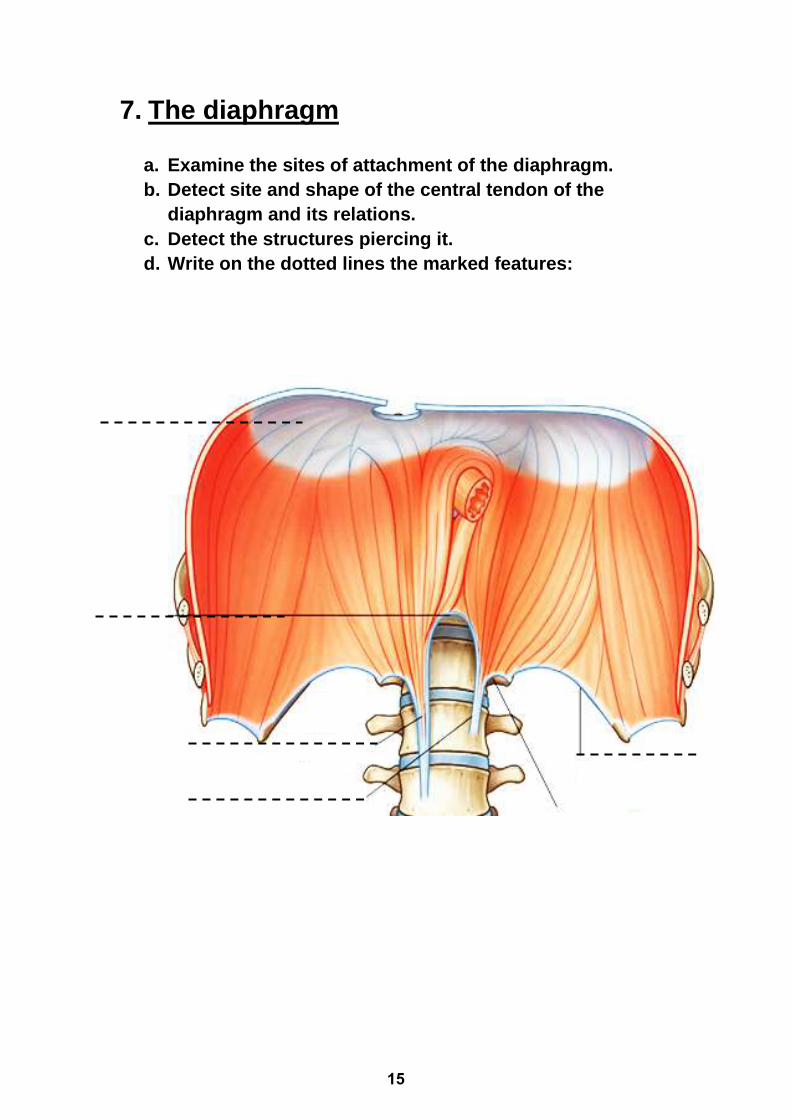
7. The diaphragm
a. Examine the sites of attachment of the diaphragm.
b. Detect site and shape of the central tendon of the
diaphragm and its relations.
c. Detect the structures piercing it.
d. Write on the dotted lines the marked features:
15
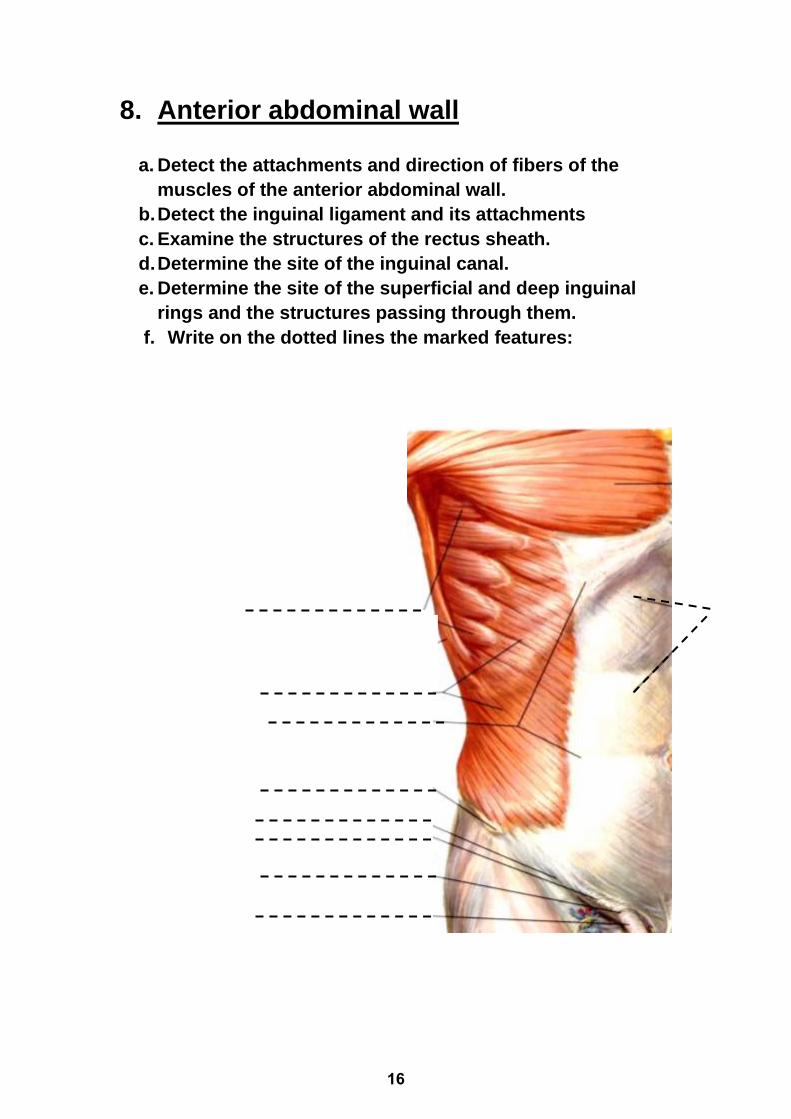
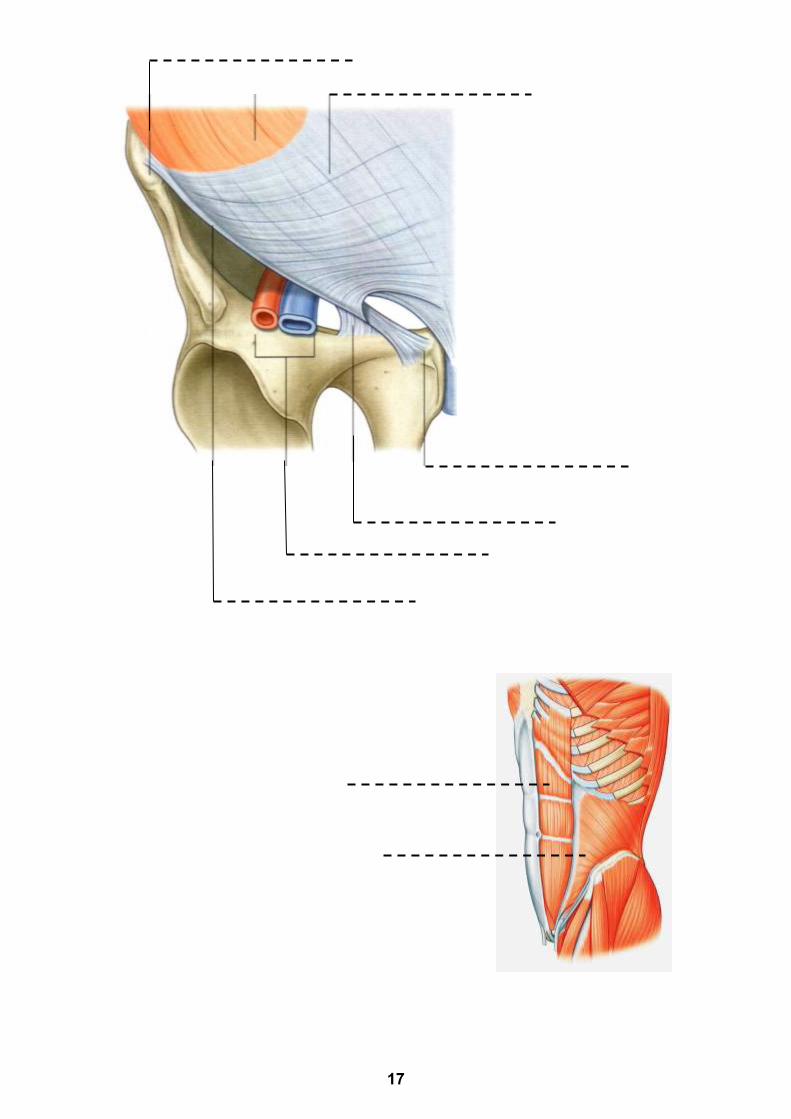
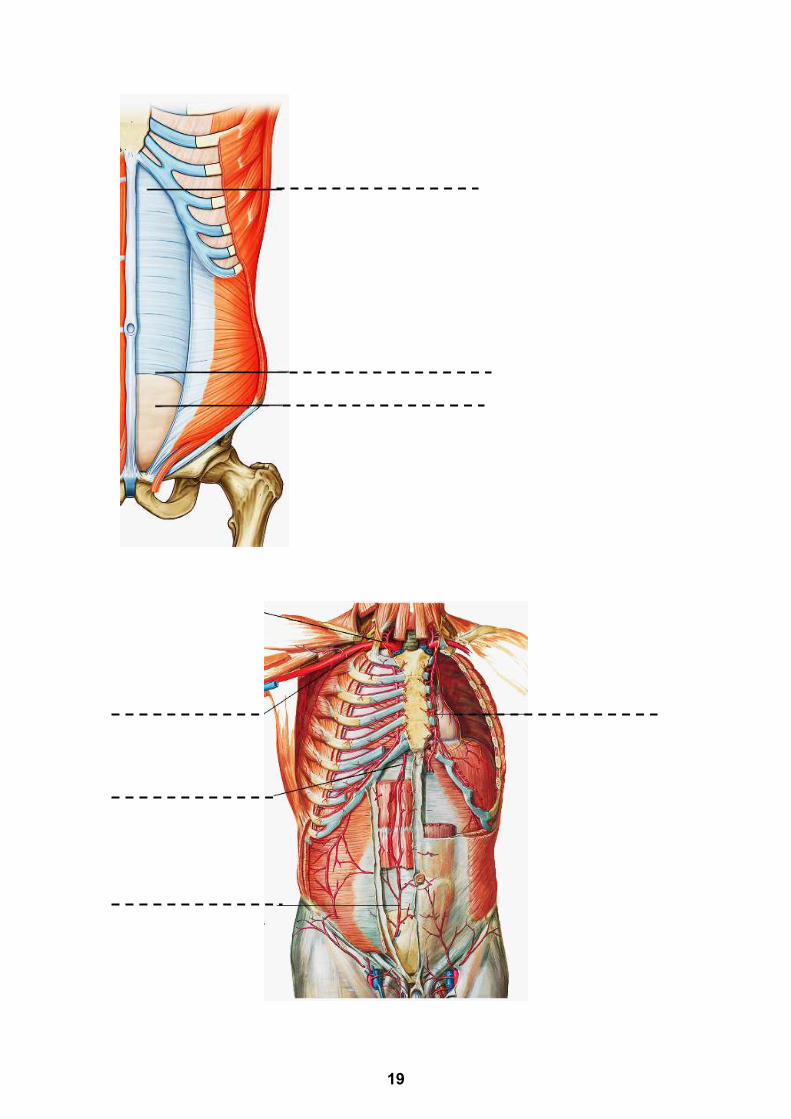
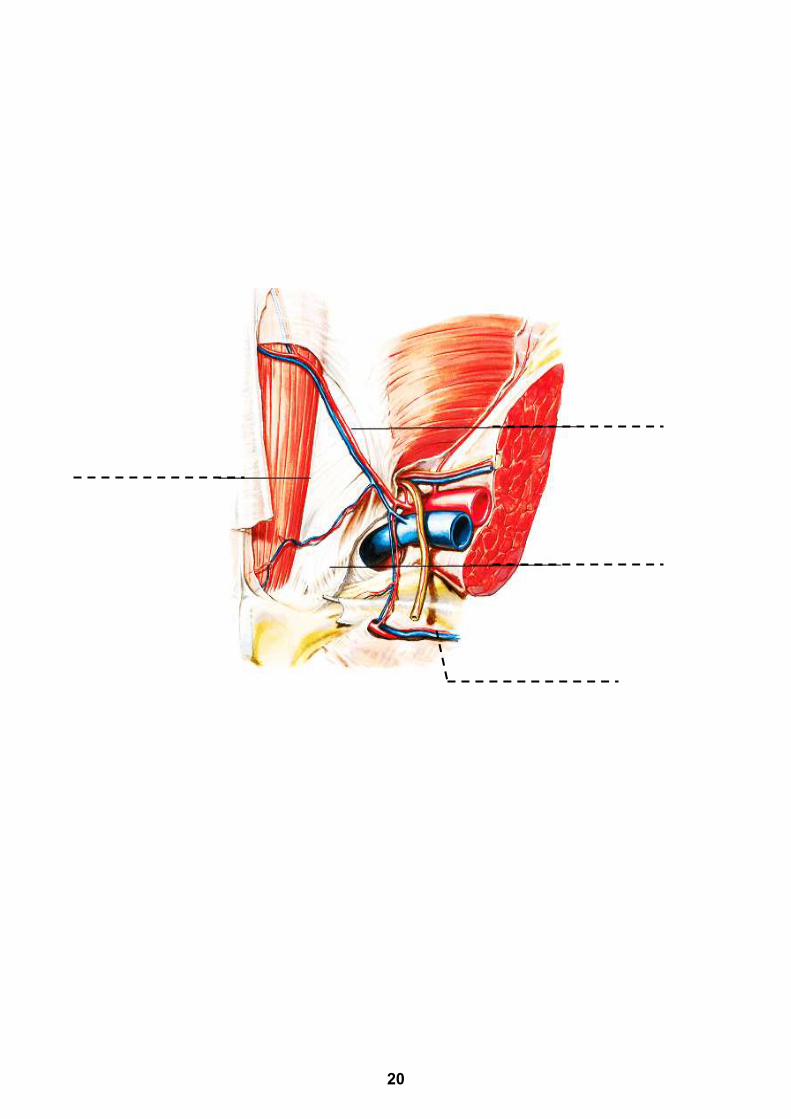
8. Anterior abdominal wall
a. Detect the attachments and direction of fibers of the
muscles of the anterior abdominal wall.
b. Detect the inguinal ligament and its attachments
c. Examine the structures of the rectus sheath.
d. Determine the site of the inguinal canal.
e. Determine the site of the superficial and deep inguinal
rings and the structures passing through them.
f. Write on the dotted lines the marked features:
16
17
18
19
20
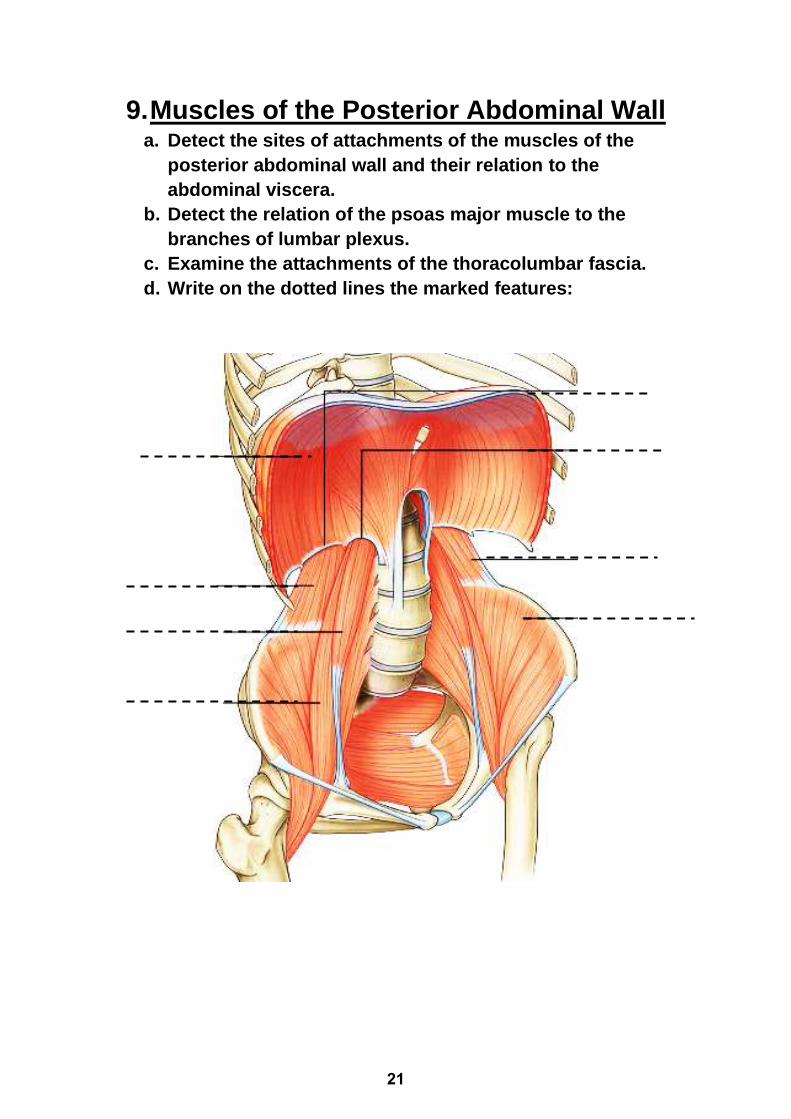
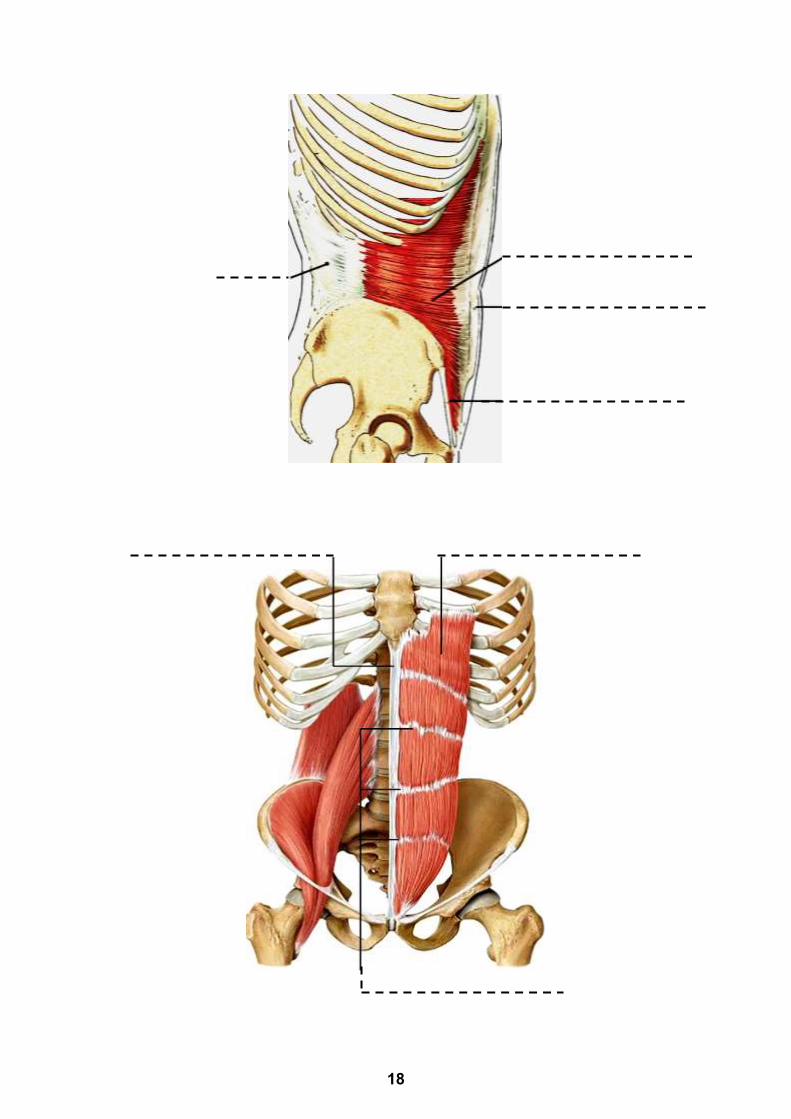
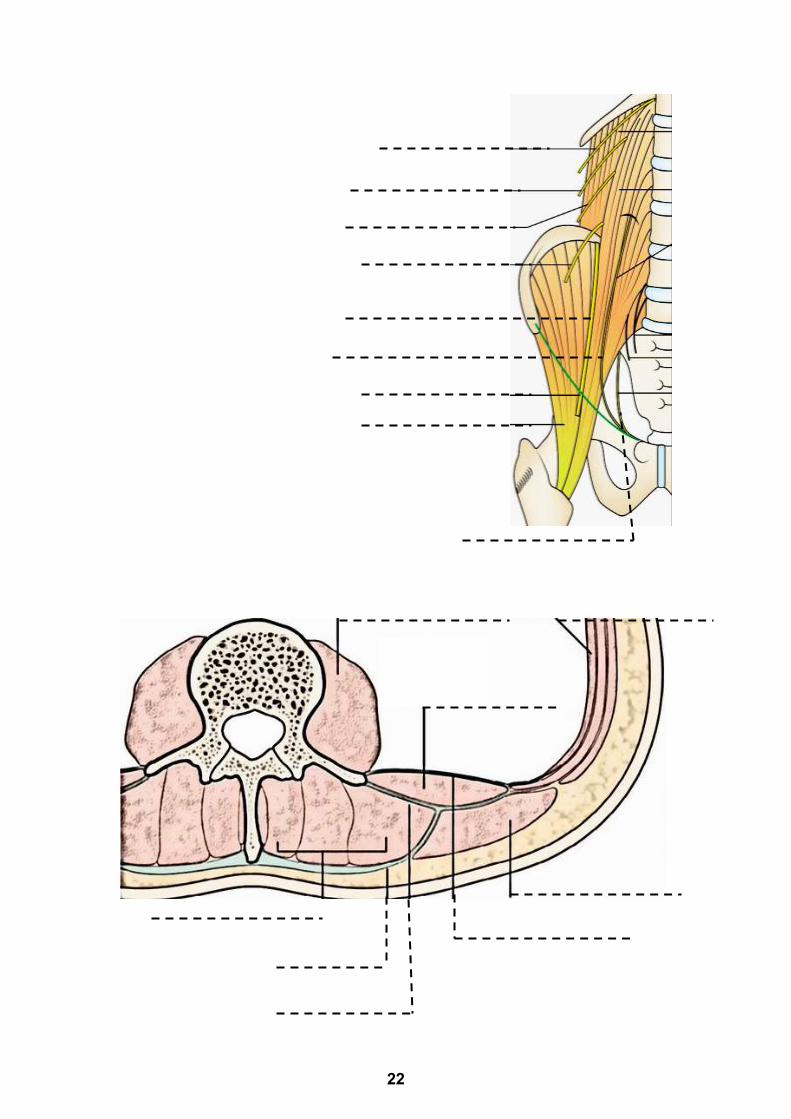
9. Muscles of the Posterior Abdominal Wall a. Detect the sites of attachments of the muscles of the
posterior abdominal wall and their relation to the
abdominal viscera.
b. Detect the relation of the psoas major muscle to the
branches of lumbar plexus.
c. Examine the attachments of the thoracolumbar fascia.
d. Write on the dotted lines the marked features:
21
22
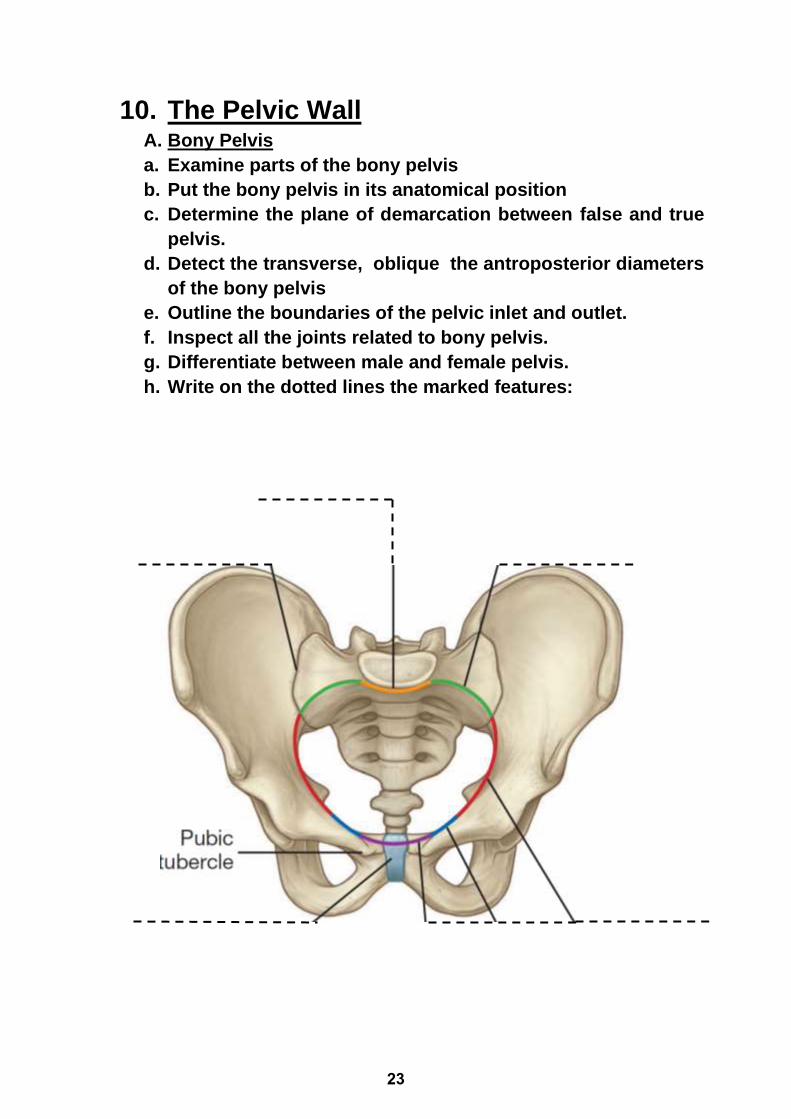
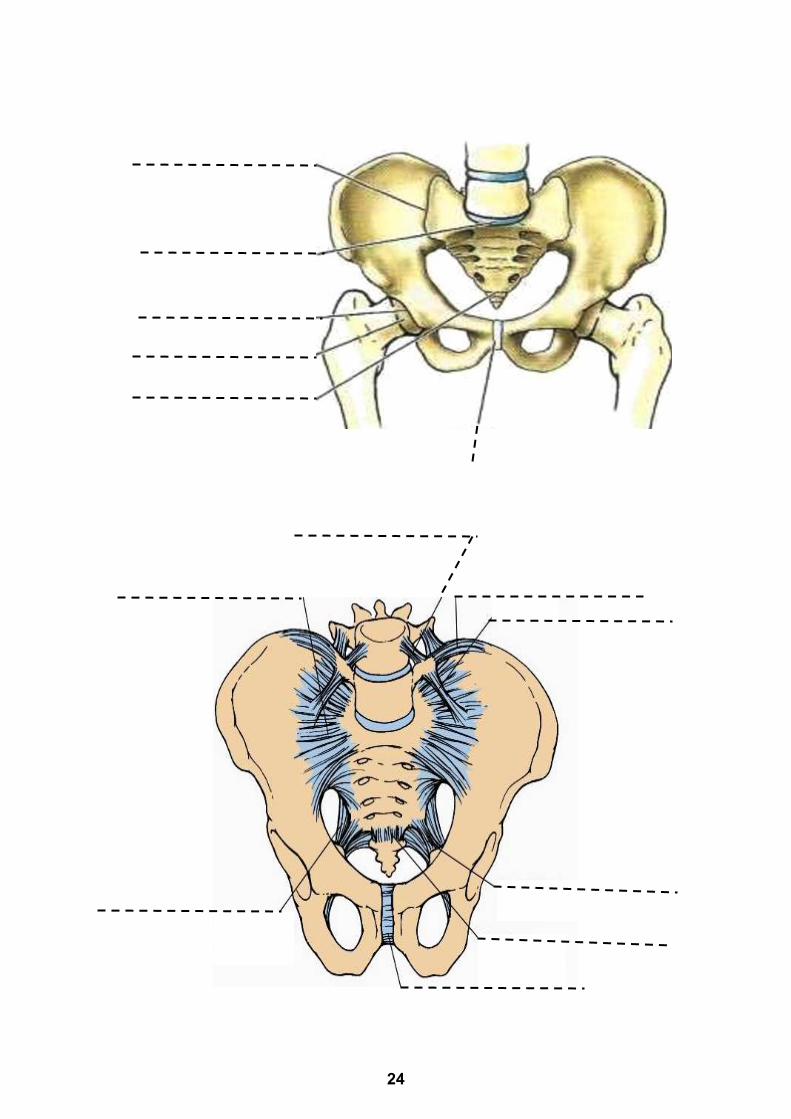
10. The Pelvic Wall A. Bony Pelvis
a. Examine parts of the bony pelvis
b. Put the bony pelvis in its anatomical position
c. Determine the plane of demarcation between false and true
pelvis.
d. Detect the transverse, oblique the antroposterior diameters
of the bony pelvis
e. Outline the boundaries of the pelvic inlet and outlet.
f. Inspect all the joints related to bony pelvis.
g. Differentiate between male and female pelvis.
h. Write on the dotted lines the marked features:
23
24
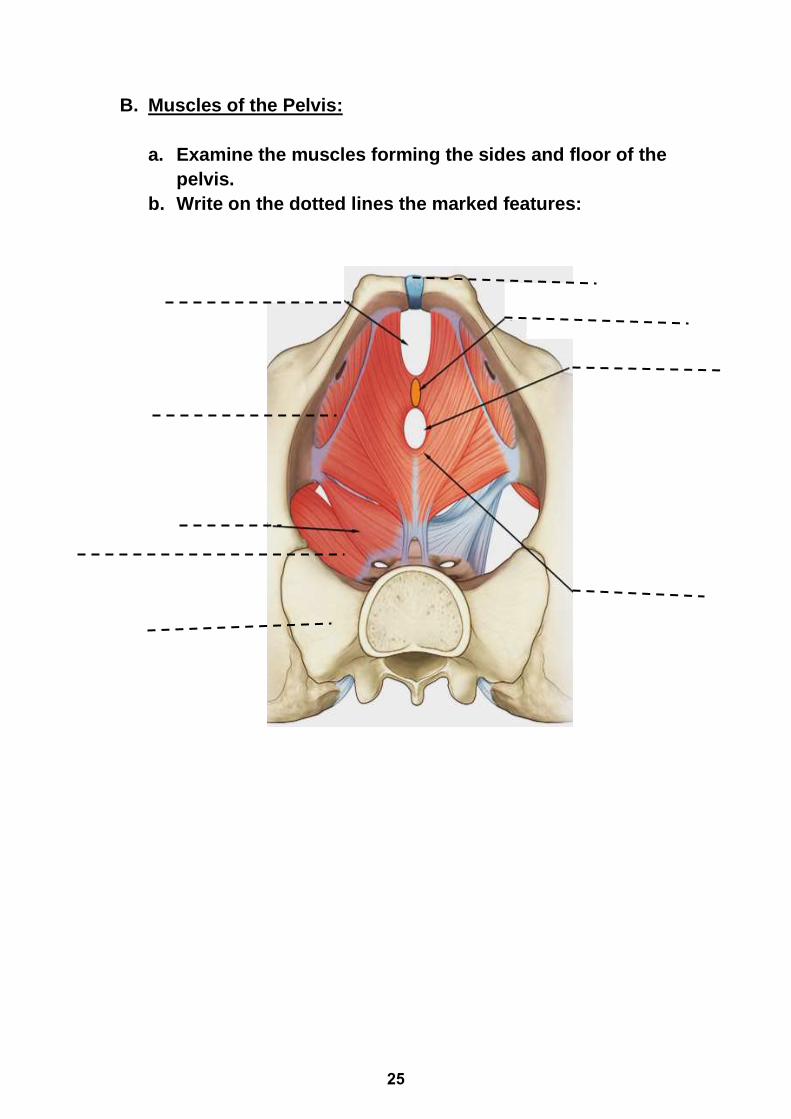
B. Muscles of the Pelvis:
a. Examine the muscles forming the sides and floor of the
pelvis.
b. Write on the dotted lines the marked features:
25
Self Assessment Questions
A. Short assay questions
1. Mention the function of the vertebral column:
2. Describe the primary and secondary curvatures of the
vertebral column and their sites.
3. Differentiate between the vertebrae of different regions of
the vertebral column.
26
4. Give the boundary of the thoracic inlet.
5. Give the boundary of thoracic outlet
6. Enumerate the structures related to the neck of the first
rib.
27
7. Classify the ribs according to their attachment to the
sternum.
8. Give the possible injuries of the internal structures as
result of rib fracture.
9. What is the cervical rib? and what is its clinical
significance?
28
13. Give the tributaries of the azygos vein.
14. Describe the sites of origin of the diaphragm.
15. Give the action and nerve supply of the diaphragm.
29
16. Mention the structures passing through the major
openings of the diaphragm.
17. Give the sources of the diaphragm development.
18. Describe different types of the diaphragmatic hernias.
30
19. Describe the attachments and the direction of the fibers of
the muscles of the anterior abdominal wall.
20. Give the contents of the rectus sheath.
21. Give the boundaries of inguinal canal.
31
B. MCQS:
1- One of the following statements is correct regarding the average
length of adult male vertebral column:
a- 100 cms
b- 50 cms
c- 40 cms
d- 70 cms
2- Regarding the average length of female vertebral column; one is
correct:
a- 70 cms
b- 65 cms
c- 50 cms
d- 55 cms
3- One statement is wrong concerning the vertebral column:
a- It is convex anteriorly in the cervical region
b- The number of thoracic vertebrae is 12
c- The intervertebral foramina lie between the laminae of vertebrae
d- Its primary curvature is C-shape
4- Which of the following characteristics is helpful in differentiating
between cervical and lumbar vertebrae:
a- Foramen transverserium.
b- Articular fact in the body.
c- Triangular vertebral canal.
d- Heavy vertebral body.
5- Which of these parts of vertebral column show concavity back-
wards in secondary curves:
a- Cervical.
b- Thoracic.
c- Sacral.
d- Coccyx.
32
6- Regarding the blood supply to the chest wall; mark the most
correct answer:
a- The posterior intercostal arteries supply the upper six intercostal
spaces.
b- The internal thoracic artery arises from the subclavian artery and
supplies the anterior part of lower six intercostal spaces.
c- The neurovascular bundle passes around the chest wall in the
subcostal groove deep to the internal intercostal muscle.
d- Arises from descending aorta only.
7- The Internal Mammary artery arises from:
a- Costocervical trunk.
b- Transverse Cervical artery.
c- Brachiocephalic artery.
d- Subclavian artery
8- Select the incorrect answer concerning the diaphragm:
a- Develops from the septum transversum and cervical myotomes.
b- Receives a nerve supply from both the phrenic and intercostal
nerves.
c- An opening in the central tendon transmits the inferior vena cava.
d- The inferior vena cava passes through the diaphragm at the level of
the T12 vertebra.
9- Regarding the movements of respiration; select the wrong answer:
a- Contraction of the diaphragm increases the vertical diameter of
thorax.
b- Elevation of 3-6 ribs is accompanied by rotation of their necks around
their longitudinal axes.
c- The amount of elevation and forward thrust of the anterior extremities
of 3-6 ribs is limited.
d- During inspiration, the last rib is fixed by the quadratus lumborum
muscle.
33
10- Regarding the intercostal arteries, choose the incorrect answer:
a- The anterior intercostal arteries give branches to the medial half of
the breast.
b- The upper two posterior intercostal arteries are branches of the
costocervical trunk.
c- The posterior intercostal arteries give branches to the spinal cord.
d- In the costal groove, the intercostal artery runs above the
accompanying vein.
11- Regarding the thoracic skeleton; choose the incorrect answer:
a- The jugular notch of the manubrium lies at the level of the disc
between T1 and T2.
b- The sternal angle lies at the level of the disc between T4 and T5.
c- The anterior longitudinal ligament prevents hyperextension of the
vertebral column.
d- The typical rib articulates with the numerically corresponding vertebra
and the vertebra above.
12- Choose the correct answer regarding the vessels of the thoracic
wall:
a- The 1st and 2nd posterior intercostal arteries are branches of the
costocervical trunk.
b- The 1st posterior intercostals veins drain into the brachiocephalic
veins.
c- The inferior hemiazygos vein arises usually from the right renal vein.
d- The lymph vessels of the thoracic wall drain into the intercostal lymph
nodes.
13- ONE of the following statements is correct regarding the intercostal
nerve:
a- It runs between the internal and innermost intercostal muscles.
b- It gives motor branches to the pleura.
c- The fifth intercostal nerve has a thoraco-abdominal course.
d- It passes in the costal groove between the intercostal artery and vein.
34
14- Mark the correct statement regarding the mechanism of respiration:
a- When the shafts of the ribs are elevated, they rise in a forward
direction.
b- The amount of forward thrust of the anterior extremities of 3-6 ribs is
much greater than that of 7-10 ribs.
c- The first rib is relatively fixed during expiration.
d- The elevating force of intercostal muscles is expended to push the
middle parts of 3-6 ribs outwards.
15- Regarding the neurovascular bundle in the intercostal space,
choose the correct statement:
a- All anterior intercostal arteries are branches from the internal thoracic
artery.
b- All intercostal nerves are the anterior rami of thoracic spinal nerves.
c- All posterior intercostal arteries are branches from descending
thoracic aorta.
d- All anterior intercostal veins drain into azygos vein.
16- One of the following structures is not present at the level of the
sternal angle:
a- The second rib articulates with sternum.
b- The trachea bifurcates.
c- The termination of the arch of the aorta.
d- The beginning of the superior vena cava.
17- Concerning the intercostal and subcostal arteries, choose the true
statement:
a- They lie highest in the costal groove.
b- First two posterior intercostal arteries are indirect branches of the
costocervical trunk.
c- Posterior intercostal arteries are indirect branches of thyrocervical
trunk.
d- All anterior intercostal arteries are direct branches from internal
thoracic and superior epigastric arteries.
18- Regarding the external intercostal muscle, indicate the wrong
statement:
a- It is most superficially placed muscle of the intercostal space.
b- Its fibers are directed downward and forward.
c- It is continued backwards as posterior intercostal membrane.
35

d- It extends from the rib tubercle to the costochondral junction.
19- Regarding the inguinal canal, choose the correct answer:
a- The deep inguinal ring lies in the fascia transversalis
b- A direct inguinal hernia comes through the deep inguinal ring
c- The posterior boundary of the canal is formed by the external oblique
aponeurosis
d- The superficial inguinal ring lies below and lateral to the pubic tubercle
20- The ligament that extends from the anterior superior iliac spine to
the pubic tubercle is the:
a- Lacunar
b- Interfoveolar
c- Inguinal
d- Ilio-pectineal
21- Regarding the motor innervation to the diaphragm, choose one
correct answer:
a- Vagus nerve
b- Thoracic splanchnic nerve
c- 3rd, 4th and 5th thoracic nerves
d- Phrenic nerve
22- Which of the following arteries is used to differentiate between
direct and indirect inguinal hernia?
a- Obturator
b- Deep external pudendal
c- Femoral
d- Inferior epigastric
23- Which nerve is identified by its position on the anterior surface of
the psoas major muscle?
a- Femoral
b- Ilioinguinal
c- Genitofemoral
d- Obturator
24- Regarding the anterior abdominal wall, one of the following
statements is correct:
a- The inferior epigastric artery ascends on the medial side of the deep
inguinal ring
36
b- The ilioinguinal and iliohypogastric nerves pierce the rectus abdominis
muscle
c- The upper part of the rectus abdominis muscle rests directly on the
fascia transversalis
d- The tendinous intersections of the rectus abdominis are connected to
the posterior wall of the rectus sheath
25- Regarding the inguinal ligament, one of the following statements is
correct:
a- It is attached laterally to the anterior superior iliac spine
b- The lacunar ligament extends from the lateral part of the inguinal
ligament to the pectineal line
c- It is attached medially to the pubic crest
d- It is pulled downwards by the Scarpa's fascia
26- Regarding the diaphragm, one of the following statements is
correct:
a- The inferior hemiazygos vein passes through the right crus
b- The sympathetic chain passes deep to the lateral arcuate ligament
c- The esophagus passes through the left crus
d- The inferior vena cava passes through the central tendon
27- Regarding the conjoint tendon, one of the following statements is
correct:
a- It lies in the medial half of the posterior wall of the inguinal canal
b- It is controlled by the iliohypogastric nerve
c- It lies posterior to the lower part of the rectus sheath
d- It is formed of the fused arched fibers of the external oblique and
transversus abdominis muscles.
28- Regarding the indirect inguinal hernia, one of the following
statements is not correct:
a- It is a common form of hernia in males
b- It pushes the posterior wall of the inguinal canal
c- The neck of the sac lies at the deep inguinal ring
d- It extends to the scrotum
37
29- Regarding the rectus abdominis, one of the following statements is
correct:
a- It arises from the front of symphysis pubis and pubic crest
b- Is inserted into seventh, eighth and ninth costal cartilages and xiphoid
process
c- Its tendinous inter sections are strongly attached to the posterior wall
of rectus sheath
d- Is supplied by ilio-inguinal nerve
30- Which one of the following nerves is a branch of the sacral plexus?
a- Inferior gluteal nerve.
b- Femoral.
c- Obturator nerve
d- Lateral cutaneous nerve of the thigh.
31- Regarding the levator ani muscle, which one of the following
statements is correct?
a- In the female, the anterior part of the muscle forms a sphincter around
the vagina.
b- It is supplied by the inferior rectal nerve through its pelvic surface.
c- It shares in the lateral wall of the ischiorectal fossa.
d- Its anterior border is related to the coccygeus muscle.
C. Fill in the blanks:
1. The typical intercostal nerve communicates with the sympathetic
trunk by ………………………… and …………………………
2. The typical intercostal nerve gives ………………………… and
…………………… cutaneous branches.
3. The anterior intercostal arteries arise from …………………………
and ………………………… arteries.
4. The posterior intercostal arteries arise from…………………………
and …………………
5. The azygos vein emerges from …………….. and passes to the
thorax by passing through ……………… opening of the diaphragm.
38
6. The azygos vein end in ………. opposite ……….. costal cartilage.
7. The right superior intercostal vein ends in……………………… vein
while the left superior intercostal vein ends in ……………… vein.
8. Regarding the diaphragm the arteries supplying the superior
surface are the ….. and ……………. arteries.
9. Regarding the diaphragm the entire motor supply is from the
……………….. while the peripheral parts of the diaphragm receive
their sensory nerve fibers from …………………
10. Nerve supply of external abdominal oblique is ………………… and
…………………
11. Arteries behind rectus abdominis are ………………… and
…………………
12. Origin of the rectus abdominis is from ………………… and
…………………
13. Two muscles arising from the inguinal ligament are …………………
and ……………
14. Attachments of conjoint tendon are ………………… and
…………………
15. The ligament which connects the spinous processes of two
vertebrae is ……………………
16. The ligament which connects the apices of two spinous processes
of vertebrae is ……………………
17. The intervertebral disc is formed of two parts: A ………… B
…………
18. The vertebral column is convex anteriorly in two regions: A
……………… B ………………
19. The neural (vertebral) foramen is present between ……………………
of vertebra
20. The vertebra which has foramen in the transverse process is
…………The vertebra which has a facet or demifacet on the side of
the body of vertebra is the …………………
39
21. Among the contents of the sacral canal are …….. and ………..
22. Antero-posterior diameter of the pelvic inlet is the distance from
…………. to ………….
23. Antero-posterior diameter of the pelvic outlet is the distance
From………….. to ………….
24. Upper surface of levator ani muscle is supplied by………nerve,
while its lower surface is supplied by……….nerve.
40
C. Cross Matching:
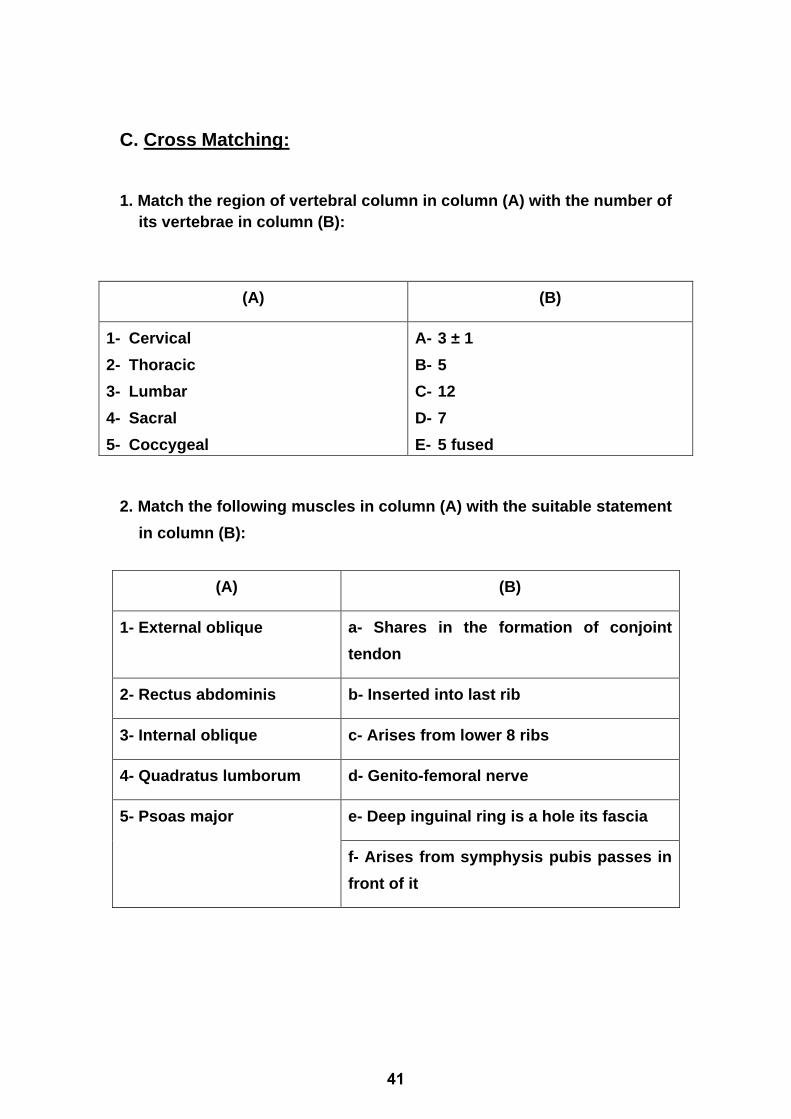
1. Match the region of vertebral column in column (A) with the number of
its vertebrae in column (B):
(A) (B)
1- Cervical
2- Thoracic
3- Lumbar
4- Sacral
5- Coccygeal
A- 3 ± 1
B- 5
C- 12
D- 7
E- 5 fused
2. Match the following muscles in column (A) with the suitable statement
in column (B):
(A) (B)
1- External oblique a- Shares in the formation of conjoint
tendon
2- Rectus abdominis b- Inserted into last rib
3- Internal oblique c- Arises from lower 8 ribs
4- Quadratus lumborum d- Genito-femoral nerve
5- Psoas major e- Deep inguinal ring is a hole its fascia
f- Arises from symphysis pubis passes in
front of it
41

42
Musculoskeletal II module MUS II 215
BY
PROF. DR. GHADA FAROUK MOHAMED
PROFESSOR & HEAD OF HISTOLOGY AND CELL BIOLOGY DEPARTMENTFACULTY OF MEDICINE - MTI
PROFESSOR OF HISTOLOGY AND CELL BIOLOGYFACULTY OF MEDICINE - ASU
Histology
43

44
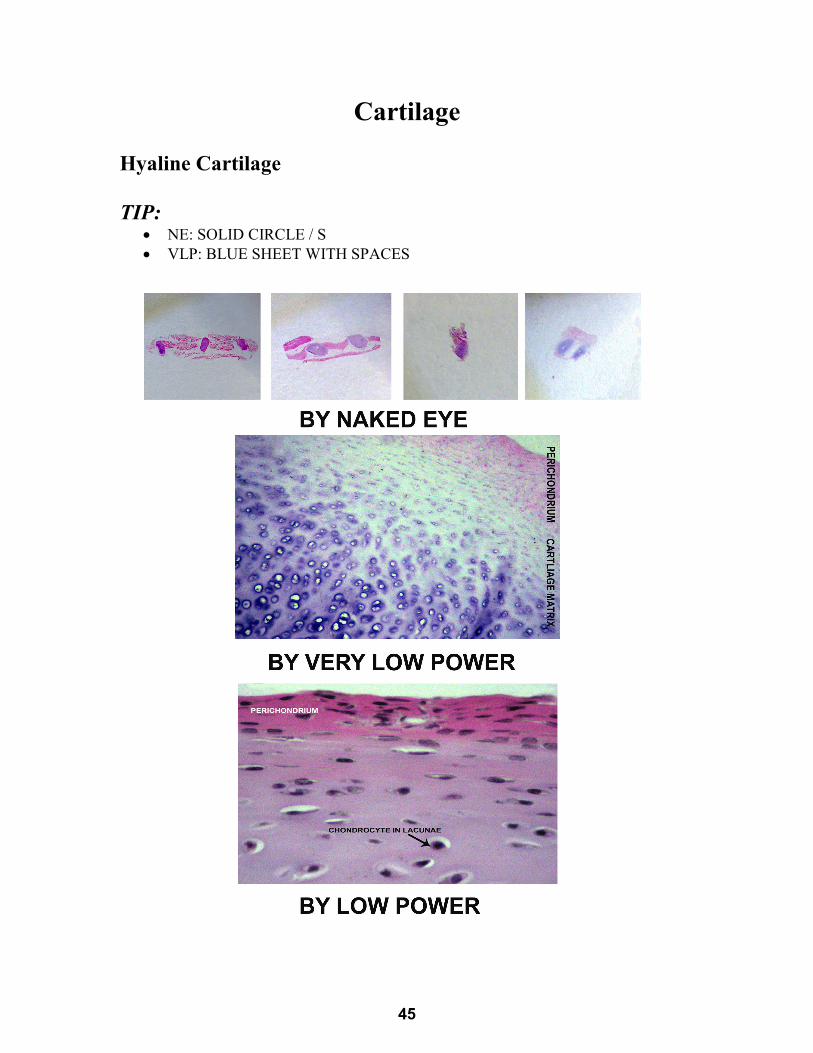
Cartilage
Hyaline Cartilage
TIP: • NE: SOLID CIRCLE / S• VLP: BLUE SHEET WITH SPACES
45
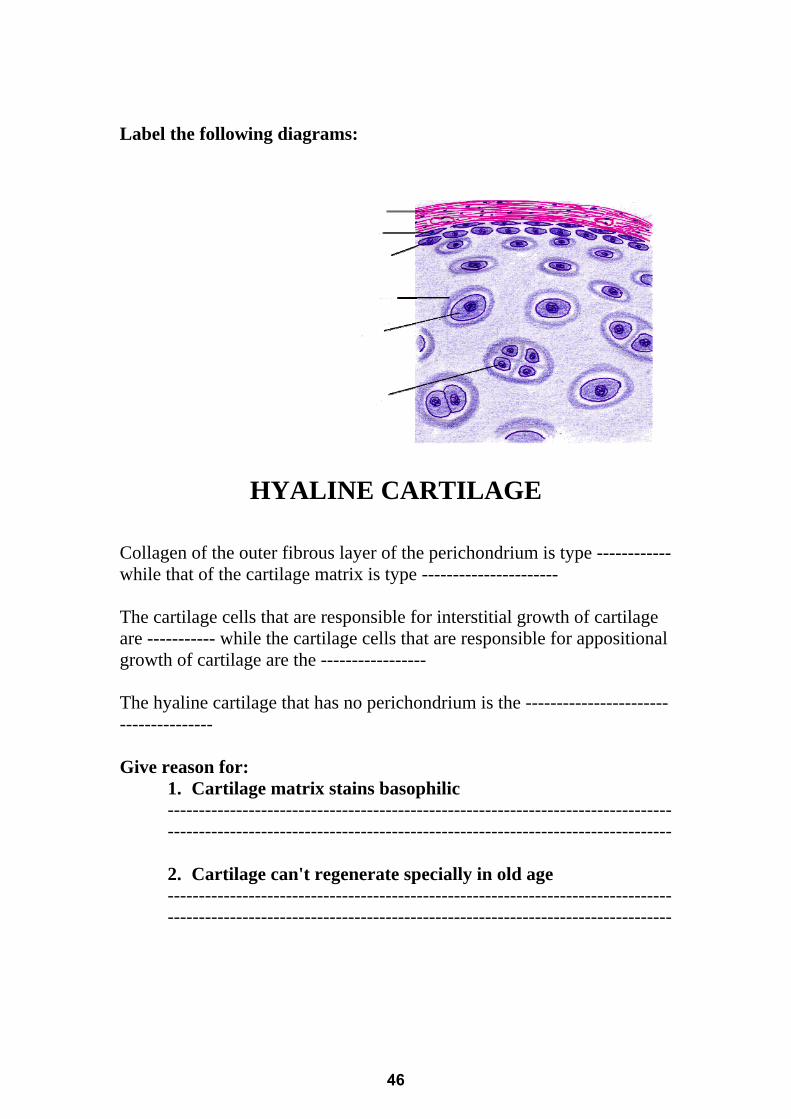
Label the following diagrams:
HYALINE CARTILAGE
Collagen of the outer fibrous layer of the perichondrium is type ------------while that of the cartilage matrix is type ----------------------
The cartilage cells that are responsible for interstitial growth of cartilage are ----------- while the cartilage cells that are responsible for appositional growth of cartilage are the -----------------
The hyaline cartilage that has no perichondrium is the --------------------------------------
Give reason for:
1. Cartilage matrix stains basophilic ------------------------------------------------------------------------------------------------------------------------------------------------------------------ 2. Cartilage can't regenerate specially in old age ------------------------------------------------------------------------------------------------------------------------------------------------------------------
46
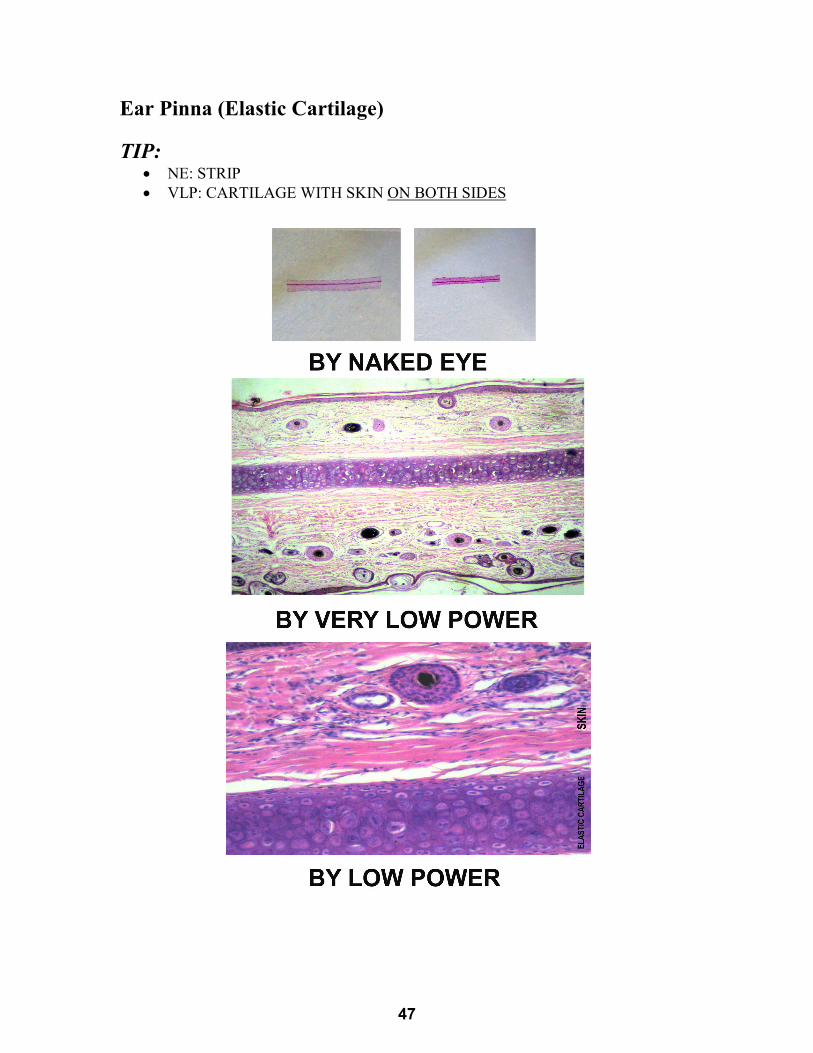
Ear Pinna (Elastic Cartilage) TIP:
• NE: STRIP • VLP: CARTILAGE WITH SKIN ON BOTH SIDES
47
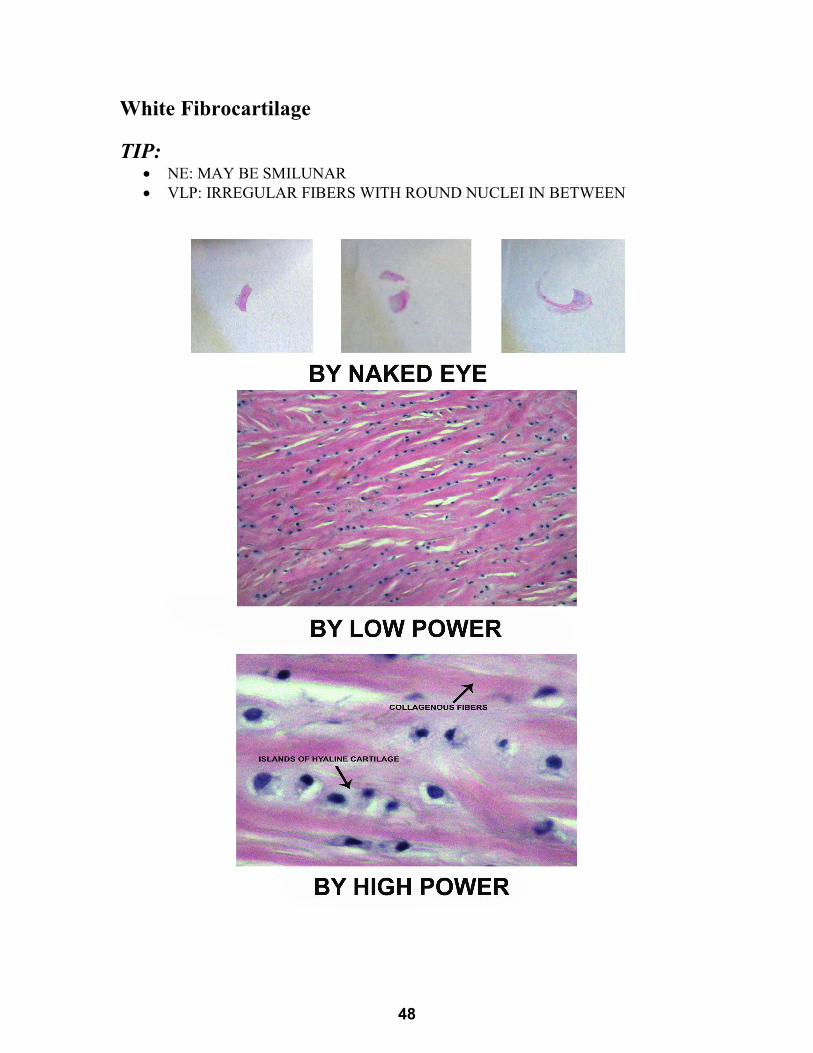
White Fibrocartilage TIP:
• NE: MAY BE SMILUNAR • VLP: IRREGULAR FIBERS WITH ROUND NUCLEI IN BETWEEN
48
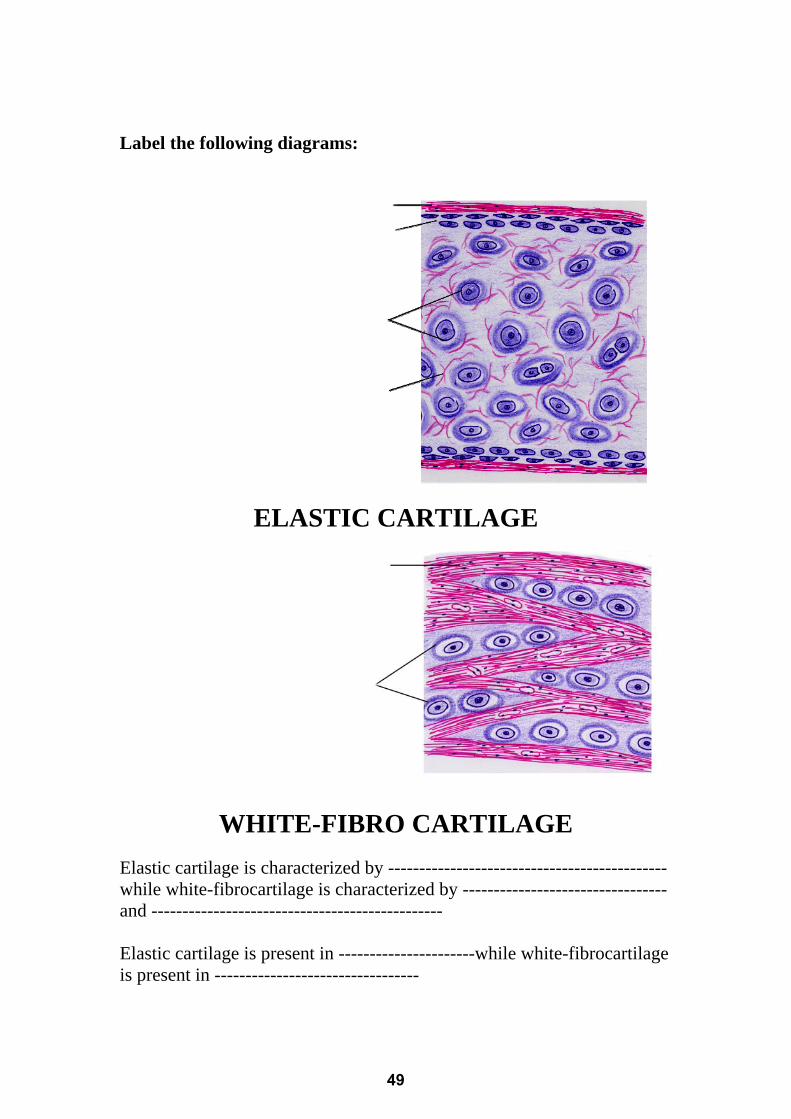
Label the following diagrams:
ELASTIC CARTILAGE
WHITE-FIBRO CARTILAGE
Elastic cartilage is characterized by ---------------------------------------------while white-fibrocartilage is characterized by --------------------------------- and -----------------------------------------------
Elastic cartilage is present in ----------------------while white-fibrocartilage is present in ---------------------------------
49
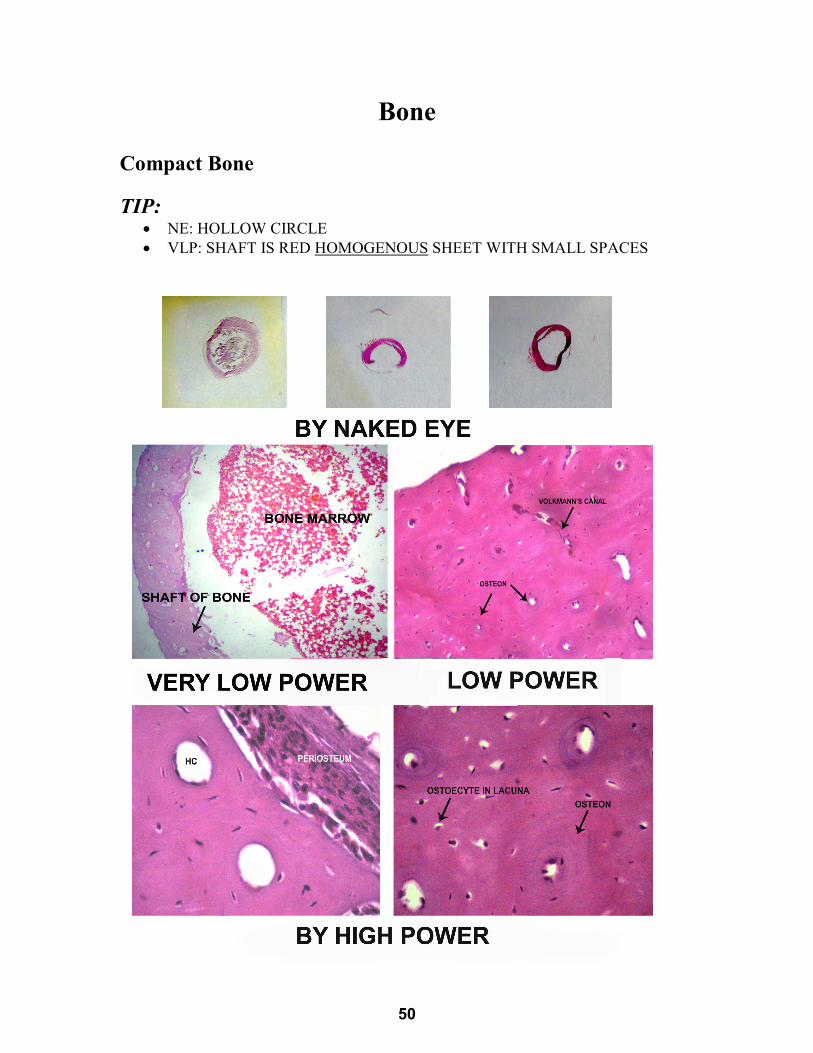
Bone Compact Bone TIP:
• NE: HOLLOW CIRCLE • VLP: SHAFT IS RED HOMOGENOUS SHEET WITH SMALL SPACES
50
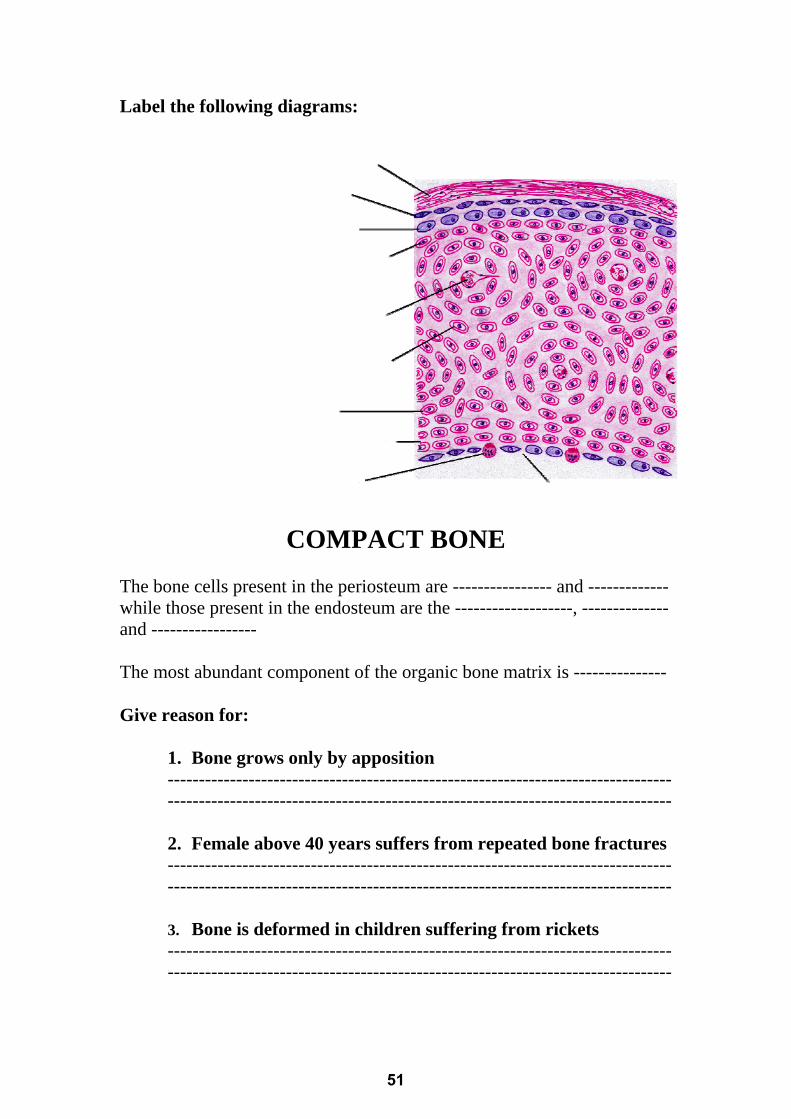
Label the following diagrams:
COMPACT BONE The bone cells present in the periosteum are ---------------- and -------------while those present in the endosteum are the -------------------, --------------and -----------------
The most abundant component of the organic bone matrix is ---------------
Give reason for:
1. Bone grows only by apposition ------------------------------------------------------------------------------------------------------------------------------------------------------------------
2. Female above 40 years suffers from repeated bone fractures ------------------------------------------------------------------------------------------------------------------------------------------------------------------
3. Bone is deformed in children suffering from rickets ------------------------------------------------------------------------------------------------------------------------------------------------------------------
51
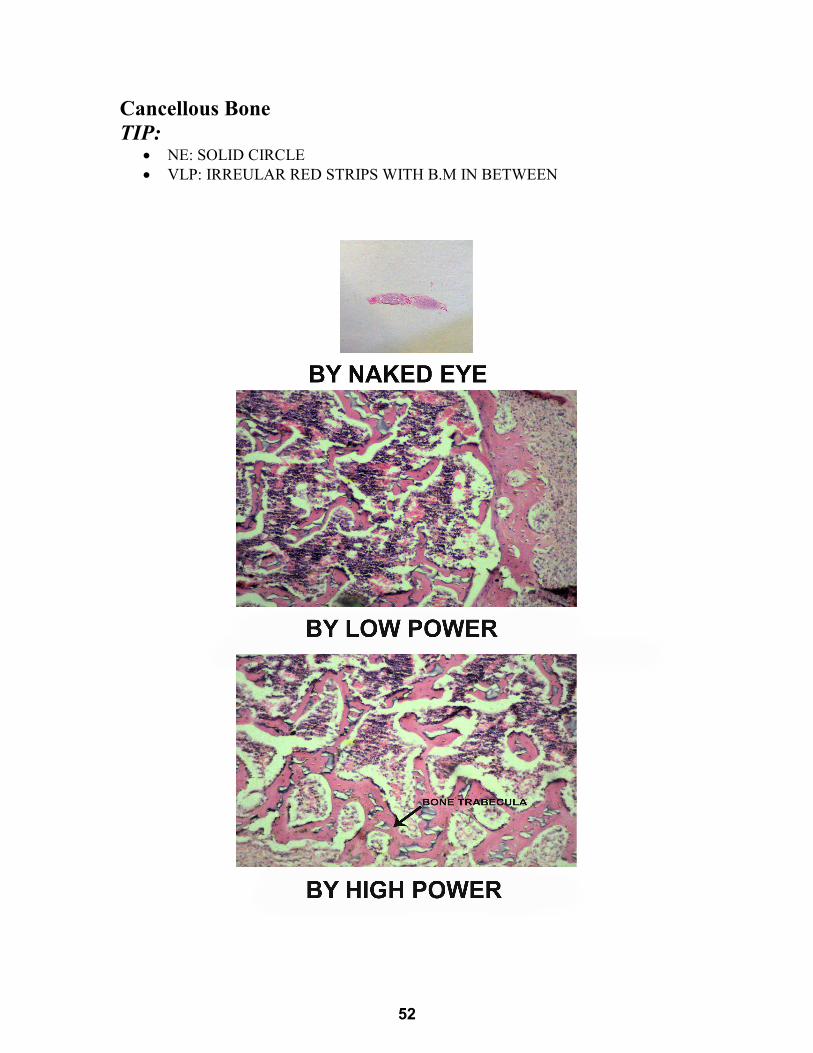
Cancellous Bone TIP:
• NE: SOLID CIRCLE • VLP: IRREULAR RED STRIPS WITH B.M IN BETWEEN
52
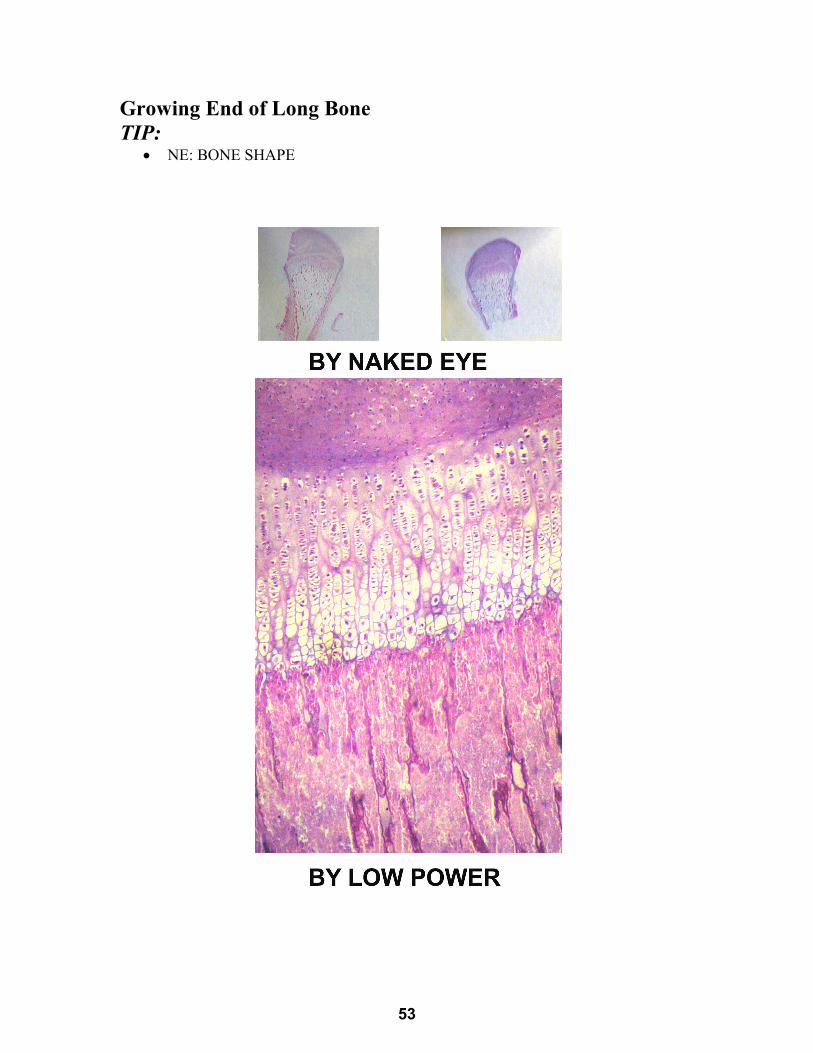
Growing End of Long Bone TIP:
• NE: BONE SHAPE
53
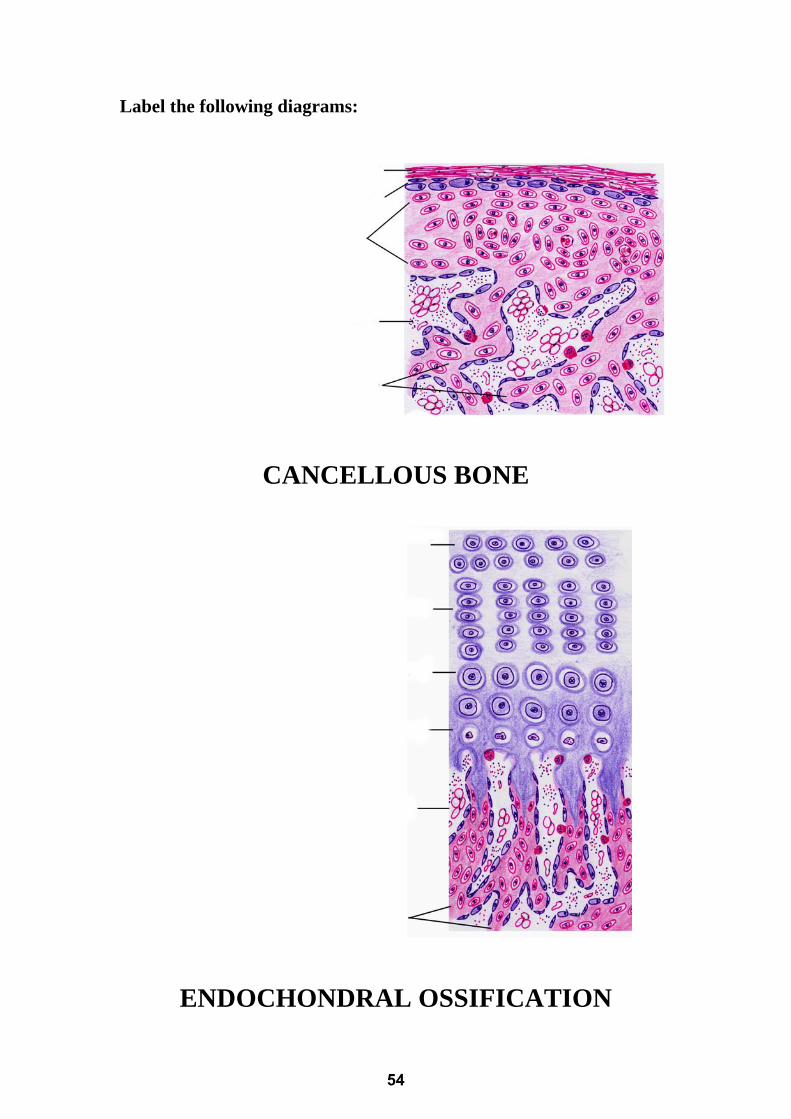
Label the following diagrams:
CANCELLOUS BONE
ENDOCHONDRAL OSSIFICATION
54
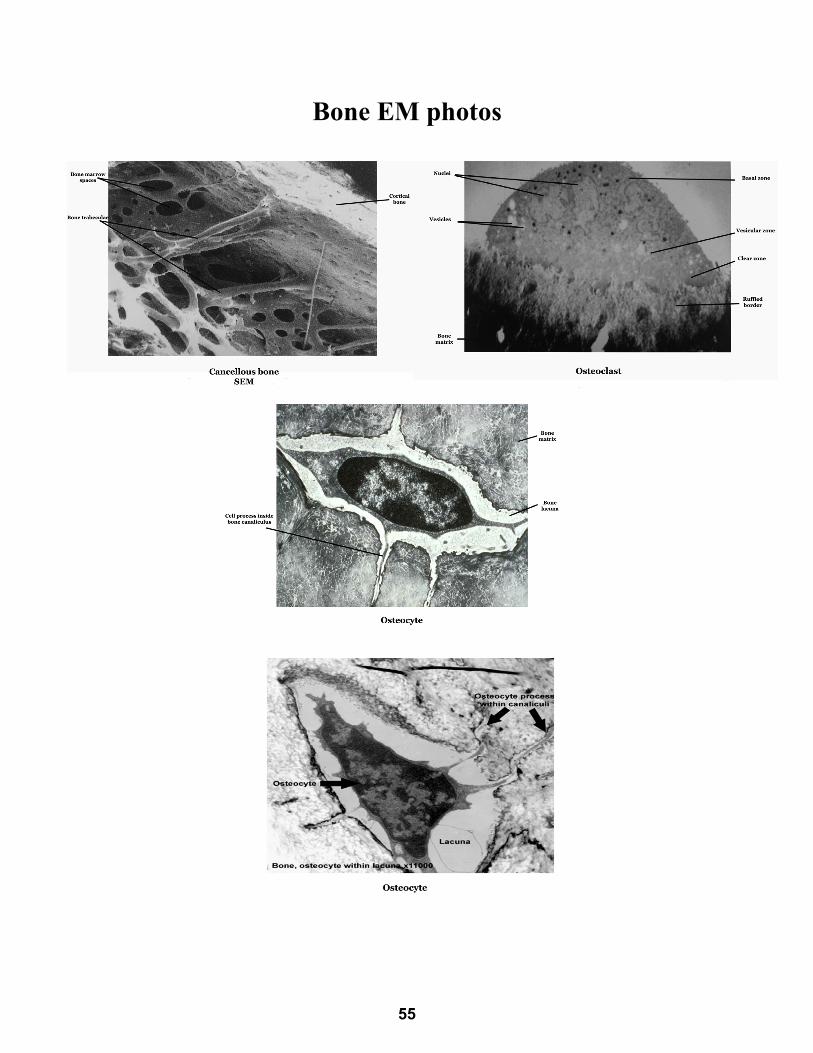
Bone EM photos
55
CARTILAGE MCQ 1. The most common type of cartilage is:
a) Yellow elastic cartilageb) Hyaline cartilagec) White fibrocartilaged) Cancellous cartilage
2. The hyaline cartilage is found in:a) Ear pinnaeb) Semilunar cartilagesc) Intervertebral discsd) Articular cartilages
3. The following are cells of cartilage:a) Fibroblasts – fibrocytes – macrophages.b) Chondroblasts – chondrocytes.c) Osteocytes – osteoblastsd) Neutrophils - eosinophils
4. The cells those are responsible for appositional growth in cartilage:a) Fibroblastsb) Osteoblastsc) Chondrocytesd) Chondroblasts
5. The cells those are responsible for interstitial growth in cartilage:a) Fibroblastsb) Osteoblastsc) Chondrocytesd) Chondroblasts
6. Chondroblast and chondrocyte could secrete:a) Collagen type Ib) Collagen type IIc) Reticular fibersd) Collagen type IV
7. Elastic cartilage is found in:a) Costal cartilageb) Fetal skeletonc) Ear pinnaed) Wall of bronchi
56
8. Chondrocytes in costal cartilage obtain their nutrition:
a) By gap junctions between the chondrocytes b) By diffusion from perichondrial vessels c) By penetrating blood vessels in their matrix d) Through specialized lymphatics
9. A 60-year old obese female came to the orthopedic clinic
complaining of knee joint pain. She was diagnosed as osteoarthritis. The most affected structure in her joint is:
a) The menisci b) The cruciate ligament c) Articular cartilage d) Upper tibial epiphysis
10. Concerning hyaline cartilage: a) It is vascular type of cartilage b) It has collagen type I in its matrix c) It is always surrounded by perichondrium d) It develops from mesenchymal C.T.
11. Cartilage matrix is characterized by: a) Being poor in water content b) Being acidophilic by H&E staining c) Presence of large amount of sulfated GAGs d) Presence of type III collagen
12. White fibro-cartilage: a) Is a vascular type of cartilage b) Has elastic fibers in its matrix c) Is surrounded by perichondrium d) Develops from ectoderm.
13. Regarding chondroblasts, they: a) Develop from chondrocytes b) Are present in cell nests c) Secrete collagen type II d) Have eccentric nucleus
14. Which of the following correctly pairs the type of cartilage to its
component? a) Elastic cartilage - type III collagen and elastin. b) Elastic cartilage - type I collagen. c) Hyaline cartilage - type IV collagen and elastin d) Hyaline cartilage -70% water.
57
15. The following structure contains hyaline cartilage:
a) Epiglottis. b) Bronchi. c) Intervertebral disc. d) Bronchioles.
16. Concerning elastic cartilage:
a) It is a vascular type of cartilage. b) It has collagen type I in its matrix. c) It is surrounded by perichondrium. d) It develops from ectoderm.
17. The cartilage which is not covered by perichondrium: a) Costal cartilage b) Articular cartilage c) Laryngeal cartilage d) Eustachian tube
18. A herniated intervertebral disc was removed surgically from the
lumbar region of a 48-year-old man. Which of the following types of tissue is located within the peripheral annulus of this patient’s intervertebral disc?
a) Dense, irregular connective tissue b) Dense, regular connective tissue c) Elastic cartilage d) Fibrocartilage
19. Intervertebral disc is formed of:
a) Hyaline cartilage b) White fibrocartilage c) Yellow elastic cartilage d) Cancellous bone
20. Concerning interstitial growth of cartilage, the true is:
a) It is due to activity of inner chondrogenic layer of perichondrium
b) It means growth of cartilage from outside c) It is the type of growth which persist throughout life d) There is no interstitial growth in cartilage
58
21. The outer fibrous layer of the perichondrium is: a) Formed of chondrogenic cells and chondroblast b) Responsible for appositional growth of cartilage c) Responsible for nourishment of cartilage d) Contain mainly elastic fibers
22. One of the following is true about chondrocytes:
a) They develop from chondrogenic cells b) They are branched cells c) They secrete collagen type I d) They are present in cell nests
23. Cartilage matrix contains:
a) Collagen type II. b) Osteonectin. c) Little tissue fluid. d) Hydroxy apatite crystals.
24. PAS positive staining of the cartilage matrix is due to presence of:
a) Chondroitin sulphate b) Glycoproteins c) Proteoglycans d) Collagen type II
25. All of the following are components of hyaline cartilage matrix
EXCEPT: a) Collagen b) Hyaluronic acid c) Capillaries d) Tissue fluid
BONE MCQ
1. One of the following is considered a bone resorbing cell: a) Osteogenic cell b) Osteocyte c) Osteoblast d) Osteoclast
2. Inorganic matrix of bone is:
a) Collagen type I and III b) Proteoglycan and glycosaminoglycan c) Glycoprotein and glycolipids d) Calcium and phosphate
59
3. The bone cell that has acidophilic cytoplasm is: a) Osteogenic cell b) Osteoblast c) Osteoclast d) Osteocytes
4. Osteocytes are connected together by:
a) Adherent junctions b) Gap junctions c) Tight junctions d) Desmosomes
5. Immature bone present in adult at one of the following:
a) Shaft of long bone b) Cancellous bone c) Tooth socket d) Flat bone
6. Bone development by one of the following:
a) Appositional b) Interstitial c) Intramembranous d) Transitional
7. The 5 zones present at any growing end of long bone are:
a) Proliferating – calcification- hypertrophy- resting -ossification
b) Resting – hypertrophy- proliferating- calcification-ossification
c) Resting –proliferating-hypertrophy-calcification-ossification d) Proliferating-hypertrophy- resting –calcification-ossification
8. One of the following is correct as regard the periosteum: a) Formed of osteocytes and osteoclasts b) Contains no blood vessels c) Responsible for appositional growth d) None of the above
9. As regard osteoclasts, they:
a) Develop from osteocytes b) Considered as bone forming cells c) Contain basophilic cytoplasm d) Are multinucleated cells
60
10. Howship’s lacunae are: a) Present in white fibrocartilage. b) Sites where osteoclasts are present. c) Increased in number in bone forming sites d) Sites of insertion of tendon to bone.
11. Compact bone is:
a) Formed of regular bone lamellae. b) Formed of branching bone trabeculae c) found in the middle of flat bones d) Characterized by absence of Haversian canal.
12. Cancellous bone:
a) Consists of circumferential bone lamellae. b) Presents in shafts of long bones. c) Formed of irregular bone lamellae. d) Their Haversian system formed of osteocytes.
13. Haversian canals are
a) Surrounded by concentric lamella b) Lined by osteoblasts c) Arranged longitudinally in bone d) All of the above
14. Under the periosteum there is:
a) Outer circumferential lamellae b) Inner circumferential lamellae c) Interstitial lamellae d) Concentric lamellae
15. A mother of a 3-year old boy came to the pediatric clinic
complaining that her child has a short stature, delayed teeth eruption and bow legs. This condition is attributed to:
a) Defective collagen content of bone b) Defective mineralization of bone c) Delayed closure of the epiphysis d) Increased bone resorption
16. Osteopetrosis is characterized by:
a) Genetic defect in the brush border of osteoclast b) Thinning out of bone trabeculae c) Defective mineralization of bone matrix d) Widening of bone marrow spaces
61
17. 60 year old female patient came to the clinic complaining of repeated fractures on minor trauma. What would you expect to find in her bone structure?
a) Thickened bone trabeculae b) Diminished bone marrow spaces c) Decreased collagen content in bone matrix d) Defective mineralization of bone matrix
18. In a 30 year old male person with pituitary adenoma “increased
growth hormone”, there will be: a) Increased thickening of bone b) Increased length of bone c) Increased bone mineralization d) Increased bone resorption
19. A patient suffering from leucopenia and anemia. The investigations
revealed marked thickening of the bone trabeculae with narrowing of the bone marrow cavities. This lesion is attributed to a defect in:
a) Osteoclasts b) Osteoblasts c) Osteocytes d) Osteoprogenitors
20. The outer circumferential lamellae are present:
a) Around endosteum b) Under periosteum c) Between Haversian systems d) Around the Haversian canal
21. The following is a character of immature bone:
a) Few number of osteocytes b) Low mineral contents c) Low amount of water d) Regular arrangement of collagen fibers
22. Bone canaliculi:
a) Connect Haversian canals to each other. b) Connect Haversian canals to periosteum. c) Contain processes of osteocytes. d) Fix periosteum to outer circumferential lamellae.
62
23. In healing of bone fracture, osteoblasts help in bone formation through secreting:
a) Alkaline phosphatase b) Acid phosphatase c) Pyrophosphates d) Collagenase
24. A 70 year old female presented to the clinic complaining of bone
aches. She was diagnosed as osteoporosis due to increased bone resorption. The cell responsible for this bone resorption is characterized by being:
a) Immotile b) Branching c) Multinucleated d) Deeply basophilic
25. Osteoperosis is characterized by: a) Genetic defect in the brush border of osteoclast b) Thinning out of bone trabeculae c) Defective mineralization of bone matrix d) Narrowing of bone marrow spaces
26. Sharpey’s fibers connect: a) Endosteum to the inner bone lamellae. b) Periosteum to the outer bone lamellae. c) Volkmann’s canals together. d) Haversian canals together.
27. One of the following characterizes osteoclasts: a) Deeply acidophilic cytoplasm b) Abundant SER c) Gap junction connecting their processes d) Small pyknotic central nucleus
28. The cells present in the inner osteogenic layer of the periosteum are: a) Osteoblasts and osteocytes b) Osteogenic cells and osteoclasts c) Osteoblasts and osteogenic cells d) Osteocytes and osteoclasts
29. Osteocytes are characterized by being: a) Present in the outer layer of periosteum b) Able to divide and differentiate c) Having processes connected by gap junctions d) Present in Howship´s lacuna
63
30. One of the following is a component of the Haversian system: a) Volkman’s canal b) Perforating fibers of Sharpey c) Concentric bone lamellae d) Inner circumferential bone lamellae
31. Which one of the following is a characteristic feature of cancellous
bone? a) It is formed of bone trabeculae and bone marrow spaces b) Its bone lamellae are regularly arranged c) It contains Haversian systems d) It is mainly present in the shaft of long bones
32. By EM, the nuclei and organelles of osteoclast are seen in the:
a) Ruffled zone b) Clear zone c) Vesicular zone d) Basal zone
33. The inner circumferential lamellae are present:
a) Around endosteum. b) Under periosteum. c) Between Haversian systems. d) Around the Haversian canal.
34. The type of junction between the processes of osteoblasts is:
a) Tight junction. b) Desmosome. c) Hemidesmosome. d) Gap junction.
35. Mature bone has:
a) Regularly arranged collagen fibers. b) Large number of cells. c) Few mineral contents. d) High water content.
36. Osteoclasts:
a) Are small immotile cells b) Have large eccentric nuclei c) Have deep basophilic cytoplasm d) Are present in bone lacunae
64
37. The periosteum contains: a) Osteoblasts and osteocytes b) Osteoblasts and osteogenic cells c) Osteogenic cells and osteoclasts d) Osteocytes and osteogenic
38. One of the following characterizes osteoblasts:
a) Deeply acidophilic cytoplasm b) Abundant SER c) Gap junction connecting their processes d) Brush border toward bone surface
39. During H&E examination of the epiphyseal plate of cartilage, the
zone of hypertrophy shows: a) Numerous cartilage cells arranged in longitudinal rows b) Large cartilage cells accumulating alkaline phosphatase c) Deposition of calcium salts with degenerating chondrocytes d) Formation of bone lamellae with bone marrow spaces
40. By EM, the clear zone of osteoclast has:
a) Finger like processes b) Endocytotic vesicles c) Nuclei and organelles d) Actin filaments
41. The endosteum contains:
a) Osteoblasts and osteocytes b) Osteoblasts and chondroblasts c) Osteogenic cells and osteoclasts d) Osteocytes and osteoclasts
42. Osteogenic cells are characterized by:
a) Being present in the outer layer of periosteum b) Being able to divide and differentiate c) Having processes connected by gap junctions d) Being present in Howship´s lacunae
43. Which of the following structures in a fully grown adult bone would
be closest to the endosteum? a) Concentric lamellae b) Interstitial lamellae c) Inner circumferential lamellae d) Outer circumferential lamellae
65
ANSWERS OF CARTILAGE MCQ ANSWERS OF BONE MCQ
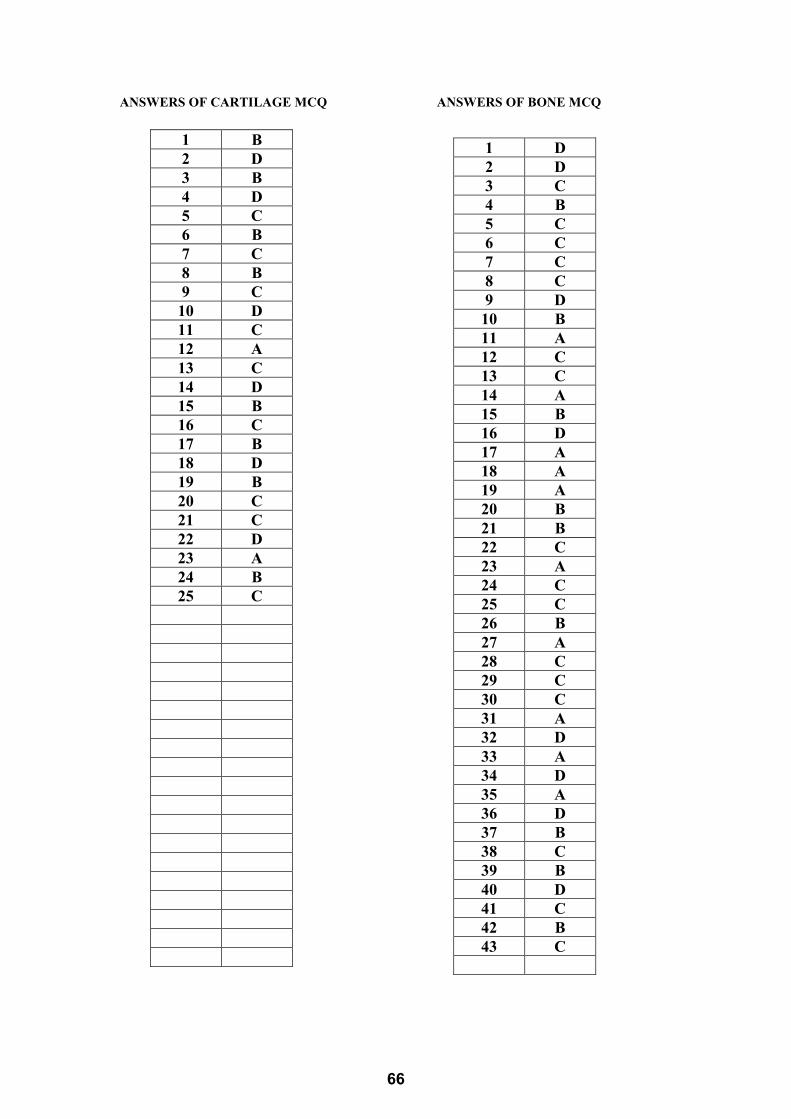
1 B 2 D 3 B 4 D 5 C 6 B 7 C 8 B 9 C 10 D 11 C 12 A 13 C 14 D 15 B 16 C 17 B 18 D 19 B 20 C 21 C 22 D 23 A 24 B 25 C
1 D 2 D 3 C 4 B 5 C 6 C 7 C 8 C 9 D 10 B 11 A 12 C 13 C 14 A 15 B 16 D 17 A 18 A 19 A 20 B 21 B 22 C 23 A 24 C 25 C 26 B 27 A 28 C 29 C 30 C 31 A 32 D 33 A 34 D 35 A 36 D 37 B 38 C 39 B 40 D 41 C 42 B 43 C
66
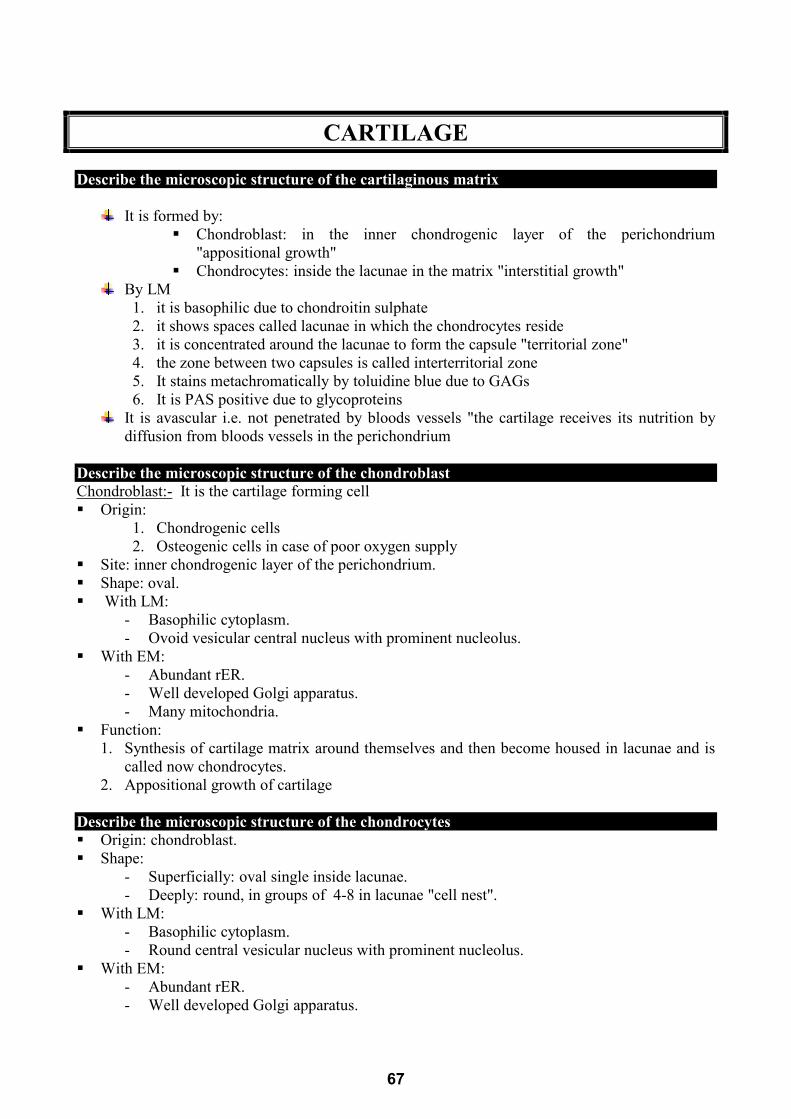
CARTILAGE Describe the microscopic structure of the cartilaginous matrix
It is formed by:
Chondroblast: in the inner chondrogenic layer of the perichondrium "appositional growth"
Chondrocytes: inside the lacunae in the matrix "interstitial growth" By LM
1. it is basophilic due to chondroitin sulphate 2. it shows spaces called lacunae in which the chondrocytes reside 3. it is concentrated around the lacunae to form the capsule "territorial zone" 4. the zone between two capsules is called interterritorial zone 5. It stains metachromatically by toluidine blue due to GAGs 6. It is PAS positive due to glycoproteins
It is avascular i.e. not penetrated by bloods vessels "the cartilage receives its nutrition by diffusion from bloods vessels in the perichondrium
Describe the microscopic structure of the chondroblast UChondroblast:-U It is the cartilage forming cell Origin:
1. Chondrogenic cells 2. Osteogenic cells in case of poor oxygen supply
Site: inner chondrogenic layer of the perichondrium. Shape: oval. With LM:
- Basophilic cytoplasm. - Ovoid vesicular central nucleus with prominent nucleolus.
With EM: - Abundant rER. - Well developed Golgi apparatus. - Many mitochondria.
Function: 1. Synthesis of cartilage matrix around themselves and then become housed in lacunae and is
called now chondrocytes. 2. Appositional growth of cartilage
Describe the microscopic structure of the chondrocytes Origin: chondroblast. Shape:
- Superficially: oval single inside lacunae. - Deeply: round, in groups of 4-8 in lacunae "cell nest".
With LM: - Basophilic cytoplasm. - Round central vesicular nucleus with prominent nucleolus.
With EM: - Abundant rER. - Well developed Golgi apparatus.
67
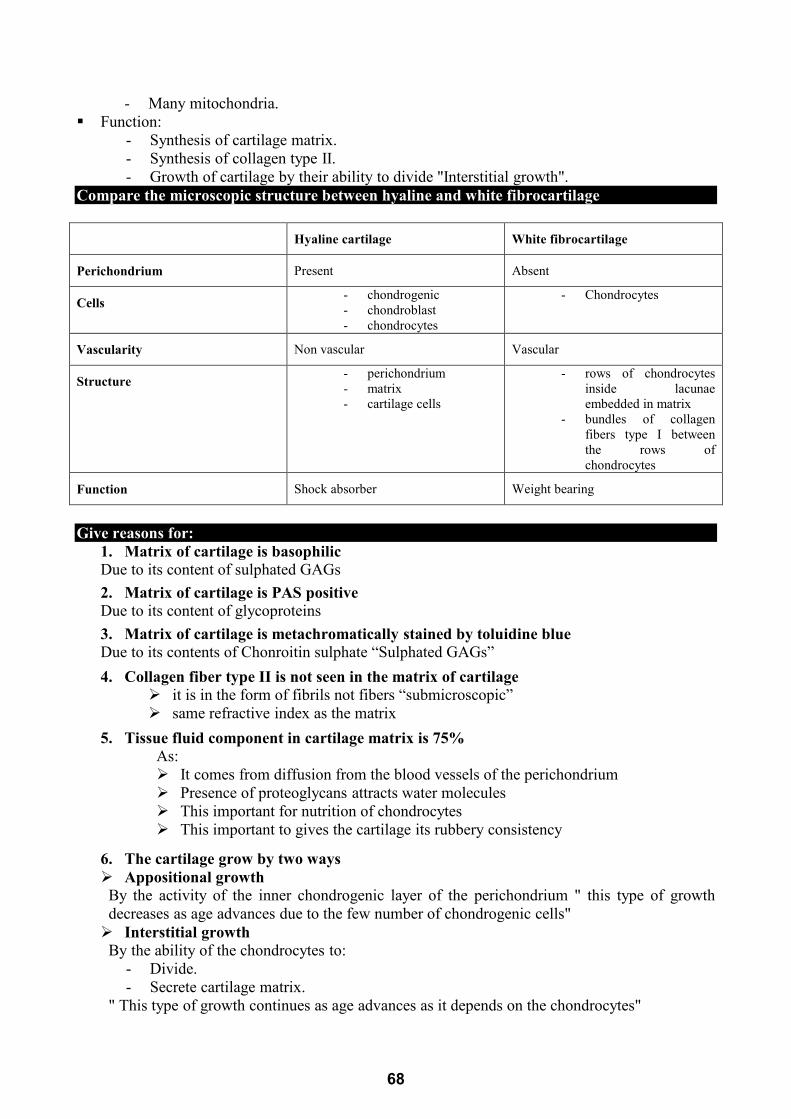
- Many mitochondria. Function:
- Synthesis of cartilage matrix. - Synthesis of collagen type II. - Growth of cartilage by their ability to divide "Interstitial growth".
Compare the microscopic structure between hyaline and white fibrocartilage Hyaline cartilage White fibrocartilage
Perichondrium Present Absent
Cells - chondrogenic - chondroblast - chondrocytes
- Chondrocytes
Vascularity Non vascular Vascular
Structure - perichondrium - matrix - cartilage cells
- rows of chondrocytes inside lacunae embedded in matrix
- bundles of collagen fibers type I between the rows of chondrocytes
Function Shock absorber Weight bearing
Give reasons for:
1. Matrix of cartilage is basophilic Due to its content of sulphated GAGs
2. Matrix of cartilage is PAS positive Due to its content of glycoproteins
3. Matrix of cartilage is metachromatically stained by toluidine blue Due to its contents of Chonroitin sulphate “Sulphated GAGs”
4. Collagen fiber type II is not seen in the matrix of cartilage it is in the form of fibrils not fibers “submicroscopic” same refractive index as the matrix
5. Tissue fluid component in cartilage matrix is 75% As: It comes from diffusion from the blood vessels of the perichondrium Presence of proteoglycans attracts water molecules This important for nutrition of chondrocytes This important to gives the cartilage its rubbery consistency
6. The cartilage grow by two ways Appositional growth By the activity of the inner chondrogenic layer of the perichondrium " this type of growth decreases as age advances due to the few number of chondrogenic cells" Interstitial growth By the ability of the chondrocytes to:
- Divide. - Secrete cartilage matrix.
" This type of growth continues as age advances as it depends on the chondrocytes"
68
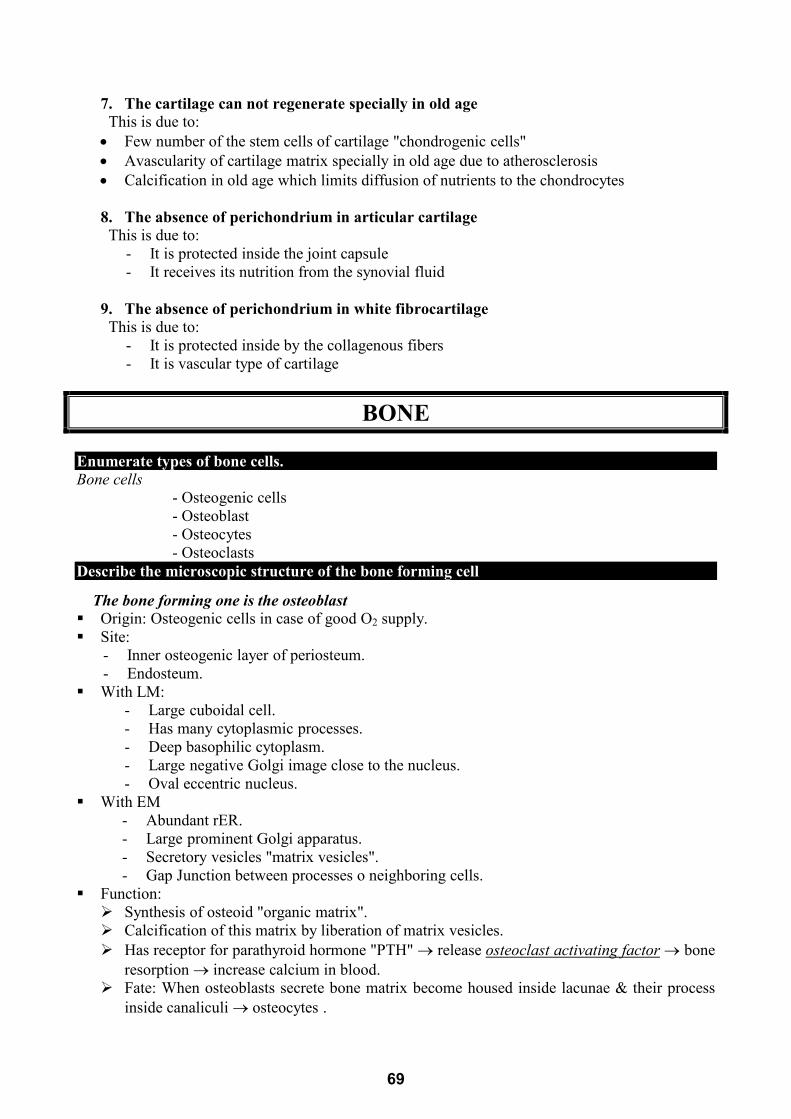
7. The cartilage can not regenerate specially in old age This is due to: • Few number of the stem cells of cartilage "chondrogenic cells" • Avascularity of cartilage matrix specially in old age due to atherosclerosis • Calcification in old age which limits diffusion of nutrients to the chondrocytes
8. The absence of perichondrium in articular cartilage This is due to:
- It is protected inside the joint capsule - It receives its nutrition from the synovial fluid
9. The absence of perichondrium in white fibrocartilage This is due to:
- It is protected inside by the collagenous fibers - It is vascular type of cartilage
BONE Enumerate types of bone cells. Bone cells
- Osteogenic cells - Osteoblast - Osteocytes - Osteoclasts
Describe the microscopic structure of the bone forming cell
The bone forming one is the osteoblast Origin: Osteogenic cells in case of good O2 supply. Site:
- Inner osteogenic layer of periosteum. - Endosteum.
With LM: - Large cuboidal cell. - Has many cytoplasmic processes. - Deep basophilic cytoplasm. - Large negative Golgi image close to the nucleus. - Oval eccentric nucleus.
With EM - Abundant rER. - Large prominent Golgi apparatus. - Secretory vesicles "matrix vesicles". - Gap Junction between processes o neighboring cells.
Function: Synthesis of osteoid "organic matrix". Calcification of this matrix by liberation of matrix vesicles. Has receptor for parathyroid hormone "PTH" → release Uosteoclast activating factor U → bone
resorption → increase calcium in blood. Fate: When osteoblasts secrete bone matrix become housed inside lacunae & their process
inside canaliculi → osteocytes .
69
Describe the microscopic structure of the bone resorping cell UOsteoclast: Origin: recently, from bone narrow precursor → many fuse → multinucleated osteoclast (from
blood monocytes old theory). Site: at bone resorption surfaces:
- Endosteum. - Bone marrow cavities.
With LM: - Large round cell. - Acidophilic cytoplasm. - Has brush border toward the bone surface. - Multinucleated (up to 50 nuclei). - Present in shallow depression in bone surface "Howship's lacuna".
EM: it has four zones: 1) Zone of ruffled border :
- Finger like processed toward the bone surface. - This is the site of bone resorption.
2) Clear zone: • Clear → no organelles. • Contain actin filament. • This anchors the osteoclast to bone surface.
3) Vesicular zone: many endocytotic vesicles & lysosomes. 4) Basal zone: contain the organelles & the numerous nuclei. Function: 1) Bone resorption: 2) It has receptors for:
o Calcitonin: decrease bone resorption o Osteoclast stimulating factor from osteoblast: increase bone resorption
Correlate the microscopic structure to the function of osteoclast
Structure Function
Ruffled border Bone resorption
Clear zone Cell fixation
Vesicular zone • Lysosomes degrading bone collagen
extracelluar
• Endocytotic vesicles containing the
degraded collagen
Basal zone Housing the nuclei and rest of cell organelles
70
Describe the microscopic structure of the Haversian system UHaversian system "Osteon" - It is the structural unit of compact bone - It runs parallel to the longitudinal axis of long bones - It is formed of: U1) Haversian canal - Longitudinal canal parallel to long axis of bone - Contain loose c.t. & neurovascular supply - Connected by transverse or oblique canal "Volkmann's canal" - Lined by endosteum: osteogenic cells & osteoblasts & osteoclasts. U2) Concentric lamellae: - Lamellae of calcified bone matrix around Haversian canal U3) Osteocytes: U inside lacunae in between these lamellae with their processes inside canaliculi Compare the microscopic structure between osteocytes and chondrocytes
Chondrocytes Osteocytes
• Shape: oval or round • Cytoplasmic branches: not branched • Number in lacunae: present singly OR in groups in
lacunae • Division: can divide • Function: responsible for interstitial growth of
cartilage
• Shape: oval • Cytoplasmic branches: branched • Number in lacunae: present singly in lacunae • Division: can't divide • Function: No Interstitial growth in bone
Compare the microscopic structure between osteoblast and osteoclast
Osteoblast Osteoclast
Site Inner osteogenic layer of periosteum and in the endosteum Endostem only
Shape Branched cell Non branched cell with brush
border toward bone surface
Cytoplasm Deeply basophilic with –ve Golgi image Acidophilic cytoplasm
Nucleus Single eccentric multinucleated
EM RER, Golgi, mitochondria and matrix vesicles
4 zones: ruffled, clear, vesicular and basal zones
Receptors For PTH For calcitonin and osteclast stimulating factor
Function Bone formation Bone resorption
71
Give reasons for: • The presence of brush border of osteoclast by LM Brush border of osteoclast seen by LM is due to:
1. Their ruffled border “finger like projection” 2. Exposed collagen fibrils after digestion of matrix
• Bone matrix is acidophilic As collagen is the main constituents " 90%" of bone matrix • No interstitial growth in bone
a. Osteocytes are surrounded by the stony hard matrix b. Osteocytes are end cells and can't divide
• Bone is deformed in children suffering from rickets Due to defective bone mineralization due to deficiency of vitamin D necessary for calcium absorption • Bone is deformed in patients suffering from scurvy "vitamin C deficiency" Due to defective formation of collagen as collagen is the main constituents " 90%" of bone matrix • Female above 40 years suffers from repeated bone fractures As above 40 years estrogen hormone decreases so bone formation decreases and bone resorption overcomes bone formation leading to thinning out of bone and repeated fractures
72
Medical Biochemistry
BY
ASSIST. PROF. DR. MARWA MATBOLI SAYED
Musculoskeletal II module MUS II 215
ASSISST. PROFESSOR & HEAD OF BIOCHEMISTRY DEPARTMENTFACULTY OF MEDICINE - MTI
ASSISST. PROFESSOR OF BIOCHEMISTRYFACULTY OF MEDICINE - ASU
73

74
Table of Contents
Subject
I. Musculoskeletal Module II
1. Introduction to clinical chemistry
2. Colorimetric estimation of blood glucose and diabetic profile
3. SGD1
4. SGD2
5. SGD
6. Work sheet
75
Musculoskeletal Module II
Introduction to Clinical Chemistry
Lab
ILOs of the current topic
By the end of this topic, the student will be able to: 1- Recognize the importance of clinical chemistry in medicine. 2- Outline the main steps of laboratory work flow cycle. 3- Interpret clinical & laboratory findings in the provided case scenario. 4- Define clinical chemistry. 5- Differentiate between plasma and serum. 6- Identify the phlebotomy equipment and the precautions for blood
sampling. 7- Recognize the different types of blood collection tubes and their uses.
Case study
Fatma, 55-year-old woman with type 2 diabetes presented to
El-Maadi Military Hospital, endocrinology clinic with
tingling and numbness sensation in her feet and hands.
Although she was diagnosed with type II diabetes mellitus in
2005, she had symptoms indicating hyperglycemia (polyuria,
polydipsia) for 2 years before diagnosis. She gave history of
unbalanced diet. She received metformin 100 mg twice daily.
She does not test her blood glucose levels at home. The
endocrinologist referred her to perform some laboratory
investigations.
In the lab
She met the doctor. He was very busy and he referred her immediately to lab
technician without taking even a brief history.
In phlebotomy room
76
5 ml of whole blood was withdrawn by the technician immediately without any
safety precaution.
The sample was divided into 2 portions as follows:
2 ml into a tube containing EDTA for Hb1Ac determination.
3 ml into a tube containing fluoride for estimation of blood glucose.
What is your clinical impression? • Type 2 diabetes mellitus complicated with diabetic neuropathy.
On what basis you diagnosed this case?
Based on: Symptoms
Laboratory results
Do you agree with laboratory procedures done to this patient? • NO
What are the proper lab procedures which would be done prior to
venipuncture? 1- Brief history taking. 2- Applying universal precautions for blood Sampling.
77
What is the branch of medicine concerned with chemical laboratory investigations?
• Clinical Chemistry
Clinical Chemistry (also known as chemical pathology, clinical biochemistry or medical
biochemistry)
Definition It is the area of clinical pathology that is generally concerned with analysis of body fluids for diagnostic and therapeutic purposes. The sections of clinical laboratory are:
• Clinical pathology Hematology Clinical chemistry Clinical microbiology Serology Blood bank Histology and cytology
Purpose of Clinical Chemistry Tests:
• Measure levels of substances found normally in human blood that have biological functions.
Examples: Glucose, Calcium. • Detect or measure non-functional metabolites or waste products.
Examples: Creatinine, Blood Urea Nitrogen (BUN). • Detect or measure substances that indicate cell damage or disease.
Examples: Liver enzymes, such as ALT, Cardiac enzymes, such as CK-MB.
• Detect or measure drugs or toxic substances: Examples: Drugs of abuse screen.
Laboratory Work Flow Cycle: The flow cycle includes the entire steps of laboratory test, starting from test ordering by a doctor until reporting the results.
78
Patient Preparation and Instructions: Certain factors may affect results of certain laboratory tests:
o Food consumption
o Medication
o Activity
o Time of day
Types of Specimens for Chemical Analysis:
• Whole blood, serum or plasma. • Urine. • Others: Cerebrospinal Spinal Fluid (CSF) and other fluids.
The phlebotomy equipment:
Disposable syringes or Vacutainer needle
Vacutainers = blood collection tubes
Gauze pads or adsorbent cotton
Tourniquet
Alcohol swap
Waste container
Gloves
Universal Precautions for Blood Sampling:
1. Spray the table with disinfectant solution (Sodium
hypochlorite) both before and after sampling.
2. Wear latex gloves on both hands.
79
3. Use Vacutainer collection equipment whenever feasible.
4. Never recap needles.
5. Used equipment should be discarded immediately after use.
6. Discard syringes and needles as a unit; never carry used sharps.
7. Sharps disposal containers should be available at the lab.
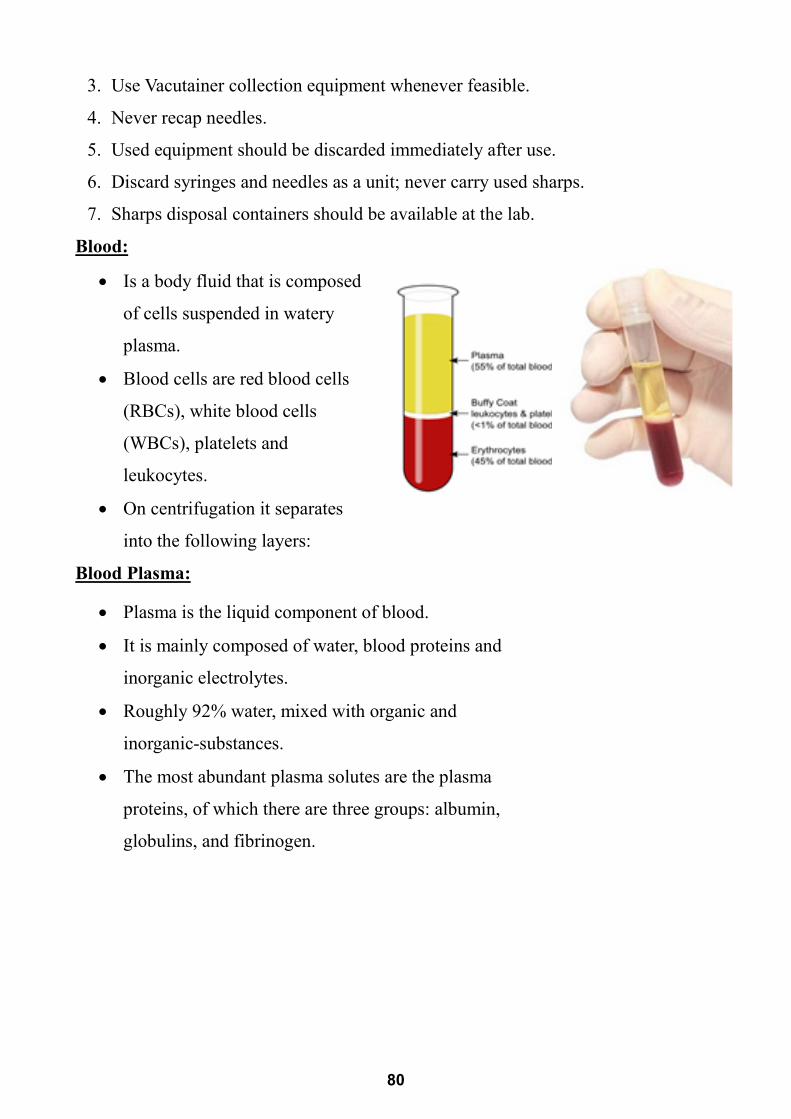
Blood:
• Is a body fluid that is composed
of cells suspended in watery
plasma.
• Blood cells are red blood cells
(RBCs), white blood cells
(WBCs), platelets and
leukocytes.
• On centrifugation it separates
into the following layers:
Blood Plasma:
• Plasma is the liquid component of blood.
• It is mainly composed of water, blood proteins and
inorganic electrolytes.
• Roughly 92% water, mixed with organic and
inorganic-substances.
• The most abundant plasma solutes are the plasma
proteins, of which there are three groups: albumin,
globulins, and fibrinogen.
80
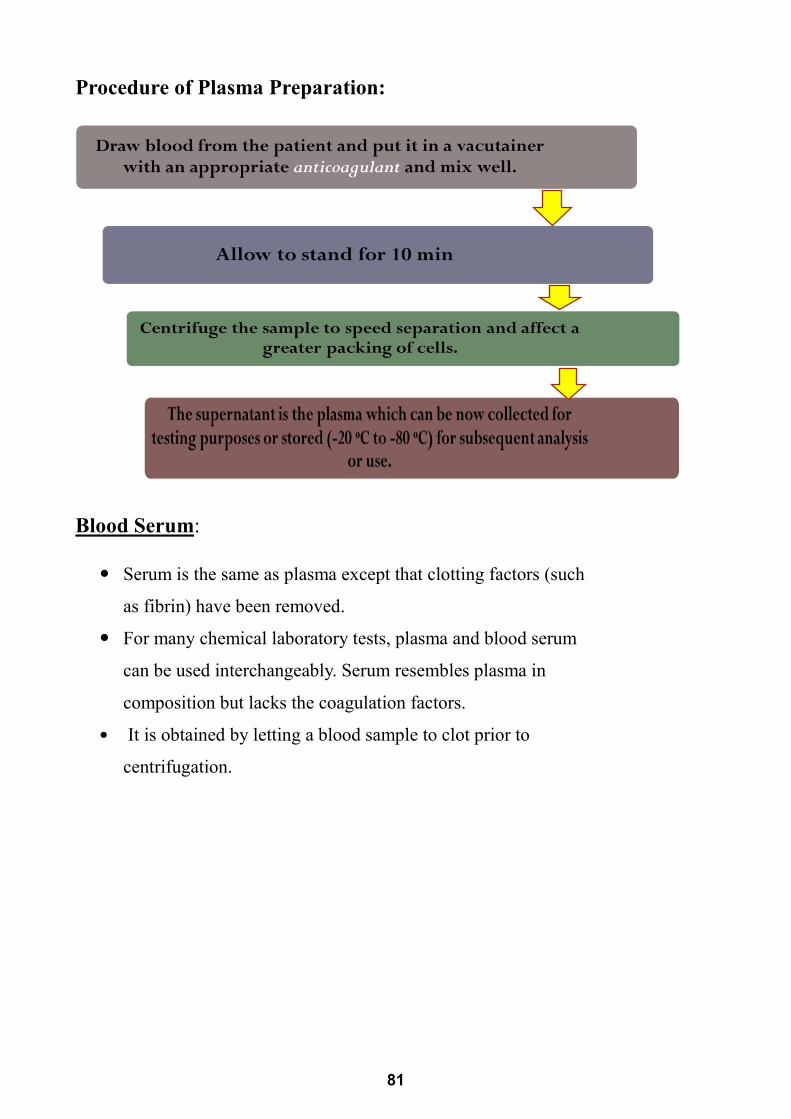
Procedure of Plasma Preparation:
Blood Serum:
Serum is the same as plasma except that clotting factors (such
as fibrin) have been removed.
For many chemical laboratory tests, plasma and blood serum
can be used interchangeably. Serum resembles plasma in
composition but lacks the coagulation factors.
It is obtained by letting a blood sample to clot prior to
centrifugation.
81
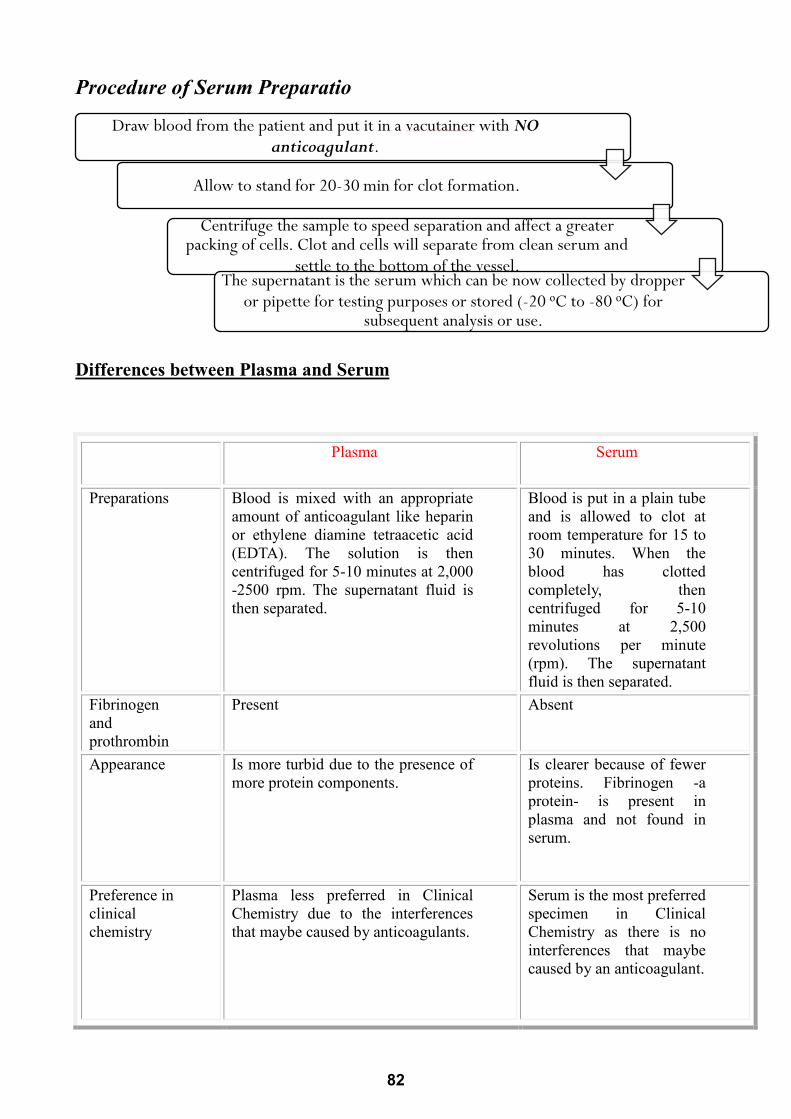
Procedure of Serum Preparatio
Differences between Plasma and Serum
Draw blood from the patient and put it in a vacutainer with NO anticoagulant.
Allow to stand for 20-30 min for clot formation.
Centrifuge the sample to speed separation and affect a greater packing of cells. Clot and cells will separate from clean serum and
settle to the bottom of the vessel. The supernatant is the serum which can be now collected by dropper
or pipette for testing purposes or stored (-20 ᵒC to -80 ᵒC) for subsequent analysis or use.
Serum Plasma Differences
Blood is put in a plain tube and is allowed to clot at room temperature for 15 to 30 minutes. When the blood has clotted completely, then centrifuged for 5-10 minutes at 2,500 revolutions per minute (rpm). The supernatant fluid is then separated.
Blood is mixed with an appropriate amount of anticoagulant like heparin or ethylene diamine tetraacetic acid (EDTA). The solution is then centrifuged for 5-10 minutes at 2,000 -2500 rpm. The supernatant fluid is then separated.
Preparations
Absent Present Fibrinogen and prothrombin
Is clearer because of fewer proteins. Fibrinogen -a protein- is present in plasma and not found in serum.
Is more turbid due to the presence of more protein components.
Appearance
Serum is the most preferred specimen in Clinical Chemistry as there is no interferences that maybe caused by an anticoagulant.
Plasma less preferred in Clinical Chemistry due to the interferences that maybe caused by anticoagulants.
Preference in clinical chemistry
82
Specimen rejection criteria: 1- Specimen improperly labeled or unlabeled.
2- Specimen improperly collected or preserved.
3- If separated plasma or serum is grossly hemolyzed.
Hemolysis of Blood:
It is liberation of hemoglobin from RBCs.
In this case plasma or serum will be pink or red
in color.
Hemolysis causes changes in measurement of a
number of analytes such as:
1- Serum K
2- Serum inorganic Phosphate.
3- SGOT
4- LDH
5- Acid phosphatase
Blood collection tubes =(Vacutainers): • The tubes are covered with a color-coded
plastic cap.
• They often include additives that mix with the blood when collected.
• The color of the tube's plastic cap indicates which additives
that tube contains.
• The tubes may contain additional substances that preserve the blood for
processing in clinical laboratory.
• Using the wrong tube may therefore make the blood unusable.
Red (Plain tube): It contains no additives and is used in tests for antibodies and drugs.
Plasma Separating Tubes:
83
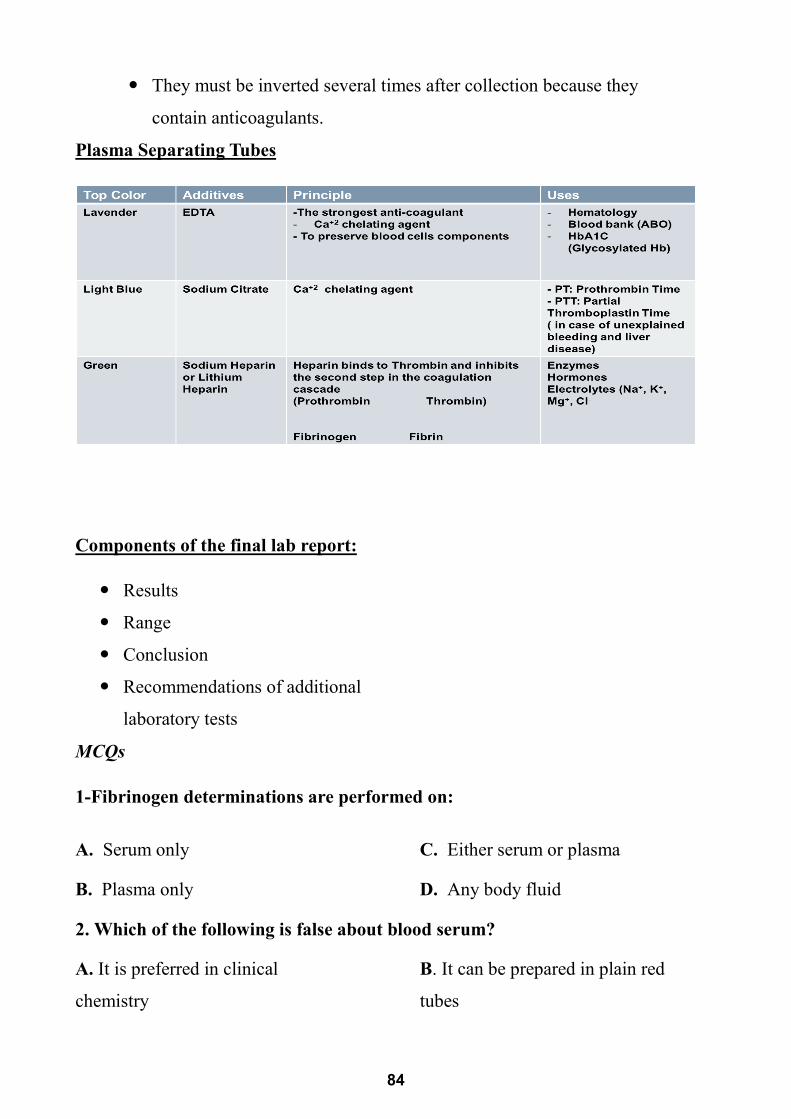
They must be inverted several times after collection because they
contain anticoagulants.
Plasma Separating Tubes
Components of the final lab report:
Results
Range
Conclusion
Recommendations of additional
laboratory tests
MCQs
1-Fibrinogen determinations are performed on:
A. Serum only
B. Plasma only
C. Either serum or plasma
D. Any body fluid
2. Which of the following is false about blood serum?
A. It is preferred in clinical
chemistry
B. It can be prepared in plain red
tubes
84
C. It contains coagulation factors D. It is more clear than plasma
3. Sodium citrate is found in what tube?
A. Gray
B. Pink
C. Green
D. Light blue
4. A clot activator that yields _______ in a green tube is called ________
A. Plasma, serum
B. Heparin (sodium or lithium),
serum
C. Serum, plasma
D. Plasma, heparin (sodium or
lithium)
5. An anticoagulant found in glucose-collecting tubes is called ________.
A. Sodium fluoride and potassium
oxalate
B. Sodium citrate and potassium
oxalate
C. Potassium oxalate and acid
citrate dextrose
D. Sodium fluoride
6. Lavender tubes contain what?
A. SPS
B. Hair
C. Heparin
D. Plasma
E. EDTA
7. What is the additive in light blue tubes?
A. Sodium cyanide
B. Sodium fluoride
C. Sodium chloride
D. Sodium citrate
8. A tube that is vitally important for coagulation tests is ______, contains
______, and yields ________.
A. Yellow, SPS, whole blood
B. Light blue, blood, EDTA
C. Orange, thrombin, serum
85
D. Light blue, sodium citrice,
serum
E. Light blue, sodium citrate,
serum
Activity 2
I. List points of similarity between serum and plasma
II. Most of the volume of normal human blood is composed of:
a) Red cells
b) Hemoglobin
c) plasma
d) white cells
Activity 3 A- 1- Identify the additive used in this vacutainer? …………………………………………………………… 2-This type of collection tube is used to separate
………………………………………………………… 3- Mention one use for this vacutainer ……………………………………………………………… B- A victim of a traffic accident was admitted to hospital with symptoms suspecting internal hemorrhage. The doctor was in hurry, he drawn a blood sample from the patient in EDTA containing tube without labeling it and he sent it immediately to lab for ABO grouping. According to the lab results, the blood was transfused to this victim, however it was incompatible. 1-Regarding this scenario, identify the error done during blood sampling
…………………………………………………………………………. 2-Enumerate two Specimen rejection criteria a)………………………………………………………………………. b)……………………………………………………………………….
86
Musculoskeletal Module II
Diabetic Profile
ILOs of the current topic
By the end of this topic, the student will be able to: 1. Explain the medical importance of determination of blood glucose
concentration.
2. Explain the principle of estimation of blood glucose concentration by
glucose oxidase reaction.
3. Perform the steps of the experiment with accurate pipetting of the volumes
required in the experiment
4. Interpret the resulting data whether it shows normoglycemic,
hyperglycemic or hypoglycemic results.
5. Correlate the results to possible medical problems causing such changes in
blood glucose level.
6. Perform oral glucose tolerance test.
7. Interpret the resulting data. Contents
Clinical case scenario Mona a 50 year old woman, weight 110 Kg suffered from Diabetes Mellitus
since15 years. She was on oral hypoglycemic medications, until two years ago her medication was changed to injectable insulin. On follow up the doctor
Diabetic profile Colorimeteric estimation of blood glucose
HbA1c
C –peptide Oral glucose tolerance test
Blood glucose meter
andLancing device
87
ordered fasting blood sugar, 2h postprandial sugar, renal function tests and HgA1C for her.
What is Diabetes mellitus? A group of metabolic disorders that is characterized by hyperglycemia and
abnormal protein, fat and carbohydrate metabolism due to defects in
insulin secretion, i.e., inadequate and deficient insulin action on target
tissues.
What are the classes of diabetes
Mellitus?
• Type I diabetes mellitus (TIDM)
• Type 2 diabetes mellitus (TIIDM)
• Gestational diabetes mellitus (GDM)
• Other specific types due to other
causes e.g. drugs or chemical induced.
What is Diabetic Profile?
Group of tests that are used to diagnose diabetes mellitus and to measure
response to treatment.
• Diabetic profile includes
Blood Glucose level Estimation:
• fasting blood glucose, post prandial, random blood glucose, OGTT
• HbA1c
• C-peptide and insulin levels
• ICA (Islet cell antibodies)
Blood Glucose Monitoring
GOAL: maintain blood glucose within normal range
IMMEDIATE BENEFIT: identification and treatment
LONG-TERM BENEFIT: decrease risk of long-term complication and
maximize health
CHALLENGE: many variables impact blood glucose
88
The diagnostic criteria of diabetes
Fasting blood glucose (FBG)
• Normal fasting glucose ……. …………<100 mg/dl • Impaired fasting glucose (IFG) ………... 100–125 mg/dl • Provisional diagnosis of diabetes …….. ≥126 mg/dl
Two hours after a 75 gm glucose (Postprandial) blood glucose (2hpp)
• Normal 2-hours postprandial glucose ……...<140 mg/dl • Impaired glucose tolerance (IGT)…..……….140–199 mg/dl • Provisional diagnosis of diabetes …………...≥200 mg/dl
Determination of plasma glucose concentration by Enzymatic method by glucose oxidase reaction
Medical importance of blood glucose
determination
1- Blood glucose monitoring is particularly
important in the diagnosis and care of diabetes
mellitus. Most people with Type 2 diabetes test at
least once per day. Diabetics who use insulin (all Type 1 diabetes and many
Type 2).
2- Blood glucose testing allows for quick response to high blood sugar
(hyperglycemia) or low blood sugar (hypoglycemia).
Principle of the glucose oxidase reaction
• Glucose is oxidized by glucose oxidase enzyme in a suitable pH
(phosphate buffer) at Carbon 1 to form gluconic acid with liberation of
hydrogen peroxide.
Glucose + O2 + H
2O
glucose oxidase
Gluconic acid + H2O
2
89
• Hydrogen peroxide is dissociated to water and oxygen atom by peroxidase
enzyme.
• The liberated oxygen is captured by a chromogen (A mixture of 4-amino antipyrine & phenol) which is converted to a red violet complex).
H2O
2 + Phenol + 4-amino antipyrine
peroxidase
Red colored
Materials required
• Pipettes & test tubes.
• Reagents
• Known glucose solution (Standard)
Pipetting station check list Mark
1 Wearing lab coat 1
2 Handling pipette correctly 1
3 Dipping pipette in solution correctly 1
4 Aspirate proper volume from a solution
1. Hold the pipette vertically; depress the plunger button to the first stop (A).
2. Place the tip just under the surface of the liquid (see Table 2) 3. Smoothly release the plunger button (B) keeping the tip at a
constant depth. 4. Carefully withdraw the tip from the liquid, touching against
the edge of the container to remove excess
1
5 Dispense the proper volume in a test tube
1. To dispense the liquid, hold the tip at an angle of around 30-45º against the wall of the receiving container. Depress the plunger button to the first stop (C) and hold for one second.
2. Push the pipette to the second stop (D) while sliding the pipette tip against the walls of the container.
1
90
• Unknown glucose solution
• Distilled water
Remember that pipetting is very important
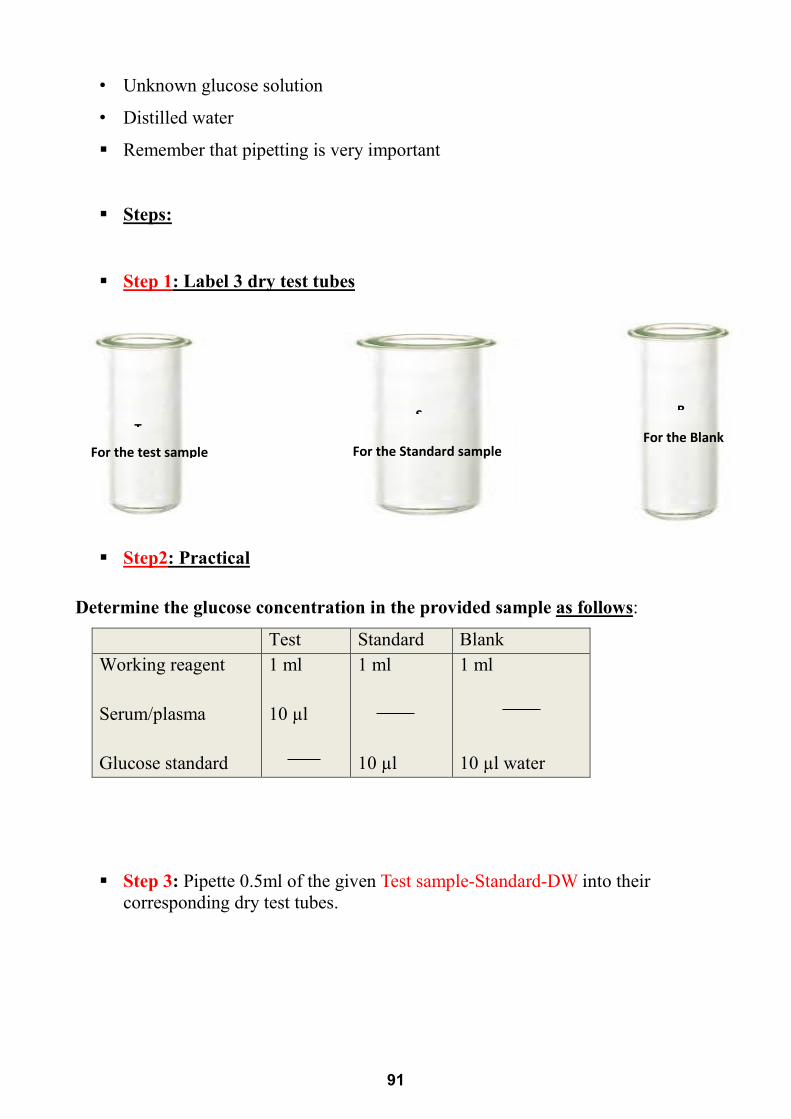
Steps:
Step 1: Label 3 dry test tubes
Step2: Practical
Determine the glucose concentration in the provided sample as follows:
Test Standard Blank Working reagent Serum/plasma Glucose standard
1 ml 10 µl
1 ml 10 µl
1 ml 10 µl water
Step 3: Pipette 0.5ml of the given Test sample-Standard-DW into their corresponding dry test tubes.
S
For the Standard sample
B
For the Blank
T For the test sample
91
Step 4: for all; Pipette 1ml of the glucose reagent into the previous 3 testtubes.
Step 5: Mix the contents of the tubes and let stand for 5 minutes at roomtemperature
Step 6: Record the absorbance of both test & standard against the blank at520 nm.
Practice the proper way to use the spectrophotometer:
1- The instrument must be warmed for at least 15 min. prior to use.
2- Use the wavelength knob to set the desired wavelength (540nm).
3- Pour the reference solution (blank) into the cuvette. Wipe the cuvette with a lab wipe. Place the cuvette into the sample holder and close the cover.
92
4- Set the zero absorbance. 5- Remove the blank cuvette then repeat step 8 with sample solution. 6- Read and record the absorbance.
Practice the proper way to use the spectrophotometer
Checklist of Activity
USING PHOTOMETER: MARK SCHEME MARK
1 PUT BLANK CUVETTE PROPERLY IN LIGHT PATH &CLOSE THE COVER 1
3 ADJUST PHOTOMETER ABSORBANCE ONTO ZERO 1
4 REMOVE THE BLANK AND PUT THE TEST CUVETTE 1
5 CLOSE THE COVER AND TAKE THE READING 1
Calculate the test concentration by the following equation
Concentration of blood glucose (mg/dl) = Absorbance of test / Absorbance of standard X ConC of standard
Materials required
A photometer, samples to be tested, blank, wipes and cuvette.
Steps 1. The instrument must be warmed for at least 15 min. prior to use.2. Use the wavelength knob to set the desired wavelength.3. Pour the reference solution (blank) into the cuvette. Wipe the
cuvette with a lab wipe. Place the cuvette into the sample holderand close the cover.
4. Set the zero absorbance.5. Remove the blank cuvette then repeat step 4 with sample solution.6. Read and record the absorbance.
Reference solution (blank) is identical to the colored sample in everything except that the compound of interest is eliminated from the solvent to concentrate on the measured compound.
Outcome is to:
Know how to use the photometer.
93
Normal values:
fasting sample: up to 100 mg/dl
2 hours postprandial: less than 140 mg/dl
Causes of hyperglycemia: 1-Diabetes Mellitus: Type 1 & type 2.
2- High epinephrine: severe emotional stress, pheochromocytoma.
3- A rare glucagon secreting tumor.
4- High cortisol: Cushing syndrome or high ACTH.
5- Intestinal glucosuria.
6- Gestational diabetes.
Causes of hypoglycemia: 1-Neonatal hypoglycemia: in RDS and pre-eclampsia.
2-Infantile hypoglycemia:
a) Glycogen storage diseases in liver.
b) Impaired gluconeogenesis. (deficiency of glucose 6 phosphatase or fructose
1,6 bisphosphatase).
c) fructose induced hypoglycemia
(deficiency of aldolase B).
d) Sever classic galactosemia
e) Deficient fatty acid oxidation (Carnitine deficiency)
3- Adult hypoglycemia: a) Over dose of insulin or oral hypoglycemic drugs.
b) Insulinoma.
c) Hypofunction of suprarenal cortex.
d) Chronic alcoholism.
e) Post prandial hypoglycemia due to sever over shooting of insulin.
HbA1c(Glycosylated hemoglobin) • It indicates how well diabetes has been controlled the 2 to 3 months before
the test.
94
• Normal Value: 4.5% - 5.7%
C-peptide level
• It differentiates between type I and II diabetes.
• A person whose pancreas does not make any insulin (type 1 diabetes) has
a low level of insulin and C-peptide.
• A person with type 2 diabetes has a normal level of C-peptide.
• Fasting normal value: 0.51- 2.72 ng/ml
Oral Glucose Tolerance Test (OGTT)
It is a medical test in which glucose is given orally and blood samples are taken
afterward to determine how quickly it is cleared from the blood.
Indications of oral GTT:
1) Diagnosis of impaired glucose tolerance (borderline cases of diabetes
mellitus).
2) Diagnosis of high risk cases to get diabetes
e.g during pregnancy (gestational diabetes).
3) Diagnosis of causes of glucosuria e.g alimentary (intestinal) & renal
glucosuria.
Precautions for OGTT: AVOID:
o Eating from midnight o Carbohydrates restriction o Severe exercise o Drinking coffee o Smoking
How the OGTT is done
1- Begin in the morning (at 7-8 AM).
2- The subject sits quietly throughout the test.
3- A fasting blood sample (time 0) is drawn.
4 -fasting urine sample is collected.
95
5-75 g anhydrous glucose is dissolved
in 250-300 ml water and is ingested
orally within 5 min.
6- Blood is drawn at intervals of 30 min
for measurement of glucose
7- Urine samples also collected (to test for glucose) every 30 min. 8- For diagnosis of gestational diabetes the test is extended for 3 hours How are the results of the glucose tolerance test evaluated?
Glucose tolerance tests may lead to one of the following diagnoses:
• Normal response: A person is said to have a normal response when the two hour glucose level is less than 140 mg/dl, and all values between 0 and 2 hours are less than 200 mg/dl. • Impaired glucose tolerance
(IGT): A person is said to have impaired glucose tolerance when the fasting plasma glucose is less than 126 mg/dl and the two hour glucose level is between 140 and 199 mg/dl. This is sometimes referred to as "prediabetes" because people with IGT have a higher risk of developing diabetes.
• Diabetes: A person has diabetes when two diagnostic tests done on different days show that the blood glucose level is high. This means either the two hour levels is greater than 200 mg/dl or the fasting glucose is noted as greater than
96
126 mg/dl. A glycosylated hemoglobin (HbA1c) level of 6.5% or more also supports a diagnosis of diabetes mellitus.
Special OGTT Results • Flat response • Gestational diabetes • Alimentary Glucosuria • Renal Glucosuria
Renal glucosuria, Renal
glucosuria is the excretion of glucose in the urine in detectable amounts at normal blood glucose concentrations.
The revised criteria for diagnosis of renal glucosuria includes: a normal oral glucose tolerance test in regard to plasma glucose concentration, normal plasma levels of insulin, glycosylated hemoglobin, with glucose present in all urine samples.
Causes:
1. Genetically inherited low renal threshold
2. Late pregnancy
3. Tubular reabsorption defect e.g. Fanconi syndrome
Alimentary (intestinal) glucosuria: a temporary condition, when a high amount of carbohydrate is taken, it is rapidly absorbed in some cases where a part of the stomach surgically removed, is the excessive glucose appears in urine producing glucosuria.
A sharp rise in plasma
glucose with early peak
values exceeding the renal
threshold and associated
with glucosuria.
97
The 2-hours post prandial level is much below the fasting level.
This is due to rapid glucose absorption followed by a burst of insulin
production which over-compensate, resulting in hypoglycemia.
Causes:
• Some healthy individuals.
• Gastrectomy.
• Hyperthyroidism.
Flat response in OGTT
Plasma glucose levels fail to rise
significantly after an oral glucose load.
Causes:
Insulinomia: over production of
insulin.
Intestinal malabsorption syndrome.
Some hormonal deficiencies e.g.
Hypopituitarism, hypothyroidism (myxedema)
Gestational diabetes
Any degree of glucose intolerance with onset or first recognition
during pregnancy
The preferred diagnostic test is the 100 gram 3 hour OGTT.
If two or more values are above the criteria, gestational diabetes is diagnosed
Blood Glucose Meter and lancing device
98
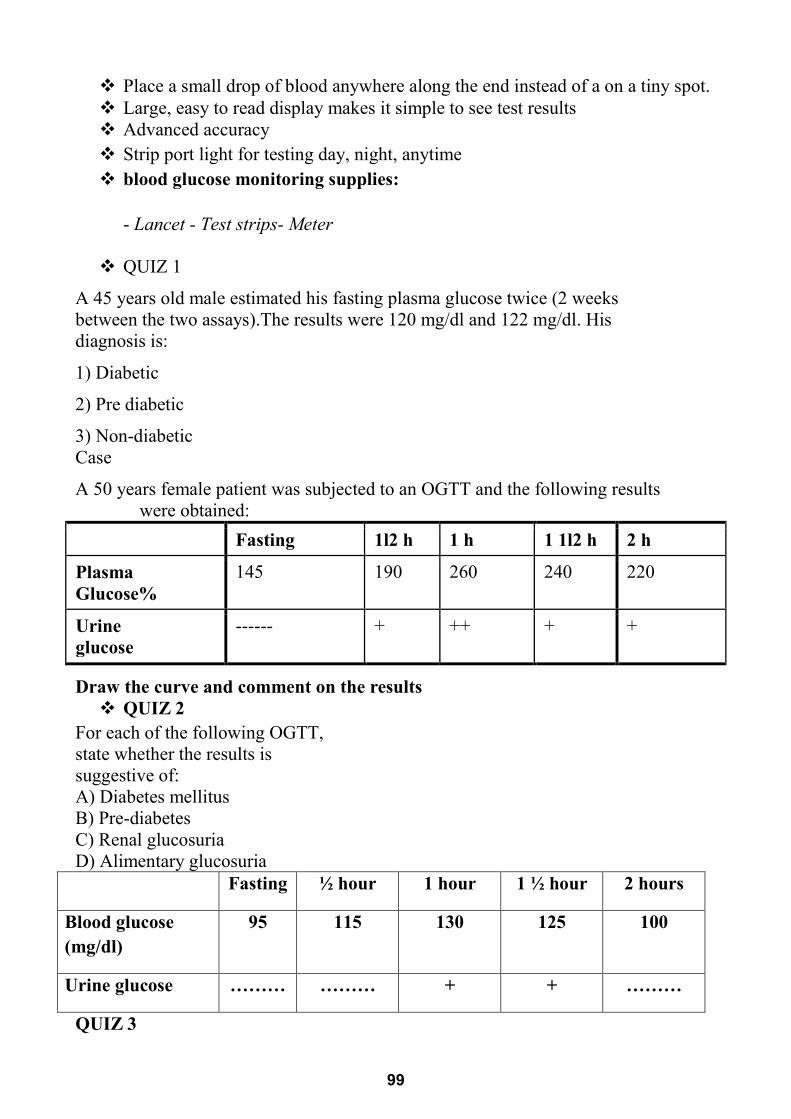
Place a small drop of blood anywhere along the end instead of a on a tiny spot. Large, easy to read display makes it simple to see test results Advanced accuracy Strip port light for testing day, night, anytime blood glucose monitoring supplies:
- Lancet - Test strips- Meter
QUIZ 1
A 45 years old male estimated his fasting plasma glucose twice (2 weeks between the two assays).The results were 120 mg/dl and 122 mg/dl. His diagnosis is:
1) Diabetic
2) Pre diabetic
3) Non-diabetic Case
A 50 years female patient was subjected to an OGTT and the following results were obtained:
2 h 1 1l2 h 1 h 1l2 h Fasting
220 240 260 190 145 Plasma Glucose%
+ + ++ + ------ Urine glucose
Draw the curve and comment on the results QUIZ 2
For each of the following OGTT, state whether the results is suggestive of: A) Diabetes mellitus B) Pre-diabetes C) Renal glucosuria D) Alimentary glucosuria
Fasting ½ hour 1 hour 1 ½ hour 2 hours
Blood glucose (mg/dl)
95 115 130 125 100
Urine glucose ……… ……… + + ………
QUIZ 3
99
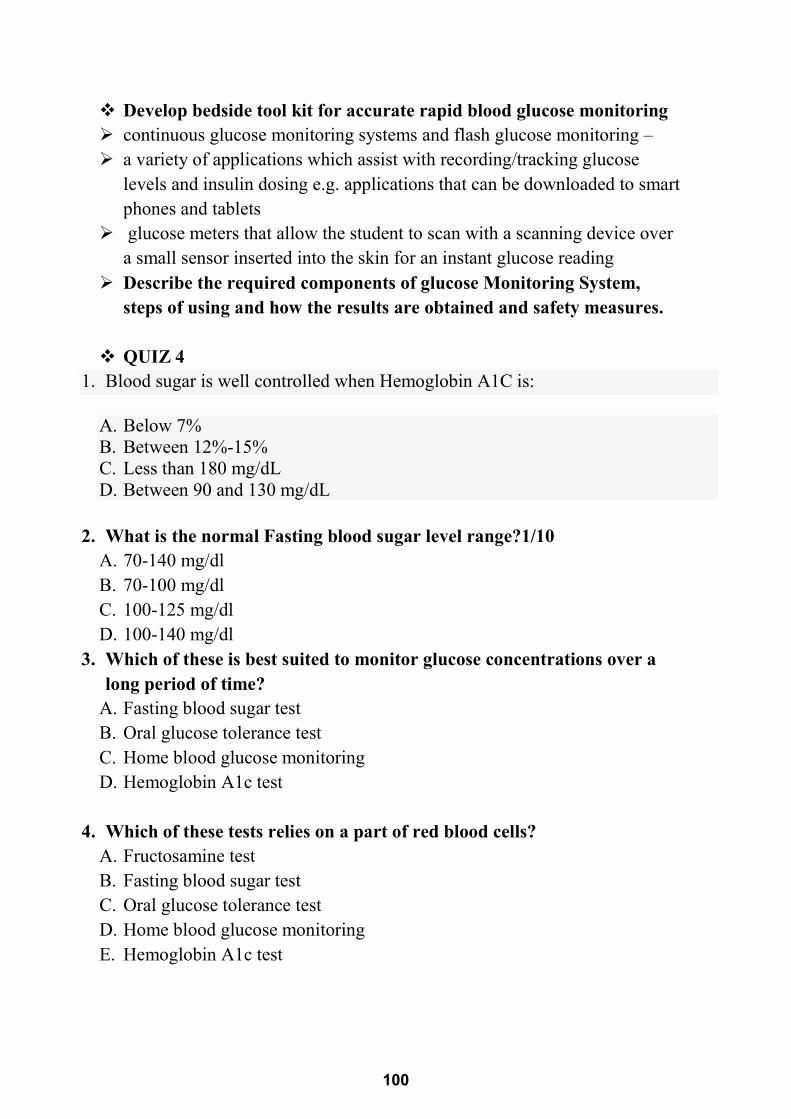
Develop bedside tool kit for accurate rapid blood glucose monitoring continuous glucose monitoring systems and flash glucose monitoring – a variety of applications which assist with recording/tracking glucose
levels and insulin dosing e.g. applications that can be downloaded to smart phones and tablets
glucose meters that allow the student to scan with a scanning device over a small sensor inserted into the skin for an instant glucose reading
Describe the required components of glucose Monitoring System, steps of using and how the results are obtained and safety measures.
QUIZ 4
1. Blood sugar is well controlled when Hemoglobin A1C is:
A. Below 7% B. Between 12%-15% C. Less than 180 mg/dL D. Between 90 and 130 mg/dL
2. What is the normal Fasting blood sugar level range?1/10
A. 70-140 mg/dl B. 70-100 mg/dl C. 100-125 mg/dl D. 100-140 mg/dl
3. Which of these is best suited to monitor glucose concentrations over a long period of time?
A. Fasting blood sugar test B. Oral glucose tolerance test C. Home blood glucose monitoring D. Hemoglobin A1c test
4. Which of these tests relies on a part of red blood cells?
A. Fructosamine test B. Fasting blood sugar test C. Oral glucose tolerance test D. Home blood glucose monitoring E. Hemoglobin A1c test
100
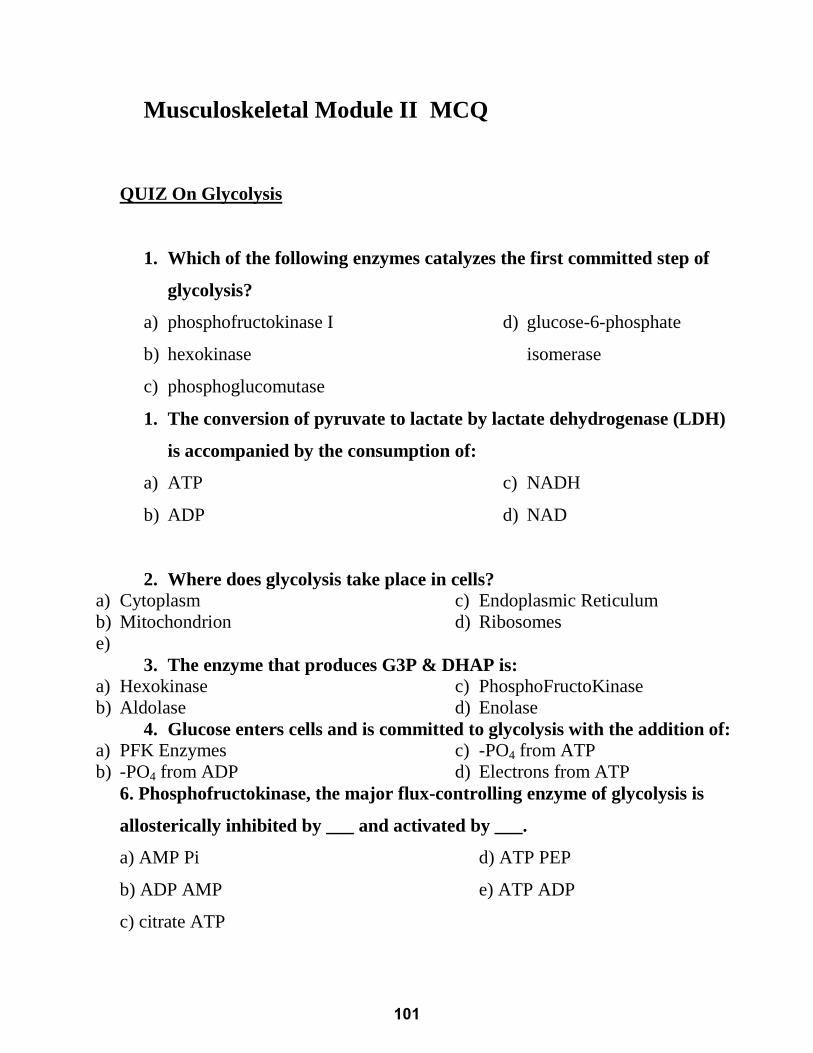
Musculoskeletal Module II MCQ
QUIZ On Glycolysis
1. Which of the following enzymes catalyzes the first committed step of
glycolysis?
a) phosphofructokinase I
b) hexokinase
c) phosphoglucomutase
d) glucose-6-phosphate
isomerase
1. The conversion of pyruvate to lactate by lactate dehydrogenase (LDH)
is accompanied by the consumption of:
a) ATP
b) ADP
c) NADH
d) NAD
2. Where does glycolysis take place in cells?
a) Cytoplasm
b) Mitochondrion
c) Endoplasmic Reticulum
d) Ribosomes
e) 3. The enzyme that produces G3P & DHAP is:
a) Hexokinase
b) Aldolase
c) PhosphoFructoKinase
d) Enolase
4. Glucose enters cells and is committed to glycolysis with the addition of:
a) PFK Enzymes
b) -PO4 from ADP
c) -PO4 from ATP
d) Electrons from ATP
6. Phosphofructokinase, the major flux-controlling enzyme of glycolysis is
allosterically inhibited by ___ and activated by ___.
a) AMP Pi
b) ADP AMP
c) citrate ATP
d) ATP PEP
e) ATP ADP
101
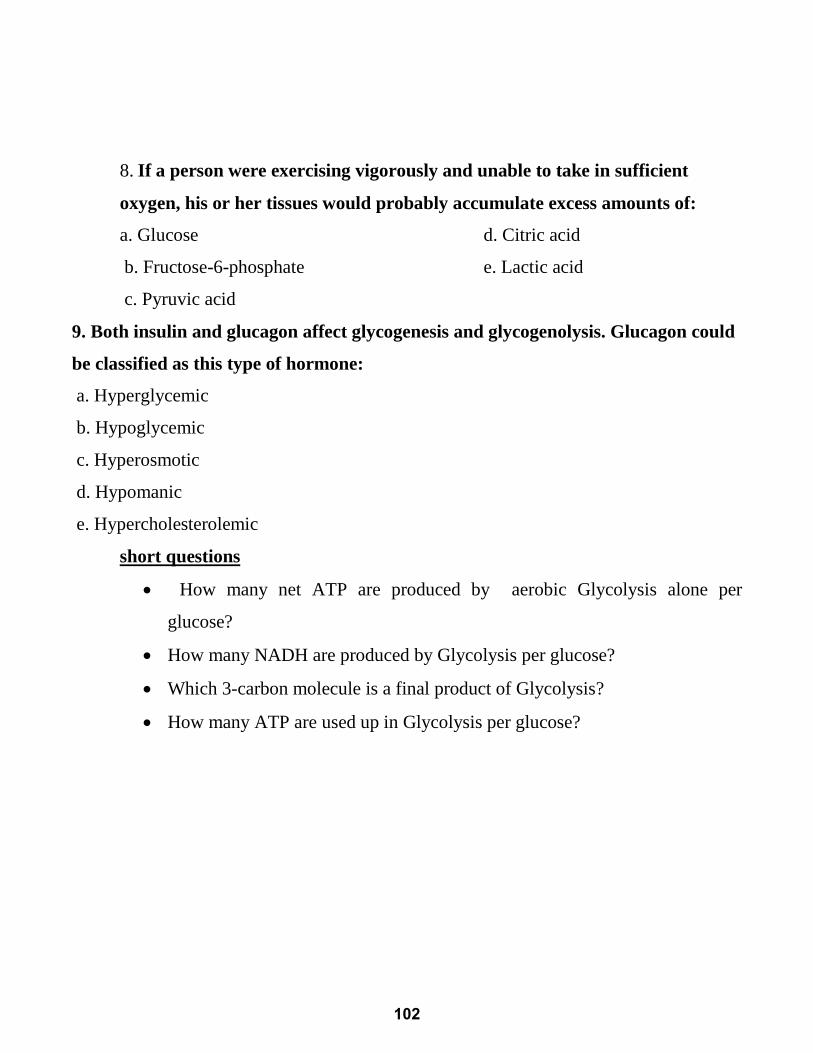
8. If a person were exercising vigorously and unable to take in sufficient
oxygen, his or her tissues would probably accumulate excess amounts of:
a. Glucose
b. Fructose-6-phosphate
c. Pyruvic acid
d. Citric acid
e. Lactic acid
9. Both insulin and glucagon affect glycogenesis and glycogenolysis. Glucagon could
be classified as this type of hormone:
a. Hyperglycemic
b. Hypoglycemic
c. Hyperosmotic
d. Hypomanic
e. Hypercholesterolemic
short questions
How many net ATP are produced by aerobic Glycolysis alone per
glucose?
How many NADH are produced by Glycolysis per glucose?
Which 3-carbon molecule is a final product of Glycolysis?
How many ATP are used up in Glycolysis per glucose?
102
Quiz on krebs cycle
1. In what part of the cell does TCA cycle take place?
A. Cytoplasm (cytosol)
B. Mitochondria
C. Ribosome
D. Nucleus
2. An anaplerotic reaction which sustains the availability of oxaloacetate is the
carboxylation of
A. Glutamate
B. Citrate
C. Pyruvate
D. Succinate
3. The number of ATP produced in the succinate dehydrogenase step is
A. 1
B. 2
C. 3
D. 4
4. Which of the following statements regarding TCA cycle is true?
A. It is an anaerobic process
B. It occurs in cytosol
C. It contains no intermediates for
Gluconeogenesis
D. It is amphibolic in nature
5. The FADH2 and NADH produced by the oxidation of one acetyl-CoA result in the
synthesis of about --- ATPs
A. 10
B. 11
C. 15
D. 20
6. The reaction succinyl COA to succinate requires
A. FAD
B. ATP
C. GDP
D. NADP
E. NAD
7. Pyruvate, the end product of glycolysis, enters the citric acid cycle after it has been
converted to
A. acetaldehyde.
B. lactic acid.
C. acetic acid.
D. acetyl-CoA.
8. The enzyme needed to catalyze Citrate into Isocitrate
A. Citrate synthase
B. Aconitase
C. Isocitrate dehydrogenase
D. Isocitrate synthase
103
9. These are formed during the cycle which carries electrons and hydrogen ions to the
Electron Transport Chain.
A. NAD+ and FAD
B. NADH and FADH
C. CO2 and H2O
D. GTP and CO2
QUIZ on Glycogen metabolism
1. Which of the following is important for glycogenesis
A. Glycogen phosphorylase
B. cAMP
C. Glucagons
D. glycogenin
E. Glycogen phosphorylase kinase
2. Von Gierk's disease is due to deficiency of:
A. Glycogen phosphorylase enzyme in
liver
B. Glycogen phosphorylase enzyme in
muscles
C. Glucose-6- phosphatase enzyme in
muscles
D. Glucose-6- phosphatase enzyme in live
QUIZ ON fatty acid oxidation
1. The enzymes of β-oxidation are found in
(A) Mitochondria
(B) Cytosol
(C)Golgi apparatus
(D)Nucleus
(E)Nucleolus
2. The acyl-CoA formed in the __ is transported to the __ for oxidation.
A. mitochondrial matrix, cytosol
B. mitochondrial matrix, inner-membrane
C. cytosol, mitochondrial matrix
D. endoplasmic reticulum, cytosol
E. microsomes, mitochondrial matrix
3. Each cycle of b oxidation produces
A. 1 FAD, 1 NADH, and 1 acetyl-CoA.
B. 1 FADH2, 1 NADH, and 1 acetyl-CoA.
C. 1 FAD, 1 NAD+, and 2 CO2 molecules.
D. 1 FADH2, 1 NADH, and 2 CO2
molecules.
E. 1 FADH2, 1 NAD+, and 1 acetyl-CoA.
104
4. Oxidation of palmitic acid (C16) involves __ rounds of oxidation and produces __ molecules of
acetyl-CoA.
A. 8, 8
B. 7, 8
C. 16, 8
D. 7, 7
E. 16, 7
105
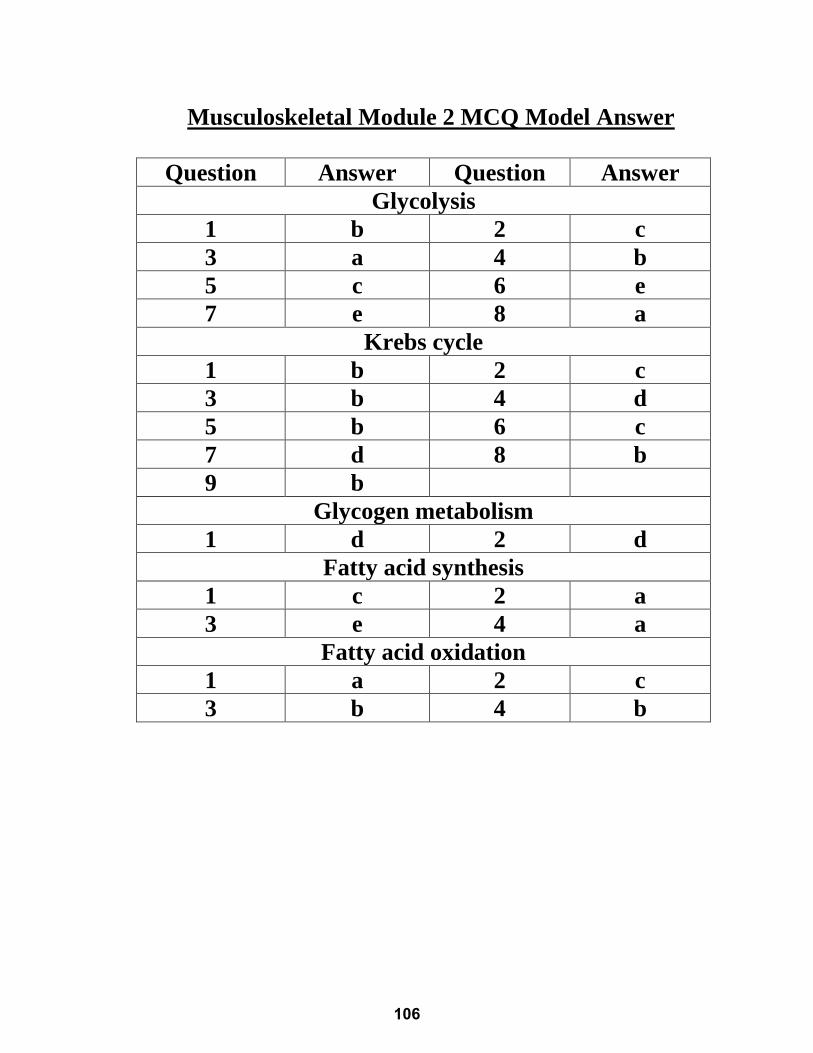
Musculoskeletal Module 2 MCQ Model Answer
Question Answer Question Answer
Glycolysis
1 b 2 c
3 a 4 b
5 c 6 e
7 e 8 a
Krebs cycle
1 b 2 c
3 b 4 d
5 b 6 c
7 d 8 b
9 b
Glycogen metabolism
1 d 2 d
Fatty acid synthesis
1 c 2 a
3 e 4 a
Fatty acid oxidation
1 a 2 c
3 b 4 b
106
STUDENT NAME:…………………………………………………………………………………..
STUDENT NUMBER: ……………………………………………………………………………..
STUDENT SECTION: ……………………………………………………………………………..
TOTAL MARK:
HEAD OF BIOCHEMISTRY DEPARTMENT
Ass. Prof .Dr. Marwa Matboli
DATE SECTION TOPIC
TIME Grade SIGNATURE
introduction to clinical chemistry Colorimetric estimation of blood glucose and diabetic profile
SGD1
SGD 2
SGD3
107

References:
Carl A. Burtis, Edward R. Ashwood and David E. Bruns (2007). Tietz
Fundamentals of Clinical Chemistry, 6th edition.
http://www.namrata.co/category/practi cal-biochemistry/normal-urine-
Jan Koolman and Klaus-Heinrich Roehm (2005). Color Atlas of
Biochemistry, 2nd edition, Thieme.
Robert, K. Murray, Daryl, K. Granner, Peter A. Mayes and Victor W.
Rodwell (2003). Harper’s illustrated biochemistry, 26th edition, McGraw-Hill.
Tietz-fundamentals-of-clinical-chemistry.
108
Pathology
BY
PROF. DR. HALA KHEIDR
Musculoskeletal II moduleMUS II 215
PROFESSOR & HEAD OF PATHOLOGY DEPARTMENTFACULTY OF MEDICINE - MTI
PROFESSOR OF PATHOLOGYFACULTY OF MEDICINE - CAIRO UNIVERSITY
109

110
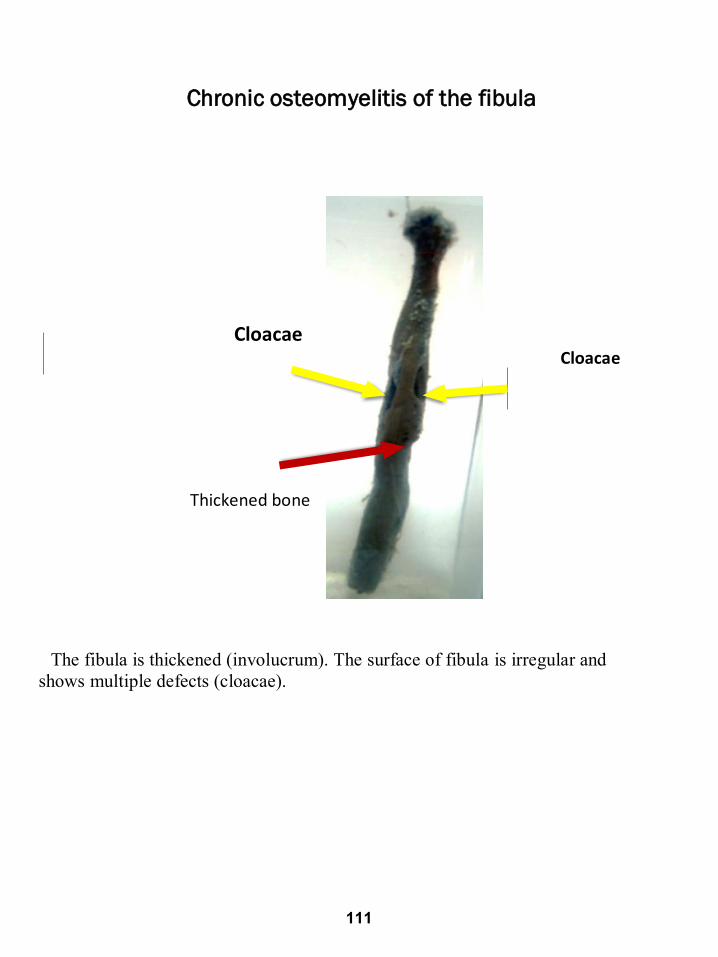
Chronic osteomyelitis of the fibula
Cloacae Cloacae
Thickened bone
The fibula is thickened (involucrum). The surface of fibula is irregular and
shows multiple defects (cloacae).
111
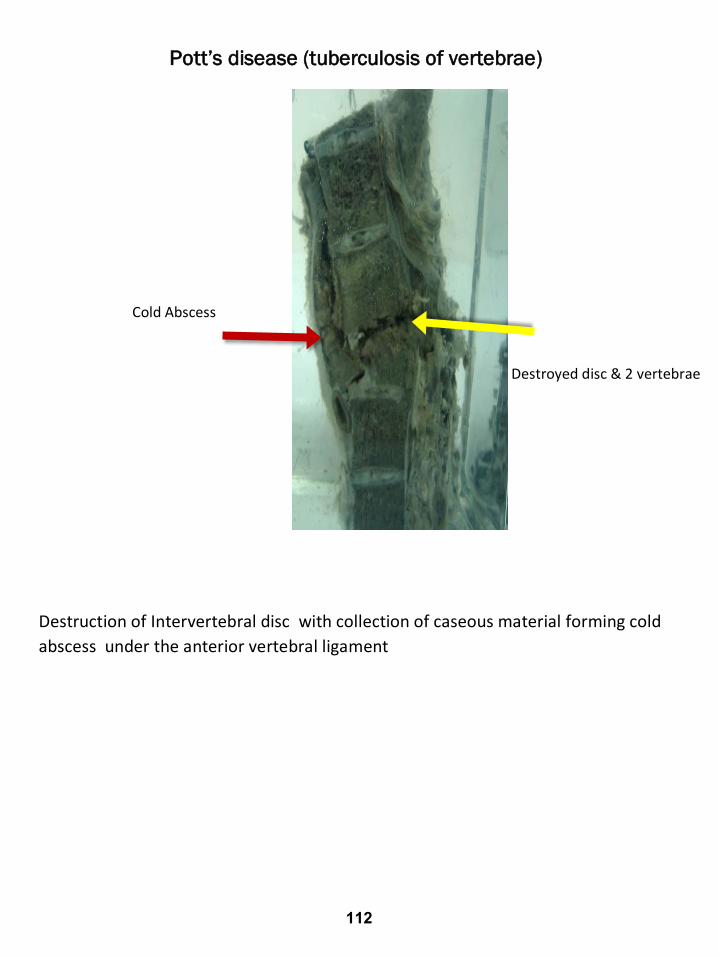
Pott’s disease (tuberculosis of vertebrae)
Cold Abscess
Destroyed disc & 2 vertebrae
Destruction of Intervertebral disc with collection of caseous material forming cold
abscess under the anterior vertebral ligament
112
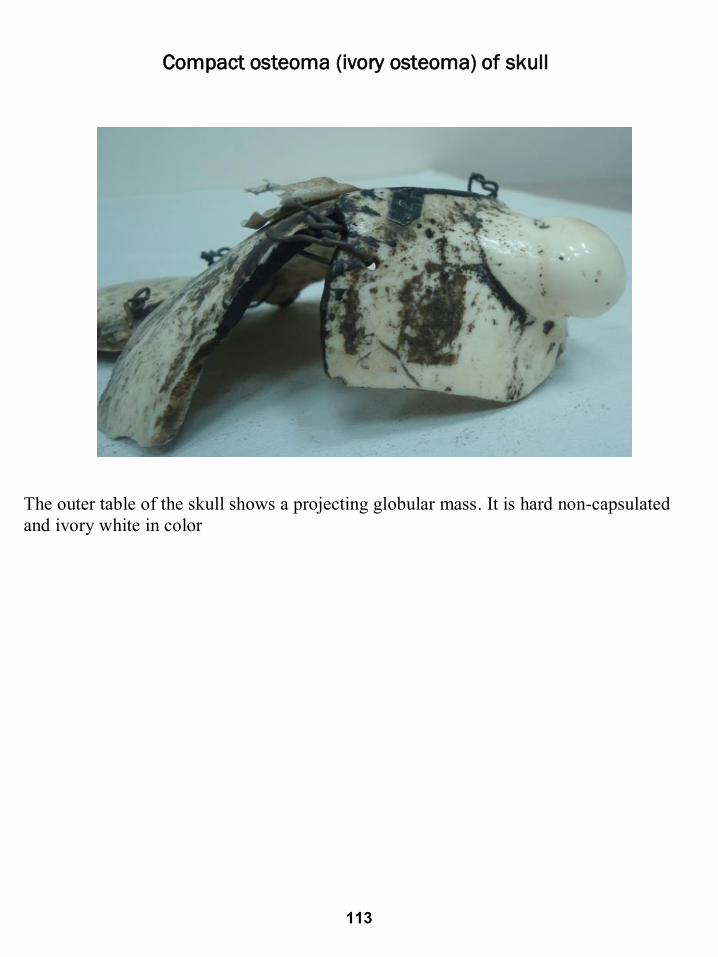
Compact osteoma (ivory osteoma) of skull
The outer table of the skull shows a projecting globular mass. It is hard non-capsulated
and ivory white in color
113
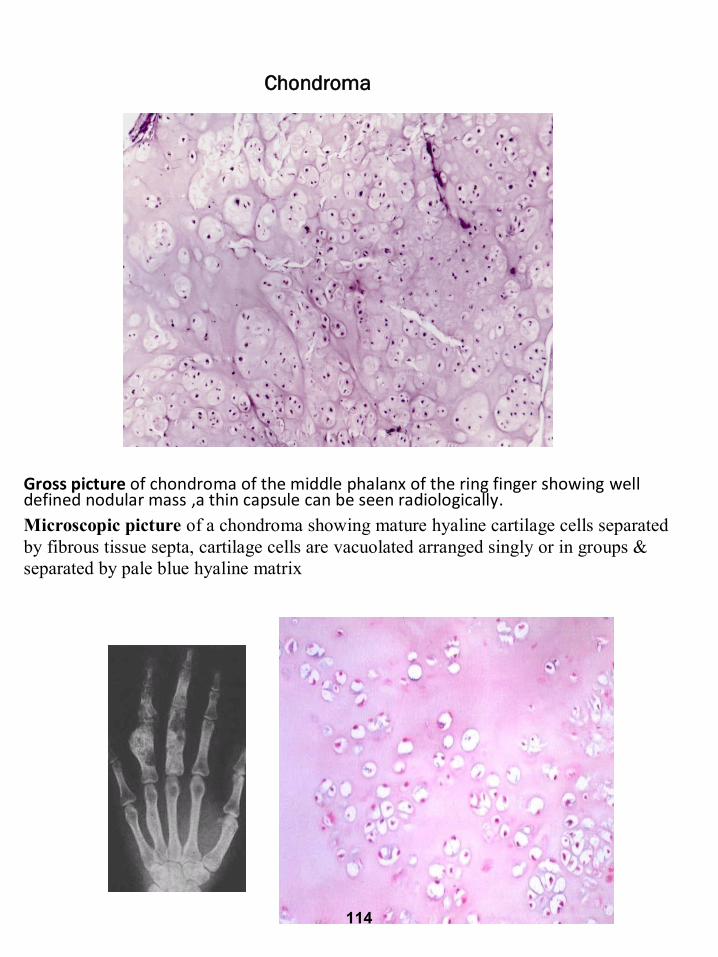
Chondroma
Gross picture of chondroma of the middle phalanx of the ring finger showing well defined nodular mass ,a thin capsule can be seen radiologically.
Microscopic picture of a chondroma showing mature hyaline cartilage cells separated
by fibrous tissue septa, cartilage cells are vacuolated arranged singly or in groups &
separated by pale blue hyaline matrix
114
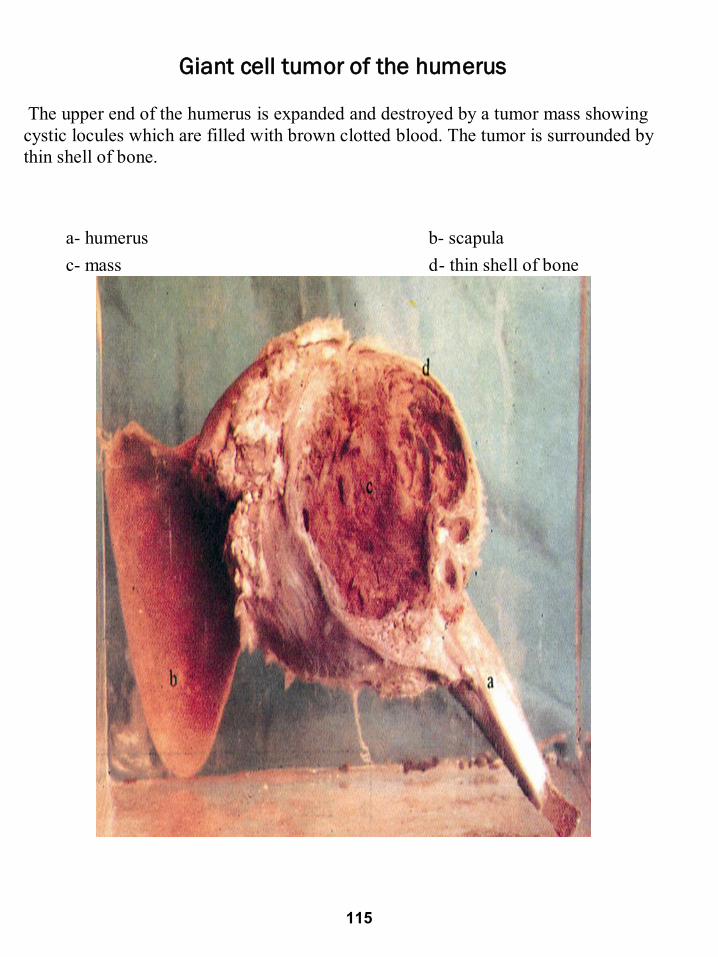
Giant cell tumor of the humerus
The upper end of the humerus is expanded and destroyed by a tumor mass showing
cystic locules which are filled with brown clotted blood. The tumor is surrounded by
thin shell of bone.
a- humerus b- scapula
c- mass d- thin shell of bone
115
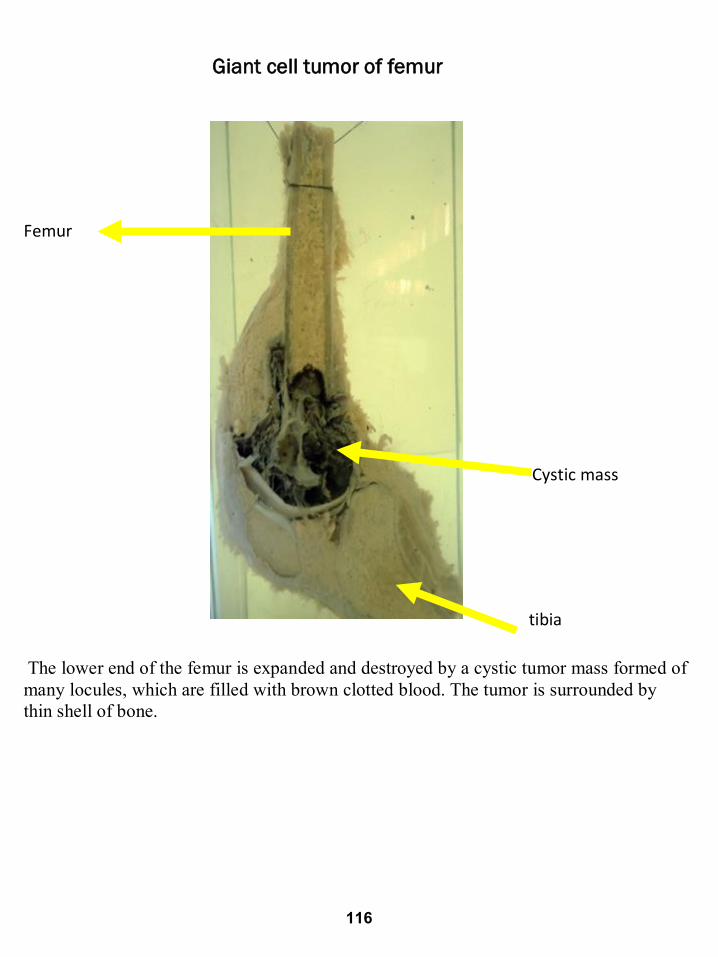
Giant cell tumor of femur
Femur
Cystic mass
tibia
The lower end of the femur is expanded and destroyed by a cystic tumor mass formed of
many locules, which are filled with brown clotted blood. The tumor is surrounded by
thin shell of bone.
116
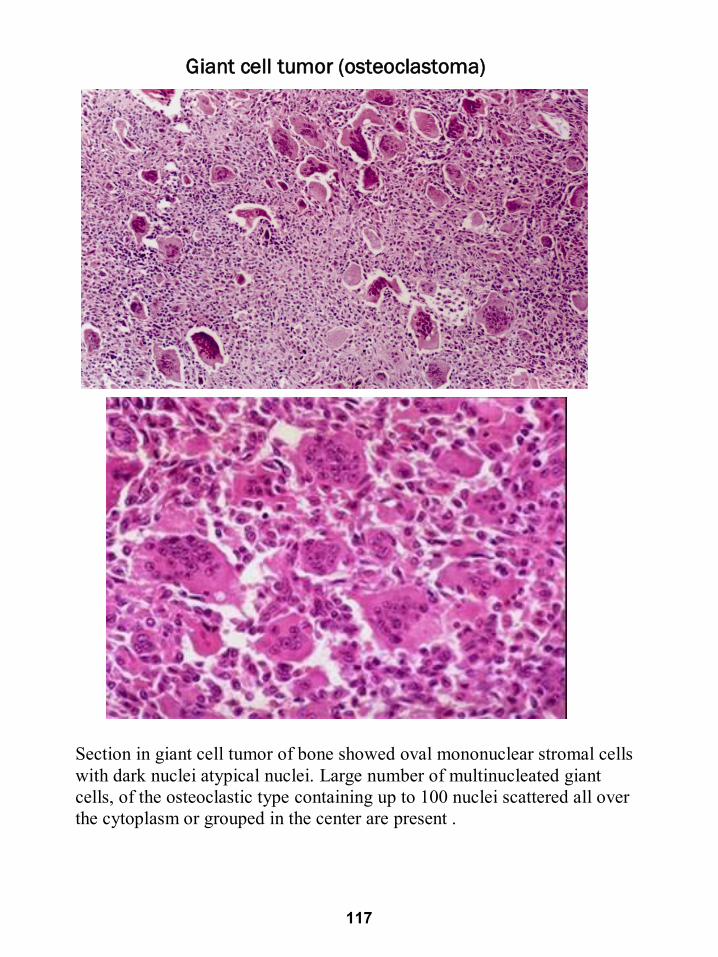
Giant cell tumor (osteoclastoma)
Section in giant cell tumor of bone showed oval mononuclear stromal cells
with dark nuclei atypical nuclei. Large number of multinucleated giant
cells, of the osteoclastic type containing up to 100 nuclei scattered all over
the cytoplasm or grouped in the center are present .
117
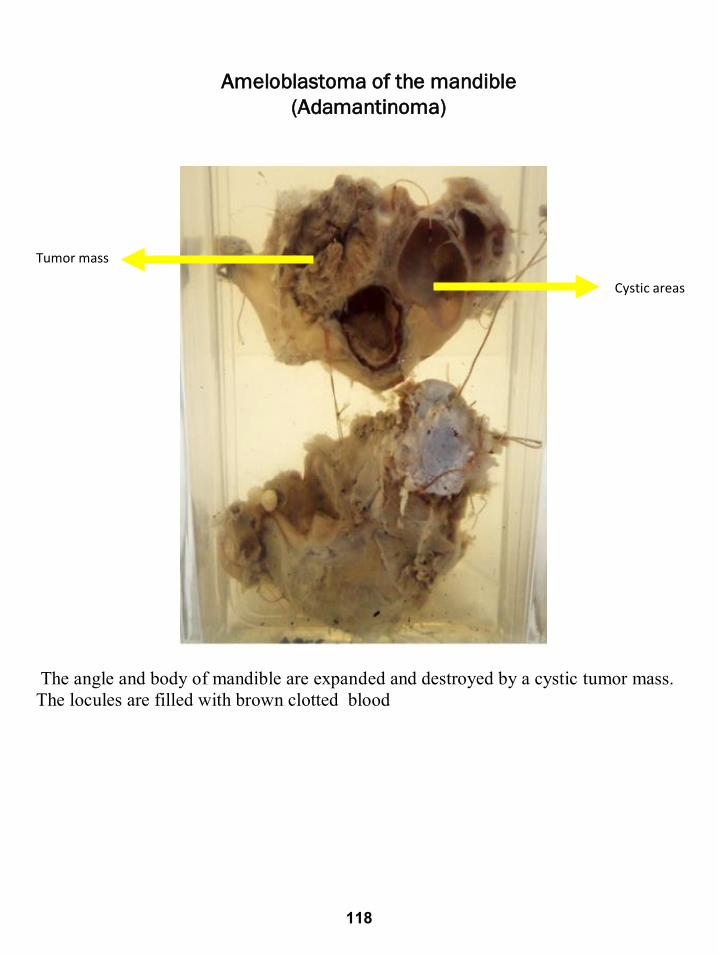
Ameloblastoma of the mandible
(Adamantinoma)
Tumor mass
Cystic areas
The angle and body of mandible are expanded and destroyed by a cystic tumor mass.
The locules are filled with brown clotted blood
118
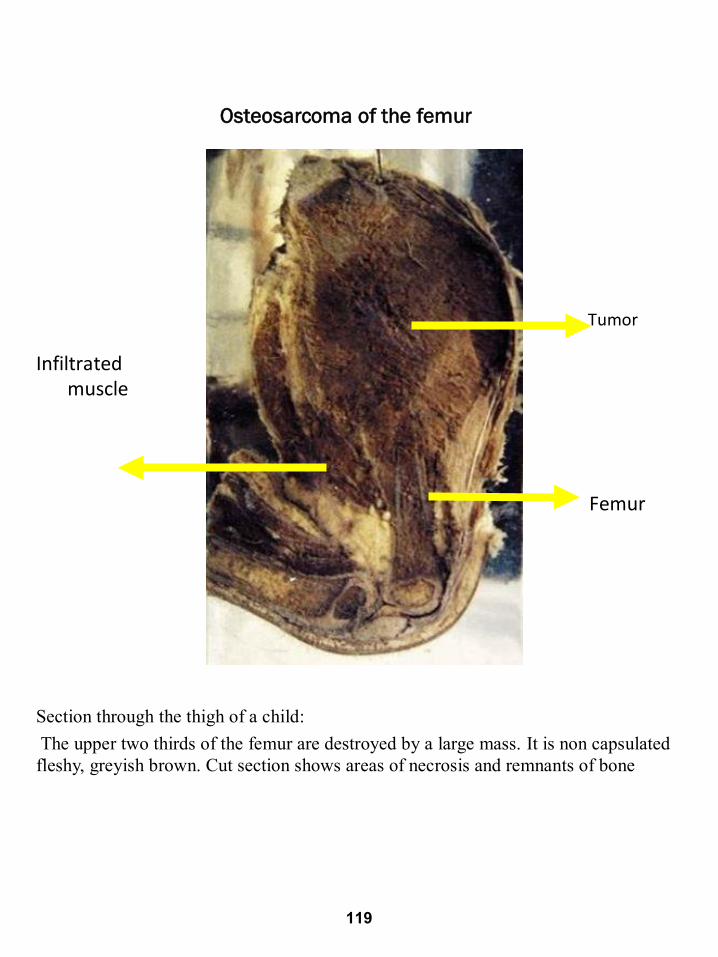
Osteosarcoma of the femur
Tumor
Infiltrated muscle
Femur
Section through the thigh of a child:
The upper two thirds of the femur are destroyed by a large mass. It is non capsulated
fleshy, greyish brown. Cut section shows areas of necrosis and remnants of bone
Femur
119
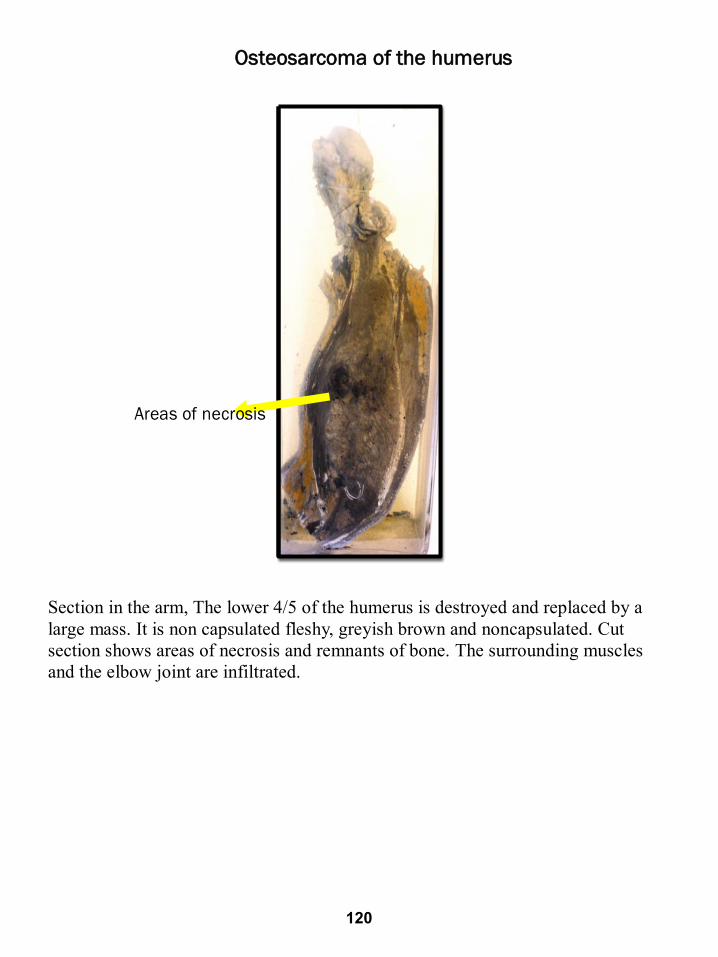
Osteosarcoma of the humerus
Areas of necrosis
Section in the arm, The lower 4/5 of the humerus is destroyed and replaced by a
large mass. It is non capsulated fleshy, greyish brown and noncapsulated. Cut
section shows areas of necrosis and remnants of bone. The surrounding muscles
and the elbow joint are infiltrated.
Arm
120
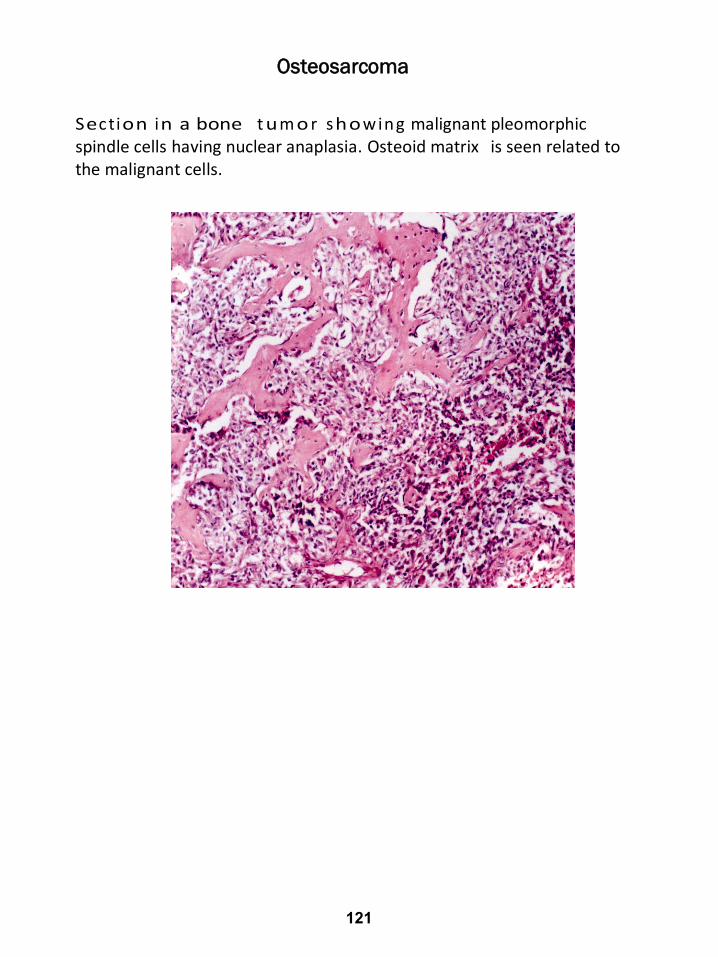
Osteosarcoma
Section in a bone t um o r showing malignant pleomorphic spindle cells having nuclear anaplasia. Osteoid matrix is seen related to the malignant cells.
121
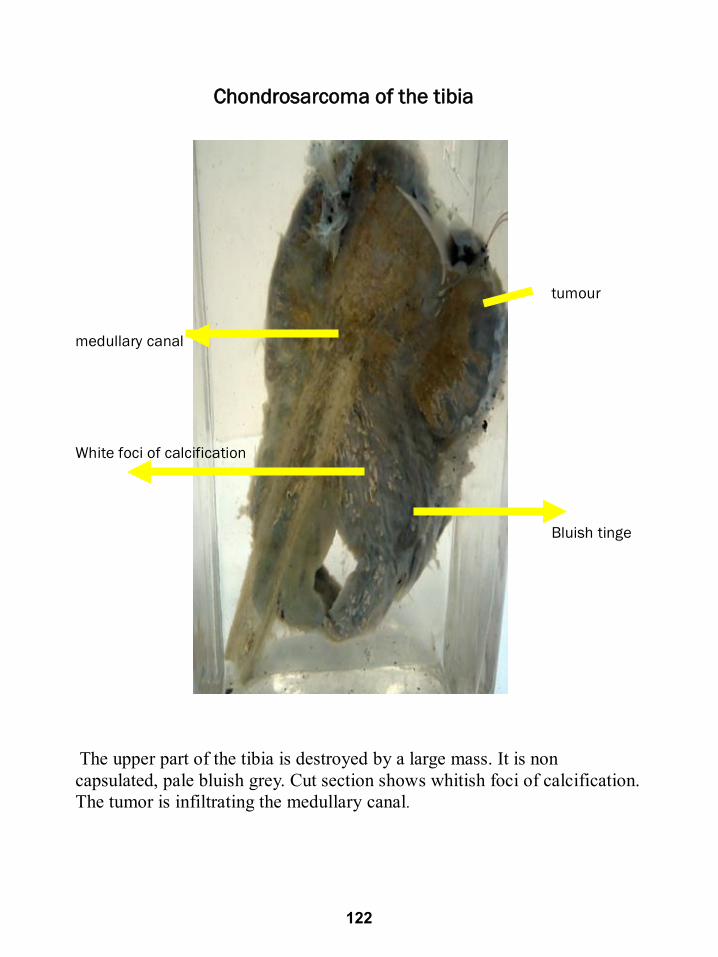
Chondrosarcoma of the tibia
tumour
medullary canal
White foci of calcification
Bluish tinge
The upper part of the tibia is destroyed by a large mass. It is non
capsulated, pale bluish grey. Cut section shows whitish foci of calcification.
The tumor is infiltrating the medullary canal.
122

Pharmacology
BY
PROF. DR. HISHAM ALSHEKHEPY
Musculoskeletal II moduleMUS II 215
PROFESSOR & HEAD OF PHARMACOLOGY DEPARTMENTFACULTY OF MEDICINE - MTI
PROFESSOR OF PHARMACOLOGYFACULTY OF MEDICINE - CAIRO UNIVERSITY
123

124
Treatment of Gout
Definition: Gout is a form of arthritis caused by excess uric acid in the
bloodstream. Increased uric acid in blood due to synthesis, (e.g.,
malignancy) or ↓excretion (e.g., due to drugs as thiazides).
It is characterized by sudden, severe attacks of pain, swelling, redness
and tenderness in the joints, often the joint at the base of the big toe.
Pathogenesis: Uric acid is synthesized from purine bases (substances
that are found naturally in your body) by xanthine oxidase enzyme & is
precipitated in joints, cartilage & kidneys when there is high levels of uric
acid in blood causing crystals. Theses crystals accumulate in joint,
causing the inflammation and intense pain of a gout attack.
Risk factors
Factors that increase the uric acid level in your body include:
• Diet. Purines are found in certain foods, so eating a diet rich in meat
and seafood and drinking beverages sweetened with fruit sugar
(fructose) increase levels of uric acid, which increased risk of gout.
Alcohol consumption, especially of beer, also increases the risk of
gout.
• Obesity. overweight, as the body produces more uric acid and
kidneys have a more difficult time eliminating uric acid.
• Medical conditions. Certain diseases and conditions increase risk
of gout. These include untreated high blood pressure and chronic
conditions such as diabetes, metabolic syndrome, and heart and
kidney diseases.
• Certain medications can increase uric acid level in blood: The
use of thiazide and loop diuretics commonly used to treat
hypertension. low-dose aspirin also can increase uric acid levels.
Diazoxide, pyrazinamide & cancer therapy
• Family history of gout. If other members of the family have had
gout, others of the same family are more likely to develop the
disease.
• Age and sex. Gout occurs more often in men, primarily because
women tend to have lower uric acid levels. After menopause,
125
however, women's uric acid levels approach those of men. Men are
also more likely to develop gout earlier usually between the ages of
30 and 50 whereas women generally develop signs and symptoms
after menopause.
• Recent surgery or trauma. Experiencing recent surgery or trauma
has been associated with an increased risk of developing a gout
attack.
Treatment of acute attack
▪ Colchicine, demecolcine.
▪ NSAIDs as indomethacin, phenylbutazone & ibuprofen.
▪ ACTH, glucocorticoids in resistant cases.
▪ IL1 inhibitors as anakinra given SC.
➢ Colchicine
Alkaloid with anti-mitotic effect. It relieves pain & inflammation of gouty
arthritis without affecting uric acid in blood. It inhibits phagocytosis &
leucocyte migration so prevents lactic acid formation & prevents
decreased pH so inhibits uric precipitation.
Uses:
1. Acute attack: 1 mg. then 0.5 mg/2 hours until pain disappears, or
diarrhea occurs (Maximum dose 6 mg).
2. Prophylaxis of gout (0.5 mg 2-3 times/week).
3. Prophylaxis of Mediterranean fever - liver cirrhosis, psoriasis
4. To improve liver function in patients with cirrhosis.
5. Skin disorders as psoriasis.
Adverse effects:
1- G.I.T. → Nausea, vomiting & Diarrhea.
2- Hepatotoxicity
3- Nephrotoxicity → Hematuria & Oliguria.
4- Bone marrow depression
5- Myopathy.
6- Reversible alopecia.
7-In acute poisoning there is hemorrhagic gastroenteritis, nephrotoxicity,
vascular damage and C.N.S. depression.
126
Treatment in between attacks
A-Uricosuric drugs 1. Probenecid:
• It increases uric acid excretion in Large dose > 1 g / day leading to decrease uric acid reabsorption from P.C.T
• Adverse effects: Nausea, loss of appetite, dizziness, vomiting, headache, sore
gums, or frequent urination NB:
➢ Small dose < 1 g / day → Uric excretion in P.C.T. → Worsens
gout.
➢ Probenecid decreases renal excretion of penicillin.
2. Sulphinpyrazone:
• Like phenylbutazone, but it has no analgesic or anti-inflammatory or
salt retaining effects.
• In therapeutic doses it has uricosuric action, but Its uricosuric action
is antagonized by salicylates
• It inhibits platelets aggregation.
• Drug interaction: it can increase the effect of warfarin and oral
hypoglycemics.
• Side effects as probenecid.
3. Benzbromarone
Potent Uricosuric Urinary excretion of uric acid (uricosuric) and
noncompetitive inhibitor of xanthine oxidase enzyme→ No
paradoxical hyperuricemia
4. Salicylates:
• Dose: more than 5 g/day (not commonly used).
• They are uricosuric in L.D. but produce uric acid retention in small
dose. They have no analgesic or anti-inflammatory action & their
action is antagonized by salicylates.
NB: Instruction during using uricosuric drugs
➢ Give plenty of fluids in gout.
➢ Alkaline urine minimizes urate deposition in kidney.
➢ In patients secreting large amount of uric acid avoid the use of
uricosurics.
➢ Uricosuric agents can be used in hyperuricemia due to cancer or
drugs.
B- Decrease uric acid synthesis.
127
• Allopurinol (active) → Alloxanthine (active metabolite).
It ↓ xanthine oxidase enzyme so ↓ uric acid in blood &↑ xanthine &
hypoxanthine which are soluble.
Used in chronic gout esp. in gouty nephropathy, renal failure, and
recurrent urate stones and in failure or intolerance of uricosuric drugs.
Side effects: allergy, headache, bone marrow depression, gut upset,
acute attack at start of treatment so give colchicine with it prophylactically.
Interactions: It is enzyme inhibitor.
NB: Rasburicase & pegylated uricase are recombinant form of urate
oxidase so convert uric acid into soluble allantoin.
. Used to prevent hyperuricemia during cancer therapy. They can
produce anaphylaxis, gut upset & hemolysis in G-6-PD deficiency.
Patient education and counseling
• Drink plenty of fluids. Stay well-hydrated, including plenty of water.
Limit how many sweetened beverages you drink, especially those
sweetened with high-fructose corn syrup.
• Limit or avoid alcohol. Talk with your doctor about whether any
amount or type of alcohol is safe for you. Recent evidence suggests
that beer may be particularly likely to increase the risk of gout
symptoms, especially in men.
• Get your protein from low-fat dairy products. Low-fat dairy
products may have a protective effect against gout, so these are your
best-bet protein sources.
• Limit your intake of meat, fish and poultry. A small amount may
be tolerable but pay close attention to what types — and how much
— seem to cause problems for you.
• Maintain a desirable body weight. Choose portions that allow you
to maintain a healthy weight. Losing weight may decrease uric acid
levels in your body. But avoid fasting or rapid weight loss, since
doing so may temporarily raise uric acid levels.
128

Clinical case:
52 years old male patient, obese, presented to his primary care doctor
because of the rapid onset of severe pain, swelling, redness, and warmth
in his left big toe. He also complained of dull pain in his left loin a few
months ago. The patient's past medical history was irrelevant except for
hypertension which was treated with hydrochlorothiazide. He prefers to
eat a huge amount of red meat every day in his lunch. On examination:
extremities are red, hot, swollen left metatarsophalangeal joint, no focal
neurologic deficit noted.
X-ray examination was done which revealed asymmetrical swelling within
the left metatarsophalangeal joint with no aberrant fracture in the bone.
Uric acid in this patient was 12mg/dl, the diagnosis was gouty arthritis
(monoarticular) in the left metatarsophalangeal joint.
Q1: What is the first-line therapy to treat pain in this patient?
a) Naproxen
b) Morphine
c) Aspirin
d) Paracetamol
Q2: If the patient was intolerant to your prescription in Q1 due to
epigastric pain when taken this medication, is there any other
alternative to relive the pain in the toe joint of this patient?
129
a) Colchicine
b) Dexamethasone
c) Rasburicase
d) Probenecid L.D
Q3: Which of the following statement describe the mechanism of the
action selected in Q2:
a) Inhibition of formation of uric acid
b) Increasing excretion of uric acid
c) Inhibition of leucocyte migration and phagocytosis
d) Conversion of poorly soluble uric acid into inactive, more soluble
metabolite
Q4: Mention another medical condition treated by the drug
prescribed in Q2, Enumerate 3 side effects for this medication?
a) Familial Mediterranean fever
b) Stroke
c) Deep venous thrombosis
d) Bronchial asthma
Q5: What is the medication should be added in between the attack
to decrease uric acid level in this patient?
a) probenecid in L.D
b) probenecid in S.D
c) Thiazide
d) Aspirin S.D
Q6: Could one of the medications prescribed by the doctor to
control the repeated attacks, responsible for developing this stone?
If your answer is yes, what is the advice to this patient to avoid the
development of this stone?
a) Drink plenty of water and to alkalinize the urine by sodium
bicarbonate.
b) Drink plenty of water and to acidify the urine by vitamin c.
c) Decrease water intake and to alkalinize the urine by sodium
bicarbonate.
d) Decrease water intake and to acidify the urine by vitamin c.
130
Q7: If the patient suffers from headaches is it preferable to take
aspirin? justify your answer?
a) Yes, as aspirin in small dose can increase renal excretion of uric
acid.
b) No, as aspirin in small dose can decrease renal excretion of uric
acid.
c) Yes, as aspirin decrease formation of uric acid.
d) Aspirin has no effect on uric acid.
Q8: All the following are goals of treatment in patient with gout
except?
a) Relieve pain and inflammation.
b) Prevent future gout attacks that could lead to permanent joint
damage.
c) Prevent the development of fibrosis in the liver.
d) Prevent kidney damage from chronically elevated urate levels.
Q9: Which of the following is not included in style modification in
patient with gout:
a) Avoid red meat & liver.
b) Avoid alcohol intake.
c) Drink plenty of fluid and always keep his urine alkaline.
d) Avoid Coffee & Tea
Q10: Which of the following drugs is contraindicated to be taken in
patient with gout?
a- Aspirin L.D. < 5 g / day. b- Probenecid L.D. < 1 g / day. c- Benzbromarone d- Diazoxide
131
Exercise (1) Answer case with explanation
1--------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
2--------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
3--------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
4--------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
5--------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
6--------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
7--------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
8--------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
9--------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
---------------------------------------------------------------------------------------------------
10----------------------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------------------------
-------------------------------------------------------------------------------------------------------
132
MCQ Musculoskeletal II
1- Select narcotic analgesic, which is a synthetic morphine derivative: a. Codeineb. Dezocinec. Fentanyld. Buprenorphine
2- Which of the following opioid analgesics is a strong mu receptor agonist?
a. Naloxoneb. Morphinec. Pentazocined. Buprenorphine
3-Indicate the narcotic analgesic, which is a natural agonist: a. Meperidineb. Fentanylc. Morphined. Naloxone
4-Select the narcotic analgesic, which is an antagonist or partial mu receptor agonist:
a. Fentanylb. Pentazocinec. Codeined. Methadone
5- Which of the following agents is a full antagonist of opioid receptors? a. Meperidineb. Buprenorphinec. Naloxoned. Butorphanol
6-. Which of the following opioid analgesics can produce dysphoria, anxiety and hallucinations?
a. Morphineb. Fentanylc. Pentazocined. Methadone
7-. Indicate the opioid analgesic, which has 80 times analgesic potency and respiratory depressant properties of morphine, and is more effective than morphine in maintaining hemodynamic stability?
a. Fentanylb. Pentazocinec. Meperidined. Codeine
133
8-Which of the following opioid analgesics is used in combination with droperidol in neuroleptanalgesia?
a. Morphine b. Buprenorphine c. Fentanyl d. Morphine
9-Fentanyl can produce significant respiratory depression by:
a. Inhibiting brain stem respiratory centre b. Suppression of the cough reflex leading to airway obstruction c. Development of truncal rigidity d. Both a and c
10-Which of the following opioid analgesics can produce an increase in the blood pressure and myocardial work?
a. Morphine b. Pentazocine c. Meperidine d. Methadone
11-Morphine causes the following effects except: a. Constipation b. Dilatation of the biliary duct c. Urinary retention d. Bronchiolar constriction
12-Therapeutic doses of the opioid analgesics:
a. Decrease body temperature b. Increase body temperature c. Decrease body heat loss d. Do not affect body temperature
13- Which of the following opioid analgesics is used in obstetric labor?
a. Fentanyl b. Pentazocine c. Meperidine d. Buprenorphine
14- Indicate the opioid analgesic, which is used for relieving the acute, severe pain of renal colic:
a. Morphine b. Naloxone c. Methadone d. Meperidine
134
15- Which of the following opioid analgesics is used in the treatment of acute pulmonary edema?
a. Morphine b. Codeine c. Fentanyl d. Loperamide
16- The relief produced by intravenous morphine in dyspnea from pulmonary edema is associated with reduced:
a. Perception of shortness of breath b. Patient anxiety c. Cardiac preload (reduced venous tone) and afterload (decreased
peripheral resistance) d. All of the above
17-Rhinorrhea, lacrimation, chills, gooseflesh, hyperventilation, hyperthermia, mydriasis, muscular aches, vomiting, diarrhea, anxiety, and hostility are effects of:
a. Tolerance b. Opioid overdosage c. Drug interactions between opioid analgesics and sedative-hypnotics d. Abstinence syndrome
18-The following has a selective morphine like effect on G.I.T.:
a- Loperamide b- Pentazocine c- Heroin d- Atropine
19-The diagnostic manifestations of acute morphine poisoning are:
a. Mydriasis, coma, and hyperventilation b. Coma, depressed respiration, hypotension and severe miosis c. Mydriasis, chills, and abdominal cramps d. Miosis, tremor and vomiting
20-Which of the following opioid agents is used in the treatment of acute opioid overdose?
a. Pentazocine b. Methadone c. Naloxone d. Fentanyl
21-Indicate the pure opioid antagonist, which has higher oral efficacy and longer duration:
a. Naloxone b. Naltrexone c. Tramadol d. Pentazocine
135
22-In contrast to morphine, methadone: a. Causes tolerance and physical dependence more slowly. b. Is more effective orally. c. Withdrawal is less severe, although more prolonged d. All of the above
23-Which of the following opioid analgesics is a partial mu receptor agonist?
a. Morphine b. Methadone c. Buprenorphine d. Fentanyl
24-Indicate a morphine derivative that is a dopaminergic agonist:
a. Heroin b. Apomorphine c. Nalbuphine d. Codeine
25-Which of the following opioid analgesics is a strong kappa receptor agonist, mu receptor antagonist and doesn’t increase cardiac work?
a. Naltrexone b. Methadone c. Nalbuphine d. Buprenorphine
26-Which of the following drugs has weak mu agonist effects and inhibitory action on norepinephrine and serotonin reuptake in the CNS?
a. Loperamide b. Tramadol c. Fluoxetine d. Butorphanol
27-Non-narcotic analgesics are mainly effective against pain associated with:
a. Inflammation or tissue damage b. Trauma c. Myocardial infarction d. Surgery
28-Non-narcotic agents cause:
a. Respiratory depression b. Antipyretic effect c. Euphoria d. Physical dependence
136
29- All of the following drugs are non-narcotic analgesics except: a. Paracetamolb. Acetylsalicylic acidc. Butorphanold. Ketorolac
30-Select the non-narcotic drug, which is aniline derivative: a. diclofenacb. Aspirinc. Baclophend. Paracetamol
31-Which of the following non-narcotic agents is salicylic acid derivative?
a. Phenylbutazoneb. Ketaminec. Aspirind. Tramadol
32-Which one of the following non-narcotic agents inhibits mainly cyclooxygenase (COX) in CNS?
a. Paracetamolb. Indomethacinc. Acetylsalicylic acidd. Ibuprofen
33-Most of non-narcotic analgesics have: a. Anti-inflammatory effectb. Analgesic effectc. Antipyretic effectd. All of the above
34-Indicate the non-narcotic analgesic, which lacks an anti-inflammatory effect:
a. Naloxoneb. Paracetamolc. Metamizoled. Aspirin
35-Correct statements concerning aspirin include all of the following except:
a. It inhibits mainly peripheral COXb. It does not have an anti-inflammatory effectc. It inhibits platelet aggregationd. It stimulates respiration by a direct action on the respiratory center
137
36-For which of the following conditions could aspirin be used prophylactically?
a. Noncardiogenic pulmonary edemab. Peptic ulcersc. Thromboembolismd. Metabolic acidosis
37-Side effects shared by NSAIDs include all the following except: a. Addictionb. Gastrointestinal ulcerationc. Hypersensitivityd. Nephropathy
38- Pharmacologic actions of acetylsalicylic acid include all of the following except:
a. Analgesicb. Antipyreticc. Anti-inflammatoryd. Promotion of platelet aggregation
39- Aspirin is used in treatment of: a. Vertigob. Peptic ulcerc. Acute left ventricular failured. Acute rheumatic fever
40- Manifestations of acute salicylate intoxication include all the following except:
a. Hyperpyrexiab. Hyperpneac. Pinpoint pupilsd. Convulsions
Musculoskeletal II Key Answers
1 c 16 d 31 c
2 b 17 d 32 a
3 c 18 a 33 d
4 b 19 b 34 b
5 c 20 c 35 b
6 c 21 b 36 c
7 a 22 d 37 a
8 c 23 c 38 d
9 d 24 b 39 d
10 b 25 c 40 c
11 b 26 b
12 a 27 a
13 c 28 b
14 d 29 c
15 a 30 d
138