migrant health: best practices & travel medicine
TRANSCRIPT

Migrant Health: Best
Practices & Travel Medicine
William Stauffer
University of Minnesota CISTM Quebec, Canada
May 26, 2015
• Financial disclosure (Critical Measures: Cultural Health Care Education) • If we discuss any off label uses of medications we will disclose to the audience

Objectives
• Important health issues in migrant populations • Important screening tests & health
interventions to promote migrant health • Important opportunities to promote health in
the pre-travel setting
• Hopefully have fun…
Thanks to Chris Greenaway innovative topic that I struggle with but never thought of as a presentation topic.

Humans and mobility • Human migration has occurred as long as humans have
been on the planet – first left Africa ~60 million years ago • UK is home to the most diverse community in the world • There are at least 1,000 French-born people living in each
of 83 different countries • The number of immigrants living in Spain grew ~8 fold
between 1990-2013 • The POOREST countries have the LEAST number of
emigrants • 84% of UAE population is foreign born

Humans and mobility • More than 200 million people live outside their
country of birth • 3% of the world’s population • 5th most populated country in the world
• In US: • ~13% of population 1st generation FB • Estimated 45,790,000 were born outside the US • Miami >60%, NYC >30%
• Almost uniformly most vulnerable and disenfranchised in health systems

11Source: Population Action International 1994
Migrating Populations, 1960-1975
22
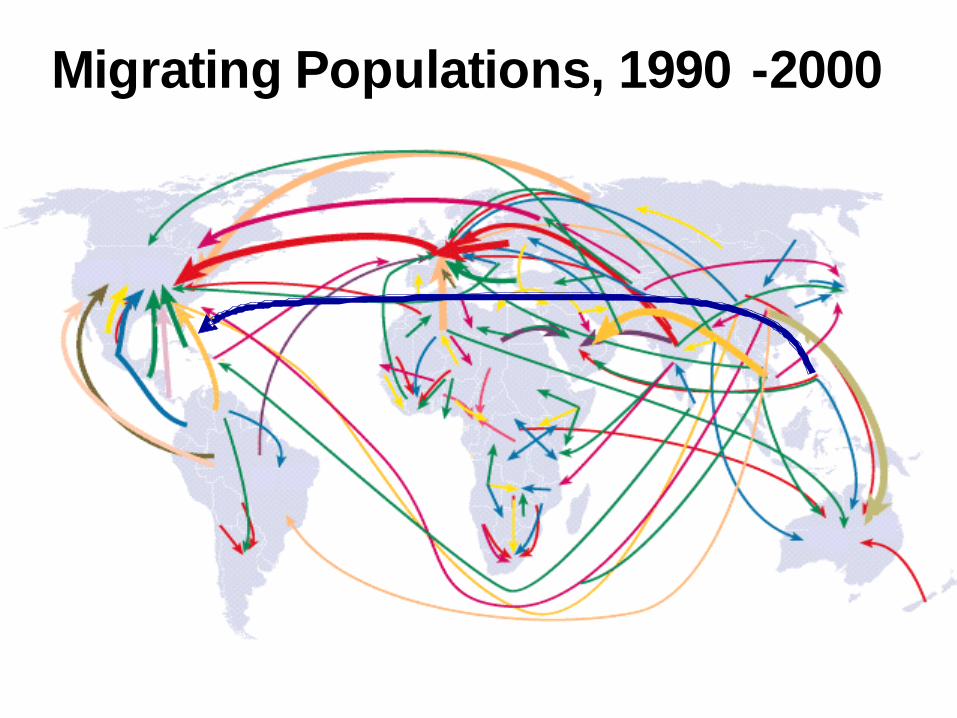
•• 2000: 175 million; >4x increase from 1975 2000: 175 million; >4x increase from 1975
•• 2050: 230 million2050: 230 million
Sources: Population Action International 1994, International Org anization for Migration, 2003
Migrating Populations, 1990 -2000


Guidelines for migrant health screening
• United States • CDC (refugee & international adoptee) • AAP (in process for all migrants & international adoptee)
• Canada • CMAJ—Canadian Collaboration for Immigrant and
Refugee Health (2011)
• Australia • Refugee
• UK • Migrant Health Assessment Sub-committee of HPSC
Scientific Advisory (2015)
• Europe • Call for development

Common components
• History & physical • Routine blood & urine testing
• CBC with diff, renal fxn, pregnancy
• Tuberculosis • Chronic or regulatory infections
• HIV, syphilis, GC/Chlamydia, hep C
• Parasitic testing • Stool, focus on strongyloides & schistosomiasis
• Misc (e.g. Toxins, vitamins) • Lead, B12
• Vaccine recommendations, including testing for active hepatitis B

Also disease specific guidelines
• Common diseases/infections • Hepatitis B • HIV • Hepatitis C • TB • Lead • Chronic non-communicable diseases (e.g. HTN, Diabetes,
lipids) • Cancers (breast, colon, prostate)
• Health Prevention Guidelines • Vaccination • Dental • Vision • Hearing

Why Screen?
• Public Health and/or Regulatory (not necessarily the same)
• Patient Centered Care • Tenants of Screening

How, when and why can pre-travel visit overlap with screening & preventive measures in migrants?
• Point of Contact: frequently disenfranchised population with limited health care access
• Travel providers may be more educated and aware
of certain diseases, particularly infections, that affect migrants (disease disparity)
• A travel provider cares about preventing
morbidity and mortality and has the opportunity by definition—this is an added opportunity

Hang with me ☺
• Case based examples (5 cases) • A bit of “read my mind” & show and tell • Please, at the conclusion, question, add or
subtract…

Case #1
33 yo female of Korean descent (adopted age 4 years), traveling to India (Mangalore) for 1 month for wedding (marrying an Indian gentlemen). • Past Medical History
• Had an ASD repaired as a child • Seasonal allergies
• Meds • Intranasal steroid prn

Case #1
33 yo female of Korean descent (adopted age 4 years), traveling to India (Mangalore) for 1 month for wedding (marrying an Indian gentlemen). • Immunizations
• Tdp UTD • Polio UTD • HPV completed • Hep B UTD • MMR UTD • Hep A none • VZV—had chicken pox as child
Case #1
33 yo female of Korean descent (adopted age 4 years), traveling to India (Mangalore) for 1 month for wedding (marrying an Indian gentlemen).
• Where is your opportunity? • Immunizations
• Tdp UTD • Polio UTD • HPV completed • Hep B UTD • MMR UTD • Hep A none • VZV—had chicken pox as child

Highlight Case
19 y/o Vietnamese male presents to the ED with 2 months wt loss, low grade fevers, swelling of the abdomen.
• Exam
• cachectic male with protuberant abdomen and the liver is > 10 cm below the costal margin with multiple palpable, non-tender nodules. In addition there is a fluid wave and he has pitting lower extremity edema.

Highlight Case
• Laboratory WBC: 9 Hgb: 9.8 (MCV 68) Plt.: 130 ESR: 88 ALT: 599
Diagnostic lab test returns
Alpha-fetoprotein 889

Highlight Case
• Laboratory WBC: 9 Hgb: 9.8 (MCV 68) Plt.: 130 ESR: 88 ALT: 599
Diagnostic lab test returns Alpha-fetoprotein 589
Alpha-fetoprotein 889

19 y.o. Vietnamese male with abdominal pain,
increased alpha-fetoprotein
The most likely etiology of this hepatocarcinoma is:
a. Hepatitis B b. Aflotoxin c. Hepatitis C d. Schistosomiasis

19 y.o. Vietnamese male with abdominal pain,
increased alpha-fetoprotein
The most likely etiology of this hepatocarcinoma is:
a. Hepatitis B b. Aflotoxin c. Hepatitis C d. Schistosomiasis

Hepatocellular carcinoma
• 4th most common cause of cancer related deaths in world: 610K/year
• A vaccine preventable cancer • Treatment available • Population specific cancer screening

Hepatitis B
• CDC recommends testing for:
• Individuals born in areas where prevalence of HBsAg is ≥ 2%, regardless of immunization status in country of origin
• US-born persons not immunized during infancy born to
parents in regions with prevalence of HBsAg ≥ 8%
Weinbaum CM et al. MMWR. 2008; 57(RR08);1-20.

Geographic distribution of hepatitis B, 2009

Hep B
• ~240 million infected worldwide, 1.2 million in US • 15-25% lead to severe liver disease and/or cancer • FYI: Asia pacific islanders make up <5% of total
US population, account for more than 50% of chronic infections.

Hepatitis B infection Among Refugees by Region of Origin, Minnesota, 2013
0%
1%
0%
8%
5%
6%
0% 5% 10% 15% 20%
Europe
North Africa/Middle East
Latin America/Caribbean
SE/East Asia
Sub-Saharan Africa
Overall Hepatitis BInfection Rate
Refugee Health Program, Minnesota Department of Health
N=2,050 screened
122/2,050
43/897
77/990
0/8
2/152
0/3

Case #1
33 yo female of Korean descent (adopted age 4 years), traveling to India (Mangalore) for 1 month for wedding (marrying an Indian gentlemen).
• Where is your opportunity? • What do you want to do with her immunizations?
• Tdp UTD • Polio UTD • HPV completed • Hep B UTD • MMR UTD • Hep A none • VZV—had chicken pox as child

Case #1
33 yo female of Korean descent (adopted age 4 years), traveling to India (Mangalore) for 1 month for wedding (marrying an Indian gentlemen).
• Where is your opportunity? • What do you want to do with her immunizations?
• Anti-B surface antibody positive • Anti-B core antibody negative • Hepatitis B surface antigen positive • Hepatitis A antibody positive

Case #1 Main Point
• Always consider hepatitis B infection, even if documented vaccination (but no documented testing)

Case #2
58 yo Hmong male traveling to Chang Mai Thailand for 3 weeks to VFR. • PMHx
• Glaucoma • Uric acid kidney stones • Chronic renal failure, has met with transplant team • LTBI (treated with 9 months INH)
• Meds • Aspirin • Lisinopril • Topical steroids
• Social History • Moved as refugee to US in 1993 • Five children, 8 grandchildren

Case #2
58 yo Hmong male traveling to Chang Mai Thailand for 3 weeks to VFR. • Immunizations
• Tdp UTD • Polio UTD • Hep B UTD (neg HBsAg) • MMR UTD • Hep A immune by serology • VZV—immune by serology

Case #2
58 yo Hmong male traveling to Chang Mai Thailand for 3 weeks to VFR. • Where is your opportunity?

Highlight Case
• One week prior • 55 year old Hmong m presented with
wheezing & SOB. • He was placed on prednisone for
“asthma”.
• Today, presents w/ fever, rash, confusion & abdominal pain.
• Quickly develops septic shock, E. coli bacteremia & dies.
• Had moved to Minnesota > 15 years prior from Thailand.


Photo provided by Charles Cartwright, PhD

55 y.o. Hmong male with SOB/Wheezing
Most likely diagnosis is? a. Urosepsis b. Ruptured viscous c. Strongyloidiasis d. Melioidosis

55 y.o. Hmong male with SOB/Wheezing
Most likely diagnosis is? a. Urosepsis b. Ruptured viscous c. Strongyloidiasis d. Melioidosis

Pt. Age Ethnicity Time in US
Outcome
1 42 Cambodia 6 mo Recovery 2 24 Hmong 3 yrs Recovery 3 34 Hmong >5 yr Recovery 4 52 Vietnamese >5yr Recovery 5 46 Hmong 8 yrs Death
6 69 Hmong 4 yrs Death
7 72 Laotian 7 yrs Death
8 49 Vietnamese >5yrs Recovery 9 34 Hmong 4 yrs Death
Newberry AM, CHEST 2005;128(5):3681-4.
Newberry AM, CHEST 2005;128(5):3681-4.

Pt. Age Ethnicity Time in US
Outcome
1 42 Cambodia 6 mo Recovery 2 24 Hmong 3 yrs Recovery 3 34 Hmong >5 yr Recovery 4 52 Vietnamese >5yr Recovery 5 46 Hmong 8 yrs Death
6 69 Hmong 4 yrs Death
7 72 Laotian 7 yrs Death
8 49 Vietnamese >5yrs Recovery 9 34 Hmong 4 yrs Death
Newberry AM, CHEST 2005;128(5):3681-4.
Newberry AM, CHEST 2005;128(5):3681-4.

Strongyloides stercoralis disseminated/hyperinfection Syndrome
• More than 100 million people infected with strongyloides worldwide.
• 10 cases of disseminated strongyloides in 7 months in Toronto1
• 151 cases of strongyloides (not disseminated) • if not diagnosed at time of arrival mean time to
diagnosis was 61 months2
1Lim S. CMAJ 2004;171(5): 479-84 2 Boulware DR, Stauffer WM et al. Am J Med 2007;120(60):545;e1-8

Strongyloides in migrants
• Strongyloides • East Africa 11%, Cambodian 42% (Australia)1 • Lao refugees, 20% positive 12 years after arrival2 • Burmese and Liberian, over 65% seropositive from migrant
serum bank3
1. Caruana SR, et al. J Travel Med. 2006;13:233-239
2. 3de Silva S, Saykao P, Kelly H, et al. Epidemiol Infect 2002:128(3):439-44. 3. Unpublished research data.
Case #2
• Test vs. presumptively treat Case #2 Main Point • Consider strongyloides (do no harm) especially in
high risk migrants who have a likelihood of receiving immunosuppression.

Case #3
• 16 yo Somali female brought by “uncle” to travel to Kenya for 3 months over the summer. • PMHx
• No significant
• Meds • None
• Social History • Family moved to US when she was 4 years of age from
Dadaab. Lives with extended family in “Little Mogadishu” in an apartment with 8 other individuals.

Case #3
• 16 yo Somali female brought by “uncle” to travel 2 Kenya for 3 months over the summer. • Immunizations/Preventive measures
• All routine immunizations are UTD • Had new arrival screening at 4 years of age
• What opportunity do you see?

Case #3
• TB screening • IGRA positive (CXR negative)
• Scheduled for latent TB treatment

25%
9%
0%
18%
30%
22%
0% 10% 20% 30% 40% 50%
Europe
North Africa/Middle East
Latin America/Caribbean
SE/East Asia
Sub-Saharan Africa
Overall TB Infection
2/8
173/986
N=2,033 screened
*Diagnosis of Latent TB infection (N=446) or Suspect/Active TB disease (N=9)
Refugee Health Program, Minnesota Department of Health
Tuberculosis Infection* Among Refugees By Region Of Origin, Minnesota, 2013
266/886
455/2,033
14/150
0/3

Case #3
• TB screening • IGRA positive (CXR negative)
• Scheduled for latent TB treatment
Red Flag: Wearing headphones, Hijab, says “I am not going”…

Case #3
• Red Flag: Guesses?

Case #3
• Female Genital Mutilation

Case #3 Main Point
• Pre-travel visit is opportunity to identify those at risk of being infected with TB as well as assessing risk and appropriate follow-up after travel.

Case #4
43 yo Congolese female going to Rwanda (outside Kigali) for 9 day trip for funeral—leaving in 5 days. • PMHx
• Malaria
• Meds • None
• Social History • Moved to U.S. 2 years ago to join family (through lottery)
from Rwanda • 4 children, three grandchildren

Case #4
43 yo Congolese female going to Rwanda (outside Kigali) for 9 day trip for funeral. • Immunizations
• Tdp had 2 recorded • Polio has 2 recorded • Hep B none • MMR UTD • Hep A none • VZV – no vaccine

Case #4
43 yo Congolese female going to Rwanda (outside Kigali) for 9 day trip for funeral. • What are your opportunities?

Case #4
43 yo Congolese female going to Rwanda (outside Kigali) for 9 day trip for funeral. • What are your opportunities?
• Tetanus, diphtheria, pertussis had 2 recorded • Polio has 2 recorded • Hep B none • MMR UTD • Hep A none • VZV – no vaccine

Case #4
43 yo Congolese female going to Rwanda (outside Kigali) for 9 day trip for funeral. • What do you want to do with her immunizations?
• Boost Tetanus, diphtheria, pertussis & polio (could do select serologies)
• Anti-B surface antibody negative • Anti-B core antibody positive • Hepatitis B surface antigen negative • Hepatitis A antibody positive • VZV antibody negative

VZV
• Mean age of developing disease is 10-15 years in tropical countries (some countries a large percentage of those >35 years are susceptible)
• Opportunity to vaccinate, especially adolescents1
1Greenaway C, et al. Epidemiol infect 2014;142(8):1695-707

Case #4
• 43 yo Congolese female going to Rwanda (outside Kigali) for 9 day trip for funeral. • Other Opportunities?
• Hint: in 2010 the US stopped requiring mandatory testing prior to immigration.
Case #4
• 43 yo Congolese female going to Rwanda (outside Kigali) for 9 day trip for funeral. • Other Opportunities?
• HIV antibody positive, confirmed with PCR

Case #4
• 43 yo Congolese female going to Rwanda (outside Kigali) for 9 day trip for funeral. • Other Opportunities?
• HIV antibody positive, confirmed with PCR
• Rate in Congolese refugees in Rwanda ~3%

HIV Screening
• CDC • Basically opt-out, everyone should be tested; annual
testing in high risk persons (MMWR Sept 22, 2006;55(14);1-17.
• Canada • Individual requesting • S/S of infection • Illness associated with “weakened immune system or a
diagnosis of TB” • Unprotected intercourse or use of shared drug equipment
with a partner whose HIV status is known to be positive • Pregnant or planning pragnancy • Victims of sexual assualt

Case #4
• 43 yo Congolese female going to Rwanda (outside Kigali) for 9 day trip for funeral. • Even More Opportunities?
Highlight Case
20 yo Somali female presenting with acute abdominal pain, anorexia & fever • <24 hours, no stool • No sign PMHx, No Meds • Social history: moved from Kenya (refugee) 14
months prior to presentation

Highlight Case
20 yo Somali female presenting with acute abdominal pain, anorexia & fever • Examination
• RRQ tenderness with sigs of peritoneal irritation (rebound, positive R leg lift)
• Laboratory • WBC: 18,000 (N88, L11, E1) • Hgb 12.4 (MCV nl) • CRP 14 (nl<0.9) • Abdominal flat plat (decreased air RLQ)
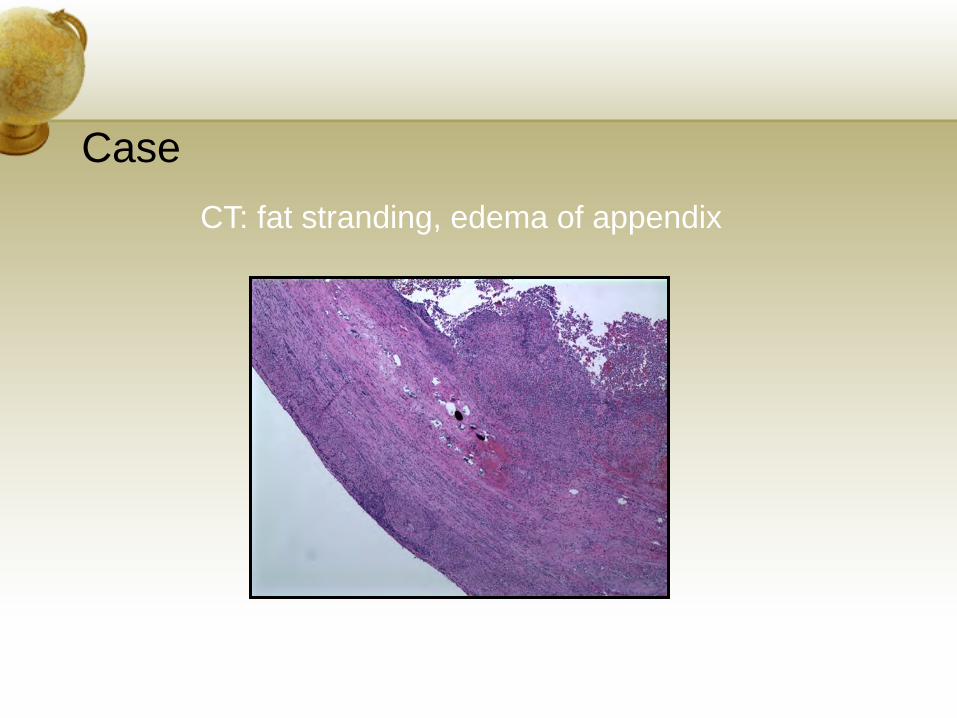
Case CT: fat stranding, edema of appendix

Case: Abdominal pain, fever

Prevalence of Schistosoma among African Refugees, 1993-2004
• 289/291 (99.3%) Schistosoma cases identified among sub-Saharan Africans
• Prevalence = 2.4% among African refugees
• Central Africans 6/51 (11.8%) • West Africans 130/2358 (5.5%) • East Africans 153/9445 (1.6%)

• Schistosomiasis • Somali, over 80% seropositive from migrant serum bank1 • Increasing case series and reports on complications after
arrival in the U.S. • Complications reported due to excessive invasive testing
1. Unpublished research data.
2. Summer AP, et al. Hematuria in children. Clin Pediatr 2006;45():177-81.

Parasitic infections in migrants
• CDC Lost Boys (Sudanese) Reunion Study (n=464)1
• 49% tested positive for strongyloidiasis by serology • 44% tested positive for Schistosomiasis mansoni or
hematobium • 22% seropositive for Both
• 69% were seropositive for Either
1 Posey DL, et al. Clin Infect Dis 2007;45(10):1210-5.

Case #4
• 43 yo Congolese female going to Rwanda (outside Kigali) for 9 day trip for funeral. • What about strongyloides? • Do you want to presumptively treat?


Case #4 Main Points
• Usually multiple opportunities • Consider HIV testing if appropriate • Consider other chronic infections with high
prevalence (e.g. schistosomiasis) • Be aware of Loa loa and risk of presumptively
using ivermectin for strongyloides

Case #5
37 yo Pakistani male planning a 2 week trip to Panama City for business. • PMHx
• Asthma and hospitalized for pneumonia 2 years ago (ID saw and had presumptive treatment for strongyloides and serology came back positive)
• Tested for LTBI and negative 2 years ago • HIV documented negative
• Meds • None
• Social history • Moved to US in 1997 with family as immigrant. Has 3
children, married.

Case #5
37 yo Pakistani male planning a 2 week trip to Panama City for business. • Imminizations
• Tdp UTD • Polio UTD • Hep B UTD (Hep B Antigen negative) • MMR UTD • Hep A immune by serology • VZV—immune by serology

Case #5
37 yo Pakistani male planning a 2 week trip to Panama City for business. • Opportunity?

Case #5
37 yo Pakistani male planning a 2 week trip to Panama City for business. • Opportunity? HINT

Case #5
37 yo Pakistani male planning a 2 week trip to Panama City for business. • Opportunity?
• Hepatitis C antibody positive, PCR confirmed

Hepatitis C
• Estimated 170 million cases worldwide, 3.2 million in the US.
• Certain populations with very high rates • E.g. Bolivia, Cameroon, Central Republic of Africa, Chad,
China, DRC, Egypt, Guinea, Mongolia, Pakistan, Rwanda, Thailand, Vietnam.
• Of every 100 persons infected with HCV • 75-85% will develop chronic infection • 60-70 will go on to develop chronic liver disease • 5-20 will develop cirrhosis over a period of 20-30 yrs • 1-5 will die from consequences (HCC or cirrhosis)

Case #5 Main Point
• Consider Hep C in higher risk populations

Conclusion
• Disease prevalence varies by population • The Pre-travel visit represents an opportunity to
screen for chronic infections which have substantial morbidly and mortality • Hepatitis B • Strongyloides • HIV • TB • Other Chronic Infections/conditions
• Hep C • Schistosomiasis
• Offers opportunity to up date routine vaccines and to establish care for chronic diseases/infections