belgian consensus meeting on travel medicine … · belgian consensus meeting on travel medicine...
TRANSCRIPT

27/11/2015
1
BELGIANCONSENSUS MEETINGon TRAVEL MEDICINE
June 26, 2015
Belgian Scientific Study Group on Travel
Medicine
Pr. A. Van Gompel & Dr U Maniewski (ITG)Pr. F. Jacobs (Hôp. Erasme, ULB)
Pr. P. Lacor & Dr L Seyler (UZ-Brussel) Dr. Ph. Leonard (CHU-ULg)
Pr. W. Peetermans (U.Z. - K.U.Leuven) Pr. S. Callens(UZ.- U.Gent) Dr. S. Quoilin (iph.fgov.be)
Dr. P. Soentjens (Belgian Defence)Pr. B. Vandercam (CHU. St. Luc, UCL)
Pr. Y. Van Laethem & Dr C Martin (CHU. St. Pierre, ULB)PART 1a yellow fever version 25/11/15
REPORTBELGIAN CONSENSUS MEETING on TRAVEL MEDICINE
June 26, 2015 – PART 1a
2015
• The consensus meeting was chaired by A. Van Gompeland Y, Van Laethem
• Secretary of the meeting was P Lacor• A preliminary PowerPoint, prepared by A. Van Gompel,
was presented• The discussion and recommendations of the
meeting are included in this finale presentation.• The ESSENTIAL SLIDES (pdf-version) & the
CONSENSUS BROCHURE (in Dutch and French) highlighting the proposals for changes will been sent to all participants. May be used for teaching.
• These documents will serve as a proposal for approval by the governmental Belgian Health Council – section Vaccinations, on 17-09-2015
• Responsable final redaction : A. Van Gompel

27/11/2015
2
Not an exhaustive review of travel medicine
• What has changed ?• Answers to questions, asked in the last months• Tips
• All slides of the consensus document, as well as the hand-outs will be available on the website of the ITM, and may be used for teaching purposes
2015
URL’s former years www.itg.beReisgeneeskunde informatie voor deskundigenhttp://www.itg.be/itg/GeneralSite/Default.aspx?l=n&WPID=293&MIID=679 Médecine des voyages information pour expertshttp://www.itg.be/itg/GeneralSite/Default.aspx?L=F&WPID=293&MIID=679
2015
27/11/2015
3
2015
http://wwwn.cdc.gov/travel/contentYellowBook.aspx
www.who.int/ith
• Sources for the update– the international literature– the 2015 congress & discussion forum of the ISTM– the “2012 & 15” edition of International Travel and Health (WHO)– the 2016 edition of Health Information for International Travel (CDC)
• The updated 2014-15-edition of “Medasso”, edited by A. Van Gompel and the staff of the medical service of the Institute for Tropical Medicine Antwerp, is also recommended as a valuable source of information.
2015

27/11/2015
4
Only these chapters are updated
They are freely downloadable
http://www.who.int/ith/en/ Only a few chapters since 2012 are updated 2014 & 2015
WHO 15-06-2015
Gebruik geen verouderde versies, daar ze onbruikbaar zijn geworden en check steeds de meest recente electronische versie !
Les éditions imprimées anciennes sont dépassées et donc inutilisables ! Consultez toujours la version électronique la plus récente.
2015

27/11/2015
5
1995 2015
Travel Medicine Seminar 19 /11/15 “Travel Medicine Seminar 20 years later”
MILITAIR HOSPITAAL (as in 1995) 14.00-14.05 Introduction
14.05-14.35 Yellow Fever Immunization: where are we up to now?CHARLOTTE MARTIN (CHU. St. Pierre - ULB)
14.35-15.05 The last-minute traveler: an update on accelerated vaccine schedulesPATRICK SOENTJENS (Defence & ITG/IMT)
15.05-15.25 Epidemiologic flashes & edge cutting news / new vaccines STEVEN CALLENS (UZ.-.U.Gent)
15.25-16.00 Coffee break
16.00-16.25 Travellers diarrheaLUCIE SEYLER (UZ.-Brussel),
16.25- 16.50 Malaria: when prevention is not clear-cutULA MANIEWSKI (ITG/IMT)
16.50-17.15 Traveller's ThrombosisPETER VERHAMME (U.Z.-K.U.Leuven)
17.15-17.45 What did change (drastically) in the last 20 years in travel medicine ? FONS VAN GOMPEL (ITG/IMT) & YVES VAN LAETHEM (CHU. St. Pierre, ULB)
Have a look at http://www.sbimc.org for the pdf’s of the powerpoints of all the lectures since 2009

27/11/2015
6
PART 1• 1.a - Vaccination for Yellow Fever• 1.b - Malaria
PART 2• 2.A - Other vaccinations• 2.B - TD, other infections, …., • 2.C - VARIA
2015
Yellow Fever
2015

27/11/2015
7
Adaptation june 2015
• Countries requiring yellow fever vaccination for entry do so in accordance with the International Health Regulations.
• Yellow fever is currently the only disease for which proof of vaccination may be required for travellers as a condition of entry to a State Party under Annex 7 of the International Health Regulations (2005).
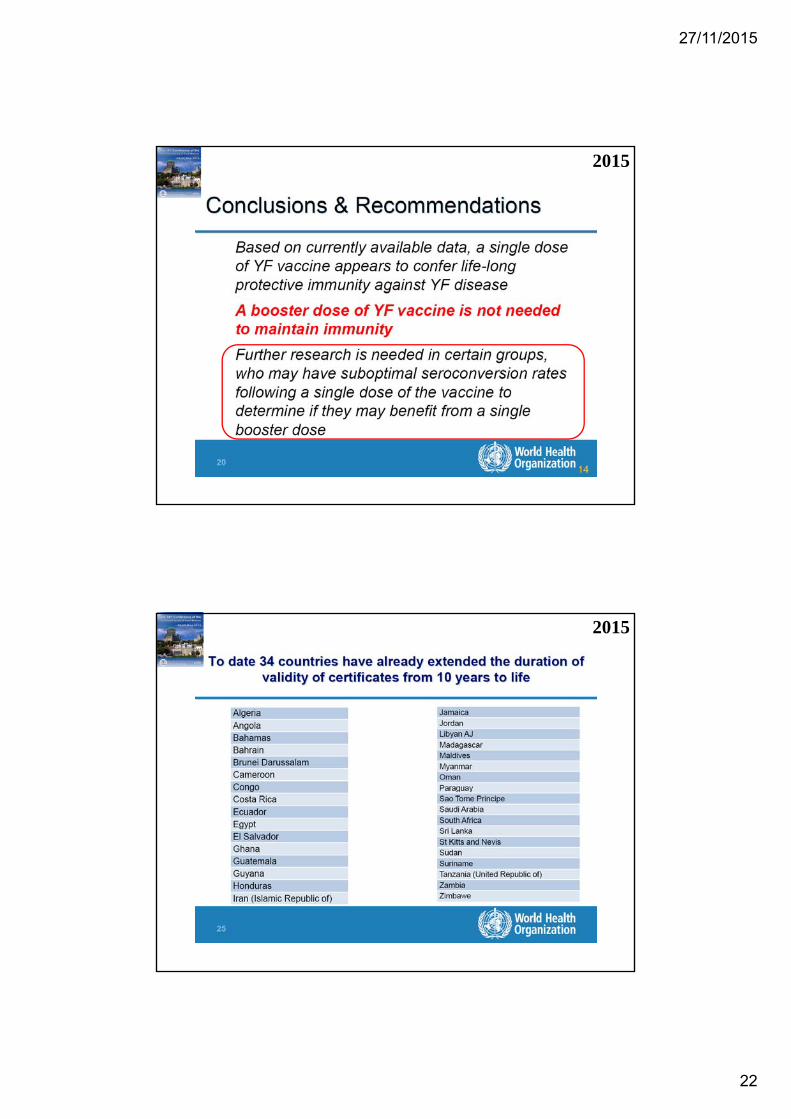
• An important change in May 2014 was the adoption by the World Health Assembly of an updated Annex 7, extending the validity of a certificate of vaccination against yellow fever from 10 years to life.
• Although this requirement will come into force only from July 2016, several countries have started implementing these new rules.
• When available, this information is included in this annex 1(http://www.who.int/ith/2015-ith-annex1.pdf?ua=1)
• This section contains information on yellow fever requirements as provided by countries.
• Country requirements are subject to change at any time. Updates can be found at: http://www.who.int/ith.
2015
Some countries already agree with this statement - amongst the countries with risk of yellow fever : Angola, Cameroon, Congo-Brazzaville (but not the Democratic Republic of Congo), Ghana, Soudan, Ecuador, SurinameParaguay and British Guyana (but not French Guyana).
2015
The WHO published a very practical list : http://www.who.int/ith/2015-ith-annex1.pdf?ua=1

27/11/2015
8
http://www.who.int/ith/2015-ith-annex1.pdf?ua=1:
2011 & 2012

27/11/2015
9
2015•Le Rwanda est devenu une région endémique à «faible risque» de fièvre jaune•Le R.D Congo: vaccination contre la fièvre jaune recommandée dans tout le pays
2015

27/11/2015
10
3 Feb 2015 2015
YELLOW FEVER - AFRICA (03): ZAMBIA CERTIFICATION CHANGE*******************************************************
A ProMED-mail post <http://www.promedmail.org>A program of the International Society for Infectious Diseases http://www.isid.org
Date: Wed 28 Jan 2015 Source: Times of Zambia [edited] <http://www.times.co.zm/?p=49194>
The Tourism Council of Zambia (TCZ) is pleased that South Africa and Botswana have finally agreed to drop yellow fever certification as a requirement for travellers from Zambia, following the World Health Organisation (WHO) declaring Zambia a yellow fever free zone.
TCZ chairperson Felix Mulenga said the decision, which was long-awaited, would significantly increase international tourist arrivals. South Africa is Zambia's leading source market for international arrivals, accounting for around 20.1 per cent of total arrivals in 2013. Health Minister Joseph Kasonde announced on Monday this week that South Africa and Botswana had with immediate effect lifted the requirements of yellow fever certification for travellers from Zambia.
The WHO found from scientific research that Zambia had reduced cases of the yellow fever. Mr Mulenga said in an interview that the removal of the yellow fever certification for travellers from South Africa or through South Africa to Zambia would significantly improve the tourist arrivals from that country. "We are happy that South Africa and Botswana have decided to drop their demands on the yellow fever certification because this was creating a negative impact on the growth of the tourism sector in Zambia. As you know, South Africa is an important market for Zambia and currently is Zambia's leading source market for tourists," Mr Mulenga said.
In 2013, the Southern Africa region recorded total arrivals of more than 22 million, representing a market share of global arrivals of approximately 2.5 per cent and a 39.9 per cent share of Africa's total arrivals. South Africa accounted for 191 048 tourist arrivals in the year under review, followed by Tanzania with 184 187.
Mr Mulenga said the yellow fever issue was an impediment to tourist arrivals as it affected the growth of the sector and that with the newdevelopment Zambia would attract desired levels of tourists and compete favourably in the region and beyond.
[Byline: Maimbolwa Mulikelela] Communicated by: ProMED-mail from HealthMap Alerts <[email protected]>
[Zambia now has been recognized as yellow fever (YF) free by the WHO.The South Africa requirements for proof of vaccination status has recently led to the sale of fake YF vaccination cards in Zambia and Zimbabwe. The change in South African requirements should end this illegal and unfortunate practice. It is good to see government vaccination status policy brought into line with this change in YF status recognized by WHO. As the facts change, then policies and regulations should change along with them and not be locked into place in perpetuity. It is important to recognize that policies can have negative economic and social consequences. One hopes that Zambia will benefit from the change in yellow fever vaccination requirements in South Africa.
201528 Jan 2015

27/11/2015
11
WHO 2013Colombia
2013 = 14 = 15
2014 = 2015

27/11/2015
12
Transit in aeroportIn principle yellow fever vaccination is not required
if the traveler stays in the transit zone of the airport for maximum 12 hours with an entry and exit record of the same day.
Some countries require vaccination certificate for any transit in an endemic country, irrespective of the duration.
The recommendation must also take into consideration that flight itineraries can change unannounced (e.g. stopover in Ethiopia or Senegal).
2015
See who-country list – not in annex 1
1 dose = lifelong ?

27/11/2015
13
2013
WER 17-05-2013 WHO-SAGE
scientific advice
“YELLOW FEVER VACCINATION
induces LIFELONGPROTECTION”
2013

27/11/2015
14
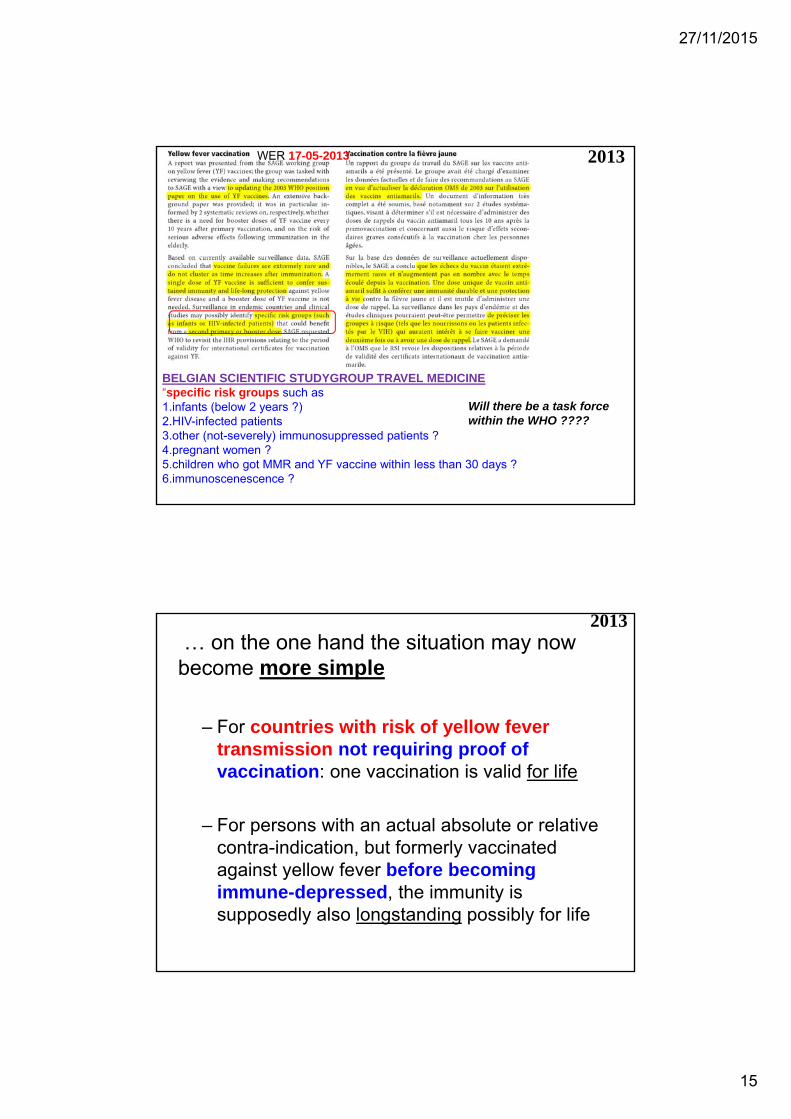
2013May 2013 scientific advice by the WHO SAGE(= Strategic Advisory Group of Experts on Immunization)
WER 17-05-2013“
2013
“specific risk groups(such as infants or HIV-infected patients)could benefit from a second primary or booster dose”
WER 17-05-2013
27/11/2015
15
2013
BELGIAN SCIENTIFIC STUDYGROUP TRAVEL MEDICINE “specific risk groups such as 1.infants (below 2 years ?) 2.HIV-infected patients3.other (not-severely) immunosuppressed patients ? 4.pregnant women ?5.children who got MMR and YF vaccine within less than 30 days ?6.immunoscenescence ?
Will there be a task force within the WHO ????
WER 17-05-2013
… on the one hand the situation may now become more simple
– For countries with risk of yellow fever transmission not requiring proof of vaccination: one vaccination is valid for life
– For persons with an actual absolute or relative contra-indication, but formerly vaccinated against yellow fever before becoming immune-depressed, the immunity is supposedly also longstanding possibly for life
2013

27/11/2015
16
… on the other hand the situation may nowbecome temporarily also more complex
– At this moment many countries (with or without risk of YF transmission) still require a renewedproof of vaccination after 10 years– if a person plans to cross the border(or in transit)
from one country with (a real or supposed) risk for YF transmission to another country
she/he will then need an up-to-date Certificate ... she/he may think to be in order “immunologically”, but not “politically” or “legally” or administratively”
– No waiver can be delivered but for proper medicalreasons (absolute or relative contra-indication)
2013
2014

27/11/2015
17
Scientific articles
PRO
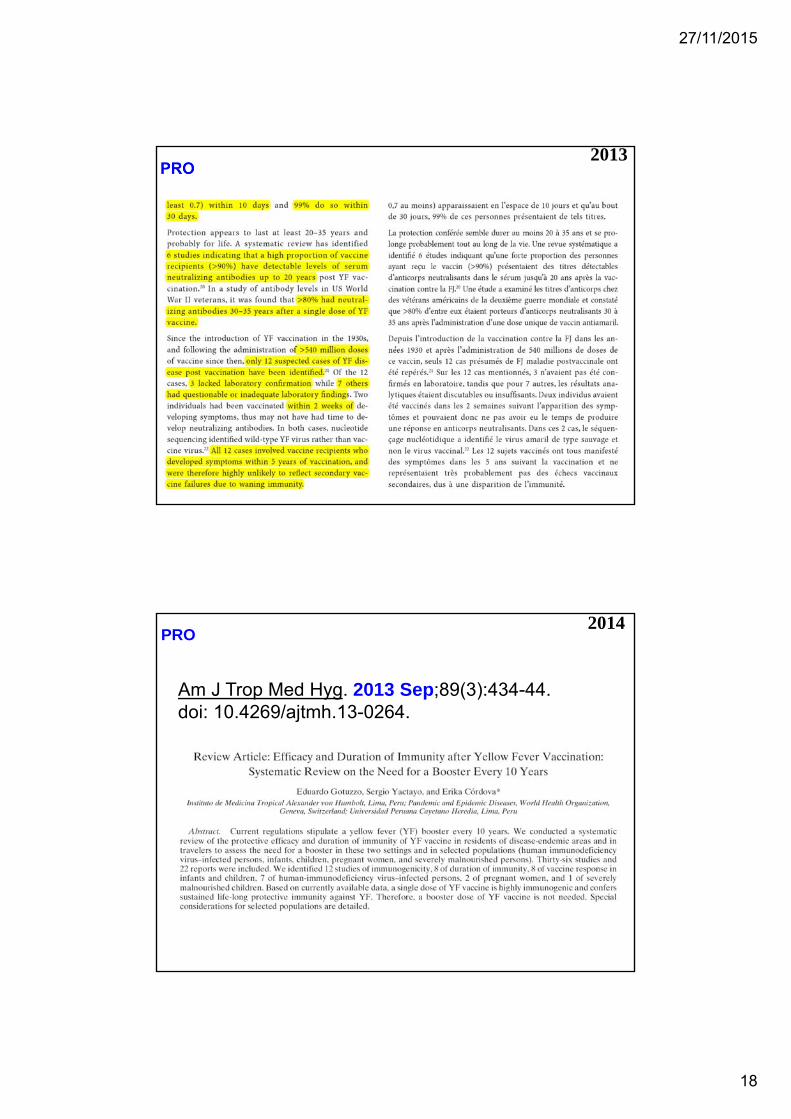
• WER 2013• AJTMH 2013
“CONTRA”( = question marks)
• Clin Microbiol Infect. 2013• Travel Med Infect Dis. 2013
2014
POSITION PAPER 05-07-2013
27/11/2015
18
2013
PRO
Am J Trop Med Hyg. 2013 Sep;89(3):434-44. doi: 10.4269/ajtmh.13-0264.
2014

27/11/2015
19
“Contra”
Clin Microbiol Infect. 2013 Oct;19(10):885-6. doi: 10.1111/1469-0691Epub 2013 Aug 8.
2014
“Contra”
Travel Med Infect Dis. 2013 Sep-Oct ;11(5):266-73. doi: 10.1016/j.tmaid.2013.08.007. Epub 2013 Sep 5
2014

27/11/2015
20
How did other countries managed this situation ?
in 2014 ? 2015 ?
2014 – 15
2015WHO

27/11/2015
21
2015
2015
27/11/2015
22
2015
2015

27/11/2015
23
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/30694/Green_Book_Chapter_35_v3_3.pdf
UK Green Book p. 447
2014 UK
2014

27/11/2015
24
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/30694/Green_Book_Chapter_35_v3_3.pdf
UK Green Book p. 447
2014
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/30694/Green_Book_Chapter_35_v3_3.pdf
UK Green Book p. 447
2015
But when ?After 2nd birth dayAfter pregnancyAfter 1 monthAfter 10 yearsBefore next travel….

27/11/2015
25
2014
ou qui ont reçu leur vaccination initiale contre la fièvre jaune: • à un âge de moins de deux ans• pendant la grossesse • avant une greffe de moelle osseuse • au cours d’une infection par le VIH • en cas d’immunodépression
FRANCE SMVe-mail de 7/5/2014
membre-smv-bounces@medecine-
voyages.fr
SWISS Tropimed®
News EpidemiologiquesJuin 2014
France & Switzerland
France BEH juin 2015
2015
France

27/11/2015
26
2015
!
USA
2015

27/11/2015
27
?
How to inform the traveler ?
he/she read on internet : “YF-vaccine is lifelong valid”
he/she is confused
2014

27/11/2015
28
How to inform the traveler ?If vaccinated more than 10 years ago and now traveling to a country for which no proofof YF-vaccination is needed : • a choice exists :
to update the vaccination or not• discuss thorougly with the client about
crossing borders, future travels, unforeseenchange of itinerary or long stop over, etc
• there is a low treshold for revaccination• let him/her make the informed choice
2014
2014

27/11/2015
29
2014
Medasso / ITG Gezondheidsadviezen voor reizigers Uitgave 2014-2015Medasso / IMT Conseils de santé pour voyageurs Edition 2012-2013
2014
Medasso / ITG Gezondheidsadviezen voor reizigers Uitgave 2014-2015Medasso / IMT Conseils de santé pour voyageurs Edition 2012-2013

27/11/2015
30
2014
We will ask WHO for a working group to work this officially out
Medasso / ITG Gezondheidsadviezen voor reizigers Uitgave 2014-2015Medasso / IMT Conseils de santé pour voyageurs Edition 2012-2013
2 Examples of pitfalls & errors
2014
There is a high risk for errors when crossing borders as was illustrated recently in some cases

27/11/2015
31
…… we heard of an ICID delegate (16th International Congress on Infectious Diseases • Cape Town,SA)
who was rightfully denied boarding by South African Airways
for the Sao Paulo Johannesburg flight
because he didn't have his International certificate of vaccination or
prophylaxis (for yellow fever vaccination) with him
and had just been in Peru for several days.
I hope this is helpful to all, remains a difficult and confusing area to keep updated on.
David O. Freedman, MD Managing Senior Director Shoreland, Inc USA
2014 From: Travel Medicine Clinical Discussion List
[[email protected]]On Behalf Of David O Freedman sent: zondag 20 april 2014 20:06
• From: Membre-smv [mailto:[email protected]] Sent: vrijdag 25 april 2014 18:46Subject: [Membre-smv] plainte
Bonjour,
Je voudrais vous faire part d'une plainte déposée par un patient à l'encontre de ma collègue du CVI, pour "défaut d'information". Cette situation doit nous rendre sans doute plus vigilant vis à vis de ces obligations administratives, totalement en décalage avec la réalité du risque encouru par nos voyageurs!
Elle voit en consultation en octobre dernier une famille :• père, mère, 3 enfants dont un bébé de 3 mois • pour un départ prévu en décembre pour 4 mois :
Cuba, Pérou, Costa Rica, Guatémala, Mexique, New York.
• Mise à jour du calendrier vaccinal, y compris BCG pour les enfants, hépatite A etc.. conseils palu, dengue, hygiène etc...une longue consultation.
En ce qui concerne la Fièvre Jaune : – elle vaccine les 2 grands, pas le bébé bien sûr, ni la maman qui allaite – pour les parents qui ont été vaccinés en 2002 elle fait réaliser une sérologie, qui
revient bien sûr positive– les 4 partent donc protégés par leur vaccination– pour le bébé elle renforce les conseils de protection anti moustiques – le risque est de toutes façons négligeable, ils ne vont pas aller en zone à risque,
en particulier pas en zone amazonienne
2014

27/11/2015
32
There is a high risk for errors when crossing borders as was illustrated recently in some cases
From: Membre-smv [mailto:[email protected]] Sent: vrijdag 25 april 2014 18:46Subject: [Membre-smv] plainte
Bonjour, Je voudrais vous faire part d'une plainte déposée par un patient à l'encontre de ma collègue du CVI, pour "défaut d'information". Cette situation doit nous rendre sans doute plus vigilant vis à vis de ces obligations administratives, totalement en décalage avec la réalité du risque encouru par nos voyageurs!
Elle voit en consultation en octobre dernier une famille :
• père, mère, 3 enfants dont un bébé de 3 mois • pour un départ prévu en décembre pour 4 mois : Cuba, Pérou, Costa Rica, Guatémala, Mexique, New York.
Hélas ! à la frontière entre le Pérou et le Costa Rica ils sont renvoyés au Pérou, doivent se faire vacciner sur place & attendre 12 jours "d'incubation" et repayer 5 billets d'avion pour revenir au Costa Rica.
Bref aujourd'hui : une lettre de plainte, une demande de contact avec l'assurance pour une indemnisation des frais engagés.
Mon analyse est : - Rien à dire sur le plan médical. - Sur le plan administratif : Certes une obligation administrative qui avait dépassé la limite de validité des 10 ans (11 ans à la date du départ...) mais en décalage avec les recommandations de l'OMS .
Il aurait sans doute fallu expliquer plus cette contrainte administrative, et faire un certificat de CI pour la maman
2014
Tip Fill in the name and date of birth
Make a scan of the yellow fever vaccination attestation
Put it in “the cloud”
2014
If a booster : when ?After 2nd birth dayAfter pregnancyAfter 1 monthAfter 10 yearsBefore next travel….

27/11/2015
33
2006 = 2015
NB. What about the “cholera stamp” in the yellow-fever-booklet (“cholera vaccine not indicated – validity indefinitely”) ? The habit of putting it on the vaccination certificate or travelers to sub-Saharan Africa should be maintained. Never needed for other regions in the world.

27/11/2015
34
Reminder about YF & MMRvaccination
2015
Vaccine 20112011

27/11/2015
35
Subjects injected YFV and MMR simultaneously had lower seroconversion rates
– 90% for rubella, – 70% for yellow fever– 61% for mumpscompared with those vaccinated 30 days apart – 97% for rubella, – 87% for yellow fever – 71% for mumps.
• Seroconversion rates for measles were higher than 98% in both comparison groups.
Geometric mean titers • for rubella and for yellow fever were approximately three
times higher among those who got the vaccines 30 days apart.
• For measles and mumps antibodies GMTs were similar across groups.
combination of measles and yellow fever vaccination 2011
• These conclusions apply to primary vaccination in children less than two years old.
• As primary vaccination against yellow fever in older children and adults, and a booster dose at any age induce stronger immune response, interference from other live virus vaccines should be less pronounced and possibly irrelevant.
2011 combination of measles and yellow fever vaccination

27/11/2015
36
POSITION PAPER 05-07-2013 2013
12-07-20132013

27/11/2015
37
CDC 2014 Simultaneous Administration of Other
Vaccines and Drugs• ACIP recommends that yellow fever vaccine be given at the
same time as other live-virus vaccines. • Otherwise, the clinician should wait 30 days between
vaccinations, as the immune response to one live-virus vaccine might be impaired if administered within 30 days of another live-virus vaccine.
• A recent study involving the simultaneous administration of yellow fever and measles-mumps-rubella (MMR) vaccines in children found a decrease in the immune response against yellow fever, mumps, and rubella when the vaccines were given on the same day versus 30 days apart.
• Additional studies are needed to confirm these findings, but they suggest that if possible, yellow fever and MMR should be given 30 days apart.
2014
2015

27/11/2015
38
Background: • The use of 2 live attenuated vaccines (LAV) is recommended
to be simultaneous or after an interval of at least four weeks between injections. • The primary objective of this study was to compare the humoral response to yellow fever (YF) and measles
vaccines among children vaccinated against these two diseases, either simultaneously or separated by an interval of 7–28 days.
Subjects and methods: • A prospective, multicenter observational study was conducted among children aged 9–15 months. • The primary endpoint was the occurrence of positive yellow fever antibodies after YF vaccine by estimating
the titers of neutralizing antibodies from venous blood samples. • Children vaccinated against YF 7–28 days after receiving the vaccine against measles (test group) were
compared with children vaccinated the same day against these two diseases (referent group).
Results: Analysis was performed on 284 children. Of them, fifty-four belonged to the test group. • Measles serology was positive in 91.7% of children. • Neutralizing antibodies against YF were detected in
– 90.7% of the test group – 92.9 of the referent group (p =0.6).
• In addition, quantitative analysis of the immune response did not show a lower response to YF vaccination when it took place 1–28 days after measles vaccination.
Discussion: In 1965, Petralli showed a lower response to the smallpox vaccine when injected 4–20 days after measles vaccination. Since then, recommendations are to observe an interval of four weeks between LAV not injected on the same day. Other published studies failed to show a significant difference in the immune response to a LAV injected 1–28 days after another LAV. These results suggest that the usual recommendations for immunization with two LAV (simultaneously or interval of 28 days) may not be correct.
Conclusion: In low income countries, the current policy should be re-evaluated. This re-evaluation should also be applied to travelers to yellow fever endemic countries.
2015 2013
CDC “2016” Simultaneous Administration of Other
Vaccines and Drugs• ACIP recommends that yellow fever vaccine be given at the
same time as other live-virus vaccines. • Otherwise, the clinician should wait 30 days between
vaccinations, as the immune response to one live-virus vaccine might be impaired if administered within 30 days of another live-virus vaccine.
• A recent study involving the simultaneous administration of yellow fever and measles-mumps-rubella (MMR) vaccines in children found a decrease in the immune response against yellow fever, mumps, and rubella when the vaccines were given on the same day versus 30 days apart.
• Additional studies are needed to confirm these findings, but they suggest that if possible, yellow fever and MMR should be given 30 days apart.
2014 = 2015

27/11/2015
39
Quid WHO ? UK ? Other countries ?
Reminder about YF vaccination
in young children
2014
27/11/2015
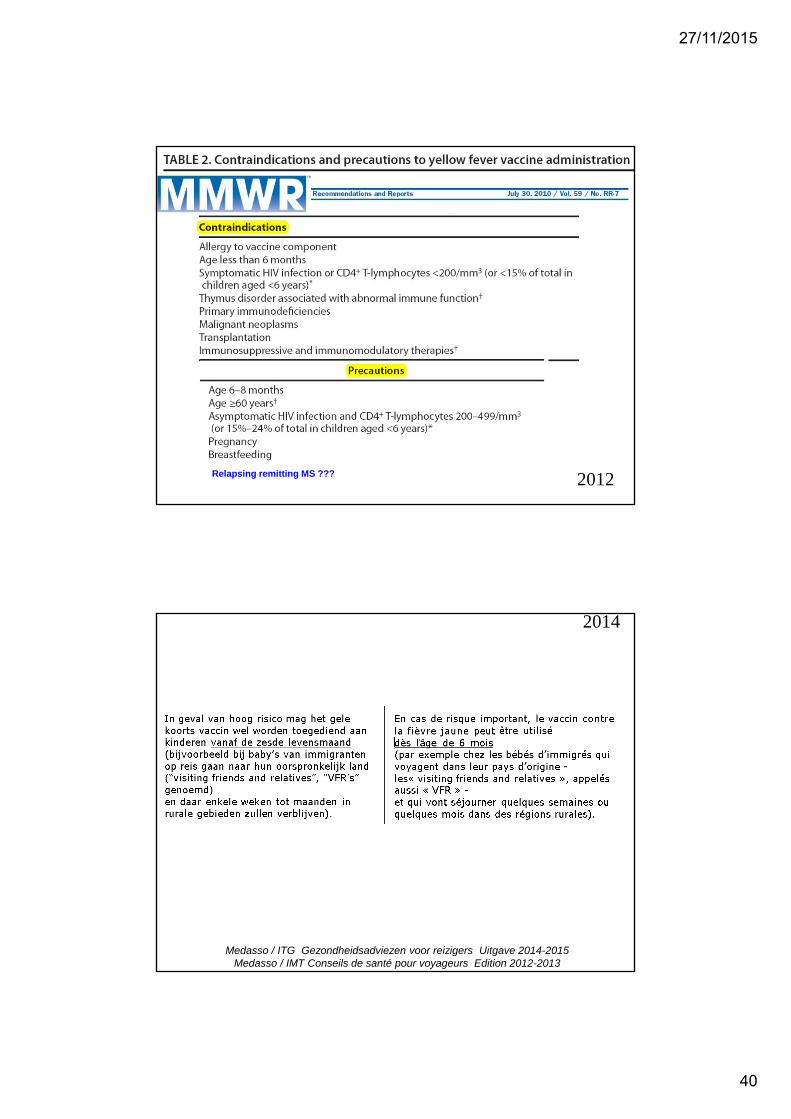
40
2012 Relapsing remitting MS ???
2014
Medasso / ITG Gezondheidsadviezen voor reizigers Uitgave 2014-2015Medasso / IMT Conseils de santé pour voyageurs Edition 2012-2013

27/11/2015
41
intervals for YF vaccination after interrupting
immunosuppressive treatment
2014
2014

27/11/2015
42
Tijdschrift voor geneeskunde – W Peetermans, H Schoemans, A Van GompelVaccinaties bij immuungecompromitteerde en chronisch zieke patiënten
references 6,10,11,12
6. Tomblyn M , Chiller T , Einsele H, et al. Guidelines for preventing infectious complications among hematopoietic cell transplant recipients: a global perspective. Bone Marrow Transplant 2009; 44: 453-455.
10. Rahier JF , Moutschen M , Van Gompel A , et al. Vaccinations in patients with immune-mediated inflammatory diseases. Rheumatology 2010; 49: 1815-1827.
“As a rule of thumb, a period of 3 months is estimated for the immune status to be completely restored (evidence Level D), except for corticosteroid therapy, where a waiting period of 1 month is thought to be sufficient (evidence Level D).”
11. Visser LG. TNF-α antagonists and immunization. Curr Infect Dis Rep 2011; 13: 243-247.
12. Visser LG. The immunosuppressed traveler. Infect Dis Clin North Am 2012; 26: 609-624.
“The duration of the immunosuppressive effect depends on
1.the half-life of the active drug component2.the recovery from the immunological effect (e.g. depleting cytotoxic effect caused by apoptosis or clonal deletion of B- or T- cells). For most immunosuppressive medications this time point has not been clearly defined”
2014
2014
Medasso / ITG Gezondheidsadviezen voor reizigers Uitgave 2014-2015Medasso / IMT Conseils de santé pour voyageurs Edition 2012-2013

27/11/2015
43
Auto-immune disease in itself is not a contra-indication for
YF-vaccination
2014
CDC – MMWR-2010 2014

27/11/2015
44
CDC – Yellow Book -2016http://wwwnc.cdc.gov/travel/yellowbook/2016/advising-travelers-with-
specific-needs/immunocompromised-travelers
Medical conditions without significant immunologic compromise …Travelers should be prepared as any other traveler
3.Travelers with a history of cancer who received their last chemotherapy treatment ≥3 monthspreviously and whose malignancy is in remission.
4.Hematopoietic stem cell transplant recipients who are >2 years post transplant, not on immunosuppressive drugs, with no evidence of ongoing malignancy, and without graft-versus-host disease.
5.Travelers with autoimmune disease (such as systemic lupus erythematosus, inflammatory bowel disease, or rheumatoid arthritis) who are not being treated with immunosuppressive or immunomodulatory drugs, although definitive data are lacking.
6.Travelers with multiple sclerosis (MS) who are not on immunosuppressive or immunomodulatory agents and those who are not experiencing an exacerbation of disease. Although the risks of using live-virus vaccines for those with MS have been debated, the National MS Society and CDC recommend following CDC guidelines for vaccination in those who lack prior immunity, who are not on immunosuppressive or immunomodulatory agents, and who are not experiencing an exacerbation of disease.
2015

27/11/2015
45
Exploring possible severe side effects
2014

27/11/2015
46
2014
Medasso / ITG Gezondheidsadviezen voor reizigers Uitgave 2014-2015Medasso / IMT Conseils de santé pour voyageurs Edition 2012-2013
2014

27/11/2015
47
2014
2014

27/11/2015
48
2014
2014
Medasso / ITG Gezondheidsadviezen voor reizigers Uitgave 2014-2015Medasso / IMT Conseils de santé pour voyageurs Edition 2012-2013

27/11/2015
49
Will the price of Stamaril be higher in the near future ?
Mail récent de la SMV-France
La discussion avec Sanofi-Pasteur-MSD (SPMSD) nous a permis d’obtenir un étalement de l’augmentation qui va s’étendre sur 3 ans selon l’échéancier ci-dessous et ne sera donc pleine que début 2017.
• 28€50 jusqu’au 1er janvier 2015 (ou mars car certains marchés se passent à ce moment)
• 32€30 jusqu’au 1er janvier (mars) 2016
• 36€10 jusqu’au 1er janvier (mars) 2017
• 38€ à partir de début 2017
2014
Travel medicine Seminar 19 /11/15 “Travel medicine Seminar 20 years later”
MILITAIR HOSPITAAL as in 1995 14.00-14.05 Introduction
14.05-14.35 Yellow fever vaccination issues CHARLOTTE MARTIN
14.35-15.05 The last-minute traveler: an update on accelerated vaccine schedulesPATRICK SOENTJENS
15.05-15.25 Epidemiologic flashes & edge cutting news / new vaccines STEVEN CALLENS
15.25-16.00 Coffee break
16.00-16.25 Travellers diarrheaLUCIE SEYLER
16.25- 16.50 Malaria: when prevention is not clear-cutULA MANIEWSKI
16.50-17.15 Traveller's ThrombosisPETER VERHAMME
17.15-17.45 What did change (drastically) in the last 20 years in travel medicine ? FONS & YVES
Have a look at http://www.sbimc.org for the pdf’s of the powerpoints of all the lectures since 2009

27/11/2015
50
End Yellow Fever
2014