mastering resuscitation gizmos and gadgets: the …
TRANSCRIPT

MASTER ING RESUSCITAT IONGIZMOS AND GADGETS:The Importance of Education
• Never Skip a Beat: Training with Mechanical CPR
• Cooling Patients in a Critical Situation
• CPR Training on the Patient: Real-time Feedback
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 1

Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 2

1
C O U R S E I N T R O D U C T I O N / A T T E S T A T I O N
Intended AudienceThis course is for emergency physicians, paramedics, EMTs, nurses, and otherhealthcare professionals who may be interested in new developments in CPR.
Original Release: 07/2010
This course is not designated for continuing education credit.
Commercial Support AcknowledgmentThe development of this activity was supported in part by a grant from ZOLLMedical Corporation.
Statement of Need CPR guidelines have been changing rapidly, with greater emphasis on maintaining acorrect frequency and sufficient depth of chest compressions. In order to assist withthis need, new products have been developed to deliver chest compressionsautomatically or to provide feedback to help rescuers maintain effective frequencyand depth. In addition, there has been a new emphasis on lowering the bodytemperature of a cardiac arrest patient in order to help prevent post-cardiaccomplications.
The purpose of this program is to present the practical experience of severalemergency services concerning these three developments.
OverviewThis course will present three articles covering the practical experience of threeEMS units in the use of a load distributing band automated CPR chestcompression device; the use of a CPR feedback device; and the use of therapeutichypothermia in cardiac arrest patients.
Author/ReviewersMedcom, Inc. is the corporate author of this educational activity. Content reviewand validation was provided by Dr. Ann Weaver and James Rouse, Dr. MichelFries, and Dr. A. Bohn.
DisclaimerAs in all educational activities, we encourage the practitioners to use their ownjudgment in treating and addressing the needs of each individual patient, takinginto account the patient's unique clinical situation. Medcom disclaims any liabilityand/or loss resulting from the information contained in this activity. The learnerspecifically agrees to indemnify and hold Medcom, the creators, producers, anddistributors of this activity harmless against any and all claims or liabilities arisingout of the use of any information provided in this activity by the learner, or byanyone directly or indirectly obtaining such information through the learner.
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 1

N E V E R S K I P A B E A T : T R A I N I N G W I T H M E C H A N I C A L C P R
Anne Weaver, MD, Consultant in Emergency Medicine and Prehospital Care,London Air Ambulance, HEMS, UK; and James Rouse, Paramedic, London AirAmbulance, HEMS, UK
Learning ObjectivesAfter completing this section, the learner should be able to:
• Describe some of the difficulties of performing CPR in a field situation
• Describe the benefit of a non-invasive cardiac support pump
• Describe a method of rapidly preparing a patient for CPR
• Discuss the importance of training and monitoring performance
IntroductionThe London Metropolitan Area contains about 11 million inhabitants, roughly thesame metropolitan area as Cologne or Paris; some of the most crowdedmetropolitan areas in Europe.
The London Helicopter Emergency Medical Service (HEMS) flies out about fiveto six times a day to treat trauma cases, and has a fleet of cars which also respondto trauma. This article will examine the rescue service's experience with amechanical device to treat patients in cardiac arrest – a load-distributing band(LDB) non-invasive cardiac support pump.
Each vehicle of the HEMS servicecarries a doctor and a paramedic.They work in close relationship withthe London Ambulance Service,which has a variety of vehicles fromrapid-response cars to standardambulance trucks, motorbikeparamedics, and a cycle response unit.
The physician response unit, just like the aircraft, carries an experienced doctorwho is a senior registrar or consultant in emergency medicine or anesthesia.Alongside the doctor, there will be a paramedic who will have worked for theLondon Ambulance Service for a significant period of time. Response times are, onaverage, below 8 minutes and the maximum is about 10 minutes to get to anyevent in the area.
2
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 2

Responders adhere to the standard ALS Guidelines, currently from 2005. Theservice carries adjuncts to help resuscitate patients. For example, they carry animpedance threshold device and a manual axis compression/decompression device.Therapeutic hypothermia is also induced during resuscitation and transport withthe use of cold saline at a dosage of 30 ml per kilogram at 4°C.
Even with adherence to ALS Guidelines and some extended ALS procedures, thedirectors of the service felt improvement was possible. London Ambulance Serviceachieves a return of spontaneous circulation ( ROSC) in approximately 25% ofcases and overall survival is around 12%. While these figures are better than mostlarge cities, it was felt the service could do better.
Problems Of On-Scene Cardiac ResponseThere are many difficulties encountered in trying to perform effective manual CPR.
In the back of an ambulance traveling between 20 and 50 miles per hour, theacceleration forces, deceleration forces, sideward forces going around cornerscontribute to ineffective manual chest compressions throughout the ambulancejourney, just when the patient most needs effective compressions.
In addition, variations in performance of chest compressions, which depend onmany human factors, have been well documented. The rate, depth, and releasevary widely. There are also factors of fatigue and distraction, and the delays whenswitching to a different provider. Another major problem, when out of hospital, isthe limited numbers of resources on scene when the first paramedic or technicianarrives. Sometimes space is confined.
Transfer to the vehicle might add 30 seconds or possibly a minute, a period typicallywithout chest compressions, which is not acceptable. This is then coupled with therelatively ineffective compressions for the drive time that can be up to 8 to 10minutes. On arrival, there's another transfer off the ambulance into the emergencydepartment, and then onto a bed. With all these factors added together, too muchtime is spent without effective chest compressions.
Strategy And TrainingIn June 2008, the service decided on a new strategy to produce early and consistenthigh-quality CPR. First, they added an experienced doctor in the car accompaniedby a paramedic, with the doctor having the skills to perform early interventions onany reversible causes of cardiac arrest. Also the service added use of a load-distributing band non-invasive cardiac support pump to maintain consistenteffective compressions, along with the other interventions already in place.
3
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 3

4
With the new strategy, it was felt that many of the pre-hospital problems werepredictable and, indeed, staff could be trained for them. Staff needed explicitinstructions for what to do under various circumstances. Appropriate training andappraisal for team members was essential.
First, standard operating procedures were developed for virtually everycircumstance, including how to get on and off the helicopter, how to pack the bag,how to do checks, and how to deliver quality CPR.
It was thought important for the team to understand the background for adoptingthe chest compression device, and also to understand the importance of qualityCPR. A study day was arranged where staff looked at actual cases, appraised theliterature, asked questions, and had focused training on the non-invasive cardiacsupport pump.
After the study day, a simulation day was scheduled. The simulation training wasarranged to be as realistic as possible. The mannequins were placed in the kind ofenvironment that a cardiac patient might be found: on the floor, outside in thewind where everyone is slightly uncomfortable. Technicians from the manufacturerwere present to demonstrate or assist. And when the service actually went live withthe equipment, they were given real-time support from the manufacturer's team tohelp with the implementation.
To keep the training realistic, it beganwith either a first responder, a member of the public, or a London AmbulanceService crew. Therefore, the scenarioincluded a handover and practiceputting on the chest compressiondevice rapidly, while someone wasdoing manual chest compressionsalready, interfering as little as possible.
To help keep things realistic, themannequins were fully clothed. Teamswere therefore realistically trained inhow to cut the clothes off quickly, getthe patient onto the backboard, andexpose the chest for the electrode pads.
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 4

5
The fastest team managed to do it in 15 seconds; however, it was consistently donein 19 or 20 seconds following a method developed in the ambulance service inRichmond, Virginia, USA. In this method, the crew first cuts down the back ofthe patient’s clothes, lays the patient on the board, and pulls the clothes off fromthe front.
The training session worked with the same equipment that they would use on alive patient, the same monitor, the same intubation pack, the same medical drugspack to keep things as realistic as possible.
Local ambulance crews were invited tocome and witness the simulations,particularly the use of the load-distributing band non-invasive cardiacsupport pump. In addition, thescenario was run in real time, so therewas no stopping for explanation ofhypothetical activity– such as "Here wewould put a cannula in." The teamactually obtained a cannula out of thepack; put it into the arm, etc. In thisway everyone could see how long itactually took.
Routine Training Is Also Critical Every member of the staff, no matter how senior, goes through a training monthwhen they're supervised on every mission and they learn a lot of detail about everypiece of equipment: how to maintain it, look after it, and how to use it well. Inaddition, there are twice-weekly case reviews to go over the physiology and theclinical care delivered to the patients.
There is also a month-long audit process to look at the performance from the timea 999 call is taken. The calls themselves are assessed to make sure that the resourceis dispatched as soon as possible. Then the entire treatment cycle is monitoredagainst key performance indicators until the patient is delivered to definitive care.The service is in the process of developing a database to record all of these CPRissues, including the use of automated devices such as the cardiac support pump.
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 5

Field Use Of The Non Invasive Cardiac Support PumpOur actual experience using the chest compression device in the pre-hospital fielddemonstrated that it can be put on within 19 seconds. The device automaticallyimproves the consistency of compressions. The support pump doesn’t get fatigued;it doesn’t get distracted; it just keeps compressing the chest from the time you putit on until you turn it off in the resuscitation room.
The load-distributing band non-invasive cardiac support pump eliminated theproblems we had in the past–variations in chest compression, the fatigue and thedistractions, and doing CPR in confined spaces, and also the difficulties of CPRduring transfer.
ConclusionIn summary, training isn’t as simple as just learning to use devices. It’s important tohave a dedicated team who understand the rationale for introducing a new piece ofequipment. It’s also important to have a clinical governance structure to maintainthe training and audit the use of the devices. And training and education has to becontinual. It has to be repeated even for permanent members of staff.The team hopes that ultimately their approach will end up the standard for cardiacarrest care for East London; and maybe be rolled out across the city.
6
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 6

7
C O O L I N G P A T I E N T S I N A C R I T I C A L S I T U A T I O N
Michael Fries, MD, Chief Medical Director, Department of Surgical IntensiveCare, University Hospital Aachen, Germany
Learning ObjectivesAfter completing this section, the learner should be able to:
• Describe post-cardiac arrest problems and their affect on mortality rates
• Describe the effects of hypothermia in post-resuscitation care
• Describe some methods of cooling a patient
IntroductionThis article will discuss the value of cooling patients in critical situations.
Cardiac arrest / ventricular fibrillation are the most critical conditions a patient canface. With no cardiac output the blood supply to the tissues begins to stop withinminutes. Studies of the cerebral microcirculation of pigs after cardiac arrest haveshown that some vessels are still carrying flow even after 20 or 30 seconds becausearterial and venous pressures equalize over a long period, giving about a 5 minutewindow before flow stops entirely i. Good quality CPR is necessary to restart ormaintain the blood flow and allow for effective defibrillation. However, we arelearning that restoration of circulation is only the beginning of resuscitation.
Long-Term Post-Cardiac MortalityPatients that are resuscitated in Europe still have a high mortality rate, typically a10 to 15 percent survival rate.
Our group conducted aretrospective study of cardiacarrest from Aachen, which is asmall city near the border withBelgium and the Netherlands,about 50 kilometers fromCologne. In this study,resuscitation was attempted on250 patients and ROSC wasachieved in 45 percent, yetonly 14% of the patients weredischarged, though most had agood neurological outcome.ii
Outcomes
n= 66(45.2) 64(44.8) 12(36.4)
GER NL B
n= 19(13.0) 17(9.1) 4(12.1)
Any ROSC
Neurologic Outcome at Discharge
YES
NO
Survived event
Discharged alive
CPC 1 or 2
CPC 3 or 4
CPC 5
n= 80(54.8) 79(55.2) 21(63.6)
n= 60(41.1) 59(41.3) 10(30.0)
n= 21(14.1) 19(13.3) 4(12.1)
n= 2(1.4) 0(0) 0(0)
n= 114(78.1) 105(73.4) 24(72.7)
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 7

8
Why do only 15 percent, overall, survive? In general, cardiac arrest produces something that we call ischemic reperfusioninjury. There is a breakdown in Adenosine Tri-phosphate (ATP); the sodiumpotassium transport channels are disrupted and free-radicals are generated. All thatleads finally to cell changes which end up in apoptosis or necrosis – permanent celldeath. This very complex pathway is shown below.
Lipton 1999 Physiology Review iii
In patients suffering cardiac arrest, this condition is now known as post-cardiacarrest syndrome, though it was originally described 25 years ago by Dr. VladimirNegovski, the famous Russian expert in resuscitation.. These micro-vascularalterations, inflammatory response, and other problems all lead to organdysfunction, mainly post-resuscitation myocardial and cerebral dysfunction.
Induction of Long-Term Functional Damage
Initiators and Activators Perpetrators1 2 3
Gene ActivationGlutamate
Cai Nitric Oxide
Δ Proteins & Phospholipase
Activity
Free Radical Action &
Peroxynitrite
Free Radicals
Gene Activation
Free Radicals
? Map Kinase
Cai
Cai
e”Transport”
? Δ Carriers
Glycolysis pH1ATP
-O2
-O2
Phospholipase FFA
ATPe”Transport”
ATP
pH1
Na/K ATPase
Membrane Depot-O2
ATP
NaGlutamatePNa
GlutamateNaMembrane Depot
Membrane Depot
Cai
Protease Activity
(Calpain)
Na/K ATPase
PNaMembrane DepotATP
Membrane Depot PK
Proteolysis
Phospholipase Activity
Phospholipid Changes
ATPPAF
CaiPhospholipase A2
Cai
Free Radicals
ATP-O2
Na
Nitric OxidePeroxynitrite
PolyADPribose PolymeraseFree Radicals
Pathways of Ischemic Cell Death
Cell Death End Stages
Critical Functional & Structural Changes
4 5
Membrane Permeability
Na/K ATPase
ProteinSynthesis
Mitochondrial Dysfunction
Prolonged Changes in Kinases or Phosphatases
Cytoskeletal Damage
Edematous Cell Change
ApoptoticCell Change
Autophagocytotic Cell Change
Ischemic Cell Change
Homogenizing Cell Change
Pathways of Ischemic Cell Death
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 8

9
We now know medicine can do much better than a 15% survival rate. Sunde andcolleagues from Oslo looked retrospectively at data from the periods before andafter hypothermia intervention was developediv. In the first group, 68 patients werestudied and 31% survived. In the later group, just after implementation oftherapeutic hypothermia — 69 patients were admitted; and in this group, theyalmost doubled the survival rate.
Aggressive Interventions Drives SurvivalWhy did they double the survival rate? Most of the variables were the same –gender distribution, time for the ambulance to arrive, initial rhythm, etc. Thedifference was a very aggressive intervention protocol which included thefollowing:
• Primary coronary intervention (PCI) to fix the underlying cause of thecardiac arrest was undertaken in 30 patients in the intervention period
• Therapeutic hypothermia was induced in all comatose suvivors
• They gave more inotropic agents and used an intra-aortic balloon pump withpatients with cardiogenic shock
• They gave more fluids and maintained tight glucose control
Table 1: Univariate analysis of prognostic factors and outcome data for patients admitted to ICUof Ulleval University Hospital in the control (1996-1998) or intervention (2003-2005) periods, presented as absolute numbers (percentage) or median values with interquartile range
Control period (n = 58)
Intervention period (n = 61)
p-ValueOR (95% CI)
46 (79)28 (48)55 (95)43 (74)49 (84)6 (4-9)18 (13-22)52 (90)33 (57)2 (1-5)4 (3-6)18 (31)15 (26)15 (26)
50 (82)43 (71)60 (98)43 (71)55 (90)6 (4-8)18 (10-27)52 (85)36 (59)2 (1-5)5 (2-8)34 (56)34 (56)34 (56)
1.2 (0.5, 2.9)2.6 (1.2, 5.4)3.3 (0.33, 32.4)0.8 (0.4, 1.9)1.7 (0.6, 5.1)
1.2 (0.5, 2.8)1.1 (0.5, 2.3)
2.80 (1.32, 5.93)3.61 (1.66, 7.84)3.61 (1.66, 7.84)
0.890.0220.360.810.510.700.980.650.820.70a
0.490.0070.0010.001
Two sided p-values for continuous variables from Mann-Whitney rank sum test. a
a
a
a
MaleAge <70WitnessedBystander CPRInitial VFAmbulance response time (min)Time to ROSC (min)Comatose on admissionMyocardial infarctionMechanical ventilation (days)Stay at ICU (days)Survival to dischargeFavourable outcome (CPC 1-2)1-Year survival
Control period (n = 58)
Intervention period (n = 61)
p-ValueOR (95% CI)
2 (3)029 (50)031 (53)2300 ± 12114 (7)
30 (49)40 (66)43 (80)8 (15)03455 ± 159427 (44)
27.0 (6.06, 121.09)n.a.2.39 (1.13, 5.08)n.a.n.a.
10.72 (3.45, 33.33)
<0.001<0.001 0.022 0.006a
<0.001<0.001<0.001
b
a
Reperfusion treatmentTherapeutic hypothermiaInotropic agentsIntra aortic balloon pumpGlyceryl trinitrateFluid balance 1st day (ml)Insulin
a
a
a
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 9

In essence they treated them as potential survivors. This is only one example of onevery dedicated city, but it shows what can be done, resulting in a 56% survival todischarge - all neurologically intact. In 2008, in Circulation and Resuscitation, anILCOR Consensus Statement about the pathophysiology of cardiac arrest andwhat can be done to prevent post-cardiac arrest syndrome, was issuedv. It providesclinicians with guidance in managing patients post arrest – something hopefully weare all doing today. The Chain of Survival now needs another link, post-resuscitation care.
One key intervention employed in Oslo wastherapeutic hypothermia and its use hasbecome much more common.
Temperature control is important. EvenNapoleon's surgeon-general, Baron JeanDominique Larrey recognized this severalhundred years ago. He made a very interestingdiscovery. When he was putting his patients infield hospitals where he had a tent with anoven in the middle, survival rates were muchlower in patients near the oven.
In Düsseldorf, German cardiothoracic surgeons were doing cardiac surgery beforethe era of the heart-lung machine, by cooling patients 15 to 18 degrees C in an icebath, which gave them a window of about 10 to 15 minutes time to open thechest, do a small procedure, and then close it again.
10
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 10

The first case of the use of hypothermia after cardiac arrest was reported byWilliams et al at Johns Hopkins in Baltimore, Marylandvi. Four patients werestudied and they were put on hypothermia, 32 to 34 degrees C, lasting for up to72 hours. They discovered that the neurological deficit was only mild or moderatein those victims after cardiac arrest.
This piqued their interest and they went on to study the phenomena. Williams etal reported on a study where they subjected dogs to ten minutes of cardiac arrestwith and without hypothermia. The percentage of recovery was significantly higherin those dogs that received hypothermia.
The late Peter Safar was the father of therapeutic hypothermia in the setting ofcardiac arrest. He was instructing people 40 years ago to support recovery by usinghypothermia after the cardiac arrest had been successfully treated.
The largest trial of hypothermiaafter cardiac arrest was the HACAtrial conducted in Viennavii. Morethan 120 patients in each of twogroups were studied. As is wellknown today, the survival rateswere much better in those patientswho received hypothermia aftercardiac arrest.
Table 1
1 2 43
Jan. 19575 yr. C. M.
Bronchogram5 minutesSevere32-34˚C. 72 hoursNone
Aug. 19579 yr. C. F.
Asthma5 minutesSevere30-32˚C. 24 hoursNone
Sept. 195738 C. M.
Stab wound5 minutesSevere32-33˚C. 48 hoursNone
Nov. 195739 C. F.
Stab wound5 minutesSevere32-34˚C. 72 hoursModerate
DateAge
Cause of arrestDuration of arrestNeurologic damageHypothermia: RangeDuration Residual neurologic defect
Case Number
Table 2
Number of Experiments Percentage of Recovery
1212
25%83%
NoneHypothermia 32-34˚C. 18-36 hours
Treatment
0
25
50
75
100
Hypothermia
Normothermia
Surv
ival
(%)
50 100 150 200
Days
0
11
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 11

One year later, the ILCOR issued an Advisory Statement in which they suggestedthat unconscious adult patients with spontaneous circulation after cardiac arrestshould be cooled to 33 to 34 degrees C for at least 12 hours when the initialrhythm was ventricular fibrillation; but they also suggested that it might be usefulto use in other rhythms because you could argue that the brain doesn’t care whythe heart was arrested.
New Aspects Of Mild Therapeutic HypothermiaThe delivery of hypothermia is an evolving procedure – and there are a number of questions to be answered. Is timing a critical issue? What method should beused to cool the patient? Are there other indications for the use of therapeutichypothermia?
In an animal study, Boddicker and colleagues subjected swine to different degreesof cooling and then cardiac arrest was experimentally inducedviii. One groupremained normothermic; one group received mild therapeutic hypothermia;another moderate hypothermia; and another one severe hypothermia. Cardiacarrest was then induced byventricular fibrillation; and thenelectric shock was given beforeCPR was begun.
The percentage of first shockssuccess was significantly higher inthe group that had moderatehypothermia, around 33 degrees C.That means cold hearts start betterthan warm hearts. You can also seethat ROSC rate was higher in thoseanimals that were cooled to 33 degrees C.
12
0
2
4
6
8
Swin
e A
chie
ving
RO
SC
Normothermia MildHypothermia
ModerateHypothermia
SevereHypothermia
Animal Condition
1
3
5
7#
0
20
40
60
80
100
% F
irst S
hock
Suc
cess
Normothermia MildHypothermia
ModerateHypothermia
SevereHypothermia
Animal Condition
10
30
50
70
90*p < 0.05 vs. Normothermia
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 12

13
This study might not beapplicable to a clinicalscenario because, of course,no one cools patients beforecardiac arrest; but what aboutcooling intra-arrest?
Becker and Abella conductedanother interesting study inmice, in which cardiac arrestwas induced, and theventricular fibrillation wentuntreated for 8 minutesbefore CPR was attemptedix.In that period, the animalswere randomized to threegroups. One wasnormothermic; another onehad intra-arrest hypothermia— which means 2 to 3minutes before CPR the animals were cooled down; and the last group had post-arrest hypothermia instituted 20 minutes after arrest. The end points were survivaland neurologic dysfunction.
What they discovered is that the survival rate was significantly higher in thoseanimals that were cooled intra-arrest when compared to the animals that receivednormothermia or had a 20 minute delay in instituting hypothermia. This isremarkable because 20 minutes is a very short delay to institute mild therapeutichypothermia.
0
2
4
10
Ani
mal
s Su
rviv
ing
Normothermic Control
Time (hours)
6
8
Post -ROSC Cooling
Intra -Arrest Cooling
0 6 18 72
(6/10)
(1/10)
A. 6 Hours
Group
0
4
8
Neu
rolo
gic
Func
tion
Scor
e
12
1 2 3
6
10
2
B. 18 Hours
Group
1 2 3
*
C. 72 Hours
Group
1 2 3
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 13
When they were looking at neurological dysfunction, they could also demonstratethat the neurologic function score was significantly better in those animals whohad intra-arrest cooling. One problem in analysis was that in the other groupsthere were only a few animals that actually survived.
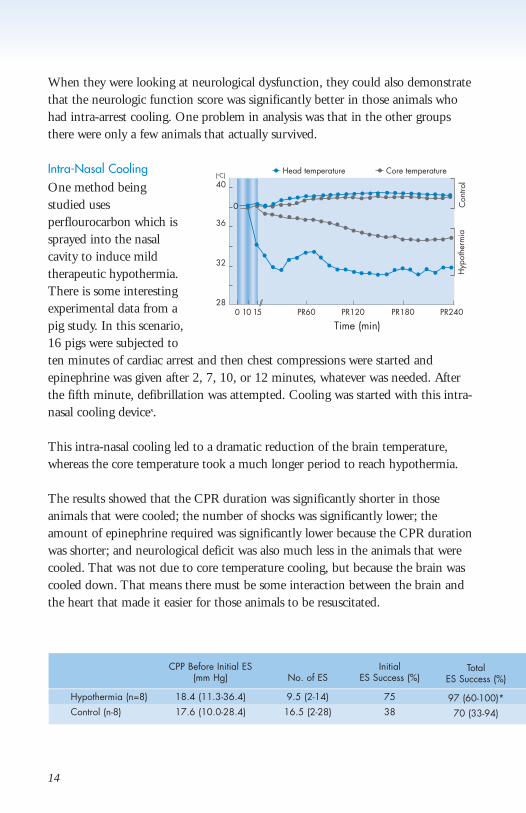
Intra-Nasal CoolingOne method beingstudied usesperflourocarbon which issprayed into the nasalcavity to induce mildtherapeutic hypothermia.There is some interestingexperimental data from apig study. In this scenario,16 pigs were subjected toten minutes of cardiac arrest and then chest compressions were started andepinephrine was given after 2, 7, 10, or 12 minutes, whatever was needed. Afterthe fifth minute, defibrillation was attempted. Cooling was started with this intra-nasal cooling devicex.
This intra-nasal cooling led to a dramatic reduction of the brain temperature,whereas the core temperature took a much longer period to reach hypothermia.
The results showed that the CPR duration was significantly shorter in thoseanimals that were cooled; the number of shocks was significantly lower; theamount of epinephrine required was significantly lower because the CPR durationwas shorter; and neurological deficit was also much less in the animals that werecooled. That was not due to core temperature cooling, but because the brain wascooled down. That means there must be some interaction between the brain andthe heart that made it easier for those animals to be resuscitated.
14
Head temperature Core temperature
0 10 15 PR6028
32
36
40
0
(oC)
PR120 PR180 PR240
Time (min)
Hyp
othe
rmia
Con
trol
CPP Before Initial ES Initial(mm Hg) No. of ES ES Success (%)
Hypothermia (n=8) 18.4 (11.3-36.4) 9.5 (2-14) 75
Control (n-8) 17.6 (10.0-28.4) 16.5 (2-28) 38
TotalES Success (%)
97 (60-100)*
70 (33-94)
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 14

15
Other Methods Of CoolingThere are different devices onthe market with differenttechnologies for coolingpatients: some devices usecold fluids that are circulatedthrough blankets. Otherdevices use cold air. And wehave one device which usesan intravascular system tocool down the patients.
There are also the poor-man’s methods–ice bags, orice-cold saline to infuse, andcooling fans.
A study just published lastyear on the effect ofdifferent cooling devicesxi.They were actually lookingat the rate of cooling andthe accuracy of maintainingthis target temperature onceit was reached. Withconventional methods and with the cold-air method (CC), the rate of cooling isnot very fast – 0.5 degree Celsius per hour and this is a problem. The other systemswere faster and did not differ greatly from each other in the rate of cooling.
The difference was in the control of temperature once the target was reached. Inthis group, the intravascular system (CG) was much more effective in keeping thistemperature at the stable level once it was reached.
Epinephrine NDS at 48 h(ug/kg) After ROSC
30 (30)* 0 (0-75)*
60 (30-120) 400 (0-400)
0.0
0.5
1.0
1.5
2.0
2.5
Hypothermia Normothermia
Conventional
o C/h
BR CC AS CG
0
20
40
60
80
100
120
140
Hypothermia Normothermia
Conventional
% o
f tim
e ou
t of r
ange
BR CC AS CG
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 15

Lack Of ImplementationIn Germany, the use of mild therapeutic hypothermia is not extensive. A surveyfrom 2008 showed that only 23% of all the ICUs studied are using itxii. More than75% are not using it because they lack experience, and to some degree, they mayfeel the methods are not yet evidence-based.It is more common in university-based hospitals. Larger ICUs often do moretherapeutic hypothermia. Internal medicine physicians do it more often thananesthesiologists.
All this raises an important question: Why are we not using a technique that weknow works? That’s a big issue in medicine in general. There are several barriers togetting a new technique implementedxiii. One is organizational context andeconomics. The technique may not be reimbursed. Or there is simply resistance toanything new. Also, of course, there are professional problems because manyproviders simply don't know about it.
The various factors cited are shown below:
16
Practice environment (organizational context)
Financial disincentives – e.g., lack of reimbursementOrganizational constraints – e.g., lack of time and staffPerception of liability – e.g., risk of formal complaint if usedPatient and relative’s expectations – e.g., no expressed wishes related to use
Prevailing Opinion (social context)
Knowledge and attitudes (professional context)
Standards of practice – e.g., usual routines differentOpinion of leaders – e.g., key persons not agreeing with evidenceMedical training – e.g., obsolete knowledge, no updateNo advocacy – e.g., by commercial companies not existent
Clinical uncertainty – e.g., benefit for this subgroup not provenNo sense of competence – e.g., not enough confidence in the skills neededNo compulsion to act – e.g., no need to do anything (new)Information overload – e.g., inability to appraise evidence
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 16

17
Other Applications For Mild Therapeutic HypothermiaUse of hypothermia is not limited to post cardiac arrest –we are finding it effectivein hypoxic ischemic encephalopathy in neonates, traumatic brain injury, andmyocardial infarction, just to name a few.
There is an interesting study that was performed in Europe by Gluckman andcolleaguesxiv. It was a multi-center trial on neonates who had hypoxia, ischemiaafter their delivery. They were randomized to two groups, one of which receivedstandard treatment and the other received head-cooling in combination withsystemic cooling. Disappointingly, there was little difference overall in survival orneurologic dysfunction. Then, they did a sub-analysis and looked at a subset inwhich EEGs were performed on the neonates. In one group of 172 withintermediate EEG changes, they found that there was a significant difference inthose who were cooled. They were doing better than the ones that receivedcontrolled treatment.
There is another famous study from Guy Clifton about cooling after traumaticbrain injuryxv. This was a large study, almost 370 people randomized to cooling orto normothermia after traumatic brain injury. Again there was no difference in thenumber of patients with poor outcome or in the number of patients who died.There were some issues with this study because there was a very long delay beforecooling was initiated. The study has been refunded by NIH and it's being redone.
Some researchers have suggestedthat what is good for the brainmight be good for the heart,too. There was some interest inthe late 1990s and the early2000s to see if cooling heartsdown after a myocardialinfarction would improveoutcomes. A small study, fromDixon et al looked at a group of42 patients, with ST segment
40 (48%)24 (29%)7 (12%)
58 (66%)34 (39%)15 (28%)
0.020.200.03
Died or severe disability at 18 monthsDied Severe neuromotor disability
Intermediate aEEG group, n=172
Cooled Control p value
05
10
15
20
25
30
35
40
4550
Infa
rct S
ize
at 3
0 D
ays
(%LV
)
Controln=18
Coolingn=18
TIMI 0-1TIMI 2-3
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 17

elevation myocardial infarction, randomized to either normothermia orhypothermia before primary PCI was performedxvi. They used an intravascularcooling device in these patients and cooled them down very rapidly from 36 degreesC to almost 34 degrees C within 30 minutes. They then continued cooling postintervention for 3 hours. They did their intervention, and then looked for adverseevents. Did the cooling do harm? They looked at the infarct size one month later.The study showed that cooling was very safe.
Unfortunately, there were no statistical differences in the infarct size. Still thisapproach was, for a period, very aggressively used.
The final results aren't in, but there is more to come. There are approximately ahundred other studies of hypothermia under way.
ConclusionMild therapeutic hypothermia is a safe therapy in various settings of ischemicperfusion injury. It definitely improved survival and neurological outcome aftercardiac arrest in adults, and also in neonates with hypoxic ischemicencephalopathy. More studies are underway to discover other areas wheretherapeutic temperature many be a key factor in improving outcomes.
18
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 18

19
C P R T R A I N I N G O N T H E P A T I E N T : R E A L - T I M E F E E D B A C K
Andreas Bohn, MD, Medical Director Emergency Services, Münster, Germany
Learning ObjectivesAfter completing this section, the learner should be able to:
• Describe one of the main problems with CPR
• Describe the appropriate rate and depth of effective chest compressions
• Describe the kinds of feedback that devices can provide
Introduction Münster, Germany is a city that has a 280,000 inhabitants and the city EMS servicetakes about 20,000 BLS calls and 6,000 ALS calls annually. We employ 250firefighter EMTS and 50 doctors in our service. Given all the reports on both theimportance of good quality CPR as well as the problem of providing high-qualityCPR, we undertook a program with Münster EMS to determine how best toimprove CPR performance. By law, all EMTs receive 30 hours of training everyyear – and it was decided to test during training whether feedback could helpimprove CPR quality, and also to determine what kind of feedback to use.
During the annual winter training of 2005, 100 teams were given different scenariosall of which involved performing 10 minutes of optimal basic life support CPR andvarious feedback devices were tested. We also measured CPR performance with nofeedback. Without reviewing all the tests and devices, the following table shows theperformance without feedback and with a visual feedback device and metronome.
In tests with a visual feedback device, and a metronome, the EMTs succeeded inproviding chest compressions at the right rate, 100 per minute. Without thefeedback, they were often delivering chest compressions far too rapidlyxvii.
Rate, of course, is not the onlyissue. Depth is also important.We defined good compressionsbased upon a study by Suttonet al in which compressions areconsidered effective if 70% ofthem are delivered to a depthof 38-51 millimeters, with thehands in the correct positionover the sternumxviii. Withoutfeedback, only 44% of theteams were successful in
115
101
80
90
100
110
120
No Feedback
Rate of Compression/min.
CPR Feedback
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 19

20
delivering good chestcompressions; but with anaudiovisual feedback systemcoaching to the correct depth,92% of the teams succeeded indelivering good chestcompressions.
Following the testing, the servicechose what appeared to be themost effective feedback devicefor our needs, the ZOLL® AEDPro®. It was small, notexpensive, and effective. The device also has an element to minimize interruptions.Whenever there’s a pause of more than 10 seconds the device says, “Start CPR,” inorder to try to minimize no-flow time.
In the 2006 training, all the EMTs and doctors were trained on the use of the deviceand the feedback.
After training, this device was rolled out for live patients, and so far 350 patients inthe Münster City area with cardiac arrests have been treated with this feedbacksystem. The results have been highly satisfactory.
StatisticsThis is Münster CPR data, from theGerman National Resuscitation Registry.The incidence of cardiac arrest in the areais comparable to that of other areas and tointernational studies that have been madein similar areas: approximately 54 arrestseach year per 100,000 inhabitants. Theaverage age is 69 years old. The Münsterservice achieves ROSC in nearly 50 percentof its cases; and those patients withfibrillation or a shockable rhythm will bedelivered successfully to the emergencydepartment 71% of the time. Responsetime is within 8 minutes in 90% of the cases.
44%
92%
0
20
40
60
80
100
No Feedback
Good Compressions
Perc
enta
ge
CPR Feedback
Münster CPR-Data
CA incidence/100.000/ y. 54
Age (mean in y.) 69
ROSC to ED all cases (%) 48
ROSC to ED VF/VT (%) 71
Bystander CPR (%) 28
Response within 8 min (%) 90
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 20

21
Real-time feedback is of great value. Our data shows that the time withoutcompression decreases during the resuscitation attempt. The delays at first areaccounted for by getting things organized and securing the airway, but then the datashow that after minute 1 to 3, the frequency of chest compression is optimal and thechest compression depth is over 4 centimeters in 80% of the cases. This continues upto nine minutes. The table also shows the data reported by Wik et al from 2005xix.This data was captured using 2000 ERC guidelines where the direction was 15compressions and two breaths, so it is not a direct comparison for the time withoutcompressions, but it is valid when looking at how much rate and depth improvedwith feedback.
The box on the far left shows the current ERC recommendationsxx. If we compareour data to the standards for basic life support as set by the Guidelines of 2005, it isevident there is still a problem with the no-flow time within the first 3 minutes ofthe resuscitation attempt. This is significantly higher than it should be. Thefrequency and depth however are good, though not yet 100%.
The EMTs understand the importance of feedback, and if for any reason, a team iswithout it, they find they miss it. The department also assesses its work and studiesthe results in regular evaluations. The team uses evaluation software supplied by themanufacturer, which tracks compression depth and frequency as well as no flow time.The software can be used to evaluate individual resuscitations and this has beenhelpful in allowing the EMTs to evaluate their performance. It is import to talkabout the results. We review every resuscitation attempt; we are re-evaluating eachcase, showing the graphs to the people that did the job; and we are talking about theimportance of good chest compressions and the importance of feedback. We havinggood success with this method of review.
Minute Minute Minute Wik et al. (2005) ERC 20051-3 4-6 7-9 (ERC 2000)
Time w/o 28% 19% 16% 38% 18%compression
Frequency of CC 84,9/min 90,7/min 91,3/min 60/min 88/min
CC depth over 4cm/1.5 inch 80% 79% 80% 27% 100%
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 21

I want to give you an idea of how such an evaluation is carried out and what thepeople see when we review their performance.
The software generates this chart below which shows several things. The top lineshows when shocks were administered. The second box shows the depth ofcompressions delivered, with the pale green bar showing the correct depth. In thisexample, the compressions were a bit too deep.
The bottom box shows the rate of compression and again the green bar shows theERC rate of between 90 and 110 compressions per minute.
The middle section shows the compressions quality, when a compression is at thecorrect rate and depth it shows as a green section. Very few of these compressionswere in target, because of the depth being too deep.
22
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 22

23
Here are samples from actualrescues.
This one shows a very goodperformance and it’s importantto tell them that. They did agood job with the feedbacksystem because if you look atthe rate of chest compressionthis looks like a machinedelivering the chestcompressions. They really didwell delivering chestcompressions at a rate of 100per minute. You also see thatalthough every chestcompression is more than 4centimeters, some exceed theGuidelines’ recommendationsfor the chest compressions; butevery single chest compressionwas deep enough. Anotherexample of how the feedbackworks.
In general, we have found that it takes a little time, perhaps 15 compressions, for therescuer to sync up with the beeping of the metronome to get the frequency correct.In this case, as soon as the rescuer realizes this sound is meant for me, he finds theright frequency and the right rhythm for the chest compressions. So we often see thatpattern in our delivery.
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 23

Is Training Necessary?Some people might questionthe need for training. Theyassume that if there is aneffective feedback system, therescuer can just follow it andthe results will be good. Let medemonstrate why we believethat training on the feedback isevery bit as important as havingfeedback on the devices. Here is an example. The firstrescuer was a trainee; and wastold to try to deliver chestcompressions. He was nottrained in the feedback system though he just came from an EMT school. He wastrained in resuscitation, but not in the use of the feedback system. The compressionswere far too fast – 150 –160 compressions per minute and the depth was tooshallow. This will not lead to a return of circulation. Even though the device wasproviding feedback, the trainee did not know to follow it. When the rescuer that was trained in the feedback system takes over and follows the feedback, the rate anddepth are correct. As a result of data like this, it is now our policy that no one can do chest compressions unless they are trained in the feedback device.
ConclusionOur experience shows that it is very difficult to deliver good-quality CPR withoutfeedback, and that feedback does help to improve CPR quality in terms of rate,depth, and interruptions. However, training on the device chosen is every bit asimportant as having the device available. That training should include manikintraining as well as debriefing actual rescues to review performance and reinforce theneed for high-quality CPR.
24
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 24

25
P O S T - T E S T
Please mark answers on Test Answer Form.
1. What is unusual about The London Helicopter Emergency Medical Service?a. They use only helicoptersb. They have replaced the normal ambulance servicec. They don't respond to traumasd. They have a physician and a paramedic on each team
2. One serious problem with much CPR delivered is ___________________.a. Inconsistency of depth and frequency of chest compressionsb. Inconsistency of airway clearingc. Too few interruptions in the procedured. Not checking for a pulse often enough
3. A non invasive cardiac support pump is designed to ___________________a. Give automatic defibrillation shocksb. Give audible cues to time manual chest compressionsc. Perform automatic chest compressionsd. Breathe for the patient and take blood pressure
4. In one effective method for removing a cardiac patient's clothing, the clothes are ___________________a. Slit down the side. b. Slit down the front.c. Slit down the backd. Torn off item by item when necessary.
5. The average survival rate following resuscitation is about ____________.a. 15% b. 7%c. 80%d. 40%
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 25

26
6. One intervention that can increase survival rates after resuscitation is ___________________ a. Immediate open heart surgeryb. Therapeutic hypothermiac. Warming the patientd. Neurological testing
7. One effective form of therapeutic hypothermia in maintaining a lowered temperature is _______________. a. Ice packsb. Intra-vascular cooling c. Cooling fansd. Cooling blankets.
8. The appropriate effective rate for chest compressions is _________ per minute.a. 140b. 60c. 100d. 40-50
9. Appropriate depth for chest compressions on an adult is _____________________ a. 28-40 millimetersb. 60 millimetersc. 38-51 millimetersd. one inch
10.TRUE or FALSE. With a feedback system training is not necessary. a. TRUEb. FALSE
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 26

27
P O S T - T E S T A N S W E R S
1. (d) They have a physician and a paramedic on each team.
One thing unusual about the London Helicopter Emergency Medical Serviceis that they have a physician and a paramedic on each team.
2. (a) Inconsistency of depth and frequency of chest compressions
One serious problem with much CPR delivered is inconsistency of depth andfrequency of chest compressions
3. (c) Perform automatic chest compressions.
A non invasive cardiac support pump is designed to perform automatic chestcompressions.
4. (c) Slit down the back
In one effective method for removing a cardiac patient's clothing, the clothesare slit down the back.
5. (a) 15%
The average survival rate following resuscitation is about 15%.
6. (b) Therapeutic hypothermia
One intervention that can increase survival rates after resuscitation istherapeutic hypothermia.
7. (b) Intra-vascular cooling
One effective form of therapeutic hypothermia in maintaining a loweredtemperature is intra-vascular cooling
8. (c) 100
The appropriate effective rate for chest compressions is 100 per minute.
9. (c) 38-51 millimeters
Appropriate depth for chest compressions on an adult is 38-51 millimeters.
10. (b) FALSE.
With a feedback system training is necessary.
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 27

28
R E F E R E N C E S :
i Ristagno G Sun S Crit Care Med. 2007 Sep;35(9):2145-9.
ii Fries M, Beckers, S et al Resuscitation. 2007 Jan;72(1):66-73.
iii Lipton 1999 Physiology Review.
iv Sunde K, Pytte M et al 2007 Resuscitation 2007 Apr;73(1):29-39.
v Nolan JP, Neumar RW, et al Resuscitation. 2008 Dec;79(3):350-79.
vi Williams GR et al Ann Surg. 1958 Sep;148(3):462-8.
vii The Haca Study Group N Engl J Med. 2002 Feb 21;346(8):549-56.
viii Boddicker KA, Zhang Y et al Circulation. 2005 Jun 21;111(24):3195-201.
ix Abella BS, Zhao, D et al Circulation. 2004 Jun 8;109(22):
2786-912004 Circ.
x TSAI MS, Barbet D, J Am Coll Cardiol. 2008 May 20;51(20):1988-90
xi Hoedemaekers CW et al Crit Care. 2007;11(4):R91.
xii Wolfrum S, Radke PW Resuscitation. 2007 Feb;72(2):207-13.
xiii Grol R, Wensing M J Aust. 2004 Mar 15;180(6 Suppl):S57-60. Review.
xiv Gluckman PD, Wyatt JS Lancet. 2005 Feb 19-25;365(9460):663-70.
xv Clifton CL, Miller ER et al N Engl J Med. 2001 Feb 22;344(8):556-63.
xvi Dixon SR Whitborn RA Am Coll Cardiol. 2002 Dec 4;40(11):1928-34.
xvii Gude et al Poster Presentation Resuscitation 2008 Ghent.
xviii Sutton RM, Donohue A, Resuscitation. 2007 Oct;75(1):161-8.
xix Wik L, Kramer- Johansen J JAMA Jan 19;293(3):299-304.
xx European Resuscitation Council guidelines for Resuscitation 2005;
Resuscitation. 2005 Dec; 67 Suppl 1.
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 28

Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 29

Printed in U.S.A. PN-157
©2010 ZOLL Medical Corporation. All rights reserved. ZOLL is a registered trademark of ZOLL Medical Corporation in theUnited States and/or other countries. All other trademarks are the property of their respective owners.
Gizmos_CEU_8_10_Layout 1 9/7/10 3:20 PM Page 30