localising a global health innovation: the pack brazil ... file from pack global to pack brazil step...
TRANSCRIPT
www.knowledgetranslation.co.za
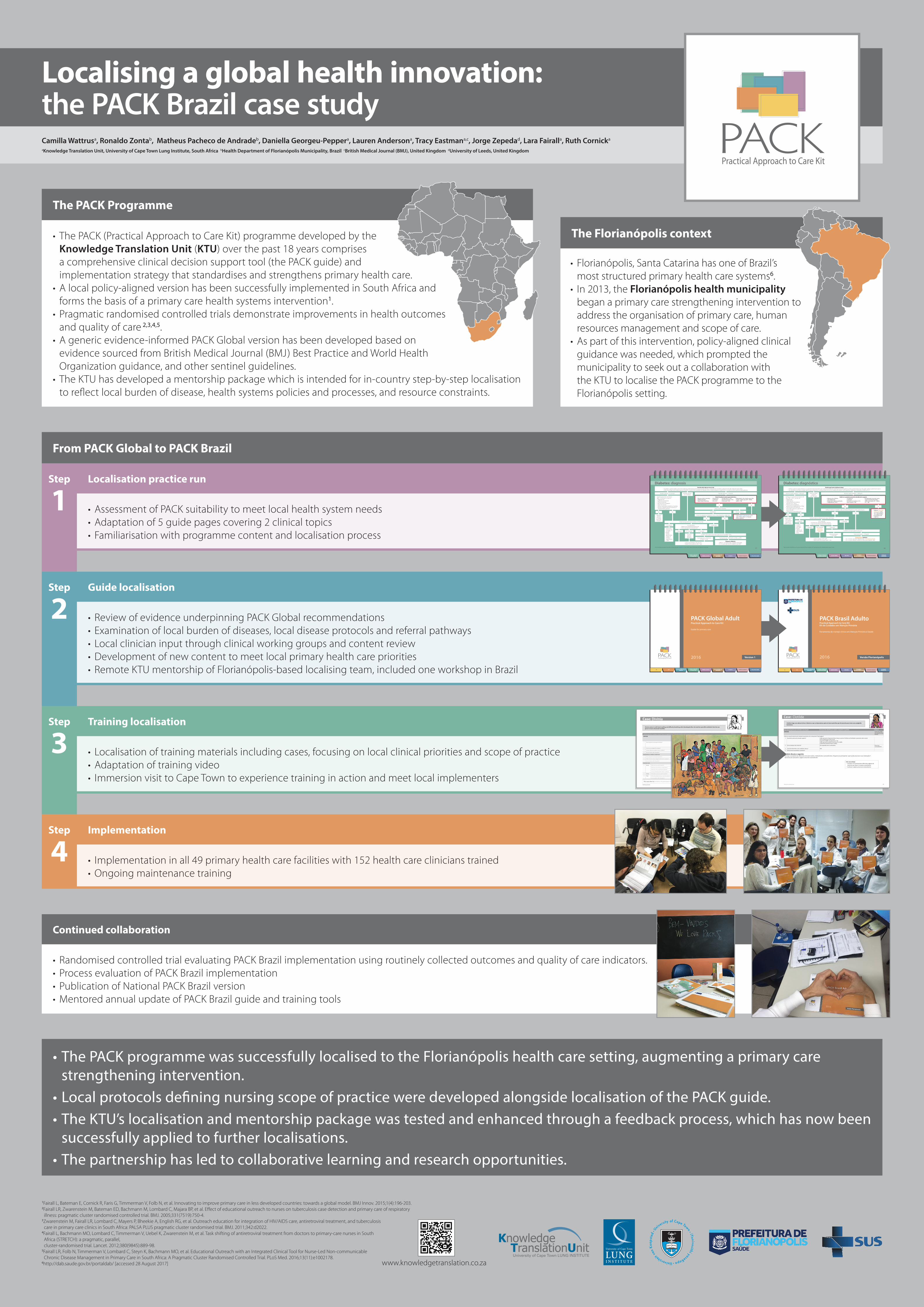
From PACK Global to PACK Brazil
Step
1Localisation practice run
• Assessment of PACK suitability to meet local health system needs • Adaptation of 5 guide pages covering 2 clinical topics• Familiarisation with programme content and localisation process
Step
2Guide localisation
• Review of evidence underpinning PACK Global recommendations• Examination of local burden of diseases, local disease protocols and referral pathways• Local clinician input through clinical working groups and content review • Development of new content to meet local primary health care priorities• Remote KTU mentorship of Florianópolis-based localising team, included one workshop in Brazil
Step
3Training localisation
• Localisation of training materials including cases, focusing on local clinical priorities and scope of practice• Adaptation of training video• Immersion visit to Cape Town to experience training in action and meet local implementers
Step
4Implementation
• Implementation in all 49 primary health care facilities with 152 health care clinicians trained• Ongoing maintenance training
Camilla Wattrusa, Ronaldo Zontab, Matheus Pacheco de Andradeb, Daniella Georgeu-Peppera, Lauren Andersona, Tracy Eastmana,c, Jorge Zepedad, Lara Fairalla, Ruth Cornicka
aKnowledge Translation Unit, University of Cape Town Lung Institute, South Africa bHealth Department of Florianópolis Municipality, Brazil cBritish Medical Journal (BMJ), United Kingdom dUniversity of Leeds, United Kingdom
1Fairall L, Bateman E, Cornick R, Faris G, Timmerman V, Folb N, et al. Innovating to improve primary care in less developed countries: towards a global model. BMJ Innov. 2015;1(4):196-203.2Fairall LR, Zwarenstein M, Bateman ED, Bachmann M, Lombard C, Majara BP, et al. Effect of educational outreach to nurses on tuberculosis case detection and primary care of respiratory illness: pragmatic cluster randomised controlled trial. BMJ. 2005;331(7519):750-4.
3Zwarenstein M, Fairall LR, Lombard C, Mayers P, Bheekie A, English RG, et al. Outreach education for integration of HIV/AIDS care, antiretroviral treatment, and tuberculosis care in primary care clinics in South Africa: PALSA PLUS pragmatic cluster randomised trial. BMJ. 2011;342:d2022.
4Fairall L, Bachmann MO, Lombard C, Timmerman V, Uebel K, Zwarenstein M, et al. Task shifting of antiretroviral treatment from doctors to primary-care nurses in South Africa (STRETCH): a pragmatic, parallel, cluster-randomised trial. Lancet. 2012;380(9845):889-98.
5Fairall LR, Folb N, Timmerman V, Lombard C, Steyn K, Bachmann MO, et al. Educational Outreach with an Integrated Clinical Tool for Nurse-Led Non-communicable Chronic Disease Management in Primary Care in South Africa: A Pragmatic Cluster Randomised Controlled Trial. PLoS Med. 2016;13(11):e1002178.
6http://dab.saude.gov.br/portaldab/ [accessed 28 August 2017]
• The PACK programme was successfully localised to the Florianópolis health care setting, augmenting a primary care strengthening intervention.
• Local protocols defining nursing scope of practice were developed alongside localisation of the PACK guide.• The KTU’s localisation and mentorship package was tested and enhanced through a feedback process, which has now been
successfully applied to further localisations.• The partnership has led to collaborative learning and research opportunities.
Localising a global health innovation: the PACK Brazil case study
The Florianópolis context
• Florianópolis, Santa Catarina has one of Brazil’s most structured primary health care systems6.
• In 2013, the Florianópolis health municipality began a primary care strengthening intervention to address the organisation of primary care, human resources management and scope of care.
• As part of this intervention, policy-aligned clinical guidance was needed, which prompted the municipality to seek out a collaboration with the KTU to localise the PACK programme to the Florianópolis setting.
The PACK Programme
• The PACK (Practical Approach to Care Kit) programme developed by the Knowledge Translation Unit (KTU) over the past 18 years comprises a comprehensive clinical decision support tool (the PACK guide) and implementation strategy that standardises and strengthens primary health care.
• A local policy-aligned version has been successfully implemented in South Africa and forms the basis of a primary care health systems intervention1.
• Pragmatic randomised controlled trials demonstrate improvements in health outcomes and quality of care 2,3,4,5.
• A generic evidence-informed PACK Global version has been developed based on evidence sourced from British Medical Journal (BMJ) Best Practice and World Health Organization guidance, and other sentinel guidelines.
• The KTU has developed a mentorship package which is intended for in-country step-by-step localisation to reflect local burden of disease, health systems policies and processes, and resource constraints.
Continued collaboration
• Randomised controlled trial evaluating PACK Brazil implementation using routinely collected outcomes and quality of care indicators.• Process evaluation of PACK Brazil implementation• Publication of National PACK Brazil version• Mentored annual update of PACK Brazil guide and training tools
Manual do treinador local 23
Case: Clotilde
Faça estas perguntas para estimular o uso do guia Forneça estes detalhes para ajudar a responder as questões Página/s
SINTOMA Tosse e/ou falta de ar ou Sintomas da face
Onde na nossa ferramenta de manejo de pacientes nós começamos? Qual página?
1 A paciente precisa de atenção urgente? Não apresenta fraqueza de face, braço ou perna. Ela fala com facilidade e apresenta visão normal. Sua temperatura está normal. Sua PA é 120/85. Sua glicemia é 110. Não apresenta edema em pernas, PA 120/85. Apresenta edema de face e sibilos.
2 Como manejar este sintoma? Ela respondeu bem à adrenalina. Prescreva racionalmente
3 É possível identificar uma condição crônica? N/A
4 Você precisa encaminhar a paciente?
Também discuta o seguinte: - Destaque o propósito das diferentes cores para exames, medicamentos e procedimentos. Pergunte aos participantes ‘quem pode prescrever essas medicações?’. - Aproveite para apresentar a página ‘prescreva racionalmente’.
Clotilde chega com edema de face e falta de ar que se desenvolveu após ela tomar penicilina que foi prescrita para tratar uma amigdalite bacteriana.
Este caso almeja: · Introduzir aos participantes diferentes páginas de
sintomas que levam a manejos semelhantes ·Conhecer a página prescreva racionalmente.
83
Diabetes: diagnósticoDecida qual teste de glicemia fazer:
• Verifique glicemia capilar aleatória se o paciente não estiver bem, tiver sintomas de diabetes (sede, aumento da frequência urinária, perda de peso) ou não puder verificar a glicemia em jejum.• Se o paciente estiver bem e puder retornar para rastreamento: verifique fatores de risco e maneje como abaixo. Se for gestante, interprete os resultados conforme 111.
Glicemia capilar aleatória < 130mg/dL Glicemia capilar aleatória
130-199mg/dL
Glicemia de jejum ≤ 125mg/dL
• Avalie e maneje o RCV 81.• Repita glicemia de jejum após 1 ano.
Diagnostique diabetes• Se < 35 anos, considere diabetes tipo 1, discuta/encaminhe.• Se ≥ 35 anos, ofereça cuidados de rotina para diabetes 84.
Glicemia de jejum > 125mg/dL
140-199mg/dL Tolerância
diminuída à glicose
110-125mg/dL• Paciente tem glicemia de jejum alterada• Faça um teste de tolerância oral à glicose1
Verifique sintomas de diabetes: sede, aumento da frequência urinária, perda de peso
Verifique glicemia de jejum após jejum de 8 horas.
Glicemia capilar aleatória > 200mg/dL
Não
Não
Não
< 110mg/dL
< 140mg/dL > 199mg/dL
Confirme com outra glicemia de jejum
• Avalie e maneje o RCV 81.
• Repita glicemia de jejum após 3 anos.
> 125mg/dL
Se entre 40-70 anos e IMC
≥ 25 verifique a glicemia a
cada 3-5 anos.
Sim
Sim
Sim
Verifique se o paciente tem fatores de risco: IMC ≥ 25 e 1 ou mais de:• Hipertensão• Sedentarismo• História familiar de diabetes
(parentes de 1° grau)•História prévia de diabetes
gestacional ou bebê grande (≥ 4,5kg)• História prévia de tolerância
diminuída à glicose ou glicemia dejejum alterada
• Síndrome do ovário policístico• Aplique cloreto de
sódio 0.9% 1L EV em 2 horas depois 1L a cada 4 horas.
• Encaminhe com urgência.
Avalie se o paciente necessita atendimento urgente:• Náusea e/ou vômitos• Dor abdominal• Respiração rápida e profunda• Temperatura ≥ 38°C
• Sonolência• Confusão• Perda da consciência 15• Dor no peito 30
• Desidratação: mucosas secas, turgor da pele diminuído, olhos encovados, PA < 90/60, FC > 100
1Faça um teste de tolerância oral à glicose depois de 8 horas de jejum, dê 75g de glicose oral e verifique glicemia após 2 horas.
SAÚDE DA MULHER CUIDADOSPALIATIVOSSAÚDE MENTAL EPILEPSIA DESORDENS
MULSCULOESQUELÉTICASDOENÇAS CRÔNICASDO ESTILO DE VIDA
PACK Brasil AdultoPractical Approach to Care KitKit de Cuidados em Atenção Primária
Ferramenta de manejo clínico em Atenção Primária à Saúde
2016 Versão Florianópolis
SAÚDE DA MULHER CUIDADOSPALIATIVOSSAÚDE MENTAL EPILEPSIA DESORDENS
MULSCULOESQUELÉTICASTB HIV DOENÇAS RESPIRATÓRIASCRÔNICAS
DOENÇAS CRÔNICASDO ESTILO DE VIDA
PACK Global AdultPractical Approach to Care Kit
Guide for primary care
2016 Version 1
WOMEN’S HEALTH PALLIATIVE CAREMENTAL HEALTH MUSCULOSKELE TAL DISORDERS
EPILEPSYTB HIV CHRONIC RESPIRATORYDISEASE
CHRONIC DISEASESOF L IFEST YLE
77
Diabetes: diagnosisDecide which glucose test to do:
• If patient is well and able to return for screening, check fasting plasma glucose after an 8-hour overnight fast. If patient is pregnant and well, interpret result 102.• Only check finger prick random glucose if patient is unwell or has symptoms of diabetes (thirst, urinary frequency, weight loss) or is unable to return easily for fasting glucose.
Random glucose < 6.1mmol/L Random glucose 6.1-11mmol/L
Fasting glucose ≤ 6.9mmol/L or HbA1c < 6.5%
• Assess and manage CVD risk 75.• Repeat fasting glucose after 1 year.
Diagnose diabetes• Refer if < 35 years as type 1 diabetes more likely.• If ≥ 35 years, give routine diabetes care 78.
Fasting glucose > 6.9mmol/L or HbA1c ≥ 6.5%
7.8-11mmol/L
6.1- 6.9mmol/L• Patient has impaired fasting glucose.• Do an oral glucose tolerance test1.
No ketones
Check urine for ketones.
Check for symptoms of diabetes: thirst, urinary frequency, weight loss
Check fasting plasma glucose after an 8-hour fast.
Ketones present
Random glucose > 11mmol/L
No
No
No
< 6.1mmol/L
< 7.8mmol/L > 11mmol/L
Confirm with another test: fasting glucose or if available, HbA1c.
• Assess andmanage CVDrisk 75.
• Repeat fasting glucose after 3 years, or if CVD or hypertension, 1 year.
> 6.9mmol/L
Recheck glucose
3-5 yearlyonce over45 years.
Yes
Yes
Yes
Check if patient has risk factors:BMI ≥ 25 and one or more of:• Hypertension• Cardiovascular disease• Physical inactivity• Family history of diabetes• High risk ancestry• Previous gestational diabetes or big baby• Previous impaired glucose tolerance or
impaired fasting glucose
• Give sodium chloride 0.9% 1L IV over 2 hours then 1L 4 hourly.
• Refer urgently.
Check if patient needs urgent attention:• Nausea and/or vomiting• Abdominal pain• Rapid deep breathing
• Drowsiness• Confusion• Fits 12
• Temperature ≥ 38oC• Unconsciousness 10• Chest pain 25
• Dehydration: dry mouth, poor skin turgor, sunken eyes, BP < 90/60, pulse ≥ 100
Impaired glucose
tolerance
1Do an oral glucose tolerance test after an 8-hour fast, give oral glucose 75g in 250mL water to drink and check glucose 2 hours later.
WOMEN’S HEALTH PALLIATIVE CAREMENTAL HEALTHMUSCULOSKELE TAL
DISORDERS EPILEPSYCHRONIC DISEASES
OF L IFEST YLE
19Training manual
Case: Divinia
Divinia comes in with facial swelling and difficulty breathing which developed after she took her penicillin antibiotic that she was given to treat a bacterial tonsillitis.
Ask these questions to prompt using the Patient-management tool Give these details to help answer the questions Page/s
SYMPTOM Cough and/or difficulty breathing
orFace Symptoms
1 Does the patient need urgent attention? • She has no weakness of the face, legs or arms.• She speaks with ease and has normal vision.• Her urine dipstick is normal.• Her temperature is normal.
2 How do you manage this symptom? She responds well to epinephrine.
3 Can you identify a possible chronic condition?
4 Do you need to refer the patient?
DIAGNOSING A CHRONIC CONDITION
5 Does the patient need urgent attention? N/A
6 What is the next step to diagnose the chronic condition? N/A
7 Do you need to refer the patient? N/A
ROUTINE CARE
8 Assess What must you ask this patient? N/A
What must you look for on examination? N/A
What tests must you do for this patient? N/A
Can you identify another chronic condition? N/A
9 Advise What advice must you give this patient? N/A
10 Treat What drug treatment do you give this patient? N/A
Do you need to refer the patient? N/A
This case aims to: Introduce the participants to different symptom pages leading to similar management.