learning objectives for this filepeople.musc.edu/~decristc/adv patho/unit 10...
TRANSCRIPT
Adv Pathophysiology Unit 10: Endocrine Page 1 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
Learning Objectives for this File: 1. Review the anatomy of the adrenal glands and its hormones 2. Appreciate the biosynthetic pathway that produces the four main hormone groups 3. Understand the biofeedback of the HPA axis 4. Review clinical correlates of over- or under-production of adrenal hormones 5. Understand the mechanism of action of glucocorticoids and expected physiologic effects 6. Understand the consequences of excess glucocorticoid administration
Adv Pathophysiology Unit 10: Endocrine Page 2 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
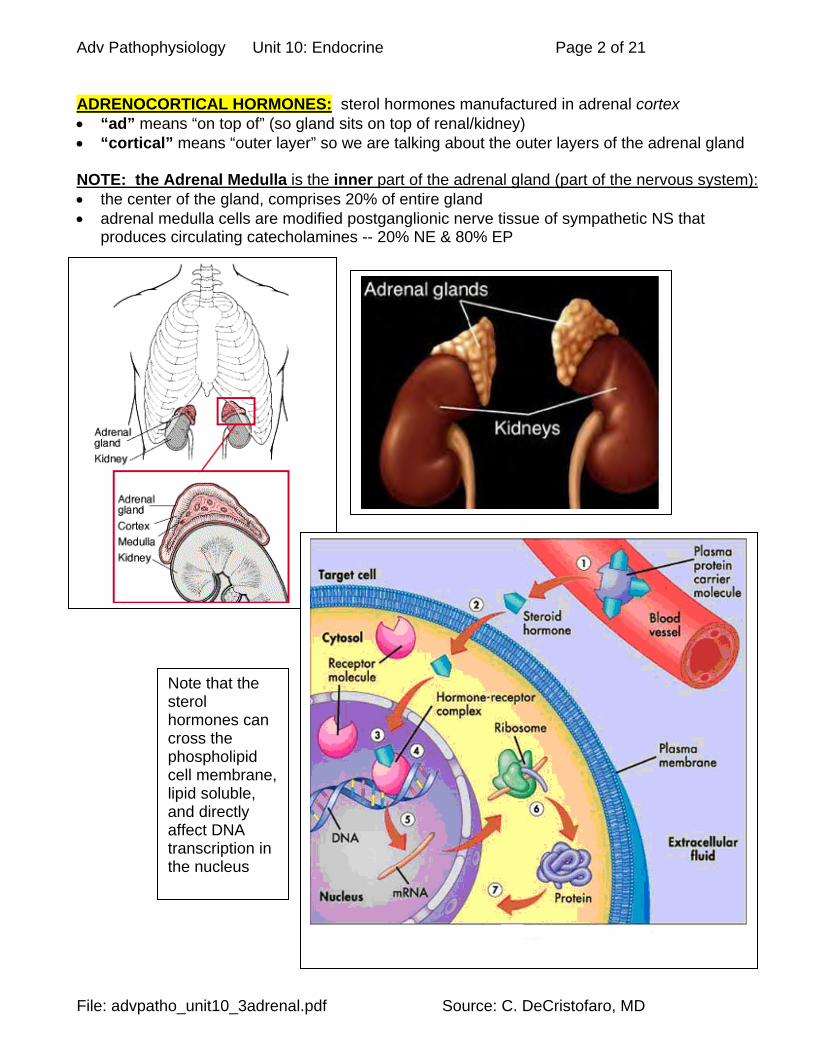
ADRENOCORTICAL HORMONES: sterol hormones manufactured in adrenal cortex “ad” means “on top of” (so gland sits on top of renal/kidney) “cortical” means “outer layer” so we are talking about the outer layers of the adrenal gland NOTE: the Adrenal Medulla is the inner part of the adrenal gland (part of the nervous system): the center of the gland, comprises 20% of entire gland adrenal medulla cells are modified postganglionic nerve tissue of sympathetic NS that
produces circulating catecholamines -- 20% NE & 80% EP
Note that the sterol hormones can cross the phospholipid cell membrane, lipid soluble, and directly affect DNA transcription in the nucleus
Adv Pathophysiology Unit 10: Endocrine Page 3 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
1. Adrenal Cortex:
80% of entire gland, has three layers. Produces a category of hormone called CORTICOSTEROIDS (mineralocorticoids,
glucocorticoids, sex hormones). WATCH OUT !! Very often, clinical use of the word "corticosteroid" is used to mean
ONLY "glucocorticoid" (i.e., cortisones, cortisol). Anatomic “zones” (layers) of the Adrenal Cortex: Outer cortex (zona glomerulosa):
o mineralocorticoids (Aldosterone) o effects on electrolytes
Middle cortex (zona fasciculata): o glucocorticosteroids (glucocorticoids, e.g. cotisols) with effects on glucose o protein & fat metabolism & sex hormones (androgens & female sex hormones).
Inner cortex (zona reticularis): o also glucocorticosteroids (glucocorticoids, e.g. cortisols) o effects on glucose, protein & fat metabolism & sex hormones (androgens & female
sex hormones). (Mnemonic: “It gets sweeter as you go inwards”) 2. Chemistry & Secretion:
steroid hormones produced from the cholesterol in the LDL lipoprotein. glucocorticoids & mineralocorticoids share some cross-reactivity in their effects on
target cells.
Chemistry of synthesis: cyclopentane ring structure, with attachments that define the chemical properties of these
hormones. The adrenal cortex mostly secretes what are called C19 and C21 steroids. Most of the C19 steroids have a "keto" group at position 17 of the cyclopentane ring, and are
therefore called 17-keto-steroids. The C21 steroids usually have a "hydroxyl" group at the 17 position, and are often called 17-
OH-corticoids (17-hydroxy-corticoids). (See pictures next page)
Adv Pathophysiology Unit 10: Endocrine Page 4 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
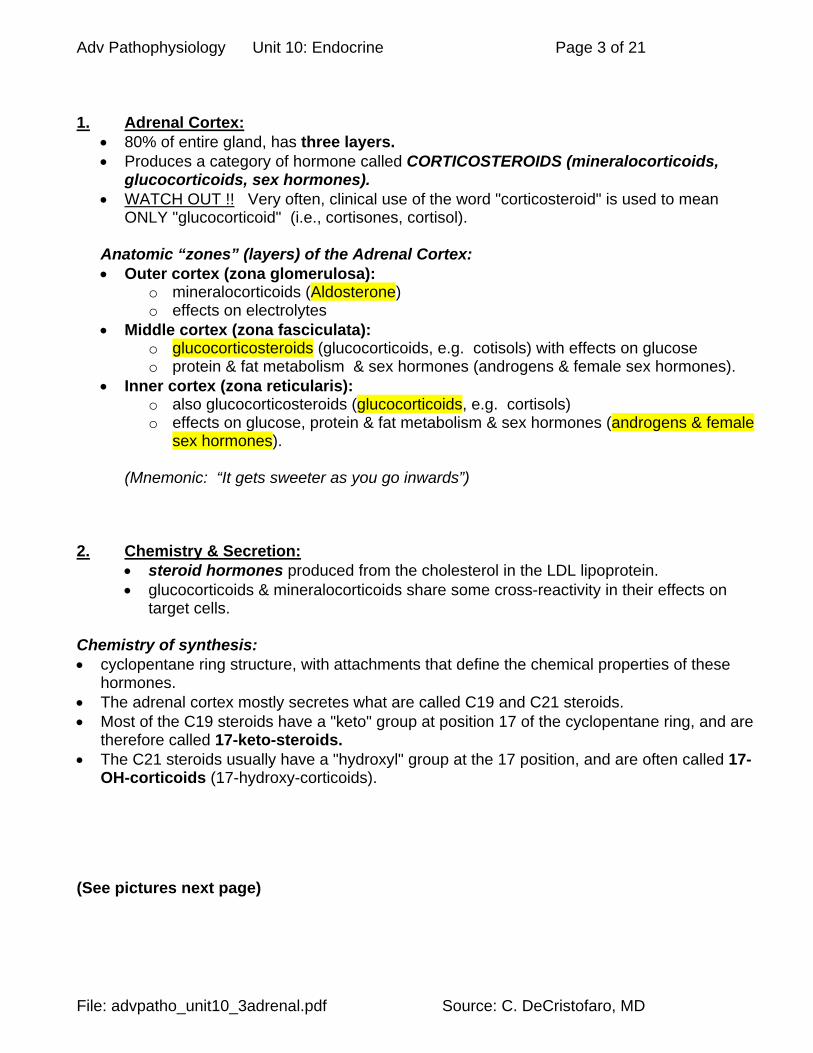
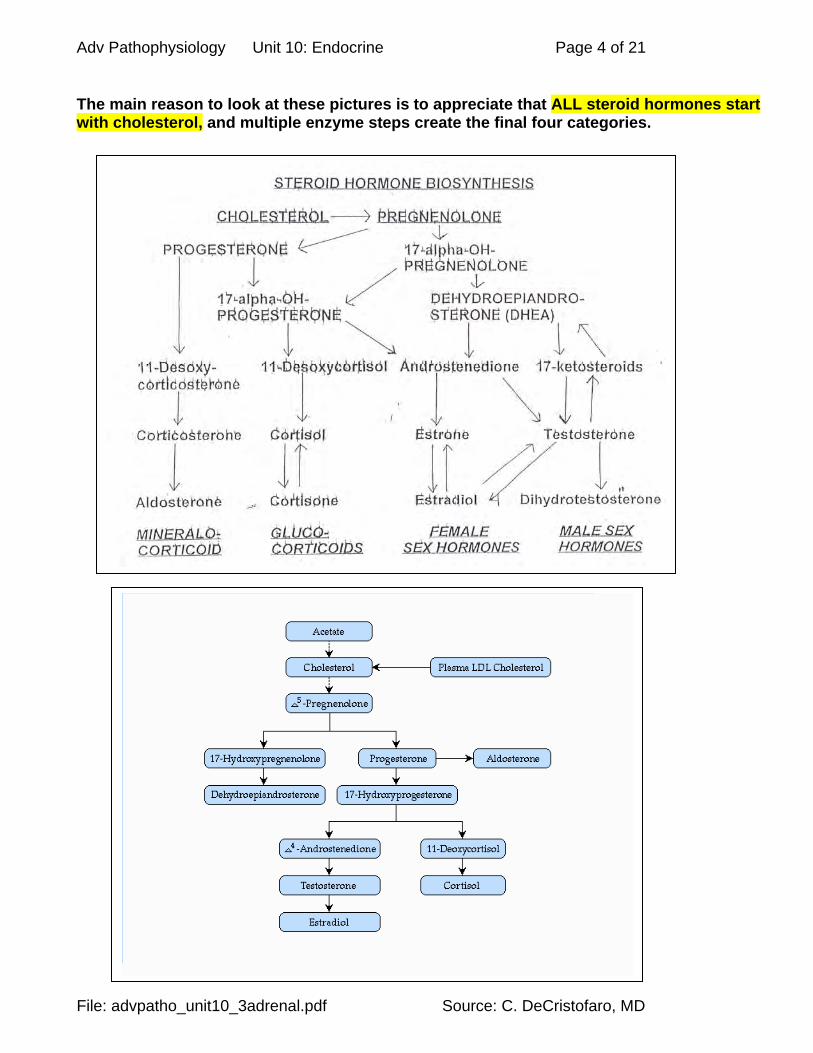
The main reason to look at these pictures is to appreciate that ALL steroid hormones start with cholesterol, and multiple enzyme steps create the final four categories.
Adv Pathophysiology Unit 10: Endocrine Page 5 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
Enzyme deficiciencies (genetic “inborn errors of metabolism”) and clinical effects: Genetic defect
o enzyme in a synthetic pathway isn’t available o also called an “inborn error of metabolism”
Congenital Adrenal Hyperplasia (CAH): o Common deficiency of enzyme 21-hydroxylase, which is needed to make cortisol in the
biosynthetic pathway within the adrenal cortex o Since this biosynthetic metabolic pathway requires multiple sequential enzyme steps:
prevents the formation of the final product – little or no cortisol as well as buildup of intermediary products which may be toxic
o Lack of final product feedback (cortisol) to the hypothalamus & anterior pituitary creates an increase in (stimulation) ACTH production
o this stimulates the cells of the adrenal cortex to proliferate, causing hyperplasia of the adrenal cortex
o (more below)
Adv Pathophysiology Unit 10: Endocrine Page 6 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
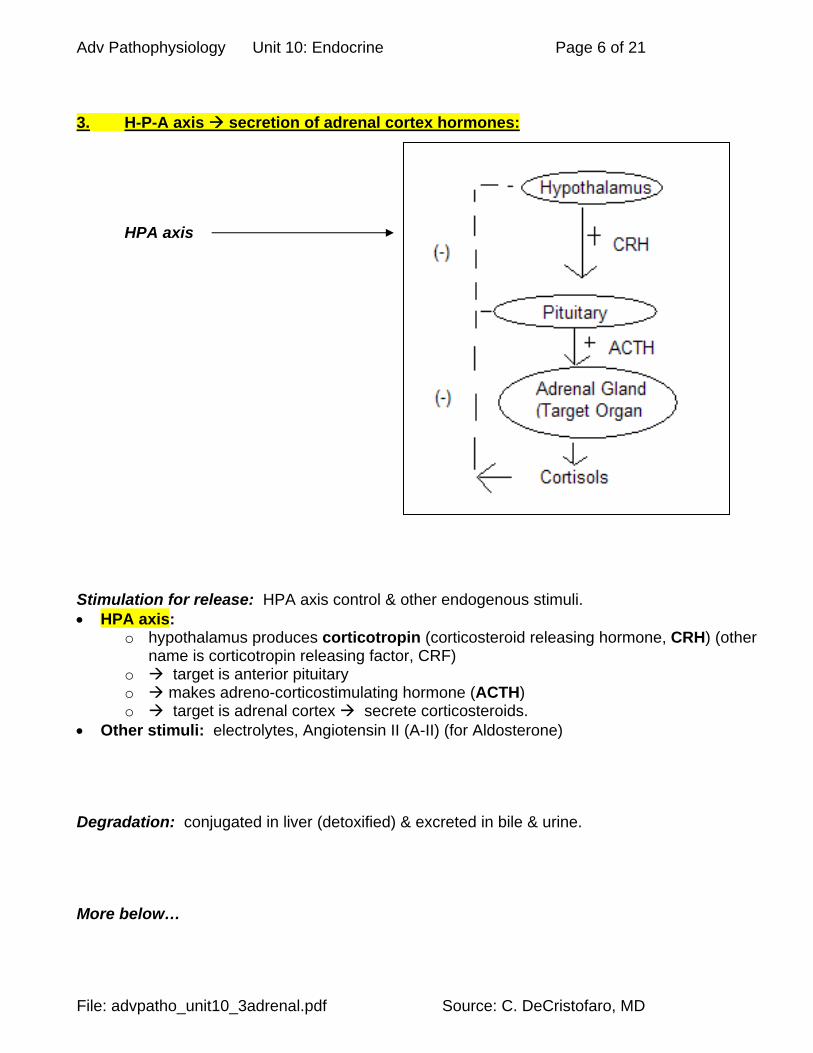
3. H-P-A axis secretion of adrenal cortex hormones:
HPA axis
Stimulation for release: HPA axis control & other endogenous stimuli. HPA axis:
o hypothalamus produces corticotropin (corticosteroid releasing hormone, CRH) (other name is corticotropin releasing factor, CRF)
o target is anterior pituitary o makes adreno-corticostimulating hormone (ACTH) o target is adrenal cortex secrete corticosteroids.
Other stimuli: electrolytes, Angiotensin II (A-II) (for Aldosterone) Degradation: conjugated in liver (detoxified) & excreted in bile & urine. More below…

Adv Pathophysiology Unit 10: Endocrine Page 7 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
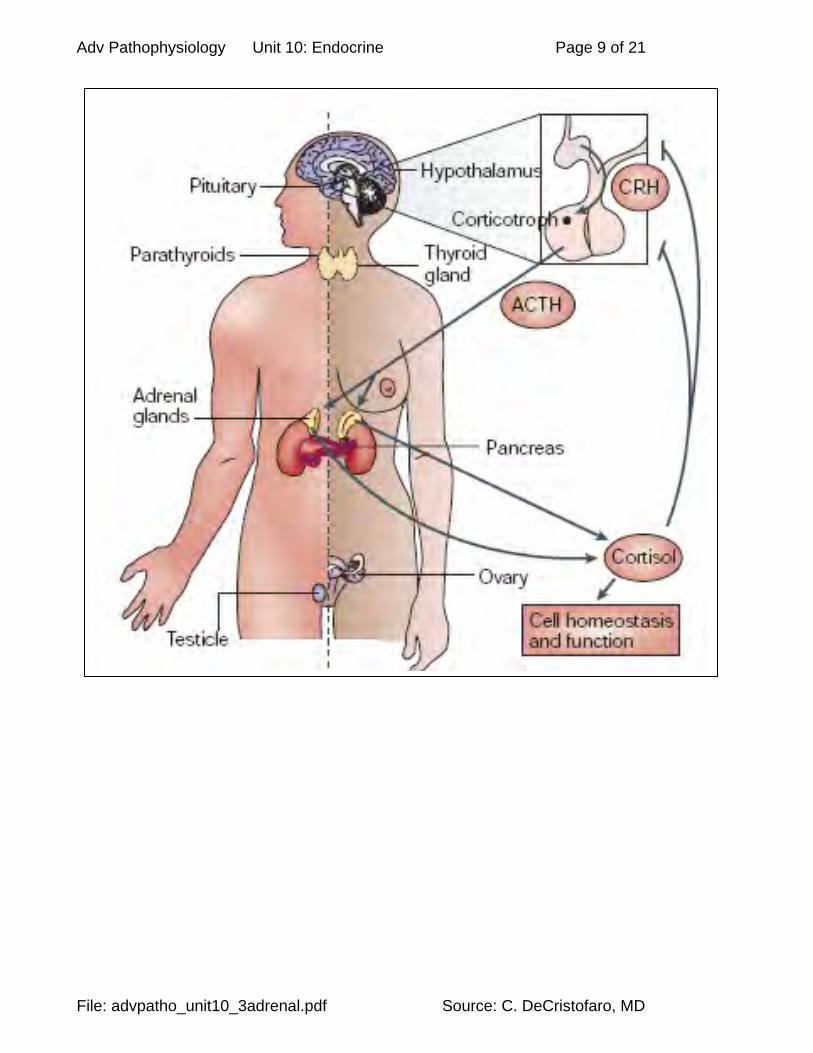
Steps in hormone release: STEP #1: in the hypothalamus
o Hypothalamus makes corticotropin (CRH, also called corticotropin releasing factor, CRF) anterior pituitary
STEP #2: in the anterior pituitary
o anterior pituitary produces a prohormone called POMC (Pro-opiomelanocortin) cleaved (cut) to produce multiple active hormones b-endorphin:
endogenous morphine MSH: melanocyte stimulating hormone
stimulates melanocytes to make melanin, to proliferate, and to migrate to skin surface overall effect is skin darkening
ACTH (adrenocorticotropic hormone): stimulates adrenal cortex to make corticosteroids (glucocorticoids,
mineralocorticoids, sex steroids) lipotropin (beta-lipotropin):
effects on adipocytes and lipid metabolism effects.
STEP # 3: in the adrenal cortex o ACTH target cells of adrenal cortex o cAMP secondary messenger system stimulates secretion of adrenocortical hormones
via multiple enzyme synthetic steps (involved metabolic pathways that are also interconnected)
o corticosteroids released to the body So, every time you make ACTH you also make other hormones that help your body deal with stress & pain.
POMC MSH
ACTH
beta-endorphin
lipotropin
Adrenal cortex
Pain control in CNS
Adipocytes (Fat cells)
Melanocytes

Adv Pathophysiology Unit 10: Endocrine Page 8 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
Understanding biofeedback diagrams: SOLID LINES ARE “POSITIVE” FEEDBACK (turn on the next cell) DASHED LINES ARE “NEGATIVE” FEEDBACK (turn off the next cell)
o How to get negative feedback? o From the PRODUCTS of the Adrenal Cortex o From the EFFECTS of the hormones on the body o Thus, action of a system SHOULD turn the system off once the desired result is
obtained o A system doesn’t keep on going!
Negative feedback: to both the hypothalamus (reduces CRF production) & anterior pituitary (reduces ACTH production) H-P-A AXIS & BIOFEEDBACK CONTROL: (+) (-) (-) (-) (+) (+) (+)
Hypothalamus (releasing or inhibiting fctors)
Anterior Pituitary (stimulating hormones)
Adrenal Cortex
Target Tissues Effects
Cortisol
ACTH
Adv Pathophysiology Unit 10: Endocrine Page 9 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD

Adv Pathophysiology Unit 10: Endocrine Page 10 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
HORMONES OF THE ADRENAL CORTEX: 1) Mineralocorticoids: mostly Aldosterone, plus some mineralocorticoid activity from the cortisones
(desoxycorticosterone, corticosterone, and cortisol). Review from renal & acid/base section. Physiology: 50% non-protein bound in plasma. Requires presence of ACTH from anterior pituitary to be secreted. BUT MAIN STIMULUS FOR SECRETION is electrolyte levels
Overall effects: conserves salt (NaCl) excretes K & H+. Stimulus for Secretion: ALDOSTERONE ALONE: potassium intake, reduced sodium intake, constriction of inferior
vena cava in thorax, standing posture, some clinical illnesses, presence of angiotensin-II (A-II).
ALDOSTERONE & GLUCOCORTICOID: both aldosterone & glucocorticoids are released: surgery, stress, trauma, hemorrhage, anxiety, AND of course with stimulus of ACTH on adrenal cortex (not as clinically important).
Targets: similar actions at each target location. Kidney: distal nephron stimulating potassium secretion (excretion), Na reabsorption
(retention), secretion (excretion) of H+. Other targets: salivary glands, sweat glands, and intestinal absorption of Na/K. Pathophysiology: Hyperaldosteronism: get rid of TOO MUCH K+ & H+
o Excess aldosterone causes hypokalemia & alkalosis with muscle weakness, some hypernatremia.
o Etiology may be tumor, or from other non-adrenal illnesses (liver cirrhosis, HF, & nephrotic syndrome).
Addison's disease: to LITTLE aldosterone get rid of TOO LITTLE K+ & H+ o too little aldosterone causes acidosis, hyperkalemia, hyponatremia & cardiac toxicity. o Can't secrete potassium, reabsorb sodium, or secrete acid since this linked to
potassium secretion. o Poor stress response o Replacement drugs (synthetics):
9-alpha-fluorocortisol, cortisone (glucocorticoids with slight mineralocorticoid activity).
Adv Pathophysiology Unit 10: Endocrine Page 11 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
2) Glucocorticosteroids: “cortisols” “counter-regulatory hormone” – released in stress Most people just say “cortisols” or “glucocorticoids” cortisols (glucocorticoids) include cortisol (95% of secretion, most potent), & corticosterone catabolic -- hormone of famine Peripheral circulation & protein bindng:
o mostly protein bound in plasma by a protein called transcortin, also called corticosteroid-binding globulin (CBG).
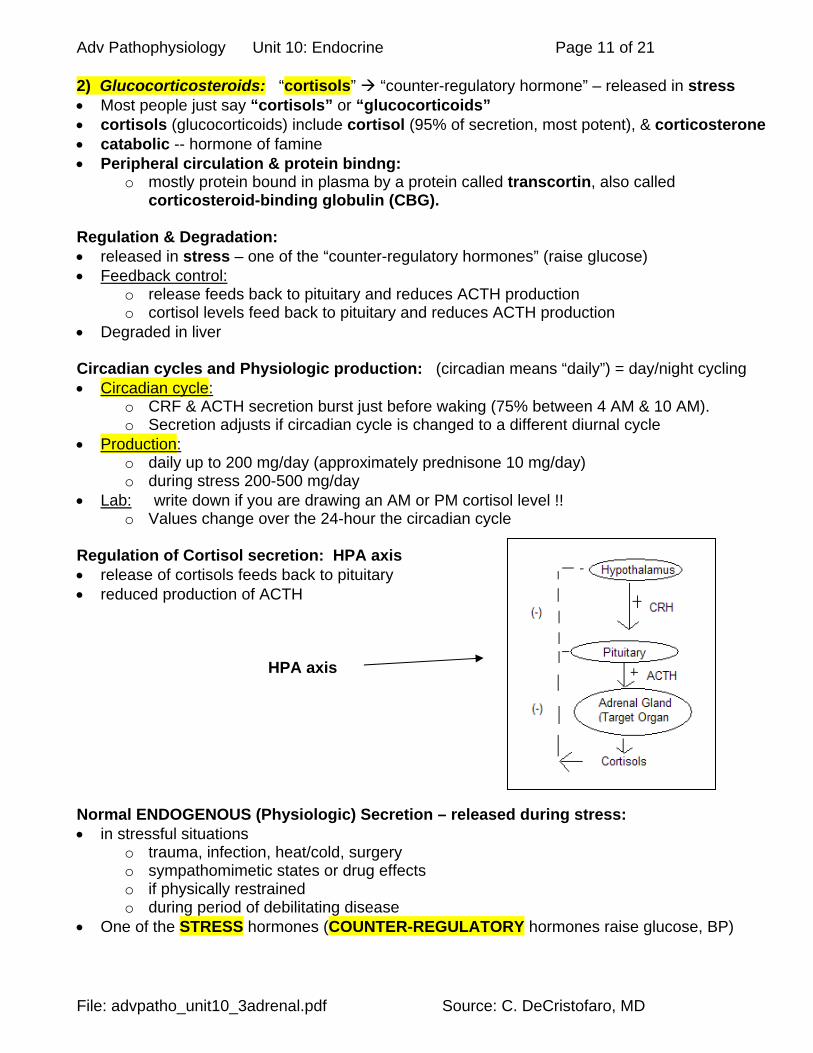
Regulation & Degradation: released in stress – one of the “counter-regulatory hormones” (raise glucose) Feedback control:
o release feeds back to pituitary and reduces ACTH production o cortisol levels feed back to pituitary and reduces ACTH production
Degraded in liver Circadian cycles and Physiologic production: (circadian means “daily”) = day/night cycling Circadian cycle:
o CRF & ACTH secretion burst just before waking (75% between 4 AM & 10 AM). o Secretion adjusts if circadian cycle is changed to a different diurnal cycle
Production: o daily up to 200 mg/day (approximately prednisone 10 mg/day) o during stress 200-500 mg/day
Lab: write down if you are drawing an AM or PM cortisol level !! o Values change over the 24-hour the circadian cycle
Regulation of Cortisol secretion: HPA axis release of cortisols feeds back to pituitary reduced production of ACTH
HPA axis
Normal ENDOGENOUS (Physiologic) Secretion – released during stress: in stressful situations
o trauma, infection, heat/cold, surgery o sympathomimetic states or drug effects o if physically restrained o during period of debilitating disease
One of the STRESS hormones (COUNTER-REGULATORY hormones raise glucose, BP)
Adv Pathophysiology Unit 10: Endocrine Page 12 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
Physiologic effects on target tissues: Anabolic: in liver/kidney promote gluconeogenesis (with required enchanced amino acid
uptake by liver & kidney) Raises glucose. Catabolic: elsewhere (muscle, skin, lymph, adipose, & connective tissues); more lipolysis in
adipocytes; muscle catabolism (release of amino acids for gluconeogenesis) Smooth muscle effects: upregulation of beta-agonist receptors, makes smooth muscle more
responsive to circulating catecholamine (e.g., bronchodilatation). This effect seen in as early as 15 minutes with parenteral administration. Helps you breathe.
Immune effects: o REDUCED: lymphocytes, monocytes, eosinophils, & basophils, production of
inflammatory mediators and cytokines, chemotaxis of WBC, phagocytosis by tissue macrophages & PMN, production of interleukin-1 & pyrogens by phagocytes, activity of COX enzyme, capillary permeability (effect on kinins), Ig production (at high doses). Overall anti-allergy effect.
o INCREASED: vasoconstriction of capillaries, numbers of PMN, production of lipocortins (annexin proteins that stabilize phospholipids in the cell membrane so they are not released to the arachidonic acid pathway that produces inflammatory mediators).
Other physiologic effects: o maturation of fetal lung – surfactant production in term fetus o helps maintain GFR in the kidney o antagonize vitamin D effects on calcium absorption in the gut (may reduce calcium
absorption and may cause hypocalcemia) osteoporosis o may reduce hematopoiesis (one of the controls on erythropoiesis in bone marrow) o reduce secretion of TSH & FSH (effects on growth, fertility) o stimulate acid/pepsin secretion by stomach parietal cells.
Overall results: Elevates blood glucose levels (excess amounts cause "adrenal diabetes" with moderate
response to insulin, more than in pituitary diabetes). o Liver: elevates blood glucose levels by stimulating hepatic gluconeogenesis; activates
DNA transcription in liver cell nuclei. o Somatic cells: reduced glucose utilization (poor glycolysis).
Reduces cellular protein everywhere (catabolism) except the liver (reduced synthesis, increased catabolism & mobilization of amino acids into bloodstream).
o (increases liver enzymes for this). o Somatic cells: If prolonged catabolism uses up structural proteins, then functional
(contractile) proteins will be used up, too (muscle atrophy). Mobilizes fatty acids:
o Adipocytes: mobilizes fatty acids o Somatic cells: increases utilization (oxidation) of FFA by cells for energy. Even so,
there is a particular adipose deposition seen in hyperadrenalism (moon facies, buffalo hump and chest/torso fat -- reason unknown)
Overall anti-allergy (immune/inflammatory cell inhibition) Fetal maturation (surfactant) (supports development/function of type-II alveolar cells) Gastric acid secretion (stimulates proton pump) Improved response to catecholamines – thus improves ventilation (enhanced response of
Beta-2 receptors to NE/EP)

Adv Pathophysiology Unit 10: Endocrine Page 13 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
Details of anti-inflammatory & immunosuppression effects: early & late stages. Blocks early stages:
o stabilizes lysosomal membranes o decreases WBC migration & phagocytosis o decreases capillary permeability o suppresses immune system -- especially T-lymphocytes o lowers fever by reducing release of interleukin-1 from WBC o prevents release of cell membrane phospholipid to arachidonic acid pathway and thus
prevents synthesis of inflammatory prostaglandins Resolution of inflammation:
o promotes healing by resolving inflammation o blocks cascade of increased inflammation.
Upregulates cellular receptors for anti-inflammatory substances: o upregulates receptors for catecholamines (?? mechanism)
Anti-allergy effects: o does not interfere with antibody-antigen complex formation o does block secondary inflammatory effects of allergic response
Immunosuppression: o reduces eosinophils & lymphocytes o causes atrophy of lymphoid tissue
Excess Cortisol from chronic EXOGENOUS (Pharmacologic) Administration OR endogenous pathological conditions: Even small amounts given pharmacologically are typically more than the endogenous amount
of cortisol produced by the body turns off system completely due to feedback (no endogenous cortisol secretion) and results in “HPA suppression” (more below)
Endogenous excess cortisol is seen in the setting of hyper adrenalism (Cushing’s disease) ANY excess cortisol situation is hypercortisolism (hypercorticism) & has adverse effects:
o Gastropathy (bleeding gastric ulcers, other GI bleeding) o Osteoporosis o Polycythemia o Adrenal diabetes (“chemical diabetes”) with hyperglycemia from insulin resistance
(impaired insulin sensitivity)Poor wound healing o Immuno-compromise and anti-inflammatory effects o Reduced linear growth in children (not improved by GH) o Avascular necrosis of the femoral head (in hip the blood supply to femoral head is
very fragile – arteriole vasoconstricts no more blood supply to hip necrosis) o Cataracts
Examples of therapeutic drugs: either fluorinated (more mineralocorticoid effects) or not. cortisone (= potency to endogenous) methylprednisone & prednisone (4 - 5 x potency) dexamethasone (30x potent, NO mineralocorticoid activity).

Adv Pathophysiology Unit 10: Endocrine Page 14 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
7. ADRENAL SEX HORMONES — Male & Female: MORE ON THIS IN REPRODUCTIVE MODULE – here for completeness only Androgens: moderately active male hormones most important are dehydroepiandrosterone (DHEA) and androstenedione they are converted to testosterone necessary for fetal and childhood male development
Testosterone: In order for Testosterone to be active at the tissue level, it must be converted to the active
form, called DHT (di-hydro-testosterone). Testosterone enzymatic conversion peripherally to DHT by enzyme 5-alpha-reductase Any testosterone left over is converted peripherally to estrogens !!
o exogenous use of androgenic drugs can actually cause a feminizing effect o “ergogenic aids” are drugs used by athletes that are androgen derivatives designed
to enhance muscle deposition and strength yet may have feminizing effect! (e.g. gynecomastia)
Female sex hormones: are secreted in tiny quantities as well.

Adv Pathophysiology Unit 10: Endocrine Page 15 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
HYPOADRENALISM SYNDROMES: Mineralocorticoid & cortisol deficiency Addison’s disease – deficiency of aldosterone and other adrenal hormones: lowered production of aldosterone
o this means LESS sodium reabsorption (retention) hyponatremia o this means LESS potassium (secretion) excretion hyperkalemia o this means LESS acid (secretion) excretion metabolic acidosis o this means LESS glucocorticoid activity as well
Etiology: o hypofunctioning adrenal glands – usually idiopathic o other causes are granulomatous disease (TB), tumor, amyloid deposition o there is a multiple endocrine syndrome called “polyglandular deficiency syndrome” o CHILDREN may be born with congenital adrenal hyperplasia (CAH)
lack of synthetic enzyme results in reduced synthesis of final product continued stimulation of adrenal gland causes hyperplasia of the gland
Clinical Findings of mineralocorticoid and glucocorticoid deficiency: o hypotension from volume contraction due to reduced Na reabsorption – in the kidney
as well as in sweat, saliva, and the GI tract (all locations of aldosterone activity) o hypotension from volume contraction – unable to concentrate the urine and so more
volume excreted o skin pigmentation (from increased melanin production) – remember that POMC
(propiomelanocortin) is broken down in the CNS to form endogenous opioids (endorphins) as well as ACTH (adrenocortical stimulating hormone) and MSH (melanocyte stimulating hormone)
o acidosis from impaired acid excretion o poor stress response o hypoglycemia
Lab Findings: o reduced glucocorticoid (cortisol) levels o reduced mineralocorticoid (aldosterone) levels o increased ACTH levels (pituitary is trying to stimulate the adrenal gland) o hemoconcentration (artificially elevated hematocrit from volume contraction) o hyponatremia and hyperkalemia with metabolic acidosis o hypotension
Adrenal (Addisonian) Crisis: o symptoms can be precipitated by stress (emotional OR physica) o stress can include infection, trauma, surgery, anesthesia, & even sodium loss from
excessive sweating o “SHOCK & FEVER” might be Addison’s
the infection causes the Addisonian crisis as well as the fever associated with hypoglycemia and depressed mentation
Treatment: o CHRONIC: Chronic management is DAILY oral prednisone and oral fludrocortisones o CRISIS: Acute management IMMEDIATE parenteral hydrocortisone with volume
expansion and sodium replacement (as needed) o See: http://emedicine.medscape.com/article/765753-treatment and Up To Date
https://www.uptodate.com/contents/adrenal-insufficiency-addisons-disease-beyond-the-basics

Adv Pathophysiology Unit 10: Endocrine Page 16 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
Congenital adrenal hyperplasia (CAH): Metabolic error with genetic enzyme deficiency or enzyme dysfunction Usually 21-hydroxylase deficiency with cortisol deficiency
o hypothalamus and pituitary continue to try to stimulate the adrenal gland o Adrenal gland can’t respond but does undergo mitotic hyperplasia as a result of the
overstimulation by ACTH Clinical:
o reduced amount of sterol synthesis (progesterone, estrogen, cortisones, aldosterone) o buildup of toxic intermediary metabolites o reduced cortisol and associated symptoms (see above Addison’s)
Incidence 1:5,000-15,000 (1:700 in Yupik Eskimo). Screening:
o universal neonatal heel-stick blood screening (21-hydroxylase deficiency screening) o infant diagnosis
1) Reduced cortisol due to deficiency of 21-OH enzyme 2) This reduces (impairs) the normal negative feedback to the hypothalamus and causes an increase in ACTH production (the hypothalamus is trying to stimulate the adrenal to make more cortisol) 3) The adrenal gland still can’t make cortisol, BUT it makes MORE of the androgens causing virilization
Adv Pathophysiology Unit 10: Endocrine Page 17 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
HPA axis suppression: Causes:
o usually due to exogenous corticosteroid treatment o sometimes a complication of heparin therapy
Pathology: o Exogenous corticosteroids suppress the hypothalamic production of CRH and the
pituitary production of ACTH o The adrenal therefore is not getting its normal stimulation to produce cortisol and
produces LESS cortisol o When the drug is taken away, it may take some time for the HPA communication to
be restored and normal cortisol production to resume – so we have hypoadrenalism
o The “rule of thumb” is that the longer you’ve received exogenous (drug) corticosteroid, that is how long you may have HPA axis suppression and hypoadrenalism
Symptoms: o Normally ASYMPTPOMATIC o BUT can result in similar presentation as Addisonian (Adrenal) crisis precipitated
by a stress (including surgery and anesthesia, infection) o
Clinical correlate: o Any dose over 5 mg prednisone/day for more than 2 weeks ANY time in the
preceding year o Even one dose of IM dexamethasone or triamcinolone counts for this!!
Clinical correlate – anesthesia implications of hypoadrenalism: o Glucocorticoid deficiency:
perioperative replacement of steroids usual is hydrocortisone 100 mg IV Q 8 h starting preop OR hydrocortisone 25 mg IV at induction, then 100 mg IV during surgery
o Mineralocorticoid deficiency: give preop mineralocorticoid such as fludrocortisones the fluorinated (halogenated) cortisones have mineralocorticoid activity
Adv Pathophysiology Unit 10: Endocrine Page 18 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
HYPERADRENALISM:
high levels of cortisol and/or related corticosteroids may include elevations of mineralocorticoid activity Cushing’s disease & syndrome: Two entities:
o Cushing's syndrome: chronic high blood levels of cortisol or related corticosteroids from any cause ACTH producing tumors (ectopic hormone production) adrenal hyperplasia or adrenal tumor
o Cushing's disease: excess pituitary production of ACTH (pituitary adenoma) Symptoms:
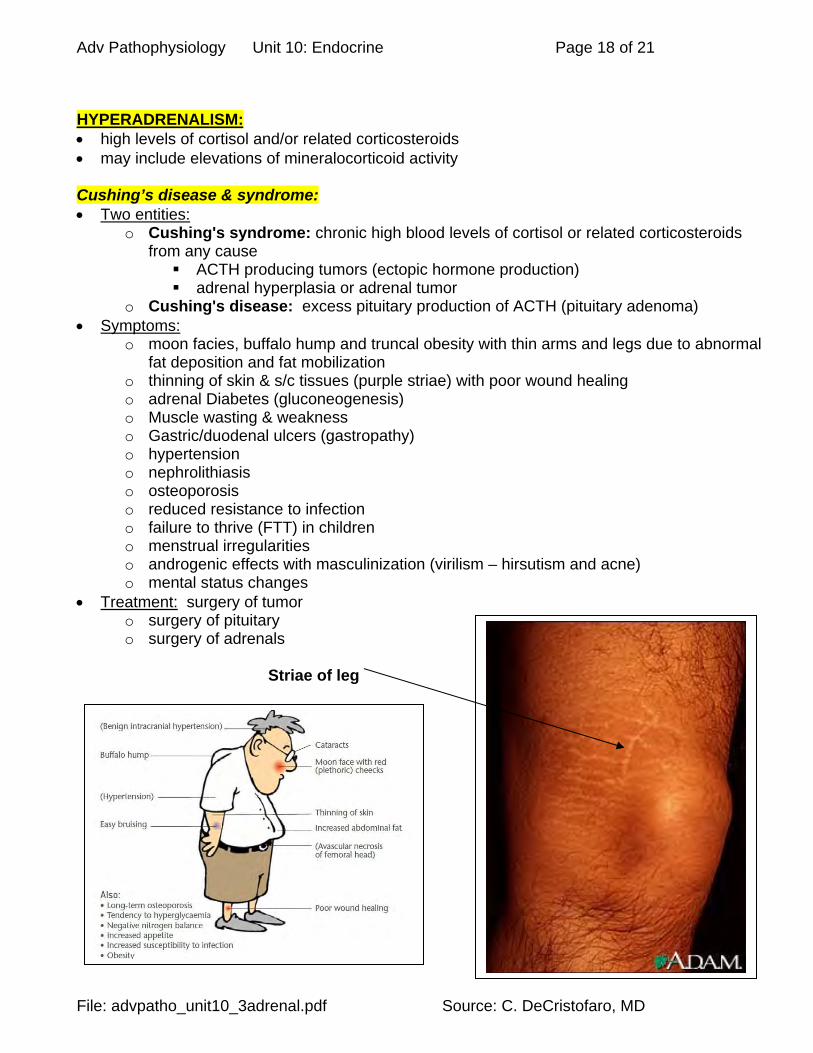
o moon facies, buffalo hump and truncal obesity with thin arms and legs due to abnormal fat deposition and fat mobilization
o thinning of skin & s/c tissues (purple striae) with poor wound healing o adrenal Diabetes (gluconeogenesis) o Muscle wasting & weakness o Gastric/duodenal ulcers (gastropathy) o hypertension o nephrolithiasis o osteoporosis o reduced resistance to infection o failure to thrive (FTT) in children o menstrual irregularities o androgenic effects with masculinization (virilism – hirsutism and acne) o mental status changes
Treatment: surgery of tumor o surgery of pituitary o surgery of adrenals
Striae of leg

Adv Pathophysiology Unit 10: Endocrine Page 19 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
Adrenogenital syndrome: virilizing adrenal tumors that produce mostly androgens. Symptoms:
o Usually pediatric o ambiguous genitalia or virilizing changes o Examples in real life: actresses Kim Novak, Jamie Lee Curtis
Lab: elevated 17-ketosteroids (derived from androgens). Primary aldosteronism (Conn’s syndrome): increased secretion of aldosterone which means:
o MORE sodium reabsorption hypernatremia o MORE potassium excretion hypokalemia o MORE acid excretion alkalosis
Pathology: o (very rare) unilateral tumor of zona glomerulosa cells (aldosteroma) o idiopathic hyperaldosteronism o bilateral adrenal hyperplasia o aldosterone secreting carcinoma of adrenal cortex
What about Cushing’s syndrome/disease? o this can also include hypersecretion of aldosterone o many of the findings in this condition, however, focus on the excess cortisol production
Clinical: o hypertension (one of the causes of secondary hypertension) o hypokalemia – muscle cramps, weakness, headaches, palpitations o metabolic alkalosis and reduced free (ionized) calcium with tetany o hypernatremia o hypervolemia o impaired glucose tolerance (i.e. prediabetes) due to hypokalemia impairing insulin
release and effect Treatment:
o surgical excision of tumor (called an “aldosterone producing adenoma” or APA) o medical management with potassium-sparing diuretic (e.g. spironolactone) and dietary
sodium restriction Secondary hyperaldosteronism: due to RAS activation Causes:
o HF, liver cirrhosis/ascites, nephrotic syndrome, diuretics – low volume states o renal artery stenosis – reduced renal perfusion o renin-secreting tumors o genetic syndromes such as Bartter & Gitelman – unable to reabsorb chloride and
salt & water wasting activate RAS causing hypokalemia & alkalosis; additionally, excessive NaCl delivery to distal nephron causes increased Na reabsorption and cotransport secretion of potassium causing hypokalemia; and, reduced chloride reabsorption results in reduced exchange for bicarbonate, causing bicarbonate retention & alkalosis.
Clinical: same as above Treatment: management of underlying condition
Adv Pathophysiology Unit 10: Endocrine Page 20 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
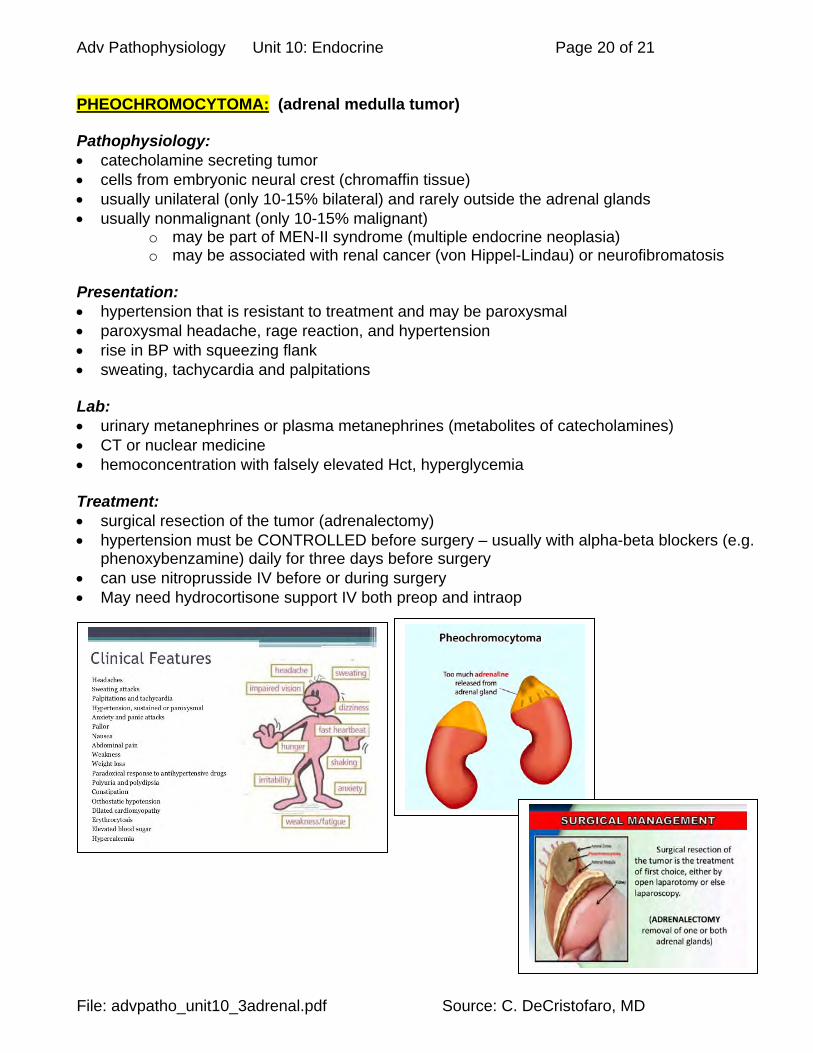
PHEOCHROMOCYTOMA: (adrenal medulla tumor) Pathophysiology: catecholamine secreting tumor cells from embryonic neural crest (chromaffin tissue) usually unilateral (only 10-15% bilateral) and rarely outside the adrenal glands usually nonmalignant (only 10-15% malignant)
o may be part of MEN-II syndrome (multiple endocrine neoplasia) o may be associated with renal cancer (von Hippel-Lindau) or neurofibromatosis
Presentation: hypertension that is resistant to treatment and may be paroxysmal paroxysmal headache, rage reaction, and hypertension rise in BP with squeezing flank sweating, tachycardia and palpitations Lab: urinary metanephrines or plasma metanephrines (metabolites of catecholamines) CT or nuclear medicine hemoconcentration with falsely elevated Hct, hyperglycemia Treatment: surgical resection of the tumor (adrenalectomy) hypertension must be CONTROLLED before surgery – usually with alpha-beta blockers (e.g.
phenoxybenzamine) daily for three days before surgery can use nitroprusside IV before or during surgery May need hydrocortisone support IV both preop and intraop

Adv Pathophysiology Unit 10: Endocrine Page 21 of 21
File: advpatho_unit10_3adrenal.pdf Source: C. DeCristofaro, MD
PRADER-WILLI SYNDROME: Genetic disorder: example of genomic imprinting – some genes are active only on the copy inherited from the
father (paternal copy) ; if this is DELETED then the child has no function since the maternal copy is not turned on
o deletion is on part of paternally derived chromosome 15 results in hypothalamic dysfunction and a host of abnormalities in development and behavior many complications Findings: hypotonia with poor suck (may need gavage feedings) and weak cry genital hypoplasia with cryptorchidism (males) and delayed menses (girls)
1. this hypogonadism causes osteoporosis & risk of pathologic fracture developmental delay hyperphagia and food foraging obesity with central apnea and complications of pulmonary hypertension and right heart
failure (cor pulmonale with RVH) short stature and GH deficiency behavioral issues including obsessive-compulsive disorder & mild mental retardation (varies) high pain threshold and high threshold for emesis may develop scoliosis Surgical procedures: management of cryptorchidism or neoplasias (Wilms tumor, testicular neoplasia) management of slipped capital femoral epiphyses (SCFE) usually between the ages of 12-
16 yo for surgical screw fixation o complication of chondrolysis (destruction of articular cartilage) o complication of avascular necrosis of femoral head (loss of hip)