learning objectives for this filepeople.musc.edu/~decristc/adv patho/unit 6 pulmonary... ·...
TRANSCRIPT

Advanced Pathophysiology Unit 6 Page 1 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Learning objectives for this file: 1. Describe the clinical presentation and pathophysiology of acute bronchitis 2. Describe COPD pathophysiologic types and clinical presentation 3. Understand the pathophysiologic compensations and complications of COPD 4. Review common management approaches to COPD 5. Describe clinical aspects of asthma-COPD overlap syndrome (ACOS). 6. Understand the pathophysiology of cor pulmonale, pulmonary hypertension, and related conditions CYSTIC FIBROSIS: see later GI module – condition has GI plus Pulmonary findings. SCLERODERMA: remember this content from prior notes – pulmonary fibrosis is a presenting problem.

Advanced Pathophysiology Unit 6 Page 2 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
ACUTE BRONCHITIS – “COUGH ILLNESS”: • acute inflammation of the tracehobronchial tree • self-limited & with eventual complete healing & return of function. • Mild disease, but may be serious in patients with underlying pulmonary or cardiac (or
other systemic) disease. • Complication: Pneumonia and/or pleurisy. PATHOPHYSIOLOGY: • acute infectious syndrome (prevalent in winter) • acute irritative syndrome (fumes, dusts, chemicals) • DDX cough-variant asthma.
o mucus membrane hyperemia, desquamation, edema, WBC infiltration, mucopurulent exudate, impaired cilia, phagocytes, lymphatics.
o may cause spasm o Can lead to acute respiratory failure in those with chronic pulmonary disease.
PRESENTATION: • prodrome of URI (coryza, malaise, chills, low grade fever, back/muscle pain, sore throat) • cough is diagnostic of acute bronchitis. • if persists, change in sputum, fever, debility, pulmonary embarrassment antibiotics • Exam:
o adventitious sounds (rhonchi, crackles, rales, wheezing) o especially consider dx. if wheeze after the cough -- differential from asthma,
coughing will often clear the wheezing). WORKUP: • CXR • ABG • sputum culture/gram stain TREATMENT: • rest • fluids • antipyretic analgesic (not ASA -- Reye's syndrome) • anti-tussive • mucolytics • Antibiotics are CONTROVERSIAL and may be used in persistent fever or purulent
sputum, or complicated presentation (underlying morbidity such as COPD, asthma, DM). A concern of the CDC is inappropriate use of antibiotics in Acute Bronchitis: Background: http://www.cdc.gov/getsmart/community/materials-references/print-materials/hcp/adult-acute-cough-illness.html Fact sheet: http://www.cdc.gov/getsmart/community/materials-references/print-materials/hcp/adult-acute-cough-illness.pdf

Advanced Pathophysiology Unit 6 Page 3 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
CHRONIC OBSTRUCTIVE PULMONARY (LUNG) DISEASE (COPD)(COLD): • This condition includes both chronic bronchitis (Type B) & emphysema (Type A) • Recently popular acronym has been COLD (for chronic obstructive lung disease) • Findings of generalized persistent A/W obstruction Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Bethesda (MD): Global Initiative for Chronic Obstructive Lung Disease, World Health Organization, National Heart, Lung and Blood Institute; 2017 GOLD Pocket Guide for Clinicians at: http://goldcopd.org/wp-content/uploads/2016/12/wms-GOLD-2017-Pocket-Guide.pdf Other guideline developers include the American Thoracic Society (ATS), American College of Physicians (ACP), American College of Chest Physicians (ACCP), European Respiratory Society (ERS). Clinical: • Mid-life onset, slowly progressive symptoms, usual smoking history of 10-20 pack years • Dyspnea during exercise, which often progresses to dyspnea at rest • Largely irreversible airflow limitation which MAY include a reversible bronchospastic
component • Remember relative contraindications to use of beta-blockers (including selective types). • Evaluate for underlying infection as a cause for exacerbation
o change in color of sputum, fever • Newer guidelines are more conservative regarding antibiotics, and include use of more
inhaled corticosteroids
Comorbidities: • common in COPD and should be actively identified • comorbidities often complicate the management of COPD, and vice versa
Airway obstruction: • with increased resistance to airflow during forced expiration. • causes long expiratory phase of ventilation. Pathophysiology: main cause is SMOKING!! • narrowing or obliteration of AW due to AW disease
o includes both large and small airways o N Engl J Med, 27 Oct 2011, at:
http://www.nejm.org/doi/full/10.1056/NEJMoa1106955 • expiratory collapse of AW due to pulmonary emphysema • most patients have elements of the different diseases:
o alveolar destruction, obstructive disease, partial reversibility o difficult to discuss diseases as completely separate entities.
• large AW cause some symptoms, but severity of disease depends on small AW destruction.

Advanced Pathophysiology Unit 6 Page 4 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Recognition: (from GOLD) • A clinical diagnosis of COPD should be considered in any patient who has dyspnea,
chronic cough or sputum production, and/or a history of exposure to risk factors for the disease.
• The diagnosis should be confirmed by spirometry. • For the diagnosis and assessment of COPD, spirometry is the gold standard as it is the
most reproducible, standardized, and objective way of measuring airflow limitation. • The presence of a postbronchodilator FEV1/FVC <0.70 and FEV1 <80% predicted
confirms the presence of airflow limitation that is not fully reversible. • Health care workers involved in the diagnosis and management of COPD patients should
have access to spirometry. • Assessment of COPD severity is based on the patient's level of symptoms, the severity of
the spirometric abnormality, and the presence of complications. • Measurement of arterial blood gas tensions should be considered in all patients with
FEV1 <50% predicted or clinical signs suggestive of respiratory failure or right heart failure.
• COPD is usually a progressive disease and lung function can be expected to worsen over time, even with the best available care.
• Symptoms and objective measures of airflow limitation should be monitored to determine when to modify therapy and to identify any complications that may develop.

Advanced Pathophysiology Unit 6 Page 5 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Epidemiology: • in USA is #2 after heart disease as cause of Social Security disability. • Prevalence is increasing • gender: men > women (although gap is narrowing). Diagnostic Testing: • CXR:
o increased AP diameter, hyperinflation, increased retrosternal space, chronic para-hilar markings, bullae.
o CXR are normal in chronic bronchitis. • Lung scans demonstrate V/Q abnormatlities (inequalities). • Spirometry:
o progressive obstructive changes (reduced FEV1) and eventually also volume changes (VC & FVC).
o FEV1/VC ratio is < 60% despite aggressive treatment -- confirms diagnosis. • CBC: Eosinophilia may be present on CBC, eventually secondary polycythemia. Complications: • Cor pulmonale (Right ventricular hypertrophy & pulmonary edema ) • Chronic hypoxemia leads also to secondary polycythemia (raise your CV risk) Natural history of COPD:
• progressive worsening with continued smoking • designations of severity determined by the “BODE” index (The Body-Mass Index,
Airflow Obstruction, Dyspnea, and Exercise Capacity Index in Chronic Obstructive Pulmonary Disease), see (2004): http://www.nejm.org/doi/full/10.1056/NEJMoa021322

Advanced Pathophysiology Unit 6 Page 6 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
STAGES OF COPD: (definitions vary by professional agency) American Thoracic Society (ATS) stages of severity: Spirometry should be performed after the administration of an adequate dose of an inhaled bronchodilator; from http://annals.org/article.aspx?articleid=479627 Note – this guideline developer uses Stages 0, I, II, III, IV
“Stage 0” (at risk): many don’t recognize that a “Stage 0” is a real stage • chronic symptoms of cough and sputum, exposure to risk factors • Normal spirometry – FEV1 80% or greater • No medication • Recommend avoidance of risk factors, aggressive immunization and do this for all higher
stages of illness Stage I (mild COPD(GOLD 1): • FEV1/FVC < 70%, FEV1 > 80% predicted, with or without symptoms • Medication: add short-acting BDs as needed Stage II (Moderate COPD)(GOLD 2): • FEV1/FVC < 70%, FEV1 < 50-70% predicted • Medication: continue short-acting BDs PRN, add long-acting BDs (1 or more),
pulmonary rehabilitation, ?? ICS if good response `
Stage III (Severe COPD)(GOLD 3): • FEV1/FVC < 70%, FEV1 < 50% predicted • Medication: continue short-acting BDs PRN, add long-acting BDs (1 or more),
pulmonary rehabilitation, ICS if repeated exacerbations Stage IV (Very Severe COPD)(GOLD 4): • FEV1/FVC < 70%, FEV1 < 30%, plus chronic respiratory failure (or right heart failure). • Medication: continue short-acting BDs PRN, add long-acting BDs (1 or more),
pulmonary rehabilitation, ICS if good response • treat complications & consider surgery • long-term Oxygen therapy (LTOT) if respiratory failure

Advanced Pathophysiology Unit 6 Page 7 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
American College of Physicians (ACP) stages of severity: Spirometry should be performed after the administration of an adequate dose of an inhaled bronchodilator; from http://annals.org/aim/fullarticle/479627/diagnosis-management-stable-chronic-obstructive-pulmonary-disease-clinical-practice-guideline#UsingSpirometrytoScreenforAirflowObstructionorDiagnoseCOPD
Note – this guideline developer uses Stages 0, I, II, III, IV GOLD 2017 stages of severity: Spirometry performed after administration of adequate dose of inhaled bronchodilator
Figure 1:Spirometric Classification of COPD Severity Based on Post-Bronchodilators FEV1
Stage I: Mild FEV1/FVC <0.70 FEV1 >80% predicted
Stage II: Moderate FEV1/FVC <0.70 50% <FEV1 <80% predicted
Stage III: Severe FEV1/FVC <0.70 30% <FEV1 <50% predicted
Stage IV: Very Severe
FEV1/FVC <0.70 FEV1 <30% predicted or FEV1 <50% predicted plus chronic respiratory failure (needs long-term oxygen therapy)
Advanced Pathophysiology Unit 6 Page 8 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
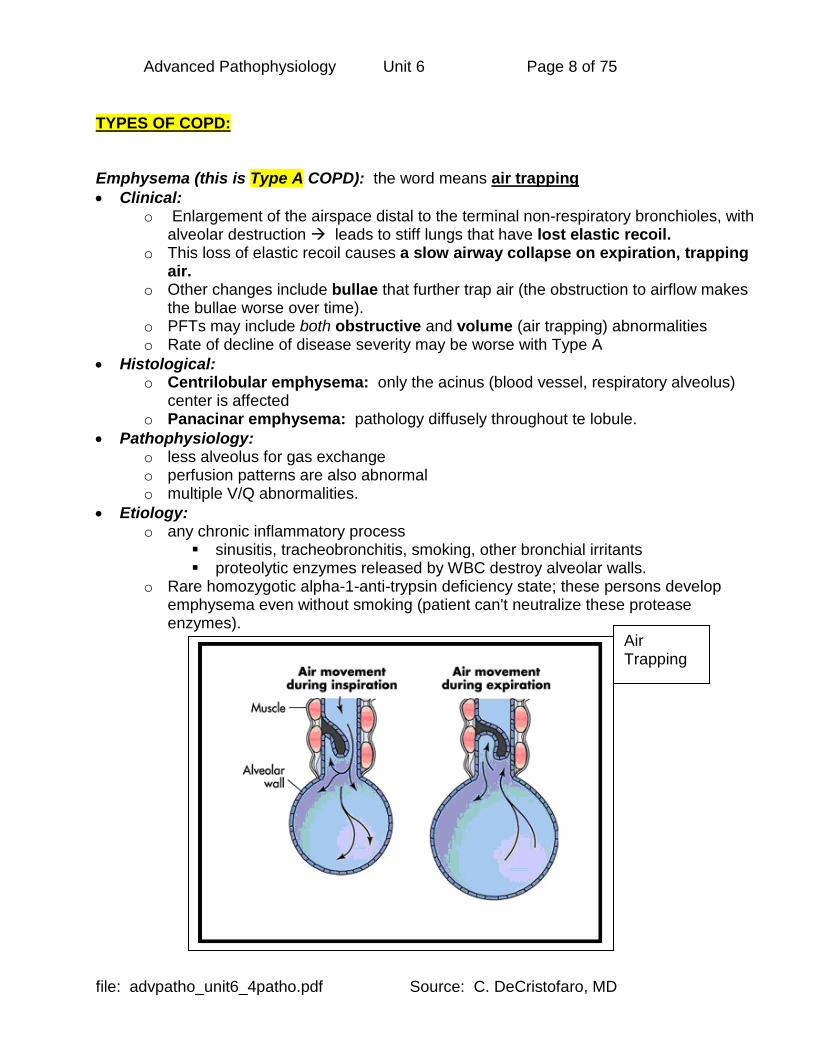
TYPES OF COPD: Emphysema (this is Type A COPD): the word means air trapping • Clinical:
o Enlargement of the airspace distal to the terminal non-respiratory bronchioles, with alveolar destruction leads to stiff lungs that have lost elastic recoil.
o This loss of elastic recoil causes a slow airway collapse on expiration, trapping air.
o Other changes include bullae that further trap air (the obstruction to airflow makes the bullae worse over time).
o PFTs may include both obstructive and volume (air trapping) abnormalities o Rate of decline of disease severity may be worse with Type A
• Histological: o Centrilobular emphysema: only the acinus (blood vessel, respiratory alveolus)
center is affected o Panacinar emphysema: pathology diffusely throughout te lobule.
• Pathophysiology: o less alveolus for gas exchange o perfusion patterns are also abnormal o multiple V/Q abnormalities.
• Etiology: o any chronic inflammatory process
sinusitis, tracheobronchitis, smoking, other bronchial irritants proteolytic enzymes released by WBC destroy alveolar walls.
o Rare homozygotic alpha-1-anti-trypsin deficiency state; these persons develop emphysema even without smoking (patient can't neutralize these protease enzymes).
Air Trapping

Advanced Pathophysiology Unit 6 Page 9 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Chronic bronchitis (Type B COPD): • develop in anyone with enough bronchial irritation – typically, smoking • Can be last development in chronic asthma. • Prolonged exposure to nonspecific bronchial irritants and accompanied by mucus
hypersecretion & structural changes in the bronchi. • Includes chronic productive cough. • Due to cigarette smoking, and/or other inhaled irritants. • Pathology:
o Bronchial walls are thickened o mucus in lumen o goblet cells increased o mucus glands increased in size
• Newer theories consider that COPD may be an “adaptive immunity” (auto-immune) condition in which damaged cells from smoking release cytokines that stimulate the immune system to create cytotoxic T-lymphocytes that then cause the specific type of tissue damage seen in COPD – this may also help explain the variability in development of COPD among smokers
Cosio MG, et al. Immunologic Aspects of Chronic Obstructive Pulmonary Disease. N Engl J Med June 4, 2009;360(23):2445-54.
Advanced Pathophysiology Unit 6 Page 10 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Related entities: • Chronic asthmatic bronchitis:
o chronic airflow obstruction due asthma, even with maximal treatment, that is due to chronic asthma without complete reversal of AW narrowing.
o But, less abnormalities seen, better response to bronchodilators (often normal CXR, usually h/o asthma, rarely cor pulmonale, usually hypoxemia, rarely hypercapnia, usual eosinophilia).
• Chronic obstructive bronchitis: o small AW disease with clinically significant obstruction. o "respiratory bronchiolitis"
• Asthma-COPD overlap syndrome (ACOS): o Many adults present with symptoms of both illnesses o Diagnosis and treatment is a challenge
ACOS information from GINA:

Advanced Pathophysiology Unit 6 Page 11 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD

Advanced Pathophysiology Unit 6 Page 12 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
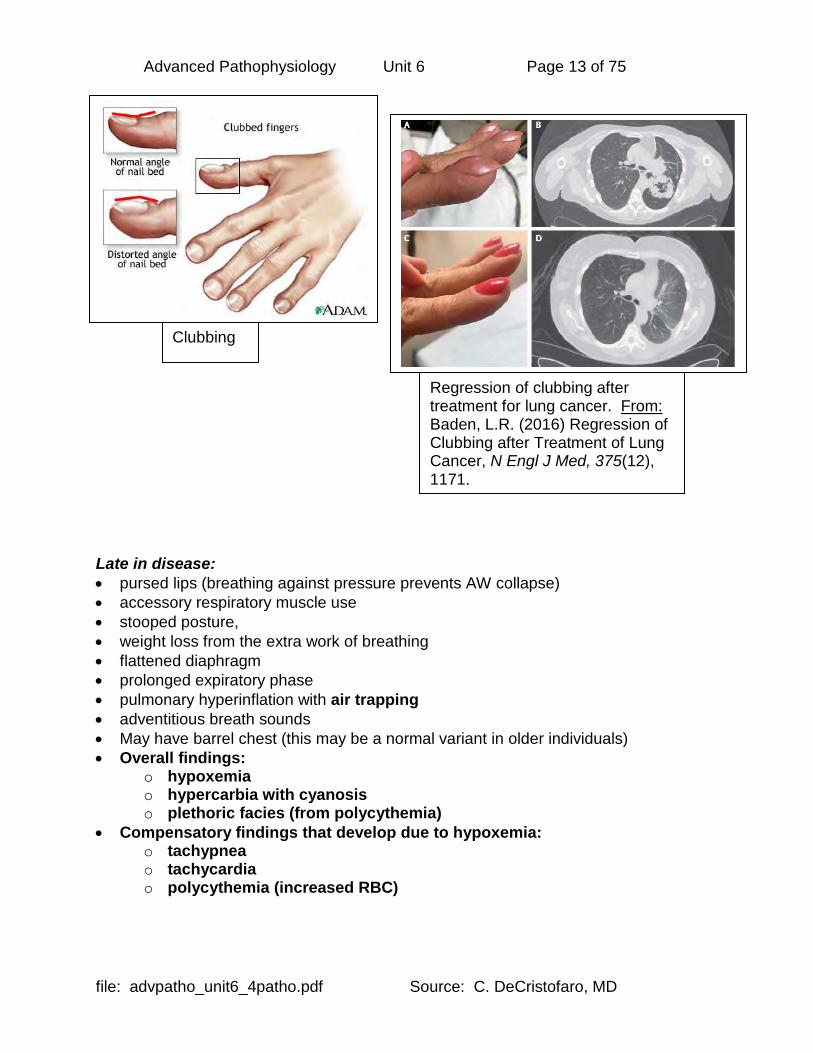
Clinical presentation of COPD: • Clubbing (occur with ANY hypoxic state) • cor pulmonale (RVH) • HF & edema • Sleep disorders occur (sleep apnea and daytime somnolence) • continuum from early adulthood. • Serial spirometry will demonstrate disease before symptoms develop. • Gradual progressive dyspnea (starts exertional, end stages is also at rest on room air). • Individual presentation varies in degree of subjective and objective symptoms & signs. • All have obstruction, with slowing of forced expiration. • Hypercapnia (increased arterial CO2)
o Due to reduced gas exchange secondary to alveolar damage o Due to hypoxic vasoconstriction and worsening of V/Q mismatch o Due to the “Haldane” effect which reduces the ability of hemoglobin to
exchange oxygen for carbon dioxide in the face of large amounts of dissolved CO2 in the blood
Overall findings: • hypoxemia • hypercarbia with cyanosis • plethoric facies (from polycythemia) Compensatory findings that develop due to hypoxemia: • tachypnea • tachycardia • polycythemia (increased RBC) Casual terminology:
• Sometimes you’ll hear clinicians talk about two different types of COPD patients: o "Pink puffers"
• actually have large amount of destroyed tissue • good ventilatory drive • however lack reserve pulmonary capacity.
o "Blue bloaters" • have hypercapnia with hypoxemia and often pulmonary HTN with cor
pulmonale • may have some reserve for exertion/illness.
Advanced Pathophysiology Unit 6 Page 13 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Late in disease: • pursed lips (breathing against pressure prevents AW collapse) • accessory respiratory muscle use • stooped posture, • weight loss from the extra work of breathing • flattened diaphragm • prolonged expiratory phase • pulmonary hyperinflation with air trapping • adventitious breath sounds • May have barrel chest (this may be a normal variant in older individuals) • Overall findings:
o hypoxemia o hypercarbia with cyanosis o plethoric facies (from polycythemia)
• Compensatory findings that develop due to hypoxemia: o tachypnea o tachycardia o polycythemia (increased RBC)
Clubbing
Regression of clubbing after treatment for lung cancer. From: Baden, L.R. (2016) Regression of Clubbing after Treatment of Lung Cancer, N Engl J Med, 375(12), 1171.

Advanced Pathophysiology Unit 6 Page 14 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Treatment: no cure. Progression stops when d/c smoking (exposure to cause) • Since disease includes tissue destruction, once destruction occurs, it is irreversible. • Stop smoking: MUST STOP EXPOSURE TO IRRITANTS (SMOKING) !! • Condition is progressive as long as smoking continues • Infection: Goals are eradication and early treatment of infection • Bronchodilatation: same medications as in asthma, with less dependence on steroid
therapy unless there is a strong asthmatic component, plus more emphasis on anticholinergics, hydration and chest PT with nebulizer therapy (prevent inspissation).
• Oxygen therapy: 24-hr oxygen therapy can discourage anaerobic infections. Criteria for specific therapy:
1) CPAP (continuous positive airway pressure) 2) LTOT (long term oxygen therapy) should be used in those with PaO2 < 55
mm Hg (O2 sat < 88%) while at rest & awake; or in those with polycythemia (Hct > 55%) , pulmonary hypertension, right heart failure, hypercapnia (PCO2 > 45 mm Hg).
3) Be sure that PaO2 is not rising above 65 torr (rise above this can result in loss of hypoxemic respiratory drive in face of chronic hypercapnia).
• Acid-base abnormalities: o Chronic respiratory acidosis leads to metabolic compensations of renal
reabsorption and generation of bicarbonate (base) so there will be an increase of HCO3- on ABG.
o Respiratory depression is common, and exacerbations need prompt, aggressive treatment.
o Avoid sedatives & hypnotics that depress respiratory drive. Other clinical concerns COMPLICATIONS: • Careful cardiac followup for cor pulmonale (cardiac complication of lung disease) • Pulmonary HTN treatments are not promising • Phlebotomy may be necessary for polycythemia.
o Anti-thrombotics for polycythemia (prothrombotic, hypercoaguable state) Alpha-1-anti-trypsin deficiency patients: • available (expensive) weekly iv Prolastin (alpha1-proteinase inhibitor replacement
therapy) as long as pt. is not smoking. • Critical to avoid ALL smoke in environment Mucolytics:
• drugs and just plain water hydration • exercise (mucociliary clearance) • postural drainage
Prophylaxis: aggressive vaccination (annual influenza, PPV boosted Q 5-7 yrs) Nutrition: Medical Nutrition Therapy (MNT)
• reduce the “respiratory ratio” refer nutritionist/dietician for prescribed diet • carbohydrate percentage of diet is reduced this reduces the amount of CO2
produced from food, and may help the hypercapnia

Advanced Pathophysiology Unit 6 Page 15 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
COR PULMONALE & SECONDARY PULMONARY HYPERTENSION: • RV enlargement secondary to lung disease • Produces secondary pulmonary artery HTN
o Does not refer to RV enlargement due to LV failure or any other cardiac causes. • Results in clinical picture of right heart failure. • Cor pulmonale also causes increased risk of thromboembolism and pt. may require long
term AC therapy. Common cause: COPD Other causes: • primary (idiopathic) pulmonary HTN • lung tissue loss (surgery, trauma) • scleroderma • diffuse interstitial fibrosis • kyphoscoliosis • obesity with alveolar hypoventilation • neuromuscular disease of the respiratory muscles. Acute cor pulmonale: • with pulmonary embolus • or with exacerbation of COPD. Article on secondary pulmonary hypertension: http://emedicine.medscape.com/article/303098-overview
Advanced Pathophysiology Unit 6 Page 16 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
PRIMARY PULMONARY HYPERTENSION: • areas of hypoperfusion & hyperperfusion somewhat similar to babies with RDS • various etiologies:
o idiopathic (genetic) o primary (drug induced) o mountain sickness
Pathophysiology: poorly understood, some theories • May be a dysregulation of sensitivity to low CO2 in the brain • May be due to dysregulation of pulmonary circulation upon exposure to hypoxia or Treatment: • diuretics, oxygen, inhaled or IV nitric oxide (NO), sildenafil (Viagra) and other vasodialtors
to vasodilate pulmonary vessels. • Lowering pulmonary arteriolar/capillary pressure reduces edema formation in over-
perfused areas, and improves perfusion in under-perfused areas. Primary pulmonary arterial hypertension (PAH): • associated with a genetic mutation called the BMPR2 gene • progressive and fatal within a few years • eventually, lung transplantation is needed – newer vasodilating drugs offer hope. Primary pulmonary hypertension (PPH): • develops as a complication of the use of anorexiant drugs. • Associated with cardiac valvular damage • Similar to Idiopathic Pulmonary HTN in presentation, also fatal Article on Primary pulmonary hypertension: http://emedicine.medscape.com/article/301450-overview

Advanced Pathophysiology Unit 6 Page 17 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
SUPERIOR VENA CAVA SYNDROME (SVCS): What is it? • compression of SVC
o this is the major drainage vessel for head, neck, upper extremities, upper thorax o in middle mediastinum and surrounded by sternum, trachea, right bronchus,
aorta, pulmonary artery, lymph nodes o goes along the right side of the mediastinum, where it can be compressed
• may include tracheal narrowing • may include obstruction of pulmonary arteries or veins Clinical factors: • usually associated with bronchogenic carcinoma (second cause is lymphoma) • may be associated with thrombus, especially if indwelling catheter • radiation is necessary to treat the SVC syndrome • drainage around the compressed SVC occurs via
o azygous & hemiazygous veins, intercostal veins, internal mammary veins

Advanced Pathophysiology Unit 6 Page 18 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Clinical presentation: • dyspnea, cough, orthopnea • swelling of trunk, upper extremity, face (“facial engorgement”) especially if raises arms • headache, nasal stuffiness • on exam, there may be jugular venous distension • if due to lung cancer, may have other associated findings (Horner syndrome, paralysis of
vocal cords, paralysis of phrenic nerve) Imaging: • chest Xray with widened mediastinum on the right • CT & MRI show the obstruction more clearly • other tests include venography, nuclear medicine scan, gallium scan Treatment: • corticosteroids & diuretics for laryngeal or cerebral edema • radiation therapy and maybe chemotherapy (for the tumor) • surgical SVC stenting
Large right paratracheal mass compressing SVC

Advanced Pathophysiology Unit 6 Page 19 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
ASPIRATION SYNDROMES: • foreign substances inhaled into the lungs (usually oral or gastric)
o normal protection against aspiration is the cough reflex, pulmonary macrophages, and the mucociliary escalator
o we typically aspirate while sleeping quite commonly, but normal protective mechanisms prevent complications of chemical pneumonia or bacterial pneumonia
o other reasons for complications of aspiration or massive aspiration may involve swallowing dysfunction or other inability to control swallowing (e.g. anesthesia)
• sequelae include damage to the lungs with respiratory compromise • can be fatal if massive (up to 25% fatality with massive aspiration) Mechanism: • normal swallowing:
o oral phase provides bolus that triggers swallowing reflex o pharyngeal phase includes laryngeal elevation and clo o closure of epiglottis, aryepiglottic folds, and true and false vocal cords – this is
what normally PREVENTS aspiration o esophageal phase when bolus passes through relaxed cricopharyngeal muscle
and enters the esophagus • abnormal swallowing:
o bolus enters hypopharynx before closure of laryngeal sphincters o DIRECT ASPIRATION: aspiration of bolus while swallowing o INDIRECT ASPIRATION: aspiration of refluxed food from stomach that enters
esophagus and then the lung Clinical presentation: • Pulmonary: wheezing from bronchospasm (if from GERD, possibly more nocturnal),
apnea with cyanotic episodes, stridor, hoarseness, sore throat, purulent sputum, chronic cough, tachypnea,
• Systemic: night sweats, fever Infant – meconium aspiration: • meconium occurs in the amniotic fluid after 34 weeks GA (contains blood, minerals, lipids) • aspiration can occur in utero or during birth passage • pathophysiology:
o chemical pneumonitis and inactivation of surfactant (from bile salts), air trapping
o if meconium staining is seen at delivery (10-15%), of these babies, 5-15% develop meconium aspiration syndrome
o baby is cyanotic, has tachypnea, tachycardia, nasal flaring, intercostal retractions
o chest Xray eventually shows patchy infiltrate, hyperaeration, pneumomediastinum, pneumothorax
• management: ET tube suctioning, steroids, surfactant via ET tube, positive pressure ventilation

Advanced Pathophysiology Unit 6 Page 20 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Pediatric: • Causes:
o Muscular: Cricopharyngeal dysfunction, cricopharyngeal incoordination of infancy, and transient pharyngeal muscle dysfunction, GER(D)
o Neurological: Isolated superior laryngeal nerve damage, vocal cord paralysis, cerebral palsy, muscular dystrophy, and Riley-Day syndrome (ie, familial dysautonomia)
o Anatomic: cleft palate, esophageal atresia, tracheoesophageal fistula, duodenal obstruction, or malrotation
• Management: o “back to bed” after feeding (do not sit up) o thickening formula or breast milk with rice cereal, small frequent meals o using proton pump inhibitors (PPI) for suspected GERD o surgery
for GERD – a Nissen fundoplication and gastrostomy for neurological impairment – a variety of laryngeal procedures (but
these remove ability to phonate)
Nissen fundoplication for GERD Adult: • pathophysiology:
o materials enter right lung more easily due to angle of right mainstem bronchus o upright posture causes materials to enter lower lobes o supine position causes materials to enter apical segment of lower lobes or
posterior segment of upper lobes • causes:
o depressed gag reflex from anesthesia (e.g. Mendelson syndrome – chemical pneumonia caused by aspiration of gastric juices)
o neurologic – such as bulbar palsy (disease affecting cranial nerves of articulation, (VII - XII), myasthenia gravis, cerebral palsy, Parkinson disease
o impaired consciousness (seizure, trauma with LOC, substance abuse – alcoholism)
o GER(D) o esophageal stricture or tracho-esophageal fistula o naso-gastric feeding tube o possibly treatment with anti-acid medications (H2B, PPI) since bacteria
normally inactivated by gastric acid are able to flourish • presentation:
o systemic – fever, headache, nausea & vomiting, anorexia, myalgia, weight loss o pulmonary – cough, tachypnea, dyspnea, pleuritic chest pain, purulent sputum o findings on examination – decreased breath sounds if consolidation, pleural rub
• complications: o bacterial pneumonia – may progress to bronchiectasis or lung abscess o chemical pneumonia (see more below)

Advanced Pathophysiology Unit 6 Page 21 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Chemical pneumonia (Mendelson’s syndrome): • first described in 1946 in OB patients undergoing anesthesia • pathophysiology:
o more likely if pH low (<2.5) and volume of aspirate high (>0.3 mL/kg – i.e. about 25 mL in adults)
o chemical burn from acid (usually severe if pH < 2.5) o inflammation follows with early and late cytokines (TNF & interleukin-8)
• presentation: o very acute (within 2 hours of aspiration) o tachypnea, wheezing, cough with frothy or pink sputum
• treatment: o antibiotics are used if CP continues beyond the initial period o use trans-tracheal aspirate to obtain sputum for microbiology & antibiotic choice o aggressive antibiotics also indicated based on comorbidities o may require intubation with positive pressure ventilation
Near drowning (an aspiration syndrome): • Presentation:
o may aspirate water, or laryngospasm may keep water out o both types have severe hypoxia.
• Management: o Water is usually absorbed from the lung into the circulation, so concentrate on
PROVIDING VENTILATION and monitoring cardiac activity. o Can use PEEP o Sequelae of respiratory arrest (& complications of acidosis) & cerebral edema
to prevent cerebral edema from hypoxia, must used osmotic diuretics hyperventilate to reduce PCO2 to 25 torr range may need ventriculostomy.
• Prognosis: o Good prognosis seen with submersion < 9 min, prehospital CPR < 25 min, regaining
consciousness after resuscitation, and immersion in cold water (slows metabolism & reduces hypoxic damage).
Bacterial pneumonia from aspiration: see below

Advanced Pathophysiology Unit 6 Page 22 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
TRACHEAL FOREIGN BODY (FB): • child is usually < 4 yrs old, but may be older (MR child, or while holding object in mouth for
some reason). • Even with Xray workup, only 60% of true FB diagnosis is made (proceed to management
if clinical suspicion exists). Presentation: • wheezing, persistent pneumonia, stridor, coughing, apnea. • Croup that doesn't improve in 5 days may be an undiagnosed FB • unilateral absence of breath sounds, hemoptysis, stridor, wheezing Workup: • CXR may be positive for hyperinflation of the obstructed lung (bronchus constricts during
expiration, trapping air that may be admitted during inspiration) & a mediastinal shift away from the obstructed side during expiration.
• CT scan thorax may be necessary. Anatomy: • The FB will TEND TO GO INTO THE RIGHT MAIN BRONCHUS, DUE TO ANATOMY --
BUT ALSO COUGHED OUT OF HERE MORE EASILY, SO ALMOST AS MANY FOUND ON LEFT MAIN BRONCHUS CLINICALLY.
• Esophageal FB may be large enough to compress trachea as well. Prevention: • Especially avoid as foods are: nuts, hot dogs, raw carrots in young children • Also, avoid using toys with small parts (age 3 y/o or younger given as age limit for toys
with small parts). • Use a cardboard toilet tissue tube to see if item a choking hazard. • Often, pacifiers sold for infant use are later recalled due to reports of fatal aspiration of
parts try to have caregivers use only solid one-piece pacifiers. Management: • only use finger-sweep if child is NOT breathing (no air movement IN or OUT). • If continues to have air movement, only try to dislodge with finger under DIRECT
visualization (may also push FB further down and occlude trachea worse, and move the FB beyond reach).
• May need to use emergency tracheostomy to maintain airway. • Usual management includes laryngoscopy or bronchoscopy under anesthesia, in the O.R. Support: • edema of airway plus instrumentation • need followup antibiotics, oxygen, corticosteroids, mist, chest PT.

Advanced Pathophysiology Unit 6 Page 23 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
PNEUMONIA: • may be bacterial or viral • airspace disease and consolidation • air spaces are filled with bacteria or other microorganisms AND exudate (pus) • types of pneumonia by CXR:
o Lobar - classical Pneumococcal pneumonia, entire lobe consolidated and air bronchograms common
o Lobular - often Staphlococcus, multifocal, patchy, sometimes without air bronchograms
o Interstitial - Viral or Mycoplasma; latter starts perihilar and can become confluent and/or patchy as disease progresses, no air bronchograms
o Aspiration pneumonia - follows gravitational flow of aspirated contents; impaired consciousness, post anesthesia, common in alcoholics, debilitated, demented pts; anaerobic (Bacteroides and Fusobacterium)
o Diffuse pulmonary infections - community acquired (Mycoplasma, resolves spontaneously) nosocomial (Pseudomonas, debilitated, mechanical vent patients, high mortality rate, patchy opacities, cavitation, ill-defined nodular) immunocompromised host (bacterial, fungal, Pneumocystis carinii, PCP)
Infiltrate (consolidation) on CXR from RML pneumonia

Advanced Pathophysiology Unit 6 Page 24 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
COMMUNITY ACQUIRED PNEUMONIA (CAP): • microbes include Strep pneumoniae, H. influenzae, Chlamydia pneumoniae, Mycoplasma
pneumoniae; sometimes Legionella, Staph aureus, respiratory viruses, endemic fungi, aerobic gram-negs, metapneumovirus
• Atypical CAP: o cough, little or no purulent sputum, fatigue. o Often called “walking pneumonia” o CXR may be negative for a month or more during initial stages o caused by Mycoplasma pneumonia may account for up to 50% of all CAP. o can also attack other viscera (spleen, even spinal cord!) o can also be viral
• Typical CAP: o cough, fever, purulent sputum, chest pain. o usually has a shaking chill (rigor) o expect Pneumococcus, except in special populations (e.g. aspiration pneumonia –
Klebsiella) • Aspiration CAP:
o different microbes, such as Klebsiella, Bacteroides, Fusobacterium o special populations:
those taking acid-suppressing drugs (H2B, PPI) since normaly GI tract colonization is inhibited by gastric acid
elderly, immunocompromised, COPD, asthma those with impaired consciousness
• Evaluation of CAP: o Imaging:
CXR in all patients with suspected pneumonia to find an infiltrate for definitive diagnosis of pneumonia – looking for infiltrate (consolidation)
o General laboratory assessment: complete blood count (CBC); serum blood urea nitrogen, glucose,
electrolytes, and liver function testing; and assessment of oxygen saturation. Persons aged 13 64 years should undergo HIV testing
o Outpatient o air-dried slide of a pretreatment deep-cough sputum sample for gram stain
and C&S o In hospitalized patients:
o 2 pretreatment blood cultures o expectorated sputum Gram stain and culture.

Advanced Pathophysiology Unit 6 Page 25 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
NOSOCOMIAL (HOSPITAL ACQUIRED) (HEALTHCARE ASSOCIATED) PNEUMONIA (NP): • NOTE the term “nosocomial” is being replaced with the term “healthcare-
associated infection” (HAI) • Hospital acquired after 1 week of hospital stay with a new CXR infiltrate • Usually fever & leukocytosis • etiologic microbes:
o aerobic gram-negative bacilli cause all cases of NP and destroy lung tissue o necrotizing type:
rapid cavitation, microabscess formation, blood vessel invasion, and hemorrhage
usually Pseudomonas aeruginosa, but can be others o non-necrotizing type: all others
• See CDC website: http://www.cdc.gov/hai/ VIRAL PNEUMONIA: • age groups:
o mostly childhood and those over 60 yo o can be mild or life-threatening
• etiologic microbes: o influenza A; respiratory syncytial virus (RSV); parainfluenza 1, 2, and 3; and
adenovirus o often multiple viral types present at the same time o often, viral infection is concomitant with bacterial infection o adenovirus is particularly contagious (air sputum droplets)
• special etiology: o SARS (Severe Acute Respiratory Syndrome) caused by coronavirus
Etiolotic criteria are fever (temperature, >38°C) and 1 clinical finding of moderate respiratory illness (e.g., cough, shortness of breath, and hypoxia), & epidemiologic criteria (travel within 10 days before onset of symptoms to an area with community transmission of SARS, or close contact within 10 days before onset of symptoms with a person known or suspected of having SARS infection)
o Avian Influenza Virus A/H5N1 virus may cause a pandemic
• treatment: o fluids, beta-agonists if bronchospasm o antibiotics if infiltrate on CXR o respiratory isolation o watch for respiratory failure (may need to be mechanically ventilated)

Advanced Pathophysiology Unit 6 Page 26 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
DIAGNOSTICS IN PNEUMONIA: Using of using diagnostics for the workup (evaluation) of pneumonia including community acquired pneumonia in adults: o CPG: https://www.guideline.gov/summaries/summary/50009/pneumonia-in-adults-
diagnosis-and-management o Evaluate severity for triage purposes:
o Use the CURB-65 severity score o See calculator: https://www.mdcalc.com/curb-65-score-pneumonia-severity
o CURB-65 score 0-1 may be able to manage at home o CURB-65 score 2 or more consider hospitalization o CURB-65 score 3 or more consider intensive care o Another score is the SOAR score (which is a modified CURB65 score) see:
http://www.fpnotebook.com/lung/Exam/SrPnmnScr.htm o Imaging:
o Chest radiography in all patients with suspected pneumonia to find an infiltrate for definitive diagnosis of pneumonia
o General laboratory assessment: o Complete blood count (CBC); serum blood urea nitrogen, glucose, electrolytes, and
liver function testing; and assessment of oxygen saturation. o Persons aged 13 64 years should undergo HIV testing (inform patient)
o Tests for an etiologic agent in ambulatory patients: o Air-dried slide of a pretreatment deep-cough sputum sample o Consider pneumococcal and legionella urinary antigen tests
o Tests for etiologic agent in hospitalized patients: o Two (2) pretreatment blood cultures o Expectorated sputum Gram stain and culture.
Sputum specimen should be a deep-cough specimen obtained before antibiotic treatment that is rapidly transported and processed within a few hours of collection.
Cytologic criteria should be used as a contingency for sputum culture, except with culture for Mycobacteria and Legionella species.
Transtracheal aspiration, transthoracic aspiration, and bronchoscopy should be reserved for selected patients and done by physicians with appropriate expertise.
Testing of induced sputum has established merit only for detection of Mycobacterium tuberculosis and Pneumocystis carinii

Advanced Pathophysiology Unit 6 Page 27 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
BRONCHIECTASIS: • abnormal and permanent dilatation (”ectasia”) of bronchi or lower airways • may be acquired (most usual) or congenital • may be focal (segmental) or diffuse (affecting large areas in both lungs) • congenital:
o related to pulmonary developmental dysplasia • acquired:
o from longstanding bronchial infection o seen in conditions like CF, immotile cilia syndrome, with FB aspiration, and
post-infectious reaction. • presentation:
o HEMOPTYSIS and atelectasis o acute respiratory distress o initially symptoms are reversible, but eventually, may not respond to treatment
• workup: CXR with “Tram track sign” (parallel densities) & CT is now gold standard. • treatment:
o antibiotics, chest PT (RT) o may need surgical resection of local segment.
LUNG ABSCESS: • Cause:
o usually from prior aspiration o or infection behind obstructed bronchus
• Microbes: Usually anaerobic, secondary to prior pneumonia that has walled off. • Workup:
o CXR shows an air-fluid level, with what appears to be a cavitary-like lesion. o Further definition on thoracic CT. o Usually needs bronchoscopy.
• Treatment: o Almost always clears with correct antibiotics over 2 - 3 weeks (until CXR is clear) o If does not, needs thoracic surgeon for resection.

Advanced Pathophysiology Unit 6 Page 28 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
CROUP: • also called acute infectious laryngotracheobronchitis. • A purely pediatric condition. • Presentation:
o occurs at ages 6 mos to 3 yrs old. o Barky cough, inspiratory stridor, resp distress (retractions, accessory muscles,
dyspnea, tachypnea) and eventual lower a/w involvement (exp. wheeze). o Usually see subglottic obstruction from edema (XRAY: steeple sign of narrowed
subglottic space). • Etiology: mostly viral (parainfluenzae). • Treatment:
o Some say ALWAYS hospitalize, ALWAYS obtain either ENT or ID consult. o Therapies include aerosol racemic epinephrine up to Q 20 min, calm environment,
cool mist, systemic steroids (if ill), laryngoscopy if no improvement in 1 days, observe for worsening (= bacterial superinfection).
• Variant: form of this illness that is allergic & recurrent (allergic recurrent croup). EPIGLOTTITIS: EMERGENCY !! • Although often said to be a “pediatric” diagnosis, can occur in BOTH in adults & kids. • Presentation: Older kids (age 2 - 7 yrs) and rarely in adults.
o High fever, respiratory distress, dysphagia, muffled voice, sit erect & drool (need to sit upright to breathe & don’t like to move).
o EMERGENCY & DON'T EXAMINE THE PHARYNX — do NOT ask child to open the mouth for viewing of the pharynx, since the extension can close off the trachea.
• Etiology: usually H. influenzae. • Workup:
o XRAY of lateral neck, showing "thumb sign" o At all times (including while getting XRAY) make sure personnel can intubate & have
equipment to do so crash cart & tubing, Ambu bag. • Treatment:
o HOSPITALIZE immediately with specialist care (ENT) o intubation may be necessary on lateral neck, may be a difficult intubation (notify
CRNA, ER staff, Anesthesia who have more intubation experience) o Antibiotic coverage with 3rd generation cephalosporin (to cover the H. influenzae). o Hib vaccine prevents that caused by the type b strain of H. influenzae, but not the
other strains. Lateral Neck X-ray: Epiglottitis with “Thumb sign” (red arrow) (thickening of aryepiglottic folds seen on white arrow)

Advanced Pathophysiology Unit 6 Page 29 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
PEDIATRIC BRONCHIOLITIS: • 2014 CPG from AAP: http://pediatrics.aappublications.org/content/134/5/e1474 • This is considered to be a pediatric diagnosis:
o common in first 2 yrs of life o increased risk with day care o usually winter & spring o may trigger future asthma
• Presentation: o viral upper respiratory prodrome o then wheezing (usually expiratory) o may have rhinorrhea; coughing; wheezing; tachypnea; and grunting, nasal flaring,
and intercostal or subcostal retractions from increased respiratory effort o increased respiratory rate, accessory muscle use or retraction o Risk for hospitalization: <6 months old, hypoxemia, respiratory distress, not
feeding, or underlying chronic diseases • Pathophysiology:
o Small airway inflammation, edema, plugging o pneumonitis & atelectasis o RSV (& other viruses) and Mycoplasma pneumoniae)
• Complications: o may result in long-term recurrent airway syndromes such as ASTHMA in later life o may progress to bronchiolitis obliterans
• Prevention: recall use of palivizumab/Synagis in at-risk infants (preemies) • Treatment:
o Bronchodilators: routine use not recommended o Corticosteroids: routine use not recommended o Antiviral therapy: routine use of aerosolized ribavirin/Virazole not
recommended; consider if severe RSV bronchiolitis or at risk for same o Antibacterial therapy: use if clinical assessment indicates bacterial
superinfection o Chest Physiotherapy: not indicated o Oxygen Supplementation: administer if PaO2 falls below 90%

Advanced Pathophysiology Unit 6 Page 30 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
From: Meissner, H. C. (2016) Viral Bronchiolitis in Children. New England Journal of Medicine, 374(1), 62-72. Retrieve from http://www.nejm.org/doi/full/10.1056/NEJMra1413456
Viruses detected in children with bronchiolitis
Progression of RSV

Advanced Pathophysiology Unit 6 Page 31 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
BRONCHIOLITIS OBLITERANS ORGANIZING PNEUMONIA (BOOP): • organizing pneumonia has granulation tissue in the distal air spaces • if granulation tissue is also in the bronchiolar lumen, this is bronchiolitis obliterans (BO) • types:
o cryptogenic (idiopathic) – 50% o cause is known or suspected from clinical history – 50%
radiation chronic infection exposure (drugs, toxins, environmental) associated conditions (sarcoid, cancer, cystic fibrosis)
• outcome: o development of chronic consolidations in the lung o some fibrosis as well and sometimes cavitations
• treatment: o steroids, RT, bronchodilators o some “relapsing” cases need to remain on steroids

Advanced Pathophysiology Unit 6 Page 32 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
ENT CONDITIONS AS CONSIDERED TO BE RESPIRATORY ILLNESSES: remember that the respiratory epithelium is continuous with the nasal/sinus passages ACUTE OTITIS MEDIA (AOM): (NOT otitis media with effusion, OME, or serous otitis) • Definition of AAP & AAFP:
o “infection of the middle ear with acute onset, presence of middle ear effusion (MEE), and signs of middle ear inflammation”
o Diagnosis controversial, charting of findings supporting diagnosis important o this is the most frequent pediatric diagnosis in a febrile child
• Presentation & Diagnosis: o A diagnostic tool is available on the CDC website -- see links above. o Presentation includes otalgia, fever, tinnitus, vertigo, draining ear. o The infant may only have nonspecific findings of fever, irritability, poor sleep,
poor feeding, vomiting, otorrhea. o Ear pulling in the child may signal onset of infection. o Often occurs after resolution of URI. o Etiologic agents vary by age, it is often secondary to a URI. o occurs more during winter months in North America
• At risk populations: o a age 6 mo - 2 yr o Down syndrome, Alaskan Eskimo, Native American, cleft palate, boys, formula
fed infants, low Socioeconomic class, sickle cell o CONTINUOUS USE OF PACIFIER (only use when falling asleep, then take
away). o in day care o treated with antibiotics within the last 3 months o recent upper respiratory infection
• Complications: o cholesteatoma o hearing loss (permanent or temporary) & thus delay in language acquisition o chronic effusion o mastoiditis (present with postr auricular swelling, erythema, pinna displacement
-- may be chronic, may need surgical I&D) that may progress to o meningitis (secondary complications of developmental retardation). o REMEMBER: if hearing loss occurs (even temporarily), then language
acquisition is also affected • Treatment:
o antibiotic therapy relieves symptoms, resolves infection, reduces complications such as meningitis and residual hearing damage
o Etiologic microbes vary by age, thus antibiotics vary with age & presentation o Surgical Treatment & Referral:
Tympanostomy: first give 2 weeks of amoxicillin, & then a second-line drug for 2 more weeks if no better.
Guidelines: recurrent otitis (3 episodes or more of AOM in 6 months, or 4 episodes in 1 year

Advanced Pathophysiology Unit 6 Page 33 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
ACUTE OTITIS MEDIA WITH EFFUSION (AOME): • same findings as above for AOM, plus bubbles or air-fluid levels behind the TM. • Concern about hearing loss with chronic effusion (and/or delay of language acquisition). • Most children have at least one episode of OME before entering school, may present as
AOM or be an incidental finding on exam Diagnosis: • Child has discomfort, maybe behavioral changes • pneumatic otoscopy, tympanometry (gold standard) • some newer approaches (acoustic reflectometry, tuning fork tests). Evaluation: • if fluid in both middle ears for total of 3 months should undergo a hearing evaluation. • May also refer before the 3 month mark!! Treatment: • more aggressive approach to therapy if present for more than 4-6 weeks, or if hearing
loss found earlier use of antibiotics. SEROUS OTITIS MEDIA (otitis media with effusion, OME): • not due to infectious etiology. • On exam, looks like bubbles behind the eardrum
o little of the inflammatory changes noted in AOM or AOME (no hyperemia, erythema) o The eardrum may be retracted (“glue ear”) o a black line horizontally across the TM may be seen if middle ear is partially full (this
is the fluid meniscus). o May be caused by reduced barometric pressure (airplane ride). o May also contribute to hearing loss, tinnitus symptoms.
• Treatment: o decongestants OR antihistamines (chlortrimeton, or newer non-sedationg
antihistamines like Zyrtec, Claritin). o Antibiotics are NOT indicated.

Advanced Pathophysiology Unit 6 Page 34 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
PHARYNGITIS: • microbes can be diphtheric, gonococcal, or Streptococcal (Group A beta-hemolytic strep,
GABHS) CDC (adults) : http://www.cdc.gov/getsmart/community/materials-references/print-materials/hcp/adult-acute-pharyngitis.html and http://www.cdc.gov/getsmart/community/materials-references/print-materials/hcp/adult-acute-pharyngitis.pdf CDC (kids): http://www.cdc.gov/getsmart/community/materials-references/print-materials/hcp/child-pharyngitis.html INFECTIOUS CAUSES OF ACUTE PHARYNGITIS
From: Wessels MR. Streptococcal pharyngitis. N Engl J Med 17 Feb 2011;364(7):648-55.

Advanced Pathophysiology Unit 6 Page 35 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Selected Laboratory:
• Strep Antigen: o GABHS rapid antigen detection o also called “Strep test” “Quick Strep” (waivered test for POL under CLIA-88) o if negative, many experts recommend that a throat culture be done (in case of a
false positive antigen test) • Throat Culture:
o gold standard for diagnosis but problem with followup (takes 24-48 hours to read)
o sensitivity 99% o only clinically useful if illness is less than 10 days old o throat swab to capture exudate and transported dry to lab for plating o also perform on family contacts of non-suppurative (non-exudative) GABHS and
if recurrent outbreaks • Antistreptolysin-O (ASO, ASLO) titer:
o useful in illness that is more than 10 days old o need acute and convalescent titers since this is a serology test
• CBC: o atypical lymphocytes and right shift in mononucleosis (viral) o left shift and band forms in GABHS (bacterial)
• Monospot: o for infectious mononucleosis o 95% sensitivity in children (poor sensitivity in infants) o GC culture or genprobe of pharynx: o if oral gonococcal infection suspected by history o if STD suspected, also perform associated tests (STS, Chlamydia genprobe,
HIV)

Advanced Pathophysiology Unit 6 Page 36 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
GABHS: • the MOST COMMON microbe in pharyngitis. • Most GABHS is accompanied by anterior cervical adenopathy and also may have
associated symptoms of headache and even GI symptoms, malaise • If positive, treat for Strep (see below) and consider culturing other family members • If negative, assume viral and observe and give comfort measures and antipyretics (not
aspirin). Prolonged symptoms indicate other bacterial etiology and need further workup and antibiotic treatment. • From the AHA, 2009 CPG on Prevention of Rheumatic Fever & Strep Pharyngitis: http://circ.ahajournals.org/content/119/11/1541 CLINICAL FINDINGS IN “GAS” PHARYNGITIS:

Advanced Pathophysiology Unit 6 Page 37 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
“CENTOR”: A CLINICAL SCORING SYSTEMS FOR GAS Current CPG from IDSA: (2012) http://www.guideline.gov/content.aspx?id=38416
• For ALL pharyngitis in children 3+ years old get Rapid Strep Antigen Detection Test (RADT)
o EXCEPTION: adults with obvious symptoms of viral origin (rhinorrhea, oral ulcers, hoarseness, cough)
o EXCEPTION: not indicated for children <3 years old because acute rheumatic fever is rare in children <3 years old and the incidence of streptococcal pharyngitis and the classic presentation of streptococcal pharyngitis are uncommon in this age group. However, selected children <3 years old who have other risk factors, such as an older sibling with GAS infection, may be considered for testing.
o If positive: treat for Strep and consider culturing other family members o If negative:
Get backup culture in children, not needed in adults give comfort measures and antipyretics (not aspirin)
• Most GABHS is accompanied by anterior cervical adenopathy and also may have associated symptoms of headache and even GI symptoms, malaise
• Prolonged symptoms indicate other bacterial etiology and need workup & antibiotic treatment
From: Wessels MR. Streptococcal pharyngitis. N Engl J Med 17 Feb 2011;364(7):648-55.
• A runny nose, cough, and vocal cord involvement almost certainly means viral etiology.
• Note the tender, swollen anterior lymph nodes is an important finding in GAS.

Advanced Pathophysiology Unit 6 Page 38 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Complications of GABHS:
• PANDAS as a complications of GABHS: o PANDAS (pediatric autoimmune neuropsychiatric disorders associated
with streptococcus infection) o No evidence exists that one antibiotic regimen is better than another to prevent
this. o Patient presents with symptoms of (usually) OCD, tic disorders, symptoms of
ADD/ADHD, depression, sleep disturbance, joint pain, and fine/gross motor changes.
o It is thought that the antibodies to Strep cross the BBB and cause these symptoms.
• Acute Rheumatic Fever (ARF) as a complicaton of GABHS: o untreated GABHS can lead to ARF o see cardiac module for more information on this syndrome
Advanced Pathophysiology Unit 6 Page 39 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
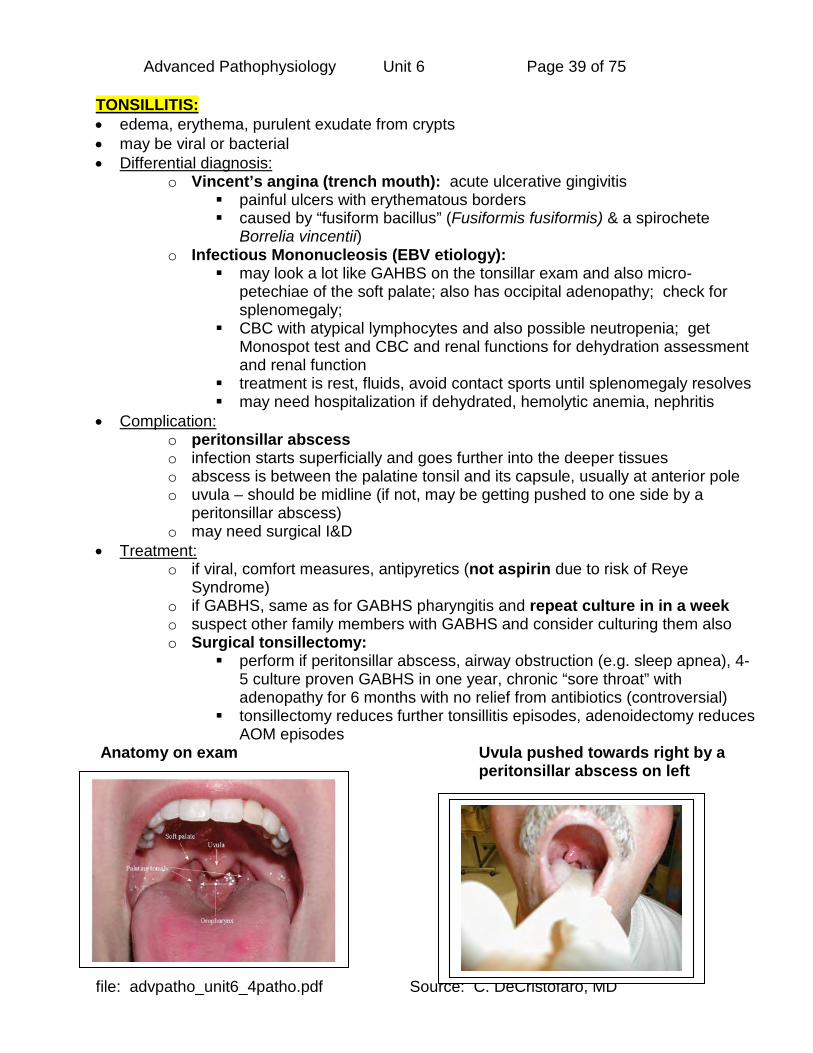
TONSILLITIS: • edema, erythema, purulent exudate from crypts • may be viral or bacterial • Differential diagnosis:
o Vincent’s angina (trench mouth): acute ulcerative gingivitis painful ulcers with erythematous borders caused by “fusiform bacillus” (Fusiformis fusiformis) & a spirochete
Borrelia vincentii) o Infectious Mononucleosis (EBV etiology):
may look a lot like GAHBS on the tonsillar exam and also micro-petechiae of the soft palate; also has occipital adenopathy; check for splenomegaly;
CBC with atypical lymphocytes and also possible neutropenia; get Monospot test and CBC and renal functions for dehydration assessment and renal function
treatment is rest, fluids, avoid contact sports until splenomegaly resolves may need hospitalization if dehydrated, hemolytic anemia, nephritis
• Complication: o peritonsillar abscess o infection starts superficially and goes further into the deeper tissues o abscess is between the palatine tonsil and its capsule, usually at anterior pole o uvula – should be midline (if not, may be getting pushed to one side by a
peritonsillar abscess) o may need surgical I&D
• Treatment: o if viral, comfort measures, antipyretics (not aspirin due to risk of Reye
Syndrome) o if GABHS, same as for GABHS pharyngitis and repeat culture in in a week o suspect other family members with GABHS and consider culturing them also o Surgical tonsillectomy:
perform if peritonsillar abscess, airway obstruction (e.g. sleep apnea), 4-5 culture proven GABHS in one year, chronic “sore throat” with adenopathy for 6 months with no relief from antibiotics (controversial)
tonsillectomy reduces further tonsillitis episodes, adenoidectomy reduces AOM episodes
Anatomy on exam Uvula pushed towards right by a peritonsillar abscess on left
Advanced Pathophysiology Unit 6 Page 40 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
ACUTE BACTERIAL SINUSITIS (ABS) (ABRS = acute bacterial rhinosinusitis): • definition:
o inflammation and/or infection of 1 or more paranasal sinuses o occurs with obstruction of the normal drainage mechanism
• types: o acute (symptoms lasting <3 wk) o subacute (symptoms lasting 3 wk to 3 mo) o chronic (symptoms lasting > 3 mo)
• presentation: o headache, increased with leaning forward or with percussion/palpation o sinus pain o persistent “cold” symptoms (rhinitis) o retro-orbital pain (if ethmoid involved) o dental pain o anosmia or paranosmia
• examination: o percussion/palpation tenderness o opacification on transillumination o purulent drainage from middle meatus
• microbes: o usually Strep pneumoniae, H. influenzae, Moraxella catarrhalis o sometimes Staph aureus & others (Group A strep, anaerobes, viruses)
• workup: o preferred test is the sinus CT
• complications: o chronic sinusitis o orbital cellulitis
CHRONIC SINUSITIS: • same therapy as for acute sinusitis, but for longer duration (14-21 days, some say 4 - 6
weeks). • Surgical drainage (windows) indicated with medical failure. If surgery is being considered,
do a sinus CT. • Some people are using neti pots (clay/ceramic pots that put liquid into the nose that then
goes into the sinuses to “wash” the sinuses) – the liquid used is saline solution ORBITAL CELLULITIS a complication of sinusitis or orbital trauma: • complication of sinusitis and/or direct trauma (hit in the eye in a fight)
o bacteria reach the orbit via wall of infected sinus, or gain entry from the outside due to trauma.
• need to confirm by CT & lab. • aggressive antibiotic (parenteral) and/or surgical treatment
o this is an emergency o difficult to treat & complications include meningitis, encephalitis, cavernous
sinus thrombosis, blindness & death

Advanced Pathophysiology Unit 6 Page 41 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
TUBERCULOSIS (TB): mycobacterial infection • infection does not always progress to active disease
o children/adolescents are at greater risk of progression. • infection in a child indicates TB in the community, and is a "sentinel" event. • transmission: by airborne droplets • presentation of active disease: cough, weight loss, night fevers • CDC guidelines: http://www.cdc.gov/tb/default.htm • Confirming suspected diagnosis:
o recover organism from body fluid which is usually sputum (pulmonary TB) o could be other body fluids – in disseminated TB (CSF, urine, bone, etc) o special techniques are used to confirm infection with these organisms o cultures (take weeks) o acid-fast staining (see below of sputum) o Chest Xray with special positioning to see cavitations in upper (more aerobic)
areas of the lung; also may see hilar adenopathy, pleural effusion; order PA, lateral and apical lordotic views (see below)
Cavitary lesion appears in Right Upper Lobe (RUL). They often “hide” behind the clavicle. This is a Postero-Anterior (PA) view. Special positioning of the patient (Apical lordotic, leaning forward into the film) is used to make the cavitations more prominent. Remember that TB is aerobic, will preferentially live in the upper regions of the lung which has relatively more Oxygen. (from: Chest Xray Atlas, Loyola University Medical Center: http://www.meddean.luc.edu/lumen/meded/medicine/pulmonar/cxr/atlas/cxratlas_f.htm
the acid-fast bacilli are seen here (they tend to bead up and appear in chains) in sputum of active TB patient (from the NIH, http://www.nhlbi.nih.gov/funding/training/tbaa/ )

Advanced Pathophysiology Unit 6 Page 42 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
• Screening: based on risk
o High Risk: annual testing o Low Risk: periodic testing (e.g. children at age 12 months and again at age 4-
6 yrs and/or 12 yrs). o Prior BCG vaccine: still do skin testing as indicated, & many clinicians
recommend as well serial CXR -- once yearly for 3 years in a row, then once every 3 years, with conconmitant TB skin testing
• Type of screening tests: o QuantiFERON-TB Gold (QFT-G) is the alternative to skin testing; a serologic
blood test that detects the release of interferon-gamma (IFN-g) in fresh heparinized whole blood from sensitized persons.
o Mantoux tine skin test (tine skin test = TST) is intradermal injection of 5 TU (of tuberculin purified protein derivative, PPD) and observation for reaction in 48-72 hours (cell-mediated sensitivity reaction, requires this length of time to develop).
• Test results interpretation: o False-positive skin test: non-TB mycobacteria, prior BCG vaccination,
hypersensitivity, false reading, poor administration of skin test, cellulitis. o False-negative skin test: anergy (immune incompetence from cancer, HIV,
immune suppressing drugs, severe illness), very recent TB infection (has not “converted” yet), very young age (< 3-6 months old), live-virus vaccination (makes skin test UNRELIABLE), overwhelming TB disease (related to immune system collapse)
• Multi-step Skin Testing: in HCW, persons over age 40, and LTC facilities o if the second test is positive, this is a "boosted reaction" from prior infection and
considered positive o If the second test is negative now, but then a future test is positive (2 years or
more later) this definitely indicates a recent conversion. o This is why we test the high-risk (& health-care workers) with two-step testing o multi-step testing NOT necessary with the QFT-G
• Classification of the tuberculin reaction: o the induration of 5, 10 or 15 mm is the cutoff for positive o the higher the risk, the lower the induration size to be positive
• Followup testing: o if once infected and treated, future PPD are NOT done. o use CXR annually x 3 years, then Q 3 years after that.

Advanced Pathophysiology Unit 6 Page 43 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
PLEURAL EFFUSION: remember that there is the visceral pleura and parietal pleura • normal parietal fluid:
o only a few tenths of an mL of fluid in the space – this is one of those potential spaces in the body
o alkaline fluid with very little protein (<1.5 g/dL) • blood supply: systemic arterial supply & venous drainage of 90%; lymphatics drain 10%
parietal pleura lymphatics drain to lymph nodes on chest wall visceral pleura lymphatics drain to mediastinal lymph nodes
• types of pleural effusions: o may be acquired or congenital o transudate from imbalance of COP & capillary HP
are usually bilateral since cause is systemic and affects both sides the same examples are systolic HF with volume overload, hypoalbuminemia,
nephrosis, hepatic cirrhosis, & iatrogenic (misplaced central line) o exudate (pus) from inflammation or infection
may affect only one side may be complication of pneumonia
• causes of pleural effusion: o infection (bacteria, TB) o inflammation – even collagen-vascular disease (e.g. lupus) o cancer o trauma o abdominal pathology o congenital (associated with polyhydramnios, Down syndrome, pulmonary
hypoplasia) • location of effusion:
o parapulmonic (arising from lung etiology) o subpulmonic (arising from abdominal etiology)
• clinical presentation: o chest pain, dyspnea o if pleurisy (inflammation) there may ba a pleural “rub” on stethoscope auscultation o dullness to percussion; decreased fremitus; decreased breath sounds o if REALLY big unilaterally, can even cause mediastinal shift to the contralateral
side • lab evaluation of pleural fluid: trying to determine if transudate or exudate
o exudate has high protein level (> 3 gm/dL), pleural LDH–systemic LDH ratio >0.6 o transudate has low protein level

Advanced Pathophysiology Unit 6 Page 44 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
• evaluation: o Xray findings: costo-phrenic angle is obscured, lateral decubitus view shows fluid
shift o complications: empyema (localized collection of pus in the pleural space)
• treatment: o removal of fluid by drainage (thoracentesis)
may be one time removal of fluid may require placement of chest tube for continuous drainage to
underwater seal that allows fluid to leave the chest, but nothing else to return to the chest
o pleurodesis may be done if the lung reinflates and there is concern that the fluid will recur, an injection of a sclerosing agent into the pleural space to bind the parietal and visceral pleura together (e.g. bleomycin, tetracycline, talc)
Thoracentesis
Arrow A shows fluid layering in the right pleural cavity; arrow B shows the normal width of the lung
costophrenic angles are obscured bilaterally

Advanced Pathophysiology Unit 6 Page 45 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
PNEUMOTHORAX • air in the potential space between the visceral and parietal pleura • air enters through:
o a communication from the chest wall o the lung parenchyma across the visceral pleura o secondary to pneumomediastinum
• types: o traumatic (stabbing, GSW) o primary spontaneous (no underlying lung disease – usually younger males) o secondary spontaneous (underlying lung disease – air enters from damaged lung) o catamenial (during menses, from bleeding into lung of endometrial tissue) o iatrogenic (from medical procedure) o from pneumomediastinum (air dissects into the neck and then to the rest of the
body) • clinical presentation:
o lung becomes smaller as the air is sucked into the pleural space o loss of lung function results o initial symptoms include sharp chest pain and acute SOB o seen more in smokers o spontaneous usually not life-threatening
• imaging: CXR, CT, ultrasound • treatment: tube thoracotomy, needle aspiration of air
Note hyperluscency (it is darker since no blood vessels are in the area – it is all air) of left lung and lung border (arrow)

Advanced Pathophysiology Unit 6 Page 46 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
This x-ray should never have been taken: the diagnosis should have been made CLINICALLY • tension pneumothorax:
o air trapping (air gets in and it can’t get out) with secondary displacement (“SHIFT”) of mediastinal structures to the other side
o this can compromises cardiac function o this can be life-threatening – might be iatrogenic, traumatic, or spontaneous
• Clinical presentation:
o findings are hyperresonance, hyperexpansion of chest wall, tachycardia, tachypnea (respiratory distress) due to hypoxia from the ipsilateral collapsed lung and contralateral compressed lung
o decreased or absent breath sounds, possibly tracheal deviation o HYPOTENSION due to compression of thin-walled cardiac atria that REDUCES
venous return cardiovascular collapse o Possibly distended neck veins (due to above) (not seen if hypovolemic)
• Treatment: o Needle decompression (thoracostomy) with large-bore needle in the second
intercostal space in the midclavicular line o Converts tension pneumothorax into a simple pneumothorax
Advanced Pathophysiology Unit 6 Page 47 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
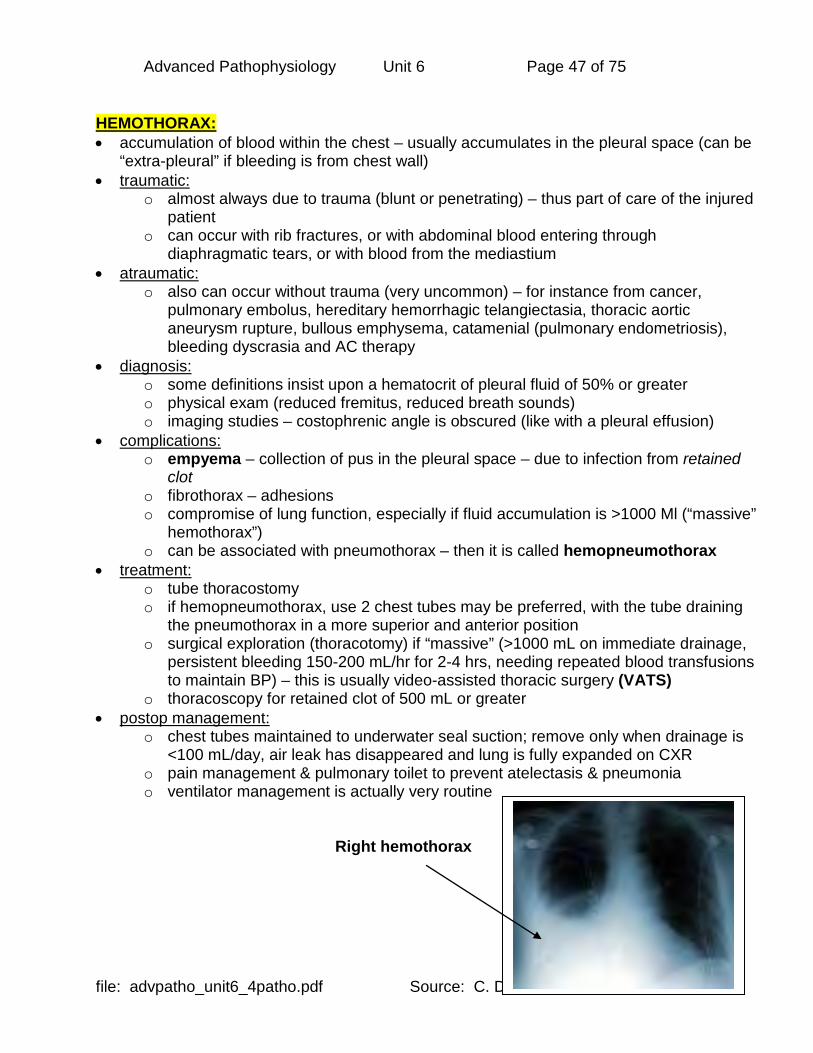
HEMOTHORAX: • accumulation of blood within the chest – usually accumulates in the pleural space (can be
“extra-pleural” if bleeding is from chest wall) • traumatic:
o almost always due to trauma (blunt or penetrating) – thus part of care of the injured patient
o can occur with rib fractures, or with abdominal blood entering through diaphragmatic tears, or with blood from the mediastium
• atraumatic: o also can occur without trauma (very uncommon) – for instance from cancer,
pulmonary embolus, hereditary hemorrhagic telangiectasia, thoracic aortic aneurysm rupture, bullous emphysema, catamenial (pulmonary endometriosis), bleeding dyscrasia and AC therapy
• diagnosis: o some definitions insist upon a hematocrit of pleural fluid of 50% or greater o physical exam (reduced fremitus, reduced breath sounds) o imaging studies – costophrenic angle is obscured (like with a pleural effusion)
• complications: o empyema – collection of pus in the pleural space – due to infection from retained
clot o fibrothorax – adhesions o compromise of lung function, especially if fluid accumulation is >1000 Ml (“massive”
hemothorax”) o can be associated with pneumothorax – then it is called hemopneumothorax
• treatment: o tube thoracostomy o if hemopneumothorax, use 2 chest tubes may be preferred, with the tube draining
the pneumothorax in a more superior and anterior position o surgical exploration (thoracotomy) if “massive” (>1000 mL on immediate drainage,
persistent bleeding 150-200 mL/hr for 2-4 hrs, needing repeated blood transfusions to maintain BP) – this is usually video-assisted thoracic surgery (VATS)
o thoracoscopy for retained clot of 500 mL or greater • postop management:
o chest tubes maintained to underwater seal suction; remove only when drainage is <100 mL/day, air leak has disappeared and lung is fully expanded on CXR
o pain management & pulmonary toilet to prevent atelectasis & pneumonia o ventilator management is actually very routine
Right hemothorax

Advanced Pathophysiology Unit 6 Page 48 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
CANCER AND THE PATHOLOGY REPORT? Biopsy: • removing a sample (piece) of tissue for microscopic and other laboratory analysis • sometimes requires anesthesia & surgery to obtain the tissue • biopsy may be done by oncologist and/or surgeon • pathology lab performs the analysis • Usefulness:
o determine the TYPE of cancer by cellular analysis o part of STAGING (determining if cancer has invaded/metastasized)
determine other attributes of the cancer cells (e.g. hormone receptors) Examples of types of biopsies: • Excisional: entire area of involved tissue (or organ) is removed • Incisional: only a portion is removed • Endoscopic fiberoptic biopsy: any area that can be accessed with fiberoptic endoscope
can have a biopsy forceps inserted into the endoscope and a piece of tissue excised • Colposcopic biopsy: using the colposcope to magnify & identify (with various chemicals)
abnormally appearing mucosa (biopsy done with forceps) • Fine needle aspiration biopsy (FNAB): small (22 gauge) needle inserted into the mass to
withdraw a cylindrical piece of tissue; can be assisted with radiology (ultrasound, CT, fluoroscopy)
• Punch biopsy: usually done for skin lesions – a small cylindrical “punch” forceps removes a “plug” of tissue
• Bone marrow biopsy: needle put into the marrow (superior iliac crest, sternum) to obtain marrow – both a liquid (marrow) specimen and then a core biopsy (of bone)
Specimen processing – histopathology processing: • Histologic sections:
o permanent section puts the specimen into a fixative (e.g. formalin) and then suspends it in wax (wax replaces the water in the specimen) – this part takes at least 1 day; the solid specimen is cut into super-fine slices (with a microtome cutter) and the wax is removed with solvents – it is then stained as a microscopic specimen for microscopic analysis (see picture below)
• Frozen sections: o done while the patient is still under anesthesia, the specimen is dropped into liquid
nitrogen and rapidly frozen, then microtomed and examined under the microscope; not done as much recently since the results are not as accurate and making clinical decisions may not be appropriate
• Smears: o liquid biopsies are smeared on a microscope slide and fixed with chemical, then
stained and examined under the microscope

Advanced Pathophysiology Unit 6 Page 49 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
H&E (hematoxylin & eosin) stain of normal pancreas (the nuclei are blue – hematoxylin; the other cell structures are pink – eosin) What is on the pathology report? • Gross description:
o this comes FIRST and describes the MACRO view o a naked eye description of the specimen as it is received in the lab
• Microscopic description: o this is the MICRO view and describes the findings of the cells after all the fixation and
processing has been completed o this may include special processing such as special stains, immunofluorescent
technology, receptor binding, etc. o evidence of cancer or metaplasia is reported o at the very end the final pathologic diagnosis is given
Good sites for pathology reports: • Overview: http://www.cancer.gov/about-cancer/diagnosis-
staging/diagnosis/pathology-reports-fact-sheet • Reading a pathology report (excellent): http://www.cancer.net/navigating-cancer-
care/diagnosing-cancer/reports-and-results/reading-pathology-report Example of a pathology report: http://www.aimatmelanoma.org/en/aim-for-answers/path-to-getting-a-diagnosis/pathology/an-example-of-a-melanoma-pathology-report.html and https://www.aimatmelanoma.org/diagnosing-melanoma/pathology/example-melanoma-pathology-report/
Advanced Pathophysiology Unit 6 Page 50 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
STAGING CANCER: Staging: • how far it has spread anatomically • also describes tissue invasion, not just distant metastasis Prognosis: • related to BOTH the staging AND the histologic type of cancer
o this includes the grade of the cancer o grading refers to the histologic attributes of the actual cancer cells microscopically o describes how ABNORMAL they are and thus implies a better or worse prognosis
Examples of staging systems: • Roman Numeral Staging system:
o cancer described by Roman numerals I-IV or called “recurrent” o Stage I usually small, localized (non-invasive), usually easily treated o Stage IV usually advanced, metastatic, inoperable o “NED” means “No Evidence of Disease” and is used to describe the situation when
cancer is no longer visible or found on diagnostic evaluation o “Recurrent” means the tumor has returned AFTER a period of time when the cancer
was NED o the recurrence can be local (same initial site as original cancer) or distant (far from the
initial site of the original cancer) • TNM system of staging: (a more precise descriptive method)
o usually used for solid tumors o T = tumor, N = nodes, M = metastasis o numbers come after the letters
T1N1M0 means T1 tumor, N1 node, no distant Metastases o T levels are T0 – T4
T0 is in situ (has not invaded adjacent neighboring tissues) T4 means direct invasion has occurred and may even involve adjacent organs
o N levels are N0 – N4 N0 is no nodes N4 is extensive node involvement
o M levels are M0 – M1 M0 is no mets; M1 there are mets
Good explanations of staging at: https://www.cancer.gov/about-cancer/diagnosis-staging/staging and http://www.cancer.org/treatment/understandingyourdiagnosis/staging WHY DO PATHOLOGY AND STAGING? • offers information on prognosis • helps guide treatment decisions – treatment protocols (e.g. chemo, radiation, surgery)

Advanced Pathophysiology Unit 6 Page 51 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
LUNG CANCER: leading cause of cancer deaths in BOTH men & women in the USA NOTE: “adenocarcinoma” refers to cancer in the lining or inner surface of an organ Definition of PRIMARY lung cancer: • in tissues of the lung, usually in the cells lining air passages • Main Types: diagnosed by microscopic analysis (histology) of biopsy
o small cell lung cancer (SCLC) less likely (20%) – THIRD most common metastasizes early
o non-small cell lung cancer (NSCLC) most common overall when all subtypes are included several sub-types:
• adenocarcinoma (30-40% of all lung cancer) – MOST common • squamous cell (30%) – SECOND most common • large cell (10%) • bronchoalveolar (looks like pneumonia on a chest XRay) • rare sub-types (carcinoid, lymphoma)
CDC statistics: (from the CDC) “Lung cancer is the leading cause of cancer death and the second most commonly diagnosed cancer (excluding skin cancer) among men and women in the United States” URL: http://www.cdc.gov/cancer/lung/index.htm Risk factors for lung and related cancers: • cigarette smoking:
o First hand smoking: if smoke >1 PPD has RR = 20-25; if quits, after 15 years RR=1 o Second hand smoking: mainstream (in room) and sidestream (breathing in smoke
next to you) o Third hand smoking: carcinogenic nitrosamines deposited on surfaces (See 2014:
http://www.sciencedirect.com/science/article/pii/S0160412014001962 ) • other: cigar & pipe smoking, air pollution, second-hand smoke, environmental (asbestos
and mesothelioma), COPD, TB infection, radon exposure

Advanced Pathophysiology Unit 6 Page 52 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Presentation: • Symptoms and signs: 75% have symptoms
o new cough, hemoptysis, chest pain, wheezing, SOB, hoarseness and repeated pulmonary infections
o may present initially with symptoms from the metastasis (especially in SCLC) o may present initially with symptoms from pleural effusion
• Metastasis: o liver, adrenals, bones, brain o SCLC especially to the bones – vertebrae, femurs, ribs
• Paraneoplastic syndromes: o the tumor makes hormones – SCLC commonly does this o common hormones include TSH may present as hyperthyroid o squamous cell may make PTH hormone hypercalcemia with Trousseau’s sign
ALARM symptoms that suggest neoplasm: • unexplained weight loss • persistent severe fatigue • hemoptysis, hematemesis, hematochezia • pain so severe it wakes you up at night • unexplained rash or fever • strong FH of cancer

Advanced Pathophysiology Unit 6 Page 53 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Evaluation – initial diagnosis: • Diagnostic Imaging:
o Chest Xray: • coin lesion (well-circumscribed mass in the lung) • nodule or nodules • mass
o CT and/or MRI o PET scan
• Diagnostic Biopsy: o Sputum cytology o Bronchoscopy with washings o Percutaneous needle biopsy (if on periphery) o Thoracentesis (if pleural effusion) o Thoracotomy (open biopsy) – tumor is usually debulked at the same time o Mediastinoscopy – especially to sample lymph nodes of mediastinum
• Overall evaluation: o may include PFTs, basic labs o looking for functional ability and co-morbidities
Mass in left lung Squamous cell lung cancer
Advanced Pathophysiology Unit 6 Page 54 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Evaluation – STAGING: • tumor TYPE, SIZE, LOCATION, METASTASIS (including lymph nodes)
o the “higher” the stage, the POORER the prognosis • Typical staging tests:
o Bone scan – looking for metastases o plain Xrays – in the case of lung cancer, if it “crosses the midline” the prognosis is
poor • Prognosis by stage: stages go higher with larger tumor, lymph node involvement
o Stage IA – 75% (small tumor size) o Stage IB – 55% (tumor >3 cm) o Stage IIA – 50% (involves ipsilateral nodes) o Stage IIB – 40% (extends to chest wall) o Stage IIIA – 10-35% (extends to chest wall and ipsilateral nodes) o Stage IIIB -- <5% (invasion of mediastinum, contralateral nodes, pleural effusion) o Stage IV -- <5% (any metastases)
Treatment: • surgical debulking of tumor, if operable
o lobectomy (3% perioperative mortality rate) o pneumonectomy (6% perioperative mortality rate) o segmentectomy (1% perioperative mortality rate) o no longer do wedge resections – more recurrence seen with this procedure
• combination of chemotherapy and radiation – protocol based on type of tumor and stage • some treatments are palliative – not for CURE, but to relieve symptoms & extend life
o cryosurgery (freezing the tumor) o radiation to shrink tumor o referral to hospice care o pain management
Other related cancer – Pleural Mesothelioma: • mesothelial cells normally line the body cavities, including the pleura, peritoneum,
pericardium, and testis • cancers arising from these cells are mesothelioma • Most common site is the pleura
o more common in males (3:1 ratio) o associated with asbestos exposure – primary exposure or secondary exposure (to
a worker who works with asbestos) o industries include building, construction, ceramics, paper mill, auto parts, railroad
and insulation o tumor develops 35-45 years after the asbestos exposure
• very poor survival rate (median survival at diagnosis is 11 months) – uniformly fatal

Advanced Pathophysiology Unit 6 Page 55 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Screening for Lung Cancer: • Annual Chest Xray (CXR) for smokers is no longer recommended – by the time a
pulmonary lesion is found this way, most will have such advanced disease that they will not benefit from therapy.
• However, low-dose CT (LDCT) of the lung based on length of time smoking (pack years) will provide clinical information that can be acted upon to change the outcome of the illness through early diagnosis.
• Recommendation: o Screen high-risk 55-80 yo who smoked 1PPD for 30 years (30 pack years) o Includes those still smoking or those who quit within the last 15 years o Use low-dose CT
• Background: o USPSTF (2014) analysis of the evidence as a basis for recommendation:
https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/lung-cancer-screening
o see information on the National Lung Cancer Screening Trial (NLCST): http://www.cancer.gov/clinicaltrials/noteworthy-trials/nlst
o 2013 current guidelines: http://www.guideline.gov/content.aspx?id=43894 o Guideline synthesis: https://www.guideline.gov/syntheses/synthesis/50489
USPSTF recommendation:

Advanced Pathophysiology Unit 6 Page 56 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
VENOUS THROMBOSIS (DVT), VENOUS THROMBOEMBOLISM (VTE) & PULMONARY EMBOLISM (PE): • DVT can lead to a traveling clot (VTE) pulmonary embolism (PE) Below picture: from New England Journal of Medicine, 6 March 2008; 358(10):1037-52 (by permission with subscription)

Advanced Pathophysiology Unit 6 Page 57 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Deep Venous Thrombosis (DVT): • Risk factors: essentially all of these conditions are procoagulative
o type of anesthesia: GA has 5x greater risk of DVT compared with epidural anesthesia for the same surgical procedure
o autoimmune disease o immune deficiency o immobilization o type A blood in younger people o cancer o stroke (CVA)
chemotherapy o procoagulative conditions: DM, hyperlipidemia, oral estrogen, polycythemia,
pregnancy o obesity o “physical inactivity: – even just amount of time spent “sitting” (especially in
women; BMJ 2011;342) o immobility
• Pathophysiology: o in the deep veins, clotting vs. fibrinolysis is in IMBALANCE o usually in the lower extremities, but can arise from pelvic, renal, or large upper
extremity veins o DVT & VTE really should be thought of at the same time when the diagnosis is
made – since even in cases of DVT with no symptoms of embolus, there is probably some element of embolization
o 2/3 of patients with PE may not have any DVT symptoms – so unfortunately, the presentation may be a clinical surprise (sometimes the site of the DVT is found at autopsy)
o “Red” (venous) clots: red blood cells and fibrin that form in the veins or atrium of the heart think about cardiac valvular disease think about atrial fibrillation management
o “White” (arterial) clots: (this is NOT what we are talking about here) mostly platelets that form in the arteries think about peripheral arterial disease (PAD) think about atherosclerotic heart disease (ASHD), cerebrovascular
disease in setting of stroke prevention, MI prevention cardio-prophylaxis
• Clinical Presentation: o due to venous obstruction o pain, tenderness, unilateral leg swelling, warmth, erythema, palpable cord o Homan’s sign – is not usually done now (may increase embolization) – it is pain
upon passive dorsiflexion of the foot as well as keeping the relaxed foot in an abnormal plantar flexion
o DIFFICULT to diagnose – even with positive findings/symptoms, actual DVT is only there 50% of the time!!

Advanced Pathophysiology Unit 6 Page 58 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Venous Thromboembolism (VTE) and Acute Pulmonary Embolus (PE): • the venous clot embolizes (travels) as a venous thromboembolism (VTE) and lodges in
the lung as a pulmonary embolus (PE) • where to the thrombi go?
o large thrombi end at the bifircation of the main pulmonary artery (or the immediate lobar branches) – result in hemodynamic compromise
o smaller thrombi travel to the more distal, smaller arteries in the lung periphery – these probably cause the pleuritic type chest pain due to inflammation of the pleural lining
• location: usually multiple and usually in the upper lobes • respiratory consequences:
o increased alveolar dead space with V/Q shunting and resultant hypoxemia o hypoxemia o symptoms of hyperventilation o possible eventual pulmonary infarction (not that common, since there is lots of
collateral circulation) • hemodynamic consequences:
o increased pulmonary vascular resistance and thus high afterload for the right ventricle this can even cause acute right ventricular failure increased right heart pressures may actually even give rise to a right-to-
left foramen ovale shunt (if the foramen is open) • clinical presentation:
o many may not have any symptoms at all !! o if mechanically ventilated – note that the PCO2 goes UP and the end-tidal CO2
(PetCO2) goes DOWN (may be only clue) o symptoms are often non-specific (abdominal pain, cough, pleuritic chest pain) o others include tachypnea, rales, fever, tachycardia, S4 gallop and increased
amplitude of S2 o of course, suspect if recent onset atrial fibrillation and/or DVT signs/symptoms
or risk factors such as immobility, physical inactivity, airplane travel, etc. • treatment:
o Hemodynamically stable: anticoagulation to prevent more clots from forming – this can reduce the
mortality rate to <5% if the PE is massive, up to 40% can die within the first hour if not treated oxygenation usually, emboli resolve via fibrinolysis AC therapy is maintained for 6 months, and for longer if recurrent
o Hemodynamically unstable: thrombolytic therapy to dissolve clot morbidity from the therapy limits its use except in these patients
o Recurrent PE or patients who can’t take AC therapy or massive PE: surgical approach with inferior vena cava (IVC) filter (Greenfield filter) reduces PE over the first 2 years sometimes placed prophylactically (e.g. in bariatric surgery)

Advanced Pathophysiology Unit 6 Page 59 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Clinical evaluation of risk and assessment for diagnosis of DVT and VTE/PE: • Clinical scoring tools such as the Caprini or Rogers score help determine risk of
developing DVT/VTE • Assessment of actual DVT/VTE/PE by other scoring tools such as Well’s or Geneva
score Caprini score:
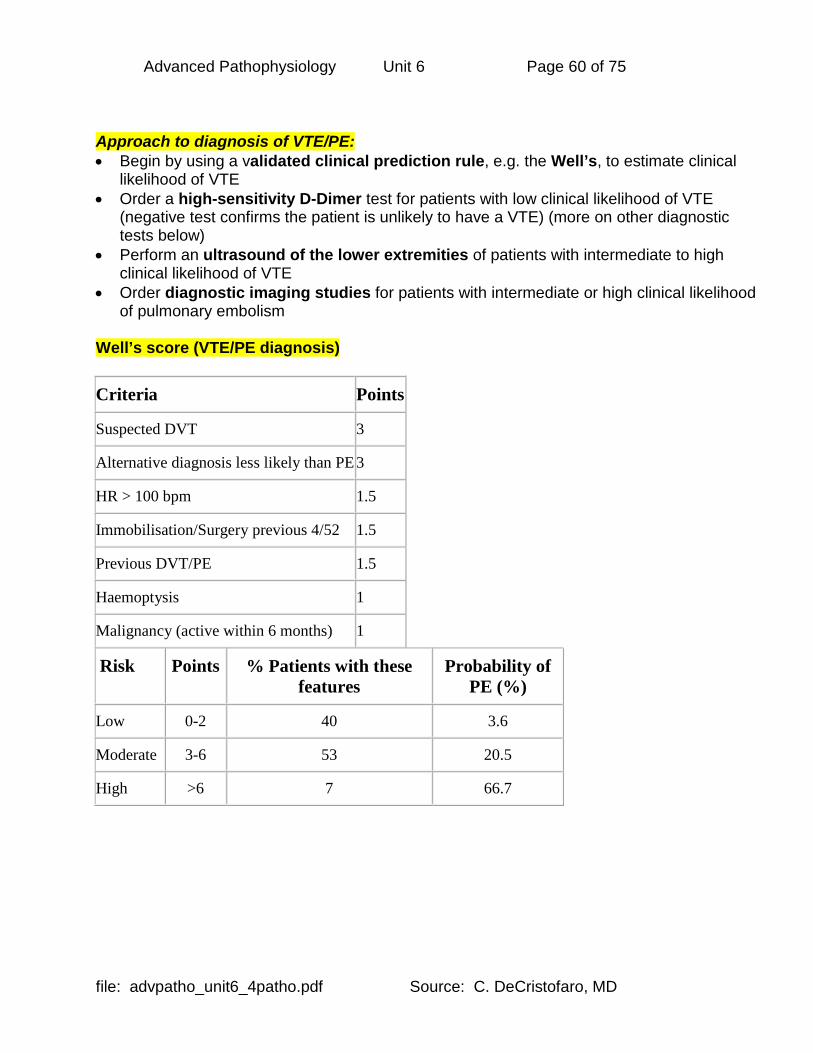
Advanced Pathophysiology Unit 6 Page 60 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Approach to diagnosis of VTE/PE: • Begin by using a validated clinical prediction rule, e.g. the Well’s, to estimate clinical
likelihood of VTE • Order a high-sensitivity D-Dimer test for patients with low clinical likelihood of VTE
(negative test confirms the patient is unlikely to have a VTE) (more on other diagnostic tests below)
• Perform an ultrasound of the lower extremities of patients with intermediate to high clinical likelihood of VTE
• Order diagnostic imaging studies for patients with intermediate or high clinical likelihood of pulmonary embolism
Well’s score (VTE/PE diagnosis)
Criteria Points
Suspected DVT 3
Alternative diagnosis less likely than PE 3
HR > 100 bpm 1.5
Immobilisation/Surgery previous 4/52 1.5
Previous DVT/PE 1.5
Haemoptysis 1
Malignancy (active within 6 months) 1
Risk Points % Patients with these features
Probability of PE (%)
Low 0-2 40 3.6
Moderate 3-6 53 20.5
High >6 7 66.7

Advanced Pathophysiology Unit 6 Page 61 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Geneva score (DVT diagnosis)
Criteria Points
Age 60-79 1
Age > 79 2
Previous DVT/PE 1
Recent Immobilisation/Surgery previous 3
HR > 100 bpm 1
pCO2 < 36 36-39
2 1
pO2 < 49 49-60 60-71 61-82
4 3 2 1
CXR Platelike atelectasis Elevation of hemidiaphragm
1 1
Risk Points % Patients with these features
Probability of PE (%)
Low 0-4 49 10
Moderate 5-8 44 38
High 9-12 6 81

Advanced Pathophysiology Unit 6 Page 62 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Simplified Revised Geneva Score & 2-level Well’s score From: Age-Adjusted D-Dimer Cutoff Levels to Rule Out Pulmonary Embolism: The ADJUST-PE Study. JAMA 2014;311(11):1117-1124. doi:10.1001/jama.2014.2135. At: http://jama.jamanetwork.com/article.aspx?articleid=1841967

Advanced Pathophysiology Unit 6 Page 63 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Capnography & PE:
• PE in spontaneously ventilating patients: o ABG results:
PCO2 goes down due to tachypnea If the embolus is MASSIVE, then PCO2 will go up
o Capnogram results: End-tidal CO2 (capnogram PETCO2) goes down – more dead space Many are saying this is a better bedside test than Well’s prediction
score • PE in mechanically ventilated patients:
o They can’t respond with tachypnea o The PCO2 goes UP and the end-tidal CO2 (capnogram PETCO2) goes down
(more dead space)
EKG findings in PE: • an S1Q3T3 pattern
o a prominent S wave in lead I; a Q wave; inverted T wave in lead III • sinus tachycardia • T wave inversion in leads V1 - V3 (right-heart strain) • Right Bundle Branch Block • low amplitude deflections

Advanced Pathophysiology Unit 6 Page 64 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Laboratory in PE: • D-Dimer (ELISA test):
o elevation indicates high probability of a thrombosis (clot) such as DVT or VTE o also used in the emergency department to help diagnose acute aortic dissection
(AAD) because as the aorta dissects into the aneurismal defect a clot is formed Useful in low PE probability patient
o negative predictive value almost 100% in these patients o positive test prompts admission and observation with fractionated heparin
• ABG (arterial blood gas): (Normal in up to 25% of patients) o Hypoxia: in 75% of patients there will be Hypoxia (PO2 60-70 mm Hg) o Respiratory Alkalosis from tachypnea: PCO2 decreased in 95% of patients (unless
embolus is MASSIVE) due to tachypnea o Mechanically ventilated: PCO2 rises, end-tidal CO2 (PetCO2) goes DOWN
• BNP (Brain natriuretic peptide): o Used in diagnosing HF o Also may predict benign course of PE if value is < 90 pg/mL
• Coagulation studies: o Complications of a PE is the pulmonary infarct, which can induce a
hypercoagulable state o Will probably be starting anticoagulants, to prevent another DVT, so coagulation
studies are important for this reason as well

Advanced Pathophysiology Unit 6 Page 65 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Doppler Ultrasound of lower extremities in PE: • Also called impedance plethysmography • Looking for deep venous thromboses of the lower extremity veins, which give rise to the
embolus that travels to the lung Remember, the PE comes from a DVT that has turned into a VTE (venous thromboembolism): 2D grayscale and color Doppler of superficial femoral DVT with “free-floating” tail

Advanced Pathophysiology Unit 6 Page 66 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Pulmonary Imaging in PE: Ventilation-Perfusion (VQ) scan in PE: • Comparing Ventilation with perfusion (Q = blood flow) • Still the gold standard of NONINVASIVE imaging at most hospitals
o other noninvasive technologies are alternatives (spiral CT, MDCT) • Remember that this study may be hard to evaluate if the patient has underlying pulmonary
pathology and an abnormal CXR • Method:
o Inhale radioactive tracer into lung take picture of VENTILATION scan o Inject radioactive tracer into veins take picture of PERFUSION scan o Any MISMATCH indicates lack of blood flow to the area possible PE
Perfusion Scan Ventilation Scan
Showing high probabilty for PE

Advanced Pathophysiology Unit 6 Page 67 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Spiral CT, CTA & MDCT in PE: • Spiral CT and CT pulmonary angiography (CTA)
o acceptable alternatives to VQ scan as initial NONINVASIVE testing o contrast also can outline the venous system and find clots that are missed on
Doppler ultrasound • Multidetector CT (MDCT) has bee used in CT angiography Picture: from New England Journal of Medicine, 6 March 2008; 358(10):1037-52 (by permission with subscription)

Advanced Pathophysiology Unit 6 Page 68 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
INVASIVE – pulmonary angiography in PE: • Gold standard of INVASIVE testing (risk of complications from procedure) • Sensitivity 98% • FIRST get the VQ scan – only do invasive testing if VQ scan doesn’t match the clinical
picture, or if the VQ scan cannot be evaluated due to technical issues o In many hospitals, spiral CT is done first instead of the VQ scan
Pulmonary Angiogram

Advanced Pathophysiology Unit 6 Page 69 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
CXR in PE: (as in other tests, only SOME patients will have these findings) • USUALLY CXR is normal in PE • Other findings that MAY be seen:
o Westermark sign of dilated proximal pulmonary vessels and distal cutoff o Elevated hemidiaphragm o “Hampton’s Hump” of pleural infiltrate pointed at hilum (wedge-shaped)
Westermark Sign Bloodflow cut off from clot “Hampton’s Hump” in pulmonary infarction

Advanced Pathophysiology Unit 6 Page 70 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
PULMONARY EDEMA & ARDS: • medical emergency – fluid is in the lungs, preventing gas exchange (alveolus isn’t filled with
air any more, it is filled with fluid) • hypoxemia due to Right Left shunting • TYPES:
• Cardiogenic • Noncardiogenic (ARDS, acute lung injury)
1) Cardiogenic Pulmonary Edema: • imbalance of Starling forces – elevated HP overwhelms COP • decompensated left ventricular systolic HF • presentation is similar to non-cardiogenic cause, but CXR is different
o usually has bilateral symmetrical infiltrates in a “bat-wing” appearance, cardiomegaly, Kerley B lines
2) Noncardiogenic Pulmonary Edema – ARDS – what’s in a name?
• “ARDS” came originally from "RDS" (the respiratory distress syndrome of the premature newborn, due to lack of surfactant)
o When it was recognized that a similar pulmonary presentation also occurred in adults, it was named "Adult RDS" -- but this has nothing to do with surfactant
• Currently, the term is “Acute RDS” o The term was designed to alert the healthcare team to the VERY VERY rapid
development of life-threatening pathology that needs IMMEDIATE action o Other terms include:
Noncardiogenic pulmonary edema Increased-permeability pulmonary edema Stiff lung Shock lung Acute lung injury
Resources: NIH and American Lung Association websites: 1) https://www.ncbi.nlm.nih.gov/pubmedhealth/PMHT0022894/ 2) http://www.lung.org/lung-health-and-diseases/lung-disease-lookup/ards/ 3) Good current overview: Thompson, Chambers & Liu (2017). Acute Respiratory Distress Syndrome. N Engl J Med, 377(6), 562-72. Retrieve from http://www.nejm.org/doi/pdf/10.1056/NEJMra1608077

Advanced Pathophysiology Unit 6 Page 71 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Pathophysiology – a response to INJURY:
• capillaries run through the walls of the air sacs (alveoli) and then oxygen diffuses into the bloodstream while carbon dioxide diffuses from blood to alveolar sac – gas exchange
• “leakier” capillaries allow fluid into the alveolar sac – it is now filled with fluid, not air – no more gas exchange
• Histology: o ARDS is associated with diffuse alveolar damage (DAD) and lung capillary
endothelial injury o The early phase is called “exudative” and the later phase is called
“fibroproliferative” Risk factors for ARDS From: Thompson, Chambers & Liu (2017). Acute Respiratory Distress Syndrome. N Engl J Med, 377(6), 562-72. Retrieve from http://www.nejm.org/doi/pdf/10.1056/NEJMra1608077

Advanced Pathophysiology Unit 6 Page 72 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Non-cardiogenic causes of pulmonary edema (ARDS): • permeability pulmonary edema – adult respiratory distress syndrome (ARDS) • note that this is really a response to INJURY and not truly a disease of its own • Criteria:
o there is the ABSENCE of left heart failure to be called ARDS o PaO2/FIO2 <200 because this is a Right Left shunt
• Injury to the lungs that might cause ARDS: o infection (sepsis, pneumonia) o drugs (cocaine, heroin) o trauma (fat emboli, contusion, massive blood transfusion) o toxins (smoke inhalation, high-oxygen therapy from free radical damage causing
diffuse alveolar damage, DAD) o aspiration o pancreatitis
• this is ALSO a restrictive lung disease since fluid-filled lungs become stiff and non-compliant
• Further complications: o treatment is positive end-expiratory pressure (PEEP) by mechanical ventilation
requires HIGHER than normal pressures and complication of barotraumas is a concern
o causes ventilator-induced lung injury (VILI) • Mnemonic: NOT CARDIAC (near-drowning, oxygen therapy, transfusion or trauma, CNS
disorder, ARDS, aspiration or altitude sickness, renal disorder or resuscitation, drugs, inhaled toxins, allergic alveolitis, contrast or contusion)
• CXR: patchy infiltrates, ground-glass appearance, progressing to “white out”
Berlin definition of ARDS From: Thompson, Chambers & Liu (2017). Acute Respiratory Distress Syndrome. N Engl J Med, 377(6), 562-72. Retrieve from http://www.nejm.org/doi/pdf/10.1056/NEJMra1608077
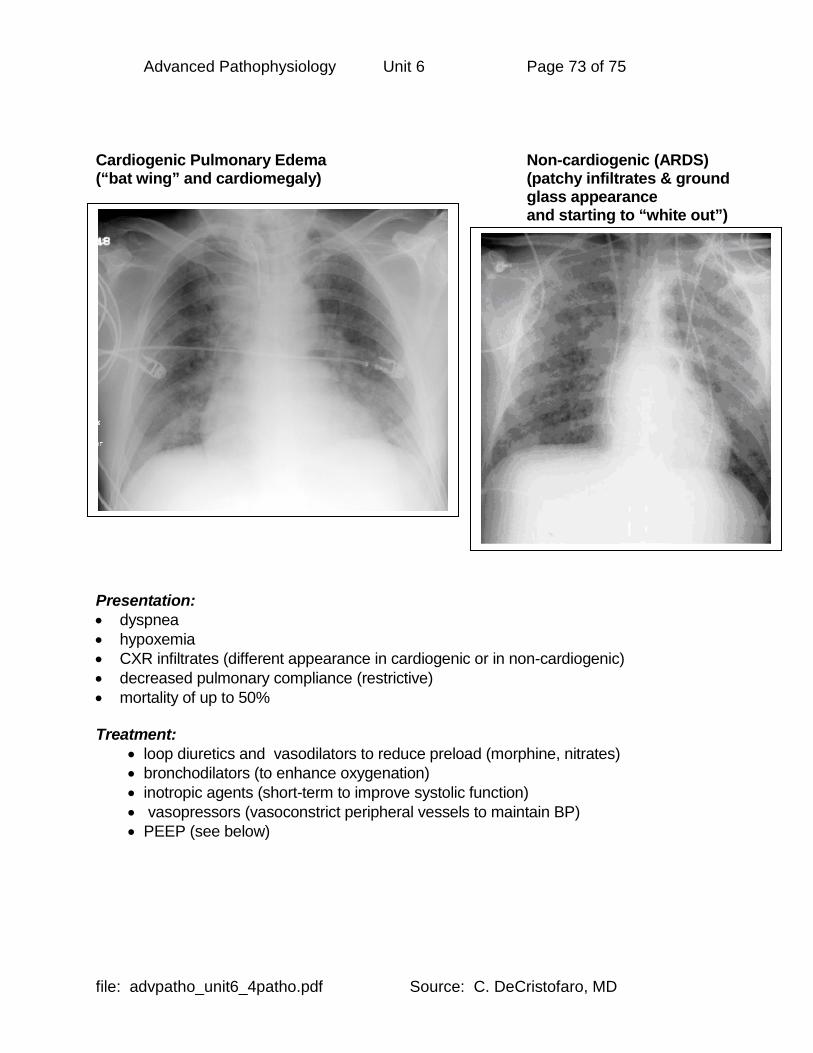
Advanced Pathophysiology Unit 6 Page 73 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
Cardiogenic Pulmonary Edema Non-cardiogenic (ARDS) (“bat wing” and cardiomegaly) (patchy infiltrates & ground
glass appearance and starting to “white out”) Presentation: • dyspnea • hypoxemia • CXR infiltrates (different appearance in cardiogenic or in non-cardiogenic) • decreased pulmonary compliance (restrictive) • mortality of up to 50% Treatment:
• loop diuretics and vasodilators to reduce preload (morphine, nitrates) • bronchodilators (to enhance oxygenation) • inotropic agents (short-term to improve systolic function) • vasopressors (vasoconstrict peripheral vessels to maintain BP) • PEEP (see below)

Advanced Pathophysiology Unit 6 Page 74 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
PEEP: (positive end-expiratory pressure ventilation) • What is PEEP?
o airway pressure is maintained above atmospheric pressure at the end of exhalation by means of a mechanical impedance (e.g. valve)
o purpose is to increase the volume of gas remaining in the lungs at the end of expiration
o this decreases shunting and improves gas exchange o clinical: used in ARDS to allow reduction in FiO2 and thus hopefully reduce
toxicity from oxygen administration • Pulmonary effects of PEEP: pushes extravascular water and improves oxygenation to
increase FRC by distending alveoli and recruiting active alveoli, this decreases shunting (better match of perfusion and ventilation)
• Cardiovascular effects of PEEP: may reduce CO via reduced venous return to the heart (from the lung); may even reduced ventricular compliance and interfere with diastolic filling.
• Clinical objectives in PEEP: o achieve PaO2 60+ at FiO2<50% (assuming normal hemoglobin level)
• What is positive pressure ventilation: o supplementing flow of air during inspiration until a preset pressure is reached
• Asthma and PEEP: o Remember that due to incomplete expiration from bronchospasm, air trapping
can occur. o This can be thought of as “auto-PEEP” (positive end expiratory pressure). o Using extrinsic PEEP will not help ventilation, and in fact can worsen ventilatory
impairment in this situation. Post-obstructive Pulmonary Edema (POPE): • What is it?
o pulmonary edema that develops AFTER the removal of an airway obstruction • Type I:
o occurs after relief from an acute obstruction o example – post-extubation laryngospasm o causes include forceful inspiration against the obstruction, redistributing fluid
from the microvasculature into the lung parenchyma (transudation into alveoli) • Type II:
o occurs after relief from a chronic obstruction o example – after surgery for tonsillar hypertrophy (tonsillectomy) o etiology is thought to be a sudden removal of PEEP (caused by the obstruction)

Advanced Pathophysiology Unit 6 Page 75 of 75
file: advpatho_unit6_4patho.pdf Source: C. DeCristofaro, MD
ACUTE MOUNTAIN SICKNESS & ASSOCIATED CONDITIONS: Acute mountain sickness (AMS) and associated conditions (HAPE, HACE): • Theoretical cause:
o Hypoxemia drives minute ventilation inducing respiratory alkalosis & low CO2 in brain this limits the rise in ventilation and causes AMS
• develops after ascending 1,000 feet in less than 24 hours (the “sleeping altitude” ) • if progresses may develop high-altitude pulmonary edema (HAPE)(fluid in the lungs)
and/or high-altitude cerebral edema (HACE)(fluid in the brain) • Prevention:
o take acetazolamide (Diamox), a carbonic anhydrase inhibitor diuretic, for several days before (& during) the ascent; this diuretic increases CO2 levels in the body/brain (induces a metabolic acidosis)
o Some evidence that the supplement Co-Q-10 may be beneficial o The only thing that will reliably prevent the problem is traveling up altitude very
slowly, only several hundred feet per day (may take weeks to get to high altitude) • Treatment: steroids, vasodilators (move them off the mountain to low altitude!) More on high altitude pulmonary edema (HAPE) and cerebral edema (HACE): • a continuum from acute mountain sickness (AMS)
o retinal hemorrhages and peripheral edema o eventually both cerebral edema and non-cardiogenic pulmonary edema (ARDS)
• Pathophysiology: o from exposure to altitudes > 2000 m (6560 ft) o continuum from acute mountain sickness to full-blown HAPE o affected by rate of ascent (more than 1000 feet per 24 hours), the final “sleeping”
elevation” and (probably genetic) predisposition o loss of NORMAL compensatory responses to reduced oxygen (increase in minute
ventilation) and increase in pulmonary vascular permeability o diagnostic right heart strain pattern on EKG and echocardiogram suggests
pulmonary hypertension o eventual altered mental status, hypotension, and death if left at high
altitude