laura conway msotr/l, cht, comt ue
TRANSCRIPT

Laura Conway MSOTR/L, CHT, COMT UE

Laura Conway MSOTR/L, CHT, COMT UE
Hand Therapy Coordinator-Gulf Coast/ Fieldwork coordinator
Select Live faculty
Select Physical/Hand Therapy, Brandon, Florida, USA
I have no financial relationships to disclose within the past 12 months
relevant to my presentation.

Proprioception
Proprius: belonging to ones own
-ception: to perceive
Dr. Elisabet Hagert

Perception and Control
Posture
Balance
Audiovisual-motor coordination
Joint stability

Preparation for motion
Control of motion
Response to motion

Proprioception- The Info Coming
in
Kinesthesia- The conscious sense of
joint motion
Joint Position Sense-Conscious
appreciation of joint position and angle.
Neuromuscular control- Unconscious
control of joints and reflexes

Kinesthesia
Muscle spindles
Skin –especially important when joint
distant from muscles spindles
Joints play increased roll when
muscle/tendon cross multiple joints

Joint position sense
Also related to muscle spindle input
Trainable
Measureable-documentable

Neuromuscular
Sense/Proprioception
Difficult to quantify.
Essential to control of the muscles
effecting a joint.
Assists in anticipatory control of the
muscles for stability and equilibrium.
Acts with the cerebellum in planning,
anticipating and executing joint control.

Neuromuscular Control
Lack of neuromuscular control places
ligament structures at risk.
System allows for coordinated function
but also protection.
Decreases with fatigue.
Development relies on
repetition.

Unconscious
Involuntary anticipatory neuromuscular
responses for joint stability and control.
Afferent input: muscle and joint
receptors
Regulated by; Rapid spinal cord
reflexes, SM cortex, cerebellum

Conscious
Willful perception of joint motion or position for stability and control
Afferent input: Muscle and skin
Regulated by: Central integration and interpretation, SM cortex, cerebellum
Riemann & Lepart, 2002

Balancing act for function
Ligament muscle reflex vs. Reciprocal
inhibition

Ligament muscle reflex
Initiates opposing muscle group
Fast
Protective

Reciprocal Inhibition
Agonist inhibits antagonist- ie. Bicep
inhibits tricep
Recurrent inhibition-normally synergistic
muscles may become antagonists-ie.
FCU inhibits FCR

Role of the sensory motor
cortices
Conscious control of the joint
Explicit motor planning

Mechanoreceptors-static
Mechanoreceptors are found within the
skin, ligaments and joint capsule.
First line of defense against injury
Pressure
Motion
Velocity
Karagiannopoulos C , Michlovitz: 2016
Mechanoreceptors-dynamic
Muscle spindles
Golgi tendon organs
May be remote i.e. fingers
Handout has detail on
mechanoreceptors

Afferent sensory input
Cerebellum
Sensory motor cortex
Motor output/
Awareness
Dorsal HornAnterior horn
Supraspinal control

Role of the Cerebellum
Unconscious neuromuscular control of
the joint
Regulates descending motor comands

Distribution of mechanoreceptors
in the wrist
Volar and radial ligaments are less
innervated and play a greater role in
stabilization with axial load.

Innervation density
Dorsal Scapholunate
Dorsal radiocarpal
Dorsal intercarpal
Palmar lunotriquetral
Triquetrocapitate/ hamate ligaments
Hagert E. 2010


Goals in proprioceptive retraining
Regain coordinated movement for
activity performance
Gain/regain muscular control to assist in
joint stability

What kinds of injuries result in
proprioceptive disruption?
Ligament injuries
TFCC injuries
Basal thumb osteoarthritis
Fractures
Peripheral nerve injuries
CNS dysfunction-concussion?
Amputation/soft tissue trauma

Sensory Motor Dysfunction after
trauma
Conscious proprioception loss
Sensibility loss
Decreased neuromuscular recruitment
Impaired strength and endurance
Misinterpretation of force/magnitude
Karagiannopoulos C JHT (2013)

How Does This Present in Our
Patients?
Movement disorder.
Dropping objects that they have the
strength to hold.
Balance
Decreased work or athletic performance.

Accurate information
Changes in tissue
may alter accuracy
of information
Pain = inhibition
Eventually cortical
reorganization

What can we do about it?
Education i.e.. “you did not drop the remote because you’re weak”
Tasks that emphasize speed, position in space, motor planning, interpretation and adjustment of posture for force.
Involve the entire body
Provide complex and challenging surfaces and distractions i.e. BOSU
Work on both conscious and unconscious control

Stages of proprioceptive reeducation
Stage Plan Purpose Example
I Basic Rehab Edema and pain control Cold corn
II Proprioceptive
awareness
Promote joint control GMI
III Joint position
sense
Ability to duplicate joint
angle
Blinded passive rom
reproduction
IV Kinesthesia Ability to sense joint
motion without audiovisual
cues
Vision occluded alpabet,
object pass, ball toss
V Conscious
neuromuscular
rehab
Strengthening specific
muscles for joint stability
Isometric
Isokinetic
Eccentric
Co-activation
VI Unconscious
neuromuscular
rehab
Reactive muscle
education
Plyometric
Rhythmic stabilization
Modified from Hagert 2010
JPS- Evaluation
Using 2 paper goniometers reproduce
40 flexion, 20 flexion 30 extension, 50
extension with vision occluded
Patient self monitors
Tape to a mirror to complete
Naveen E et al. Assessing Proprioceptive Function: Evaluating Joint Position
Matching Methods Against Psychophysical Thresholds. Physical Therapy, Volume 94,
Issue 4, 1 April 2014, Pages 553–561


Graded Motor Imagery
Pain control
Visual feedback
Joint positon sense
Stimulate somatosensory cortex

GMI: Procedural Steps
GMI Procedural Order
Laterality Reconstruction
Imagery
Mirror Box Therapy

Motor/functional
empathy
Implicit motor imagery
Explicit Motor imagery
Mirror therapy
Motor/ functional exposure
Occupation/higher level
exposure

Implicit Motor Planning Activity
Recognize app Hand Flash Cards
Magazine
recognition
Circle
○ 5 right hands
○ 5 left hands
○ 5 right eyes
○ 5 left feet

Explicit Motor Imagery
Darts
Putting

Treatment activities:
Mirror Therapy In the box! Prepare your client!
Mirror Box “Rules to Live By:”
1. If it hurts, STOP.
2. Client must watch the mirror at all times
Start non-threatening & progress as able!

At first just have them observe the hand
Remove or add all jewelry to reflect affected hand
Initiate gentle active motion
Progress to object manipulation
Textures
Gripping
Touching face
Ask about changes in symptoms
May be disorienting
Initiate movement inside the box

Treatment activities:
Mirror therapy• Bounce/roll tennis ball
• Smush/squeeze sponges
• Digiflex squeeze
• Theraputty
• Desensitization buckets
• Warm/cold water baths
• Weight bearing exercise
• Continued AROM in all
planes

Kinesthesia
Varied weight ball/sponge/cotton ball toss
Blind targeting-Coins in bankBalls in a cup
Sort byTextureWeight-eggsShapetemperature

Labyrinth lunacy
Tilt Games

Sorting
By weight By Temperature

Texture Resistance to
pressure

Conscious neuromuscular rehab tasks
Mirror feedback
PVC pipe
Theraband alphabet
Kendama
Isometrics
○ Magazine
○ Flexbar
○ Tennis ball and racket
○ Paddle ball
○ Tennis ball bounce
○ Walk outs

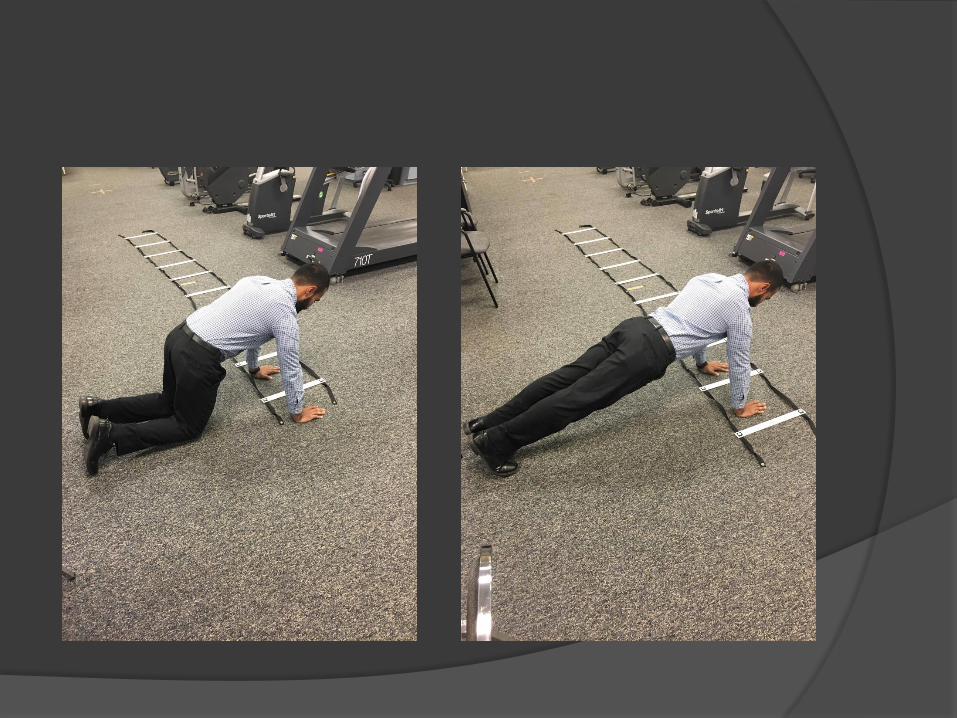
Mirror Feedback
Scapular Stabilization
Also wrist, opposition, elbow ect……..


Weighted alphabet exercises
supine>standing

Coactivation tasks

Conscious neuromuscular
training
Isokinetic
Isometric
Eccentric
Co-activation

Isokinetic exercise
Requires specialized machines
Maintains constant speed throughout
arc of motion despite increased effort
Increases both strength and endurance

Isometric
Performed at a fixed
joint angle
Excellent for building
stability
Decrease
pain/fear/avoidance
Low risk of injury
May be bilaterally
relevant *GMI

Eccentric
Control through deceleration
Activation of antagonist
Greater joint stability
Recruitment

Co-activation
Simultaneous agonist/ antagonist
contraction

Co-activation Tasks/ Unconscious Control
Hula hoop
Body blade
Water bottle
Plank activities
○ Step up
○ Bosu
○ Balance pad
Gyroscope
BOING
PVC pipe

Hula Hoop

BOING

PVC pipes
Various size pipes
2 caps
PVC Glue
Filling
Water
Marbles-add sponges or
fluido medium for sound
Sand
weights
Medium shift from end to
end
Pronation supination
Uni/bilateral
Rapid exchange
***Add Balance mat
BOSU
Occlude vision walk

Gyroscope Ball

Dart Throwers motion
Suggested as a way to stabilize and
minimize risk to a disrupted SL joint
Facilitated FCU and ECRL isolated
motion inhibits ECU to stabilize and
reduce disruption

40 degrees of
extension
20 degrees of radial
deviation
0 degrees of flexion
0 degrees of ulnar
deviation
Earlier, safer more
stable motion.
Functional
Dart Throwers Motion
Garcia-Elias M, Serrallach XA, Serra JM. Dart-throwing motion in patients with scapholunate instability: a dynamic four-
dimensional computed tomography study. J Hand Surg Eur Vol. 2014;39(4):346e35

Tape
Assist
Agonist
Antagonist
Tactile cue

Technology!
Apps-Tilt games Mouse Maze
Fall Down
Aerox
Tilt Maze
Labyrinth lunacy

Functional Tasks
Reassure that they
can use the hand-
just don’t handle the
china.
Complex resistive
patterns that require
frequent
accommodation.
Cleaning, baking,
painting, music.

High Level Additions
Walking
Balance pad
BOSU
Visual distraction
Vision occluded

Labyrinth
Theraband alphabet
Dynaflex
Frisbee with marbles
Varied weight ball toss
Vision occluded coin in bank
Dixie cup ball catch
Paddle ball

Case: Anna
Anna is a 32 y/o female performance
artist/acrobat. She sustained a high
energy Galeazzi fx while performing and
inverted ring act. She was fixated with a
volar plate and immobilized in pronation
for 6 weeks.

1.
FOOSH
2. Radius
FX
4. Distal ulna
migrates distally
4. radius
migrates
proximally
3. DRUJ
disruption
Mechanism
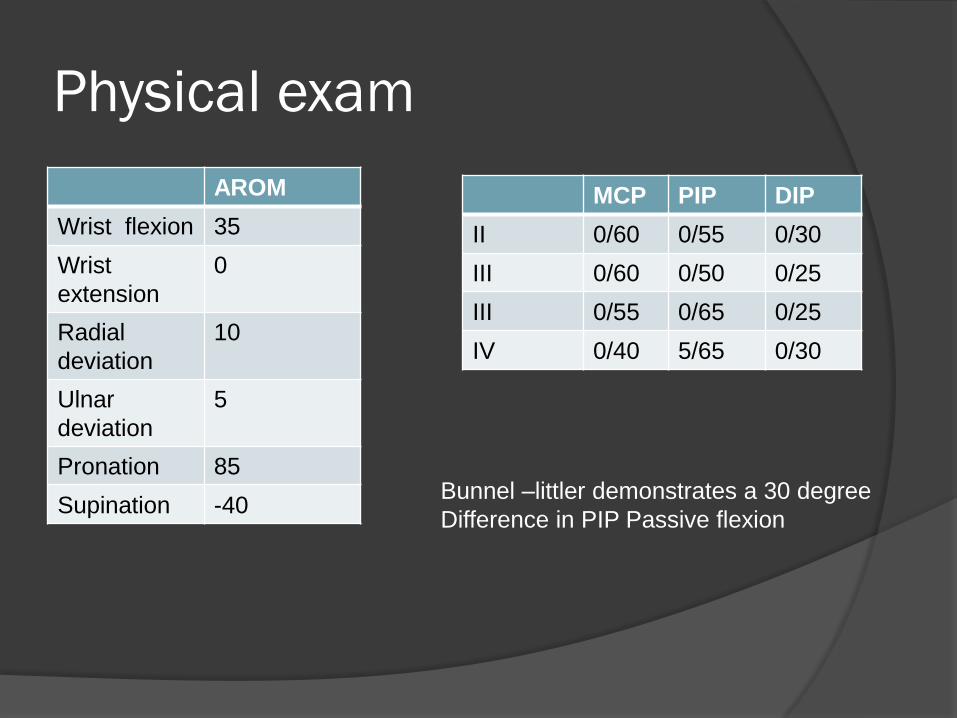
Physical exam
AROM
Wrist flexion 35
Wrist
extension
0
Radial
deviation
10
Ulnar
deviation
5
Pronation 85
Supination -40
MCP PIP DIP
II 0/60 0/55 0/30
III 0/60 0/50 0/25
III 0/55 0/65 0/25
IV 0/40 5/65 0/30
Bunnel –littler demonstrates a 30 degree
Difference in PIP Passive flexion
Impression
Edema
Intrinsic tightness
Supination -40 degrees
Maladaptive grasp pattern- wrist flexed
with grasp
Diffuse hypersensitivity
Highly motivated, athlete

Assessment of JPS
Assess the ability to reproduce a passive joint position after a 3 second delay.
MCID at 8 and 12 weeks
5.0 and 7.09
Greater baseline data
needs investigation
Karagiannopoulos and Michlovitz 2016

Proprioceptive concerns
Highly dynamic vocational needs
Must be able to support her body weight
on wrists when inverted
Must be able to safely lift and support
another performer
High degree of tortion and axial force
across joints
Sense of velocity

Goals
Proximal and distal joint stability
Accurate JPS at speed and under load
Joint protection at extremes of range
Tolerance/ accuracy of assessment of
force through joint
Strength and endurance
Eventual return to performance

Early interventions
Edema management
Cold corn-counter irritant
Functional grasp activities
Gross bilateral activities
GMI
Graded motor imagery
Pain control
Visual feedback
Joint positon sense
Stimulate somatosensory cortex

Late/ advanced interventions
Isometrics
Rhythmic stabilization-water bottle, body
blade
Weight bearing tasks
Eccentrics
Task simulation

Grading
Alter wrist angle
Vision occluded
Unstable surface
Alter shoulder angle
Speed
Unstable weight
Moving feet





Job specific simulation
Rolling stool hand
walks
Sustained overhead
hold with unstable
surface
Sustained overhead
carry
Weight bag lift
Walking/ stepping
with body blade
Weight bag catch
and throw

Dosing
Based on task demands
Begin with high reps
Focus and engagement important
Limit with decreased performance
accuracy*especially with athletes

Outcomes
Wrist extension and supination deficit
Swelling and pain following long practice
or multiple performances
Able to modify her act and perform
safely

Case: Eric
Patient is a 42 y/o RHD male with a 6
month complaint of lateral elbow, forearm
and shoulder pain. He is a competitive
pistol marksman. 3 years ago he was in a
MVA with C3-C5 herniation. Pain after
practice and rapid decline in performance
after ½ hour. Weight trains.

Physical exam
Mills, Cozen’s and Maudsley’s negative.
Gross grip R #124 L #115
No heat upon palpation
Joint play equal bilaterally at the elbow
Pain not reproduced with palpation.

Physical Exam
Unilateral atrophy/ weakness of trapezius, rhomboids, supraspinatus and infraspinatus.
Scapula protracted, elevated and
Positive CPR for cervical radiculopathy (cervical rotation<60, +ULTT, +spurlings, relief with traction) Traction -
Palpation of the triangular interval/ space painful with pain radiating to forearm

Right shoulder has a rounded posture
Tight pec minor, subscapularis, teres
major
Shoulder external rotation 60 (85)
degrees
+ Flip sign
Kibler test 2.5 cm at 45 degrees

Impression
C3-C5 radiculopathy
Suprascapular nerve impairment
Radial nerve irritation
Scapular dyskinesia

Proprioceptive concerns
Decreased triceps, anconeus and wrist extensor control
Scapular position while shooting increases radial nerve symptoms
Poor proximal stability
Radiculopathy
Decreased control with athletic performance
Rapid fatigue with athletic performance
Goals
Increase positional awareness of
scapula throughout range
Increase ability to maintain scapular
stability underload
Increase endurance of scapular
stabilizers

Intervention
PT to address radicular symptoms
Proximal stabilization exercises
Soft tissue mobilization
Neural mobilization
Capsular stretching to regain external
rotation

JPS in the mirror
Begin with static positions
Vision occluded
Unstable surface
Unstable load
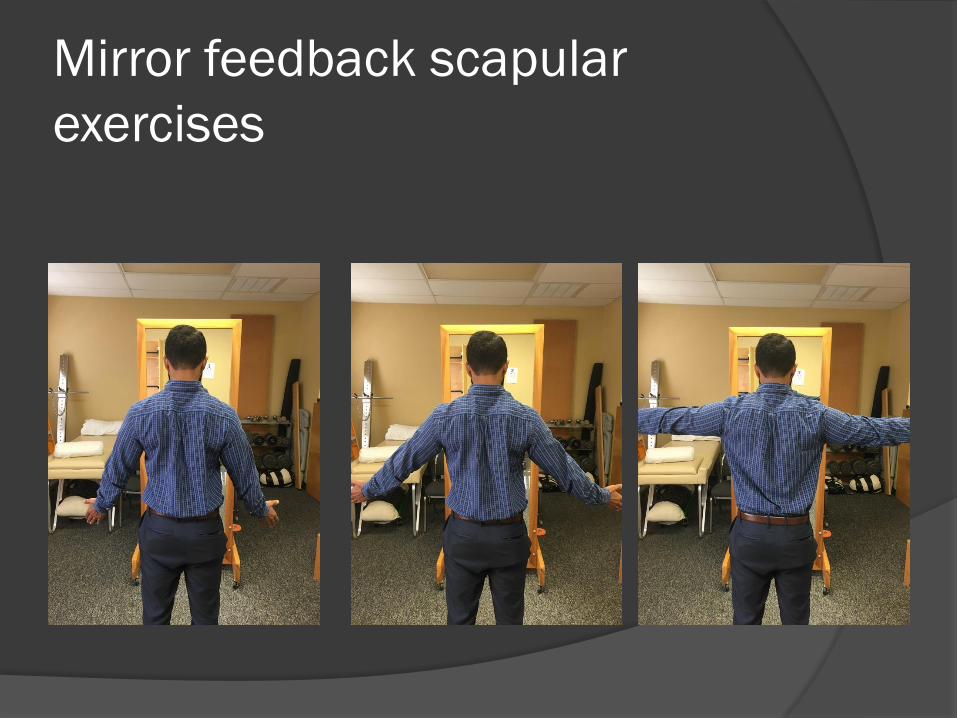
Mirror feedback scapular
exercises

Rhythmic stabilization>adjacent arc of
motion>unstable surface


Weighted alphabet exercises
supine>standing
Outcome
Improved pain
Increased practice time tolerated to
normal
Independent in self management
Referred for reassessment with hand
surgeon and possible neurosurgery
referral

Case: Noreen
Patient is a 65 y/o female 6 weeks s/p
trapeziectomy with ligamentous
reconstruction. Patient is evaluated after
pin and cast removal.
Has the “dropseys”

References
Butler, D. S., & Moseley, L. S. (2003). Explain pain. Adelaide: NOI Publications.
Cavalcante M, Rodriguez C, Mattar R. Mechanoreceptors and nerve endings in the triangular fibrocatilage in the human wrist. J Hand Surg. 2004;29A:432-435.
Garcia-Elias M, Serrallach XA, Serra JM. Dart-throwing motion in patients with scapholunate instability: a dynamic four-dimensional computed tomography study. J Hand Surg Eur Vol. 2014;39(4):346e35
Hagert E. Proprioception of the wrist joint:A review of current concepts and possible implications on rehabilitation of the wrist. JHT . 2010; 23:2-17.
Hagert E, Persson J, Werner M, Llung B. Evidence of Wrist proprioceptive reflexes elicited after stimulation of scapholunate interosseous ligament. J hand Surg AM. 2009:34:642-651.
Hagert E, Ljung B. Differences in the presence of mechanoreceptors and nerve structures between wrist ligaments may imply differential roles in stabilization. J orthop Res. 2005; 757-763.
Karagiannopoulos C, Sitler M, Michlovitz S, Tierney R. A descriptive study on wrist and hand sensory-motor impairment and function following distal radius fracture intervention. JHT. 2013:26: 204-215.
Karagiannopoous C, Michlovitz S. Rehabilitation strategies for wrist sensorimotor control impairment: from theory to practice. JHT. 2016;29:154-165.
Marini F, Squeri V, Morasso P, Masia L. Wrist Proprioception: Amplitude or positional coding?. Frontiers in neorobotics. 2016;10 1-8.
Moseley, G. L., Butler, D.S., Beames, T.B., & Giles, T.J. (2012). The Graded Motor imagery handbook. Adelaide, Australia: Noigroup.
Riemann B, Meyers J, Lepart S. Comparison of ankle, knee, hip and trunk corrective action shown during single leg stance on firm, foam and multiaxial surfaces. Archives of Phys Med Rehab.; 2003:84: 90-95.
Ramachandran, V. S., & Altschuler, E. L. (2009). The use of visual feedback, in particular mirror visual feedback, in restoring brain function. Brain, 132, 1693-1710
Ramachandran, V.S., & Altschuler, E.L. (2010). Reflections on the hand. Pain, 149, 171-172.
Ramachandran, V. S., & Hirstein, W. (1998). The perception of phantom limbs: The D.O. Hebb lecture. Brain, 121, 1603-1630.

Thank You!