kite pharma - jefferies · 2 forward looking statements/safe harbor to the extent statements...
TRANSCRIPT
Kite Pharma:Focused on the CureArie Belldegrun, MD, FACSChairman, President, & Chief Executive Officer
2
Forward Looking Statements/Safe HarborTo the extent statements contained in this presentation are not descriptions of historical facts regarding Kite Pharma, Inc.(“Kite,” “we,” “us,” or “our”), they are forward-looking statements reflecting management’s current beliefs and expectations.Forward-looking statements are subject to known and unknown risks, uncertainties, and other factors that may cause ouror our industry’s actual results, levels or activity, performance, or achievements to be materially different from thoseanticipated by such statements. You can identify forward-looking statements by words such as “anticipate,” “believe,”“could,” “estimate,” “expect,” “intend,” “may,” “plan,” “potential,” “predict,” “project,” “should,” “will,” “would” or the negativeof those terms, and similar expressions that convey uncertainty of future events or outcomes. Forward-looking statementscontained in this presentation include, but are not limited to, statements regarding: (i) the success and timing of ourproduct development activities and clinical trials; (ii) the ability and willingness of the National Cancer Institute (NCI) tocontinue research and development activities relating to our product candidates; (iii) our ability to obtain and maintainregulatory approval of KTE-C19 and any other product candidates; (iv) our ability to further develop and commercialize ourproduct candidates; (v) our plans to research, discover and develop additional product candidates, including through oursubsidiary Kite Pharma EU, and next generation product candidates, including a next-generation CAR with an “on/off”switch; (vi) our and our partners’ ability to develop, manufacture and commercialize our product candidates and to improvethe manufacturing process; (vii) the size and growth potential of the markets for our product candidates, and our ability toserve those markets; (viii) the rate and degree of market acceptance of our product candidates; (ix) our ability to attract andretain key scientific or management personnel; (x) the anticipated timing of clinical data availability; (xi) the anticipatedtiming of commercial launch of KTE-C19; (xii) our plans to expand geographically; (xiii) our ability to meet the milestonesset forth herein and (xiv) our expectations regarding our ability to obtain and maintain intellectual property protection forour product candidates.
Various factors may cause differences between Kite's expectations and actual results as discussed in greater detail in Kite'sfilings with the Securities and Exchange Commission (SEC), including without limitation in its Quarterly Report on Form 10-Q filed with the SEC on May 9, 2016. Except as required by law, we undertake no obligation to publicly update any forward-looking statements, whether as a result of new information, future events or otherwise. This presentation shall notconstitute an offer to sell or the solicitation of an offer to buy securities, nor shall there be any sale of securities in any stateor jurisdiction in which such offer, solicitation or sale would be unlawful prior to registration or qualification under thesecurities laws of any such state or jurisdiction.
Changing
Empowering
Utilizing
Advancing
Optimizing
Building
Kite: Focused on the Cure
a patient’s own immune system to combat cancer
two technology platforms to address both hematologic and solid tumors
our lead product candidate in four pivotal studies and preparing for 2017 commercial launch
and automating in-house manufacturing to bring cell therapies to the broad market
a pipeline of future cancer therapies with innovative internal R&D and collaborations with select industry leaders
the paradigm of cancer treatment
3
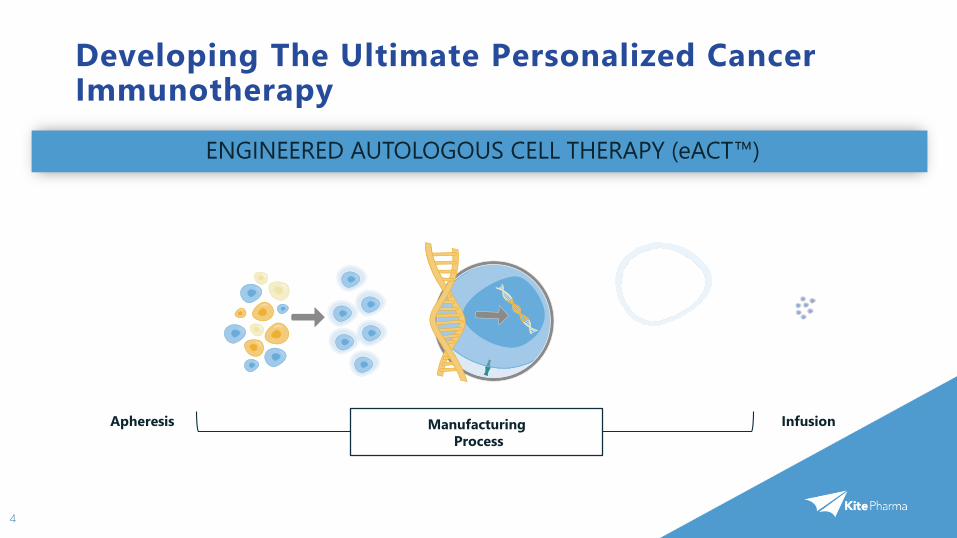
Developing The Ultimate Personalized Cancer Immunotherapy
4
ENGINEERED AUTOLOGOUS CELL THERAPY (eACT™)
Apheresis ManufacturingProcess
Infusion
5
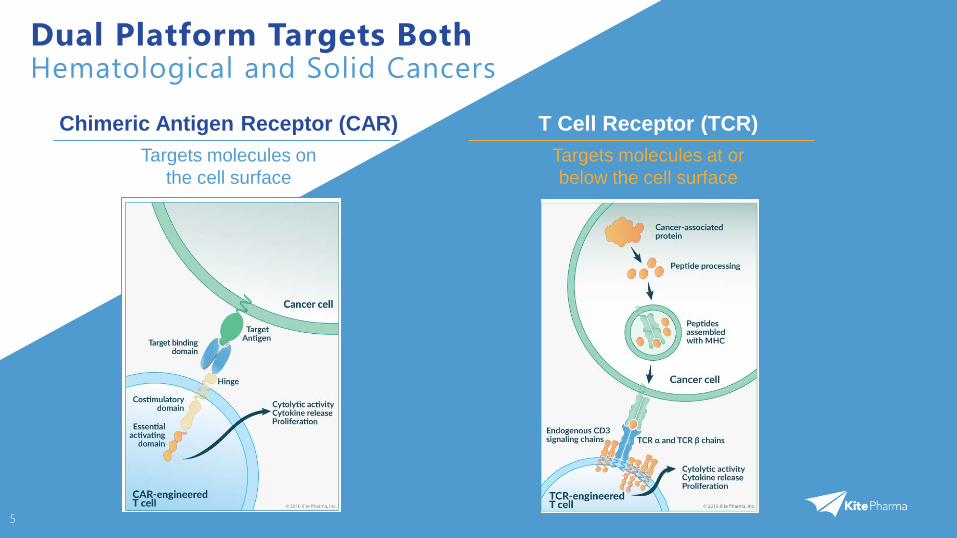
Dual Platform Targets Both Hematological and Solid Cancers
Chimeric Antigen Receptor (CAR)Targets molecules on
the cell surface
T Cell Receptor (TCR)Targets molecules at or below the cell surface
6
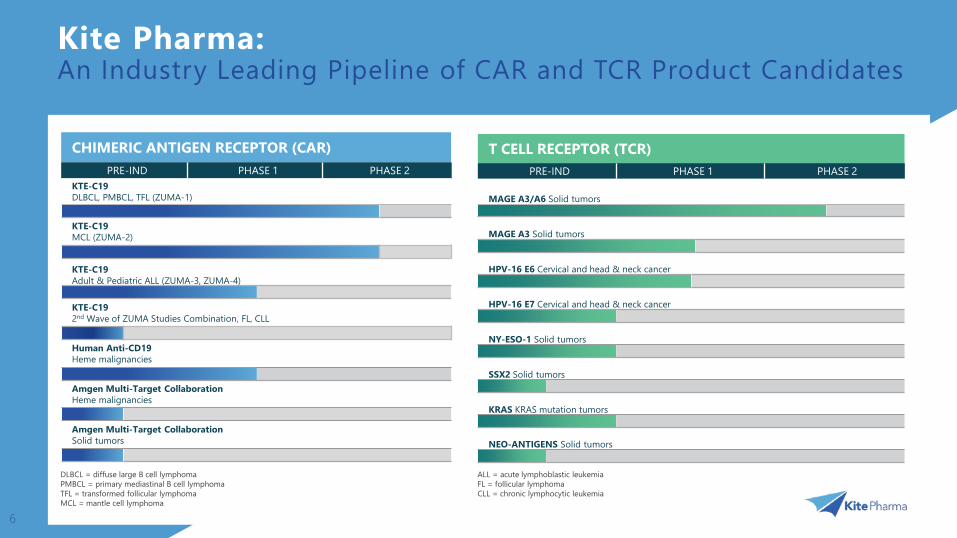
Kite Pharma: An Industry Leading Pipeline of CAR and TCR Product Candidates
DLBCL = diffuse large B cell lymphomaPMBCL = primary mediastinal B cell lymphomaTFL = transformed follicular lymphomaMCL = mantle cell lymphoma
ALL = acute lymphoblastic leukemiaFL = follicular lymphomaCLL = chronic lymphocytic leukemia
CHIMERIC ANTIGEN RECEPTOR (CAR)PRE-IND PHASE 1 PHASE 2
KTE-C19 DLBCL, PMBCL, TFL (ZUMA-1)
KTE-C19 MCL (ZUMA-2)
KTE-C19 Adult & Pediatric ALL (ZUMA-3, ZUMA-4)
KTE-C19 2nd Wave of ZUMA Studies Combination, FL, CLL
Human Anti-CD19Heme malignancies
Amgen Multi-Target Collaboration Heme malignancies
Amgen Multi-Target Collaboration Solid tumors
T CELL RECEPTOR (TCR)PRE-IND PHASE 1 PHASE 2
MAGE A3/A6 Solid tumors
MAGE A3 Solid tumors
HPV-16 E6 Cervical and head & neck cancer
HPV-16 E7 Cervical and head & neck cancer
NY-ESO-1 Solid tumors
SSX2 Solid tumors
KRAS KRAS mutation tumors
NEO-ANTIGENS Solid tumors
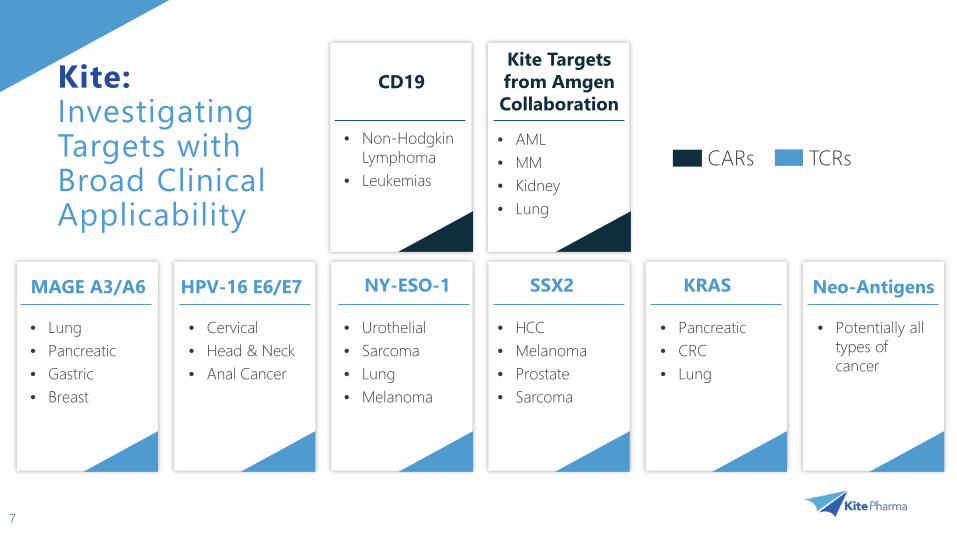
Kite: Investigating Targets with Broad Clinical Applicability
7
CD19
• Non-Hodgkin Lymphoma
• Leukemias
NY-ESO-1HPV-16 E6/E7 SSX2 KRAS Neo-Antigens
• Urothelial• Sarcoma• Lung• Melanoma
• Lung• Pancreatic• Gastric• Breast
• Cervical• Head & Neck• Anal Cancer
• HCC• Melanoma• Prostate• Sarcoma
• Pancreatic• CRC• Lung
• Potentially all types of cancer
TCRsCARs
MAGE A3/A6
Kite Targets from Amgen Collaboration
• AML• MM• Kidney• Lung

Executive Management and Scientific Team Have a Proven Track Record of Success
8
Scientific Advisory BoardOwen N. Witte, MD (Chairman)UCLA
Ronald Levy, MD Stanford School of Medicine
James Allison, PhDThe University of Texas MD Anderson Cancer Center
Antoni Ribas, MD, PhDUCLA
James Economou, MD, PhDUCLA
Padmanee Sharma, MD, PhDThe University of Texas MD Anderson Cancer Center
Zelig Eshhar, PhDTel Aviv Sourasky Medical Center & Weizmann Institute of Science
Inder Verma, PhDThe Salk Institute
Donald Kohn, MDUCLA
Special AdvisorSteven A. Rosenberg, MD, PhD
NCI/KITE CRADA
Kite Pharma EUTon N. M. Schumacher, PhDChief Scientific Officer
Executive ManagementArie Belldegrun, MD, FACSChairman, President and CEO
Cynthia M. ButittaChief Operating Officer
Paul JenkinsonChief Financial Officer
David D. Chang, MD, PhDEVP R&D, Chief Medical Officer
Shawn C. TomaselloChief Commercial Officer
Tim MooreEVP, Technical Operations
Helen S. KimEVP, Business Development
Margo R. Roberts, PhDChief Scientific Officer
Jeff Wiezorek, MD, MSSVP, Clinical Development
Chiron

Strategic Collaborations TCR
CAREnabling Technologies
Surgery Branch
Experimental Transplantation & Immunology Branch
Leveraging Academic and Industry Collaborations for Next Generation Technologies
9

Significant Accomplishments
10
• Initiated four KTE-C19 pivotal studies in DLBCL, MCL, adult, and pediatric ALL under two separate company INDs
• Received Breakthrough Therapy Designation for KTE-C19 under company IND in the US and PRIME Designation in the EU
• Secured Orphan Drug Designation for KTE-C19 in the US and EU for all our hematological indications
• Established European operations with T-Cell Factory acquisition, NKI agreement and launched Kite EU
• Built out the company with the addition of over 100 new hires, including the Chief Commercial Officer and EVP of Technical Operations
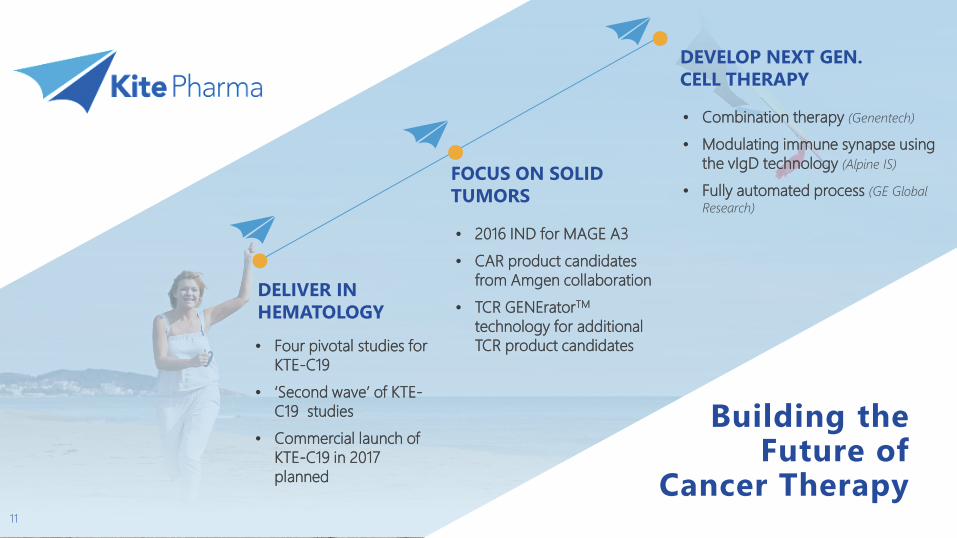
Building the Future of
Cancer Therapy11
DELIVER IN HEMATOLOGY• Four pivotal studies for
KTE-C19• ‘Second wave’ of KTE-
C19 studies • Commercial launch of
KTE-C19 in 2017 planned
FOCUS ON SOLID TUMORS
• 2016 IND for MAGE A3 • CAR product candidates
from Amgen collaboration • TCR GENEratorTM
technology for additional TCR product candidates
DEVELOP NEXT GEN.CELL THERAPY
• Combination therapy (Genentech)
• Modulating immune synapse using the vIgD technology (Alpine IS)
• Fully automated process (GE Global Research)
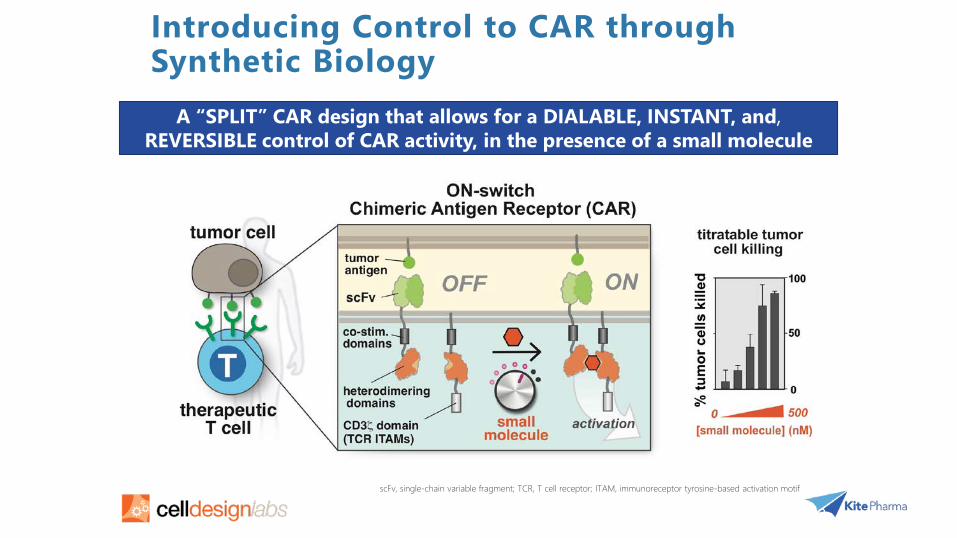
Introducing Control to CAR through Synthetic Biology
scFv, single-chain variable fragment; TCR, T cell receptor; ITAM, immunoreceptor tyrosine-based activation motif
A “SPLIT” CAR design that allows for a DIALABLE, INSTANT, and,REVERSIBLE control of CAR activity, in the presence of a small molecule
32
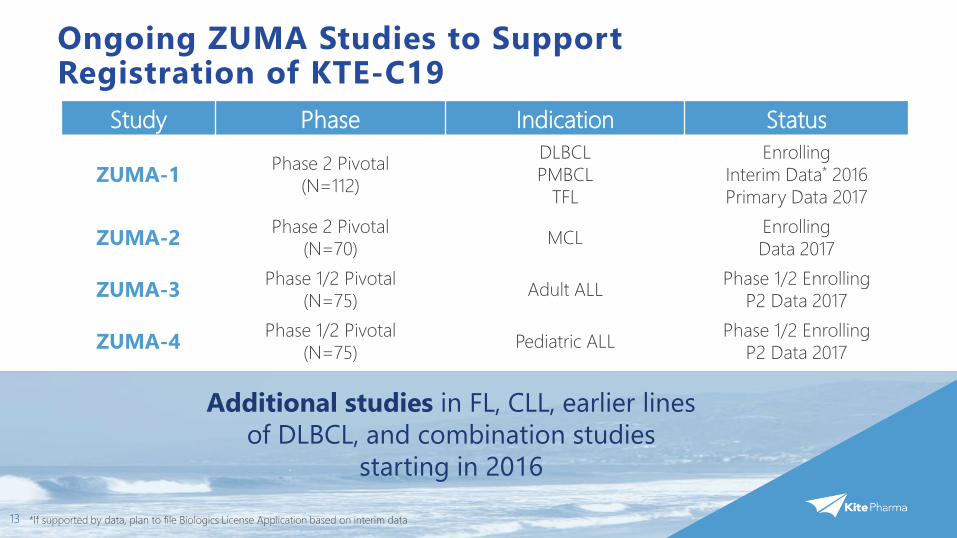
Ongoing ZUMA Studies to Support Registration of KTE-C19
13
Study Phase Indication Status
ZUMA-1 Phase 2 Pivotal(N=112)
DLBCLPMBCL
TFL
EnrollingInterim Data* 2016Primary Data 2017
ZUMA-2 Phase 2 Pivotal(N=70) MCL Enrolling
Data 2017
ZUMA-3 Phase 1/2 Pivotal(N=75) Adult ALL Phase 1/2 Enrolling
P2 Data 2017
ZUMA-4 Phase 1/2 Pivotal(N=75) Pediatric ALL Phase 1/2 Enrolling
P2 Data 2017
Additional studies in FL, CLL, earlier lines of DLBCL, and combination studies
starting in 2016
*If supported by data, plan to file Biologics License Application based on interim data
14
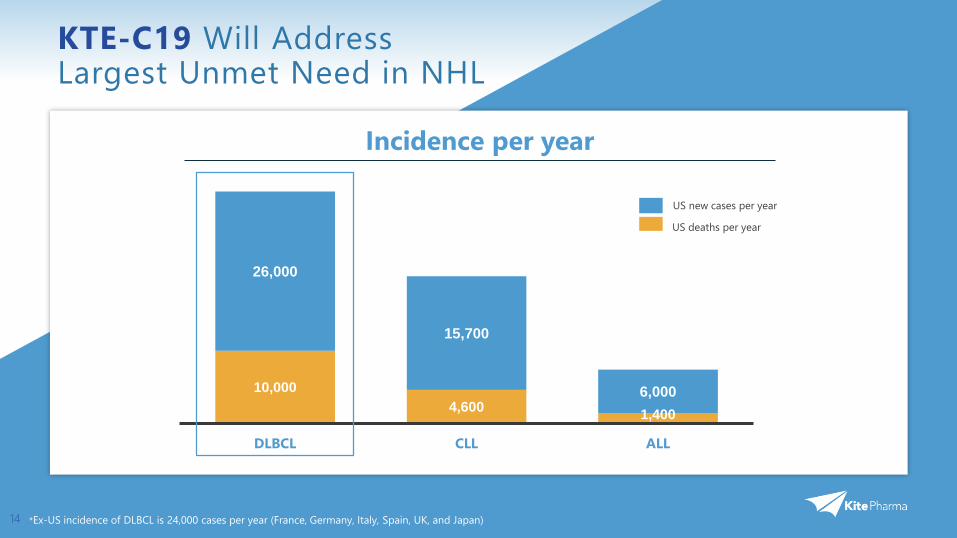
KTE-C19 Will Address Largest Unmet Need in NHL
*Ex-US incidence of DLBCL is 24,000 cases per year (France, Germany, Italy, Spain, UK, and Japan)
10,0004,600 1,400
26,000
15,700
6,000
DLBCL CLL ALL
Incidence per year
US deaths per year
US new cases per year
15
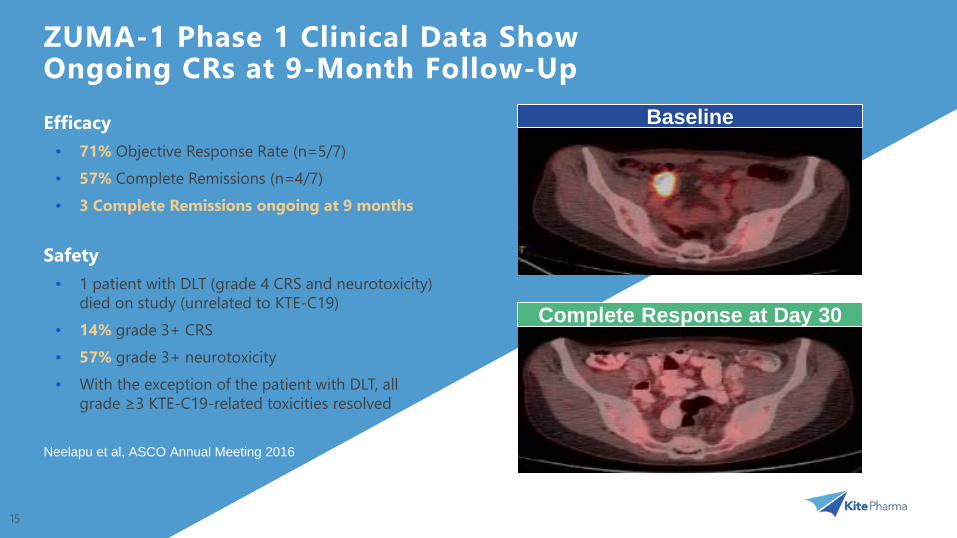
ZUMA-1 Phase 1 Clinical Data Show Ongoing CRs at 9-Month Follow-Up
Complete Response at Day 30
BaselineEfficacy• 71% Objective Response Rate (n=5/7)• 57% Complete Remissions (n=4/7)• 3 Complete Remissions ongoing at 9 months
Safety• 1 patient with DLT (grade 4 CRS and neurotoxicity)
died on study (unrelated to KTE-C19)• 14% grade 3+ CRS• 57% grade 3+ neurotoxicity• With the exception of the patient with DLT, all
grade ≥3 KTE-C19-related toxicities resolved
Neelapu et al, ASCO Annual Meeting 2016

SCHOLAR-1: the first and largest patient-level meta-analysis of chemorefractory DLBCL
SCHOLAR-1 is a retrospective analysis of 635 patients with chemorefractory DLBCL from 4 studies/institutions
Patients with chemorefractory DLBCL have consistently poor outcomes regardless of refractory subgroup, line of therapy, and disease stage
These data provide a historical benchmark for future studies in chemorefractory DLBCL
Median OS
6.6 months
Overall response rate
26% (18% PR & 8% CR)
17
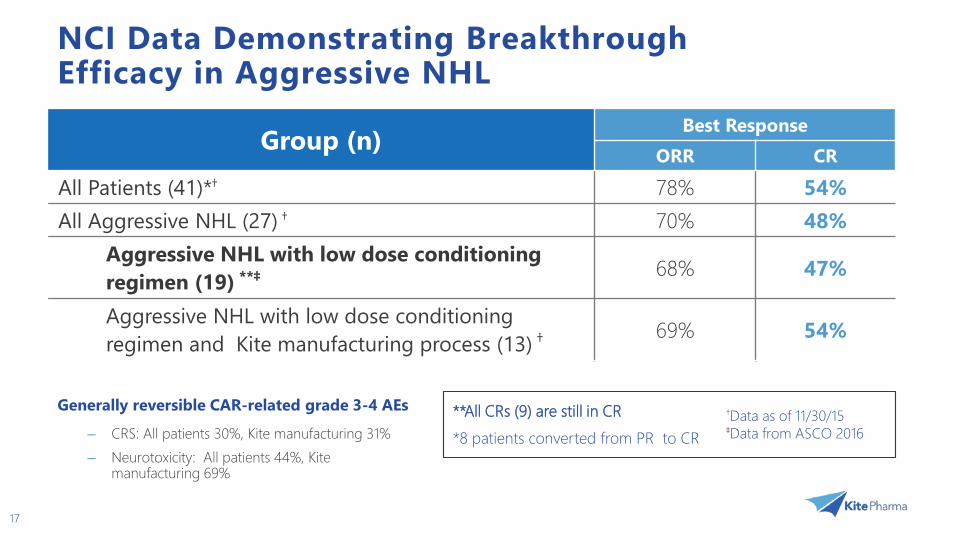
NCI Data Demonstrating Breakthrough Efficacy in Aggressive NHL
17
Group (n) Best ResponseORR CR
All Patients (41)*† 78% 54%All Aggressive NHL (27) † 70% 48%
Aggressive NHL with low dose conditioning regimen (19) **‡ 68% 47%
Aggressive NHL with low dose conditioning regimen and Kite manufacturing process (13) † 69% 54%
†Data as of 11/30/15‡Data from ASCO 2016
**All CRs (9) are still in CR*8 patients converted from PR to CR
Generally reversible CAR-related grade 3-4 AEs
– CRS: All patients 30%, Kite manufacturing 31%– Neurotoxicity: All patients 44%, Kite
manufacturing 69%
18
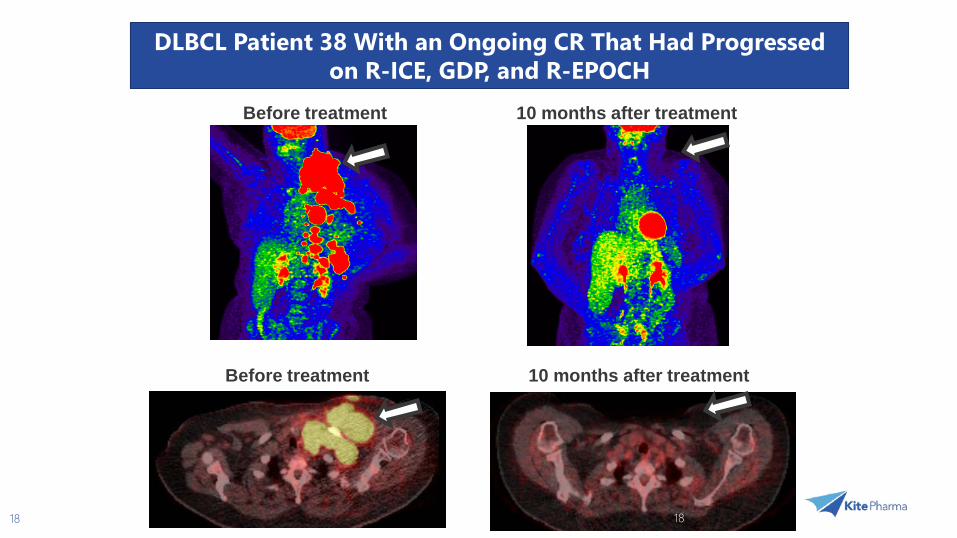
Before treatment 10 months after treatment
Before treatment 10 months after treatment
18
DLBCL Patient 38 With an Ongoing CR That Had Progressed on R-ICE, GDP, and R-EPOCH

19
Manufacturing On Track for KTE-C19 Launch in 2017
In-house clinical manufacturing in full operation
Commercial facility in close proximity to LAX airport
Capacity to produce 4,000-5,000 patient therapies per year
Modular design is scalable and cost effective
Site to produce KTE-C19 and all TCR products

4 Ongoing Registration Studies in >40 Sites
9
21
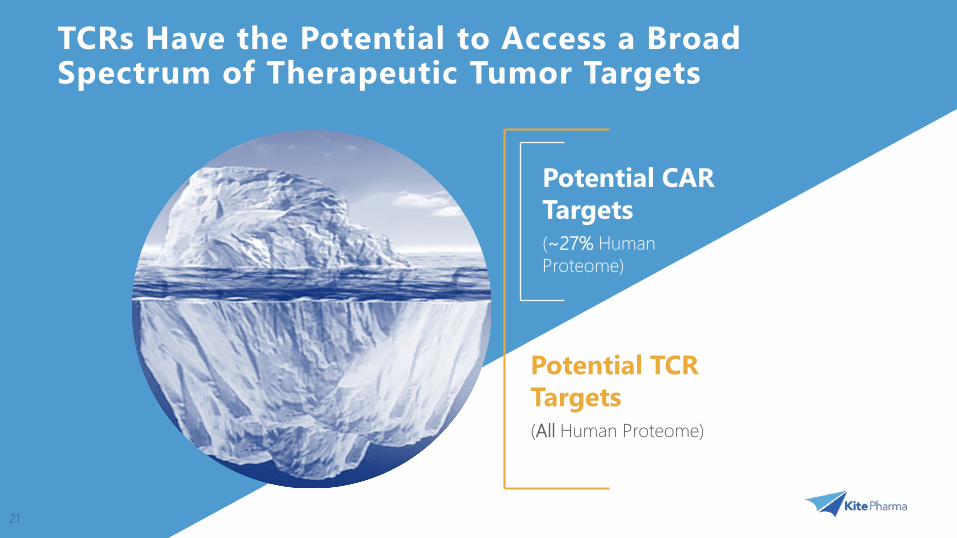
TCRs Have the Potential to Access a Broad Spectrum of Therapeutic Tumor Targets
Potential CAR Targets(~27% Human Proteome)
Potential TCR Targets(All Human Proteome)
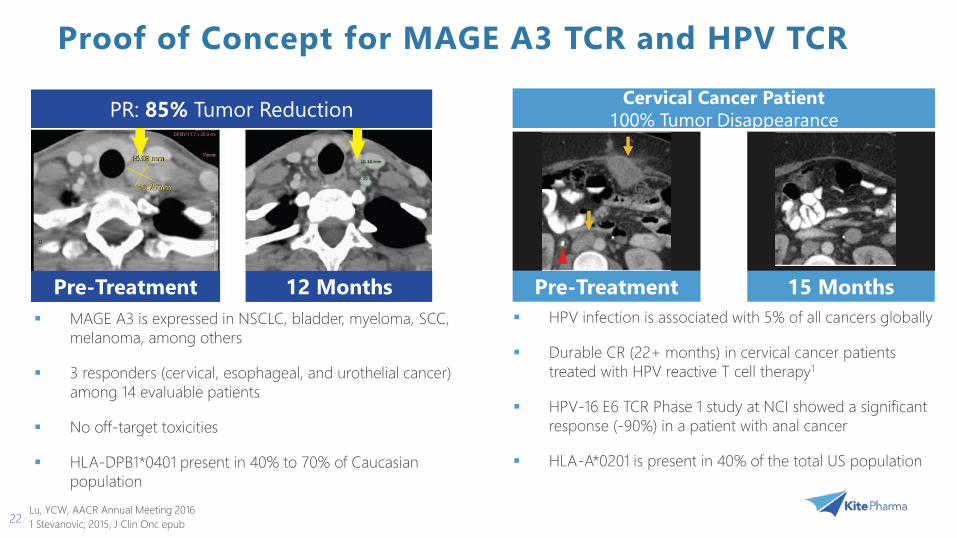
Proof of Concept for MAGE A3 TCR and HPV TCR
22
MAGE A3 is expressed in NSCLC, bladder, myeloma, SCC, melanoma, among others
3 responders (cervical, esophageal, and urothelial cancer) among 14 evaluable patients
No off-target toxicities
HLA-DPB1*0401 present in 40% to 70% of Caucasian population
PR: 85% Tumor Reduction
Pre-Treatment 12 Months
Cervical Cancer Patient100% Tumor Disappearance
HPV infection is associated with 5% of all cancers globally
Durable CR (22+ months) in cervical cancer patients treated with HPV reactive T cell therapy1
HPV-16 E6 TCR Phase 1 study at NCI showed a significant response (-90%) in a patient with anal cancer
HLA-A*0201 is present in 40% of the total US population
Pre-Treatment 15 Months
Lu, YCW, AACR Annual Meeting 20161 Stevanovic, 2015, J Clin Onc epub
Innovating the Next Generation of Products
23
Validate Target Selectivity Advance Cancer-Specific
Targets
Target Selection
Improve Target Fidelity of CAR/TCR Constructs
Modulate CAR/TCR Function in vivo
Reduce Immunogenicity
CAR/TCROptimization
Automate Manufacturing Selectively Expand Potent T
Cell Subsets ex vivo
Manufacturing
Overcome Immune Suppression
Combination Therapy Introduce Gene Editing or
Gene Modulation
Tumor Microenvironment
Optimize in vivo T Cell Expansion Improve Safety Management Identify Predictive Biomarkers for
Safety and Efficacy
Clinical Development
2016 Projected Milestones
Report interim data for Phase 2 ZUMA-1
File KTE-C19 BLA on interim data
Complete qualification/validation of manufacturing facility
Initiate KTE-C19 clinical studies in Europe
Initiate Phase 1b/2 combination study of Kite’s KTE-C19 and Genentech’s atezolizumab
File IND for first Kite TCR product: MAGE A3
25
Changing
Empowering
Utilizing
Advancing
Optimizing
Building
Kite: Focused on the Cure
a patient’s own immune system to combat cancer
two technology platforms to address both hematologic and solid tumors
our lead product candidate in four pivotal studies and preparing for 2017 commercial launch
and automating in-house manufacturing to bring cell therapies to the broad market
a pipeline of future cancer therapies with innovative internal R&D and collaborations with select industry leaders
the paradigm of cancer treatment
25