innovation presentation - agency for clinical innovation · abn 89 809 648 636 (c•)) call for...
TRANSCRIPT

Innovation Presentation: Template
Name Position Facility

Issues Identified
__j Window Dama g e - Forward l__ ~---~----~(L~l~,~l~2~,~R~1~,~R~2~)~------_J~
Condition: A forward flight deck w indow has one or more of these:
• An electrical arc • A delamination • A crack
Objective:
• Is shattered .
To remove electrical power, If needed, to prevent arcing. To reduce differential pressure and descend if the inner pane is shattered or cracked .
Ll:J c Ri I GjG 1 Choose one:
W indow is d e laminated only:
Continue normal operation .
•••• W indow is arcing:
.,..,.Go t o s tep 2
Window Is crack e d or shattered:
.,..,.Go t o step 5
2 WINDOW HEAT switch (affected w indow) ...... . . .. ... . ... . . OFF
Limit a irspeed to 250 Knots maximum below 10,000 feet.
3 Pull both WINDSHIELD AIR controls. This vents conditioned air to the inside of the w indshield for defogging .
4 Continue normal operation .
•••• T Continued on next pea- T
Borille~- C'oforr-08orlq:.M.a,tlc~-«AI*1~..-.8AM MfW.,...t•*"too•
April 25,2013 06-27l70-7Q8·VOZ(Q8) I . I I
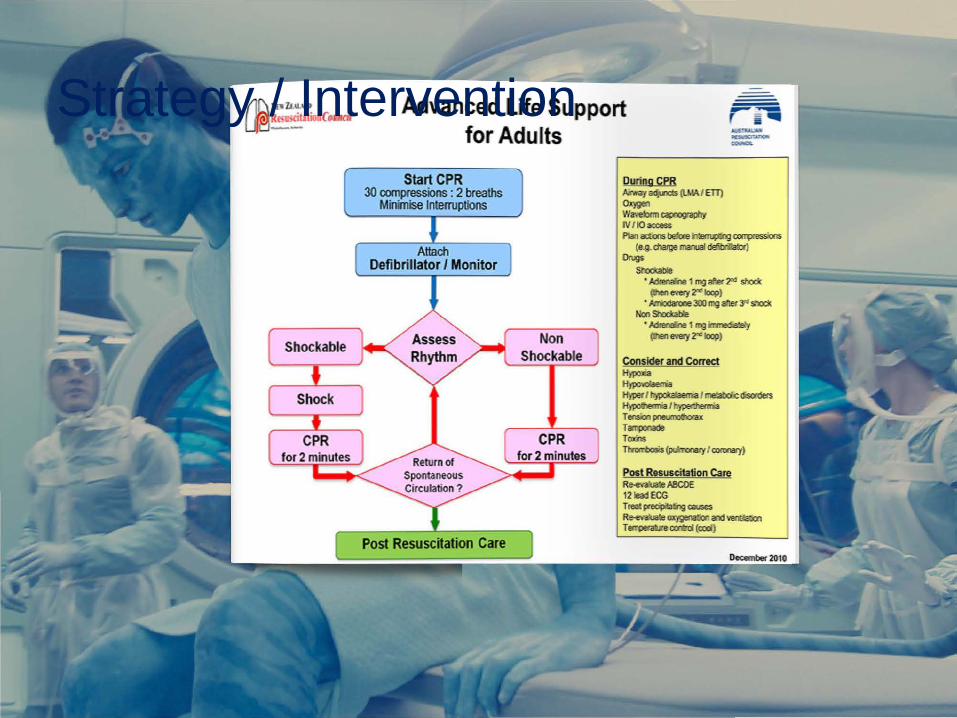
Strategy / Intervention
Advanced Life Support for Adults
Start CPR 3() compressions : 2 breaths
Mininise Interruptions
Attach Defibrillator I Monitor
Post Resuscitation Care
Non Shockable
CPR
Ourina CPR Mlr.TJ-a6Jrds (UIA/ ETT) OX)9EI:l W<M!iJrm ~IO!Ja¢"1 IV / 10 access ftarl acUins bebe Mm.¢ngWI\XessUIS
(e.~chatge nam1 detirra:ct) ~
Shx:i<able • ~ 1 mg af'er2" slafc
(!hen e=y l"" loop) ' AlriOcl;rone 300 rrg after ~ sllocX
Non Shcdable • lodleoalne 1 mg irlvnedia:a'y
(lhen e=y zx loop)
Consider and Correct Hypoxia Hypodaetria Hypef I h')'potalaema I ne!abcU:: disorders Hyopollelrria f l"lypEdhenria Tension~ T~ Tams Tmrnbosis ~/cnronary)
Post Resuscitation Care ~ABCtlE 12 1eadECG Treol ~~causes R...~~andverda:xn Tenpm.reooo:za (cool)

Outcomes / Results and
NO PULSE
(c••) CALL FOR HELP
Attach defibrillat or or monit or
CPR: 30 COMPRESSIONS : 2 BREATHS
<: 100 PER MINUTE
START CPR
<: 5 CM DEEP
ROTATE COMPRESSORS
MINIMISE INTERRUPTIONS
0 CRASH CART
Paddles cr pads in left '11 daxillary line over sixth intercostal space and r ight parasternal area over secord intercostal space. In patients with a PPM or lCD put paddles or pa:ls on the chest wall at least 8 CJTl from the PPM or lCD.
Airw~y adjun:ts (LMA or ETI)
High-flow oxygen
Intravenous or intraosseous ~ccess
Waveform capnography
Plan actions before interrupting compressions
If the rhythm is shockable (VF or pulseless VT) the'l shock
For al shocks use monophasic 360 J or biphasic 200 J
CPR 2 minutes
continued next page

www.ecinsw.com.au
Level 4, Sage Building , PO Box 699 T 02 9464 4674 www.ecinsw.com.au
67 Albert Avenue, Chatswood NSW 2067 Chatswood NSW 2057 F 02 9464 4728 ABN 89 809 648 636

(C•)) CALL FOR HELP
Protect airway
l ligh-flow oxygen
Attem pt IV access
.1.1.\ INFORM TEAM
If IV access then take blood tor FBC, EUC, CaMgPh, anticonvulsant levels, and cult ure
Check blood glucose (from IV or fingerprick). If blood glucose < 3.5 mmoi/L then give ......IV dextrose 10% 5 mL/ <g, followed by infusion of IV dextrose 10% at 5 ml/kgthour, and check blood glucose again in 5 mintues.
Unless given pre-hospital. give:
IV or IM midazolam 0.15 mg/kg (see chart below, maximum 5 mg)
buccal or intranasal midazolam 0.3 mg/kg (see chart below, max1mum 10 mg)
IV diazepam 0.25 mg/kg (maximum 10 mg)
Age (years) Weight Midazolam Midazolam IV/IM Buccal/Intranasal
< 1 5 - 10kg 0.75- ' .5 mg 1.5-3mg
1. 2 10 kg 1.5mg 3mg
1-4 1 s ke 2.?<; me 4.Sme
5-6 20 kg 3 mg 6mg
7. 10 30 kg 4.5mg 9mg
11 '2 40 kg 5 mg 10mg
>13 50 kg S mg 10mg
If still fitting after 5 minutes g1ve:
IV or IM midazolam 0.15 mg/kg (see chart on previous page, maximum 5 mg)
buccal or Intranasal mldazolam 0.3 mg/kg (see chart, maximum 1 o mg)
IV diazepam 0.25 mg/kg(maximum 10 mg)
If still fitting after 5 minutes g1ve:
IV or 10 phenytoin zo mgtkg over 20 m1ntues (or IV/10 phenytion 1 o mgtkg if already on phenytoin) with ECG monitoring. Phenytoin is preferred over the next two options.
IV or 10 phenobarbitone 20 mgt kg (or IV/10 phenobarbitone 10 mglkg if already on phenobarbitone)
if no IV or 10 access give PR paraldehyde 0.4 mllkg diluted 50:50 with NSaline or olive oil (do not give IV or 10 or IM)
If seizures continue:
seek expert advice
consider rapid sequence induction w1t h thiopentone or propofol
consider pyridoxine
arrange PICU transfer

lnflllte cuff to 20 to JO cmll 20
Check tube placement:
end-tidal co, (If us1ng eolounmeter then "go for go d. w1th1n SIX breaths)
auscultation
Secure tube
Record position at lips (approximately 21 em in females. 23 em in males)
IF ASTHMA OR COPD THEN GO TO PAGE 34 (OBSTRUCTIVE STRATEGY)
INITIAL VENTILATOR SETTINGS FOR LUNG-PROTECTIVE STRATEGY
Mode VC-SIMV
VT 6 mL/kg of ideal body weight
5' 5'2" 5 '4" 5'6" 5'8" 5'10" 6' 6'2" 6 '4" Height
1~cm1~cm1~cm1~cm1ncm 1ncm 1~cm1~cm1~cm
VTmale 305 320 3€0 385 415 440 470 490 520
VT female 275 295 330 360 385 415 440 470 490
VT pregnant 370 390 440 480 510 550 585 625 650
RR 18 /min
Pmax40cmH,O
20
"~~ 2 60 RR 18/min
FiO, start at FiO, 100% and PEEP 5, then titrate to saturations 88 to 95%
FiO,(%)
PEEP (cmH,U)
I:E 1:1 .5
40 40
s
Autoflow on with slope.../
continued next page
so 8
50 EO 70 70 70
1U 1U lU 12 14
80
14
90
14

(C•)) CALL FOR HELP .. 0 CRASH CART
If newborn is term gestation, breathing or crying and good tone, then:
routine care
prevent heat loss
stay with mother
ongoing evaluation
If not term gestat ion, breat hing or crying, or good tone, then:
prevent heat loss
ensure open airway
stimulate
If heart rate > 100 and laboured breathing or persistent cyanosis. then:
ensure open airway
monitor oxygen saturations
ron~irlPr CPAP
If he~rt r~te < 100, gasping or apnoea, then for 30 seconds:
positive pressure ventilation
monitor oxygen saturations
It heart rate < 1 oo then tor 30 seconds:
ensure open airway
reduce leaks
constder increasing pressure and oxygen
If he~rt r~te < 60 then for 30 seconds:
add chest compressions (three compressions then a breath, at a rate of one compression every half a second)
100% oxygen
consider intubation or LMA
If heart rate< 60 then:
continue chest compressions
intravenous or intraosseous access (consider umbilical vein catheter; the umbilical stump has one vein and two arteries)
IV adrenaline 10 to 30 meg/kg (0.1 to 0 .3 ml /kg of 1:10,000 adrenaline, ~ 1 mL of 1:10,000 adrenaline for an average term nevtborn)
consider volume expansion (IV normal sa ine 10 ml/kg)
If heart rate< 60 after a few minutes then:
repeat IV adrenaline 10 to 30 meg/kg (0.1 to 0.3 mUkg of 1 :10,000)
consider volume expansion (IV normal sa ine 10 ml/kg)
seek expert advice
Target pre-ductal (right hand) oxygen saturations after birth:
1 minute 60.70 'lo
2 minutes 65.86 'lo
3 minutes 70.90 'lo
4 minutes 75 · 90 'lo
5 minutes 80 · 90 'lo
10 minutes 85. 90 'lo

Airwoy .. ....... .. ............ 1
Anar>hyl.:>xis . .. . . . . .. 1 0
Asystole. .. ... .. .. . ........ 1 ~ BrudyLardta .. .. ......... 1 7
f'EA. ...... .. . ... ............. 19
Sratus Fpl/cptkus ....... 73 svr . ........................... .. 2~ TdchycanJia .................. 26 1 orsa<.1es ...... ..... ........ . 79
Ventilation ............. .. ... 30
VF ......................... ...... :Jg VT ...... . ...................... 4~ VT- PuJsete..,s .......... . . 4S
ACI
PAEDIATRIC
Rrc~dyc f( It l PFA
'>tdtu EpiiL·ptt '-'> <,vr TcJch).( rc/1
VI
VJ
VT f>t (>/
NEWBORN
...
~ Emergency ~ Care Tnslitute
~
60 .63
.b8
11
16
18 .. ..... 80
83 .88
91