in vivo imaging of apoptosis in patients with acute stroke ... clark.pdf · in vivo imaging of...
TRANSCRIPT

B R A I N R E S E A R C H 1 1 0 3 ( 2 0 0 6 ) 1 3 – 1 9
ava i l ab l e a t www.sc i enced i r ec t . com
www.e l sev i e r. com/ l oca te /b ra in res
Research Report
In vivo imaging of apoptosis in patients with acute stroke:Correlation with blood–brain barrier permeability
Mordechai Lorberboyma,⁎, Francis G. Blankenbergb, Menahem Sadehc, Yair Lamplc
aDepartment of Nuclear Medicine of the Edith Wolfson Medical Center, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, IsraelbDepartment of Radiology, Stanford University Hospital, 300 Pasteur Drive Stanford, CA 94305, USAcDepartment of Neurology of the Edith Wolfson Medical Center, Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel
A R T I C L E I N F O
⁎ Corresponding author. Fax: +011 972 3 53584E-mail address: [email protected] (M
0006-8993/$ – see front matter © 2006 Elsevidoi:10.1016/j.brainres.2006.05.073
A B S T R A C T
Article history:Accepted 15 May 2006Available online 30 June 2006
Background: We wished to determine the ability of radiolabeled annexin V to concentrate atsites of ischemic injury in patients with acute cerebral stroke. Secondly, we sought tocorrelate annexin V imaging in these patients with the degree of blood–brain barrier (BBB)breakdown. Methods: Twelve patients with acute stroke had a complete neurologicalexamination, including the National Institutes of Health (NIH) stroke scale and theGlasgow Coma Score (GCS). A non-contrast CT scan was performed on all patients. A SPECTof the brain was obtained 2 h after injection of annexin V. The integrity of the BBB wasevaluated in seven patients using Tc-99m-DTPA brain SPECT. Results: All patients had aninfarct in the MCA territory. Eight patients had abnormal increased annexin V activity,which was more common in patients with cortical strokes (P = 0.01). The concentration ofannexin had no correlation to the volume of stroke, but it was significantly and inverselyrelated to the GCS on admission (r = −0.7, P = 0.02). Foci of apoptosis were notedcontralateral to the affected hemisphere as well. All seven patients who underwent DTPASPECT showed breakdown of the BBB. DTPA uptake was significantly and positivelyassociated with NIH score (r = 0.80, P = 0.01) and inversely associated with GCS (r = −0.89,P = −0.03). Conclusion: This study shows that it is possible to identify in vivo regions ofischemic neuronal injury using radiolabeled annexin V in patients with acute stroke.Annexin imaging can play a major role in the selection of therapy in the initial periodfollowing stroke in adults.
© 2006 Elsevier B.V. All rights reserved.
Keywords:Acute strokeApoptosisBlood–brain barrierAnnexin V
1. Introduction
The use of technetium-99m hydrazine nicotinamide labeledannexin V (99mTc-HYNIC-annexin V), an in vivo imagingmarker of apoptosis, has been reported in several clinicalinvestigations of acute heart transplant rejection, myocardi-al ischemia, and tumor treatment (Belhocine et al., 2002;Haas et al., 2004; Kartachova et al., 2004; Narula et al., 2001;
94.. Lorberboym).
er B.V. All rights reserved
Thimister et al., 2003). However, there have been nopublished reports on the clinical use of 99mTc-HYNIC-annexin V for the imaging of patients suffering fromcerebral artery stroke or other neurologic diseases such asmultiple sclerosis, Alzheimer's, ALS, and the autoimmunecerebral vasculitides in which apoptosis may play a signif-icant role (Du et al., 1996; Hara et al., 1997; Thompson, 1995;Vexler et al., 1997).
.

14 B R A I N R E S E A R C H 1 1 0 3 ( 2 0 0 6 ) 1 3 – 1 9
In one experimental model, 99mTc-HYNIC-annexin Vimaging was able to detect neuronal apoptosis within 2 hafter reversal of global hypoxia (D'Arceuil et al., 2000).Abnormally increased uptake of annexin V occurred despitethe presence of an intact blood–brain barrier (BBB) asassessed by co-injection of In-111 DTPA and dual energyscintigraphy as well as concurrent Gd-DTPA bolus trackingincluding delayed post-Gd-DTPA MR imaging of the brainand cerebellum. In a second model, remarkable focalradiolabeled annexin uptake was observed as soon as 2 hafter reperfusion injury, well before any evidence of BBBbreakdown as confirmed by concurrent Gd-DTPA bolusperfusion and delayed post-Gd-DTPA MR scanning (Mari etal., 2004). In both models, 99mTc-HYNIC-annexin V was co-injected with equimolar amounts of fluorescent labeledannexin V. Surprisingly, fluorescent annexin V was able topass the intact BBB and localize within the cytoplasm ofischemic neurons despite its relatively high molecularweight of 35 kDa. These results suggest the existence of anactive annexin V uptake mechanism by which this proteincan cross the BBB and the cell membrane of ischemic or“physiologically stressed” neurons.
Other studies on animal models have shown that reducedblood flow to the brain can alter the BBB permeability andregulatory transport functions (Belayev et al., 1996; Kuroiwa etal., 1988). We have shown in a human study that Tc-99m-DTPA brain SPECT is the technique of choice for theassessment of BBB disruption. Combined with quantitativeanalysis in patients with acute stroke, SPECT imaging of theBBB is significantly related to clinical outcome (Lorberboym etal., 2003).
Considering that stroke is the third most common cause ofdeath and a major cause of long-term disability (Peters et al.,1998), imaging studies have an important role in assessing thelocation and extent of the stroke, in determining tissueviability, in patient prognosis and in clinical management.Understanding the pattern and distribution of apoptosis instroke may elucidate the mechanisms of neuronal injury andrepair, which may lead to new therapies that may preventneuronal loss.
In this current investigation, we wished to determine if99mTc-HYNIC-annexin V SPECT imaging could detect sites ofischemic injury as identified on CT scanning on admission ofpatients suffering from an acute stroke. Secondly, we wishedto correlate annexin V uptake with the location and degree ofdisruption of the blood–brain barrier (BBB) as assessed byfollow up SPECT with 99mTc-DTPA performed 1 day afterannexin V imaging.
2. Results
2.1. Normal distribution of annexin V
At 2 h post-injection of Tc-99m-annexin V in all five controlpatients, activity was noted in the calvarium, venous sinusesand choroids plexus, with minimal blood-pool activity. Noparenchymal uptake of annexin V was observed within thecerebrum or posterior fossa in control patients.
2.2. The volume of stroke
Abnormal annexin uptake had no correlation to the volume ofstroke as at CT. The volume of stroke was significantly relatedto the NIH and GCS scores (P = 0.01).
2.3. Annexin V imaging in patients with acute stroke
Eight patients had abnormal increased uptake of annexin Vcorresponding to the pathological infarct regions identified byCT (Fig. 1). The mean AI was 4.7 ± 4.7 (range 1.6–15.6, Table 2).The uptake was either focal or multifocal in these 8 cases.Abnormal annexin uptake was present in all 7 patients withcortical strokes and in 1 of 5 patients with subcortical strokes(P = 0.01). Abnormal annexin uptake was significantly andinversely related to the consciousness score on admission(r = −0.7, P = 0.02). In five of eight patients with abnormalstudies, foci of annexin V uptakewere also noted contralateralto the affected hemisphere.
2.4. DTPA SPECT imaging
All seven patients who underwent DTPA SPECT showedbreakdown of the BBB. The mean DI was 9.9 ± 7.9 (range 3.2–26.3). DTPA ratio was significantly and positively associatedwith NIH score (r = 0.80, P = 0.01) and inversely associated withGCS (r = −0.89, P = −0.03). There was no significant correlationbetween the AI and the DI (r = −0.28, P = 0.54). In all cases,image fusion showed only partial overlap between DTPA andannexin V: DTPA was more widely distributed, except in onecase (Fig. 2).
3. Discussion
Apoptosis plays a critical role in the pathogenesis of a numberof disorders including cerebral and myocardial ischemia,autoimmune and neurodegenerative diseases, epilepsy, trau-matic brain injury, organ and bone marrow transplantrejection, and tumor response to chemotherapy and radiation(Belhocine et al., 2002; Blankenberg et al., 1998; Vriens et al.,1998).
Intranucleosomal DNA fragmentation, a main feature ofthe PCD pathway of cell death, has been found in animalmodels of brain ischemia and in human post-stroke tissue(Chen et al., 1997). Twomain pathways have been identified asplaying a role in the PCD pathway after stroke. The caspase-dependent pathways are characterized by expression andactivation of caspase-3 (Chen et al., 1998) and overexpressionof X-chromosome-lined inhibitors of caspase-3 and caspase-7(Namura et al., 1998). This pathway is rapidly activated afterischemia in the penumbral area. The caspase-independentpathway is based on activation of apoptosis-inducing factor(AIF) and its release from damagedmitochondria (Zhang et al.,2002). It seems that the latter pathway is also activated post-ischemia in the penumbral region.
Regardless of the particular trigger, all cells, includingneurons, rapidly redistribute phosphatidylserine (PS, a anionicconstitutive membrane lipid) from the inner to outer leaflet of

Fig. 1 – Annexin V in stroke. (A) Annexin V brain SPECT in a patient with a right peri-ventricular stroke, showing a widerdistribution of annexin (top, arrows) compared to the CT findings (bottom). (B) Another patient with a cortical stroke localized tothe left MCA region shows extensive stroke on CT (bottom) with selective uptake of annexin in the same region (top, arrows),crossing the midline.
15B R A I N R E S E A R C H 1 1 0 3 ( 2 0 0 6 ) 1 3 – 1 9
the plasma membrane lipid bilayer shortly after the onset ofapoptosis (van Heerde et al., 1995). It is at this point thatannexin V, an endogenous human protein, recognizes andbinds to membrane-bound PS that is selectively expressed onapoptotic cells (Zwaal and Schroit, 1997). Due to its highaffinity for PS expressing cells, annexin V has been labeledwith fluorescein dyes for the in vitro detection of apoptoticneurons, fibroblasts, carcinomas, lymphomas, as well ashematopoietic, endothelial, smooth muscle, and embryoniccells (O'Brien et al., 1997).
Recent investigations have shown that pathophysiologicstresses on neurons and other cells can also cause low tointermediate levels of PS exposure without being associatedwith an irreversible commitment to cell death in whichmuch higher levels of PS would be expected (Geske et al.,2001; Hammill et al., 1999). These lower levels of PSexpression have been linked to a newly described endocyticpathway that is activated by annexin V (Kenis et al., 2004).Annexin V binding to sites of PS exposure reverses themovement of PS containing domains within the cell
membrane from blebbing (evagination) into invagination.This results in formation of annexin V containing intracel-lular vesicles, thereby permitting the trafficking of thisprotein within apoptotic cells. Furthermore, this annexin Vpump mechanism appears to exist in vivo in cardiomyocytesthat express PS reversibly on their surface in the setting ofmild ischemia/reperfusion-related stress. This endocyticpump may be the mechanism by which radiolabeled andfluorescent forms of annexin V gain access to the brainthrough the BBB and neuronal membranes in experimentalanimal models of cerebral ischemia (D'Arceuil et al., 2000;Mari et al., 2004).
Radiolabeled forms of annexin V have also been used invitro and more recently in vivo for the detection of apoptoticcells and tissues (Blankenberg et al., 1998). Organ uptakevalues and absorbed doses indicate that Tc-99m-annexin isaccumulated mainly in the kidneys and to a lower degree inthe liver and spleen (Kemerink et al., 2001). Since uptake in thenormal brain is negligible, it is an ideal tracer for imagingapoptosis in this organ.

Fig. 2 – Annexin V compared to DTPA distribution. Two patients, one with a left MCA stroke (A) and one with a right MCAstroke (B), showing annexin uptake in the stroke region (top, arrows), with more extensive Tc-99m-DTPA uptake in thecorresponding regions (bottom).
16 B R A I N R E S E A R C H 1 1 0 3 ( 2 0 0 6 ) 1 3 – 1 9
In this study, the uptake of annexin V was evident notonly in the ischemic hemisphere but also in the contralat-eral “normal” hemisphere, suggesting contralateral neuronalinjury and/or stress after acute stroke in a similar fashion asthat observed in experimental animal models (D'Arceuil etal., 2000; Mari et al., 2004). Significant increases in thetranscription of a number of genes within both hemispheresand striatum in animals suffering from unilateral MCAischemic injury have been noted by previous investigators(Kim et al., 1998; Rohatgi et al., 2004). A genetic link wassuggested for contralateral brain injury mediated via dia-schisis, possibly induced from the ischemic cortex andstriatum through a polysynaptic transneural pathways.Polysynaptic pathways may also be activated with highlevels of excitatory neurotransmitter release causing contra-lateral stress with subsequent PS exposure on neuronsoutside the actual site of infarct.
These observations further support the idea that annexinV imaging of PS expression in the human brain may definetissues at risk for cell death that may recover or be amenable
to therapeutic intervention. Because the actual cell loss inthese patients is gradual in contrast to the immediateirreversible damage caused by severe prolonged ischemia,there may be a therapeutic window to inhibit (or reverse)early apoptosis with pharmacologic blockade.
One potential downside to the use of HYNIC-annexin V isthe relatively high nonspecific uptake of the tracer in thecalvarial bone marrow that may limit its usefulness inperipheral lesions of the posterior fossa and skull base.SPECT/CT or fusion imaging with separate SPECT and imagedata sets may help but are not likely to completely solve theproblem of confounding calvarial bone uptake as spatialregistration and image fusion are rarely ideal in the clinicalsituation. Possible solutions involve the use of alternativeforms of radiolabeled annexin V such as annexin V-128 (Taitet al., 2005). This recombinant mutant of human annexin Vcan be site-specific labeled 99mTc on a five-amino acid tag.Once labeled, annexin V-128 has a markedly lower (less than10%) nonspecific renal cortical and bone marrow uptake oftracer as compared with HYNIC-labeled annexin V. Annexin
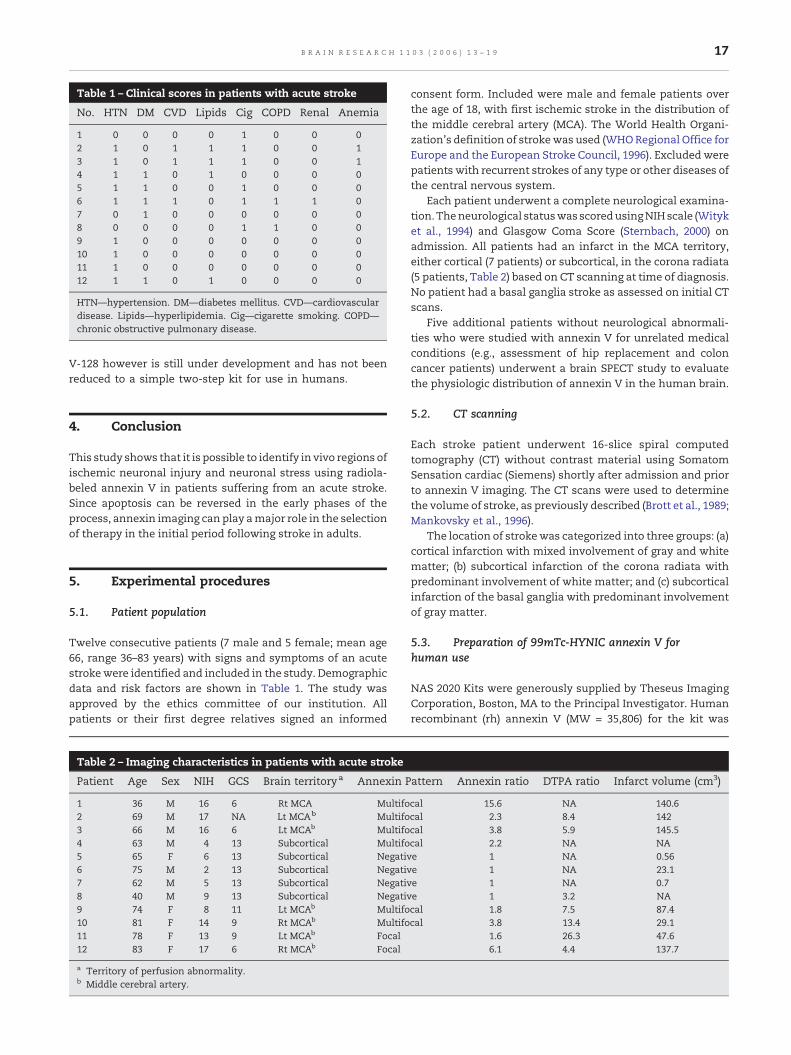
Table 1 – Clinical scores in patients with acute stroke
No. HTN DM CVD Lipids Cig COPD Renal Anemia
1 0 0 0 0 1 0 0 02 1 0 1 1 1 0 0 13 1 0 1 1 1 0 0 14 1 1 0 1 0 0 0 05 1 1 0 0 1 0 0 06 1 1 1 0 1 1 1 07 0 1 0 0 0 0 0 08 0 0 0 0 1 1 0 09 1 0 0 0 0 0 0 010 1 0 0 0 0 0 0 011 1 0 0 0 0 0 0 012 1 1 0 1 0 0 0 0
HTN—hypertension. DM—diabetes mellitus. CVD—cardiovasculardisease. Lipids—hyperlipidemia. Cig—cigarette smoking. COPD—chronic obstructive pulmonary disease.
17B R A I N R E S E A R C H 1 1 0 3 ( 2 0 0 6 ) 1 3 – 1 9
V-128 however is still under development and has not beenreduced to a simple two-step kit for use in humans.
4. Conclusion
This study shows that it is possible to identify in vivo regions ofischemic neuronal injury and neuronal stress using radiola-beled annexin V in patients suffering from an acute stroke.Since apoptosis can be reversed in the early phases of theprocess, annexin imaging can play amajor role in the selectionof therapy in the initial period following stroke in adults.
5. Experimental procedures
5.1. Patient population
Twelve consecutive patients (7 male and 5 female; mean age66, range 36–83 years) with signs and symptoms of an acutestrokewere identified and included in the study. Demographicdata and risk factors are shown in Table 1. The study wasapproved by the ethics committee of our institution. Allpatients or their first degree relatives signed an informed
Table 2 – Imaging characteristics in patients with acute stroke
Patient Age Sex NIH GCS Brain territory a Annexin P
1 36 M 16 6 Rt MCA Multifo2 69 M 17 NA Lt MCAb Multifo3 66 M 16 6 Lt MCAb Multifo4 63 M 4 13 Subcortical Multifo5 65 F 6 13 Subcortical Negativ6 75 M 2 13 Subcortical Negativ7 62 M 5 13 Subcortical Negativ8 40 M 9 13 Subcortical Negativ9 74 F 8 11 Lt MCAb Multifo10 81 F 14 9 Rt MCAb Multifo11 78 F 13 9 Lt MCAb Focal12 83 F 17 6 Rt MCAb Focal
a Territory of perfusion abnormality.b Middle cerebral artery.
consent form. Included were male and female patients overthe age of 18, with first ischemic stroke in the distribution ofthe middle cerebral artery (MCA). The World Health Organi-zation's definition of strokewas used (WHORegional Office forEurope and the European Stroke Council, 1996). Excluded werepatients with recurrent strokes of any type or other diseases ofthe central nervous system.
Each patient underwent a complete neurological examina-tion. Theneurological statuswas scoredusingNIHscale (Wityket al., 1994) and Glasgow Coma Score (Sternbach, 2000) onadmission. All patients had an infarct in the MCA territory,either cortical (7 patients) or subcortical, in the corona radiata(5 patients, Table 2) based on CT scanning at time of diagnosis.No patient had a basal ganglia stroke as assessed on initial CTscans.
Five additional patients without neurological abnormali-ties who were studied with annexin V for unrelated medicalconditions (e.g., assessment of hip replacement and coloncancer patients) underwent a brain SPECT study to evaluatethe physiologic distribution of annexin V in the human brain.
5.2. CT scanning
Each stroke patient underwent 16-slice spiral computedtomography (CT) without contrast material using SomatomSensation cardiac (Siemens) shortly after admission and priorto annexin V imaging. The CT scans were used to determinethe volume of stroke, as previously described (Brott et al., 1989;Mankovsky et al., 1996).
The location of strokewas categorized into three groups: (a)cortical infarction with mixed involvement of gray and whitematter; (b) subcortical infarction of the corona radiata withpredominant involvement of white matter; and (c) subcorticalinfarction of the basal ganglia with predominant involvementof gray matter.
5.3. Preparation of 99mTc-HYNIC annexin V forhuman use
NAS 2020 Kits were generously supplied by Theseus ImagingCorporation, Boston, MA to the Principal Investigator. Humanrecombinant (rh) annexin V (MW = 35,806) for the kit was
attern Annexin ratio DTPA ratio Infarct volume (cm3)
cal 15.6 NA 140.6cal 2.3 8.4 142cal 3.8 5.9 145.5cal 2.2 NA NAe 1 NA 0.56e 1 NA 23.1e 1 NA 0.7e 1 3.2 NAcal 1.8 7.5 87.4cal 3.8 13.4 29.1
1.6 26.3 47.66.1 4.4 137.7

18 B R A I N R E S E A R C H 1 1 0 3 ( 2 0 0 6 ) 1 3 – 1 9
produced by expression in Escherichia coli as previouslydescribed (Funakoshi et al., 1987). Hydrazine nicotinamide(HYNIC) derivatized annexin V was prepared for later radi-olabeling with a 99mTc-tricine precursor complex according toprior protocols (Larsen et al., 1995; Vanderheyden et al., 2002;Verbeke et al., 2003).
The two-vial kit includes a vial of 0.5 ml (0.25 mg) frozenliquid HYNIC-rh-annexin V conjugate solution (vial 1) and avial of lyophilized stannous tricine containing approximately20 mg tricine and 500–650 μg stannous chloride (vial 2).Radiolabeling was conducted at room temperature. 30–50 mCi(0.4–0.6ml) of Tc-99m-pertechnetate was added to the HYNIC-rh-annexin V conjugate (vial 1). The lyophilized stannoustricine (vial 2) was reconstituted with 3 ml of sterile saline.Then, an aliquot of 0.3 ml of stannous tricine solution wasadded to the HYNIC-rh-annexin V vial. The vial was mixedgently, allowed to incubate at room temperature, diluted bythe addition of 2 ml sodium chloride for injection, and testedfor quality by visual inspection, pH, and radiochemical puritytesting with instant thin layer chromatography (ITLC) SG andACD (acid citrate/dextrose) solution, and pH strips necessaryfor the quality control of the product. Radiochemical purity ofthe drug product was verified to be greater than 90%radiochemical purity, as determined by ITLC (ACD) in eachdose administered. Each 15 mCi to 20 mCi (555 to 740 MBq)99mTc-HYNIC-rh-annexin V dose was administered throughan indwelling intravenous (IV) line, utilizing the sterile syringefilter (0.22 μm) supplied as part of each 99mTc-HYNIC-rh-annexin V kit.
5.4. Annexin V SPECT imaging
SPECT images were obtained in the study group shortly afterthe CT scan. In two patients, the study was performed lessthan 24 h after the onset of stroke symptoms and in theremaining 10 patients at 24–48 h after the stroke. A dual headgamma camera (Elscint-Helix, Haifa, Israel) equipped with apair of low energy, high-resolution collimators was used.Images were acquired in a 128 × 128matrix at 6° angular steps,with 40 s in each step.
Acquired images were transferred to a dedicated Xelerisworkstation (General Electric Medical Systems) for processing.Raw SPECT data were reconstructed using a commerciallyavailable Ordered Subset Expectation Maximization algorithm(OSEM; two iterations, ten subsets) and post-filtered using aButterworth filter (cutoff frequency, 0.5; order, 10.0). TheSPECT images were evaluated together with the CT scan.
A quantitative index of apoptosis (AI) was defined as theratio of mean count per pixel in the infarcted region comparedto the mean count per pixel in the contralateral hemisphere,in areas without increased annexin V uptake.
5.5. DTPA SPECT imaging
The integrity of the BBB was evaluated in a subgroup of sevenpatients available for imaging (6 with cortical and one withsubcortical stroke) using DTPA brain scintigraphy at 24 h afterthe annexin imaging. Each patient in this subgroup received740 MBq Tc-99m-DTPA, and a SPECT study was performed 2 hlater, using the same acquisition parameters as outlined
above for annexin imaging. A quantitative index of BBBbreakdown (disruption index, DI) was defined as the ratio ofmean count per pixel in the infarcted region compared to themean count per pixel in the contralateral non-affectedhemisphere.
Image fusion of the annexin V and DTPA studies wasperformed with a commercially available software programusing a semi-automatic voxel-based algorithm. Both SPECTstudies were evaluated based on fused images and on side-by-side evaluation as well.
5.6. Statistical analysis
Analysis of data was carried out using SPSS statistical analysissoftware (SPSS Inc., Chicago, IL, USA, 1999). Normalcy ofdistribution of continuous variables was assessed using theKolmogorov–Smirnov test (cutoff at P = 0.05). Values werecompared by each of the comorbidities using the t test forindependent samples. Associations between continuous clin-ical and imaging data were described using Pearson's corre-lation coefficients. All tests were two-sided and consideredsignificant at P < 0.05.
Acknowledgments
This study was supported in part by Theseus ImagingCorporation, Cambridge, MA, USA. We thank Ms. ShulaCalman and Ms. Vered Pilosof for their technical assistance.
R E F E R E N C E S
Belayev, L., Busto, R., Zhao, W., Ginsberg, M.D., 1996.Quantitative evaluation of blood brain barrier permeabilityfollowing middle cerebral artery occlusion in rats. Brain Res.739, 88–96.
Belhocine, T., Steinmetz, N., Hustinx, R., et al., 2002. Increaseduptake of the apoptosis-imaging agent (99m)Tc recombinanthuman Annexin V in human tumors after one course ofchemotherapy as a predictor of tumor response and patientprognosis. Clin. Cancer Res. 8, 2766–2774.
Blankenberg, F.G., Katsikis, P.D., Tait, J.F., et al., 1998. In vivodetection and imaging of phosphatidylserine expressionduring programmed cell death. Proc. Natl. Acad. Sci. U. S. A. 95,6349–6354.
Brott, T., Marler, J.R., Olinger, C.P., et al., 1989. Measurements ofacute cerebral infarction: lesion size by computed tomography.Stroke 20, 871–875.
Chen, J., Jin, K., Chen, M., et al., 1997. Early detection of DNA strandin apoptosis and neuronal cell death after transient focalischemia: implication for the role of DNA damage in apoptosisand neuronal cell death. J. Neurochem. 69, 232–245.
Chen, J., Nagayama, T., Jin, K., et al., 1998. Induction of caspase-3protease may mediate delayed neuronal death in thehippocampus after transient cerebral ischemia. J. Neurosci. 18,4914–4928.
D'Arceuil, H., Rhine, W., de Crespigny, A., et al., 2000. 99mTcannexin V imaging of neonatal hypoxic brain injury. Stroke 31,2692–2700.
Du, C., Hu, R., Csernansky, C.A., Hsu, C.Y., Choi, D.W., 1996. Verydelayed infarction after mild focal cerebral ischemia: a role forapoptosis? J. Cerebr. Blood Flow Metab. 16, 195–201.
Geske, F.J., Lieberman, R., Strange, R., Gerschenson, L.E., 2001.

19B R A I N R E S E A R C H 1 1 0 3 ( 2 0 0 6 ) 1 3 – 1 9
Early stages of p53 induced apoptosis are reversible. Cell DeathDiffer. 8, 182–191.
Funakoshi, T., Hendrickson, L.E., McMullen, B.A., Fujikawa, K.,1987. Primary structure of human placental anticoagulantprotein. Biochemistry 26, 8087–8092.
Haas, R.L., de Jong, D., Valdes Olmos, R.A., et al., 2004. In vivoimaging of radiation-induced apoptosis in follicular lymphomapatients. Int. J. Radiat. Oncol. Biol. Phys. 59, 782–787.
Hammill, A.K., Uhr, J.W., Scheuermann, R.H., 1999. Annexin Vstaining due to loss of membrane asymmetry can be reversibleand precede commitment to apoptotic death. Exp. Cell Res. 251,16–21.
Hara, H., Friedlander, R.M., Gagliardini, V., et al., 1997. Inhibition ofinterleukin 1β converting enzyme family proteases reducesischemic and excitotoxic neuronal damage. Proc. Natl. Acad.Sci. 94, 2007–2012.
Kartachova, M., Haas, R.L., Olmos, R.A., Hoebers, F.J., vanZandwijk, N., Verheij, M., 2004. In vivo imaging of apoptosis by99mTc-Annexin V scintigraphy: visual analysis in relation totreatment response. Radiother. Oncol. 72, 333–339.
Kemerink, G.J., Boersma, H.H., Thimister, P.W., et al., 2001.Biodistribution and dosimetry of 99mTc-BTAP-annexin-V inhumans. Eur. J. Nucl. Med. 28, 1373–1378.
Kenis, H., van Genderen, H., Bennaghmouch, A., et al., 2004. Cellsurface-expressed phosphatidylserine and annexin A5 open anovel portal of cell entry. J. Biol. Chem. 279, 52623–52629.
Kim, Y., Truettner, J., Zhao, W., Busto, R., Ginsberg, M.D., 1998. Theinfluence of delayed postischemic hyperthermia followingtransient focal ischemia: alterations of gene expressionJ. Neurol. Sci. 159, 1–10.
Kuroiwa, T., Shibutani, M., Okeda, R., 1988. Blood–brain barrierdisruption and exacerbation of ischemic brain edema afterrestoration of blood flow in experimental focal cerebralischemia. Acta Neuropathol. 76, 62–70.
Larsen, S.K., Solomon, H.F., Caldwell, G., Abrams, M.J., 1995.[99mTc]tricine: a useful precursor complex for theradiolabeling of hydrazinonicotinate protein conjugates.Bioconjug. Chem. 6, 635–638.
Lorberboym, M., Lampl, Y., Sadeh, M., 2003. Correlation of Tc-99mDTPA SPECT of the blood–brain barrier with neurologicoutcome after acute stroke. J. Nucl. Med. 44, 1898–1904.
Mankovsky, B.N., Patrick, J.T., Metzger, B.E., Saver, J.L., 1996. Thesize of subcortical ischemic infarction in patients with andwithout diabetes mellitus. Clin. Neurol. Neurosurg. 98,137–141.
Mari, C., Karabiyikoglu, M., Goris, M.L., Tait, J.F., Yenari, M.A.,Blankenberg, F.G., 2004. Detection of focal hypoxic–ischemicinjury and neuronal stress in a rodent model of unilateral MCAocclusion/reperfusion using radiolabeled annexin V. Eur. J.Nucl. Med. Mol. Imaging 31, 733–739.
Namura, S., Zhu, J., Fink, K., et al., 1998. Activation and cleavage ofcaspase-3 in apoptosis induced by experimental cerebralischaemia. J. Neurosci. 18, 3659–3668.
Narula, J., Acio, E.R., Narula, N., et al., 2001. Annexin-V imaging for
noninvasive detection of cardiac allograft rejection. Nat. Med.7, 1347–1352.
O'Brien, I.E.W., Reutingsperger, C.P.M., Holdaway, K.M., 1997.Annexin-V and TUNEL use in monitoring the progression ofapoptosis in plants. Cytometry 29, 28–33.
Peters, K.D., Kochanek, K.D., Murphy, S.L., 1998. Deaths: final datafor 1996. Natl. Vital Stat. Rep. 47, 1–100.
Rohatgi, T., Henrich-Noack, P., Sedehizade, F., et al., 2004.Transient focal ischemia in rat brain differentially regulatesmRNA expression of protease-activated receptors 1 to 4.J. Neurosci. Res. 75, 273–279.
Sternbach, G.L., 2000. The Glasgow coma scale. J. Emerg. Med. 19,67–71.
Tait, J.F., Smith, C., Blankenberg, F.G., 2005. Structuralrequirements for in vivo detection of cell death with99mTc-annexin V. J. Nucl. Med. 46, 807–815.
Thimister, P.W., Hofstra, L., Liem, I.H., et al., 2003. In vivo detectionof cell death in the area at risk in acute myocardial infarctionJ. Nucl. Med. 44, 391–396.
Thompson, C.B., 1995. Apoptosis in the pathogenesis andtreatment of disease. Science 267, 1456–1462.
Vanderheyden, J.L., Verbeke, K., Kieffer, D., et al., 2002.Technetium, rhenium and other metals in chemistry andnuclear medicine. Editoriali Padova 6, 335–338.
van Heerde, W.L., de Groot, P.G., Reutelingsperger, C.P.M., 1995.The complexity of the phospholipid binding protein annexin V.Thromb. Haemost. 73, 172–179.
Verbeke, K., Kieffer, D., Vanderheyden, J.L., et al., 2003.Optimization of the preparation of 99mTc-labeledHynic-derivatized Annexin V for human use. Nucl. Med. Biol.30, 771–778.
Vexler, Z.S., Roberts, T.P.L., Bollen, A.W., Derugin, N., Arieff, A.I.,1997. Transient cerebral ischemia. association ofapoptosis induction with hypoperfusion. J. Clin. Invest. 99,1453–1459.
Vriens, P.W., Blankenberg, F.G., Stoot, J.H., et al., 1998. The use oftechnetium Tc 99m annexin V for in vivo imaging of apoptosisduring cardiac allograft rejection. J. Thorac. Cardiovasc. Surg.116, 844–853.
WHO Regional Office for Europe and the European Stroke Council,1996. Report on Pan European Consensus Meeting on StrokeManagement, Helsingborg, Sweden, November 1995. WorldHealth Organization, Copenhagen Denmark.
Wityk, R.J., Pessin, M.S., Kaplan, R.F., Caplan, L.P., 1994. Serialassessment of acute stroke using the NIH stroke scale. Stroke25, 362–365.
Zhang, X., Chen, J., Graham, J., et al., 2002. Intranuclear localizationof apoptosis-inducing factor (AIF) and large scale DNAfragmentation after traumatic brain injury in rats and inneuronal cultures exposed to peroxynitrite. J. Neurochem. 82,181–191.
Zwaal, R.F., Schroit, A.J., 1997. Pathophysiologic implications ofmembrane phospholipid asymmetry in blood cells. Blood 89,1121–1132.