immunization summit pneumo finalr
TRANSCRIPT

Pneumococcal Conjugated Pneumococcal Conjugated Vaccine (PCV) :Vaccine (PCV) :
Is the introduction to the Is the introduction to the National Immunization Program in National Immunization Program in
Sri Lanka justified ?Sri Lanka justified ?
Dr. Pushpa Ranjan Wijesinghe, MDConsultant Epidemiologist
Presentation at the Immunization Summit 2011

Is introduction of PCV a dilemma for Is introduction of PCV a dilemma for
National EPI managers ? National EPI managers ? • Need for achieving MDGs and role of immunization • Opportunities for introduction of appropriate new
vaccines to the NPI • Are we going to use these opportunities ?
• Inequity
• public sector responsibility • If so, will there be a place for pneumococcal vaccines?• Is scientific evidence available for such a decision ?
• If the decision is made, is it self- sustainable in the longer run ?

Consensus statement
The immunization stake holder's meeting -2007 • Pneumococcal vaccines :
• Current disease burden (2007) is inadequate for decision making
• Due to high pneumonia specific morbidity, mortality and high AB resistance of S.pneumoniae, consideration of the pneumococcal vaccine in future given the financial feasibility and GAVI support
• Extension of surveillance activities to more sentinel sites to represent different geographical regions, further strengthening and revisit in 2008
Does the disease burden warrant health
intervention ?
• Consensus statement –The immunization stake holder's meeting -2007
“Current disease burden (2007) is inadequate for decision making “
• Is the situation different in 2010 ?
“ High AB resistance of S.pneumonia “ • Is this real in the Sri Lankan context ?
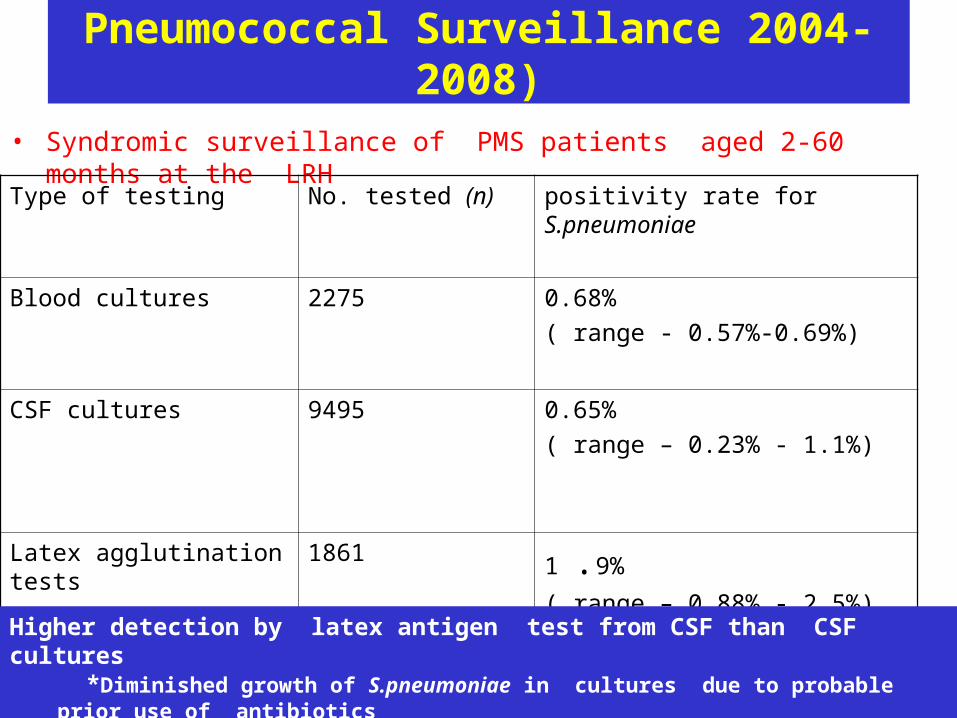
Pneumococcal Surveillance 2004-2008)
• Syndromic surveillance of PMS patients aged 2-60 months at the LRH
Type of testing No. tested (n) positivity rate for S.pneumoniae
Blood cultures 2275 0.68%
( range - 0.57%-0.69%)
CSF cultures 9495 0.65%
( range – 0.23% - 1.1%)
Latex agglutination tests 1861 1 .9%
( range – 0.88% - 2.5%)
Higher detection by latex antigen test from CSF than CSF cultures *Diminished growth of S.pneumoniae in cultures due to probable prior use of antibiotics
Source : SAPNA

Incidence rate /100000 and estimates of PMS for
Colombo district and Sri Lanka
Syndrome Incidence rate *
(per 100000)
Estimate for Colombo district *
Estimate for
Sri Lanka
All cause pneumonia
1342 2227 23551
All cause meningitis
519 866 9030
All cause sepsis
390 651 6786
All cause PMS 2251 3759 39167
•Epidemiological and economic analysis of pneumococcal disease in Sri Lanka conducted by Dr. S.Kularatne for the Epidemiology Unit - 2009
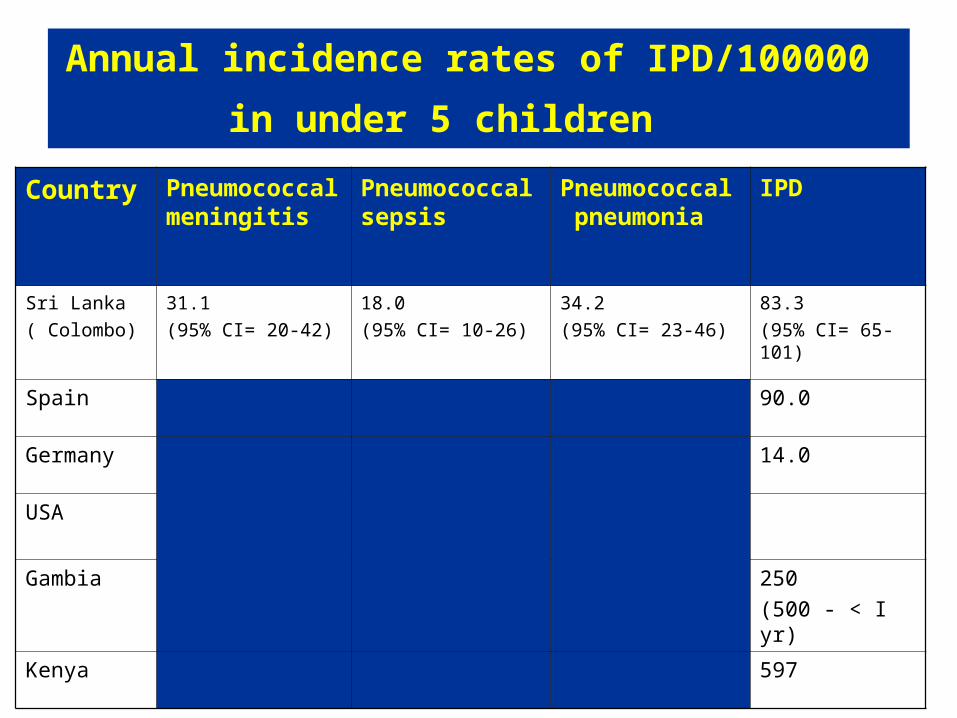
Annual incidence rates of IPD/100000
in under 5 children Country Pneumococcal
meningitisPneumococcal sepsis
Pneumococcal pneumonia
IPD
Sri Lanka
( Colombo)
31.1
(95% CI= 20-42)
18.0
(95% CI= 10-26)
34.2
(95% CI= 23-46)
83.3
(95% CI= 65-101)
Spain 90.0
Germany 14.0
USA
Gambia 250
(500 - < I yr)
Kenya 597
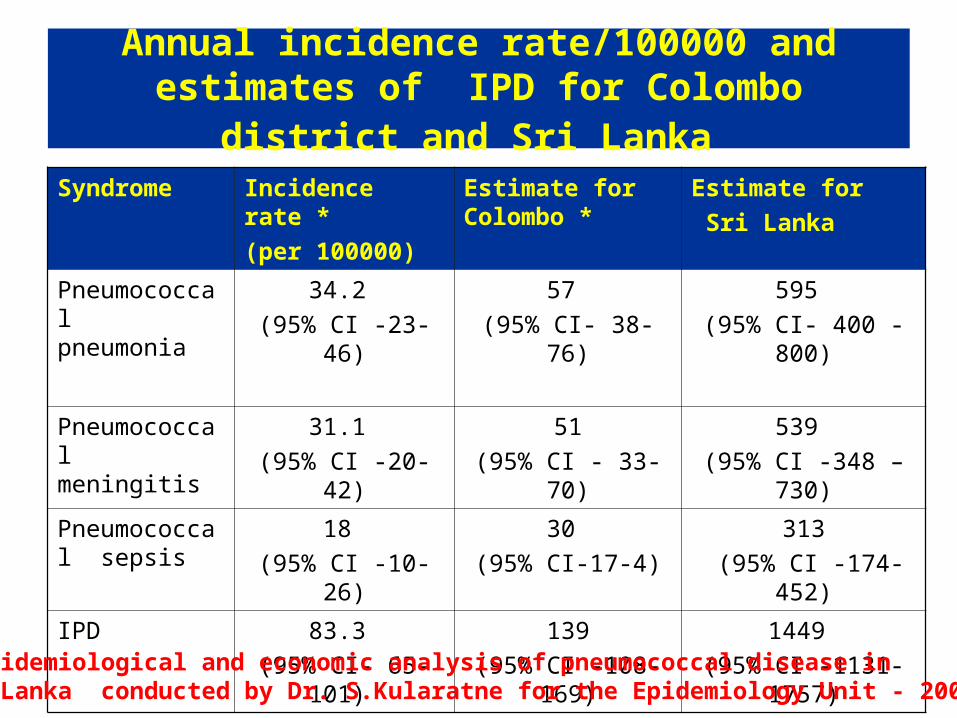
Annual incidence rate/100000 and estimates of IPD for Colombo district and Sri Lanka
Syndrome Incidence rate *
(per 100000)
Estimate for Colombo *
Estimate for
Sri Lanka
Pneumococcal pneumonia
34.2
(95% CI -23-46)
57
(95% CI- 38-76)
595
(95% CI- 400 -800)
Pneumococcal meningitis
31.1
(95% CI -20-42)
51
(95% CI - 33-70)
539
(95% CI -348 – 730)
Pneumococcal sepsis
18
(95% CI -10-26)
30
(95% CI-17-4)
313
(95% CI -174-452)
IPD 83.3
(95% CI- 65-101)
139
(95% CI -108-169)
1449
(95% CI -1131-1757)
* Epidemiological and economic analysis of pneumococcal disease in Sri Lanka conducted by Dr. S.Kularatne for the Epidemiology Unit - 2009

Pneumococcal surveillance ( 2004-2009)
Antibiotic Sensitive Intermediate resistant
Resistant
Penicillin 53 (42%) 41(33%) 31(25%)
Co-trimaxazole 33 (26%) 21(17%) 71(57%)
Chlorampenicol 99(79%) 00 26 (21%)
Erythromycin 42(33%) 01(1%) 82(66%)
Cefotaxime 94(75%) 25(20%) 06(5%)
Antibiotic sensitivity of Pneumococcal isolates ( n=125)
Source : SAPNA
Is there an appropriate vaccine?Is there an appropriate vaccine?
• PCV 7 – contains 7 sero -types– 4, 6b,9v,14,18C, 19F, 23F
– a licensed product
• PCV 9 – Contains additional serotypes – 1 & 5– unlicensed product
• PCV 10 – contains additional serotype - 7
• PCV 13– contains additional serotypes- 3,6A,9A
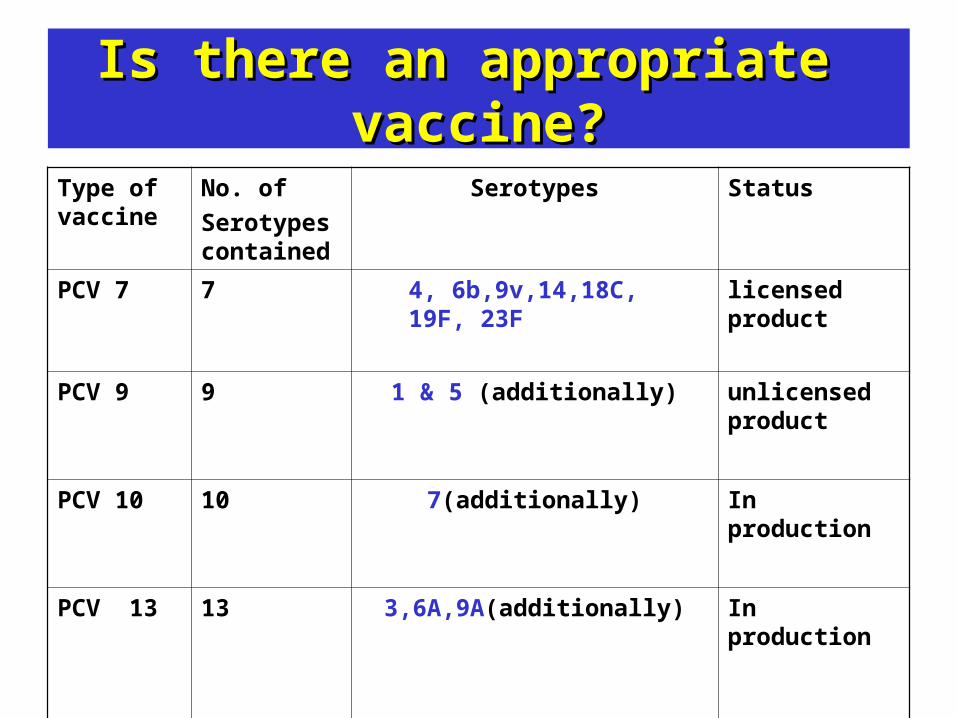
Is there an appropriate vaccine?Is there an appropriate vaccine?
Type of vaccine
No. of
Serotypes contained
Serotypes Status
PCV 7
7 4, 6b,9v,14,18C, 19F, 23F licensed product
PCV 9 9 1 & 5 (additionally) unlicensed product
PCV 10 10 7(additionally) In production
PCV 13
13 3,6A,9A(additionally) In production

Pneumococcal surveillance ( 2004-2009)
Distribution of serotypes in Sri Lanka ( LRH & 5 sites) Coverage of PCV 7 = 62.2%Coverage of PCV 10=63.1%Coverage of PCV 13= 69.7%
1
4
1 1
22
1 1 10
21 1
4
1 1 1 1 1 1
29
0
5
8
1 1
4 4
11
1
5
7
0
5
10
15
20
25
30
35
1 3 4 13
14
15
16
20
23
38
11a
11c
15b
15c
16a
17f
18A
18F
19c
19f
22
23a
23f
33b
35,4
2
47f
6A
6B
9N
9V
NT
Type
Nu
mb
er
Coverage of PCV 7 = 62.2%Coverage of PCV 10=63.1%Coverage of PCV 13= 69.7%

Are the globally available Are the globally available safety and efficacy data safety and efficacy data
conclusive ?conclusive ?
Is there a need for local immunogenicity/efficacy and
safety data ?

End points evaluated
Individual randomized (direct effect)
Cluster randomized ( + herd immunity)
Individually RCT Individual
Efficacy (95% CI) Efficacy (95% CI) Efficacy (95% CI) Efficacy (95% CI)
IPD –vaccine
sero types
94% (80-99%) 83% (21-96%) 71%(46-86%)
IPD-all pneumococal types
89% ( 74-96%) 52 % (-7-79%) 45%(19-62%)
Radiologically confirmed pneumonia
26% ( 7-41%) -21% ( -62-9%) 35%(26-43%)
Well defined clinical pneumonia
6% ( 1-11%)
Severe clinical pneumonia
-
Hospital admissions 13% (6-19%)
Mortality (all cause) 14%(2-24%)
Vaccine type acute Otitis media
54% (41-64%)
All cause acute otitis media
6%(4-9%) 6% ( -4-16%)
Source : WHO
SafetySafety –– key pointskey points
• Generally safe and well tolerated • even among children infected with HIV
• Post marketing surveillance• No significant serious AE among 30 million users in USA
• Most common reported adverse events • Injection site reactions (slight soreness and swelling) • Transient fever above 38.5 C
• Rare adverse events• Febrile seizures • Hypotonic-Hypo responsive Episodes (HHE)
• Very rare adverse events • Urticarea, angioneurotic oedema, erythema multiforme and
hypersensitivity including anaphylaxis

Preventable number of cases by PCV 7
in Sri Lanka
Non vaccinated scenario
Vaccinated – vaccine recipients (90%)
Vaccinated – vaccine non recipients
(10%)
Total cases prevented by vaccine
IPD 1444 120 25 1299
Non Pnc PMS
38280 25417 5206 7657
Efficacy – 83% for IPD
Can the vaccine be incorporated in to the Can the vaccine be incorporated in to the current EPI schedule ?current EPI schedule ?
• Currently 2 recommended schedules of 3 doses
– 6 weeks, 10 weeks and 14 weeks
– 2 months, 4 months and 6 months
• Compatible with pentavalent 3 doses• No need for an additional clinic visit

What are the costs involved ?What are the costs involved ? Approximate cost for vaccines
5 $
per a dose
(376843 X 5 $ X 3) 56 52645 $
per year
Treatment cost in a non vaccinated scenario
Per Pnc PMS
&
other PMS
cases
(25714 RS X1444)
+
(12495 Rs X 38280)
45 56221 $
per year
Treatment cost in a vaccinated scenario
Per Pnc PMS
&
other PMS
cases
(25714 Rs X 145)
+
(12495 Rs X 30623)
34 49668 $
per year
Treatment cost saved from vaccination
11 06553 $
per year
Additional space due to increasing Cold chain requirements
Volume per dose
59.7cm3/dose *
(1130529 X 59.7) 67.5 m3

Is the suggested vaccine cost effective ?Is the suggested vaccine cost effective ?
GAVI’s economic analysis
GAVI’s estimated
Cost effectiveness ratio for
Sri Lanka
Estimated
Cost effectiveness ratio based on
Sri Lankan study
Cost effective in 71/72
GAVI eligible countries
( including Sri Lanka )
4211 $ per
DALY averted
7397 Rs per
DALY averted
Benchmark – WHO CHOICE

Where are we compared to the previous Where are we compared to the previous
summitsummit ??• Availability of an estimate of the disease burden for the
Colombo district as a model for decision making
• Availability of an estimate of treatment cost • More comprehensive collection of sero types from LRH and 5 other hospitals
• Wide representativeness • Antibiotic resistance data • Circulating serotypes ( n=125)
Where are we compared to the previous Where are we compared to the previous
summitsummit ??• Availability of a vaccine ( 7,10,13 valent) with a high coverage for
available serotypes
• Comprehensive data on safety and immunogenicity of the intended vaccine
• Availability of results of an economic analysis as a guiding tool for decision making
• Established infra structure ,expertise on and experience in post introduction surveillance of new vaccines
• Availability and delivery of the intended vaccine in the private sector • WHO support for continued surveillance ( disease and laboratory)

Points for the discussionPoints for the discussion
• Is introduction of pneumococcal vaccine justifiable ? – Disease burden, economic burden – Competing priorities (MMR, typhoid) – Financial sustainability
• SL- no longer being GAVI eligible • Self financing potential
• Can a tentative timeline be determined ?– consideration of the pneumococcal vaccine in future given the financial
feasibility and GAVI support – immunization stake holder's meeting - 2007
• What are the other constraints ?• How can we overcome them? • Any concerns of participants ?

AcknowledgementAcknowledgement
• Dr. Nihal Abeysinghe for vision and guidance • Dr. Paba Palihawadana and Dr T.S.R.Pieris for continued vision & support • Dr.Ranjit Batuwanthdawe for the pioneering work • Dr. Malka Dissanayake & Dr.Kumudu Karunaratne for enabling
information generation• Dr.Sanjeewa Kuaratne for initiating epidemiological and economic analysis• All microbiologists at the SPnSN for their contributions • MLTs at the LRH microbiology lab for the excellent work • All pediatricians at the LRH for their precious contributions • Dr. Mark Stein Hoff, Prof. Kurian Thomas, Professor Lalitha Kesewan • Microbiology team @ the Christian Medical College , Vellore, Tamil Nadu • GAVI’s Pneumo ADIP, John Hopkins University, USA• International Clinical Epidemiological Network (INCLEN)• All research assistants of the SAPNA ( Sri Lanka) for the hard work• Iresha, Roshan, Priyangika for coordinating all the work