il paziente nascosto: la psicosomatica in medicina · il paziente "nascosto": la...
TRANSCRIPT

Il paziente "nascosto":
la psicosomatica in medicina
Piero Porcelli
Dip. Scienze Psicologiche, della Salute e
del Territorio
Università d’Annunzio di Chieti

DSM-IV
Somatization Disorder
Pain Disorder
Undiff.Somatoform Disorder
Somatic Symptom Disorder
DSM-5
Somatoform Disorder NOS Unspecified SSD
Conversion Disorder Conversion Disorder
Body Dysmorphic DisorderBody Dysmorphic Disorder
(OC and Related Dis.)
Illness Anxiety Disorder
Factitious Disorder(separated section)
Factitious Disorder
Imposed on Self/Another
Hypochondriasis
PFAMC(Other Conditions that May Be a
Focus of Clinical Attention)
Psychological Factors Affecting
Other Medical Conditions
Working Group for ICD-11
•Bodily Distress Syndrome
(BSS) for MUS
•Health Anxiety (HA) replacing
Hypochondriasis
•Hypochonadriasis moved to
OC and Related Disorders
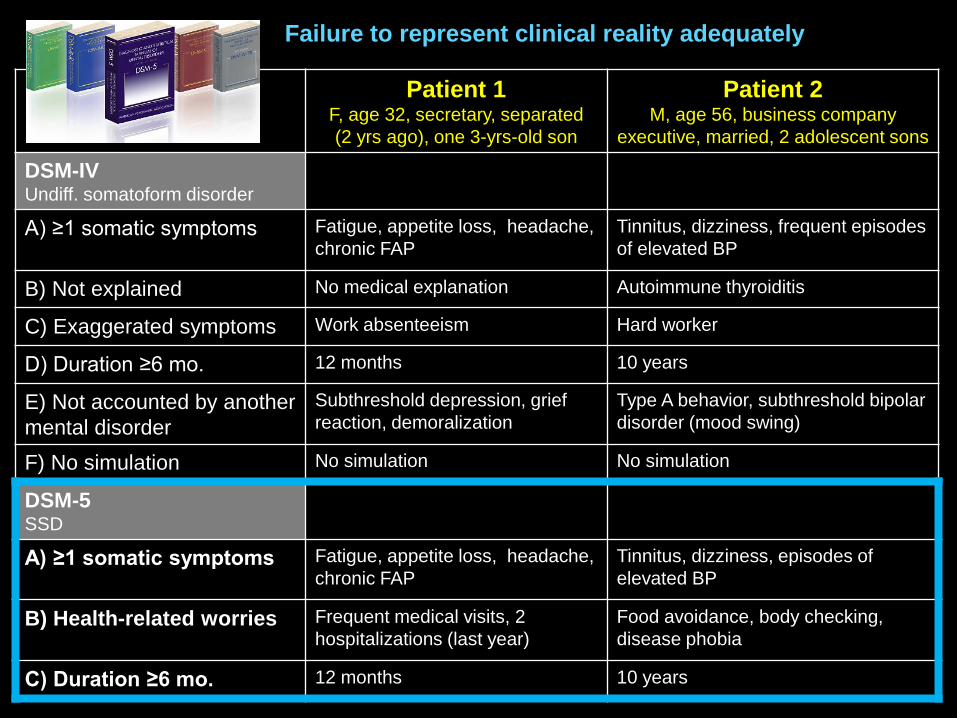
Patient 1F, age 32, secretary, separated
(2 yrs ago), one 3-yrs-old son
Patient 2M, age 56, business company
executive, married, 2 adolescent sons
DSM-IVUndiff. somatoform disorder
A) ≥1 somatic symptoms Fatigue, appetite loss, headache,
chronic FAP
Tinnitus, dizziness, frequent episodes
of elevated BP
B) Not explained No medical explanation Autoimmune thyroiditis
C) Exaggerated symptoms Work absenteeism Hard worker
D) Duration ≥6 mo. 12 months 10 years
E) Not accounted by another
mental disorder
Subthreshold depression, grief
reaction, demoralization
Type A behavior, subthreshold bipolar
disorder (mood swing)
F) No simulation No simulation No simulation
DSM-5SSD
A) ≥1 somatic symptoms Fatigue, appetite loss, headache,
chronic FAP
Tinnitus, dizziness, episodes of
elevated BP
B) Health-related worries Frequent medical visits, 2
hospitalizations (last year)
Food avoidance, body checking,
disease phobia
C) Duration ≥6 mo. 12 months 10 years
Failure to represent clinical reality adequately

Rather than
grounding on
symptoms as in DSM
(high reliability, low
validity), RDoC re-
oriented to explore
ways of incorporating
such methods as
genetics, neuro-
imaging, and
cognitive science into
future diagnostic
schemes based upon
behavioral
dimensions and
neural systems.

Caspi et al, Clin Psychol Sci 2014
PSYCHOPATOLOGY COMORBIDITYThe longitudinal Dunedin Health and Development Study
(N = 1037; assessments at age 18-21-26-32-38)
The higher a person scores on p, the worse that person fares on indicators tapping severity, duration of
disorder, extent of sequential comorbidity, adult life impairment, childhood developmental history, family
history of liability to psychiatric illness, and brain function from early life to midlife
3 higher-order
factors with
liabilities for
Antisocial and
Substance-use
Disorders
(Externalizing)
Depression and
Anxiety Disorders
(Internalizing)
Psychotic
Spectrum
Disorders
(Thought
Disorder)
Can = cannabis
CD = Conduct Disorder

Psychiatric research may benefit from approaching
psychopathology as a system rather than as a
category, identifying dynamics of system change
(eg, abrupt vs gradual psychosis onset), and
determining the factors to which these systems are
most sensitive (eg, interpersonal dynamics and
neurochemical change) and the individual variability
in system architecture and change.
A. Change tends to occur gradually in response to
changes or stress (red arrows)
B. System may initially resist change and then
reach a tipping point that involves a sudden and
dramatic shift to an alternative state, maybe
triggered by a massive stress
C. Transitions may be preceded by an increase in
random variance and volatility or, alternatively, a
critical slowing down of activity
DYNAMIC MODELS OF
PSYCHOPATHOLOGY
Nelson et al, JAMA Psychiatry 2017

NETWORK APPROACH TO DIAGNOSIS
Borsboom D, World Psychiatry 2017
Progression from mental health (= stable state of a weakly connected network)
to mental disorder (= alternative stable state of a strongly connected network)
After an asymptomatic phase, in which the network is dormant (Phase 1), an external event (E1) activates some of the symptoms (Phase 2), which in turn activate connected symptoms (Phase 3).
If the network is strongly connected, removal of the external event does not lead to recovery: the network is self-sustaining and is stuck in itsactive state (Phase 4).

CORPO
MENTE
CORPO
MENTE

AFFECT AWARENESS OPERATORY THINKING
Difficulty identifying feelings
Unawareness of feelings. Experience of chronic
dysphoria or show emotional outbursts (rage,
weeping) but inability to link feelings with memory
and fantasies. Inability to distinguish emotions from
feelings
Difficulty describing feelings to
others
Inability to express and communicate emotional
and mental states to others. Difficulty in
understanding emotions in other persons (empathy)
and their perspective (ToM)
Constricted imaginative processes
Marked paucity of fantasies, daydreaming, dream
recalls, wit, playing
External-oriented thinking style
Selective focus on everything is outward, factual,
concrete. Oversimplification and avoidance of
ambiguities or emotional nuances of inner life.
Report of events and actions with no affective
involvement
ALEXITHYMIA

EMOTIONS
• Biological component of affect
• Neurophysiologic and motor-
expressive domain of response
• Genetic programs (hard wired: fear, anger,
sadness, happiness, disgust, surprise)
• Mediated by subcortical and
limbic structures
• Largely based on non-verbal clues
• “play out in the theater of the body”
(A.Damasio, 2003)
• Predominant in right brain hemisphere
FEELINGS
• Psychological component of affect
• Subjective, cognitive-experiential
domain of response
• Individual schemas and developmental
factors
• Mediated by cortical structures
• Largely based on the symbolic function
• “play out in the theater of the mind”
(A.Damasio, 2003)
• Predominant in left brain hemisphere
How do emotions get represented symbolically so that they can be experienced
consciously as feelings that can be named, regulated, and expressed through fantasies?
IMPLICIT
Things we do without monitoring them on a moment-
by-moment basis (eg, bike riding)
EXPLICIT
Situation in which we can put our experiences into
words because we are aware of their occurrence

0
20
40
60
80
100
Classic psychosomatic disorders and
psychoneurotic diordersDisorders of affect regulation
OCD Obsessive-Compulsive Disorder
CAD Coronary Artery Disease
BED Binge Eating Disorder
Sex Multiple Sexual Dysfunction
RA Rheumatoid Arthritis
UC Ulcerative Colitis
SAD Social Anxiety Disorder
NFA Near-Fatal Asthma
TTM Trichotillomania
CFS Chronic Fatigue Syndrome
MDD Major Depression Disorder
CIN Cervical Intraepithelial Neoplasia
SA Suicide Attempters
SLE Systemic Lupus Erythematosus
BN Bulimia Nervosa
TMD Temporomandibolar
HCFU Health Care Frequent Users
CSPG Chronic Severe Pathol Gambling
Dissoc Dissociative Disorder
FGID Functional GI Disorders
AN Anorexia Nervosa
PREVALENCE OF ALEXITHYMIA

ALEXITHYMIA
• Deficit in cognitive processing of emotions
• Trauma and severe physical illness (secondary alexithymia)
• Somatization syndromes (MUS, somatosensory amplification)
• Disorders of affect regulation (hypochondriasis, panic, depression, eating, addiction)
• Insecure attachment patterns
• Decoupling stress hypothesis (higher resting state and physiological hyper-arousal as
salivary cortisol, but low stress perception)
• Sparse findings on immune imbalance of inflammatory markers
• High mortality risk
(Kuopio Ischemic Heart Disease study, 20-year follow-up: RR=1.2, same as HDL-C e
History of CV diseases)
• Deficit of brain inter-emispheric transfer
• Lower dACC and PFC activity/volume and higher AI/SS I-II activity
Defense
I know but can’t tell
Deficit
I don’t know and can’t tell
Overall consensus:
It is not a psychopathology or a category but a
personality dimension

Multidetermined disorders, arising from a composite of factors affecting the gut mucosa and
microflora, the nervous system and its extrinsic neural connections in the gut, and signaling
within the brain and the spinal cord.
These disorders are best understood from a biopsychosocial perspective; as such it would
appear unlikely that any single biomarker – such as mucosal histology, cardiovascular
reactivity, gut permeability, and blood, stool, or genetic markers – can explain the symptoms
and will emerge as a diagnostic tool for these disordersKellow , Am J Gastroenterol 2010
Functional GI Disorders

Psychiatric pts(n = 52)
FGID pts(n = 58)
Anxiety26%
Somatoform26%
Mood24%
Adjustment24%
0%
20%
40%
60%
80%
100%
Comor -
Comor +

Psych w/ GI
FGID w/ psych
0 20 40 60 80
TAS-20
0
5
10
15
20
GSRS SOM OC INT DEP ANX HOS PHOB PAR PSY
SCL-90-R
p < .001

Psychiatric
patients
FGID
patients
Same GI
symptoms
alexithymia
GI medical setting
psychopathology
psychiatric setting


Cognitive, affective, and behavioral response stemming
1) from fear of GI sensations or symptoms, and …
2) the context in which these visceral sensations and symptoms occur.
It is focused specifically on the IBS core features (abdominal pain and bowel
habit) in specific contexts as situations involving food and eating, like
restaurants and parties or locations in which bathroom facilities are not known
or difficult to reach.
Briefly, GSA relates to hypervigilance to, and fear, worry, and avoidance of, GI
sensations and contexts.
Earlier findings showed that GSA was associated to more severe IBS
symptoms, psychological distress, poor quality of life, and mediated the
relationship between general psychological distress and IBS severity.
Gastrointestinal-Specific Anxiety
(GSA)

ALEXITHYMIA TAS-20
GSA Visceral Sensitivity Index (VSI)
Psy distress HADS
Functioning SF-12
IBS symptomsGI Symptom Rating Scale-IBS
(GSRS-IBS)
IBS severityIBS Severity Scoring System
(IBS-SSS)
Mild IBS = score 75–175
Moderate = 175–300
Severe = >300177 IBS patients assessed at
- baseline
- after 6 months of as-needed tx

Block 1: age, GSRS-IBS score, HADS, PCS, MCS
Block 2: VSI
Block 3: TAS-20
The order of forced variables in the 2nd and 3rd blocks was revered in two different models.
The relative contribution of VSI and TAS-20 was very similar, either when
− VSI was forced before TAS-20 (R2 = 0.51, ΔR2 = 0.14, β = 0.307)
− TAS-20 was forced before VSI (R2 = 0.56, ΔR2 = 0.19, β = 0.532).
PREDICTING IBS SEVERITY
Large effect size for
being alexithymic,
higher if also with
higher GSA
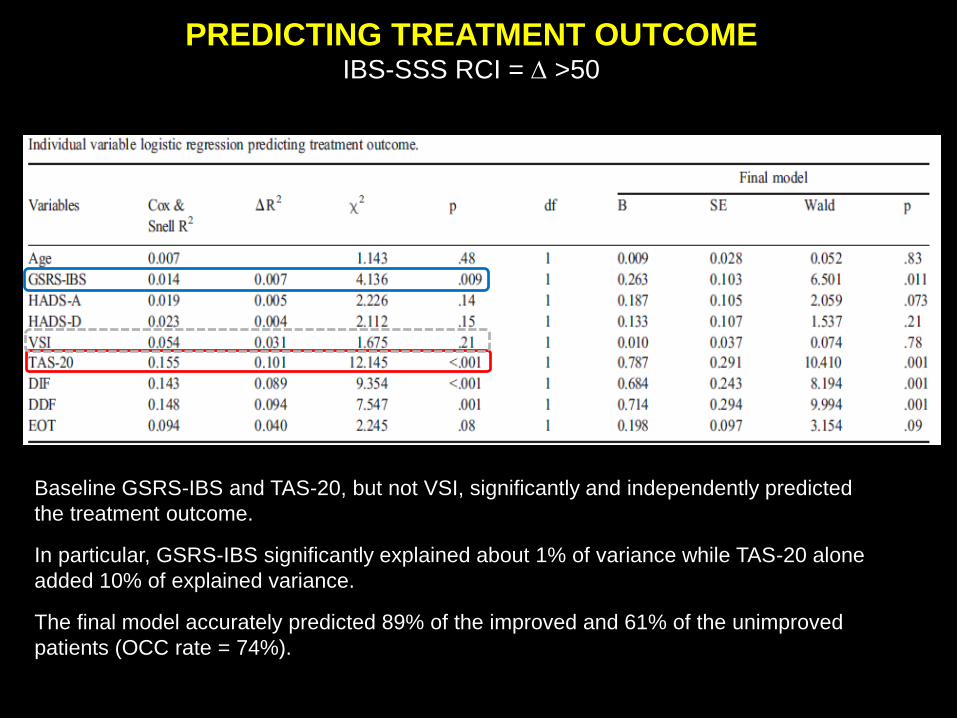
PREDICTING TREATMENT OUTCOMEIBS-SSS RCI = D >50
Baseline GSRS-IBS and TAS-20, but not VSI, significantly and independently predicted
the treatment outcome.
In particular, GSRS-IBS significantly explained about 1% of variance while TAS-20 alone
added 10% of explained variance.
The final model accurately predicted 89% of the improved and 61% of the unimproved
patients (OCC rate = 74%).

0
2
4
6
Baseline 3 months Post-therapy Follow-up
Anxiety
Depression
Somatic Symptoms
ALEXITHYMIA AND SOMATIC SYMPTOMS IN HCV+ PATIENTS
DURING IFN THERAPY
N = 111 pts (men 53%, mean age 51, lifetime psychopathology 34%)
0
10
20
30
Baseline 3 months Post-therapy
Follow-up
%
Biological AE
BASELINE• SCID
• TAS-20
• PHQ-15
AT EACH VISIT
• HADS
• Somatic symptoms
• Biological AE
1. Fever
2. Headache
3. Muscle and joint pain
4. Diarrhea
5. Gut discomfort
6. Fatigue
7. Poor appetite
8. Weight loss (>10%)
9. Hair loss
10. Loss of libido
11. Itching
12. Skin rush
13. Dyspnea
14. Cough
15. Eye drying
16. Sleep problems
5-point scale
1 (none) to
5 (most severe)
Main outcome
no. of symptoms
graded as 4-5 (severe
and most severe)
Most common biological Adverse Events:
• Anemia (hemoglobin < 6.5 g/dL)
• Neutropenia (absolute neutrophils count
< 500/mm3)
• Thrombocytopenia (platelets <
25.000/mm3)
Grade 3 (severe) and 4 (disabling) of the
National Cancer Institute criteria
(Common Terminology Criteria for
Adverse Events v3.0, 2006)

MULTIPLE REGRESSION:
partial r
• Baseline: R2 = .80, F = 68.552, p < .001
• 3 months: R2 = .42, F = 77.566, p < .001
• Post-therapy: R2 = .38, F = 70.662, p < .001
• Follow-up: R2 = .77, F = 56.772, p < .001
SOMATIC SYMPTOMS
Gender
Past psychopathology
Alexithymia
Somatization
Anxiety
Depression
SVR
Baseline 3 months End therapy Follow-up
Alexithymiar = .54
Somatizationr = .66
Alexithymiar = .35
Somatizationr = .64
Depressionr = .54
Depressionr = .42
DV = no. of somatic symptoms at each assessment time point
Pre
dic
tors
Porcelli et al, Psychother Psychosom 2014; 83: 310-311

• Paura soverchiante e irrazionale di incontinenza fecale (abbastanza severa
da “mimare” il panico)
• Ruminazioni ideative focalizzate specificamente sull’alvo (dall’umiliazione in
pubblico all’indisponibilità del bagno fuori casa)
• Rituali compulsivi finalizzati a mantenere il controllo corporeo, soprattutto
trascorrere un’enorme quantità di tempo in bagno e limitare l’alimentazione
• Profilo dei sintomi simile al DOC: pensieri ossessivi che innalzano il livello
dell’ansia e rituali compulsivi finalizzati a mitigare l’ansia
• Sintomi sparsi sovrapponibili a disturbo di panico, fobia sociale, fobia
specifica, agorafobia senza panico
Hatch ML, Behav Res Ther 1997

trigger
uscire di casa
(autonomia)
reazione ansiosa
blocco affettivo arousal SNA
pensiero
calmo quando mi
scarico
sintomo
rituale compulsivo
Alexithymia

CONCLUSIONI
• Il paziente "nascosto" o le dimensioni "nascoste" dietro la nosografia
categoriale: evoluzione temporale della sintomatologia, interazione fra
caratteristiche del paziente e circostanze ambientali, fattori latenti unificatori
della sintomatologia, funzioni di personalità (es. alexithymia).
• In gastroenterologia (FGID, IBD, HCV), l'alexithymia può giocare un ruolo
importante nella gestione clinica del paziente nell'influenzare e predire:
• il setting a cui il paziente si rivolge o viene inviato;
• la percezione di gravità e l'esito dell'intervento terapeutico nei disturbi
funzionali del tratto digestivo;
• la presentazione di sintomi fisici in modo inconsueto o anche mascherare
una sindrome psicopatologica (es. ossessivo-compulsiva) come fase di
riacutizzazione di una malattia cronica (es. IBD)
