icl: chondral injury of the knee: current controversies in
TRANSCRIPT
ICL: Chondral Injury of the Knee: Current Controversies in 2021
Aaron Krych, MDJack Farr, MD
Andreas Gomoll, MD
Paul Caldwell, MD
Rachel Frank, MD

©2017 MFMER | slide-2
Get it Right the First Time!Aaron J. Krych, MD
Mayo Clinic Orthopedic Surgery and Sports Medicine
©2017 MFMER | slide-3
Standard cartilage imaging: every patient!
• Good set of standard plain radiographs
• Standing AP, PA flexion
• Lateral
• Merchant
• Hip to ankle long-leg standing
• MRI (3T if possible)
©2017 MFMER | slide-4
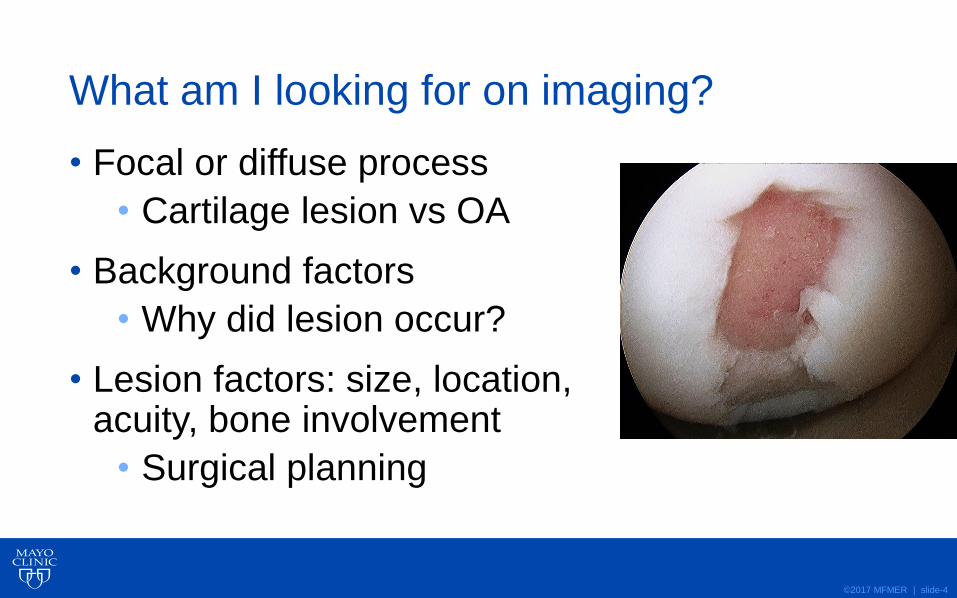
What am I looking for on imaging?
• Focal or diffuse process
• Cartilage lesion vs OA
• Background factors
• Why did lesion occur?
• Lesion factors: size, location, acuity, bone involvement
• Surgical planning
©2017 MFMER | slide-5
What does imaging tell me?
• Focal or diffuse process
• Cartilage lesion vs OA
• Background factors
• Why did lesion occur?
• Lesion factors: size, location, acuity, bone involvement
• Surgical planning
©2017 MFMER | slide-6
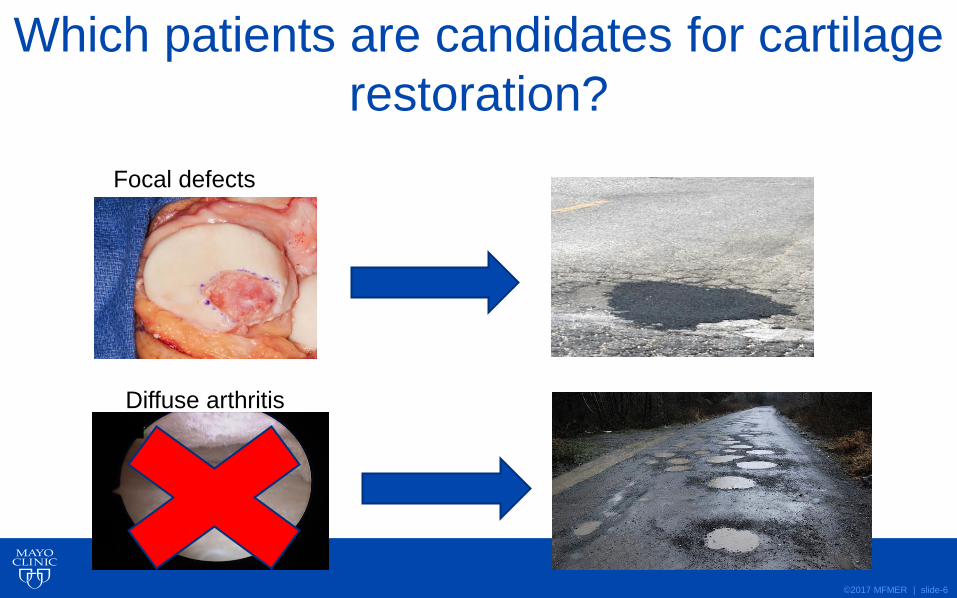
Which patients are candidates for cartilage
restoration?
Focal defects
Diffuse arthritis

©2017 MFMER | slide-7
44M steamfitter, adventure racing, heli-skiing

©2017 MFMER | slide-8
44M steamfitter, adventure racing, heli-skiing
©2017 MFMER | slide-9
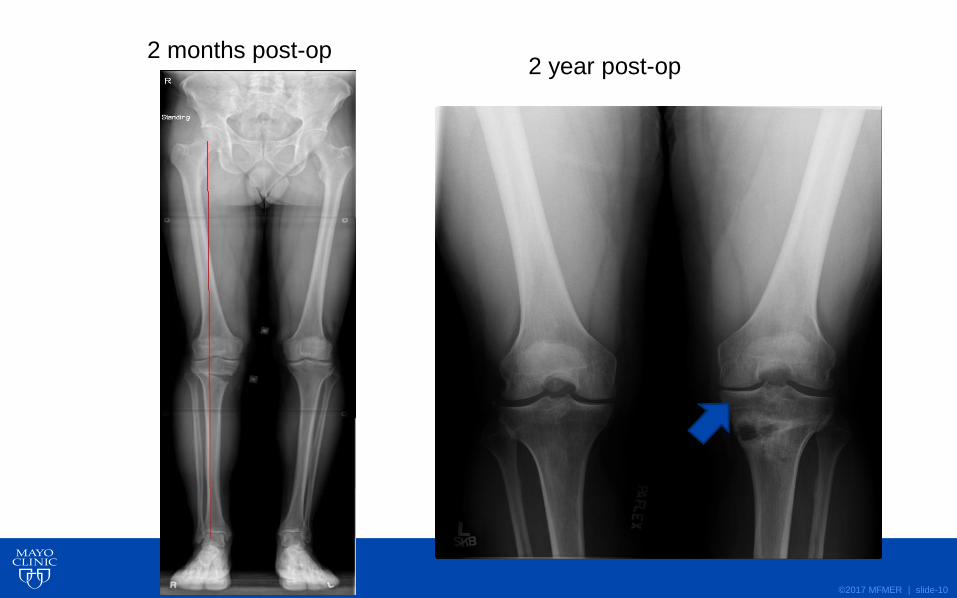
©2017 MFMER | slide-10
2 months post-op2 year post-op
©2017 MFMER | slide-11
What does imaging tell me?
• Focal or diffuse process
• Cartilage lesion vs OA
• Background factors
• Why did lesion occur?
• Lesion factors: size, location, acuity, bone involvement
• Surgical planning
©2017 MFMER | slide-12
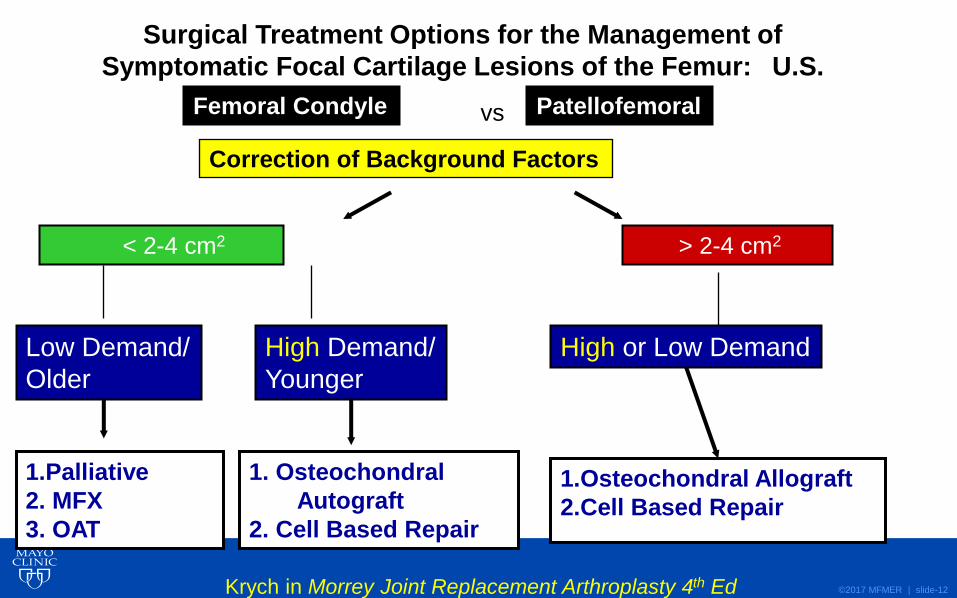
Surgical Treatment Options for the Management of
Symptomatic Focal Cartilage Lesions of the Femur: U.S.
Femoral Condyle
< 2-4 cm2 > 2-4 cm2
Low Demand/
Older
High Demand/
Younger
High or Low Demand
1.Palliative
2. MFX
3. OAT
1. Osteochondral
Autograft
2. Cell Based Repair
1.Osteochondral Allograft
2.Cell Based Repair
Krych in Morrey Joint Replacement Arthroplasty 4th Ed
Correction of Background Factors
Patellofemoralvs

©2017 MFMER | slide-13
Learning from Failure in Cartilage Repair Surgery:
An Analysis of Failure Mode of the Primary Procedure in Consecutive Cases at a Tertiary Referral Center
• Purpose:
• To determine common failure modes in primary cartilage restoration
• Goal: Improve surgical decision-making and patient outcomes
• Materials & Methods:
• Tertiary care center experience, single surgeon
• All revisions for failed cartilage surgery 2011 – 2017
Krych OJSM 2018
©2017 MFMER | slide-14
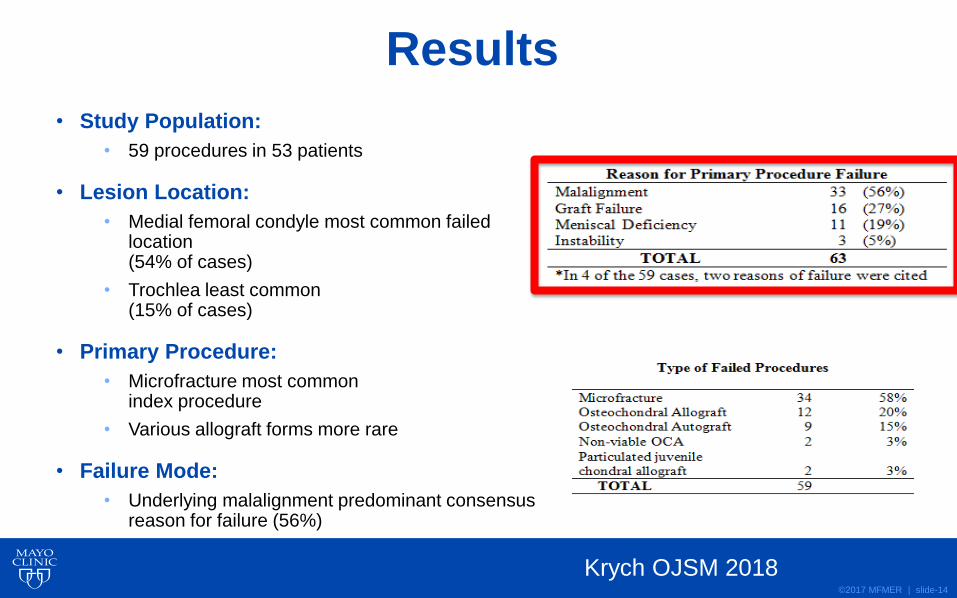
• Study Population:
• 59 procedures in 53 patients
• Lesion Location:
• Medial femoral condyle most common failed location(54% of cases)
• Trochlea least common(15% of cases)
• Primary Procedure:
• Microfracture most commonindex procedure
• Various allograft forms more rare
• Failure Mode:
• Underlying malalignment predominant consensus reason for failure (56%)
Results
Krych OJSM 2018
©2017 MFMER | slide-15
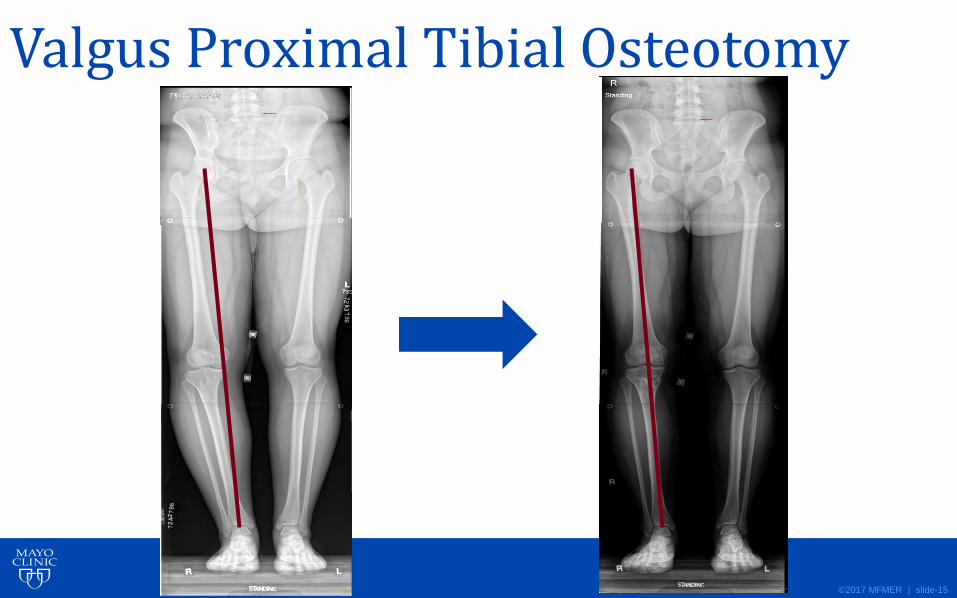
Valgus Proximal Tibial Osteotomy
©2017 MFMER | slide-16
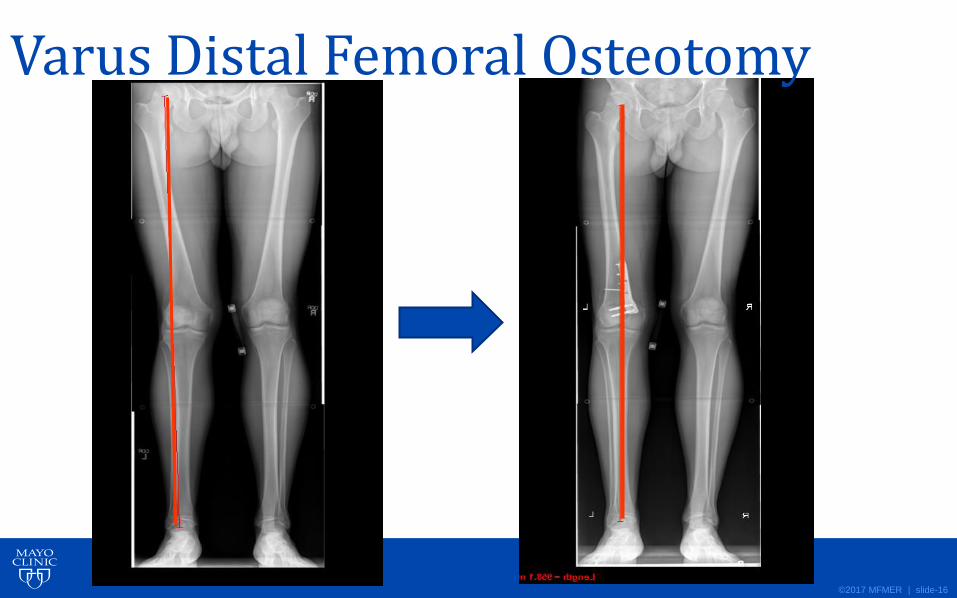
Varus Distal Femoral Osteotomy
©2017 MFMER | slide-17
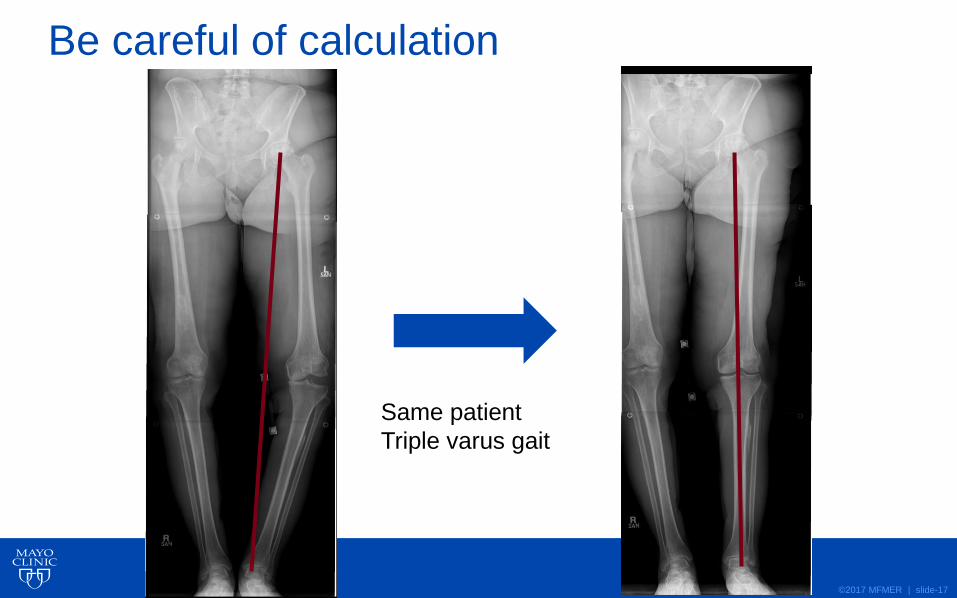
Be careful of calculation
Same patient
Triple varus gait
©2017 MFMER | slide-18
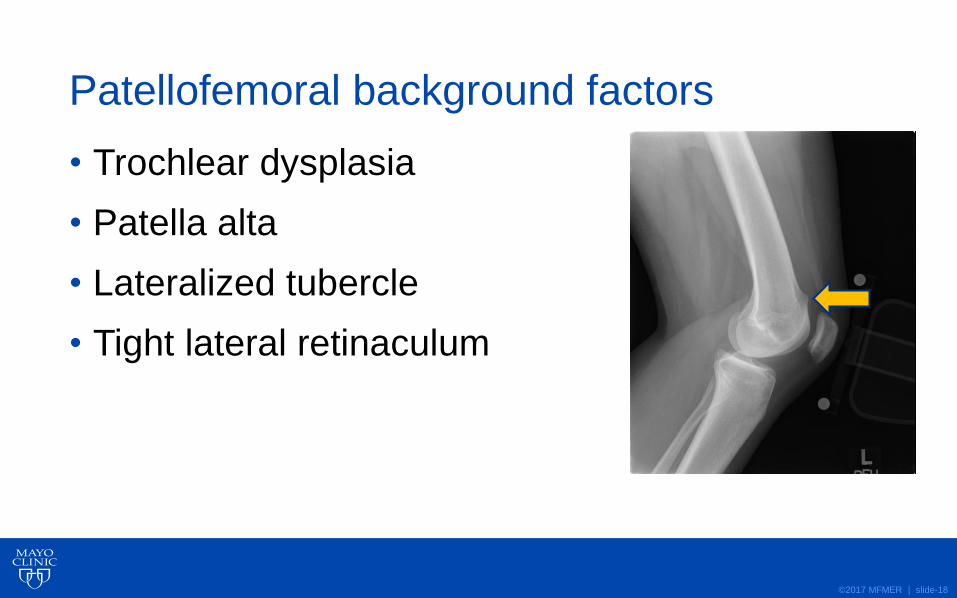
Patellofemoral background factors
• Trochlear dysplasia
• Patella alta
• Lateralized tubercle
• Tight lateral retinaculum
©2017 MFMER | slide-19
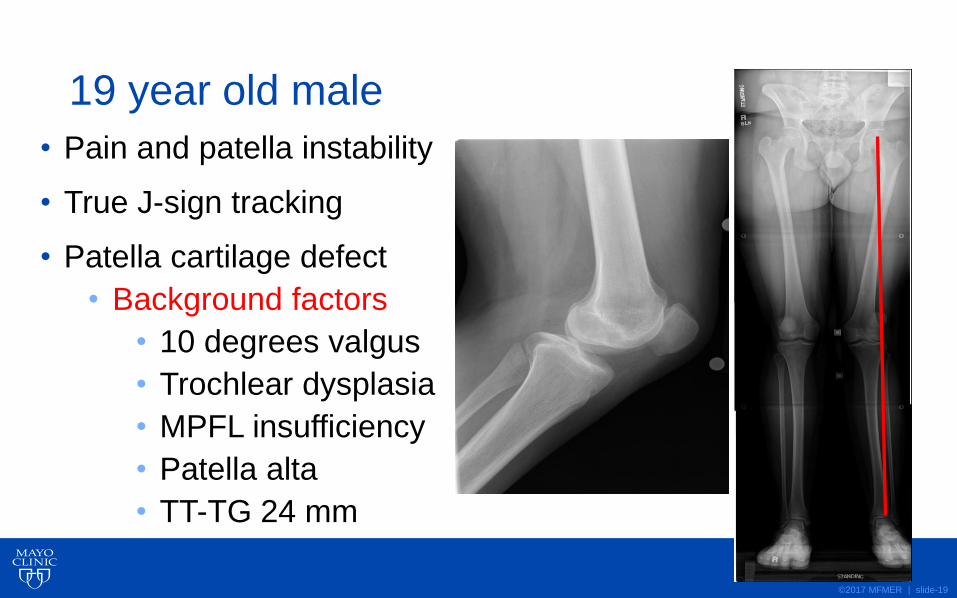
19 year old male
• Pain and patella instability
• True J-sign tracking
• Patella cartilage defect
• Background factors
• 10 degrees valgus
• Trochlear dysplasia
• MPFL insufficiency
• Patella alta
• TT-TG 24 mm
©2017 MFMER | slide-20
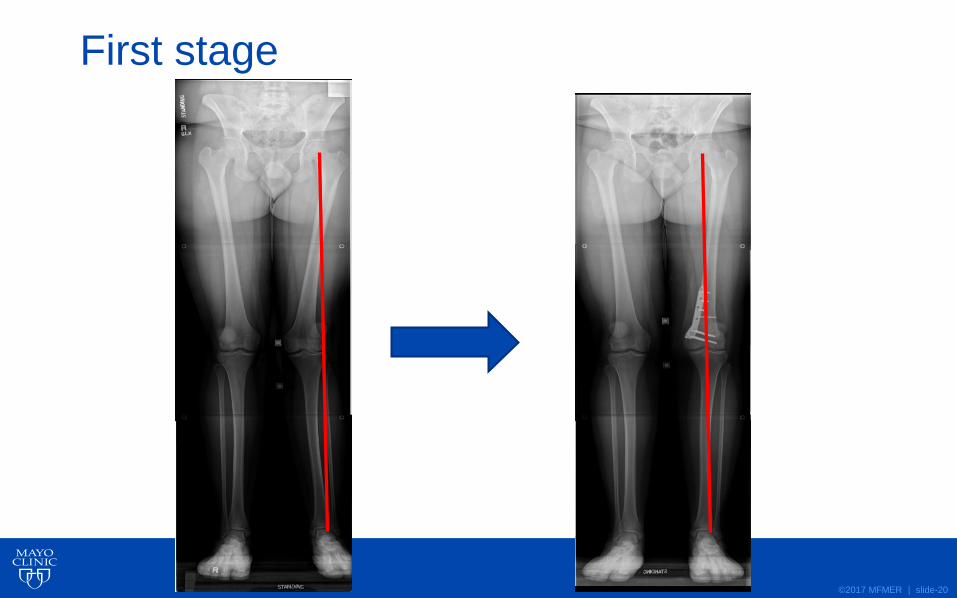
First stage

©2017 MFMER | slide-21
Intra-op J-sign
©2017 MFMER | slide-22
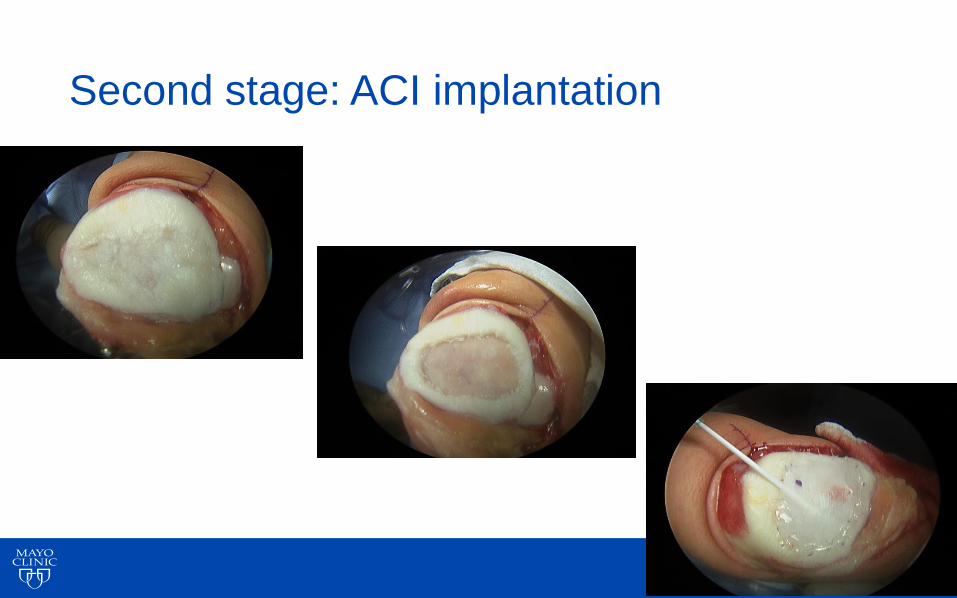
Second stage: ACI implantation
©2017 MFMER | slide-23
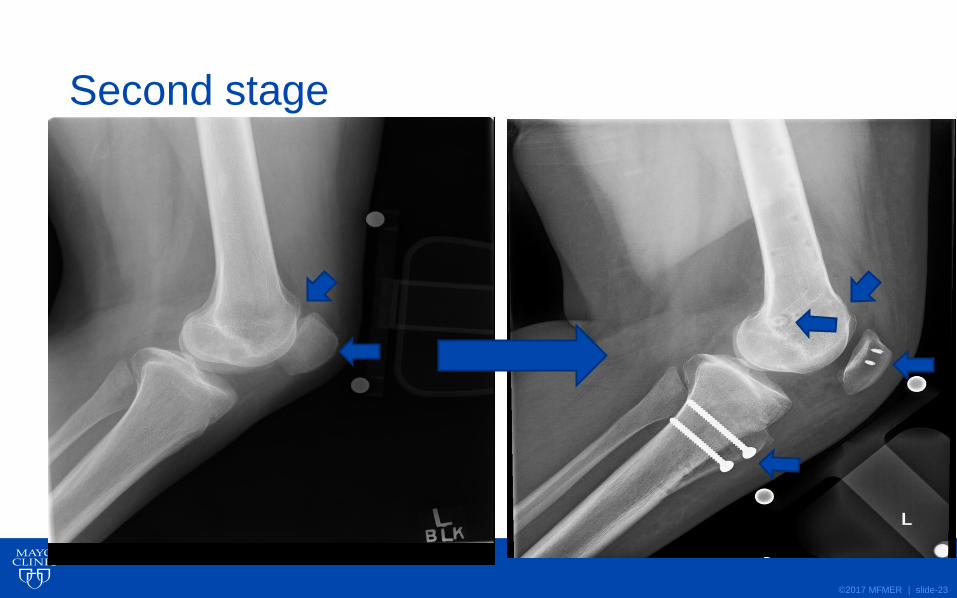
Second stage

©2017 MFMER | slide-24
Correction of J-sign 3 months post-op
©2017 MFMER | slide-25
What does imaging tell me?
• Focal or diffuse process
• Cartilage lesion vs OA
• Background factors
• Why did lesion occur?
• Lesion factors: size, location, acuity, bone involvement
• Surgical planning

©2017 MFMER | slide-26
32M acute LFC lesion
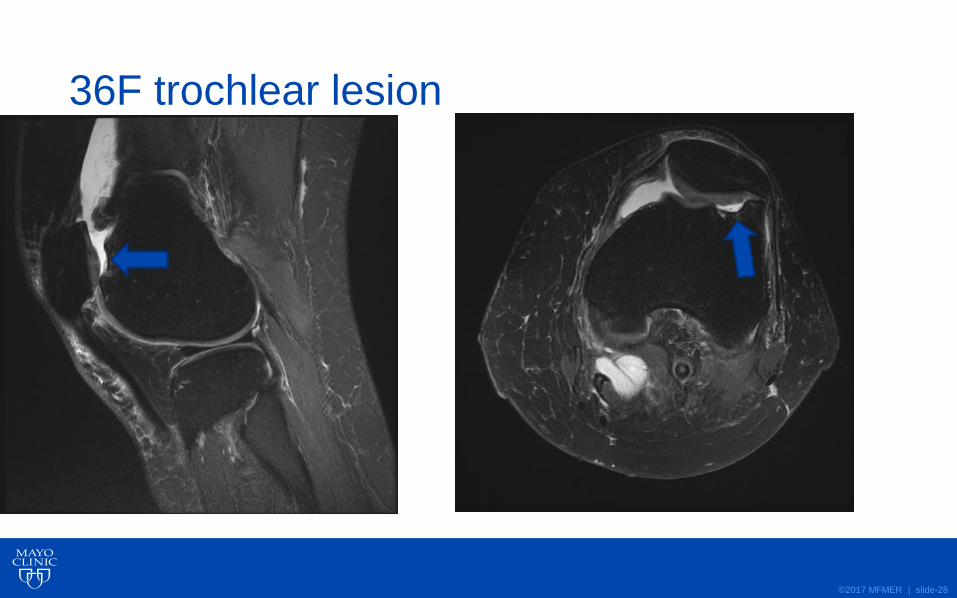
Use axial MRI
©2017 MFMER | slide-27
MRI: Chondral or osteochondral
OCA
OAT
©2017 MFMER | slide-28
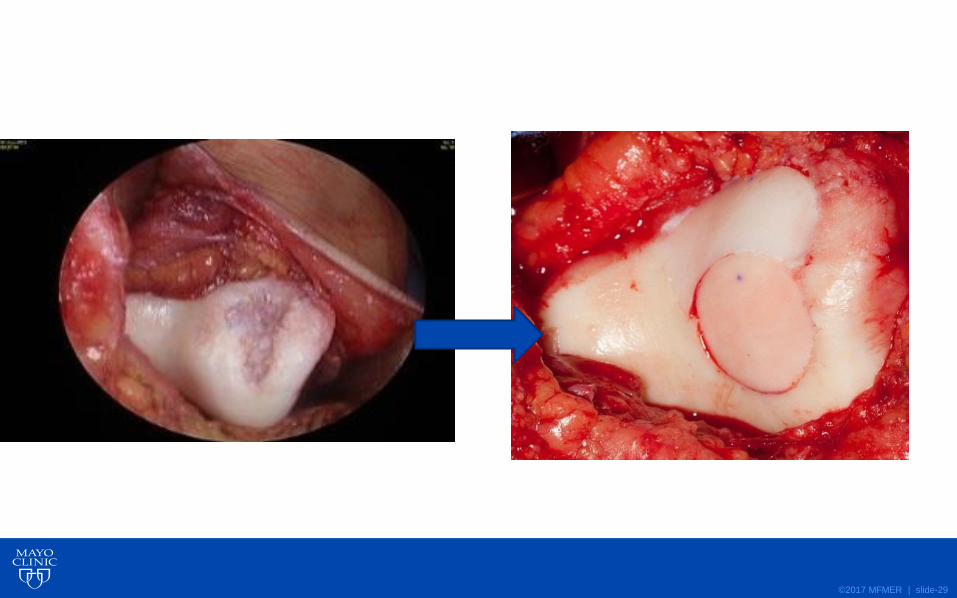
36F trochlear lesion
©2017 MFMER | slide-29

©2017 MFMER | slide-30
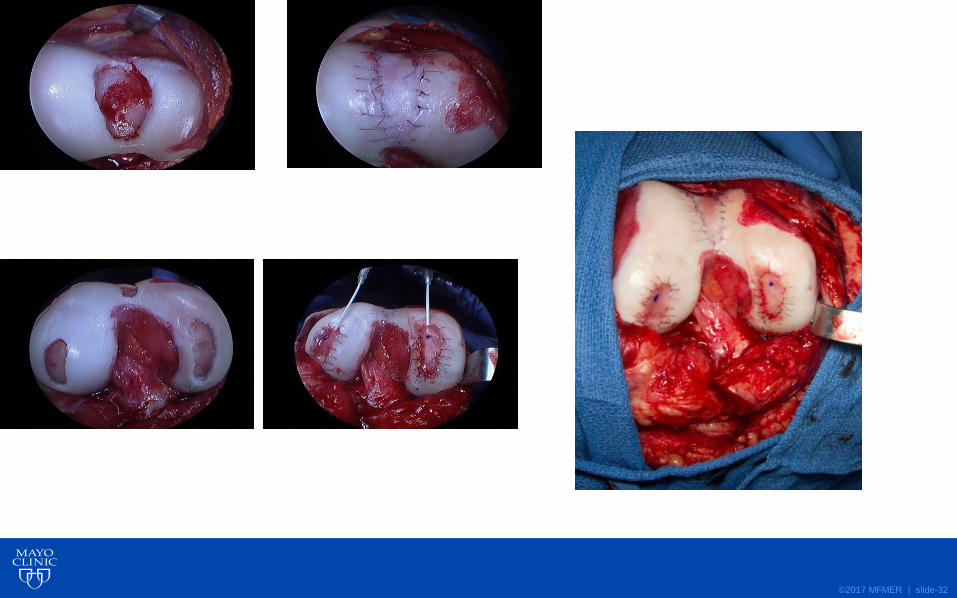
Trochlea chondral lesion
©2017 MFMER | slide-31
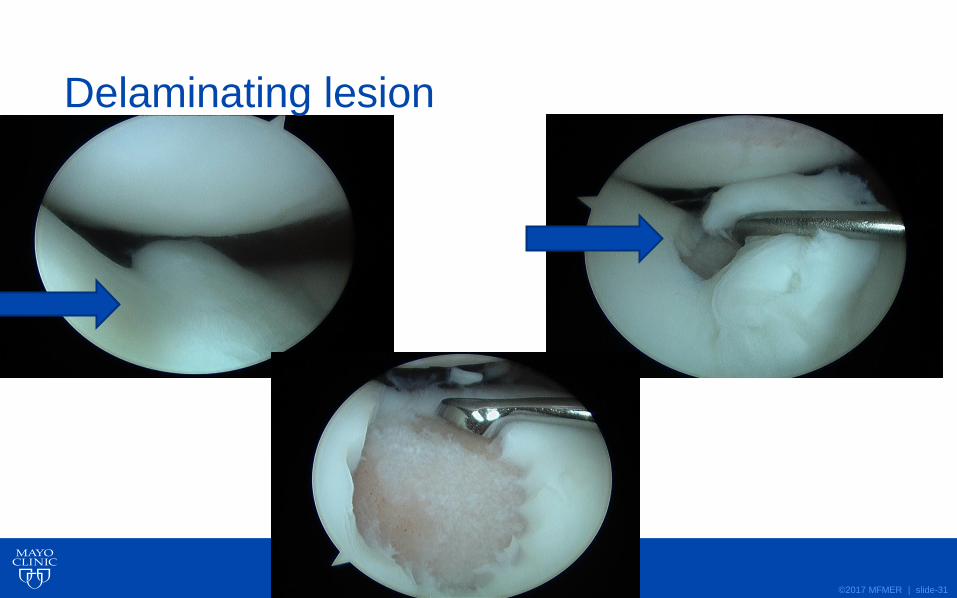
Delaminating lesion
©2017 MFMER | slide-32
©2017 MFMER | slide-33
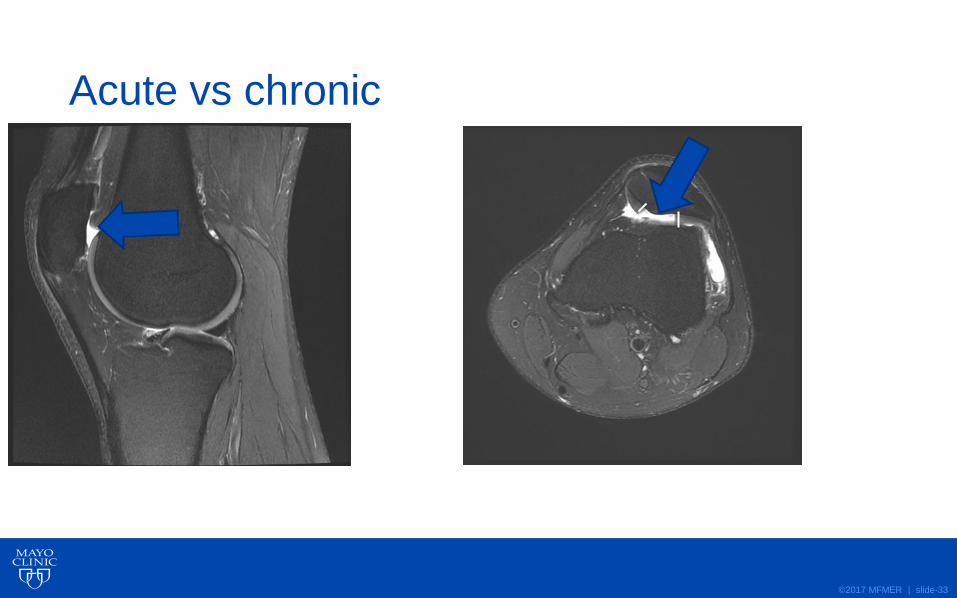
Acute vs chronic
©2017 MFMER | slide-34
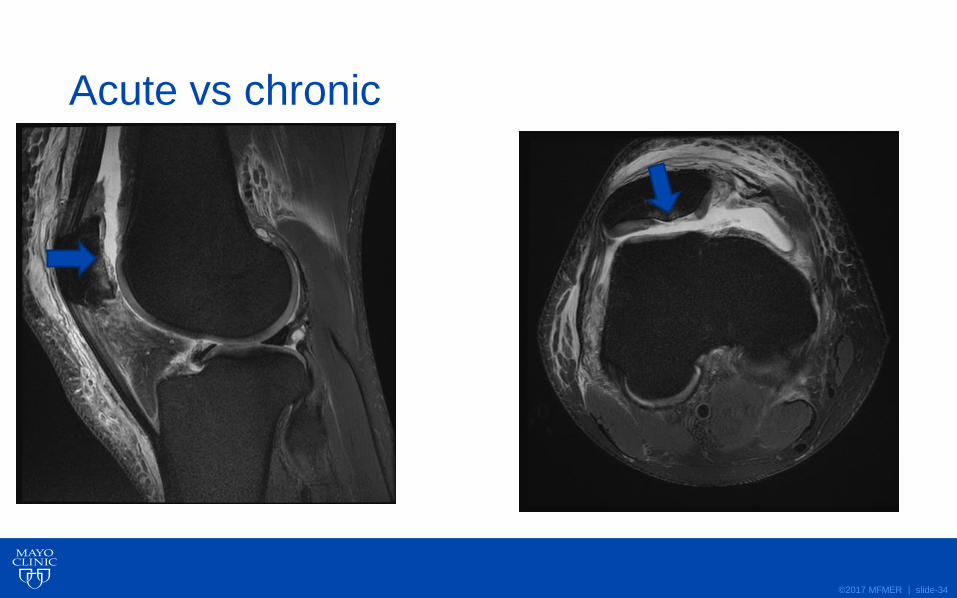
Acute vs chronic
©2017 MFMER | slide-35
MRI: Location
OCA
OAT
©2017 MFMER | slide-36
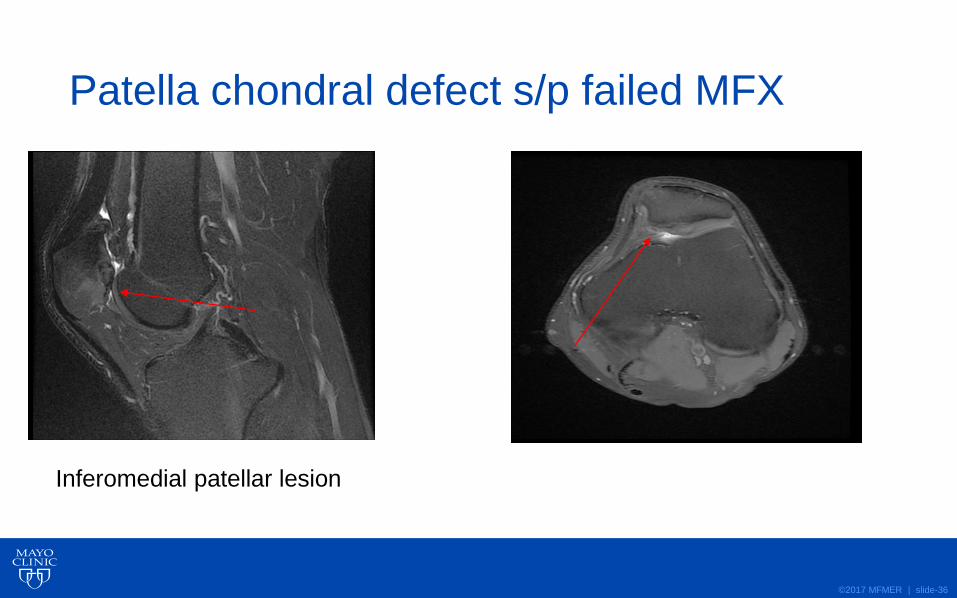
Patella chondral defect s/p failed MFX
Inferomedial patellar lesion
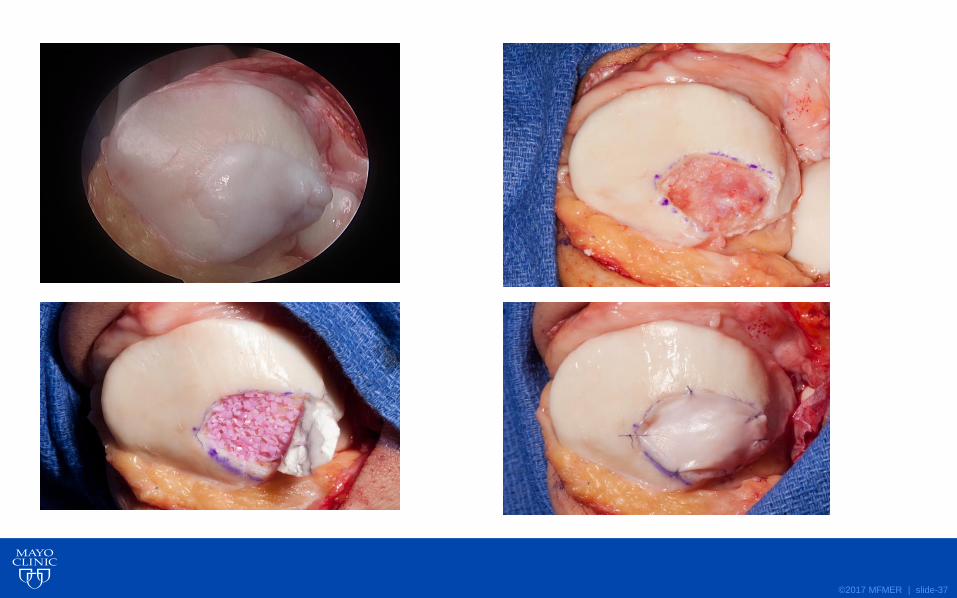
©2017 MFMER | slide-37
©2017 MFMER | slide-38
What do we expect benchmarks to be?• Improved pain
• Improved function
• Long-term outcomes are durable
• Failures
• Osteoarthritis
• Total knee replacements
©2017 MFMER | slide-39
What do we expect benchmarks to be?• Improved pain
• Improved function
• Long-term outcomes are durable
• No failures
• No osteoarthritis
• No total knee replacements
©2017 MFMER | slide-40
Will I have improvement in pain?
Patient
• “I will be pain free”
Clinician
• “We can improve your pain during activities of daily living”
©2017 MFMER | slide-41
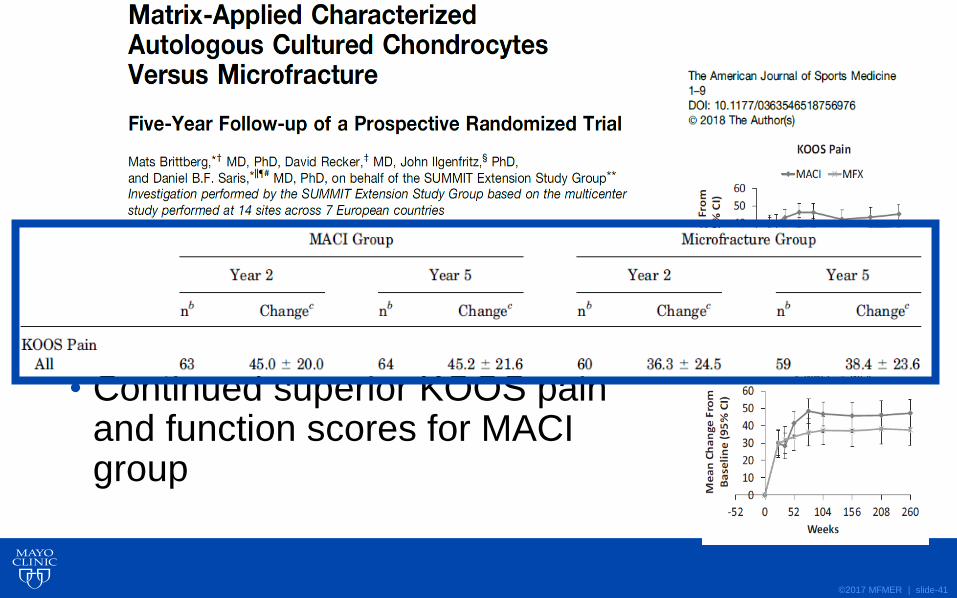
• SUMMIT (MACI vs MFX) 5 year f/u
• 128 of 140 patients included
• Continued superior KOOS pain and function scores for MACI group
©2017 MFMER | slide-42
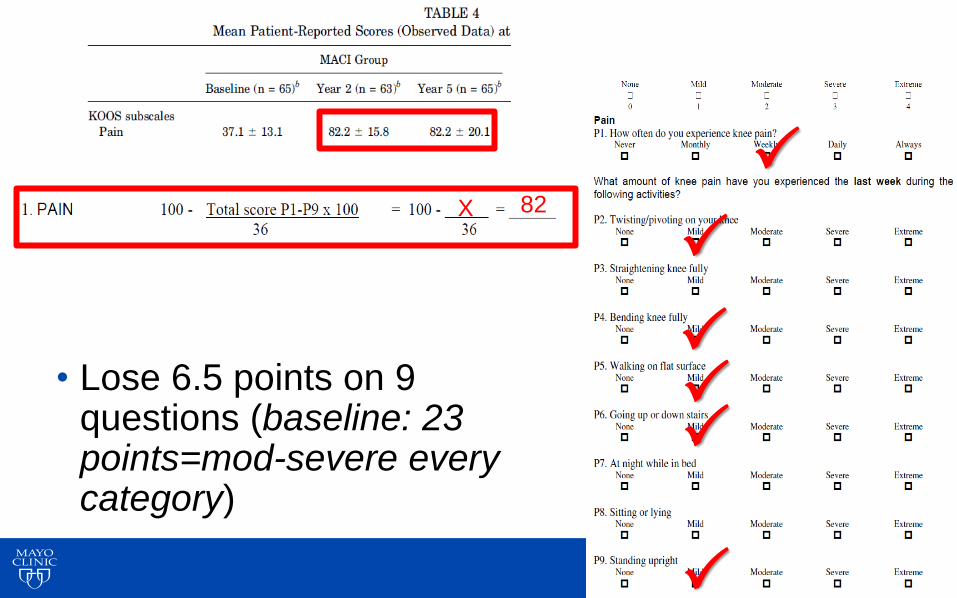
• Lose 6.5 points on 9 questions (baseline: 23 points=mod-severe every category)
X 82
©2017 MFMER | slide-43
Will I have improvement in pain?
Patient
• “I will be pain free”
Clinician
• “We can improve your pain during activities of daily living”
©2017 MFMER | slide-44
How does my patient compare to literature?
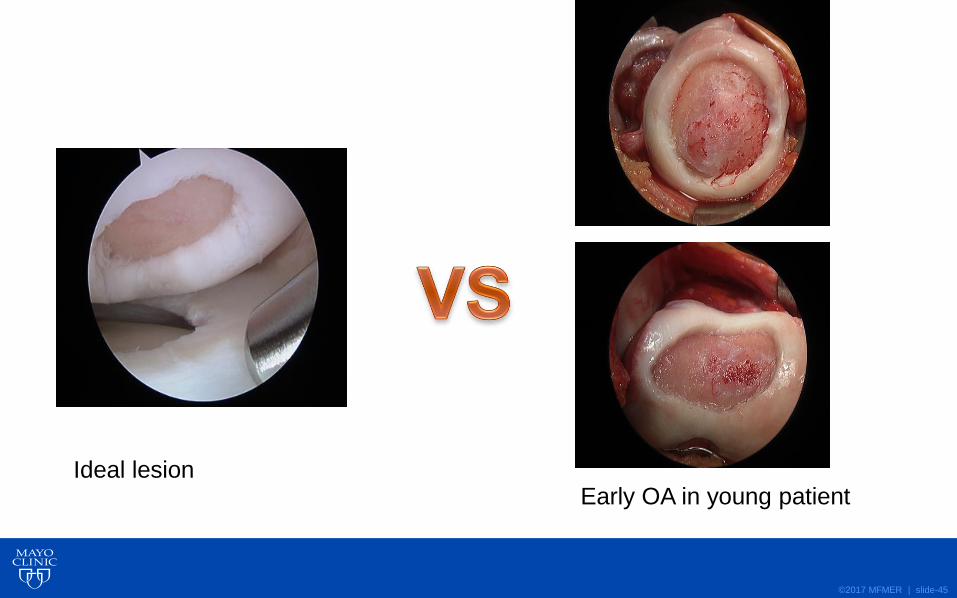
©2017 MFMER | slide-45
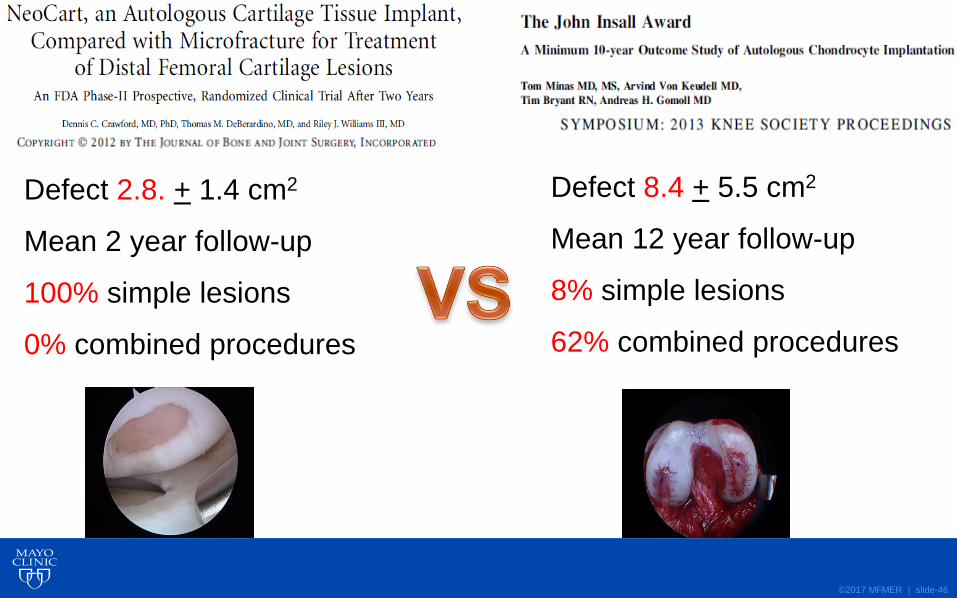
Ideal lesionEarly OA in young patient
©2017 MFMER | slide-46
Defect 2.8. + 1.4 cm2
Mean 2 year follow-up
100% simple lesions
0% combined procedures
Defect 8.4 + 5.5 cm2
Mean 12 year follow-up
8% simple lesions
62% combined procedures
©2017 MFMER | slide-47
Get it Right the First Time!
• Develop standard approach for every patient
• X-rays can help determine focal vs diffuse
lesions, background factors
• Study MRIs to plan cartilage surgery: size,
location, acuity, bone involvement
• Manage patient expectations!