how does the genetic profile of adpkd impact the disease course? dr. york pei 1
TRANSCRIPT

HOW DOES THE GENETIC PROFILE OF ADPKD IMPACT THE DISEASE COURSE?
Dr. York Pei
1

Genotype-Phenotype Correlations in ADPKD
Adapted from:Barua M, et al. J Am Soc Nephrol 2009; 20:1833-41.Cornec-Le Gall E, et al. J Am Soc Nephrol 2013; 24(6):1006-13.
PKD1 mutations ~75% of cases PKD2 mutations ~25% of cases
Phenotype:• More cysts than PKD2• Median age at ESRD ~55 years and
more severe disease associated with truncating mutations• Mild disease similar to PKD2 with
most non-truncating mutations
Phenotype:• Fewer cysts than PKD1• Median age at ESRD ~75 years• Associated with less renal
and extrarenal complications than PKD1

Truncating Mutations Cause More Severe Disease in PKD1 than PKD2
NB: Median age at ESRD occurs ~20 years earlier in PKD1 than PKD21
1. Hateboer N, et al. Lancet 1999; 353(9147):103-7.
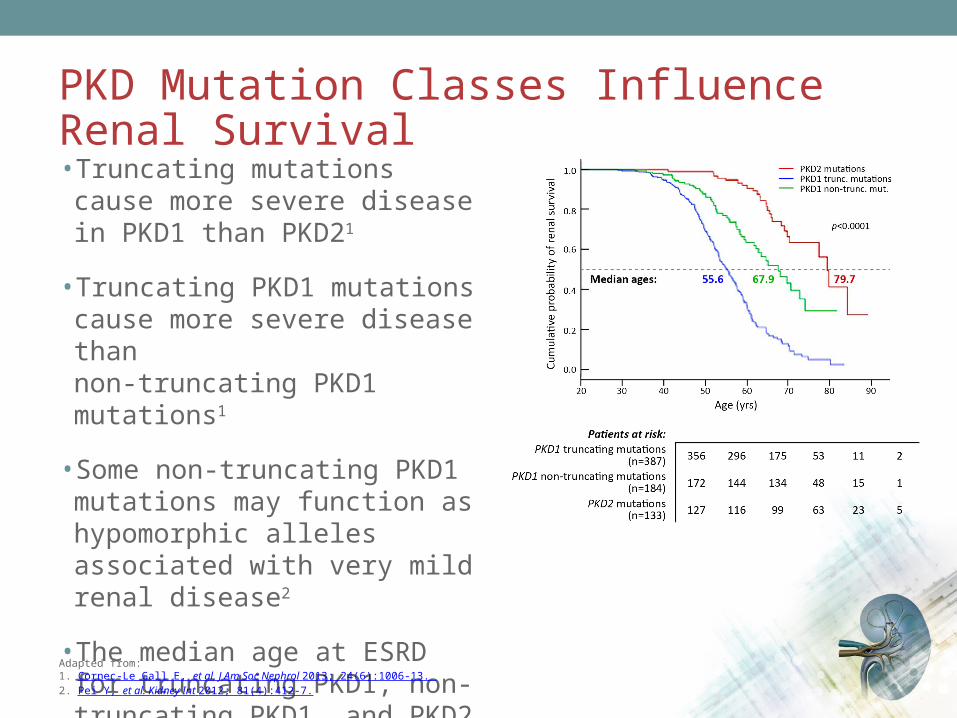
PKD Mutation Classes Influence Renal Survival
• Truncating mutations cause more severe disease in PKD1 than PKD21
• Truncating PKD1 mutations cause more severe disease than non-truncating PKD1 mutations1
• Some non-truncating PKD1 mutations may function as hypomorphic alleles associated with very mild renal disease2
• The median age at ESRD for truncating PKD1, non-truncating PKD1, and PKD2 mutations are 55.6, 67.9, and 79.7 years, respectively1
Adapted from: 1. Cornec-Le Gall E, et al. J Am Soc Nephrol 2013; 24(6):1006-13. 2. Pei Y, et al. Kidney Int 2012; 81(4):412-7.

WHAT IS THE TYPICAL PATTERN OF CYST DEVELOPMENT AND PROGRESSION IN ADPKD?
Dr. Philip McFarlane
2

Timeline of Cyst Burden and Kidney Function in ADPKD
GFR: glomerular filtration rate.Adapted from: Grantham JJ, et al. N Eng J Med 2006; 354(20):2122-30.

Over Time, Cysts Develop and Expand Resulting in Loss of Kidney FunctionExample of Progression in One Patient
GFR: glomerular filtration rate; CKD: chronic kidney disease; TKV: total kidney volume.
Over 13 years, TKV increased by 300% with a 53% loss of kidney function
Age 30CKD Stage 1
GFR 93 mL/min TKV 1441 mL
Age 37CKD Stage 2
GFR 61 mL/min TKV 2775 mL
Age 43CKD Stage 3
GFR 44 mL/min TKV 4459 mL
Normal TKV is ~250 mL in women and ~350 mL in men.

Total Kidney Volume Correlates with Total Cyst Volume
Examples of correlations in individual patients
Kidney growth is highly variable and each individual has their own growth curve.
Measurement variability = inter-observer 2.1%, intra-observer 2.4%, day-to-day 2.4%.Adapted from Grantham JJ, et al. N Eng J Med 2006; 354(20):2122-30.

WHAT ARE THE RISK FACTORS FOR ADPKD DISEASE PROGRESSION?Dr. Neera Dahl
3
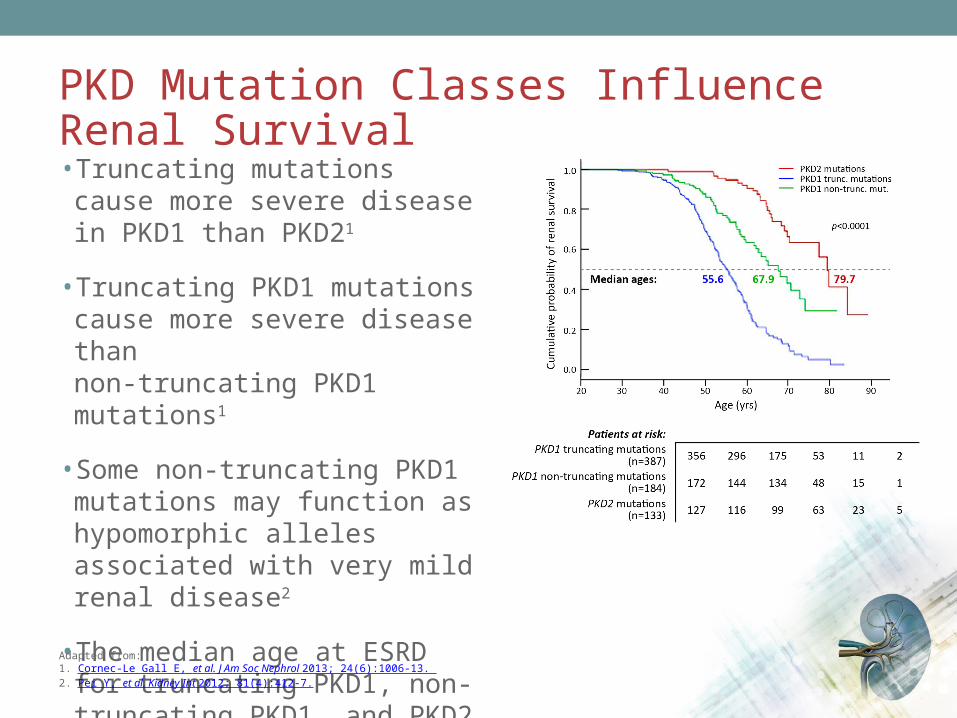
PKD Mutation Classes Influence Renal Survival
• Truncating mutations cause more severe disease in PKD1 than PKD21
• Truncating PKD1 mutations cause more severe disease than non-truncating PKD1 mutations1
• Some non-truncating PKD1 mutations may function as hypomorphic alleles associated with very mild renal disease2
• The median age at ESRD for truncating PKD1, non-truncating PKD1, and PKD2 mutations are 55.6, 67.9, and 79.7 years, respectively1
Adapted from: 1. Cornec-Le Gall E, et al. J Am Soc Nephrol 2013; 24(6):1006-13. 2. Pei Y, et al. Kidney Int 2012; 81(4):412-7.

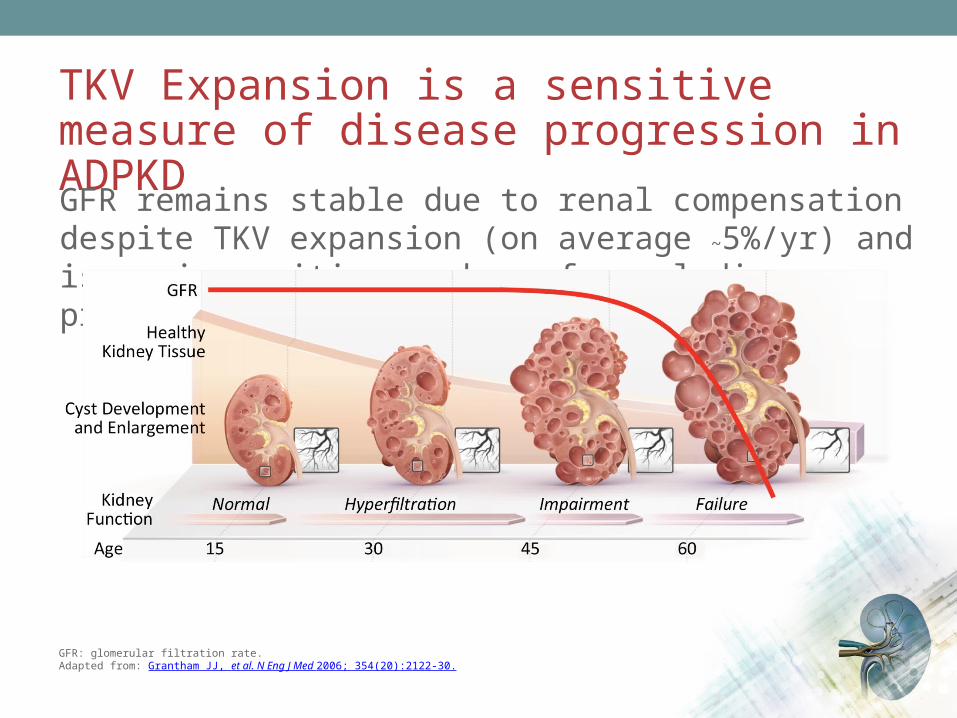
TKV Expansion is a sensitive measure of disease progression in ADPKD
GFR remains stable due to renal compensation despite TKV expansion (on average ~5%/yr) and is an insensitive marker of renal disease progression.
GFR: glomerular filtration rate.Adapted from: Grantham JJ, et al. N Eng J Med 2006; 354(20):2122-30.

Clinical Risk Factors in ADPKD
Potentially modifiable traits that are associated with poorer prognosis in ADPKD:
• Lower serum HDL-cholesterol1
• Greater urine sodium excretion1
• Higher urine osmolality1
• Higher serum uric acid2
• Greater body surface area, body mass index1
• Higher protein intake1
• Higher blood pressure1
• Albuminuria1
• Diabetes3
Adapted from:1. Torres V, et al. Clin J Am Soc Nephrol 2011; 6(3):640-7.2. Helal I, et al. Nephrol Dial Transplant 2013; 28(2):380-5.3. Reed B, et al. Nephrol Dial Transplant 2012; 27(7):2862-5.
WHAT IS THE RELATIONSHIP BETWEEN GROWTH IN KIDNEY VOLUME AND KIDNEY FUNCTION IN ADPKD?Dr. Philip McFarlane
4
TKV Expansion is a sensitive measure of disease progression in ADPKD
GFR remains stable due to renal compensation despite TKV expansion (on average ~5%/yr) and is an insensitive marker of renal disease progression.
GFR: glomerular filtration rate.Adapted from: Grantham JJ, et al. N Eng J Med 2006; 354(20):2122-30.
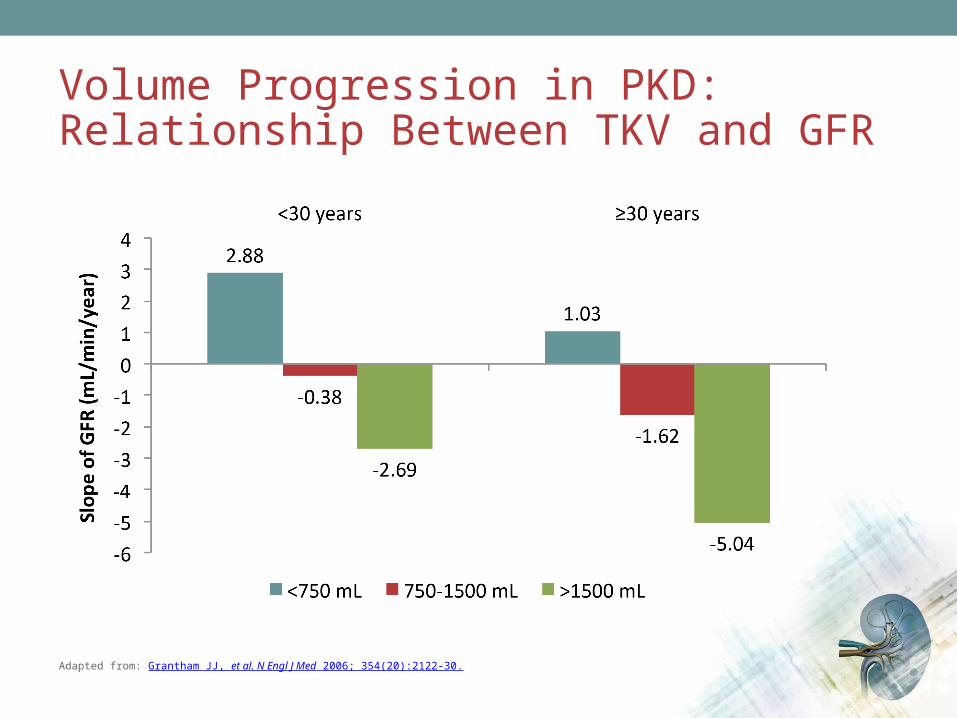
Volume Progression in PKD: Relationship Between TKV and GFR
Adapted from: Grantham JJ, et al. N Engl J Med 2006; 354(20):2122-30.

Changes in Height-adjusted TKV and eGFR Over Time in ADPKD
htTKV: height-adjusted total kidney volume; GFR by iothalamate clearance.NIH CRISP Studies. Chapman AB, et al. Clin J Am Soc Nephrol 2012; 7(3):479-86. (supplemental data)

WHAT IS THE ROLE OF TKV IN PRACTICE?Dr. Neera Dahl
5

Controversies with Total Kidney Volume
•Should TKV be used to measure disease progression in clinical trials for ADPKD?
•Which imaging approach should be used?
•Should TKV be used to ascertain prognosis and monitor disease progression in clinical practice? How?
TKV: Finding a Place in Research and the Clinic
•Data from CRISP supports the inclusion of TKV as a tool for study population enrichment and as a primary endpoint in RCTs
•Further data informing the association between TKV and outcomes would be welcome
•There is no current consensus on the use of renal imaging as part
of routine care
•There is no consensus on the preferred imaging modality (US, MRI or CT) or formula for measuring/estimating TKV
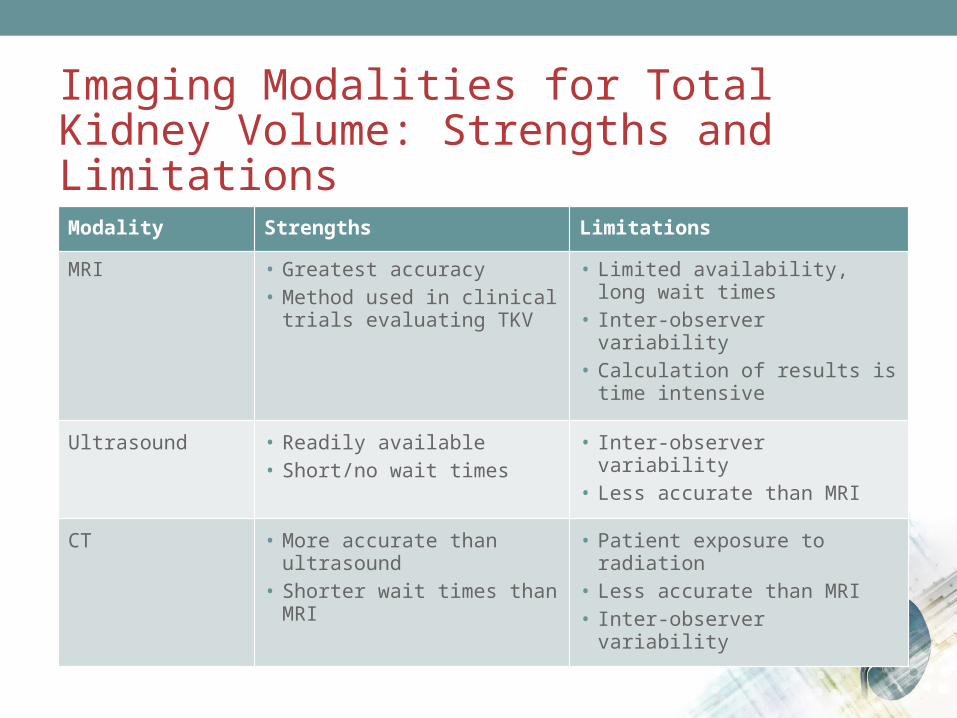
Imaging Modalities for Total Kidney Volume: Strengths and Limitations
Modality Strengths Limitations
MRI • Greatest accuracy• Method used in clinical trials
evaluating TKV
• Limited availability, long wait times• Inter-observer variability• Calculation of results is time
intensive
Ultrasound • Readily available• Short/no wait times
• Inter-observer variability• Less accurate than MRI
CT • More accurate than ultrasound• Shorter wait times than MRI
• Patient exposure to radiation• Less accurate than MRI• Inter-observer variability
HOW DO YOU DIAGNOSE ADPKD AND WHAT IS THE ROLE OF GENETIC TESTING?
Dr. Ahsan Alam
6

Ultrasonographic Diagnostic Criteria for ADPKD
Population Criteria for Diagnosis of ADPKD
At-risk individuals from ADPKD families of unknown genotype
Ages 15 to 39 years ≥ 3 (unilateral or bilateral) renal cysts
Ages 40 to 59 years ≥ 2 cysts in each kidney
For at-risk individuals aged 60 yr, in whom renal cysts are numerous in both PKD1 and PKD2 and among whom simple cysts are frequently found
≥ 4 cysts in each kidney
NB. < 2 renal cysts in at-risk individuals aged ≥40 years is sufficient to exclude the disease
Pei Y, et al. J Am Soc Nephrol 2009; 20:205-12.

Counselling Before Screening for an Individual with a Family History of ADPKD•Counsel first and make the decision to test on a case-by-case basisPOSSIBLE BENEFITS OF TESTING POTENTIAL DRAWBACKS OF TESTING
Certainty regarding diagnosis that may influence family planning and insurability (including negative test results)
The potential for discrimination (e.g., health insurability, employment)
Early detection and treatment of disease complications
Psychological burden of a chronic disease
Identification of genetically unaffected family members for living related-donor renal transplantation
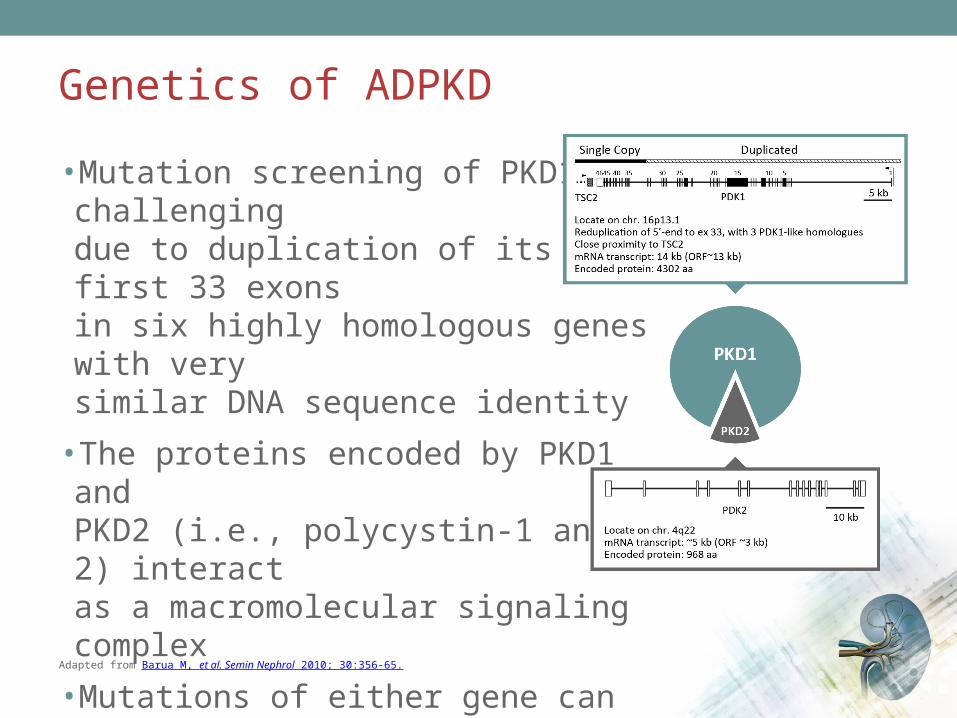
Genetics of ADPKD
•Mutation screening of PKD1 is challenging due to duplication of its first 33 exons in six highly homologous genes with very similar DNA sequence identity
•The proteins encoded by PKD1 and PKD2 (i.e., polycystin-1 and -2) interact as a macromolecular signaling complex
•Mutations of either gene can interrupt polycystin signaling pathway resulting in similar clinical manifestations
Adapted from Barua M, et al. Semin Nephrol 2010; 30:356-65.

Dr. York Pei
WHAT IS THE EVIDENCE SUPPORTING THE USE OF WATER THERAPY FOR ADPKD?
7
Rationale for Water Therapy in ADPKD
•cAMP is one of the key drivers of cyst enlargement
• In animal models, ingestion of large amounts of water promotes diuresis by suppressing plasma levels of arginine vasopressin (AVP) and renal levels of cAMP, slowing cyst progression
Adapted from: Wang CJ, et al. Clin J Am Soc Nephrol 2011; 6(1):192-7.
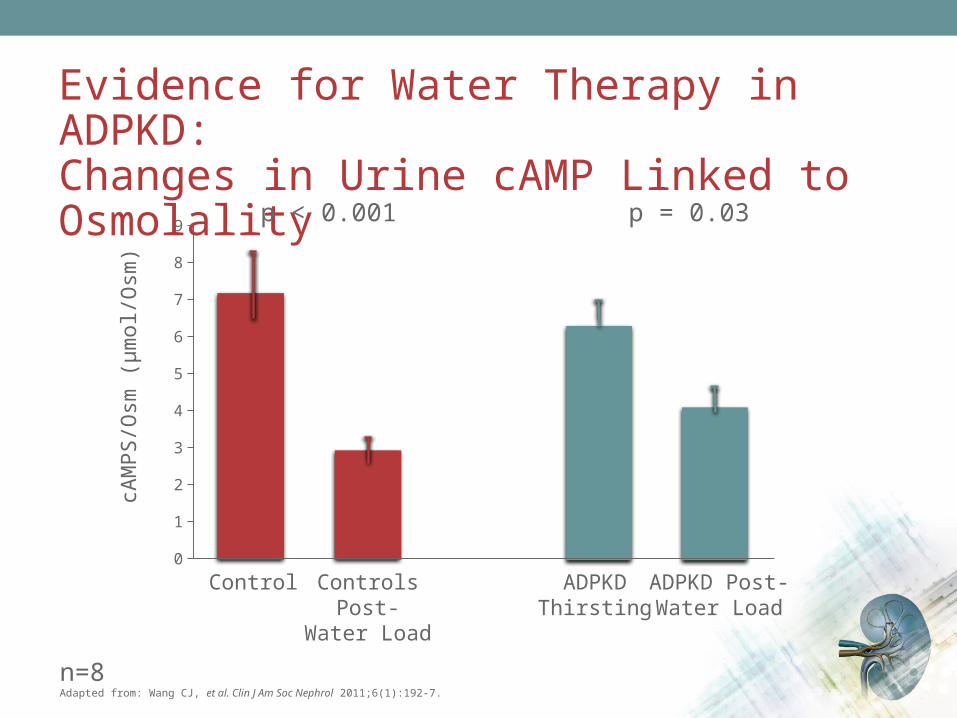
Evidence for Water Therapy in ADPKD:Changes in Urine cAMP Linked to Osmolality
n=8Adapted from: Wang CJ, et al. Clin J Am Soc Nephrol 2011;6(1):192-7.
0
1
2
3
4
5
6
7
8
9
cAM
PS/O
sm (µ
mol
/Osm
)
p < 0.001 p = 0.03
Control Controls Post-Water Load
ADPKDThirsting
ADPKD Post-Water Load

Observational Study:No Benefit from Water Therapy in ADPKD
Adapted from: Higashihara E, et al. Nephrol Dial Transplant 2014;29(9):1710-9.
High water intake group Free water intake group
Key limitations of the study• Small sample size• One-year duration• Underpowered, inconclusive
P = 0.047 P = 0.39 P = 0.011 P = 0.35
Chan
ge o
f tot
al k
idne
y vo
lum
e(m
L / y
ear)
-150-100
-500
50100150200250300350400450500
Chan
ge o
f eG
FR(E
q) s
lope
(mL
/ min
/ 1.
73m
2 / y
ear)
-30
-25
-20
-15
-10
-5
0
5
10
15
Total Kidney Volume eGFR
Summary: Current Understanding ofWater Therapy for ADPKD•There is no consensus as to whether increased water can alter the natural course of disease
•The size and quality of the limited available evidence makes definitive conclusions impossible at this point
•There is no consensus or evidence on the appropriate volume of water to recommend–3-4 L daily may be appropriate
– It is unknown if goals can be achieved over the longer term
• Increased water consumption does have known benefits for prevention of nephrolithiasis1
•Adherence to water therapy is difficult for many patients
1. Hall PM. Cleve Clin J Med 2009; 76(10):583-91.
WHAT IS THE PRESUMED MECHANISM OF ACTION OF TOLVAPTAN?Dr. Philip McFarlane
8
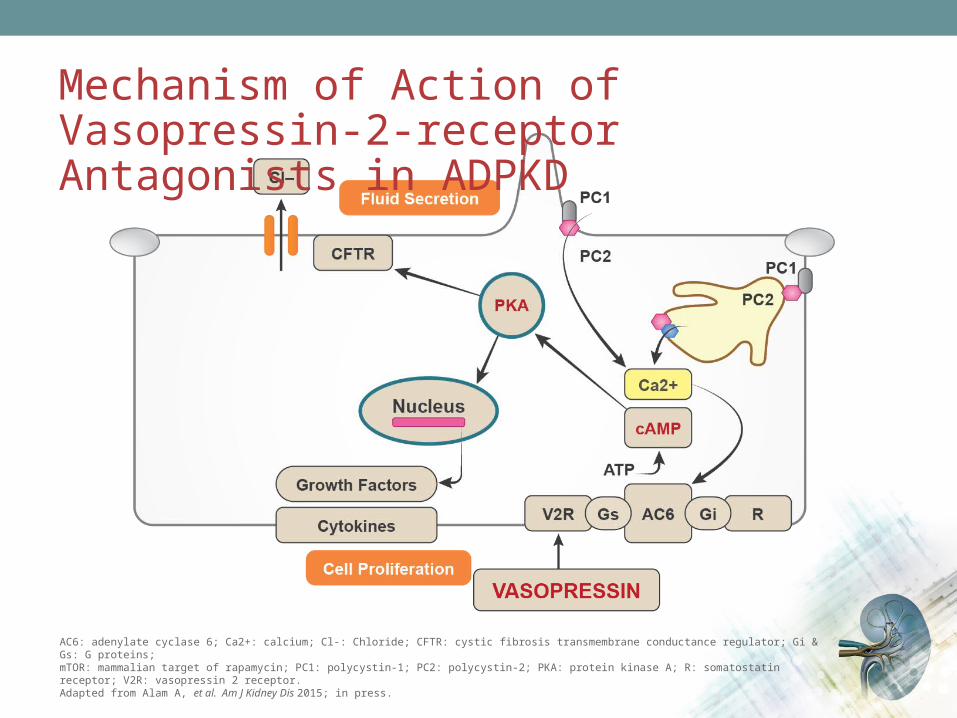
Mechanism of Action of Vasopressin-2-receptor Antagonists in ADPKD
AC6: adenylate cyclase 6; Ca2+: calcium; Cl-: Chloride; CFTR: cystic fibrosis transmembrane conductance regulator; Gi & Gs: G proteins;mTOR: mammalian target of rapamycin; PC1: polycystin-1; PC2: polycystin-2; PKA: protein kinase A; R: somatostatin receptor; V2R: vasopressin 2 receptor. Adapted from Alam A, et al. Am J Kidney Dis 2015; in press.

Mechanism of Action of Tolvaptan
cAMP: adenosine 3 , 5 -cyclic monophosphate ′ ′Adapted from Otsuka Canada Pharmaceuticals Inc. PrJINARC™ Product monograph. Date of Preparation: February 11, 2015.
Administration of tolvaptan
↓ binding of vasopressin at the V2 receptor in the kidney
↓ adenylate cyclase activity
↓ intracellular cAMP concentrations
↑ in free water clearance(i.e., aquaresis)
↓ in urine osmolality ↓ rate of growth of total kidney volume
↓ rate of formation and enlargement of kidney cysts

WHAT ROLE CAN MODULATION OF THE RAAS AND BLOOD PRESSURE PLAY IN THE TREATMENT OF ADPKD?Dr. Ahsan Alam
9

Impact of Different BP Targets in Early ADPKD: Design of the HALT-PKD Study A•Double-blind, placebo-controlled trial
• 558 hypertensive participants with ADPKD
– 15 to 49 years old
–Baseline eGFR >60 mL/min/1.73 m2
• 2 randomizations:
–BP target: standard (120/70 to 130/80 mmHg) or low (95/60 to 110/75 mmHg) target range
–RAAS blockade: ACE inhibitor (lisinopril) + placebo or an ARB (telmisartan)
• Followed for 5 years
• Primary efficacy outcome: Annual % change in total kidney volume
Adapted from Schrier RW, et al. N Engl J Med. 2014 Nov 15. [Epub ahead of print].
Possible imbalance in randomization: mutations

Different BP Targets in Early ADPKD: Changes in Total Kidney Volume and eGFR (HALT-PKD Study A)
BP: blood pressure; TKV: total kidney volume; eGFR: estimated glomerular filtration rate; LVMI: left-ventricular mass index; UAE: urinary albumin excretion.Adapted from Schrier RW, et al. N Engl J Med 2014;371(24):2255-66
Conclusion of the BP analysis: As compared with standard BP control, rigorous BP control was associated with a slower increase in TKV, no overall change in the eGFR, a greater decline in the LMVI, and greater reduction in UAE.
Standard blood pressure
Low blood pressure, 5.6%/yrStandard blood pressure, 6.6%/yrDifference, -1.0 percentage points/yr (95% CI, -1.6 to -0.2)P=0.006
Follow-up (mo)
L n To
tal K
idne
y Vo
lum
e (m
L)
0 24 48 60
6.9
7.0
7.1
7.2
7.3
7.4
Low blood pressure, -2.9 mL/min/1.73 m2/yrStandard blood pressure, -3.0 mL/min/1.73 m2/yrDifference, -0.1 mL/min/1.73 m2/yr (95% CI, -0.3 to 0.6)P=0.55
Follow-up (mo)
Obs
erve
d eG
FR (m
L/m
in/1
.73
m2 )
40
50
60
80
90
70
0 24 48 7212 36 60 84 96
Low blood pressureStandard blood pressureLow blood pressure
Changes in TKV Changes in eGFR

WHAT ARE THE DATA SUPPORTING USE OF TOLVAPTAN FOR ADPKD?
Dr. Neera Dahl
10

Tolvaptan in ADPKD:Design of the Pivotal TEMPO 3:4 Trial•3-year, placebo-controlled trial
• Interventions: Tolvaptan twice daily or placebo
• Subjects: 1,445 patients with ADPKD–Baseline TKV > 750 mL by MRI (mean baseline 1705 mL in tolvaptan group; 1668 mL
in placebo group)
–Baseline estimated creatinine clearance ≥60 mL/min (mean baseline 104 mL/min in both groups)
•Primary outcome: Annual rate of change in TKV
•Composite secondary outcome: time to progression (worsening kidney function,* clinically significant kidney pain,† worsening hypertension‡ or worsening albuminuria§)
•Additional secondary outcome: Change in the slope of kidney function, measured by the reciprocal of the serum creatinine level* ≥25% reduction in the reciprocal of the serum creatinine level from the value at the end of the dose-adjustment period, reproduced after at least 2 weeks); †necessitating medical
leave, pharmacologic treatment (narcotic or last-resort analgesic agents), or invasive intervention; ‡changes in blood-pressure category, as defined in the protocol, or worsening of hypertension requiring an increase in hypertensive treatment; § according to sex-specified categories as defined in the protocolTKV: Total kidney volumeAdapted from Torres VE, et al. N Engl J Med 2012; 367(25):2407-18
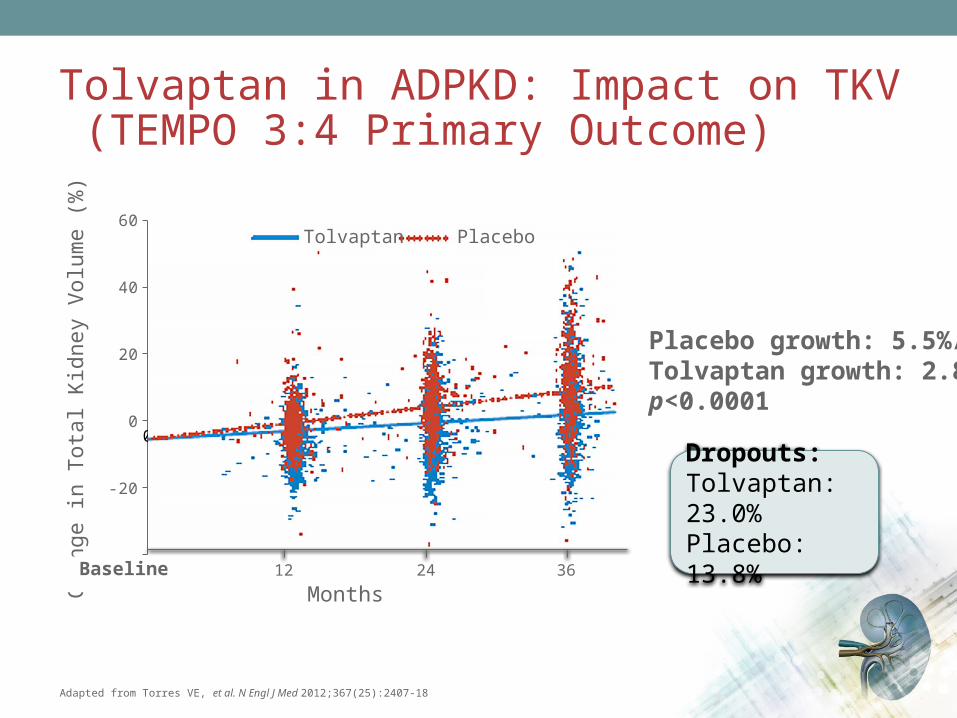
Tolvaptan in ADPKD: Impact on TKV (TEMPO 3:4 Primary Outcome)
Adapted from Torres VE, et al. N Engl J Med 2012;367(25):2407-18
Placebo growth: 5.5%/yrTolvaptan growth: 2.8%/yrp<0.0001
Dropouts:Tolvaptan: 23.0%Placebo: 13.8%
0 4 8 12 16 20 24 28 32 36 40
-40
-20
0
20
40
60
Months12 24 36
Chan
ge in
Tot
al K
idne
y Vo
lum
e (%
)
Baseline
Tolvaptan Placebo
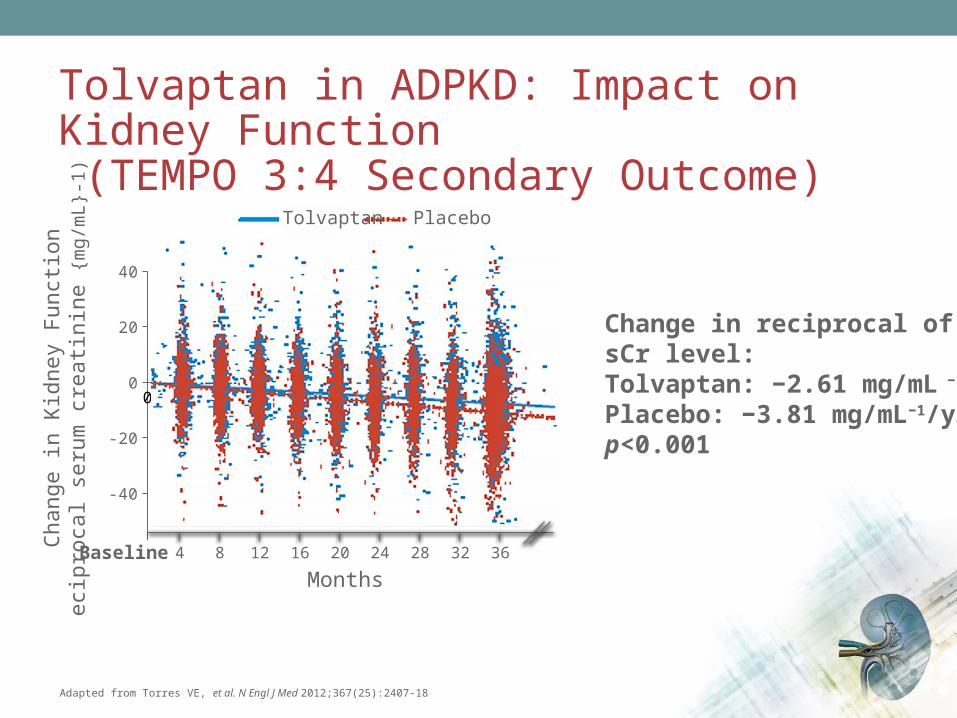
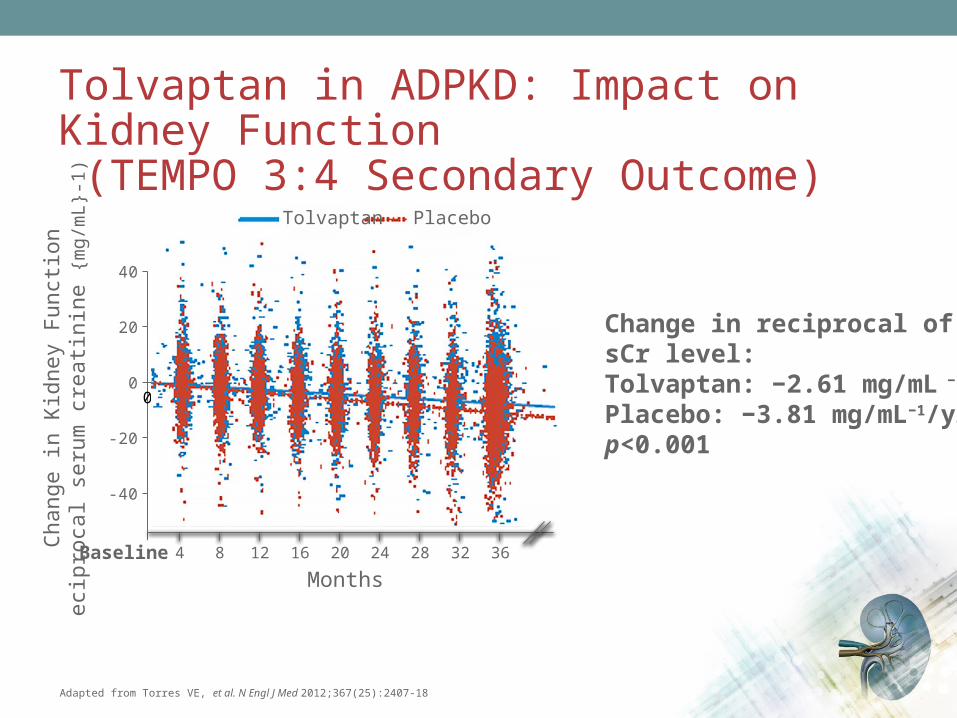
Tolvaptan in ADPKD: Impact on Kidney Function (TEMPO 3:4 Secondary Outcome)
Adapted from Torres VE, et al. N Engl J Med 2012;367(25):2407-18
Change in reciprocal of the sCr level:Tolvaptan: −2.61 mg/mL −1/yr Placebo: −3.81 mg/mL−1/yrp<0.001
0 4 8 12 16 20 24 28 32 36 40
-60
-40
-20
0
20
40
MonthsBaseline
Chan
ge in
Kid
ney
Func
tion
ecip
roca
l ser
um c
reati
nine
{mg/
mL}
-1) Tolvaptan Placebo
1284 242016 363228

Tolvaptan in ADPKD: Impact on Kidney Pain (TEMPO 3:4 Secondary Outcome)
Adapted from Torres VE, et al. N Engl J Med 2012;367(25):2407-18
0 4 8 12 16 20 24 28 32 360
0.1
0.2
0.3
Cum
ulati
ve E
vent
Haz
ard
Study Months
Placebo
Tolvaptan
Hazard ratio, 0.64 (95% CI, 0.47-0.89)P=0.007 by Cox model
Baseline
Tolvaptan 961 870 835 811 792 776 763 752 744 642
Placebo 483 472 463 454 446 438 428 422 418 359
No. At Risk

Tolvaptan: The First Approved Treatment For Slowing Disease Progression in ADPKD
•Tolvaptan is indicated to slow the progression of kidney enlargement in patients with autosomal dominant polycystic kidney disease (ADPKD)
• In ADPKD, kidney enlargement reflects renal cyst burden
Otsuka Canada Pharmaceuticals Inc. PrJINARC™ Product monograph. Date of Preparation: February 11, 2015.
WHAT IS THE STATUS OF THE EVIDENCE FOR THE USE OF MTOR INHIBITORS FOR ADPKD?Dr. Paul Tam
11

Clinical Study of mTOR Inhibition in ADPKD: Sirolimus •18-month, open-label, RCT (n=100)
• Interventions: Sirolimus 2 mg daily vs. standard care
•Baseline TKV: 875 mL in sirolimus group, 987 mL in control group
•Baseline eGFR: 92 mL/min
•Primary endpoint: total kidney volume at 18 months
Adapted from Serra AL, et al. N Engl J Med 2010; 363(9):820-9.
Key limitations of the study• Small numbers• Short duration • Non-maximal dosing of the drug?• Strictly an early PKD cohort
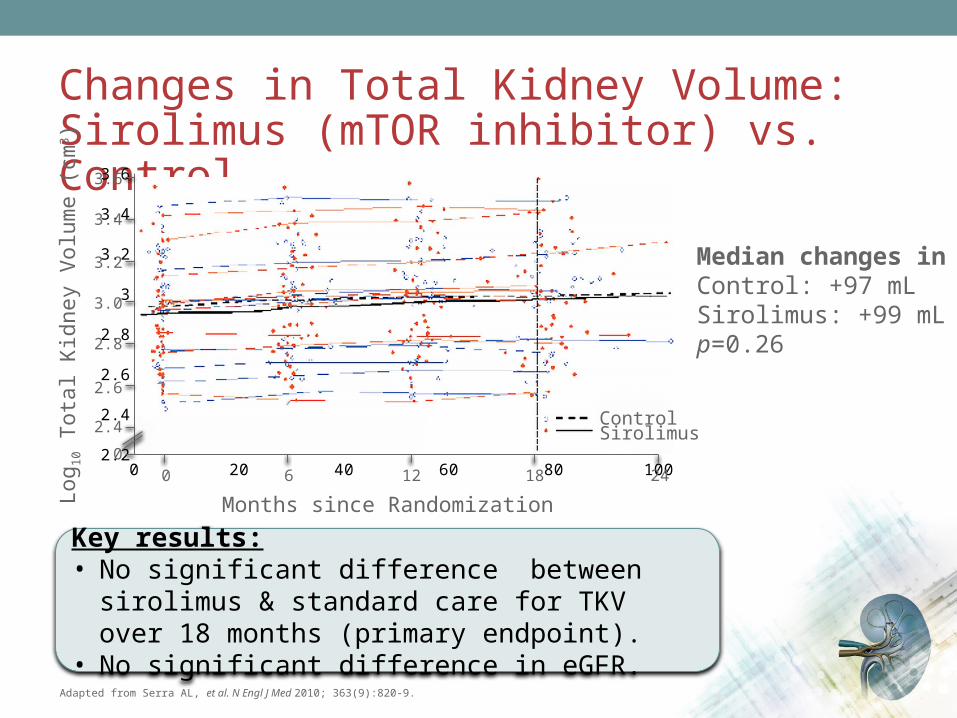
Changes in Total Kidney Volume:Sirolimus (mTOR inhibitor) vs. Control
Adapted from Serra AL, et al. N Engl J Med 2010; 363(9):820-9.
Key results:• No significant difference between sirolimus & standard
care for TKV over 18 months (primary endpoint).• No significant difference in eGFR.
Median changes in TKV:Control: +97 mLSirolimus: +99 mLp=0.26
0 20 40 60 80 1002.2
2.4
2.6
2.8
3
3.2
3.4
3.6
Log 10
Tot
al K
idne
y Vo
lum
e (c
m3 )
Months since Randomization12 18 2460
ControlSirolimus
0
2.4
2.6
2.8
3.0
3.2
3.4
3.6

mTOR Inhibition in ADPKD: Everolimus
• 2-year, double-blind trial (n=433)
• Interventions: Everolimus 2.5 mg b.i.d. vs. placebo
•Baseline TKV: 2028 mL in everolimus group; 1911 mL in placebo group
•Baseline eGFR: 53 ml/min in everolimus; 56 ml/min in placebo
• Primary outcome: Change in TKV
Adapted from Walz G, et al. N Engl J Med. 2010;363(9):830-40.
Key limitations of the study• 32.7% of the treated patients dropped out: no
MRIs were available• Investigators estimated the missing data by
imputation (i.e., analysis was not ITT)
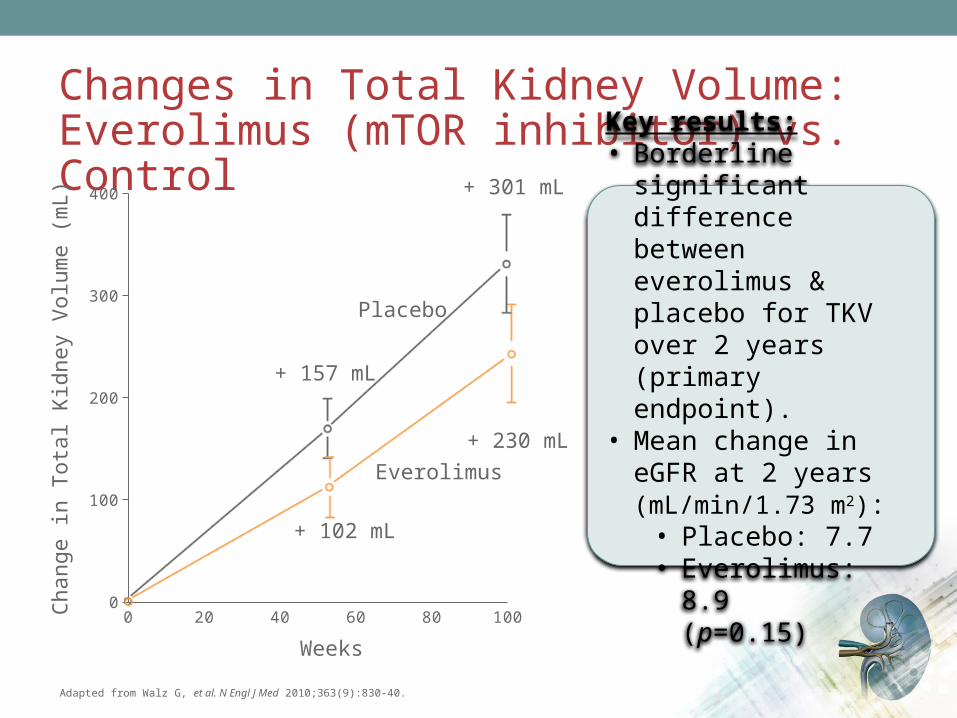
Changes in Total Kidney Volume:Everolimus (mTOR inhibitor) vs. Control
Adapted from Walz G, et al. N Engl J Med 2010;363(9):830-40.
Key results:• Borderline significant
difference between everolimus & placebo for TKV over 2 years (primary endpoint).
• Mean change in eGFR at 2 years (mL/min/1.73 m2):• Placebo: 7.7• Everolimus: 8.9
(p=0.15)
0 20 40 60 80 1000
100
200
300
400
Chan
ge in
Tot
al K
idne
y Vo
lum
e (m
L)
+ 157 mL
+ 102 mL
+ 301 mL
+ 230 mL
Weeks
Placebo
Everolimus

mTOR Inhibition for ADPKD:Summary of Current Knowledge•Conclusion of recent meta-analysis of sirolimus studies (4 RCTs):1
– In ADPKD patients, treatment with sirolimus is safe and can effectively slow kidney growth, but it seems not to slow down the decrease of GFR
•However, data are not currently strong enough to recommend the use of these therapies in ADPKD
• It appears from the study by Walz et al that mTOR inhibitors are poorly tolerated at higher doses
•Further study is required
1. Liu YM, et al. Transplant Proc 2014; 46(1):66-74.
SHOULD WE BE SCREENING FOR INTRACRANIAL ANEURYSMS IN ADPKD PATIENTS?Dr. Navdeep Tangri
12
Cardiovascular Complications of PKD:Intracranial Aneurysms•Higher prevalence in ADPKD (9-12%) than in the general population (2-3%)1-6
• In ADPKD prevalence is ~20-27% among those with a family history and ~6% in those lacking a family history1-5,7
• Account for 4-7 % of all deaths in ADPKD8
• Screening:–A family history of ruptured aneurysms or sudden death is a strong indication
for MRI-based screening1
• Repeating negative screens in patient with positive family history can be done in 5-10 years, but there are no data to guide rescreening
– If positive – refer to neuro/vascular surgery for treatment or follow up– Screening in those without a family history is controversial – can be based
on physician and patient preferences
1. Ruggieri P, et al. Radiology 1994; 91:33-9.2. Irazabal MV, et al. Clin J Am Soc Nephrol 2011;6:1274-85.3. Huston J, et al. J Am Soc Nephrol 1993;3:1871-7.4. Xu HW, et al. Stroke 2011;42:204-6.
5. Graf S, et al. Nephrol Dial Transplant 2002;17:819-23.6. Vlak MH, et al. Lancet Neurol 2011;10:626-36.7. Chapman AB, et al. N Eng J Med 1992;327:916-20.8. Ecder T, et al. Nat Rev Nephrol 2009;5(4):221-8.
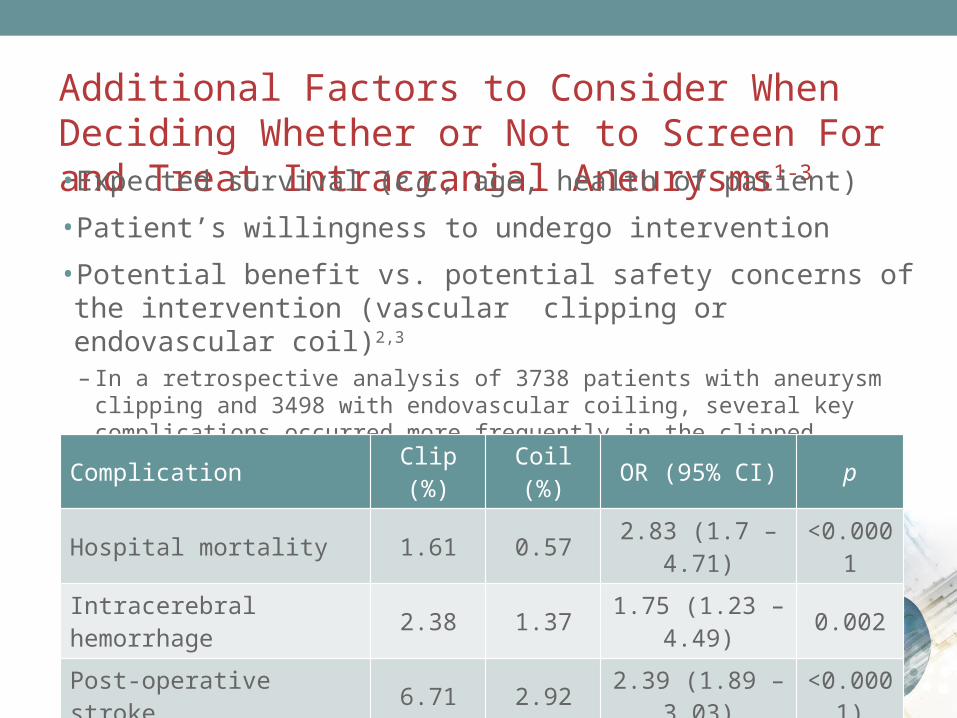
Additional Factors to Consider When Deciding Whether or Not to Screen For and Treat Intracranial Aneurysms1-3
• Expected survival (e.g., age, health of patient)
• Patient’s willingness to undergo intervention
• Potential benefit vs. potential safety concerns of the intervention (vascular clipping or endovascular coil)2,3
– In a retrospective analysis of 3738 patients with aneurysm clipping and 3498 with endovascular coiling, several key complications occurred more frequently in the clipped population:2
1. Rozenfeld MN, et al. AJNR Am J Neuroradiol 2014;35:3-9.2. Alshekhlee A, et al. Stroke 2010; 41:1471-6.3. Brinjikji W, et al. AJNR Am J Neuroradiol 2011;32:1071-5.
Complication Clip (%) Coil (%) OR (95% CI) p
Hospital mortality 1.61 0.57 2.83 (1.7 – 4.71) <0.0001
Intracerebral hemorrhage 2.38 1.37 1.75 (1.23 – 4.49) 0.002
Post-operative stroke 6.71 2.92 2.39 (1.89 – 3.03) <0.0001)

HOW IS TOLVAPTAN DOSED AND TITRATED?Dr. Philip McFarlane
13
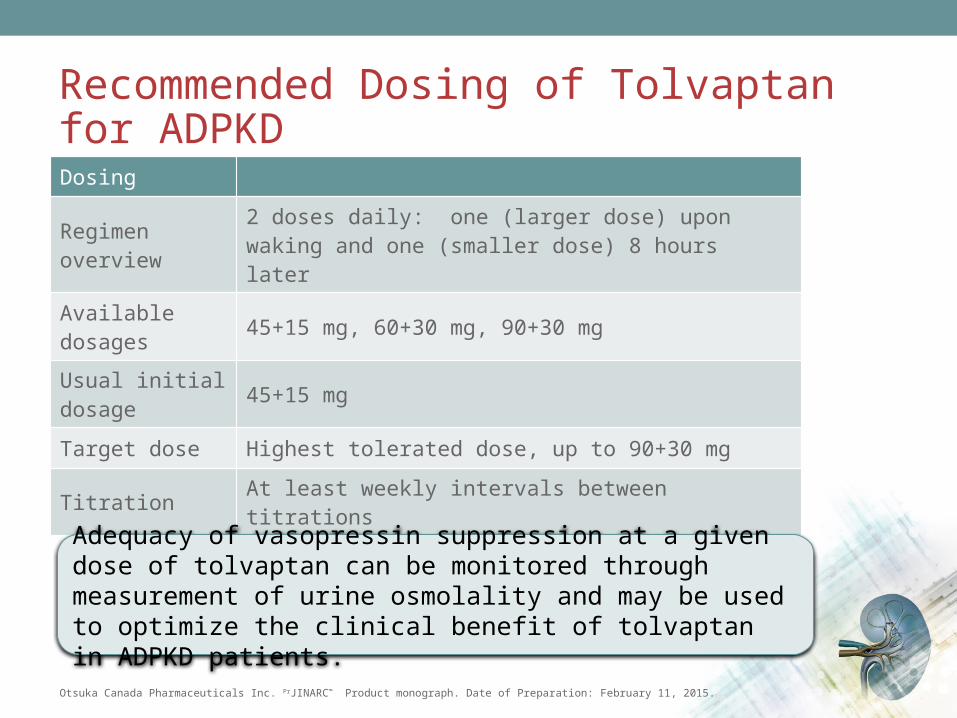
Recommended Dosing of Tolvaptan for ADPKD
Otsuka Canada Pharmaceuticals Inc. PrJINARC™ Product monograph. Date of Preparation: February 11, 2015.
Dosing
Regimen overview 2 doses daily: one (larger dose) upon waking and one (smaller dose) 8 hours later
Available dosages 45+15 mg, 60+30 mg, 90+30 mg
Usual initial dosage 45+15 mg
Target dose Highest tolerated dose, up to 90+30 mg
Titration At least weekly intervals between titrations
Adequacy of vasopressin suppression at a given dose of tolvaptan can be monitored through measurement of urine osmolality and may be used to optimize the clinical benefit of tolvaptan in ADPKD patients.

WHAT POTENTIAL DRUG INTERACTIONS SHOULD WE BE AWARE OF WITH TOLVAPTAN?Dr. Paul Tam
14
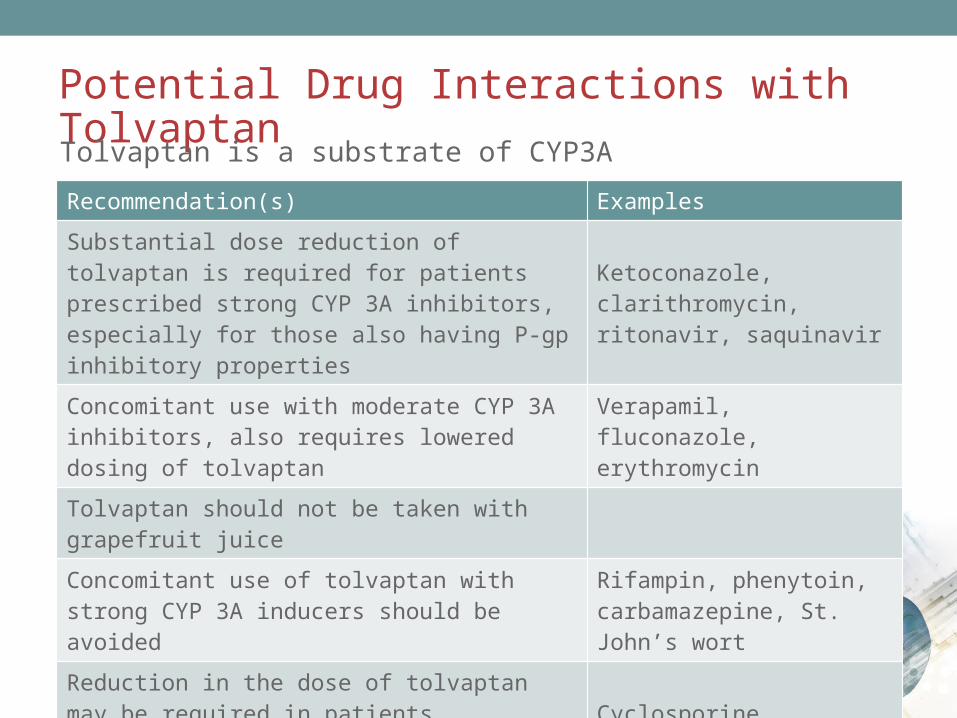
Potential Drug Interactions with TolvaptanTolvaptan is a substrate of CYP3A
Otsuka Canada Pharmaceuticals Inc. PrJINARC™ Product monograph. Date of Preparation: February 11, 2015.
Recommendation(s) Examples
Substantial dose reduction of tolvaptan is required for patients prescribed strong CYP 3A inhibitors, especially for those also having P-gp inhibitory properties
Ketoconazole, clarithromycin, ritonavir, saquinavir
Concomitant use with moderate CYP 3A inhibitors, also requires lowered dosing of tolvaptan
Verapamil, fluconazole, erythromycin
Tolvaptan should not be taken with grapefruit juice
Concomitant use of tolvaptan with strong CYP 3A inducers should be avoided
Rifampin, phenytoin, carbamazepine, St. John’s wort
Reduction in the dose of tolvaptan may be required in patients concomitantly treated with P-glycoprotein (P-gp) inhibitors
Cyclosporine, quinidine

WHAT IS THE TOLVAPTAN HEPATIC SAFETY AND MONITORING PROGRAMME (HSMP)?Dr. Navdeep Tangri
15

Key Elements of the Tolvaptan Hepatic Safety Monitoring and Distribution (HSMD) Programme
1. Restriction of prescription to physicians experienced in the diagnosis and treatment of PKD
2. Deliver tolvaptan and HSMD education to healthcare professionals
3. Patient education
4. Patient-prescriber agreement form (PPAF) prior to initiation of treatment
5. Controlled distribution of tolvaptan supply to pharmacies
6. Tracking liver enzymes and function tests
Otsuka Canada Pharmaceuticals Inc. Information on file.

Reporting LFT Result Status and Clinically Significant Elevations with Tolvaptan
• Personnel from the tolvaptan HSMD Programme will send a monthly fax to each prescriber of tolvaptan– List of all patients in the practice taking tolvaptan for ADPKD – Physician (or proxy) will need to tick off checkboxes indicating whether
or not their tolvaptan patients:
• Have done their blood work according to schedule
• Have had normal results from the liver function testing
– Completed form is to be returned by fax
Otsuka Canada Pharmaceuticals Inc. Information on file.
For more information on the tolvaptan hepatic safety monitoring and distribution programme, click here
The Patient-Prescriber Agreement Form (PPAF) for Tolvaptan in ADPKD
•When the patient and provider decide to undertake treatment with tolvaptan, a signed, duly-documented, product-specific patient-prescriber agreement(PPAF) is required
• The PPAF outlines:– Relevant patient selection criteria– Expected benefits and risks of treatment– Need for mandatory hepatic function monitoring– That tolvaptan is a long-tem therapy and avoiding
interruptions/discontinuations is recommended
Otsuka Canada Pharmaceuticals Inc. PrJINARC™ Product monograph. Date of Preparation: February 11, 2015.
HOW SHOULD WE ASSESS TOTAL KIDNEY VOLUME?Dr. Neera Dahl
16

Total Kidney Volume in ADPKD: Overview
• ADPKD is characterized by progressive cystic kidney enlargement preceding the decline in GFR by several decades
•Markers of renal function (e.g., GFR) do not accurately reflect disease progression, particularly in mild-moderate disease
• TKV increases progressively throughout the course of disease
• TKV is imperfect as a marker, but does correlate with complications of disease (e.g., hypertension, gross hematuria, microalbuminuria, proteinuria)
• To date, there is no consensus on the best method or schedule for measuring TKV

Imaging Modalities for Total Kidney Volume: Strengths and Limitations
Modality Strengths Limitations
MRI• Greatest accuracy• Method used in clinical trials
evaluating TKV
• Limited availability, long wait times• Inter-observer variability• Calculation of results is time
intensive
Ultrasound• Readily available• Short/no wait times
• Inter-observer variability• Less accurate than MRI
CT• More accurate than ultrasound• Shorter wait times than MRI
• Patient exposure to radiation• Less accurate than MRI• Inter-observer variability

WHAT IS THE LIVER TOXICITY PROFILE OF TOLVAPTAN IN ADPKD?Dr. York Pei
17
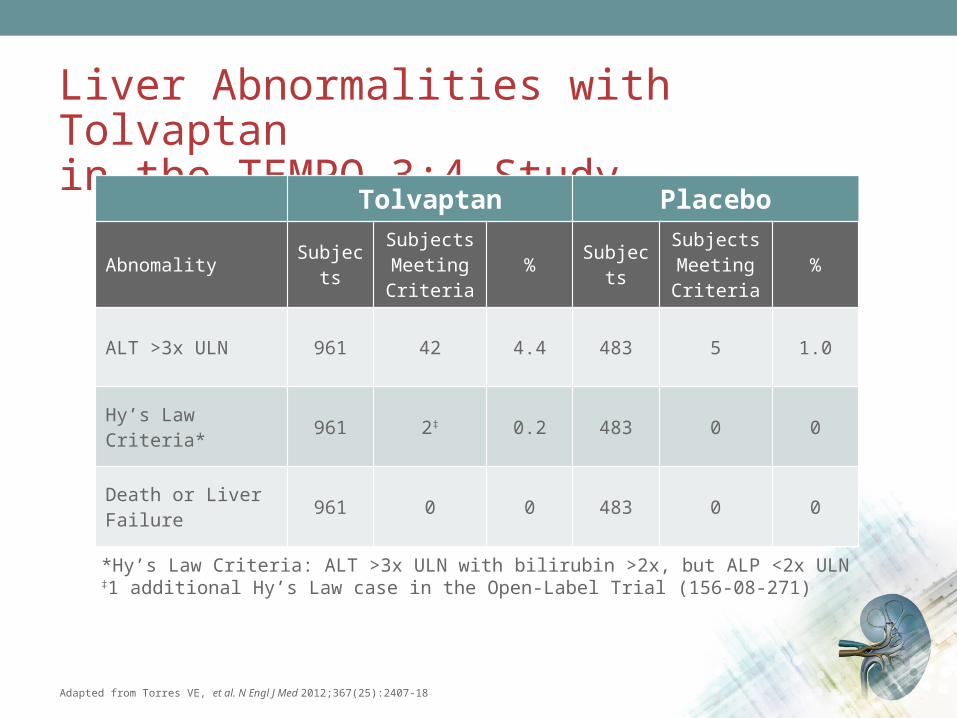
Liver Abnormalities with Tolvaptan in the TEMPO 3:4 Study
Adapted from Torres VE, et al. N Engl J Med 2012;367(25):2407-18
Tolvaptan Placebo
Abnomality SubjectsSubjects Meeting Criteria
% SubjectsSubjects Meeting Criteria
%
ALT >3x ULN 961 42 4.4 483 5 1.0
Hy’s Law Criteria* 961 2‡ 0.2 483 0 0
Death or Liver Failure 961 0 0 483 0 0
*Hy’s Law Criteria: ALT >3x ULN with bilirubin >2x, but ALP <2x ULN‡1 additional Hy’s Law case in the Open-Label Trial (156-08-271)

Time to First Elevation in ALT (>3x ULN) With Tolvaptan: 18-Month “Window of Susceptibility”
0 4 8 12 16 20 24 28 32 360.00
0.01
0.02
0.03
0.04
0.05
0.06
0.07
0.08
0.09
0.10
Prop
ortio
n of
Sub
ject
sw
ith E
leva
tion
Months in Study
Tolvaptan
Placebo
Adjudicated as Probable or Highly Likely (TLV: 16/35 in Study 251)ʺ ʺ ʺ ʺ
Hy’s Law: 156-04-251
Hy’s Law: 156-08-271 (Open-Label)
Days in Study 0 100 200 300 400 500 600 700 800 900 1000 1100
Tolvaptan N= 961 884 836 812 769 774 765 751 740 734 726 268
Placebo N= 483 476 468 459 452 445 442 433 425 422 415 147Torres VE, Chapman AB, Devuyst O, et al. N Engl J Med 2012;367(25):2407-18.
Data on file, Otsuka Pharmaceutical Canada Inc .

Warning on Hepatic Toxicity with Tolvaptan
• In clinical trials, 3 individuals experienced ALT >3x ULN with bilirubin >2x ULN– Includes 2 of 957 patients in the TEMPO study and 1 in an open-label study– All 3 returned to normal liver function after stopping tolvaptan
Otsuka Canada Pharmaceuticals Inc. PrJINARC™ Product monograph. Date of Preparation: February 11, 2015.
WARNING: IDIOSYNCRATIC HEPATIC TOXICITYTolvaptan use has led to idiosyncratic elevations of blood alanine and
aspartate aminotransferases (ALT & AST), rarely associated with concomitant elevations of total bilirubin. To help mitigate the risk of
liver injury, blood testing for hepatic transaminases is required prior to initiation of tolvaptan, then continuing monthly for 18 months, every 3 months for the next 12 months, and then every 3-6 months thereafter
during treatment with tolvaptan
WHAT IS THE PRESUMED MECHANISM OF ACTION OF TOLVAPTAN AND WHAT IS THE EVIDENCE OF EFFICACY?Dr. Navdeep Tangri
18

Mechanism of Action of JINARC™ (tolvaptan)
cAMP: adenosine 3 , 5 -cyclic monophosphate ′ ′Adapted from Otsuka Canada Pharmaceuticals Inc. PrJINARC™ Product monograph. Date of Preparation: February 11, 2015.
Administration of tolvaptan
↓ binding of vasopressin at the V2 receptor in the kidney
↓ adenylate cyclase activity
↓ intracellular cAMP concentrations
↑ in free water clearance(i.e., aquaresis)
↓ in urine osmolality ↓ rate of growth of total kidney volume
↓ rate of formation and enlargement of kidney cysts

Tolvaptan in ADPKD: Impact on TKV (TEMPO 3:4 Primary Outcome)
Adapted from Torres VE, et al. N Engl J Med 2012;367(25):2407-18
Placebo growth: 5.5%/yrTolvaptan growth: 2.8%/yrp<0.0001
Dropouts:Tolvaptan: 23.0%Placebo: 13.8%
0 4 8 12 16 20 24 28 32 36 40
-40
-20
0
20
40
60
Months12 24 36
Chan
ge in
Tot
al K
idne
y Vo
lum
e (%
)
Baseline
Tolvaptan Placebo
Tolvaptan in ADPKD: Impact on Kidney Function (TEMPO 3:4 Secondary Outcome)
Adapted from Torres VE, et al. N Engl J Med 2012;367(25):2407-18
Change in reciprocal of the sCr level:Tolvaptan: −2.61 mg/mL −1/yr Placebo: −3.81 mg/mL−1/yrp<0.001
0 4 8 12 16 20 24 28 32 36 40
-60
-40
-20
0
20
40
MonthsBaseline
Chan
ge in
Kid
ney
Func
tion
ecip
roca
l ser
um c
reati
nine
{mg/
mL}
-1) Tolvaptan Placebo
1284 242016 363228

Tolvaptan in ADPKD: Impact on Kidney Pain (TEMPO 3:4 Secondary Outcome)
Adapted from Torres VE, et al. N Engl J Med 2012;367(25):2407-18
0 4 8 12 16 20 24 28 32 360
0.1
0.2
0.3
Cum
ulati
ve E
vent
Haz
ard
Study Months
Placebo
Tolvaptan
Hazard ratio, 0.64 (95% CI, 0.47-0.89)P=0.007 by Cox model
Baseline
Tolvaptan 961 870 835 811 792 776 763 752 744 642
Placebo 483 472 463 454 446 438 428 422 418 359
No. At Risk

Tolvaptan for the Treatment of ADPKD: Conclusions on Efficacy
• In the pivotal clinical study, tolvaptan showed efficacy in:–Slows progression of increase in kidney volume
–Slows deterioration of kidney function
– Improves symptoms (e.g., pain)

Effect of Tolvaptan Across CKD Stages• Overall tolvaptan reduced
the rate of TKV growth from 5.5% per year to 2.8% per year
• Analysis by CKD subgroup showed a consistent and significant effect favoring tolvaptan
Analysis of eGFR slopes showed a statistically significant effect favoring tolvaptan in subjects in CKD stages 2 and 3

WHAT HAPPENS IF YOU STOP TOLVAPTAN THERAPY?Dr. Neera Dahl
19
What happens if you stop tolvaptan therapy?•When tolvaptan is stopped, polyuria and polydipsia return rapidly (within 24 hours) to
pre-tolvaptan values.
• Tolvaptan interruptions were discouraged during the TEMPO trial but could happen due to surgery or various concomitant diseases with a risk of acute alteration of fluid balance.
• Tolvaptan was stopped for short periods of times (less than 27 consecutive days) during the TEMPO trial and these interruptions have not been associated with untowards side effects nor with evidence of increased total kidney volume or deterioration of renal function. However, when tolvaptan is interrupted for longer durations eg. for more than a month, an increased rate of kidney volume growth is seen which returns to a slower level of growth after resuming therapy with tolvaptan. It is expected that an ADPKD patient stopping tolvaptan will have a progression of his/her kidney deterioration similar to what was happening before starting to take tolvaptan.
• Short term (7days) administration of tolvaptan has been demonstrated to decrease total kidney volume (Kidney Int. 2011 Aug; 80(3): 295–301) but there is no published data on clinical measurements obtained after stopping tolvaptan.