heamtology reviewer (midterm)
DESCRIPTION
HahahaTRANSCRIPT

Hematology (Midterm)VITAMIN B12 AND FOLIC ACID DEFICIENCY
Megaloblastic anemia Proposed early in1960’s as the
methylfolate trap Characterized by defective
synthesis in DNA Result from lack of folic acid or Vit.
B12 Macrocytic anemia(large RBCs in
the circulation) Associated with ineffective
erythropoiesis MCV> 100 fl but normal MCHC Macrocytic or normochromic Presence of megaloblast in BM and
macrocytico Due to the defective DNA
synthesis Vit B12(cobalamin and
folate deficiency Vitamin B12
o Essential nutrient consisting of tetrapyrrole(corrin) ring containing cobalt.
o Transfer of methyl group from 5-methyl THF to homocysteine
o Sources Diary product( fish,
eggs, meat) No Vit. B12 is present
in vegetables Folic acid or folate
o Used for any form of vitamin folic acid
o Synthetic form in supplement and fortified food
o Plays as an important role in metabolism of amino acids and nucleotides
o Circulate in the blood as methyl folate
o Source: green vegetables, yeast and cereals
Vit B12 Absorptiono Vit B12 transport is
mediated by three different binding protein that are capble of vinding the vitamin at its required physiological con’c
Intrinsic factor(IF) forms a protective complex with B12that is transported in the GI tract
o Transcobalamin II (TCII)- a beta- globulin produced by the liver and the dominant carrier of B12 after absorption. Also the main agent for rapid transport of Vit. B12.
o R (rapid) Proteins/ R- binders
o Transcobalamin I (TCII) - an alpha- globulin produce by granulocytes. A circulatin reserve store (methyl cobalamin) of B12.
o Transcobalamin III (C III) – also an alpha-globulin and may act as a defence by depriving pathogens of B12.
Two Mechanismso Active (75%)- requires the
presence of intrinsic factor (a glycoprotein produced by the mucosa).
o Passive – occurs by diffusion and works when pharmacological doses of vitamin B12 are ingested.
Storage siteso Total amount of vitamin in
the body is 2-5mgo Major site: livero Excreted through the bile
and shedding of intestinal epithelial cells
o Most excreted Vit. B12 is again absorbed by the
intestine. (enterohepatic circulation)
Signs and Symptomso fatigueo muscle weaknesso loss of appetite/weight losso diarrheao nauseao fast heartbeato smooth or tender tongueo tingling in hands and feeto numbness in extremities
Causes/ Individuals at Risk of Megaloblastic Anemia
Ageo -Older people >60
Family History Dietary Habits Strict vegetarian who doesn’t eat
any animal or dairy products and doesn’t take a vitamin B12 supplement
1

Hematology (Midterm) Alcoholics
Laboratory Diagnosis Screening Tests
o Complete Blood Count ↓ Hb, Hct,RBCs, WBCs,
Platelets ↑MCV, MCH ( normal
MCHC )o Morphology
Hypersegmented Neutrophils, oval macrocytes, anisocytes, poikilocytes, RBC inclusions (Howell Jolly, Cabot Rings, Basophilic Stippling)
Absolute reticulocyte count
decreased Gastric Assay
For achlorhydia (inability to produce HCl) thus dietary B12 can’t be sparated from the protein in food.
Specific TestBone Marrow Examination Asynchrony of Nucleus and
cytoplasm Hypercellular, ↑erythroppoietic
Activity, Giant metamyelocyte Chemistry Tets for serum B12 or serum folate
or RBC folate Competitive Protein- Binding Radioassay for B12 and Folate Patients B12 and folate in serum
compete with Co-labeled cobalamin and I-labeled folic acid
B12 binder: Hog IFThe Schilling Test
Measure viable IF and absorption of B12
Urinary excretion of co-labeled folic acid
To test the absorption of radiolabeled B12 in the absence and presence of orally administered IF
IF Deficiency if 2nd test is normal, B12 malabsorption if bothe tests are abnormal.
Normally 7% is excreted of the administered dose of Co-B12. 3% for Pernicious Anemia
Specific TestDeoxyuridine Suppression Test
o Very sensitiveo Defect in thymidine
synthesis either b12 or folate deficiency
Urinary Excretion of Methylmalonic Acid
o Specific test: because only B12 together with a specific
enzyme converts methylmalonic CoA to succinyl CoA
X-ray or Endoscopic Studieso This for suspected Pernicious
Anemia (PA) Bone Marrow Changes
o Markedly hypercellular o Myeloid: erythroid ratio
decreaesed or reversedo Erytropoiesis:
MEGALOBLASTIC
PERNICIOUS ANEMIA autoimmune disorder gastric atrophy of parietal cells Reduced secretion of IF (intrinsic
factor) vitamin B12 deficiency
Etiology Impaired RBC production caused
by: Cobalamin deficiency may result
from the following:o Inadequate dietary intake o Atrophy or loss of gastric
mucosa o Functionally abnormal IFo Bacterial overgrowth in
intestine
Morphology and classification Macrocytic Anemia
Improper blood cell formation
Impaired DNA synthesis
Vit. B12 deficiency Lack of intrinsic factor Inadequate diet Loss of gastric mucosa Ileal dysfunction
Pathogenesis Genetic factor
o Common blood group Ao Ancestry( Northern
European, Asean Ancestry)o Eye color (blue), white skin
complexion Autoimmune factor
o Pre-existing autoimmune disease
o Ab against parietal cells & IF Three types of Antibodies
Type 1- blocks vitamin B12 and IF binding
Type 2- prevents binding of IF- B12 complex with ileal receptors
Type 3- against specific structures in the parietal cell.
Clinical Signs & Symptoms Macrocytic anemia Glossitis Paleness of the skin
2

Hematology (Midterm) Fatigue Shortness of breath Peripheral neuropathy degeneration of spinal cord Paresthesia
o Tingling sensation due to nerve dysfunction
Screening & Confirmatory Test Ab against parietal cells & IF Endoscopy Serum B12 level- <160 ng/L CBC Count MCV- >100 fL Bone marrow examination Schilling Test
How is the test is performed?o Includes four different stages
Stage I: two doses of vit. B12 First dose: radioactive
form of Vit.B12 (mouth) Second dose: larger dose
by shot 1 hr later Urine collection over the
next 24 hrs Abnormal:
inability of PC to secrete IF Stage I is done 3- 7 days
later Stage II
First dose: Radioactive VitB12 w/ IF
o Abnormal: Proceed to Stage III
Stage III Done after taking
Antibiotics for 2 weekso May cause due to VitB12
consumption by bacteria Stage IV
Pancreatic enzyme for 3 days Followed by radioactive dose
of VitB12 Normal Results
o A normal result would require urinating eight to 40 percent of the radiolabelled vitamin B12 within 24 hours.
Abnormal Resultso Abnormal stage one and
normal stage two indicates the stomach is unable to make intrinsic factor.
BM-Megaloblasts present PS-Macrocytes are observed
o 6-lobed polymorphonuclear leukocyte is present
NON-MEGALOBLASTIC MACROCYTIC ANEMIA
Macrocytosis- due to the excess RBC membrane occurs in patient with chronic diseases.
o MCV of about 100-105 fL can occur with chronic alcohol use These are disorders in which the
macrocytosis is not primarily due
to vitamin B12 or folic acid deficiency
Here the macrocytes are “ROUND”
Related to changes owing to disruption of the cholesterol-to-phospholipid ratio
Diagnosis- CBC, RBC indices,
reticulocyte count, and peripheral smear
- Hematocrit and Hemoglobin
- Sometimes bone marrow examination
- Absence of hypersegmented neutrophils and macroovalocytes
PS- stomatocytes, reticulocytes BM- Megaloblast Iron deficiency Etiology and Morphology
- develops when the intake of iron is not enough to meet the standard level-impaired absorption-there is a chronic loss of hemoglobin in the body- gastrointestinal tract
abnormalities
IRON DEFICIENCY ANEMIA is characterized by variable degrees
of microcytosis (MCV <80 fl) and hypochromia (MCHC <32 g/dl) which results in widening of the central palor accounting for >1/3 of the total RBC diameter.
The variation in cell size results in higher RDW reflecting the fact that iron deficiency is acquired disorder with different levels of hemoglobin production in red cells.
Pathogenesis Hemoglobin synthesis is impaired
as a consequence of reduced iron supply.
There a defect in cellular proliferation.
Survival of erythroid precursors and erythrocytes is reduced
3

Hematology (Midterm)Signs and Symptoms
Fatigue and other nonspecific symptoms
Epithelial tissue Immunity and infection Pica Genitourinary system Skeletal system
Screening and confirmatory test used to determine the type of anemia
Screening Routine CBC
o If CBC findings show a hypochromic, microcytic anemia with an elevated RDW but no consistent shape changes to the RBCs patient is suspected Iron deficiency
o elevated RDW [RBC distribution width]
o RBC count & hematocrit decreases
As the hemoglobin level continues to fall, microcytosis and hypochromia become more prominent, with progressively declining values for mean cell volume (MCV), mean cell hemoglobin (MCH), and mean cell hemoglobin concentration (MCHC).
Low absolute reticulocyte count--diminished rate of effective erythropoiesis because this is a non regenerative anemia
Confirmatory testso serum iron total iron-binding
capacity (TIBC) transferrin saturation serum ferritin
Serum iron is a measure of the amount of iron bound to transferrin (transport protein) in the serum.
Principle: Serum ferric iron is first removed from attachment to transferrin by the addition of a chemical such as 0.05N hydrochloric acid.
Measurement: Spectrophotometry at 562 nm
Reference Range: 50-150 ug/dL Male-125 um/dL Female- 100 um/dLTIBC
is an indirect measure of transferrin and the available binding sites for iron in the plasma.
Principle: The concentration of transferring is measured indirectly by measuring the ability of serum transferring to bind rion.
Measurement: Spectrophotometry at 562 nm
Reference Range: 250-450 ug/dL (adult)
Transferrin saturation may only be obtained if serum iron and TIBC values are available and computed.
Principle: The percent of transferrin saturated with iron can be calculated from the total iron and the TIBC:
Transferrin saturation= Serum ironTIBC
X 100
Reference Range: 20-55% saturation
Serum ferritin is an easily accessible surrogate for stainable bone marrow iron. The iron studies are used collectively to assess the iron status of an individual. Shows that, as expected, serum ferritin and serum iron values are decreased in iron deficiency anemia, a state called sideropenia.
Measurement: Radioimmunoassays Reference range: Men: 15-200 ug/L Women: 12-150 ug/L
ADDITIONAL TEST Free erythrocyte protoporphyrin is
an early indicator of an iron metabolism disorder.
Measurement: Hematofluorometer Reference Range: <50 ug/dL Therapeutic trial of iron provides a
less invasive and less expensive diagnostic assessment
Zinc protoporphyrin is assayed fluorometrically
Peripheral blood film from a patient with hypochromic, microcytic anemia.(X1000)
Iron deficiency anaemia: peripheral blood film showing hypochromic microcytes, elliptocytes, pencil cells and fragmented cells.
(x1000) Bone marrows smear from a
patient with iron deficiency anemia. (x 1000)
Perl’s Prussian blue stain showing hemosiderin in a fragment of bone marrow. (x1000)
ANEMIA OF CHRONIC DISEASE
Anemia is commonly associated with systemic diseases, including chronic inflammatory conditions such as rheumatoid arthritis, chronic infections such as tuberculosis or human immunodeficiency virus infection, and malignancies.
4

Hematology (Midterm)
o Cartwright was the first to suggest although the underlying diseases seem quite disparate, the associated anemia may be from a single cause, proposing the concept of anemia of chronic disease. The anemia represents the most common anemia among hospitalized patients.
o Anemia of chronic inflammation is the preferred term since not all chronic diseases are associated with this form of anemia.
Cytometric classification
Normochromic, normocytic anemia (normal MCHC, normal MCV).
o These include:
o anemias of chronic diseaseo Infection (parvovirus B19)o anemia of renal diseaseo aplastic anemiao Myelophthisic anemia
Hypochromic, microcytic anemia (low MCHC, low MCV).
o These include:
o iron deficiency anemia, thalassemia
o anemia of chronic disease (rare cases)
o Sideroblastic Anemia
Normochromic, macrocytic anemia (normal MCHC, high MCV).
o These include:
Vitamin B12 deficiency Aplastic Anemia Myelodysplastic syndrome Erythroluekemia Chronic Liver disease folate deficiency and some drugs
B. Etiology
o Three Pathogenic Mechanism to explain the development of anemia during illness:
a.1 Impaired mobilization of iron Low serum iron level Decreased iron in marrow erythroid
precursor
Normal or increased iron in the marrow store
a.2. Impaired marrow response to anemia
Deficiency in erythropoietin level Response of erythroid marrow to
erythropoietin may be reduced a.3. Shortening of red cell survival Mild reduction in RBC’s life span as
a result of extra corpuscular factors including overactive histiocyte destruction of red cells.
o Factors that Contribute to the Anemia of Chronic Inflammation
Impaired Ferrokinetics
Diminished erythropoiesis and a blunted response to erythropoietin
III. Mechanism or pathogenesis of the anemia
Impaired Ferrokinetics First Acute Phase Reactant
o Role of Hepcidin Levels increase during
inflammation Hormone produced by
hepatocytes to regulate body iron levels
Interacts with ferroportin
When body iron levels decrease, hepcidin production by enterocytes decreases
Nonspecific defense against invading bacteria.
Second Phase Acute Reactant
o Lactoferrin Iron binding protein in
the granules of neutrophils.
Greater avidity in iron than transferrin
Are important intracellularly
Released in plasma during inflammation
Third Acute Phase Reactant
o Ferritin Increased levels in the
plasma bind to some iron
Unavailable for incorporation into hemoglobin
5

Hematology (Midterm) Effects: abundant in
bone marrow macrophages
release to developing erythrocyte is slowed
Diminished erythropoiesis and a blunted response to erythropoietin
IV. Definitive Signs and Symptoms
o Anemia of chronic disease is often mild. You may not notice any symptoms.
o When symptoms occur, they may include:
Feeling weak or tired Headache Paleness Shortness of breath
V. Screening and Confirmatory Tests to determine the type of anemia
Peripheral blood pictureo Mild anemiao Hemoglobin concentration-
9 to 11g/dLo Without reticulocytosis
Cells are normocytic and normochromic
o Microcytosis and hypochromia develop in about one third of patients
Leukocytosis and Thrombocytosis
Sideroblastic and Refractory AnemiaSideroblastic anemias
are iron-utilization anemias that are usually part of a myelodysplastic syndrome,
causing a normocytic-normochromic anemia with high RBC distribution width or a microcytic-hypochromic anemia, particularly with increased serum iron and ferritin and transferrin saturation.
a form of anemia in which the bone marrow produces ringed sideroblasts rather than healthy red blood cells (erythrocytes).
In sideroblastic anemia, the body has iron available but cannot incorporate it into hemoglobin, which red blood cells need to transport oxygen efficiently.
ClassificationCongenital sideroblastic anemia
Hereditary sideroblastic anemias are usually small (microcytic) and of poor color
(hypochromic) and thus must be distinguished from iron deficiency and thalassemia.
- X-linked sideroblastic anemia:
most common congenital cause of sideroblastic anemia and involves a defect in ALAS2, which is involved in the first step of heme synthesis. Although X-linked, approximately one third of patients are women due to skewed X-inactivation.
Autosomal recessive sideroblastic anemia
involves mutations in the SLC25A38 gene. \
it is involved in mitochondrial transport of glycine.
o Glycine is a substrate for
ALAS2 and necessary for heme synthesis. The autosomal
recessive form is typically severe in presentation.
Acquired clonal sideroblastic anemia Clonal sideroblastic anemias fall
under the broader category of myelodysplastic syndromes (MDS).
Three forms exist and include refractory anemia with ringed
sideroblasts (RARS), refractory anemia with ringed
sideroblasts and thrombocytosis (RARS-T),
refractory cytopenia with multilineage dysplasia and ringed sideroblasts (RCMD-RS). These anemias are associated with increased risk for leukemic evolution.
Acquired reversible sideroblastic anemia
6
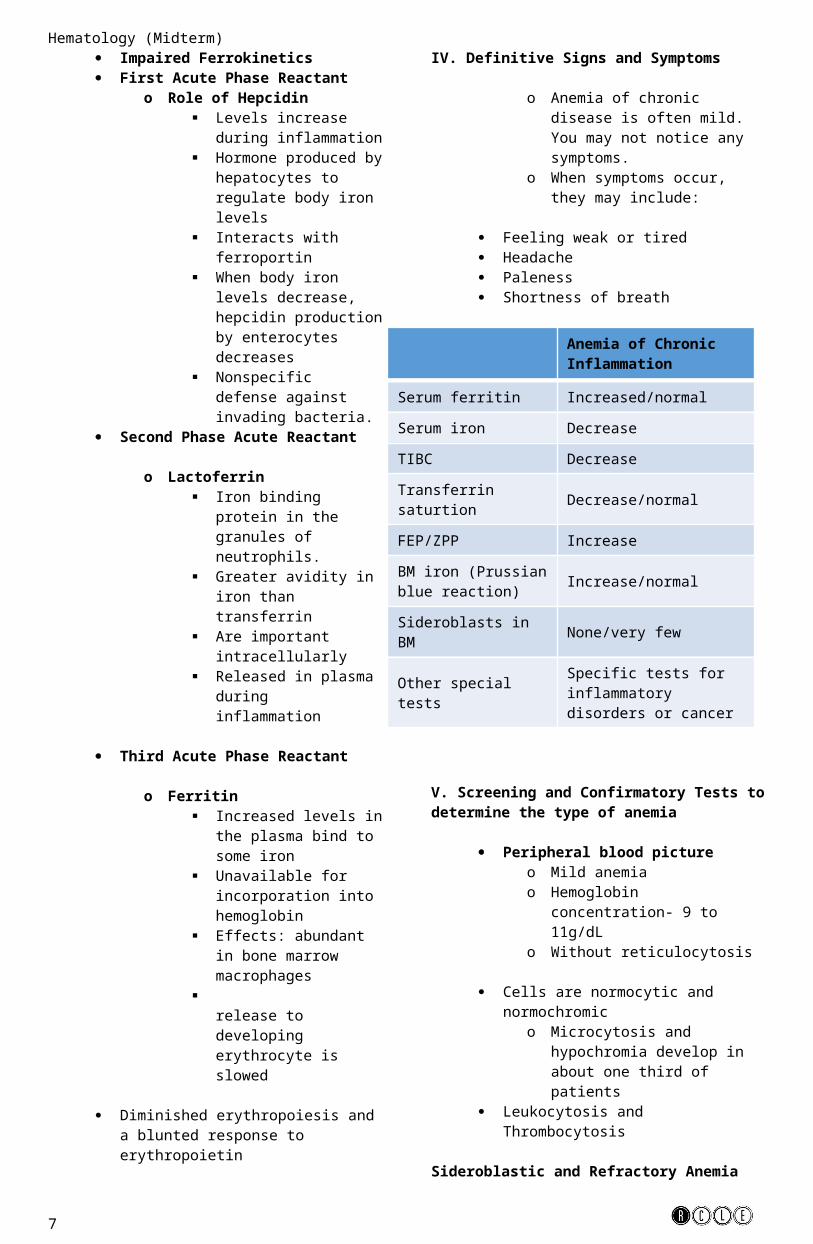
Anemia of Chronic Inflammation
Serum ferritin Increased/normal
Serum iron Decrease
TIBC Decrease
Transferrin saturtion
Decrease/normal
FEP/ZPP Increase
BM iron (Prussian blue reaction)
Increase/normal
Sideroblasts in BM None/very few
Other special testsSpecific tests for inflammatory disorders or cancer
Hematology (Midterm) Causes include excessive alcohol
use (the most common cause of sideroblastic anemia), pyridoxine deficiency, lead poisoning, and copper deficiency.
Excess zinc can indirectly cause sideroblastic anemia by decreasing absorption and increasing excretion of copper.
Antimicrobials that may lead to sideroblastic anemia include isoniazid, chloramphenicol, cycloserine, and linezolid.
Pathogenesis The process begins in the
mitochondrion with the condensation of glycine and succinyl-CoA to form delta-amino levulinic acid (ALA). Pyridoxal phosphate is a cofactor in the reaction. ALA then moves to the cytoplasm where several additional enzymatic transformations produce coproporphyrinogen III. This molecule enters the mitochondrion where additional modifications, including the insertion of iron into the protoporphyrin IX ring by ferrochelatase, produce heme. Defects in the cytoplasmic steps of heme biosynthesis cause various forms of porphyria. Functional abnormalities of the enzyme porphobilinogen deaminase, for instance, produce acute intermittent porphyria.
In contrast, defects in the steps of heme biosynthesis that occur within the mitochondrion produce sideroblastic anemias. For instance, perturbations of the enzymatic activity of delta-amino levulinic acid synthase (ALAS) produce sideroblastic anemia. The X-linked hereditary sideroblastic anemias result from mutations in the gene encoding ALA-S.
Definitive Signs and Syptoms- Skin paleness, Fatigue,
Dizziness, Enlarged spleen and liver
Screening and Confirmatory Tests Routine laboratory testing may be
used to discover incidental disease. Genetic testing provides
confirmation of the diagnosis for most patients with hereditary hemochromatosis.
Liver biopsy with assessment of iron staining and degree of scarring in liver specimens is essential to determining the degree of organ damage.
Blood Picture
o Peripheral blood smear showing many hypochromic and microcytic cells.
o Bone marrow smear showing erythroid hyper plasia, erythroblasts with defective hemoglobinization and erythroblasts containing multiple Pappenheimer bodies and most erythroid precursors are ring sideroblasts.
7
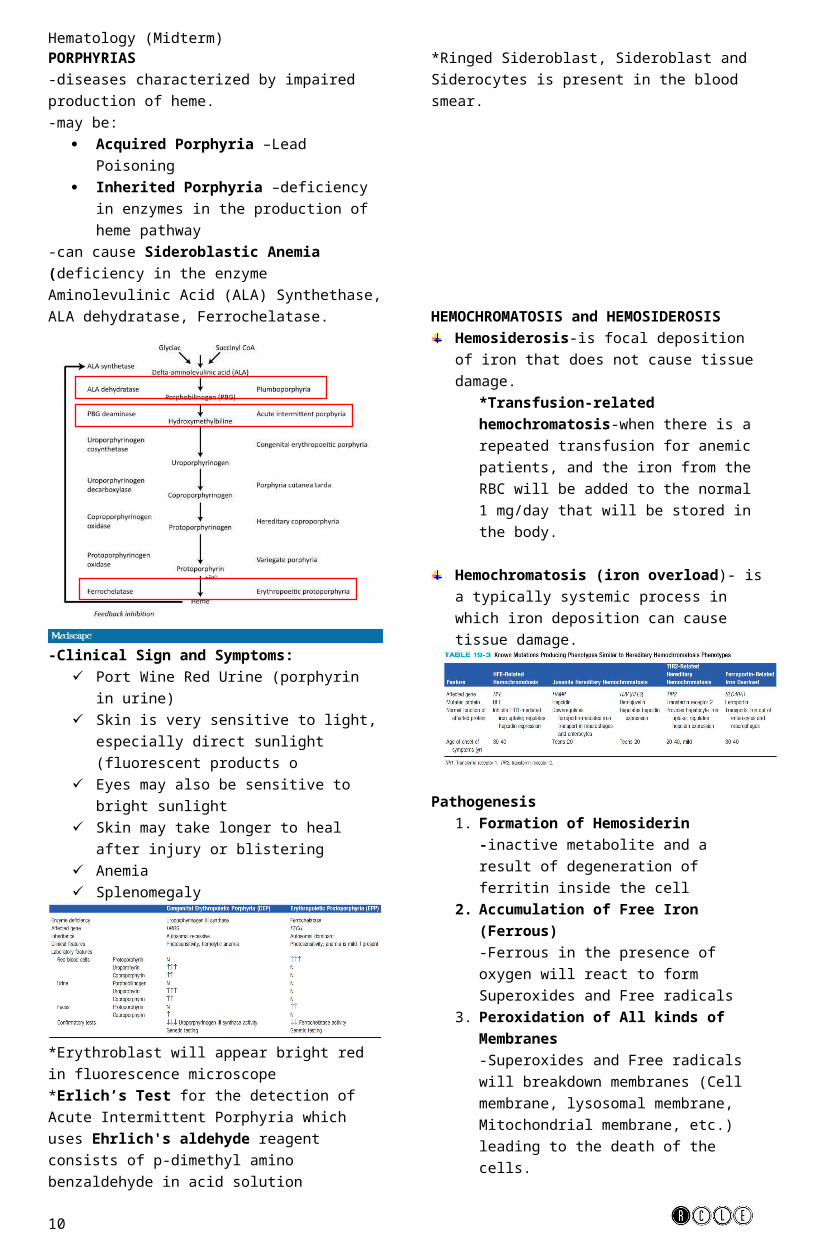
Hematology (Midterm)PORPHYRIAS-diseases characterized by impaired production of heme. -may be:
Acquired Porphyria –Lead Poisoning Inherited Porphyria –deficiency in enzymes in
the production of heme pathway-can cause Sideroblastic Anemia (deficiency in the enzyme Aminolevulinic Acid (ALA) Synthethase, ALA dehydratase, Ferrochelatase.
-Clinical Sign and Symptoms: Port Wine Red Urine (porphyrin in urine) Skin is very sensitive to light, especially direct
sunlight (fluorescent products o Eyes may also be sensitive to bright sunlight Skin may take longer to heal after injury or
blistering Anemia Splenomegaly
*Erythroblast will appear bright red in fluorescence microscope*Erlich’s Test for the detection of Acute Intermittent Porphyria which uses Ehrlich's aldehyde reagent consists of p-dimethyl amino benzaldehyde in acid solution*Ringed Sideroblast, Sideroblast and Siderocytes is present in the blood smear.
HEMOCHROMATOSIS and HEMOSIDEROSISHemosiderosis-is focal deposition of iron that does not cause tissue damage.
*Transfusion-related hemochromatosis-when there is a repeated transfusion for anemic patients, and the iron from the RBC will be added to the normal 1 mg/day that will be stored in the body.
Hemochromatosis (iron overload)- is a typically systemic process in which iron deposition can cause tissue damage.
Pathogenesis1. Formation of Hemosiderin
-inactive metabolite and a result of degeneration of ferritin inside the cell
2. Accumulation of Free Iron (Ferrous) -Ferrous in the presence of oxygen will react to form Superoxides and Free radicals
3. Peroxidation of All kinds of Membranes-Superoxides and Free radicals will breakdown membranes (Cell membrane, lysosomal membrane, Mitochondrial membrane, etc.) leading to the death of the cells.
Clinical Signs and Symptoms Golden Color Skin-hemosiderin deposition Cirrhosis-induced Jaundice in the Liver-
sometimes it could lead to cancer Bronze diabetes-Hemochromatosis in diabetic
patients (pancreas is affected) Congestive Heart Failure
Tests Transferrin Saturation-Screening Test Genetic Testing-Confirmatory Test
*Serum Ferritin is elevated in hemochromatosis
Treatment Withdrawal of Blood-for hereditary
hemochromatosis patients Iron-chelating drugs (Desferrioxamine)
-bind with excess iron then eliminated in order for the iron to not accumulate in the plasma
8

Hematology (Midterm)SICKLE CELL ANEMIA
Hemoglobin S (α2 β26GluVal )
-congenital chronic hemolysis-substitution of Glutamate to Valine in the 6th Amino acid of the Beta Globin Chain-Glutamate has a charge of (-1) and Valine has a charge of (+0), a change of (+1) charge, so that’s why Hemoglobin S migrate to other area in electrophoresis-Glutamate is polar (hydrophilic), Valine is non-polar (Hydrophobic)-has a Hb S polymer that is long and slender-low oxygen tension leads to polymerization of Hemoglobin SSickle Cells
Reversible Sickle Cells-Hb S-containing erythrocytes that change in shape in response to oxygen tension.-normal biconcave when oxygenated, and changes in shape when deoxygenated-causes vassoocclusive complication (can pass through the microvasculature because it is normal biconcave when oxygenated, and it will change shape in tissues because it will be deoxygenated)
Irreversible Sickle Cells-do not change in shape whether it will be oxygenated or not.-Elongated sickle cells with a point at each end-removed by the spleen and there is a less chance that it will enter the microcirculation and cause vasoocclusions.
Intracellular Hydration-Polymerized deoxyhemoglobin activates Psickle
membrane channel which decreases the oxygen to less than 50 mm Hg and allowing the influx of Ca2+ which will activate second membrane channel called Gardos Channel-Gardos channel stimulates the efflux of K+ and Cl-, water efflux will then follow to maintain equilibrium-Water efflux causes dehydration of the cell, thereby the HbS concentration is higher, so as a result polymerization of HbS is intensify
Pathogenesis1. Hb S in RBCS is less soluble forming
tactoids/liquid crystals that causes sickling2. Blood becomes more viscous when sickle cells
and polymers are formed3. Increase Blood viscosity cause decrease blood
flow. 4. Increase blood flow prolongs the exposure of
Hb S-containing erythrocytes to a hypoxic environment.
5. Hypoxic environment lowers pH which decreases oxygen affinity, which further promotes sickling
6. Occlusion of capillaries and arteries by sickled RBCs and infarction of surrounding tissues
Clinical Signs and Symptoms Vasoocclusion-main problem Splenomegaly due to splenic sequestration Episodes of Pain Acute chest syndrome (fever, chest pain and
presence of pulmonary infiltrates Pulmonary hypertension-fatal
Tests Peripheral Blood Smear
*Wright stain is used and the presence of a long, curved cell with a point at each end is present.*Target cell is also present
Old Screening Test*addition of sodium metabisulfite (a reducing agent) on a slide with a drop of blood, the mixture is sealed under a coverslip. Hemoglobin is reduced into its deoxygenated form, then it promote polymerization of HbS (if HbS is present), the morphology of the cell will change, and it is examine microscopically.
Hemoglobin Solubility Test-reagent used: Saponin and Sodium dithionite*Saponin-promotes lysed of RBC, releasing Hb*Dithionite-react with Hb converting it to its deoxygenated form-Deoxygenated HbS is insoluble and precipitates in the solution which causes turbidity. Normal Hb is clear
Electrophoresis*Cellulose Acetate-co-migrate with Hb D and G*Citrate Agar-migrate alone after Hb C
Treatment-Supportive Treatment
Neonatal screening Chilhood prophylactic penicillin theraphy Bone marrow transplantation Treatment with hydroxyurea
*Sickle cell trait is resistance against infection with Plasmodium falciparum.
Hemoglobin C-Harlem (C-Georgetown)-double substitution , 6th AA, Glutamate to Valine, 73rd AA, Asparagine to Aspartate-Positive in Hemoglobin Solubility Test
Hemoglobin C (α2β2 6GluLys)
-Has hemoglobin C Crystal, also known as gold bar crystals (hexagonal crystals)-produce mild hemolytic anemiaHemoglobin E (α2β2
26GluLys)Hemoglobin D (α2β2
121GluGln)Hemoglobin G (α2
68AsnLys β2)Hemoglobin O-Arab (α2β2
121GluLys)
9
Hematology (Midterm)
10
Hematology (Midterm)UNSTABLE HEMOGLOBIN VARIANTS-results from genetic mutations to globin genes creating hemoglobin products that precipitate in vivo, producing Heinz bodies causing a hemolytic anemia. -majority of these variants are β chain variants-before it was called Congenital non spherocytic hemolytic anemia or Congenital Heinz body anemia -properly called Unstable Hemoglobin disease-all patients are heterozygous because homozygous is not suitable for life-most prevalent unstable hemoglobin is Hb Köln
Causes of Hemoglobin Variants1. Substitution of a charged for an uncharged
amino acid in the interior of the molecule2. Substitution of a polar for a non polar amino
acid in the hydrophobic heme pocket3. Substitution of an amino acid in the α and β
chains at the intersubunit contact points4. Replacement of an amino acid with proline in
the α helix section of a chain5. Deletion or elongation of the primary structure
Clinical Signs and Symptoms Hemolytic Anemia Jaundice Splenomegaly Dark Urine (contains dipyrrole)
Tests Peripheral Blood Smear
-prominent basophilic stippling-Supravital stains woul dhow Heinz bodies (larger and numerous)
Electrophoresis-not detected because it migrates together with normal AA pattern
Isopropanol Precipitation Test-Isopropanol @ 37 degrees C weakens the bonding forces of the hemoglobin molecule. If unstable hemoglobins are present, rapid precipitation occurs in 5 minutes, heavy flocculation occurs after 20 minutes. *Normal hemoglobin does not precipitate until approximately 40 minutes.
Heat denaturation Test-incubation @ 50 degrees C for 1 hour. *Unstable hemoglobin show a flocculent precipitation*little or no precipitation for normal hemoglobin
High Performance Liquid Chromatography DNA-based globin gene analysis
Treatment*In severe cases, Spleen must be remove to reduce sequestration and rate of removal of RBCs
HEMOGLOBINS WITH INCREASE AND DECREASED OXYGEN AFFINITY
Recall: Deoxygenated Hemoglobin
-Tensed state-low affinity for heme ligand: oxygen-high affinity for Bohr protons and 2, 3-BPG
Oxygenated Hemoglobin-Relaxed state-high affinity for heme ligand: oxygen-low affinity for Bohr protons and 2, 3-BPG
Hemoglobins with Inceased Oxygen Affinity-Hb Abruzzo and Hb Crete-failed to release oxygen resulting to hypoxia-hypoxia triggers kidney to release erythropoietin, which leads to compensatory erythropoiesis-do not precipitate in vivo to produce hemolysis-no abnormal RBC morphology-detected by Electrophoresis using Citrate agar (pH 6.0) or by gel electrophoresis. -Oxygen Affinity measurement for definitive diagnosis-patients are usually normal and don’t require treatment
Hemoglobin with Decreased Oxygen Affinity-Hb Kansas-quickly release oxygen to the tissues, which results in normal to decreased hemoglobin concentration and slight anemia-detected by Starch gel electrophoresis, HPLC, or DNA-based globin gene analysis
THALASSEMIA-group of heterogeneous disorders in which one or more globin chains are reduced or absent
11

Hematology (Midterm)-results to hypochromic, microcytic anemia due to decreased production of hemoglobin
ALPHA THALASSEMIA-caused by a deletion of one or both of the α genes on chromosome 16, resulting in reduced or absent production of α chains-tetramers of γ chains may precipitate as Hb Bart in the fetus and newborn-tetramers of β chains may precipitate as Hb H in the adult-divided into:
o Silent carrier α-thalassemia-result of the deletion, or rarely a non deletional mutation, of one of four α genes (-α/αα) or (αTα/αα)-associated with a normal RBC profile and is asymptomatic
o α-Thalassemia minor-result of the deletion of two α genes (-α/-α) or (--/αα) -mild, asymptomatic, microcytic, hypochromic anemia, HbA2 is not elevated
o Hb H disease-result of the deletion of three of the four α genes (--/-α)-HbH inclusions (excess β chains) precipitate in older circulating RBCs, causing a hemolytic anemia-RBCs are microcytic and hypochromic, similar to β-thalassemia intermedia
o Hb Bart hydrops fetalis-result of the deletion of four of the α genes (--/--)-severe anemia in utero-incompatible with life
BETA THALASSEMIA-clinically manifested as:
o Silent Carrier State (βsilent/β)-caused by one mutated β gene that produces a small decrease in β chains. -normal blood picture
o β-Thalassemia Minor-mild, asymptomatic, microcytic, hypochromic anemia-elevated HbA2 level
o β-Thalassemia Major-severe anemia leading to transfusion dependence
o β-Thalassemia Intermedia-manifest abnormalities with a severity between those of β-Thalassemia Major and β-Thalassemia Minor
*Hb Lepore thalassemia-hereditary persistence of fetal hemoglobin
TESTS (for both α and β Thalassemia)o Complete Blood Count
-hemoglobin and hematocrit are decreased-low MCV, MCHC-RBC Distribution Width (RDW) is elevated
o Reticulocyte Count-elevatedo Bone Marrow Examinationo Osmotic Fragility Test-decreasedo Supravital Staining
*HbH inclusion-greenish blue bodieso Electrophoresis
APLASTIC ANEMIA-is a rare but potentially fatal bone marrow failure syndrome.
Acquired Aplastic Anemia-classified as idiopathic (70%) when the cause is unknown and as secondary (10%) when the cause is identified-pancytopenia is common (decrease blood cells)
Inherited Aplastic Anemia-show manifestations of the disorder at an early age and may have physical malformations.
o Fanconi Anemia- Chromosome instability disorder characterized by aplastic anemia, physical abnormalities, and cancer susceptibility.
o Dyskeratosis Congenita-bone marrow failureo Shwachman-Diamond Syndrome
-pancreatic insufficiency, cytopenia, skeletal abnormalities, and a predisposition for hematologic malignancies.
12

Hematology (Midterm)PURE RED CELL APLASIA-is a rare disorder of erythropoiesis characterized by a selective and severe decrease In erythrocyte precursors in an otherwise normal bone marrow. -characterized by severe anemia (normocytic), reticulocytopenia, and normal RBC and platelet count.
Acquired Pure Red Cell Aplasia-can be categorized into:
Primary PRCA-may be idiopathic or autoimmune related.
Secondary PRCA-may occur in association with an underlying thymoma, hematologic malignancy, solid tumor, infection, chronic hemolytic anemia, collagen vascular disease, or exposure to drugs or chemicals.
-in young children it is also known as Transient eryhtoblastopenia of childhood-Transfucions are initial therapy
Congenital Pure Red Cell Aplasia: Diamond-Blackfan Anemia-A congenital erythroid hypoplastic disorder of early infancy-mutations in genes that code for structural ribosome proteins-Mutations in these ribosomal proteins disrupt ribosome biogenesis in DBA-macrocytic anemia with reticulocytopenia-normal WBC and platelets-treatment is RBC transfusion and corticosteroids
CONGENITAL DYSERYTHROPOETIC ANEMIA (CDA)-heterogeneous group of rare disorders characterized by refractory anemia, reticyclopenia, hypercellular bone marrow with markedly ineffective erythropoiesis, and distinctive dysplastic changes in bone marrow erythroblasts. -classified into:
CDA I CDA II CDA III
MYELOPHTHISIC ANEMIA-infiltration of abnormal cells into the bone marrow and subsequent destruction and replacement of the normal hematopoietic cells.-Cytokines, growth factors, and other substances are releases that suppress hematopoiesis or destroy stem, progenitor, or stromal cells, which results in peripheral cytopenias.-if the infiltration and proliferation of the abnormal cells disrupts the normal bone marrow architecture, premature release of immature cells from the bone marrow occurs.-mild to moderate with normocytic erythrocytes and reticulocytopenia.-presence of teardrop erythrocytes and nucleated RBCs, but immature myeloid cells (leukoerythroblastic peripheral blood picture), megakaryocyte fragments, and giant platelets also may be present
ANEMIA OF CHRONIC KIDNEY DISEASES-anemia occurs in most patients with chronic kidney disease-anemia caused by inadequate production of erythropoietin by the kidneys-anemia can also be caused by Uremic toxins accumulate in the blood because of the kidney failure, and they inhibit erythropoiesis and shorten the life span of the RBCs-normocytic , normochromic Red blood cells
13