health & sanitation
TRANSCRIPT

HEALTH & SANITATION
By:
Tarushi Kulshrestha

OUTLINE Objective of study
methodology
Health
Health issues
Sanitation
Improper sanitation ;potential cause for illhealth
Waste management
conclusion
OBJECTIVE OF STUDY:
To understand the concept of health & sanitation
relation between health & sanitation
To study Health and sanitation related issues in
India

HEALTH
The general condition of a person's mind and body,
usually meaning to be free from illness, injury or pain
The World Health Organization(WHO) defined health in its
broader sense in 1946 as
“ A state of complete physical, mental, and social well-
being and not merely the absence of disease or
infirmity”
Although this definition has been subject to controversy, in
particular as lacking operational value and because of the
problem created by use of the word "complete," it remains
the most enduring.

DETERMINANTS Lifestyle: the aggregation of personal decisions (i.e., over
which the individual has control) that can be said to
contribute to, or cause, illness or death;
Environmental: all matters related to health external to
the human body and over which the individual has little or
no control;
Biomedical: all aspects of health, physical and mental,
developed within the human body as influenced by genetic
make-up.
HEALTH ISSUES IN INDIA
Child malnutrition
High infant mortality rate
Disease
Poor sanitation Safe drinking water
Female health issue
Rural health
Rural health care services
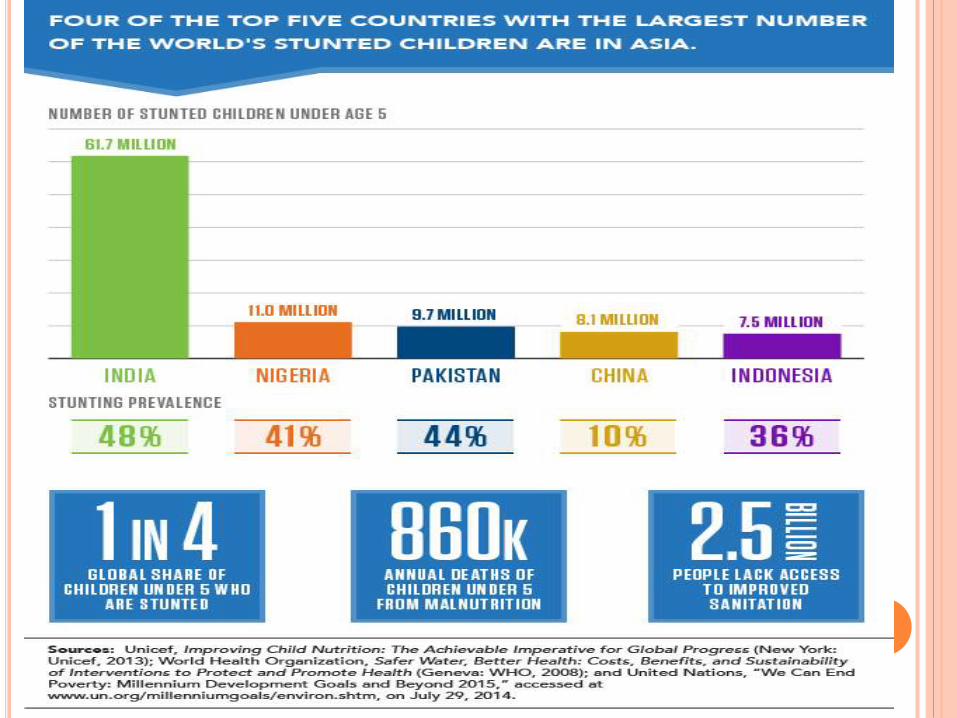
•According to a 2005 report, 42% of India’s children below the
age of three were malnourished, which was greater than the
statistics of sub-Saharan African region of 28%.
• One in every three malnourished children in the world lives in
India.The estimates varies within the country.It is estimated
that,Madhya pradesh is having the highest rate of 55 % and
Kerala the lowest with 27 %.
•Although India’s economy grew 50% from 2001–2006, its child-
malnutrition rate only dropped 1%, lagging behind countries of
similar growth rate.

CHILD MALNUTRITION
A well nourished child is one whose weight and height
measurements compare very well within the standard
normal distribution of heights and weights of healthy
children of same age and sex.
Malnutrition impedes the social and cognitive development
of a child.These irreversible damages result in lower
productivity.
hinder a child’s intellectual development.
reduces the immune defence mechanism,which heightens
the risk of infections.[
Inadequate care of these women already underdeveloped,
especially during pregnancy, leads them in turn to deliver
underweight babies who are vulnerable to further
malnutrition and disease.

DIFFERENT FORMS OF MALNUTRITION
Protein-energy malnutrition (PEM), also known as
protein-calorie malnutrition
Iron deficiency : nutritional anaemia which can lead
to lessened productivity, sometimes becoming
terminal
Vitamin A deficiency, which can lead to blindness or
a weakened immune system
Iodine deficiency, which can lead to serious mental
or physical complaints
Foliate deficiency itself can lead to insufficient birth
weight or congenital anomalies such as spina
bifida.
HIGH INFANT MORTALITY RATE
Despite health improvements over the last thirty years, lives
continue to be lost to early childhood diseases, inadequate
newborn care and childbirth-related causes. More than two
million children die every year from preventable infections.
Approximately 1.72 million children die each year before
turning one.
The under five mortality and infant mortality rates have
been declining, from 202 and 190 deaths per thousand live
births respectively in 1970 to 64 and 50 deaths per
thousand live births in 2009. However, this decline is
slowing. Reduced funding for immunization leaves only
43.5% of the young fully immunized.

DISEASES
Diseases such as dengue fever, hepatitis, tuberculosis, malaria and pneumonia continue to plague India due to increased resistance to drugs.[In 2011, India developed a totally drug-resistant form of tuberculosis.HIV/AIDS in India is ranked 3rd highest among countries with the amount of HIV-infected patients.National AIDS Control Organisation, a Government of India 'Apex Body' is making efforts for managing the HIV/AIDS epidemic in India.Diarrheal diseases are the primary causes of early childhood mortality.These diseases can be attributed to poor sanitation and inadequate safe drinking water in India.India also has the world's highest incidence of Rabies.
However in 2012 India was polio-free for the first time in its history.Thiswas achieved because of the Pulse PolioProgramme started in 1995-96 by the government of India.
Indians are also at particularly high risk for atherosclerosis and coronary artery disease. This may be attributed to a genetic predisposition to metabolic syndrome and adverse changes in coronary artery vasodilation. NGOs such as the Indian Heart Association and the Medwin Foundation have been created to raise awareness of this public health issue

POOR SANITATION & SAFE DRINKING WATER
As more than 122 million households have no toilets, 33%
lack access to latrines, over 50% of the population (638
million) defecate in the open.(2008 estimate).This is
relatively higher than Bangladesh and Brazil (7%) and
China (4%).
Although 211 million people gained access to improved
sanitation from 1990–2008, only 31% use the facilities
provided. Only 11% of Indian rural families dispose of stools
safely whereas 80% of the population leave their stools in
the open or throw them in the garbage. Open air defecation
leads to the spread of disease and malnutrition through
parasitic and bacterial infections.

POOR SANITATION & SAFE DRINKING WATER
Several million more suffer from multiple episodes of diarrhoea
and still others fall ill on account of Hepatitis A, enteric fever,
intestinal worms and eye and skin infections caused by poor
hygiene and unsafe drinking water.
Access to protected sources of drinking water has improved from
68% of the population in 1990 to 88% in 2008.
However, only 26% of the slum population has access to safe
drinking water,and 25% of the total population has drinking water
on their premises.
This problem is exacerbated by falling levels of groundwater
caused mainly by increasing extraction for irrigation.
Insufficient maintenance of the environment around water
sources, groundwater pollution, excessive arsenic and fluoride in
drinking water pose a major threat to India's health.

FEMALE HEALTH ISSUES
Maternal deaths are similarly high. The reasons for this high mortality are that few women have access to skilled birth attendants and fewer still to quality emergency obstetric care. In addition, only 15 per cent of mothers receive complete antenatal care and only 58 per cent receive iron or folate tablets or syrup.
Women's health in India involves numerous issues. Some of them include the following:
Malnutrition : The main cause of female malnutrition in India is the tradition requiring women to eat last, even during pregnancy and when they are lactating.
Breast Cancer : One of the most severe and increasing problems among women in India, resulting in higher mortality rates.
Polycystic ovarian disease (PCOD): PCOD increases the infertility rate in females. This condition causes many small cysts to form in the ovaries, which can negatively affect a woman's ability to conceive.
Maternal Mortality : Indian maternal mortality rates in rural areas are one of the highest in the world.
RURAL HEALTH CARE SERVICES
The quality of Indian healthcare is varied. In major
urban areas, healthcare is of adequate quality,
approaching and occasionally meeting Western
standards. However, access to quality medical care
is limited or unavailable in most rural
areas, although rural medical practitioners are
highly sought after by residents of rural areas as
they are more financially affordable and
geographically accessible than practitioners
working in the formal public health care sector.

SANITATION
The hygienic means of promoting
health through prevention of human contact with
the hazards of wastes as well as the treatment and proper
disposal of waste as wastes may cause health problems.

SANITATIONSanitation includes all four of these engineering
infrastructure items (even though often only the first
one is strongly associated with the term "sanitation"):
Excreta management systems
Wastewater management systems
Solid waste management systems
Drainage systems for rainwater, also called
stormwater drainage

SANITATION
Wastes include
human and animal excreta,
solid wastes,
domestic wastewater (sewage, sullage, greywater),
industrial wastes and
agricultural wastes

SANITATION
Hygienic means of prevention can be
by using engineering solutions (e.g., sewerage, wastewater treatment, storm water drainage, solid waste management, excreta management),
simple technologies (e.g., pit latrines, dry toilets, UDDTs, septic tanks),
simply by personal hygiene practices (e.g., hand washing with soap, behavior change)

Gasification Technology
Refuse Derived Fuel (RFD) Plants
Bioreactor Landfill
SANITATION A POTENTIAL CONTRIBUTOR TO
MALNUTRITION
For our nation, the issue is not a lack of food, but rather a
lack of toilets for its population—one-half of India's
population, at least 620 million people, defecates outside.
The interaction between diarrheal disease and malnutrition
is well established. Diarrhea is often caused by a lack of
clean water for proper hand-washing. A lack of toilets
further exacerbates the problem as feces on the ground
contribute to contaminated drinking water and water
resources in general.
The World Health Organization estimates that 50 percent of
malnutrition is associated with repeated diarrhea or
intestinal worm infections from unsafe water or poor
sanitation or hygiene.
COMPOSTING
long tradition particularly in rural India
difficult process because the waste arrives in a mixed form and contains a lot of non-organic material.
When mixed waste is composted, the end product is of poor quality. The presence of plastic objects in the waste stream is especially problematic, since these materials do not get recycled or have a secondary market.
The first large-scale aerobic composting plant in the country was set up in Mumbai in 1992 to handle 500 t/ day of MSW by Excel Industries Ltd.
Another plant with 150 t/day capacity has been operated in the city of Vijaywada, and
over the years a number of other plants have been implemented in the principal cities of the country such as Delhi, Bangalore, Ahmadabad, Hyderabad, Bhopal, Lucknow and Gwalior.

INCINERATION
In India the incineration is a poor option as the waste consists mainly high organic material (40–60%) and highinert content (30–50%) also low calorific value content (800–1100 kcal/kg), high moisture content (40–60%) in MSW and the high costs of setting up and running the plants .
The first large-scale MSW incineration plant was constructed at Timarpur, New Delhi in 1987 with a capacity of 300 t/day and a cost of Rs. 250 million (US$5.7 million) by Miljotecknik volunteer, Denmark. The plant was out of operation after 6 month and the Municipal Corporation of Delhi was forced to shut down the plant due to its poor performance.
Small incinerators, in many cities in India, are being used for burning hospital waste however
GASIFICATION TECHNOLOGY
Gasification is the solid waste incineration under oxygen deficient
conditions, to produce fuel gas.
In India,there are very few gasifiers in operation, but they are
mostly for burning of biomass such as agro-residues, sawmill
dust, and forest wastes.
Gasification can also be used for MSW treatment after drying,
removing the inert and shredding for size reduction.
Gasification unit installed at Gaul Pahari campus, New Delhi by
Tata Energy Research Institute (TERI) and other is installed at
Nohar, Hanungarh, Rajasthan by Narvreet Energy Research and
Information (NERI) for the burning of agro-wastes, sawmill dust,
and forest wastes.
The waste-feeding rate is about 50–150 kg/h and its efficiency
about 70–80%. About 25% of the fuel gas produced may be
recycled back into the system to support the gasification process,
and the remaining is recovered and used for power generation

REFUSE DERIVED FUEL (RFD) PLANTS
It produces an improved solid fuel or pellets from MSW.
The RDF plant reduces the pressure on landfills.
Combustion of the RDF from MSW is technically sound and
is capable of generating power.
RDF may be fired along with the conventional fuels like coal
without any ill effects for generating heat.
Operation of the thermal treatment systems involves not
only higher cost, but also a relatively higher degree of
expertise.
Many RDF plants are in operation in India, in Bangalore
RFD plant ,The RDF plant at Deonar, Mumbai ,The
Hyderabad RDF plant
The RDF production is about 210 t/day as fluff and pellets,
and it is going to be used for producing power (about 6.6
MW)

LANDFILLING A landfill is an area of land onto or into which waste is deposited. The aim is to avoid
any contact between the waste and the surrounding environment, particularly the groundwater.
In India open, uncontrolled and poorly managed dumping is commonly practiced, giving rise to serious environmental degradation.
60%- 90% of MSW in cities and towns are directly disposed of on land in an unsatisfactory manner.
Rainy season. Worsens the situation
The pollution of groundwater, though largely unassessed, is definitely a threat posed by the dumping of wastes. Such dumping activity in many coastal towns has led to heavy metals rapidly leaching into the coastal waters. The
daily cover techniques are poor, which makes leakage easier. This is mainly because of a lack of knowledge and
skill on the part of the local authorities. This forces local authorities to curtail the implementation of even known
precautions and practices. However, it appears that landfilling would continue to be the most widely adopted
practice in India in the coming few years, during which certain improvements will have to be made to ensure the
sanitary landfilling, even though the major cities like Delhi, Mumbai, Kolkata and Chennai are facing the
problem of the limited availability of land for waste disposal

BIOREACTOR LANDFILL
constructed and operated to optimise moisture content and increase the rate of anaerobic biodegradation.
Theprincipal function that distinguishes bioreactor landfills from conventional landfills is leachate recirculation.
The goal is to increase the rate of bio-degradation to achieve maximum gas generation rate and output so as to
optimise recovery for energy production. This approach also aims to minimise the landfill stabilisation time and
reduce the period of monitoring and liability retention. The bioreactor option is a direct result of engineering and
building a new generation of environmentally sound landfills; it provides environmental security while
permitting and encouraging rapid stabilization of the readily and moderately decomposable organic waste
components

Source: Information from web site of CPCB The Central Pollution Control Board

MSW is usually disposed as it is without any
treatment. Most of MSW is still disposed off in
dumps causing
severe environmental and health risks. The
progress in moving towards sanitary landfills and/or
disposing
through well designed and well operated
incinerators is rather slow.
Municipal Solid Waste Management in India-Current State and Future Challenges: A Review



Source:report of steering committee on health for 12th five year plan

Source:report of steering committee on health for 12th five year plan
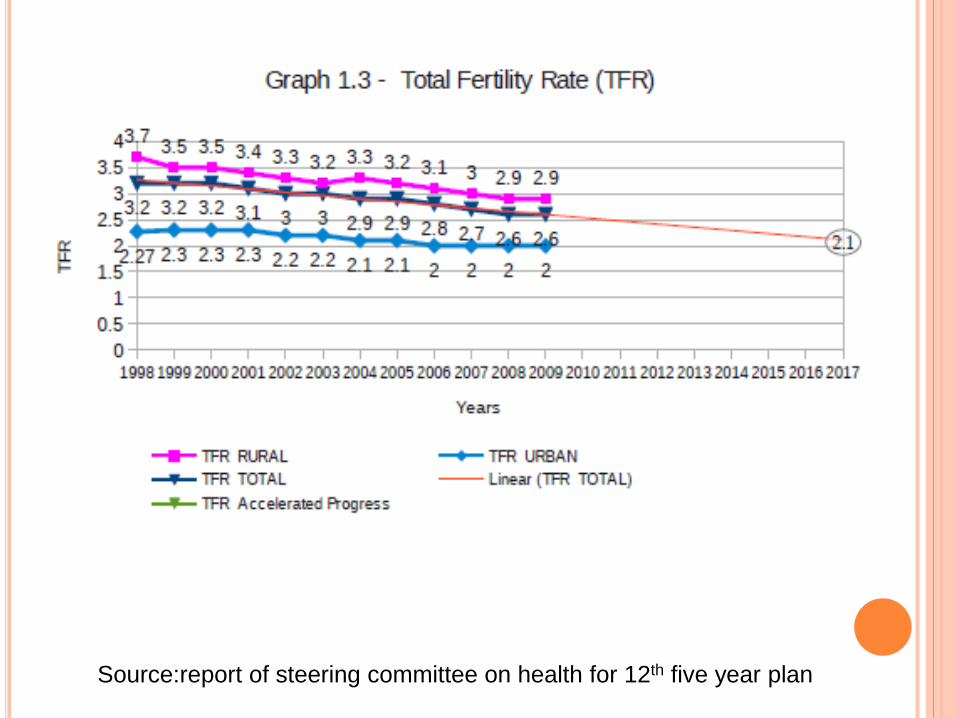
Source:report of steering committee on health for 12th five year plan

Source:report of steering committee on health for 12th five year plan

Source:report of steering committee on health for 12th five year plan
MORE THAN 50% OF MATERNAL & CHILD DEATHS
TAKE PLACE IN STATES LIKE BIHAR,
JHARKHAND,ASSAM,UTTAR PRADESH, MADHYA
PRADESH, CHATTISGARH,ORISSA & RAJASTHAN

Source:report of steering committee on health for 12th five year plan

THE VERY HIGH RATE OF URBANISATION COUPLED WITH
IMPROPER PLANNING AND POOR FINANCIAL CONDITION HAS
MADE PROPER SANITATION IN INDIAN CITIES A HERCULEAN
TASK.
India, with a population of over 1.21 billion account for 17.5%
of the world population (Census of India 2011)
Urban agglomerations
Cities Population
Greater Mumbai 18.4 Millions
Delhi UA 16.3 Millions
Delhi UA 14.1 Millions
Chennai UA 8.7 Millions
Bangalore UA 8.5 Millions
Source: censusindia.gov.in/2011-Documents/UAs-Cities-Rv.ppt

CONCLUSION:
Awareness and education is the major tool to
overcome health and sanitation issues.
Proper and improved sanitation will eradicate major
health concerns
Healthy mind lives in healthy body and healthy
mind ensures happy living and progress.