guidelines for the management of insomnia may 2017 for the... · 1.1.2 insomnia can be classified...
TRANSCRIPT

GUIDELINES FOR THE MANAGEMENT OF INSOMNIA MAY 2017
This policy supersedes all previous policies relating to Insomnia
Guidelines for the management of insomnia_PHA08_May 2017 i
Policy title GUIDELINES FOR THE MANAGEMENT OF INSOMNIA
Policy reference
PHA08
Policy category CLINICAL
Relevant to All CLINICAL STAFF IN THE TRUST
Date published May 2017
Implementation date
May 2017
Date last reviewed
February 2017
Next review date
March 2019
Policy lead LUCY REEVES, Chief Pharmacist
Contact details Email: [email protected] Telephone:
Accountable director
DR VINCENT KIRCHNER, ACTING MEDICAL DIRECTOR
Approved by
Drugs and Therapeutics Committee February 2017
Approved by (Committee):
Quality committee 16 May 2017
Document history
Date Version Summary of amendments
Feb 2017 6 Melatonin restricted for sleep disorders in patients with learning disabilities.
Feb 2015 5 Use of hypnotics in medical conditions, tapering schedules, driving offence
Mar 2014 4 What is not recommended
Mar 2012 3 Zopiclone has been included as a first line hypnotic
Mar 2010 2 Review
Dec 2007 1 New Guidelines
Membership of the policy development/ review team
AUDREY COKER, LEAD PHJARMACIST FOR CLINICAL SERVICES.
Consultation
Dr Lucinda Donaldson, Consultant for Perinatal Services, Dr Gina Waters Consultant for Perinatal Services.
DO NOT AMEND THIS DOCUMENT
Further copies of this document can be found on the Foundation Trust intranet.

Guidelines for the management of insomnia_PHA08_May 2017 ii
Contents Page
1 Introduction 1
2 Aims and objectives 2
3 Scope of the policy 2
4 Key points 2
5 Assessment of insomnia 3
6 Promote sleep hygiene principles 5
7 Treatment of insomnia 6
8 Monitoring 9
9 Melatonin 10
10 Dissemination and implementation arrangements 10
11 Training requirements 10
12 Monitoring and audit arrangements 10
13 Review of the policy 11
14 References 11
Appendix 1: Algorithm for the assessment and management of transient
/short term insomnia.
13
Appendix 2: Medicines for which management of insomnia would be a
non-formulary indication as a main indication.
16
Appendix 3 How to manage withdrawal of long-term benzodiazepine
and z-hypnotic use
18
Appendix 4: Equality impact assessment tool 19
Guidelines for the management of insomnia_PHA08_May 2017 1
1 INTRODUCTION
1.1.1 Insomnia is a condition of unsatisfactory sleep, either in terms of sleep onset, sleep maintenance or early waking. Insomnia impairs daytime well-being and subjective abilities and functioning, and so can be considered a ‘24-hour’ disorder. It is important to recognize that insomnia is a subjective disorder, and its diagnosis is through clinical observations rather than via measurements. However, in some cases it may be possible to identify and remedy a physical cause for insomnia. Insomnia often starts with a specific problem, for example a stressful life event such as the loss of a job or change to a more demanding one, or through something that changes sleep patterns such as the birth of a child or starting shift work. In some people this acute insomnia persists into a chronic state. Factors involved in the persistence of insomnia are not fully established, but include anxiety about sleep, maladaptive sleep habits and the possibility of an underlying vulnerability in sleep-regulating mechanisms. Persistence of the precipitating stressor can also contribute. Some cases of insomnia are precipitated by, or are co-morbid with, other psychiatric disorders, especially anxiety and depression, or by physical illness such as cancer or arthritis. The nature of sleep changes with age. Older age is associated with poorer objectively measured sleep with shorter sleep time, diminished sleep efficiency, and more arousals, and these changes may be more marked in men than in women1.
1.1.2 Insomnia can be classified according to cause:
Transient insomnia may occur in those who normally sleep well and may be due to an alteration in the conditions that surround sleeping e.g. noise, or to an unusual pattern of rest e.g. shift work or travelling between time zones (jet lag)2. It may also be associated with acute disorders. It may only be short term, lasting between 1-4 weeks.
Primary insomnia is insomnia that occurs when no co-morbidity is identified. Commonly the person has conditioned or learned sleep difficulties with or without heightened arousal in bed. Typically primary insomnia has a duration of at least one month3.
Comorbid (or secondary) insomnia is when insomnia occurs as a symptom of or is associated with other conditions including medical or psychiatric illness or drug or substance misuse3.
1.1.3 Insomnia can also be categorised according to duration or likely duration. Whilst definitions can vary, insomnia is categorised as:
Short-term if insomnia lasts between one to four weeks3.
Long-term (or persistent) if insomnia lasts for four weeks or longer3.
Part of a state of high arousal secondary to severe psychiatric disturbance.
1.1.4 The underlying cause of insomnia also needs to be identified and corrected whenever possible. Relatively short-term insomnia may be helped by a very limited course of a benzodiazepine or other hypnotic medicine, but is more usually managed without hypnotics. Long-term use of hypnotic medication is not justified and may be hazardous or itself be the cause of sleep problems. In chronic insomnia, physical or psychiatric causes should be considered especially in the elderly.

Guidelines for the management of insomnia_PHA08_May 2017 2
2 AIMS AND OBJECTIVES
2.1.1 To provide clear guidance on the appropriate and safe use of medication to control insomnia.
3 SCOPE OF THE GUIDELINE
3.1.1 The guideline covers both the benzodiazepine hypnotics and z-hypnotics. It is aimed at all clinical staff working in Camden and Islington NHS Foundation Trust.
3.1.2 This guideline relates to pharmacological management of insomnia. The guideline is only concerned with prescribing benzodiazepines for the treatment of insomnia. Their role in anxiety management is NOT within the scope of this document.
4 KEY POINTS
Table 1: Medicine choice in the management of insomnia
Options Medicine choice Comments First line Zopiclone 3.75mg tablets, 7.5mg tablets. Sch 4 CD
Second line Temazepam 10mg, 20mg tablets, liquid 10mg in 5ml. Sch 3 CD.
Third line Zolpidem 5mg tablets, 10mg tablets
Pregnant women
Promethazine NICE CG 192. Off-label.
4.1.1 Inpatients should not routinely be written up for hypnotics. This is rarely necessary and may establish a need to continue afterwards.
4.1.2 With increased awareness of the problems of benzodiazepine dependence, proper use and careful patient selection is essential. See Appendix 1 for ‘How to manage withdrawal of long-term benzodiazepine and z-hypnotic use’.
CSM ADVICE2
1. Benzodiazepines are indicated for the short-term relief (two to four weeks only) of
anxiety that is severe, disabling or subjecting the individual to unacceptable distress,
occurring alone or in association with insomnia or short-term psychosomatic, organic or
psychotic illness.
2. The use of benzodiazepines to treat short – term ‘mild’ anxiety is inappropriate and
unsuitable.
3. Benzodiazepines should be used to treat insomnia but only when it is severe,
disabling or subjecting the individual to extreme stress.
CSM ADVICE
Guidelines for the management of insomnia_PHA08_May 2017 3
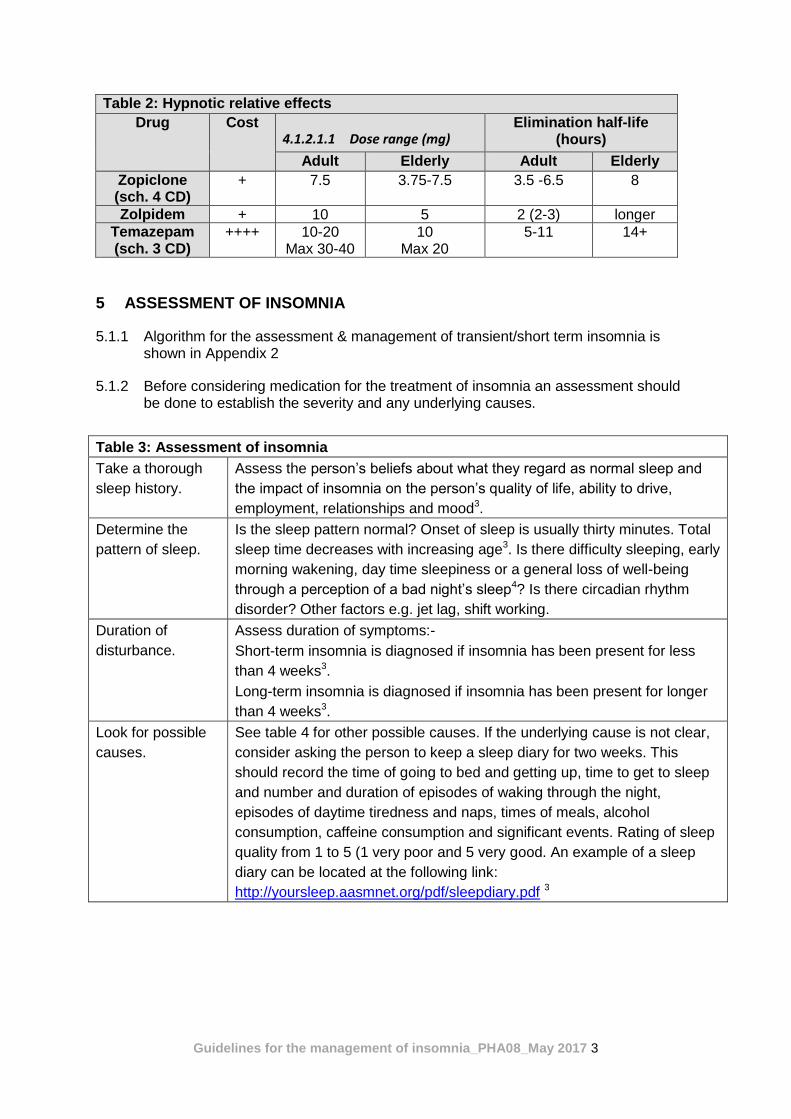
Table 2: Hypnotic relative effects
Drug Cost 4.1.2.1.1 Dose range (mg)
Elimination half-life (hours)
Adult Elderly Adult Elderly
Zopiclone (sch. 4 CD)
+ 7.5 3.75-7.5 3.5 -6.5 8
Zolpidem + 10 5 2 (2-3) longer
Temazepam (sch. 3 CD)
++++ 10-20 Max 30-40
10 Max 20
5-11 14+
5 ASSESSMENT OF INSOMNIA
5.1.1 Algorithm for the assessment & management of transient/short term insomnia is shown in Appendix 2
5.1.2 Before considering medication for the treatment of insomnia an assessment should be done to establish the severity and any underlying causes.
Table 3: Assessment of insomnia
Take a thorough
sleep history.
Assess the person’s beliefs about what they regard as normal sleep and
the impact of insomnia on the person’s quality of life, ability to drive,
employment, relationships and mood3.
Determine the
pattern of sleep.
Is the sleep pattern normal? Onset of sleep is usually thirty minutes. Total
sleep time decreases with increasing age3. Is there difficulty sleeping, early
morning wakening, day time sleepiness or a general loss of well-being
through a perception of a bad night’s sleep4? Is there circadian rhythm
disorder? Other factors e.g. jet lag, shift working.
Duration of
disturbance.
Assess duration of symptoms:-
Short-term insomnia is diagnosed if insomnia has been present for less
than 4 weeks3.
Long-term insomnia is diagnosed if insomnia has been present for longer
than 4 weeks3.
Look for possible
causes.
See table 4 for other possible causes. If the underlying cause is not clear,
consider asking the person to keep a sleep diary for two weeks. This
should record the time of going to bed and getting up, time to get to sleep
and number and duration of episodes of waking through the night,
episodes of daytime tiredness and naps, times of meals, alcohol
consumption, caffeine consumption and significant events. Rating of sleep
quality from 1 to 5 (1 very poor and 5 very good. An example of a sleep
diary can be located at the following link:
http://yoursleep.aasmnet.org/pdf/sleepdiary.pdf 3
Guidelines for the management of insomnia_PHA08_May 2017 4
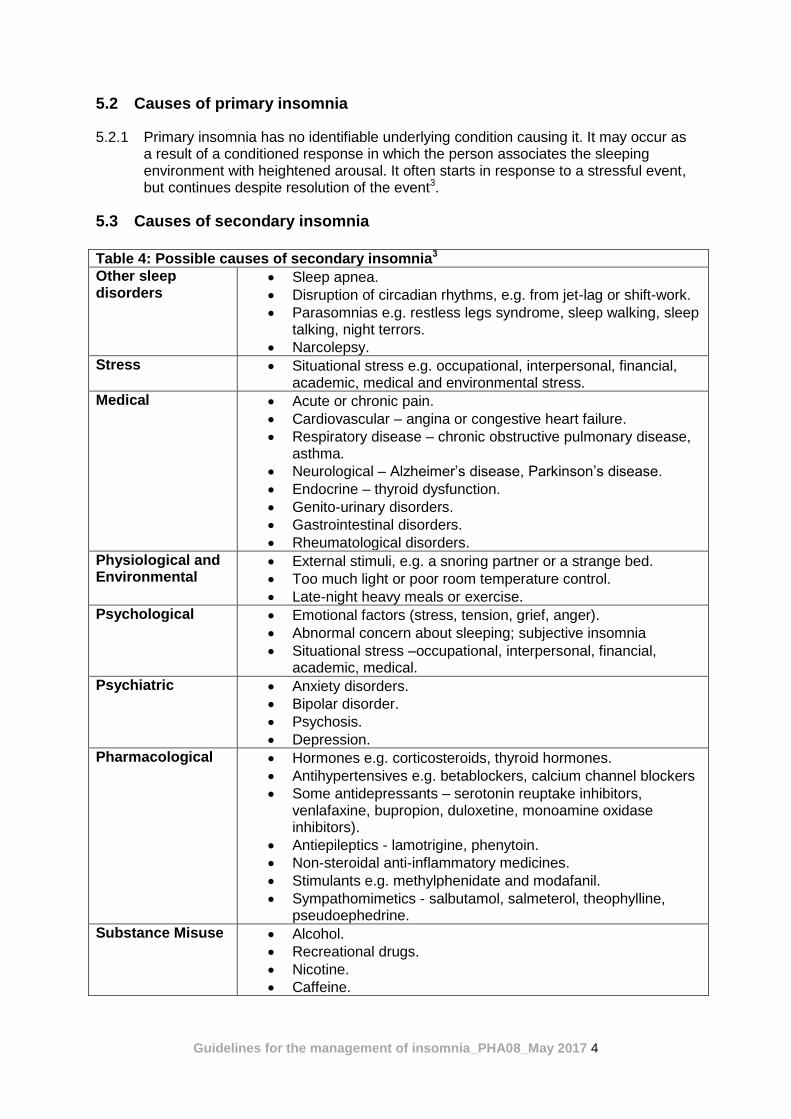
5.2 Causes of primary insomnia
5.2.1 Primary insomnia has no identifiable underlying condition causing it. It may occur as a result of a conditioned response in which the person associates the sleeping environment with heightened arousal. It often starts in response to a stressful event, but continues despite resolution of the event3.
5.3 Causes of secondary insomnia
Table 4: Possible causes of secondary insomnia3
Other sleep disorders
Sleep apnea.
Disruption of circadian rhythms, e.g. from jet-lag or shift-work.
Parasomnias e.g. restless legs syndrome, sleep walking, sleep talking, night terrors.
Narcolepsy.
Stress Situational stress e.g. occupational, interpersonal, financial, academic, medical and environmental stress.
Medical Acute or chronic pain.
Cardiovascular – angina or congestive heart failure.
Respiratory disease – chronic obstructive pulmonary disease, asthma.
Neurological – Alzheimer’s disease, Parkinson’s disease.
Endocrine – thyroid dysfunction.
Genito-urinary disorders.
Gastrointestinal disorders.
Rheumatological disorders.
Physiological and Environmental
External stimuli, e.g. a snoring partner or a strange bed.
Too much light or poor room temperature control.
Late-night heavy meals or exercise.
Psychological Emotional factors (stress, tension, grief, anger).
Abnormal concern about sleeping; subjective insomnia
Situational stress –occupational, interpersonal, financial, academic, medical.
Psychiatric Anxiety disorders.
Bipolar disorder.
Psychosis.
Depression.
Pharmacological
Hormones e.g. corticosteroids, thyroid hormones.
Antihypertensives e.g. betablockers, calcium channel blockers
Some antidepressants – serotonin reuptake inhibitors, venlafaxine, bupropion, duloxetine, monoamine oxidase inhibitors).
Antiepileptics - lamotrigine, phenytoin.
Non-steroidal anti-inflammatory medicines.
Stimulants e.g. methylphenidate and modafanil.
Sympathomimetics - salbutamol, salmeterol, theophylline, pseudoephedrine.
Substance Misuse Alcohol.
Recreational drugs.
Nicotine.
Caffeine.
Guidelines for the management of insomnia_PHA08_May 2017 5
6 PROMOTE SLEEP HYGIENE PRINCIPLES
6.1.1 Sleep hygiene aims to make people more aware of behavioural, environmental and temporal factors that may be detrimental or beneficial to sleep. Advise the person to:
Establish fixed times for going to bed and waking up (and avoid sleeping in after a poor night’s sleep)3.
Try to relax before going to bed3.
Maintain a comfortable sleeping environment not too hot, cold, noisy or bright3.
Avoid napping during the day3.
Avoid caffeine, nicotine and alcohol within six hours of going to bed3.
Consider complete elimination of caffeine from the diet3.
Avoid exercise before bedtime (although exercise earlier in the day is beneficial.
Avoid eating a heavy meal late at night3.
Avoid watching or checking the clock throughout the night3.
Only use the bedroom for sleep or sexual activity3.
Have a copy of the sleep hygiene leaflet from the Choice and Medication leaflet - http://www.choiceandmedication.org/candi/pdf/handyfactsheetsleephygiene.pdf
6.1.2 CBT (Cognitive Behavioural Therapy) for insomnia can be provided by psychologists to patients being referred to them6.
7 TREATMENT OF INSOMNIA
7.1 Initiation
7.1.1 All patients should have an objective assessment of their sleep documented on sleep charts/diary. Consideration of the cause of the insomnia should be made2.
7.1.2 Information and advice on sleep hygiene3 should be the norm and may in many cases prevent the need to prescribe hypnotics. Indiscriminate and routine use of hypnotics is not recommended2.
7.1.3 Hypnotics should be reserved for short courses in the acutely distressed. Tolerance to their effects develops within 3-14 days of continuous use and long-term efficacy cannot be assured. A major drawback of long-term use is that withdrawal can cause rebound insomnia and a withdrawal syndrome2.
7.1.4 Ensure where possible any current sedative medicines are prescribed at night and medicines likely to disturb sleep are prescribed during the day.
7.1.5 Advise the person not to drive while taking the medicine until they know how it affects them (especially just after starting or changing the dose). It is against the law to drive if your driving ability is impaired by this medicine 7
7.1.6 Z-hypnotics are recommended by NICE for the short-term management of severe insomnia that interferes with normal daily life and should be prescribed for short periods2. Zopiclone is 1st line hypnotic in the Trust, whilst temazepam is second –
Guidelines for the management of insomnia_PHA08_May 2017 6
line. Zolpidem is included as a third-line agent, however it is contraindicated in patients with a psychotic illness2.
7.1.7 Use the lowest effective dose4,8.
7.1.8 Use intermittent dosing (alternate nights or less) where possible4.
7.1.9 If prescribed on the ‘as required’ side of the prescription chart hypnotics should not be administered routinely to patients at a set time, but must be timed to the normal time the patient retires to bed.
7.1.10 Prescribe for short-term use (no more than four weeks) in the majority of cases4,8.
7.1.11 Be alert for rebound insomnia/withdrawal symptoms4.
7.1.12 Advise patients of the interaction with alcohol and other sedating medicines4,8.
7.2 Cautions
7.2.1 For further information check the specification of product characteristics or contact the Pharmacy department for advice.
7.2.2 Avoid the use of hypnotics in patients with respiratory disease or severe hepatic impairment and addiction-prone individuals4.
7.2.3 Z-hypnotics in hepatic impairment:
Zopiclone – can precipitate coma. Reduce the dose. Avoid in severe impairment2.
Zolpidem – can precipitate coma. Reduce the dose to 5mg. Avoid in severe impairment2.
7.2.4 Z-hypnotics in renal impairment:
Zopiclone – start with small doses in severe impairment. Increased cerebral sensitivity.
Zolpidem – Use with caution.
7.2.5 Benzodiazepines in hepatic impairment: benzodiazepines can precipitate coma if used in hepatic impairment. If treatment is necessary, temazepam has a shorter half-life compared to some other benzodiazepines. Smaller doses should be initiated and avoid in severe impairment2.
7.2.6 Benzodiazepines in renal impairment: patients with renal impairment have increased cerebral sensitivity to benzodiazepines. Smaller doses should be started in severe impairment2.

Guidelines for the management of insomnia_PHA08_May 2017 7
7.3 Pregnancy and Breastfeeding
Non-medicine measures are preferred4.
For patients with serious and chronic problems, promethazine may be considered9.
7.3.1 Z-hypnotics in pregnancy:
Zopiclone- avoid regular use (risk of neonatal withdrawal symptoms). High doses during late pregnancy or labour may cause neonatal hypothermia, hypotonia and respiratory depression2.
Zolpidem – avoid especially in the first trimester5. Avoid regular use (risk of neonatal withdrawal symptoms). High doses during late pregnancy or labour may cause neonatal hypothermia, hypotonia and respiratory depression2.
7.3.2 Z-hypnotics in breast-feeding:
Zopiclone – present in milk – avoid2.
Zolpidem – small amounts present in milk – avoid2.
7.3.3 Benzodiazepines in pregnancy: there is a risk of neonatal withdrawal symptoms when benzodiazepines are used in late10 pregnancy and use should be avoided. High doses administered during late pregnancy or labour may cause neonatal hypothermia, hypotonia and respiratory depression2. Temazepam should be avoided especially in the first and third trimester11. Evidence for teratogenicity is unconfirmed. First trimester exposure to benzodiazepines has been associated with increased risk of oral clefts in newborns, although one study failed to confirm this association. Benzodiazepines have also been associated with pylorostenosis and alimentary tract atresia, but a replication of these finds is required 4.
7.3.4 Benzodiazepines in breast-feeding: Benzodiazepines are present in milk and should be avoided if possible2.
7.4 Short-term insomnia (<4 weeks)
7.4.1 Consider a short course of a hypnotic only if day time impairment is severe2 on an ‘as required’ basis.
7.4.2 Use the lowest effective dose for the shortest period possible. The exact duration would depend on the underlying cause, but treatment should not be continued for longer than two weeks3.
7.4.3 Advise the person further prescriptions for hypnotics will not usually be given, ensure the reasons for this is understood and document in the person’s notes. Do not issue out further prescriptions without seeing the person again3.
7.4.4 If there is no response to the first hypnotic, do not prescribe another3.
7.4.5 If the person experiences adverse effects considered to be directly related to the hypnotic, consider switching to another3.
7.4.6 Review after two weeks and consider referral for cognitive behavioural therapy if symptoms persist3.

Guidelines for the management of insomnia_PHA08_May 2017 8
7.4.7 Diazepam is not generally recommended, but it can be useful if insomnia is associated with day time anxiety2,3.
7.5 Long-term insomnia (>4weeks)3
7.5.1 Advise on good sleep hygiene and regular exercise3.
7.5.2 Refer to psychological services (Improving Access to Psychological Therapies) for cognitive or behavioural intervention3.
7.5.3 Pharmacological management is generally not recommended for the long-term management of insomnia. However for people with severe symptoms or an acute exacerbation of persistent insomnia, a short course of a hypnotic may be considered for immediate relief of symptoms3 on an ‘as required’ basis.
7.5.4 Use the lowest effective dose for the shortest period possible. The exact duration would depend on the underlying cause, but treatment should not be continued for longer than two weeks3. Up to four weeks may occasionally be required, but continued use should always be re-assessed after two weeks3.
7.5.5 Advise the person further prescriptions for hypnotics will not usually be given, ensure the reasons for this is understood and document in the person’s notes. Do not issue out a further prescriptions without seeing the person again3.
7.5.6 Hypnotics are not recommended for long-term use as there are concerns regarding their safety. Potential adverse events include day time sedation, poor coordination, cognitive impairment and related concerns about risk of driving accidents and falls. Long-term use of hypnotics can lead to the development of tolerance, physical and behavioural dependence, adverse effects on withdrawal, rebound insomnia and increased mortality3.
7.5.7 Use caution when prescribing hypnotics for older people3.
8 MONITORING
8.1.1 As benzodiazepines and z-hypnotics cause drowsiness and increase the effects of alcohol, patients should be advised not to drink alcohol5. If a patient appears intoxicated (with alcohol), then administration of the hypnotic should be withheld.
8.1.2 Hypnotics may impair judgement and increase reaction time and so affect ability to drive and operate machinery. Moreover the hangover effect of a night dose may impair driving the following day5.
8.1.3 A paradoxical increase in hostility, aggression, anxiety and perceptual disorders may be reported by patients taking benzodiazepines. Adjustment of the dose (up or down) sometimes attenuates the impulses5.
8.1.4 Benzodiazepines and z-drug hypnotics should be avoided in the elderly because the elderly are at greater risk of becoming ataxic and confused leading to falls and injury7. The use of benzodiazepines and Z-hypnotics is associated with an increased risk of falls and hip fractures in the elderly12. If prescribed hypnotics, this group of patients must be closely monitored on the ward. A falls assessment must be carried out:- http://cift-ap06/sorce/apps/sorce_doc_manager/Actions/view_doc.aspx?docid=3192&revid=3205

Guidelines for the management of insomnia_PHA08_May 2017 9
8.1.5 On discharge, night sedation should be stopped or continuing use justified in the notes. Information should be relayed to primary care/ secondary care colleagues if prescribing of hypnotics is to continue. All changes should be discussed with the patient. If a patient is being discharged on a hypnotic or prescribed a hypnotic in outpatients, a care plan should be written to the GP in relation to stopping it.
8.1.6 Where prolonged administration is unavoidable, hypnotics should be discontinued as soon as feasible and the patient warned that sleep may be disturbed for a few days before normal rhythm is re-established; broken sleep with vivid dreams may persist for several weeks4. See appendix 1 (How to manage withdrawal of long-term benzodiazepine / z-hypnotic use).
9 Melatonin
9.1.1 Melatonin is restricted in the formulary for sleep disorders in patients with learning disabilities (off label indication). Treatment should be in accordance with NICE guidance 17 as follows (9.1.2.to 9.1.4):
9.1.2 Consider behavioural interventions for sleep problems in children, young people and adults with a learning disability and behaviour that challenges that consist of:
a functional analysis of the problem sleep behaviour to inform the intervention (for example, not reinforcing non-sleep behaviours)
structured bedtime routines.
9.1.3 Do not offer medication to aid sleep unless the sleep problem persists after a behavioural intervention, and then only:
after consultation with a psychiatrist (or a specialist paediatrician for a child or young person) with expertise in its use in people with a learning disability
together with non-pharmacological interventions and regular reviews (to evaluate continuing need and ensure that the benefits continue to outweigh the risks).
9.1.4 If medication is needed to aid sleep, consider melatonin[2].
9.1.5 Higher doses, up to a maximum of 12mg daily, may be required for this patients with learning disability
9.1.6 Treatment should be reviewed regularly, at 3-6 monthly intervals.

Guidelines for the management of insomnia_PHA08_May 2017 10
10 DISSEMINATION AND IMPLEMENTATION ARRANGEMENTS
10.1.1 This document will be circulated to all managers who will be required to cascade the information to members of their teams and to confirm receipt of the procedure and destruction of previous procedures/policies which this supersedes. It will be available to all staff via the Foundation Trust intranet. Managers will ensure that all staff are briefed on its contents and on what it means for them.
11 TRAINING REQUIREMENTS
For training requirements please refer to the Trust’s Mandatory Training Policy and
the Learning and Development Guide on the Trust intranet”
There is a junior doctors’ induction programme which signposts key prescribing
procedures and medicines management policies. There is also access to the policy
folder on the Trust intranet via the induction package.
12 MONITORING AND AUDIT ARRANGEMENTS
Elements to be monitored
Lead How trust will monitor
compliance
Frequency
Reporting arrangements Which committee or group will the monitoring report go to?
Acting on recommendations and Lead(s)
Which committee or group will act on recommendations?
Change in practice and lessons to be shared How will changes be implemented and lessons learnt/ shared?
Hospital patients are being prescribed hypnotics in line with the policy.
Chief Pharmacist.
All prescriptions for hypnotics on inpatient charts are clinically screened by a
Pharmacist
Prior to dispensing.
ongoing Drugs and Therapeutics Committee
Drugs and Therapeutics Committee
Review of policy; implementation practices and procedures
Hypnotic prescribing Chief Pharmacist
Audit annual Drugs and Therapeutics Committee
13 REVIEW OF THE POLICY
March 2019

Guidelines for the management of insomnia_PHA08_May 2017 11
14 REFERENCES
1. `Journal of Psychopharmacology 24(11) 1577-1600. available at
www.bap.org.uk/pdfs/Bap_Sleep_Guidelines.pdf by S.J.Wilson
2. BNF September 2016.
3. Clinical Knowledge Summary available online at:
http://cks.nice.org.uk/insomnia#!diagnosissub
4. Taylor D., Paton C., Kapur S. Editors. The South London and Maudsley NHS
Foundation Trust. Oxleas NHS Foundation Trust. Prescribing Guidelines. 12th
Edition. London. Informa Healthcare. 2015.
5. Sanofi. The specification of product characteristics. Stilnoct. (4th September 2014)
(online). Available: https://www.medicines.org.uk/emc/medicine/25411 (accessed 9th
of December 2014).
6. Email from Jeff Halperin to Rashmika Shah. CBTi. 29 April 2014.
7. Drug Safety update. Drugs and driving: blood concentration limits to be set for certain controlled drugs in a new legal offence.(online). Available: https://www.gov.uk/drug-safety-update/drugs-and-driving-blood-concentration-limits-to-be-set-for-certain-controlled-drugs-in-a-new-legal-offence (accessed 29th January 2015).
8. Chawla J. and Benbadis S.R. Insomnia treatment and management. (updated 25th
August 2014). (online). Available: http://emedicine.medscape.com/article/1187829-
treatment#aw2aab6b6b3 (accessed 9th of December 2014).
9. National Institute for Health and Clinical Excellence. Antenatal and postnatal mental health. Clinical management and service guidance. NICE clinical guidance 192. Last updated June 2015. https://www.nice.org.uk/guidance/cg192/resources/antenatal-and-postnatal-mental-health-clinical-management-and-service-guidance-35109869806789 (accessed 9th January 2017).
10. E-mail from Dr Nisha Shah to Audrey Coker. Nisha Shah RE: Benzodiazepines and Z-hypnotics. 5th December 2014.
11. Actavis. The specification of product characteristics. Temazepam. (30th October
2014) (online). Available: https://www.medicines.org.uk/emc/medicine/29058
accessed 9th of January 2017).
12. Bazire S. The Psychotropic Drug Directory. The professionals’ pocket handbook and aide memoire. 2016.
13. Baldwin D.S. et al. Evidence based guidelines for the pharmacological treatment of anxiety disorder. Recommendations from the British Association for Psychopharmacology. Journal of psychopharmacology, 19 (6) (2005), p567 – 596.
14. Baldwin et al. Benzodiazepines: Risks and benefits. A reconsideration.2013, Journal of Psychopharmacology 27(11) 967–971.
15. Department of Health (England), the Scottish Government, Welsh Assembly Government and Northern Ireland Executive.Drug Misuse and Dependence. (online) Available: http://www.nta.nhs.uk/uploads/clinical_guidelines_2007.pdf (accessed 9th of December 2014).
16. National Institute for Health and Clinical Excellence. Benzodiazepine and Z-drug withdrawal. (online) Available:: http://cks.nice.org.uk/benzodiazepine-and-z-drug-withdrawal#!scenario (accessed 9th of December 2014).
17. National Institute for Health and Clinical Excellence. NICE Guidance (NG11) Challenging behaviour and learning disabilities: prevention and interventions for people with learning disabilities whose behaviour challenges. May 2015

Guidelines for the management of insomnia_PHA08_May 2017 12
APPENDIX 1
How to manage withdrawal of long-term benzodiazepine and z-hypnotic use:
Benzodiazepines
Benzodiazepines are widely acknowledged to cause dependence and tolerance and
withdrawal symptoms (see below) can occur after 4-6 weeks of continuous use4. Short-
acting ones such as lorazepam are associated with more problems on withdrawal than the
longer-acting ones such as diazepam4. To avoid or reduce the severity of these problems,
good practice states that benzodiazepines should not be prescribed as hypnotics or
anxiolytics for longer than four weeks4.
Withdrawal symptoms from benzodiazepines4
Physical: Psychological:
Stiffness Anxiety/Insomnia
Weakness Nightmares
Gastrointestinal disturbance Depersonalisation
Paraesthesia Decreased memory and concentration
Flu-like symptoms Delusions and hallucinations
Visual disturbances Depression
Managing withdrawal
Confirm usage by:
Checking the prescription
Urine screening if obtained illicitly (very short-acting benzodiazepines may not
give a positive urine screen despite daily use)4.
A tolerance test is required if patient has been obtaining illicit supplies. No benzodiazepines
or alcohol should be consumed for twelve hours before the test. A test dose of 10mg
diazepam should be administered and patient observed for 2-3 hours (20mg if consumption
of > 50mg daily is claimed or suspected). If there are no signs of sedation, it is generally safe
to prescribe the same dose as the test dose, three times daily. Some patients may require
much higher doses. In these cases inpatient assessment would be better4.
Problematic withdrawal can be anticipated if4:
Previous attempts have been unsuccessful
Lack of social support
History of alcohol/polydrug abuse
Withdrawal seizures
Elderly patients
Severe psychiatric/physical disorders
Personality disorder

Guidelines for the management of insomnia_PHA08_May 2017 13
Withdrawal is too rapid
All above must be taken into consideration and patient monitored closely during
benzodiazepine withdrawal. Discontinuation symptoms have their peak severity at two days
for short half-life and four to seven days for long-half-life benzodiazepines13.
All patients should be made aware of the risks of dependence if they continue benzodiazepines in regular dosage over a longer period. A clinical judgement has to be made as to whether alternatives may be more suitable, for each patient, and for each proposed medication14. There is increasing evidence that long-term prescribing (especially of more than 30 mg diazepam equivalent per day) may cause harm. Clinicians may be faced with requests to continue a prescription for maintenance benzodiazepines. To prevent symptoms of benzodiazepine withdrawal, the clinician should continue the prescription but the dose should be gradually reduced to zero. Very rarely should doses of more than 30 mg diazepam equivalent per day be prescribed15.
Prescribing to assist withdrawal should only be initiated where there is clear evidence of benzodiazepine dependency from the patient’s history, observed symptoms and drug testing. The aim should be to prescribe a reducing regimen for a limited period of time15. The rate of withdrawal is often determined by an individual’s capacity to tolerate symptoms. Benzodiazepines, including diazepam, can be withdrawn in proportions of about one-eighth (between one-tenth and one-quarter) of the daily dose every fortnight. In dependence on therapeutic doses, the dose can be reduced initially by 2–2.5 mg and if withdrawal symptoms occur, then the dose can be maintained until symptoms improve. If the patient is not coping and is experiencing severe withdrawal symptoms, it may be necessary to increase the dose to alleviate the symptoms15.
If very high dose prescribing is required the patient should be referred for specialist assessment. Specialist practitioners then need to exercise caution in their assessments and prescribing. If the patient is stable and free of withdrawal symptoms, at for example 50 mg a day, the dose should be gradually reduced at a faster rate than suggested, for example by half over six weeks and then the planned rate of reduction should be again reviewed in line with the guidance outlined previously. This faster rate of reduction from very high doses led to no convulsions even in a group who had a high incidence of these during previous benzodiazepine withdrawals15. In the inpatient setting it is appropriate to provide a slow withdrawal regimen over one to four weeks, with diazepam starting at a daily dose of no more than 30 mg, and usually less, given in divided doses15
. If the patient is in agreement, benzodiazepines should be withdrawn in line with the following considerations:
Switching to diazepam – patients should be offered the equivalent dose of diazepam as it has a long half-life. The approximately equivalent doses are in table 64.
Table 6: Switching from benzodiazepine to diazepam: doses4,14,15
Benzodiazepine Approximate dose (mg) equivalent to 10mg diazepam
Nitrazepam 10mg
Oxazepam 30mg
Temazepam 20mg
Zaleplon* 20mg
Zopiclone 15mg
Zolpidem 20mg
*These are non-formulary medicines.
Guidelines for the management of insomnia_PHA08_May 2017 14
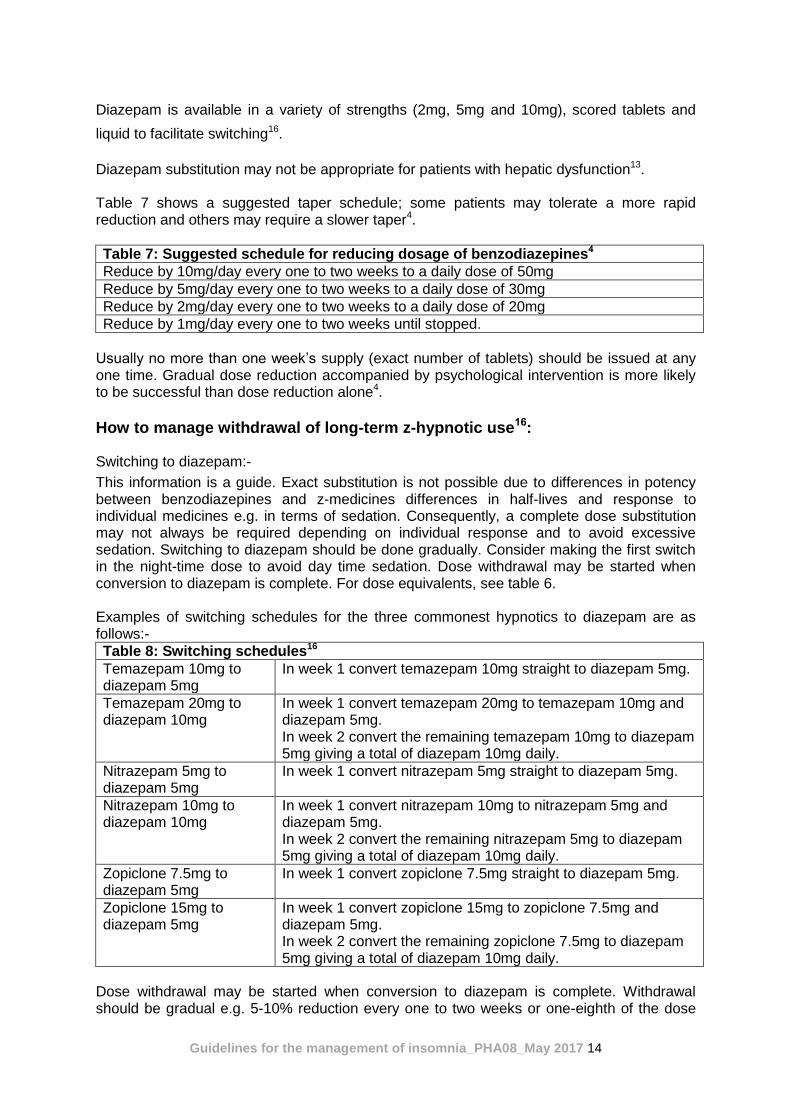
Diazepam is available in a variety of strengths (2mg, 5mg and 10mg), scored tablets and
liquid to facilitate switching16.
Diazepam substitution may not be appropriate for patients with hepatic dysfunction13.
Table 7 shows a suggested taper schedule; some patients may tolerate a more rapid reduction and others may require a slower taper4.
Table 7: Suggested schedule for reducing dosage of benzodiazepines4
Reduce by 10mg/day every one to two weeks to a daily dose of 50mg
Reduce by 5mg/day every one to two weeks to a daily dose of 30mg
Reduce by 2mg/day every one to two weeks to a daily dose of 20mg
Reduce by 1mg/day every one to two weeks until stopped.
Usually no more than one week’s supply (exact number of tablets) should be issued at any one time. Gradual dose reduction accompanied by psychological intervention is more likely to be successful than dose reduction alone4.
How to manage withdrawal of long-term z-hypnotic use16:
Switching to diazepam:-
This information is a guide. Exact substitution is not possible due to differences in potency between benzodiazepines and z-medicines differences in half-lives and response to individual medicines e.g. in terms of sedation. Consequently, a complete dose substitution may not always be required depending on individual response and to avoid excessive sedation. Switching to diazepam should be done gradually. Consider making the first switch in the night-time dose to avoid day time sedation. Dose withdrawal may be started when conversion to diazepam is complete. For dose equivalents, see table 6. Examples of switching schedules for the three commonest hypnotics to diazepam are as follows:-
Table 8: Switching schedules16
Temazepam 10mg to diazepam 5mg
In week 1 convert temazepam 10mg straight to diazepam 5mg.
Temazepam 20mg to diazepam 10mg
In week 1 convert temazepam 20mg to temazepam 10mg and diazepam 5mg. In week 2 convert the remaining temazepam 10mg to diazepam 5mg giving a total of diazepam 10mg daily.
Nitrazepam 5mg to diazepam 5mg
In week 1 convert nitrazepam 5mg straight to diazepam 5mg.
Nitrazepam 10mg to diazepam 10mg
In week 1 convert nitrazepam 10mg to nitrazepam 5mg and diazepam 5mg. In week 2 convert the remaining nitrazepam 5mg to diazepam 5mg giving a total of diazepam 10mg daily.
Zopiclone 7.5mg to diazepam 5mg
In week 1 convert zopiclone 7.5mg straight to diazepam 5mg.
Zopiclone 15mg to diazepam 5mg
In week 1 convert zopiclone 15mg to zopiclone 7.5mg and diazepam 5mg. In week 2 convert the remaining zopiclone 7.5mg to diazepam 5mg giving a total of diazepam 10mg daily.
Dose withdrawal may be started when conversion to diazepam is complete. Withdrawal should be gradual e.g. 5-10% reduction every one to two weeks or one-eighth of the dose
Guidelines for the management of insomnia_PHA08_May 2017 15
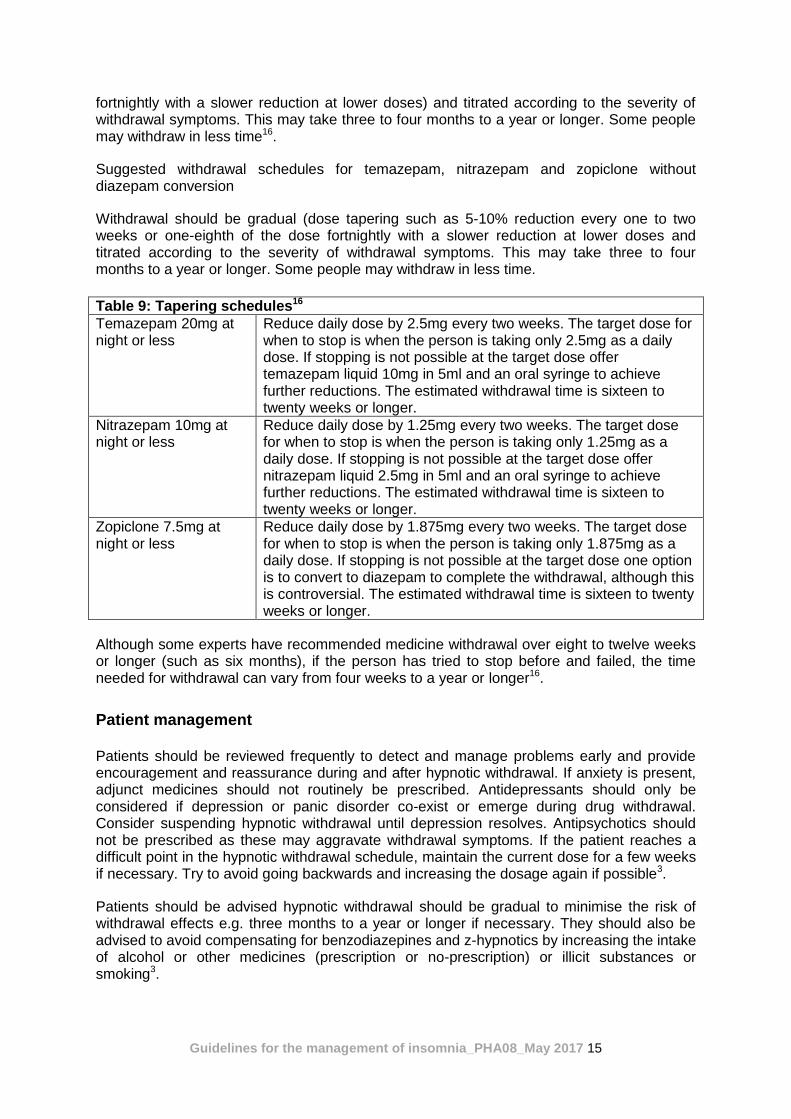
fortnightly with a slower reduction at lower doses) and titrated according to the severity of withdrawal symptoms. This may take three to four months to a year or longer. Some people may withdraw in less time16.
Suggested withdrawal schedules for temazepam, nitrazepam and zopiclone without diazepam conversion
Withdrawal should be gradual (dose tapering such as 5-10% reduction every one to two weeks or one-eighth of the dose fortnightly with a slower reduction at lower doses and titrated according to the severity of withdrawal symptoms. This may take three to four months to a year or longer. Some people may withdraw in less time.
Table 9: Tapering schedules16
Temazepam 20mg at night or less
Reduce daily dose by 2.5mg every two weeks. The target dose for when to stop is when the person is taking only 2.5mg as a daily dose. If stopping is not possible at the target dose offer temazepam liquid 10mg in 5ml and an oral syringe to achieve further reductions. The estimated withdrawal time is sixteen to twenty weeks or longer.
Nitrazepam 10mg at night or less
Reduce daily dose by 1.25mg every two weeks. The target dose for when to stop is when the person is taking only 1.25mg as a daily dose. If stopping is not possible at the target dose offer nitrazepam liquid 2.5mg in 5ml and an oral syringe to achieve further reductions. The estimated withdrawal time is sixteen to twenty weeks or longer.
Zopiclone 7.5mg at night or less
Reduce daily dose by 1.875mg every two weeks. The target dose for when to stop is when the person is taking only 1.875mg as a daily dose. If stopping is not possible at the target dose one option is to convert to diazepam to complete the withdrawal, although this is controversial. The estimated withdrawal time is sixteen to twenty weeks or longer.
Although some experts have recommended medicine withdrawal over eight to twelve weeks or longer (such as six months), if the person has tried to stop before and failed, the time needed for withdrawal can vary from four weeks to a year or longer16.
Patient management
Patients should be reviewed frequently to detect and manage problems early and provide encouragement and reassurance during and after hypnotic withdrawal. If anxiety is present, adjunct medicines should not routinely be prescribed. Antidepressants should only be considered if depression or panic disorder co-exist or emerge during drug withdrawal. Consider suspending hypnotic withdrawal until depression resolves. Antipsychotics should not be prescribed as these may aggravate withdrawal symptoms. If the patient reaches a difficult point in the hypnotic withdrawal schedule, maintain the current dose for a few weeks if necessary. Try to avoid going backwards and increasing the dosage again if possible3.
Patients should be advised hypnotic withdrawal should be gradual to minimise the risk of withdrawal effects e.g. three months to a year or longer if necessary. They should also be advised to avoid compensating for benzodiazepines and z-hypnotics by increasing the intake of alcohol or other medicines (prescription or no-prescription) or illicit substances or smoking3.
Guidelines for the management of insomnia_PHA08_May 2017 16
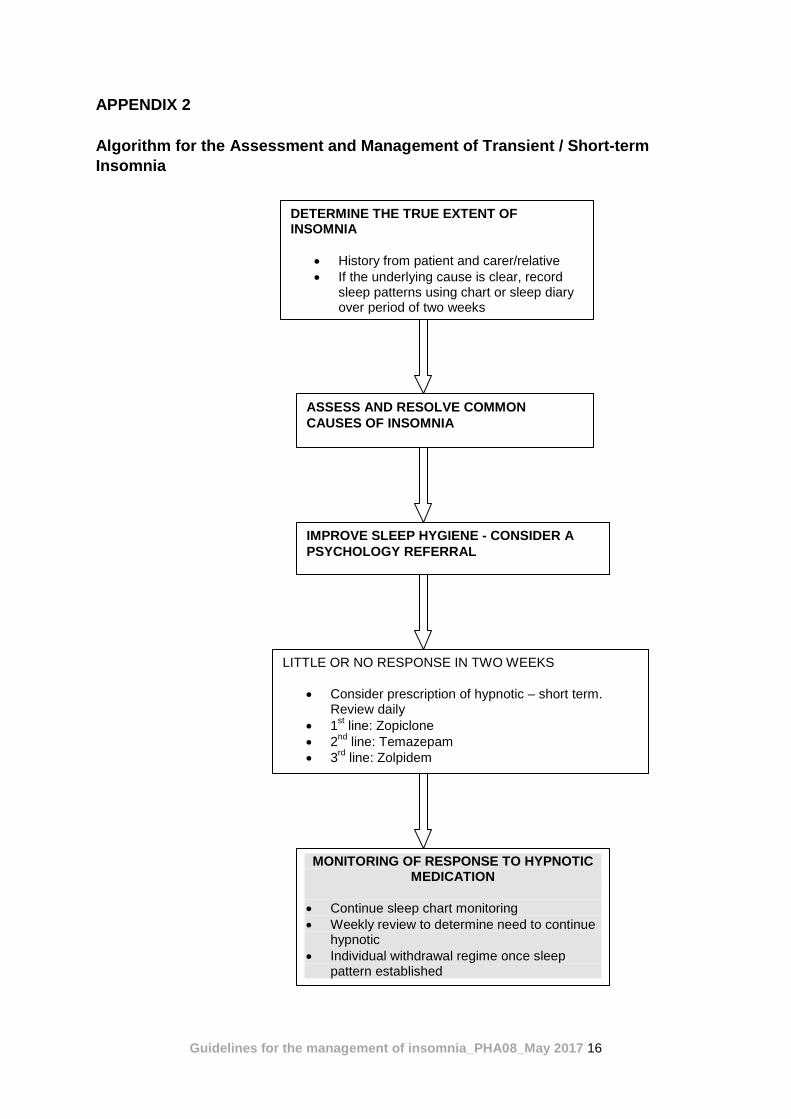
APPENDIX 2
Algorithm for the Assessment and Management of Transient / Short-term
Insomnia
DETERMINE THE TRUE EXTENT OF INSOMNIA
History from patient and carer/relative
If the underlying cause is clear, record sleep patterns using chart or sleep diary over period of two weeks
ASSESS AND RESOLVE COMMON
CAUSES OF INSOMNIA
LITTLE OR NO RESPONSE IN TWO WEEKS
Consider prescription of hypnotic – short term. Review daily
1st line: Zopiclone
2nd
line: Temazepam
3rd
line: Zolpidem
IMPROVE SLEEP HYGIENE - CONSIDER A
PSYCHOLOGY REFERRAL
MONITORING OF RESPONSE TO HYPNOTIC MEDICATION
Continue sleep chart monitoring
Weekly review to determine need to continue hypnotic
Individual withdrawal regime once sleep pattern established

Guidelines for the management of insomnia_PHA08_May 2017 17
APPENDIX 3
Medicines not approved in the trust formulary for the treatment of insomnia (as a main indication). Table 5: Medicines for which management of insomnia would be a non-formulary indication (as main indication).
GROUP OF MEDICINES
REASONS AND EXPLANATIONS
Antidepressants There is limited evidence for efficacy of doxepin, trimipramine, trazodone, paroxetine in insomnia. Antidepressants may affect a wide range of brain receptors and have longer-lasting carry-over effects than traditional hypnotic drugs – antidepressants are associated with increased risks of road accidents especially early in treatment in depression. Beware of toxicity of tricyclic antidepressants in overdose1. SSRIs as a class generally disrupt sleep early in course of treatment1. Taking SSRIs, venlafaxine, mirtazapine increases the risk of restless legs syndrome and periodic limb movements in sleep (PMLS), and SSRIs are known to induce or exacerbate sleep bruxism1.
Antipsychotics Side effects are common because of the pharmacological actions of these medicines and there are a few reports of abuse. Together these indicate no indication for use as first-line treatment1. Side effects include weight gain, metabolic syndrome, extrapyramidal symptoms and risk of tardive dyskinesia. There are some case reports of abuse of quetiapine in inpatients and prisoners1. Antipsychotic medicines may have useful sedative effects when prescribed for co-morbidities e.g. depression, mania, schizophrenia and acutely disturbed behaviour.
Antihistamines Antihistamines have a limited role in psychiatric and primary care practice for the management of insomnia. These are sedating and can be bought over – the – counter. These have long duration of action and can often cause drowsiness the following day1. The sedative effect of antihistamines diminish after a few days of continued treatment. Side-effects include headache, psychomotor impairment and antimuscarinic effects2. Promethazine is included in the formulary as an alternative sedative if a patient is tolerant to benzodiazepines in rapid tranquillisation.
Diazepam, nitrazepam, flurazepam
These are not recommended because their long half-life commonly gives rise to next-day residual effects and repeated doses tend to be cumulative2. Diazepam may be used in specific circumstances (point 9).
Chloral hydrate, clomethiazole, barbiturates
Barbiturates and chloral hydrate are toxic in overdose11. Barbiturate, chloral hydrate, and clomethiazole are not recommended. There is insufficient evidence to support their use and the potential for adverse effects is significant3.
Oxazepam Included in the formulary for off-label use in alcohol detoxification only.
Melatonin A non-formulary application is required for it’s licensed indication of a
primary sleep disorder.
A non-formulary application would be required for the above.
Guidelines for the management of insomnia_PHA08_May 2017 18
Appendix 4: Equality Impact Assessment Tool
Yes/No Comments
1. Does the policy/guidance affect one group less or more favourably than another on the basis of:
Race no
Ethnic origins (including gypsies and travellers) no
Nationality no
Gender no
Culture no
Religion or belief no
Sexual orientation including lesbian, gay and bisexual people
no
Age no
Disability - learning disabilities, physical disability, sensory impairment and mental health problems
no
2. Is there any evidence that some groups are affected differently?
no
3. If you have identified potential discrimination, are any exceptions valid, legal and/or justifiable?
n/a
4. Is the impact of the policy/guidance likely to be negative?
no
5. If so can the impact be avoided? n/a
6. What alternatives are there to achieving the policy/guidance without the impact?
n/a
7. Can we reduce the impact by taking different action?
n/a