global vascular guidelines: a new pathway for...
TRANSCRIPT

GLOBAL VASCULAR GUIDELINES:A NEW PATHWAY FOR LIMB SALVAGE
Michael S. Conte MDProfessor and Chief, Vascular and Endovascular Surgery
Co-Director, Center for Limb PreservationCo-Director, Heart and Vascular CenterUniversity of California, San Francisco
DF Con 2018

Disclosures Symic, Inc (SAB) Abbott Vascular (advisory board) VasaRx (co-founder) BEST-CLI Trial (EC Co-Chair; NHLBI) Co-Editor, Global Vascular Guidelines on the
management of chronic limb-threatening ischemia

WFVS
The Global Vascular Guidelines (GVG) initiative is sponsored by an international consortium of vascular societies, led by
the European Society for Vascular Surgery (ESVS), the Society for Vascular Surgery
(SVS), and the World Federation of Vascular Societies (WFVS)

WFVS
Global Vascular Guideline for the Management of Chronic Limb-Threatening Ischemia
Michael S. Conte MD, Andrew W. Bradbury MBA, MD, FRCSPhilippe Kolh MD, PhD (Co-Editors)

Rationale for a Global Vascular Guideline in CLTI
• Growing global prevalence of disease and risk factors• High patient and public health costs• Diverse specialties/providers and care settings• Highly variable utilization of vascular interventions• Wide disparity in outcomes, unclear standard of care • Continuously evolving technology, shifting practice patterns• Lack of consensus definitions and disease staging a major limitation to
evidence-based medicine and clinical/outcomes research• Define Key Research Questions• Foster Improved Care and Quality Outcomes for Patients
WFVS

A New Framework for Evidence‐Based Care in Chronic Limb Threatening Ischemia (CLTI)
• Definitions• Staging of disease• Anatomic patterns• Evidence‐based
revascularization• UNDER FINAL
REVIEW (release Q1 2019)

Definitions: CLTIThe term critical limb ischemia (CLI) is outdated and fails to encompass the full spectrum of patients who are evaluated and treated for limb-threatening ischemia in modern practice
Instead, the term chronic limb-threatening ischemia (CLTI) is proposed, in order to include a broader and more heterogeneous group of patients with varying degrees of ischemia that can often delay wound healing and increase amputation risk.
WFVS
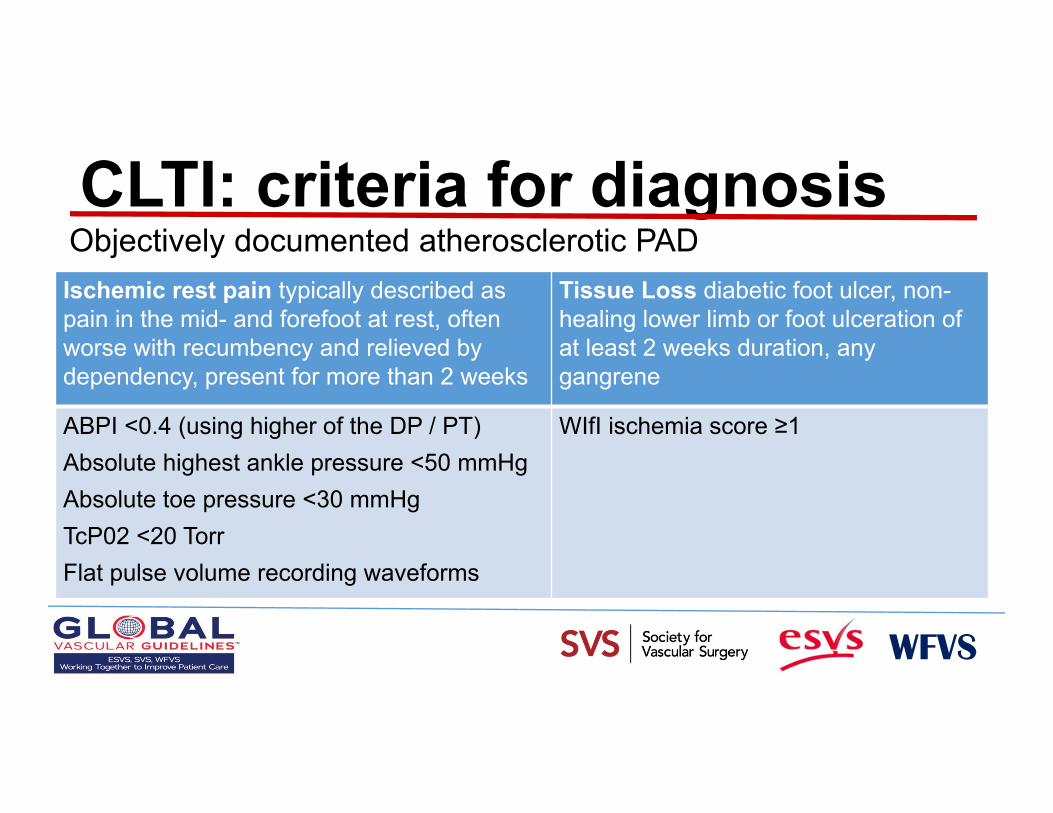
CLTI: criteria for diagnosis
WFVS
Ischemic rest pain typically described as pain in the mid- and forefoot at rest, often worse with recumbency and relieved by dependency, present for more than 2 weeks
Tissue Loss diabetic foot ulcer, non-healing lower limb or foot ulceration of at least 2 weeks duration, any gangrene
ABPI <0.4 (using higher of the DP / PT)Absolute highest ankle pressure <50 mmHgAbsolute toe pressure <30 mmHgTcP02 <20 TorrFlat pulse volume recording waveforms
WIfI ischemia score ≥1
Objectively documented atherosclerotic PAD
Need for Structured Decision Making in CLTI
PLAN: Patient Risk Limb threat severity: WIfI Staging ANatomic pattern of disease: GLASS system
WFVS

WFVS


WFVS
Risk stratification tools
High Risk defined as expected perioperative mortality >5% OR expected 2 year survival
<50%

Simons J, et al. J Vasc Surg (in press)
VQI Survival Model for CLTIN= 38,470; PVI= 24,214; LEB= 14,256
Risk group POD 2-YR survivalLOW <3% >70%MEDIUM 3-5% 50-70%HIGH >5% <50%

Importance of Limb Staging in CLTI Broad spectrum of complexity and risk for limb loss
Complicates analysis of outcomes and treatment decisions Previous classification systems inadequately capture the full range
of neuro-ischemic compromise Fallacy of a specific hemodynamic threshold for “critical” ischemia SVS Wound, Ischemia, Foot Infection (WIfI) system
Characterizes each of the three major components Grouped into 4 stages based on estimated risk for limb loss Multiple validation reports
WFVS


Wound Grade – Clinical Category
Grade Clinical Description
0 Ischemic rest pain; Pre‐gangrenous skin change, without frank ulcer or gangrene (Pedis or UT Class 0)
1 Minor tissue loss: small shallow ulceration) < 5 cm2 on foot or distal leg (Pedis or UT Class 1); no exposed bone unless limited to distal phalanx
2 Major tissue loss: deeper ulceration(s) with exposed bone, joint or tendon, ulcer 5‐10 cm2
not involving calcaneus – (Pedis or UT Classes 2 and 3); gangrenous changes limited to digits. Salvageable with multiple digital amps or standard TMA + skin coverage
3 Extensive ulcer/gangrene > 10 cm2 involving forefoot or midfoot; full thickness heel ulcer > 5 cm2 + calcaneal involvement. Salvageable only with complex foot reconstruction, nontraditional TMA (Chopart/Lisfranc); flap coverage or complex wound management needed
WFVS

Ischemia Grade – Noninvasive AssessmentGrade ABI Ankle SP TP
0 > 0.80 > 100 mm Hg > 60 mm Hg
1 0.60‐0.79 70‐99 mmHg 40‐59 mm Hg
2 0.40‐0.59 50‐69 mm Hg 30‐39 mm Hg
3 < 0.40 < 50 mm Hg < 30 mm Hg
ABI=ankle brachial index; SP= systolic pressure; TP=toe pressure
WFVS

WFVS

Study (year): # Limbs at Risk Stage 1 Stage 2 Stage 3 Stage 4
Cull (2014):151 37 (3%) 63 (10%) 43 (23%) 8 (40%)
Zhan (2015): 201 39 (0%) 50 (0%) 53 (8%) 59 (64%)*
Darling (2015): 551 5 (0%) 111 (10%) 222 (11%) 213 (24%)
Causey (2016): 160 21 (0%) 48 (8%) 42 (5%) 49 (20%)
Beropoulis (2016): 126 29 (0%) 42 (2%) 29 (3%) 26 (12%)
Ward (2016): 98 5 (0%) 21 (14%) 14 (21%) 58 (34%)
Darling (2017): 992 12 (0%) 293 (4%) 249 (4%) 438 (21%)
Robinson (2017): 262 48 (4%) 67 (16%) 64 (10%) 83 (22%)
Mathioudakis (2017): 279 95 (6.5%) 33 (6%) 87 (8%)** 64 (6%)***
N = 2820 (weighted mean) 291 (3.2%) 728 (6.8%) 803 (8.5%) 998 (24%)
Median (% 1 year amputation) 0% 8% 8% 22%
Risk of amputation vs SVS WIfI Stage

Limb staging and appropriateness of revascularization
WFVS
• CLTI represents a range of limb severity and ischemia as described in WIfI staging.
• Severe ischemia (WIfI ischemia grade 3) mandates revascularization for limb salvage
• With increased stages of limb threat (WIfI stages 3, 4) moderate degrees of ischemia (grades 1, 2) may be appropriate to address
• Low risk limbs (WIfI Stage 1) should be treated with wound care; revascularization should be reserved for failure to heal (50% within 4‐6 weeks) or clinical signs of deterioration
• Not indicated for Ischemia grade 0

Benefit of revascularization varies with severity of limb threat and ischemia
3
2
1
0
High benefit
Low/Nil benefit
1 2 3 4Limb Severity (WIfI Stage)
Severity of Ischem
ia(W
IfIIschem
ia
Grade
)
N/A
N/A

Rationale for a new anatomic staging system in CLTI
WFVS
• Schemes focused on individual lesions (e.g. TASC) or overall burden of disease (e.g. Bollinger) are not useful for defining evidence-based revascularization in CLTI
• Restoration of in-line flow to the foot is a primary technical goal of revascularization in CLTI, particularly in patients with tissue loss
• Factors that determine clinical success for endovascular and open bypass surgery are intrinsically different

GLASS*: Assumptions and Approach
WFVS
• Focus on Infrainguinal Disease (SFA origin to foot)• Clinician defines the primary Target Artery Path (TAP) • Femoro-popliteal (FP) and Infra-popliteal (IP) segments separately
graded (0-4), then combined into Three GLASS Stages for the limb (I-III)
• Infra-malleolar (pedal) disease graded; used as a modifier only• Calcification graded as Severe or not; simplified system • *Global Limb Anatomic Staging System

GLASS: Target Artery Path and Limb-Based Patency
WFVS
• Restoration of in‐line flow to the ankle and foot is a primary goal• Target artery path (TAP): the selected continuous route of in‐line
flow from groin to ankle• TAP usually involves the least diseased IP artery; may be
angiosome‐based• Limb‐based patency (LBP): maintained patency of the TAP. Lost
when:• Occlusion, critical stenosis, or re‐intervention affecting any portion of the TAP (anatomical failure), and/or:
• Fall in ABI (≥ 0.15) or TBI (≥ 0.10), or ≥ 50% stenosis in the TAP, in the presence of recurrent or unresolved clinical symptoms (e.g. rest pain, worsening/persistent tissue loss; signifying hemodynamic failure)

WFVS

WFVS

WFVS
GLASS: Consensus Staging of TAP Complexity for Endovascular Intervention


FP grading: SFA: no significant stenosisPopliteal: no significant stenosisFP grade = 0IP grading: TAP = peroneal arteryPeroneal: CTO 3‐10cmIP grade = 3
GLASS Stage = II

FP grading: Total length of SFA disease: 10‐20 cmPopliteal disease: <5cm does not involve trifurcationCalcification + 1FP grade = 4IP grading: TAP= peroneal arteryPeroneal: stenosis TP trunkIP grade = 2 GLASS Stage = III

Preferred initial revascularization strategy:average risk CLTI patient with available GSV
