giornata mondiale contro la rabbia. la situazione
TRANSCRIPT
Giornata mondiale contro la rabbia.La situazione epidemiologica e le
iniziative dell’Italia.
Roma, 30 settembre 2019Ministero della Salute
Workshop
Aggiornamento sulla profilassi pre e post -esposizione
Federico Gobbi
Dipartimento di Malattie Infettive e Tropicali e Microbiologia

Among all the infectious diseases, rabies is the most easy to prevent
Louis Pasteur

Travel-associated human rabies
Rabies causes fatal encephalitis
- an estimated 59.000 - 70.000 human deaths every year in endemic
regions
- estimated risk for an animal bite in travellers:
calculated 0,4 % per month staying in an endemic country
- 3 deaths per year in travellers
Background
Hampson et al. PloS Negl Trop Dis 2015
WHO Wkly Epidemiol Rec 2010
Gautret: JTravelMed 2012; Vaccine 2012; Curr Opin Infect Dis 2012
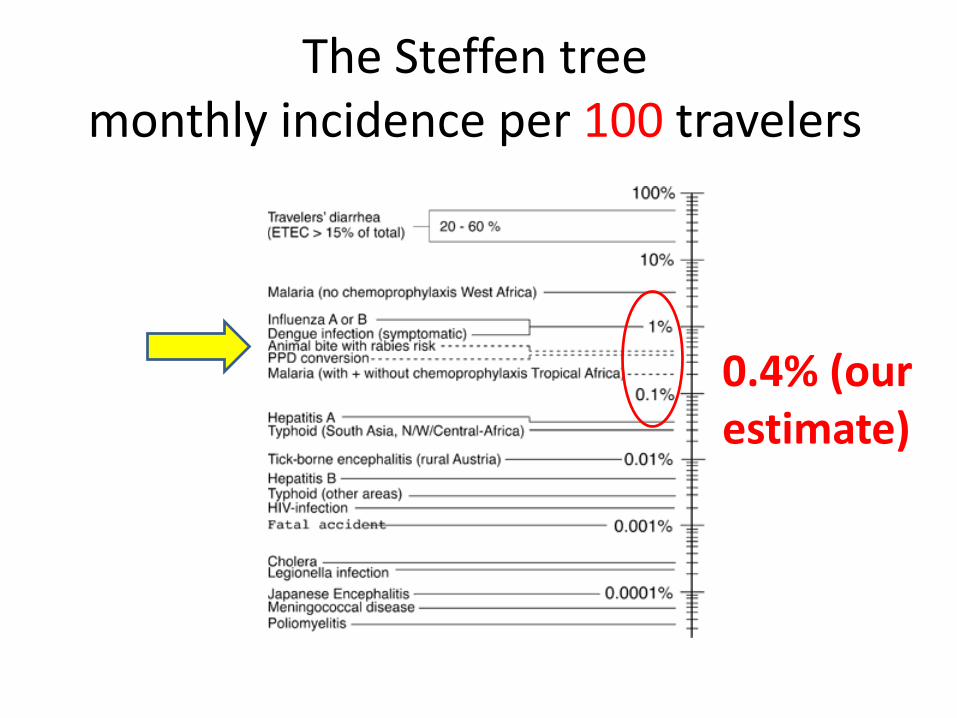
The Steffen treemonthly incidence per 100 travelers
0.4% (our estimate)

7
Institut Pasteur de Paris
The 10th of October 2017
Un cas de rage importé en France chez un enfant
Hospitalisé à Lyon, le garçon de 10 ans avait été mordu par un chien contaminé lors d’un séjour en août 2017 au Sri Lanka.
Background

Only the seventh known case in the United Kingdom since 2000.
England's health service issued a reminder Monday for travellers to avoid coming into contact with animals when travelling to rabies affected countries, particularly those in Asia and Africa
The 12th of Nov 201858 old Briton dies from rabies after cat bite in Morocco

The 6th of May 2019
Norwegian woman dies fromrabies after Philippines puppy bite
Birgitte Kallestad, 24 year old, was on holiday withfriends when they found the puppy on a street.
She fell ill soon after returning to Norway, and died on Monday at the hospital where she worked.
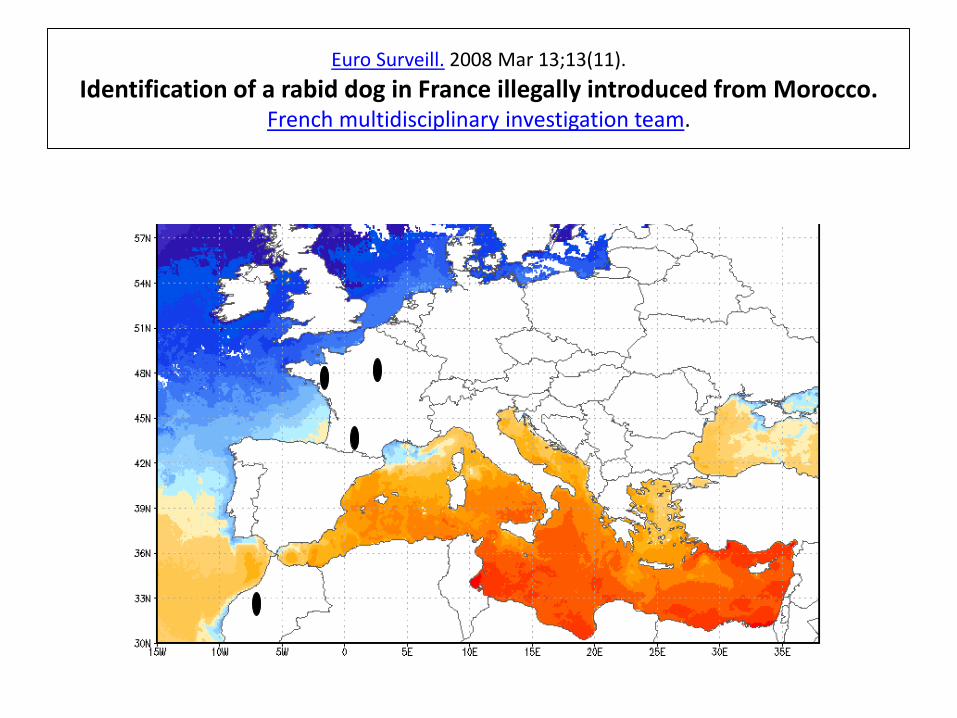
Euro Surveill. 2008 Mar 13;13(11).
Identification of a rabid dog in France illegally introduced from Morocco.French multidisciplinary investigation team.

Globalizzazione

60 cases in 1990-2012

10 new cases in 2013-2019
• Taiwan ex. Philippine (migrant)• US ex. Guatemala (Migrant)• The Netherlands ex. Haïti (not documented)• The Netherlands ex. India (Indian married a Dutch)• France ex. Mali (VFR)• UK ex. India (not documented)• France ex. Sri Lanka (Tourist)• UK ex. Morocco (Tourist)• Qatar ex. Nepal (Migrant)• Norway ex. Philippines (Tourist)

• 2.6 cases per year, increase from 2004
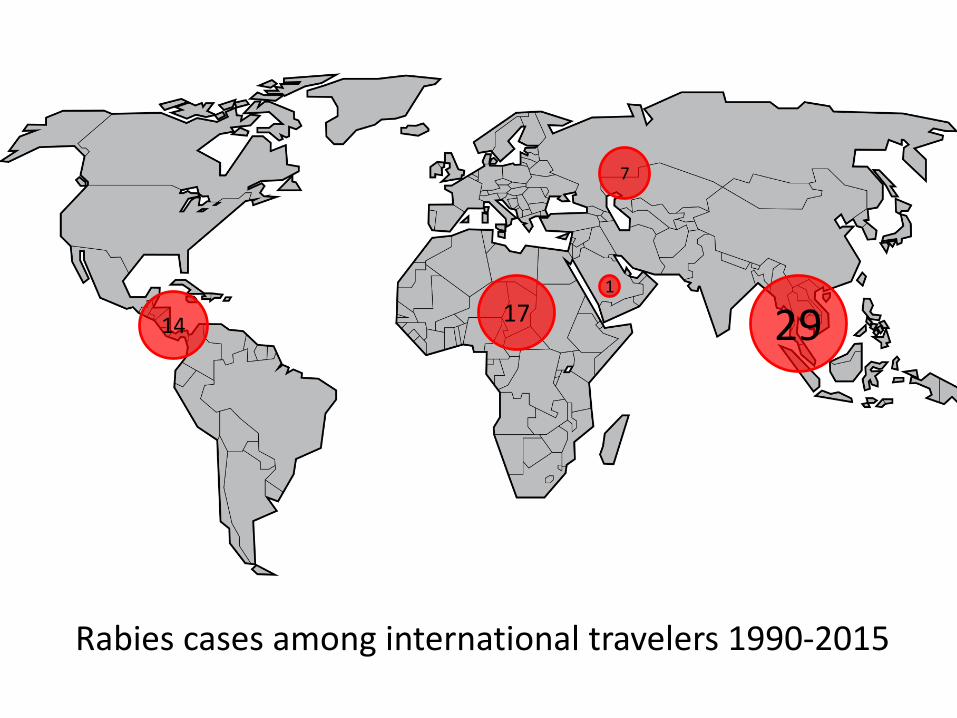
2917
7
14
1
Rabies cases among international travelers 1990-2015
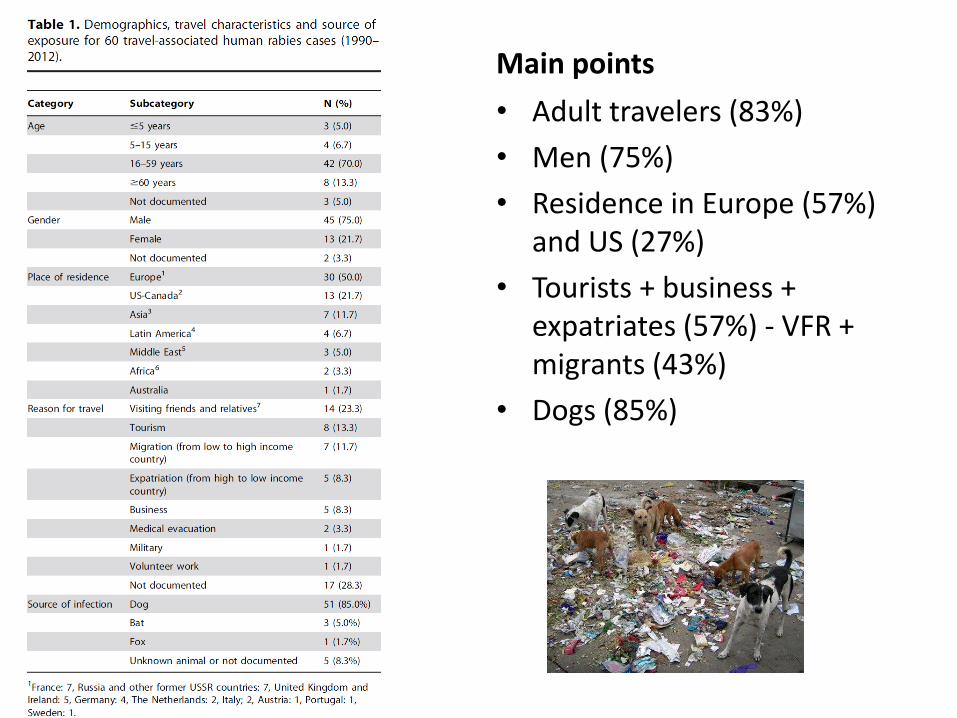
Main points
• Adult travelers (83%)
• Men (75%)
• Residence in Europe (57%) and US (27%)
• Tourists + business + expatriates (57%) - VFR + migrants (43%)
• Dogs (85%)

• Mean incubation time 274 days (9 months)
• 9 case < 30 days
• 1 case 12 days after dog bite in India
• 1 case 15 days after bat bite in Mexico
• 1 case 5 years afterimmigration from China
• 1 case 8 years after dog exposure in Brazil
• 1 case 10 years after dog bite in Myanmar

1997-2012
2697 injured travelers receiving rabies PEP (1.5%)
45 sites
74% seen after travel
25% seen during travel
Origin: Western Europe: 32%, North East Asia: 17%, Australia New Zealand: 17%,South East Asia: 14%,
North America: 10%

• 42% in South East Asia, 32% other Asiancountries, 9% Africa, 7% Latin America, 3% Middle East : top countries : Thailand, Indonesia, Nepal, China, India.
• Median travel duration : 15 days (patients seen after travel), 20 days (patients seenduring travel)
• Animal species: 60% dog, 24%, NHP, 10% cat, 2% bat
• 2/3 of NHP exposure occured in Asia, 90% occurred in tourists


WHO Stategic Advisatory Group of Experts (SAGE) on immunization
• Rabies vaccines: WHO Position paper – April 2018 (WER, 16, 2018, 93:201-220)

• WHO guidelines > 2-visit regimen for rabies PrEP: 2ID or 2IM
Rabies PrEP
21IM
2²ID

Post-exposureprophylaxis

Risk assessment



Effective100%

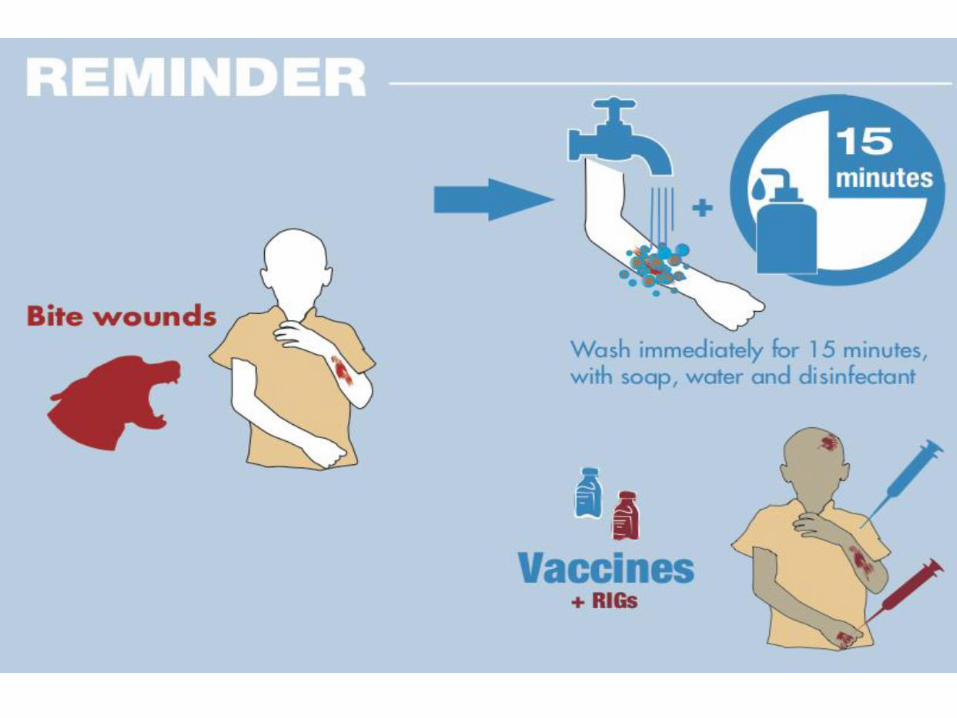
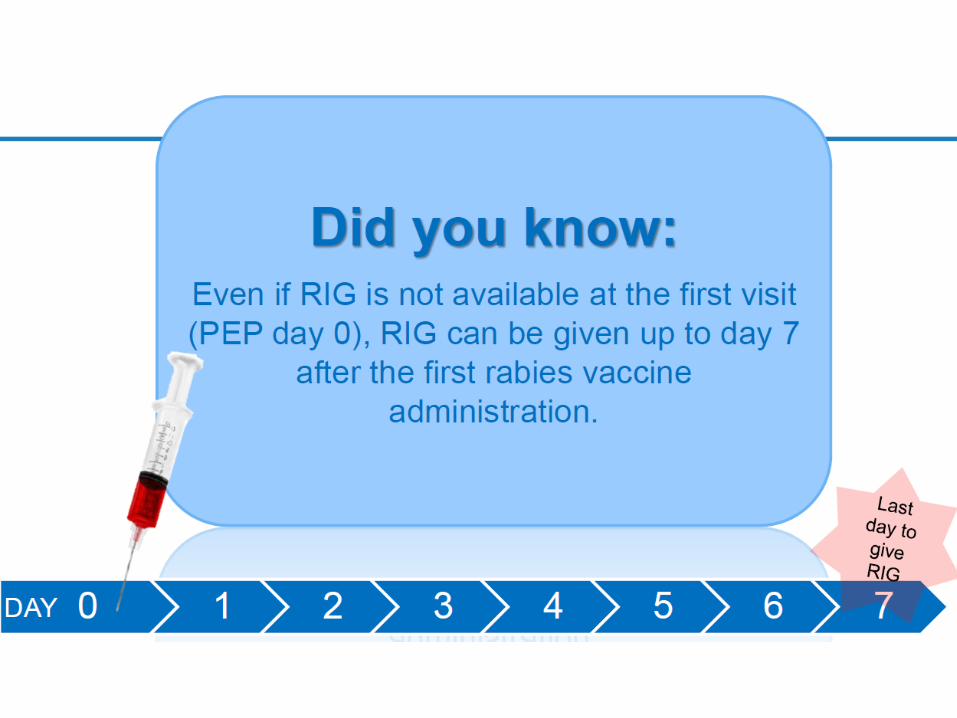
• Additional IM administration of any remainingRIG at a site distant to the wound is a commonpractice. Its benefits are likely to be verylimited. Not recommended anymore.
• Data from rabies-endemic setting have shownthat even in the absence of RIG, withthorough wound washing plus immediatevaccination and completion of the PEP course > 99% patients survive.


Primary Regimens
Route Regimen Days
0 3 7 14 28
Previous WHO
Guidelines (2010)
IM Essen
Current WHO
Guidelines (2018)
IM Shortened
Essen

Primary Regimens
Route Regimen Days
0 3 7 14 21
Previous WHO
Guidelines (2010)
IM Zagreb
Current WHO
Guidelines (2018)
IM Zagreb
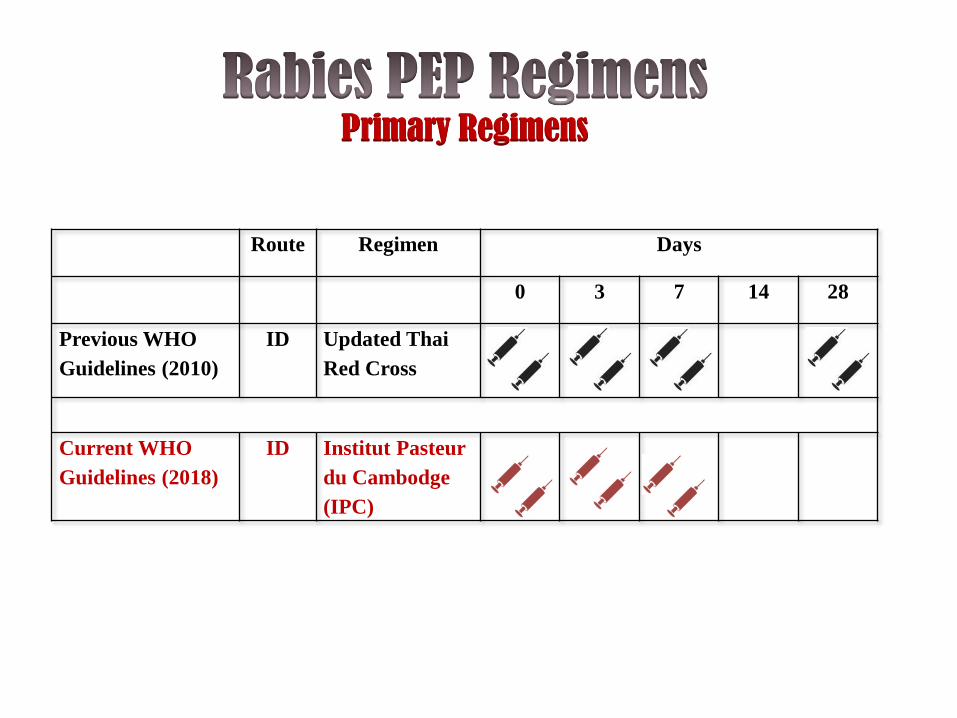
Primary Regimens
Route Regimen Days
0 3 7 14 28
Previous WHO
Guidelines (2010)
ID Updated Thai
Red Cross
Current WHO
Guidelines (2018)
ID Institut Pasteur
du Cambodge
(IPC)

Alternative Regimens (WHO 2018)
Route Regimen Days
0 3 7 14 28
1 ID
Updated Thai Red
Cross 2 2 2 0 2
2 ID
1-month,
simplified 4-site4 0 2 0 1
3 ID 1-week, 4-site4 4 4 0 0
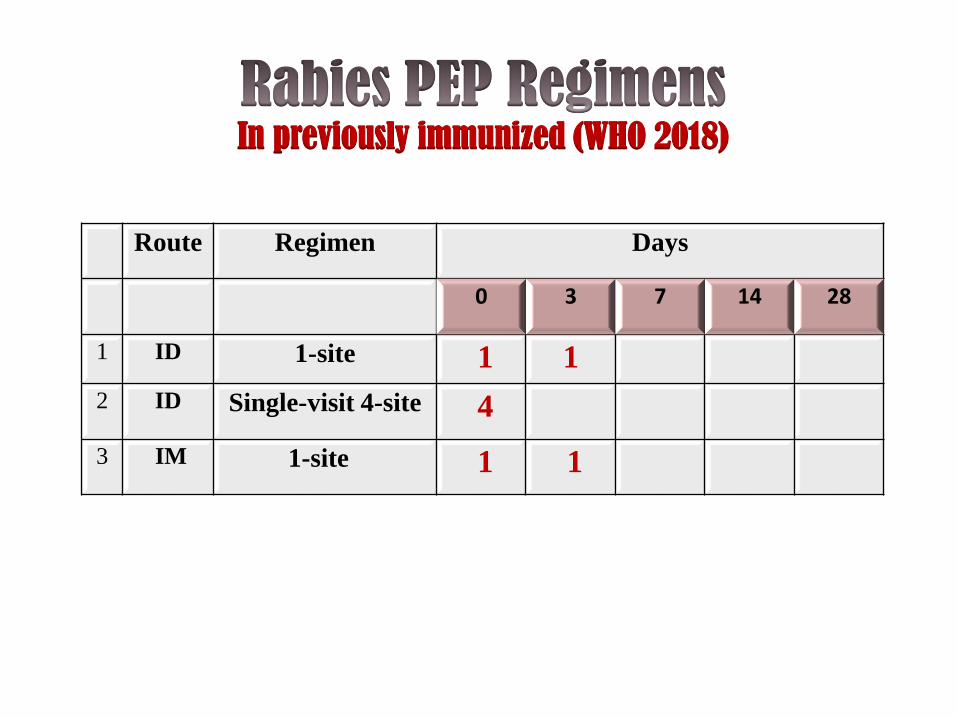
In previously immunized (WHO 2018)
Route Regimen Days
0 3 7 14 28
1 ID 1-site 1 1
2 ID Single-visit 4-site 4
3 IM 1-site 1 1

A few points
• PEP should be administered as soon as possible
• There is no time limit to administer PEP in case of type III exposure (however, if vaccine supply is limited, vaccine can be reserved for exposure that occured within 12 months)
• There are no contra-indications to PEP
• In case of repeted exposure < 3 months afterprevious PEP, only wound treatment isrequired

For dog, cat and ferret-related injuries
• If the animal remains healthy for 10 daysstarting from the date of the bite, PEP can bediscontinued
In any case
• When possible, suspect animals should behumanely euthanized and tested for rabies. PEP can be discontinued if the animal is proved by appropriate laboratory examination to be free of rabies

Potentially immunocompromizedpatients
• If CD4 < 200/mm3, use RIG in both category II and III exposure, even in previouslyimmunized patients.
• A 3-visit vaccination schedule should befollowed (ID or IM – D0, 7, 21-28) or a 2-visit schedule (ID or IM, D0, 7) with serologicaltesting 2-4 weeks after first rabies vaccine administration to assess whether an additional vaccine administration is needed.
