fraktur intertrokanter
DESCRIPTION
englishTRANSCRIPT
CLOSED FRACTURE LEFT INTERTROCHANTER OF FEMUR
PRESENTED BY :Ummu Asma' binti Mohd RosliC 111 10 877
ADVISOR :dr. Satria Prawira Putradr. Ery Wildan
SUPERVISOR : dr. M. Ruksal Saleh , Ph.D, Sp.OT(K)
Orthopaedic and Traumatology DepartmentMedical Faculty of Hasanuddin University
Makassar 2015
CASE REPORT

PATIENT'S IDENTITY• Name : Mrs. AT
• Number Register : 045034
• Sex : Female
• Age : 69 years old
• Date of Admission : August 22nd , 2015

HISTORY TAKING• Chief complaint : Pain at left thigh
• Anamnesis : Suffered since 3 days before admitted to the Hasanuddin University hospital after fell in toilet.
• Mechanism of Trauma : Patient cannot walk properly due to Parkinson's disease. she suffered
this disease since 2 years ago, and controlled with Sinemet, 3 times daily.
she walk with her walking stick. she accompanied by her maid everyday. because her maid was not
around that day, she tried to go to toilet by herself, and fell onto toilet floor on her left thigh. because her children was not around, she stay at home for 3 days before admitted to RSUH.
No prior treatment

GENERAL STATUS
General condition : wellnourished,compos mentis (GCS 15)
Vital signs : BP = 130/80 mmHg; HR = 86x/minutes, reguler, palpable RR = 16x/minute T =36,5
NRS : 4/10

LOCAL REGIONLeft Thigh Region
Look There is deformity, there is swelling, no hematom
Feel There is tenderness
Move Active and passive movement of the hip joint cannot be evaluated
NVD • Sensibility is good. • Pulsation of the dorsal pedis artery are palpable.• Capillary refill time <2”

CLINICAL PHOTOS
LATERAL VIEW
ANTERIOR VIEW

LEG LENGHT DISCREPANCY
R LALL 90 cm 88 cmTLL 83 cm 81 cmLLD 2 cm

LABORATORY FINDING
◦ WBC : 10.227 x 103 mm3◦ RBC : 4.63 x 106 /mm3◦ HGB : 13.3 g/dL◦ HCT : 38.6 %◦ PLT : 246 x 103 /mm3

PHOTOOF FEMUR
AP/ LATERAL
FRACTURE

PELVIS PHOTO FRACTURE

DIAGNOSIS
CLOSED FRACTURE LEFT INTERTROCHANTER OF FEMUR

MANAGEMENT• IVFD RINGER LACTATE 20
DROP/MINUTES• ANALGESIC
• PLAN FOR ORIF DYNAMIC HIP SCREW

DISCUSSION
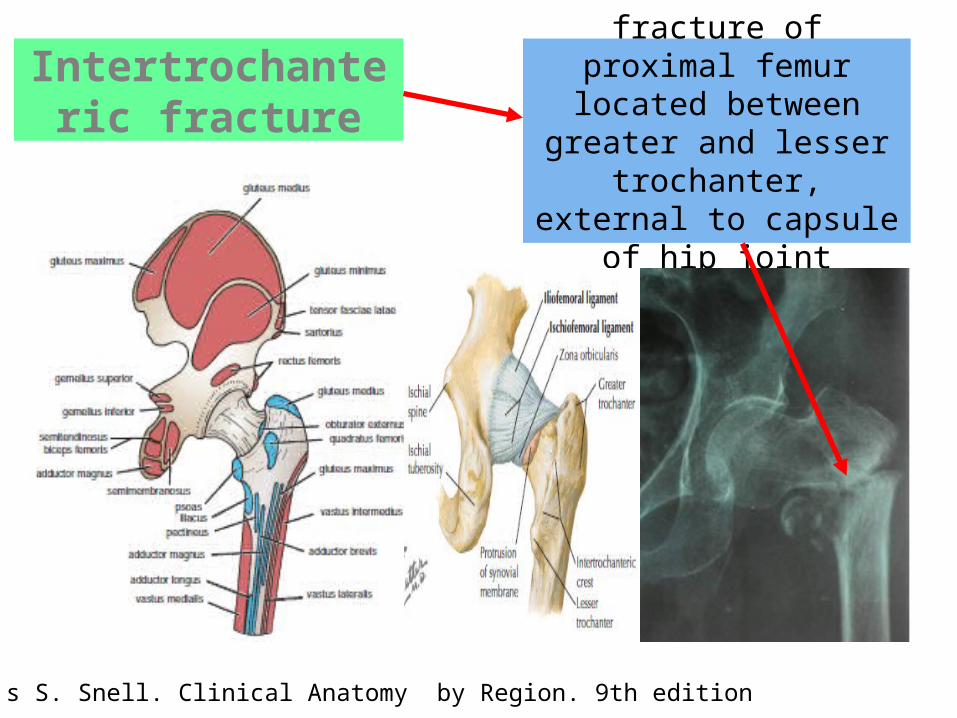
Intertrochanteric fracture
fracture of proximal femur located between greater
and lessertrochanter, external to
capsule of hip joint
Richard's S. Snell. Clinical Anatomy by Region. 9th edition

ARTERIES
NERVES
Netter Concise Orthopedic, 2nd edition, 2002

• women: men= 8 :1• age : 66-76 yo• unstable gait• direct impact to
greater trochanteric area(low energy fall)
PATIENT'S EVALUATIONTHEORITICALLY
mrs AT69 yohistory of Parkinson diseasefell on her left thigh on toilet floor directly
PATIENT'S
Koval, Kenneth j.; Zuckerman, joseph d. handbook of fractures, 4th edition
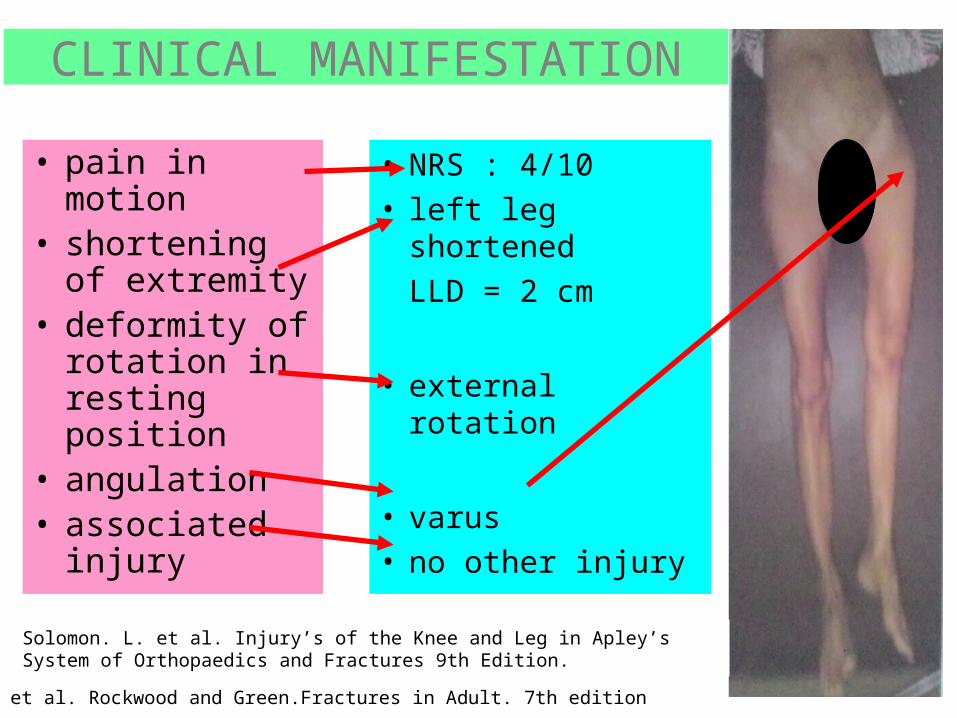
CLINICAL MANIFESTATION• pain in motion• shortening of
extremity• deformity of
rotation in resting position
• angulation• associated
injury
• NRS : 4/10• left leg shortened
LLD = 2 cm
• external rotation
• varus• no other injury
Robert et al. Rockwood and Green.Fractures in Adult. 7th edition
Solomon. L. et al. Injury’s of the Knee and Leg in Apley’s System of Orthopaedics and Fractures 9th Edition.

EVANS-JANSEN
OTA
classificationdegree of stability
degree of communition
BOYD AND GRIFFIN
Robert et al. Rockwood and Green.Fractures in Adult. 7th edition

OTA/AO classification
Robert et al. Rockwood and Green.Fractures in Adult. 7th edition
EVANS-JANSEN

Associated Diseases of Mrs. AT
• Parkinson's Disease - loss of dopaminergic neuron, altered calcium metabolism : poor bone density
• Osteoporosis - menopause, decrease estrogen, reduction BMD : pathologic fracture
mitochondria,calcium and cell death, BBA 1787(5) :335-44

Mrs. AT has history of Parkinson's Disease and taking Sinemet
What is Sinemet??
Levodopa (100 mg) + carbodopa (25 mg)
levodopa : metabolic precursor of dopaminecarbodopa : decrease peripheral conversion to
dopamine
Parkinsonism, Drugs that acts in the central system, Basic and ClinicalPharmacology, 11th ed
do not affect bone healing and do not lead to decrease of BMD

From radiologic exam, there is demineralisation of Mrs. AT's bone
Diagnosis : Osteoporosis senilis
woman69 yo

screening for osteoporosis
BMD (bone mineral density) measure calcium and other minerals
T-SCORE
NORMAL >-1,0
OSTEOPENIA -1.0-(-0,25)
OSTEOPOROSIS <-2,5
SEVERE OSTEOPOROSIS <-2.5 + HISTORY OF FRACTURE
WHO classification
X-RayPEHistory Taking
•CLOSED FRACTURE LEFT
INTERTROCHANTER OF FEMUR
•OSTEOPOROSIS•PARKINSON'S
DISEASE
EVIDENCES LEADING TO DIAGNOSIS

• ADMINISTER INTRAVENOUS FLUID• ANALGESIC
INITIAL TREATMENT

OPERATIVE TREATMENTOpen ReductionInternal Fixation
1. unstable fracture- reverse oblique2. to get the patient up and walking
as soon as possible 3. reduce the complications
associated with prolonged recumbency.
WHY?
dynamic hip screw
Robert et al. Rockwood and Green.Fractures in Adult. 7th edition

Gamma Nail
Implant of choice for Mrs. AT
unstable pathologicfracture
Lavini F et al.: The Treatment of Stable and Unstable Proximal Femoral Fractures with a New Trochanteric Nail: Results of a Multicentre Study with the Veronail. Strategies Trauma Limb Reconstr 2008 April; 3(1): 15–22.
protects the biological healing potential of the fracture site
minimises the classic complications of screw cut out, collapse and gait disturbance
The elasticity within the nail favours fracture healing (0% non-union rate)
may prevent secondary deformities

contraindication for operative treatment
non-ambulatory or chronic dementia patients with pain that is controllable with analgesics and rest
terminal disease with less than 6 weeks of life expected, unresolvable medical comorbidites that preclude surgical
treatment active infectious diseases that preclude insertion of a
surgical implant
Mrs. AT does not has any C/O for operation
Robert et al. Rockwood and Green.Fractures in Adult. 7th edition

Treatment for Associated Diseases• Parkinson's Disease : continue her drugs,
refer to Neurologist• Osteoporosis Senilis :
-Keep out of drugs lead to decrease BMD : steroid,anticoagulant,antipsychotic,anticancer-Morning sunlight : rich vit D (20-30 mins)-Biphosphonate-Hormone therapy (estrogen agonist or progesterone)
How to Manage Postmenopausal Osteoporosis? Acta Clin Belg 66(6) :443-7

Rehabilitation for Mrs. AT(Pathologic Fracture)
• Isometric exercise (0-3 days): contracts muscle by press heel on bed repeatedlypatient still in pain,continue this exercise
• Isotonic exercise (4-7 days) : passive movement of extremity (ROM) - only if the pain already diminished
• Isokinetic exercise (7 days-healed) :active movement of extremity - pain diminished and until joint can be used normally

Robert et al. Rockwood and Green.Fractures in Adult. 7th edition
COMPLICATION
IMPLANT MALFUNCTION
MALUNION
INFECTION
PNEUMONIA
BEDSORES
EMBOLISM

PROGNOSIS
• Quo at vitam : dubia• Quo at sanationam : dubia• Quo at functionam : dubia
