federal healthcare reform – what’s next? willis human capital practice legislative and...
TRANSCRIPT

Federal Healthcare Reform – What’s Next?Willis Human Capital PracticeLegislative and Regulatory Update
Jay M. Kirschbaum, JD, LLM, FLMIPractice LeaderNational Legal & Research Group
This material and any accompanying remarks are provided for informational purposes only and nothing contained in either should be taken as a legal opinion or as legal advice Copyright 2010 All rights reserved
2
When you come to a fork in the road
take it.
- Yogi Berra
3
Healthcare Reform Impact on employers, employees, insurers Immediate issues for employers and employees
New Notices Grandfathered Status - What is it and how meaningful is it? Preventive Services Mandate New Appeals Process Annual and Lifetime Dollar Limit Prohibition and Waiver Process Adult Child Guidance “Insurance Reforms” OTC Guidance
Q&A Future issues for employers and employees if time permits
Highlights included on slides
4
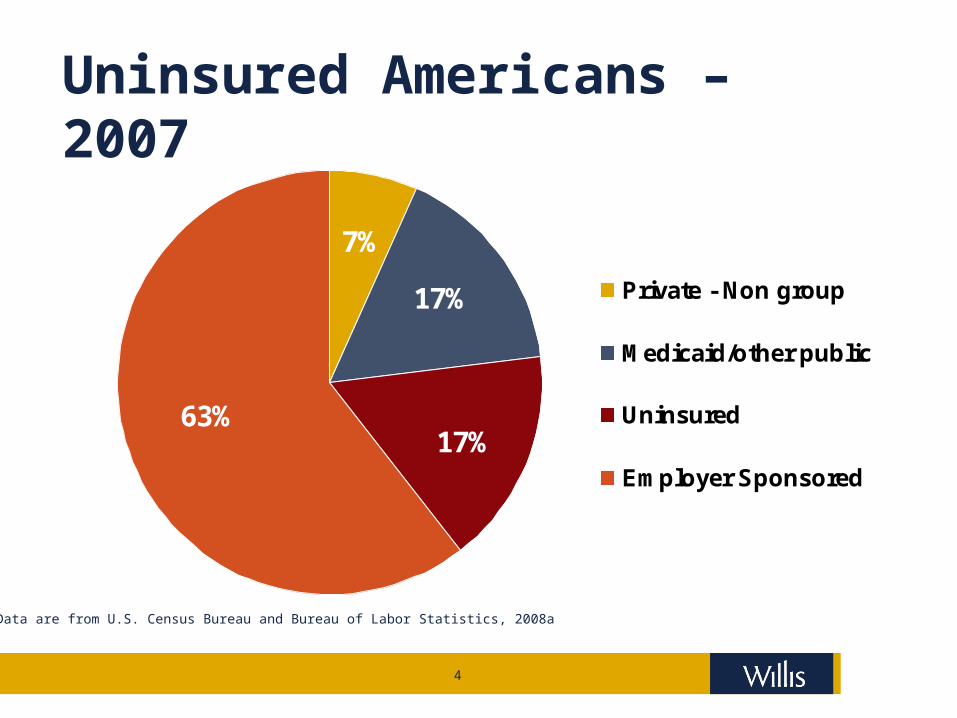
7%
17%
17%63%
Private - Non group
Medicaid/other public
Uninsured
Employer Sponsored
Uninsured Americans – 2007
Data are from U.S. Census Bureau and Bureau of Labor Statistics, 2008a
5
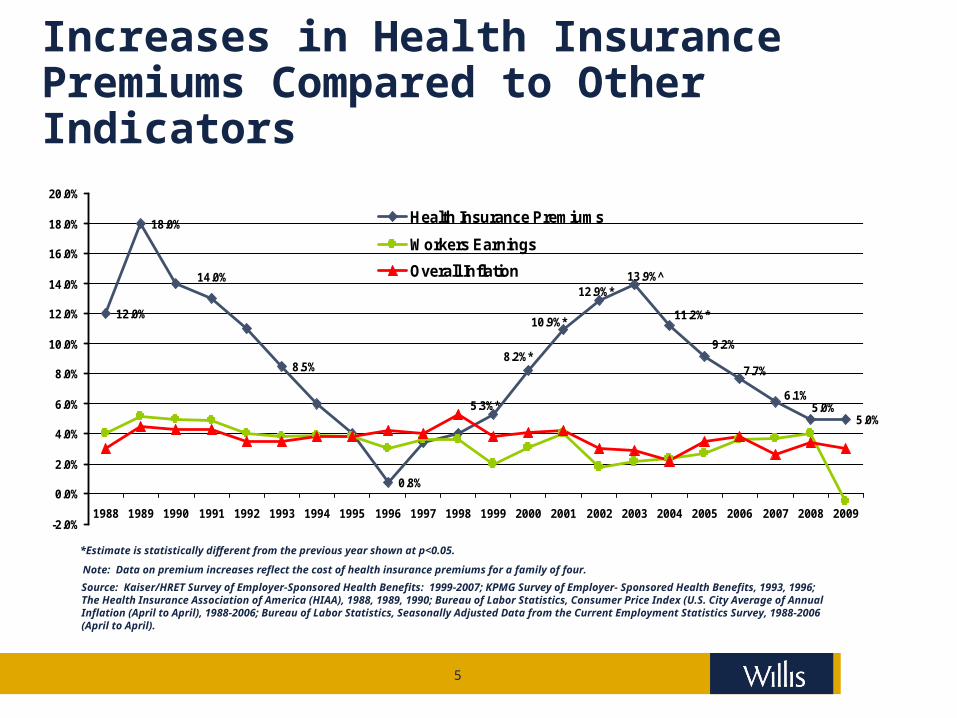
Increases in Health Insurance Premiums Compared to Other Indicators
Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits: 1999-2007; KPMG Survey of Employer- Sponsored Health Benefits, 1993, 1996; The Health Insurance Association of America (HIAA), 1988, 1989, 1990; Bureau of Labor Statistics, Consumer Price Index (U.S. City Average of Annual Inflation (April to April), 1988-2006; Bureau of Labor Statistics, Seasonally Adjusted Data from the Current Employment Statistics Survey, 1988-2006 (April to April).
*Estimate is statistically different from the previous year shown at p<0.05.
Note: Data on premium increases reflect the cost of health insurance premiums for a family of four.
12.0%
18.0%
8.5%
0.8%
5.0%5.0%
6.1%
7.7%
9.2%
13.9%̂12.9%*
5.3%*
14.0%
8.2%*
10.9%*11.2%*
-2.0%
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
18.0%
20.0%
1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Health Insurance Premiums
Workers Earnings
Overall Inflation

6

7
EXISTING MEASURES
Recent federal healthcare reform measures affecting employers
1996 HIPAA (portability,
nondiscrimination, standard electronic transactions, privacy, security, etc.)
MHPA NMHPA WHCRA
2003 MMA (HSAs and Medicare
Part D)
2008 GINA MHPA amendments Michelle’s Law MSP reporting
2009 CHIPRA ARRA (COBRA subsidy, breach
notification, comparative effectiveness research)
COBRA subsidy extension (does not seem to be in works again)
8
EXISTING MEASURES
Recent state healthcare reform measures affecting employers Mandates to cover older dependent children Pay or play statutes
San Francisco: Pay $X/hour toward healthcare under employer-sponsored plan or under public program‒ Supreme Court refused appeal‒ 9th Circuit decision stands and law remains in effect
Massachusetts: Make fair and reasonable contributions toward health coverage or pay a penalty‒ Also required to provide a cafeteria plan to avoid free rider
surcharge‒ Individual mandate subject to minimum coverage criteria‒ Connector
9
PPACA – Several Parts
Patient Protection and Affordable Health Care Act Passed by House March 21, 2010 Signed by President March 23, 2010
Reconciliation Bill - “Side car” (Health Care and Education Reconciliation Act of 2010) Passed by Senate with changes Passed by House March 25, 2010 Signed by President March 30, 2010
10
Post-Legislative Political Headlines
Financial Charge-Downs Announced by major employers Q1 adjustment to earnings
‒ Medicare Part D Rx subsidy becoming taxable‒ Ex: AT&T $1 Billion charge
State Lawsuits 20 Attorneys General filing lawsuits challenging the constitutionality of individual
insurance mandate Public reaction – Numerous polls negative
CBS News poll (conducted 3/29-4/1/10)‒ “53% of Americans disapprove of the new reforms, including 39% who say they
disapprove strongly“ Rasmussen – 9/4/10 (essentially unchanged since passage)
‒ 56% favor repeal (45% strongly)‒ 38% oppose repeal (30% strongly)‒ 51% feel it will be bad for the country‒ 37% feel it will be good
AHIP and HHS Dialogue “zero tolerance for this type of misinformation and unjustified rate increases”
Republican stance – defund the implementation
11
CHANCE FOR REPEAL AFTER NOVEMBER ELECTIONS? Essentially zero (Rassmussen and all other
pollsters) Senate seats up for election
‒ 18 – D‒ 18 – R
Republicans may gain majority in Senate (unlikely)‒ Biden tie-breaking vote
Even if gain majority in House (more likely but still no sure thing)‒ No credible chance to gain 2/3 votes
needed to overturn certain Presidential veto
Perhaps after 2012 Republican stance – defund the
implementation if gain majority
12
FEDERAL HEALTH CARE REFORM – OVERALL FINANCIAL IMPACT
13
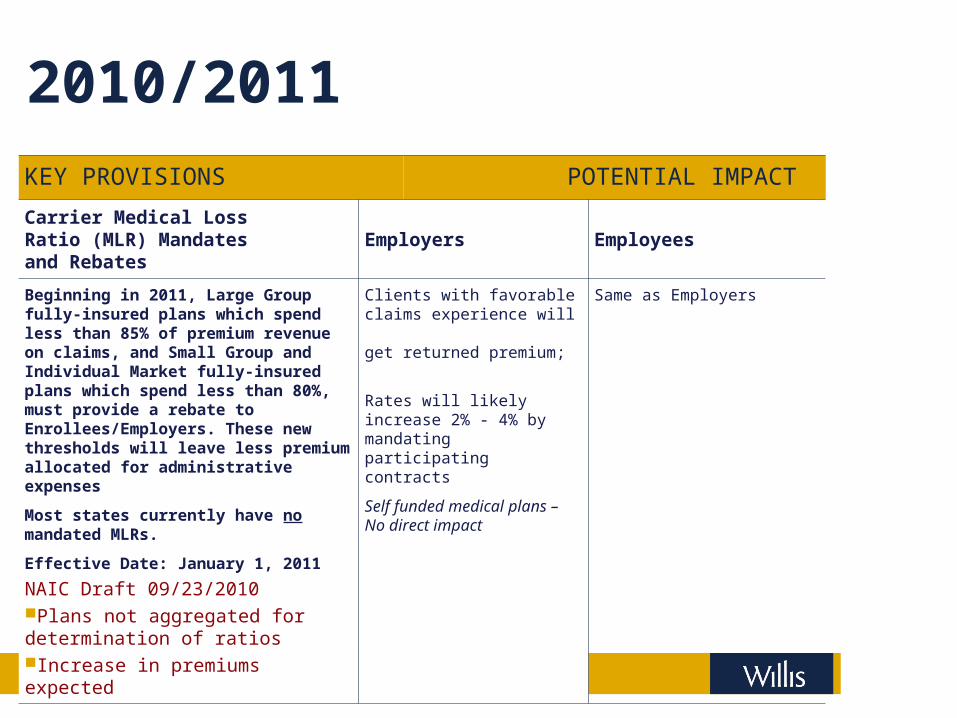
2010/2011KEY PROVISIONS POTENTIAL IMPACT
Carrier Medical Loss Ratio (MLR) Mandates and Rebates
Employers Employees
Beginning in 2011, Large Group fully-insured plans which spend less than 85% of premium revenue on claims, and Small Group and Individual Market fully-insured plans which spend less than 80%, must provide a rebate to Enrollees/Employers. These new thresholds will leave less premium allocated for administrative expenses
Most states currently have no mandated MLRs.
Effective Date: January 1, 2011
NAIC Draft 09/23/2010Plans not aggregated for determination of ratiosIncrease in premiums expected
Clients with favorable claims experience will get returned premium;
Rates will likely increase 2% - 4% by mandating participating contracts
Self funded medical plans – No direct impact
Same as Employers
14
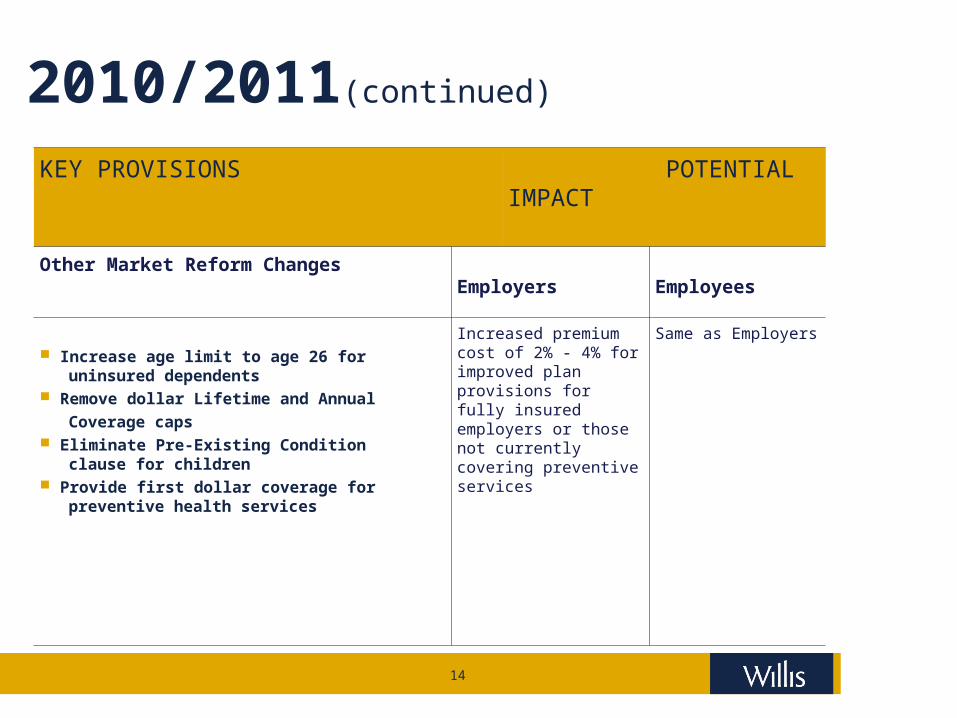
2010/2011(continued)
KEY PROVISIONS POTENTIAL IMPACT
Other Market Reform Changes Employers Employees
Increase age limit to age 26 for uninsured dependents Remove dollar Lifetime and Annual
Coverage caps Eliminate Pre-Existing Condition clause for children Provide first dollar coverage for preventive health services
Increased premium cost of 2% - 4% for improved plan provisions for fully insured employers or those not currently covering preventive services
Same as Employers
15
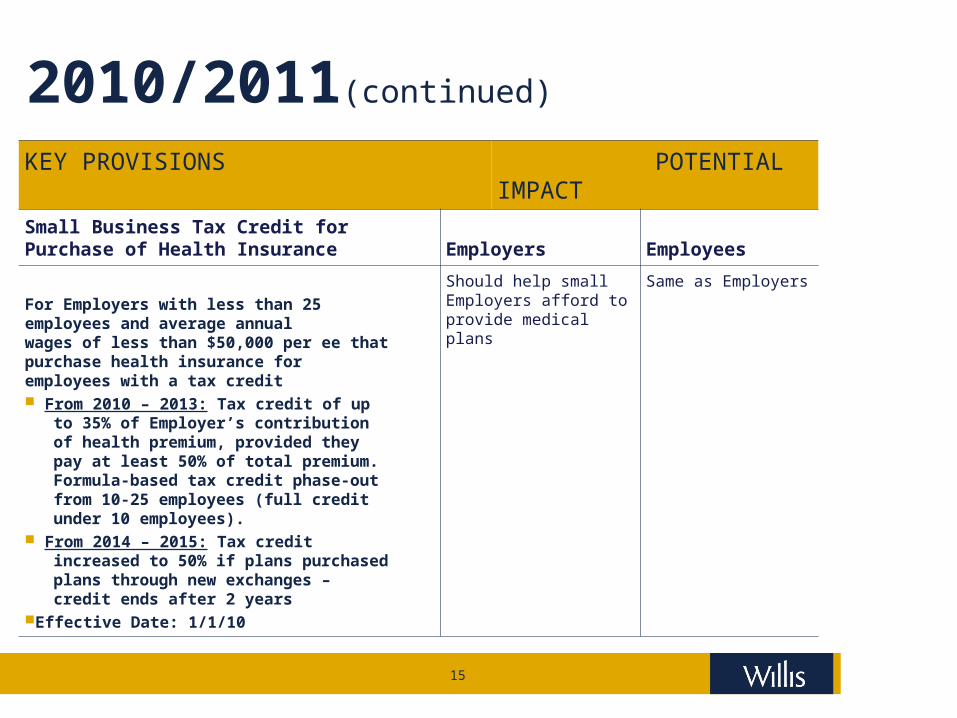
2010/2011(continued)
KEY PROVISIONS POTENTIAL IMPACT
Small Business Tax Credit for Purchase of Health Insurance
Employers Employees
For Employers with less than 25 employees and average annual wages of less than $50,000 per ee that purchase health insurance for employees with a tax credit From 2010 – 2013: Tax credit of up to 35% of Employer’s contribution of health premium, provided they pay at least 50% of total premium. Formula-based tax credit phase-out from 10-25 employees (full credit under 10 employees). From 2014 – 2015: Tax credit increased to 50% if plans purchased plans through new exchanges – credit ends after 2 yearsEffective Date: 1/1/10
Should help small Employers afford to provide medical plans
Same as Employers
16
What HR Will Be Asking/AskedHR Policy Issues and Questions* Short term impact between now and 2014? What steps do we take NOW to mitigate anticipated cost increases? Will employers eliminate group coverage and pay the penalties?
Push employees to the exchanges Reduce current expenses Negative impact on
‒ Recruiting and retaining talent and‒ Increase employee unrest‒ Concern with whether exchanges will actually work‒ Will employees be able to obtain comparable coverage at comparable cost?‒ What will the employer get for the $2,000?
Remember – tax benefits still apply! What steps to take between now and 2014 to position plans?
‒ Permit option to implement coverage if exchanges do not work? Consider different strategies for different lines of business
What is the long term strategic plan? Regardless of group benefits sponsorship, what will your strategies be to maximize health
and productivity?
*HR Policy Association Issues Brief provided initial questions for this slide
17
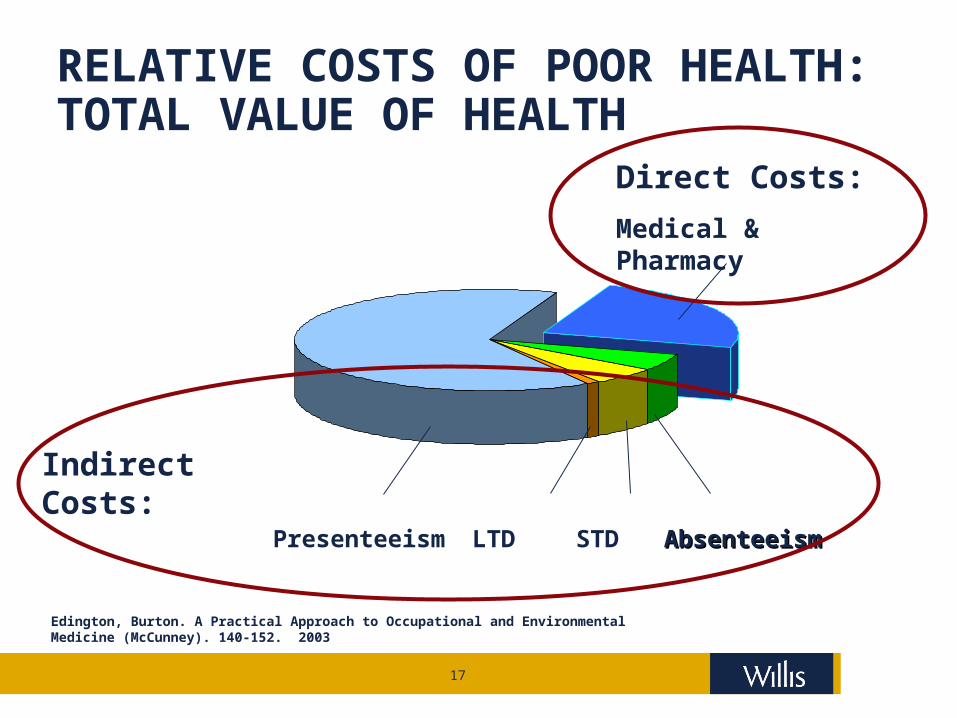
RELATIVE COSTS OF POOR HEALTH: TOTAL VALUE OF HEALTH
Presenteeism AbsenteeismAbsenteeismSTDLTD
Direct Costs:
Medical & Pharmacy
Indirect Costs:
Edington, Burton. A Practical Approach to Occupational and Environmental Medicine (McCunney). 140-152. 2003
18
FEDERAL HEALTH CARE REFORM – IMPACT ON PLAN COMPLIANCE
19
COMPLIANCE IMPACT Open Enrollment 2011New Notices Dependents Model Notice – if dependent coverage is offered Grandfather Model Notice – if grandfathered disclose impact Lifetime Limits Model Notice
General Periodic Notice Requirements Patient Protection Model Notice CHIPRA Model Notice WHCRA Model Notice General Notice of Pre-Existing Condition Exclusion HIPAA Special Enrollment Rights Sample Initial Notice of COBRA Continuation Rights
Provide COBRA Notice (required at enrollment). Compliance considerations for purposes of delivery of Initial Notice to spouse.
HIPAA Notice of Privacy Practices Provide HIPAA Notice of Privacy Practices (although not required, some employers
provide this every open enrollment). Model HIPAA 3-year Notice
provided every three years if new notice is not provided each year CMS Notification of SSN Refusal - Model Form
Provide CMS Group SSN Collection Form — when an employee and/or spouse refusesto provide an SSN to be provided to CMS (collect annually).
Michelle’s Law Sample Notice
20
GRANDFATHERED PLANS
21
Who are you going to believe, me or your own eyes?
- Chico Marx
22
GRANDFATHERED PLANS
What is a Grandfathered Plan? What is the Impact? Any group health plan or individual plan in existence as
of March 23, 2010 Some compliance exemptions – but only for insurance
reforms All grandfathered plans must meet minimum coverage
requirements for purposes of meeting the individual mandate
Regulations issued permit some minor changes to retain status Most plans will lose status Determine value of status
23
GRANDFATHERED PLANS
What is a Grandfathered Plan?
IRS – 26 CFR Parts 54 and 602
DOL – 29 CFR Part 2590
HHS – 45 CFR Part 147 Any group health plan or individual plan in which an
individual was enrolled on March 23, 2010 (as long as it
maintains that status under the rules of the IFR) Applies to each benefit package (undefined) Does not lose status just because people (even all) who were enrolled on
3/23/2010 cease to be enrolled New policy, contract or certificate after 3/23/10 (FAQ – Will address
this in future guidance) Loses grandfathered status Special rule for collectively bargained plans
24
GRANDFATHERED PLANS
What is a Grandfathered Plan (cont)? Family members and new employees can join Anti-abuse rules
M&A‒ Principal purpose can’t be to use grandfather
Change in plan eligibility‒ Transfers must be for bona fide employment based reason
25
GRANDFATHERED PLANS
Maintenance of Grandfathered Status? Disclosure mandate Documentation requirement Changes that will cause plan to lose grandfathered status
Elimination of benefits‒ To diagnose or treat a particular condition
Increase in percentage cost-sharing (co-insurance) Increase in fixed-amount cost-sharing other
than a copayment (deductible or OOP) Increase in fixed-amount copayment
‒ More than $5 + medical inflation (since 3/23/10)‒ And more than medical inflation (currently .3%) plus
15% (since 3/23/2010) New policy, contract or certificate after 3/23/10 (may
change with new guidance)
26
GRANDFATHERED PLANS
Maintenance of Grandfathered Status (cont.) ? Changes that will cause plan to lose grandfathered status (cont.)
Decrease in contribution rate (by more than 5 percentage points)‒ Based on employer’s cost of coverage‒ Based on formula
Changes in annual limits‒ Adding limit or decreasing current
Decrease in lifetime limits Value of grandfathered status?
Uncertain Calculate value of status vs. need for design
changes
27
ISSUES AFFECTING EMPLOYERS AND PLANSRequirements and Prohibitions Effective first day of the first plan year that starts on or after
September, 23, 2010 Grandfathered and non-Grandfathered plans
No lifetime dollar limits on essential benefits No rescissions (retroactive revocation of coverage) except for
fraud/intentional misrepresentation of a material fact No annual limits on dollar value of “essential health benefits”
‒ Except as permitted by HHS until 2014 Must cover children of covered individual up to age 26
‒ No tax dependent requirement‒ Married/unmarried‒ Not child or spouse of dependent‒ Tax favored basis‒ Up to 1/1/2014 grandfathered plans can exclude if eligible for employment
based coverage (other than a parent’s plan) No pre-ex condition exclusions for enrollees under 19 (applies to all for 2014
plan year) Amend plan and SPD, prepare for 2011 open enrollment
28
ISSUES AFFECTING EMPLOYERS AND PLANSAdult child coverage mandate Applies only if plan provides dependent child coverage Applies to:
Major medical Health reimbursement arrangement Limited medical (or mini-med) – but see below
Excluded (HIPAA-portability excepted) Retiree only Dental and vision if “stand alone” Health flexible spending account Health savings account Long-term care Specified disease (cancer, etc.) Fixed/Hospital indemnity Supplemental Disability On-site clinics
Applies for children (as defined) but not dependents

29
ISSUES AFFECTING EMPLOYERS AND PLANSAdult child coverage mandate Applies for children (as defined) but not dependents
Includes natural sons and daughters, step-children, foster and adopted children.
DOL Website Posting (9/21) - Grandchildren and others not so defined‒ Can be covered by plan (even as a dependent)‒ Adult child rules will not be mandatory‒ Plan permitted to cover them in the same way
30
ISSUES AFFECTING EMPLOYERS AND PLANSRequirements and Prohibitions-cont. Effective first plan year starting on or after September, 23, 2010 Non-Grandfathered plan—same as grandfathered plus
Requirement for coverage of certain preventive health services and immunizations without cost to covered individuals*
Insured plans subject to nondiscrimination rules currently applicable to self insured plans
Cover dependent child through age 26‒ Cannot exclude those with other employment based coverage*
Implement and provide notice of available internal and external appeals processes*
Allow participants to choose any primary care provider available to them* Choice of pediatrician as child’s primary care provider* Access to emergency services* Access to obstetrical and gynecological care* Wellness programs may not require disclosure/collection of information
relating to presence of firearms and benefits cannot be based on firearm ownership
Plan documents and SPD - does not apply necessarily to grandfathered plans
*Amplified in recent regulation
31
PREVENTIVE SERVICES COVERAGE MANDATENon-grandfathered plans may not impose any cost-sharing for preventive services Rating of A or B by US Preventive Services Task Force
Immunizations that meet recommendations of Advisory Committee on Immunization Practices of the CDC
Infants, children and adolescents - preventive care and screenings in guidelines by the Health Resources and Services Administration (“HRSA”)
Women - any other preventive care and screenings as provided in the HRSA guidelines (not yet issued)
32
PREVENTIVE SERVICES COVERAGE MANDATENon-grandfathered plans may not impose any cost-sharing for preventive services Exceptions
Office visits – ‒ if billed separately, can apply co-pay or deductible‒ If not billed separately, and primary purpose is for preventive care, no cost-
sharing Out-of-Network Providers
‒ Plan not required to pay for OON provision of services‒ Plan not prohibited from imposing OON cost-sharing even for preventive
services “Reasonable” medical management permitted Services not described – can be provided with cost-sharing
33
PREVENTIVE SERVICES COVERAGE MANDATENon-grandfathered plans may not impose any cost-sharing for preventive services Miscellaneous
Effective plan years starting on or after 9/23/2010 or, if later, one year after recommendation or guideline is issued
Changes to guidelines or recommendations – ‒ Plan can stop providing the services if they are no longer recommended‒ May have to give advance notice
34
INTERNAL AND EXTERNAL APPEALS PROCESSNon-Grandfathered plans must implement internal and external appeals process
Effective for plan years starting after 9/23/2010
Internal Appeals – based on ERISA required procedures Must adhere to internal appeals rules or deemed exhausted Meaning – claimant can go directly to external appeals or court
External Appeals – DOL Tech Release - Issued 8/23/2010 Insured plans – not employer responsibility
State process for insurance issuers – not ERISA plan/employer responsibility If available, they can be used, otherwise new federal rules apply
Self-insured plans If subject to state requirements (church, government plans, MEWAS)
‒ If state rules available, they can be used, otherwise new federal rules apply Self- funded, non-grandfathered ERISA plans
‒ New federal rules apply
35
INTERNAL AND EXTERNAL APPEALS PROCESSNon-Grandfathered plans must implement internal and external appeals process Internal Claims appeal IFR issued 7/22/2010 Adverse benefit determination
Includes rescission (retroactive termination of coverage) Does not include eligibility
Urgent Care Claims – must be decided as soon as possible, but no longer than 24 hours
Procedural criteria Provide, in advance, new or additional evidence considered Disclose, in advance, any new rationale for denying claim Avoid conflict of interest – reviewers cannot be chosen on likelihood of
upholding initial adverse benefit determination or paid bonuses based on claims denied
36
INTERNAL AND EXTERNAL APPEALS PROCESSNon-Grandfathered plans must implement internal and external appeals process External Appeals (cont.) Procedural criteria (continued)
Notice requirements‒ Culturally and linguistically appropriate‒ Additional identifying information regarding claim (such as date of service,
amount of claim, etc.)‒ Additional information regarding claim denial (such as denial code and
meaning)‒ Contact information for health insurance commissioner or ombudsman‒ Strict adherence to internal process or internal process deemed exhausted
37
INTERNAL AND EXTERNAL APPEALS PROCESSDOL Technical Release – applies as safe harbor until further guidance Plan must consider request for external appeal if filed within 4 months of final adverse benefit decision
Preliminary review by plan Required within 5 days of receipt Must determine
Claimant covered by plan Denial based on ineligibility (not subject to external review) Claimant exhausted internal review process if required Claimant provided all necessary info to process review Within 1 day of determination must inform claimant, in writing, if request is not
eligible or incomplete
38
INTERNAL AND EXTERNAL APPEALS PROCESSDOL Technical Release – applies as safe harbor until further guidance Consideration of external appeal – ineligible or incomplete If not eligible, must include reasons and EBSA contact info In not complete, must describe info necessary to complete Claimant has remainder of 4 months or 48 hours (whichever is greater) to cureIf eligible for external review – assign to independent review organization (IRO) Must have at least three accredited IROs available and other rules to prevent
bias If IRO reverses, plan must immediately provide coverage or pay claimTech Release 2010-02 Enforcement grace period until 07/01/2011 for some changes
Urgent care determination timeframe Culturally and linguistically appropriate notices Broader content and specificity requirements Substantial compliance
39
LIFETIME AND ANNUAL LIMITSLifetime and annual dollar limits on “essential health benefits” prohibited Dollar limits on non essential benefits permitted Applies to dollar limits
Silent on other types of limits Presumption that number of visits, number of procedures, limits on cost per
procedure, etc., are permissible Annual limits phased in
$750,000 - Plan years starting on or after 09/23/2010 $1,250,000 - Plan years starting on or after 09/23/2011 $2,000,000 - Plan years starting on or after 09/23/2012 No limits - Plan years starting on or after 01/01/2014
Limited Medical (“mini-med”) – HHS may waive annual limits for plan years starting before 01/01/2014 if limits would result in Significant decrease in access to benefits or Significant increase in premiums for plan or coverage

40
LIFETIME AND ANNUAL LIMITSLifetime and annual dollar limits on “essential health benefits” prohibited Essential benefits in legislation – no further clarification, yet, in regulations
Ambulatory patient services Emergency services Hospitalization Maternity and newborn care Mental health and substance use disorder services, including behavioral
health treatment Prescription drugs Rehabilitative and habilitative services Laboratory services Preventive and wellness services and chronic disease management Pediatric services, including oral and vision care
IFR permits interpretation of essential health benefits based on “good faith efforts” to comply with a “reasonable interpretation” as long as that is consistently applied
41
LIFETIME AND ANNUAL LIMITSLifetime and annual limits on “essential benefits prohibited” (cont.) Excluded benefits
Health (NOT dependent care) FSA, MSA, HSA Integrated health reimbursement arrangement (HRA) Retiree-only plans (including HRA) Any HIPAA-excepted benefits (limited scope dental & vision, specified
disease, hospital fixed indemnity, supplemental) Stand-alone HRA – comments requested
Participant or beneficiary previously met lifetime limits Must provide notice and, if not currently enrolled, open enrollment period (of
at least 30 days) For first plan year starting after 09/23/2010
‒ Model notice from DOL‒ Can be included with annual enrollment materials if the notice is
“prominently” displayed If enrolled but some plan options not available, must permit to choose among
all coverage options generally available under the plan
42
WAIVER PROCESS FOR LIMITED BENEFIT (“mini-med”) PLANS
Waiver Requirements Insurers can apply for contract and applies to holders Plan offered prior to 9/23/10 for plan year beginning between 9/23/10 and
9/23/11 Application must be submitted not less than 30 days before the beginning of
such plan year Plan or policy year that begins before 11/02/10 not less than 10 days before
the beginning of such plan year Plan administrator or CEO should retain documents in support of application
for potential examination by the Secretary HHS will process complete waiver applications within 30 days of receipt
Pre 11/02/10 plan years processed at least 5 days prior to plan year Waiver applies only for the 9/23/10 plan year
Plan must reapply for subsequent plan years prior to 1/1/14
43
WAIVER PROCESS FOR LIMITED BENEFIT (“mini-med”) PLANS
Waiver Requirements (cont.)
The application must include: Terms of the plan for which waiver is sought; Number of individuals covered by the plan submitted; Annual limit(s) and rates applicable to the plan submitted Brief description of why compliance with IFR would result in a
significant decrease in access to benefits for those currently covered by such plans or significant increase in premiums paid by those covered by such plans along with any supporting documentation; and
Attestation, signed by the plan administrator or Chief Executive Officer of the issuer of the coverage, certifying plan was in force prior to 9/23/10; and application of restricted annual limits to the plan would result in
significant decrease in access to benefits or significant increase in premiums paid
44
PHYSICIAN AND OTHER PROVIDER CHOICESPhysician and other provider choice issues Participant can choose as primary care provider
Any network primary care provider available (excluding specialists) Any network pediatrician available (for children)
Women can see health care professional in ob/gyn without preauthorization or referral Not required to be a physician Plan can require further treatment to be subject to authorization or referral
Plan must provide notice of these rights Model notice from DOL Also must be in SPD
45
EMERGENCY SERVICES
Plan must provide emergency services Without prior authorization (in and out of network)
But can require notification Benefit reduction for failure to obtain authorization violates this provision
Out of network co-payments and co-insurance can be no more restrictive than in-network
Rules set minimum standards for amount of payment for OON services But, remaining balance for OON services can still be enrollee’s responsibility
Deductibles and out-of-pocket limits for OON services can differ from in-network But – cannot apply separately for emergency services Example - $250 deductible for in-network and $500 OON. Can apply $500 to
emergency (as long as it is not only for emergency)
46
PREEXISTING CONDITIONS EXCLUSIONSPreexisting Condition Exclusions Prohibited Relatively small impact on employer plans (vs. individual coverage) given
HIPAA applications Limited time, only if 63 day break, etc. But there are additional restrictions
Preexisting condition exclusions entirely eliminated All participants
‒ Plan years starting on or after 01/01/2014 Enrollees under age 19
‒ Plan years starting first plan year that begins on or after 09/23/2010 (01/01/11 for calendar year plans)
Treatment requirement eliminated Cannot refuse treatment or coverage for any condition present prior to
effective date of coverage regardless of prior medical advice, diagnosis, care, or treatment
47
PREEXISTING CONDITIONS EXCLUSIONSPreexisting Condition Exclusions Prohibited (cont.) Applies to health status generally
Cannot deny coverage of conditions of individual based on information before effective date of coverage including pre-enrollment questionnaire, physical examination, or review of records
Does NOT require plan to provide coverage for conditions that would otherwise be excluded just because it arose prior to the effective date of the coverage
48
RESCISSIONS
New requirement regarding rescission of coverage (vs. revocation) Generally, plans cannot “rescind” coverage once an enrollee is covered Exceptions
Acts or practice by the covered individual consisting of fraud or intentional misrepresentation of a material fact ‒ No clarity on “material” or intent‒ Inadvertent omission or unintended misrepresentation will not permit a
recession Nonpayment of premiums
Cancellation permitted (not retroactive so not a rescission of coverage) Withdrawal from the market of the issuer or product (applies mainly to
insurance providers) Relocation outside service area Cessation of membership in sponsoring organization

49
RESCISSIONS
New requirement regarding rescission of coverage (vs. revocation) (cont.) Applies to “rescission”
Cancellation or discontinuance of coverage that has a “retroactive effect”‒ Void as of any date before the cancellation‒ Voids benefits paid prior to cancellation
Cancellation that applies prospectively is not a rescission (so not prohibited) Can also rescind retroactively if it is attributable to failure to pay premiums
for the period of coverage Advance notice required, when rescission is allowed
50
OTHER REQUIREMENTS
2011 Changes apply to Grandfathered and non-Grandfathered plans Health insurers report medical loss ratio to HHS and provide rebates to enrollees
if MLR is than 85% (80% for small groups) Auto enrollment for large employers (200 or more employees)
Immediate/retroactive effective date – unlikely OTC medications cannot be reimbursed pre-tax from FSA, HSA, HRA or MSA
Amend plans and SPDs Non-qualifying distributions from HSA and
MSA penalty increase to 20% Review material for HDHP and HSA contributions (vendor resp.?)
W-2 reporting of the value of employer providedcoverage (issued in January, 2012) Gather data for reporting on 2011 coverage
‒ Work with payroll vendors for details‒ COBRA premium calculation for 2011 will be
critical for many purposes

51
OTC GUIDANCE ISSUED
Prescription defined: Written or electronic order for a medicine or drug meeting legal
requirement state in which medical expense incurred Issued by individual legally authorized Effective date 1/1/11 regardless of employer's plan year and grace
period, if any Reimbursements after 1/1/11 prohibited even if funds set aside in 2010 Does NOT apply to non medicines or drugs such as (equipment,
supplies or diagnostic devices) Ex. - crutches, bandages and
blood sugar test kits.
52
OTC GUIDANCE ISSUEDDebit cards The IRS will not challenge the use of health FSA and HRA debit cards
for expenses incurred through January 15, 2011 because of inability to comply with substantiation requirement of debit card usage.
Medical expenses other than OTC medicines or drugs can continue to be reimbursed through debit card.
Debit cards may continue to be used at pharmacies that do not have a qualifying Inventory Information Approval System, as long as the store satisfies the requirement that 90% of its gross receipts were for medical care expenses and substantiation is properly submitted.
Retroactive amendments to conform torequirements if adopted no later thanJune 30, 2011, is permissible
53
EARLY RETIREE REINSURANCE PROGRAMCommenced as of June 1, 2010 ERRP Provisions
Employment based plans‒ State or local government, employee organization, VEBA, multiemployer
Early retiree = age 55 but not Medicare eligible 80% of medical claim at least $15k not exceeding $90k Claims incurred between June 1, 2010 and
January 1, 2014 Tax free

54
EARLY RETIREE REINSURANCE PROGRAM ERRP Provisions (cont.)
Application process open Not first come first served Errors will cause application to be returned Conditions
‒ Cost savings programs for chronic or high cost conditions and fraud and abuse
‒ Restrictions on use of proceeds‒ Subject to audits‒ Certified by Secretary of HHS‒ Sponsor must have PHI agreement with plan or insurer‒ Document actual medical claims costs‒ Medical costs = health benefits (e.g., not long-term care)‒ Payments must lower plan costs not be returned to general revenues
55
SMALL EMPLOYER INCENTIVES2011 Simple Cafeteria Plans
Safe harbor from nondiscrimination rules for cafeteria plans (and benefits offered through a cafeteria plan)
All “nonexcludable” employees eligible to participate Certain minimum contribution requirements met Employed an average of 100 or fewer employees on business days during
either of the two preceding years Small employer tax credit
25 or fewer employees with average annual wages of less than $50,000 Tax credit up to 35% (25% for tax exempt employers) of the employer’s
contribution‒ employer contributes at least 50% of a benchmark premium
10 or fewer employees with annual wages of less than $25,000 will be eligible for full credit
Credits phase out as size and wage increases Determine if credit applies or if plan can be amended to come within limits

56
CLASS ACT
2011 Optional for employers
Government run voluntary long term care program‒ Once program begins, participating employers required to automatically
enroll employees who do not opt out and facilitate payroll deductions‒ Eff. in 2011, but HHS must provide guidance
Employees must opt-out of program—if not wanting to participate Pays cash benefits of an average $50 per day Five year vesting period before
benefits provided‒ Prepare additional payroll deductions
and opt-out election‒ Prepare and distribute employee
communications
57
MISCELLANEOUS - GENERAL AND NEW STUFF
1099 reporting PPACA §9006 application to all vendors of more than $600 Possible political fix – failed in amendment to Small Business Jobs Act of
2010 Politically unpopular so opponents look for ways to pass repeal of that
provision Additional benefit to self-employed Small Business Jobs Act of 2010 (HR 5297) -
§2042 – Deduction for health insurance costs in computing self-employment taxes in 2010

58
Post-2011 Issues
59
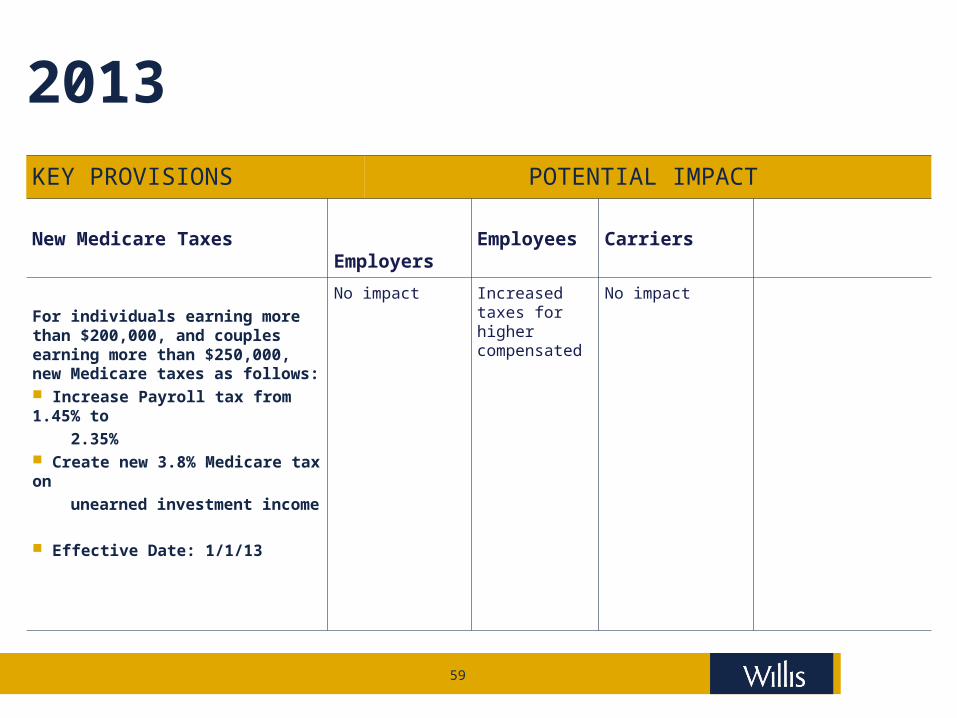
2013KEY PROVISIONS POTENTIAL IMPACT
New Medicare Taxes Employers Employees Carriers
For individuals earning more than $200,000, and couples earning more than $250,000, new Medicare taxes as follows: Increase Payroll tax from 1.45% to
2.35% Create new 3.8% Medicare tax on
unearned investment income
Effective Date: 1/1/13
No impact Increased taxes for higher compensated
No impact
60
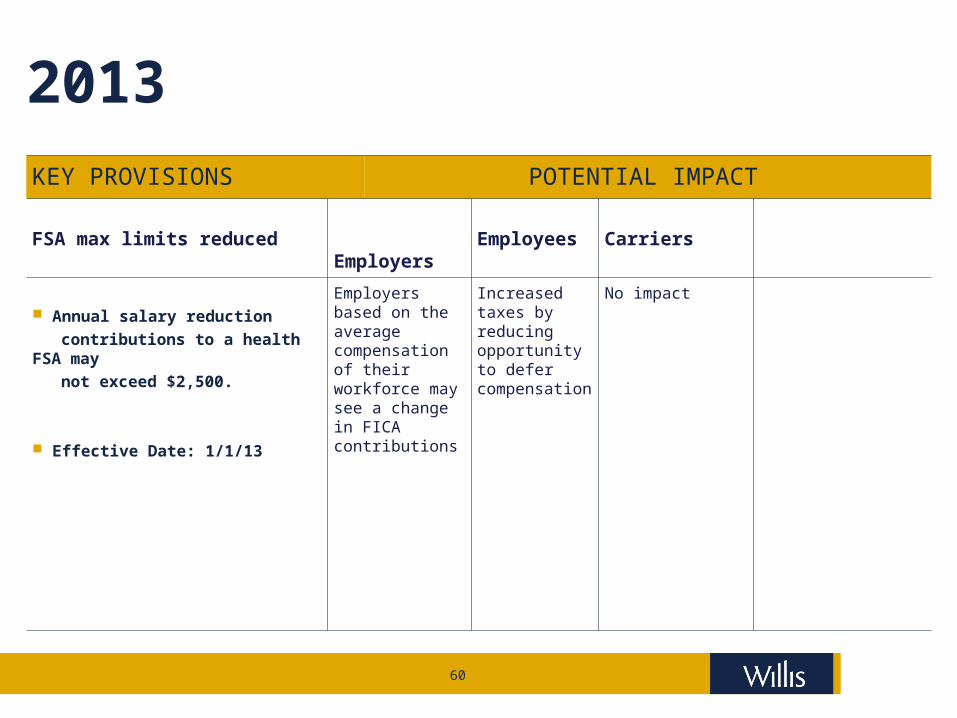
2013KEY PROVISIONS POTENTIAL IMPACT
FSA max limits reduced Employers Employees Carriers
Annual salary reduction
contributions to a health FSA may
not exceed $2,500.
Effective Date: 1/1/13
Employers based on the average compensation of their workforce may see a change in FICA contributions
Increased taxes by reducing opportunity to defer compensation
No impact
61
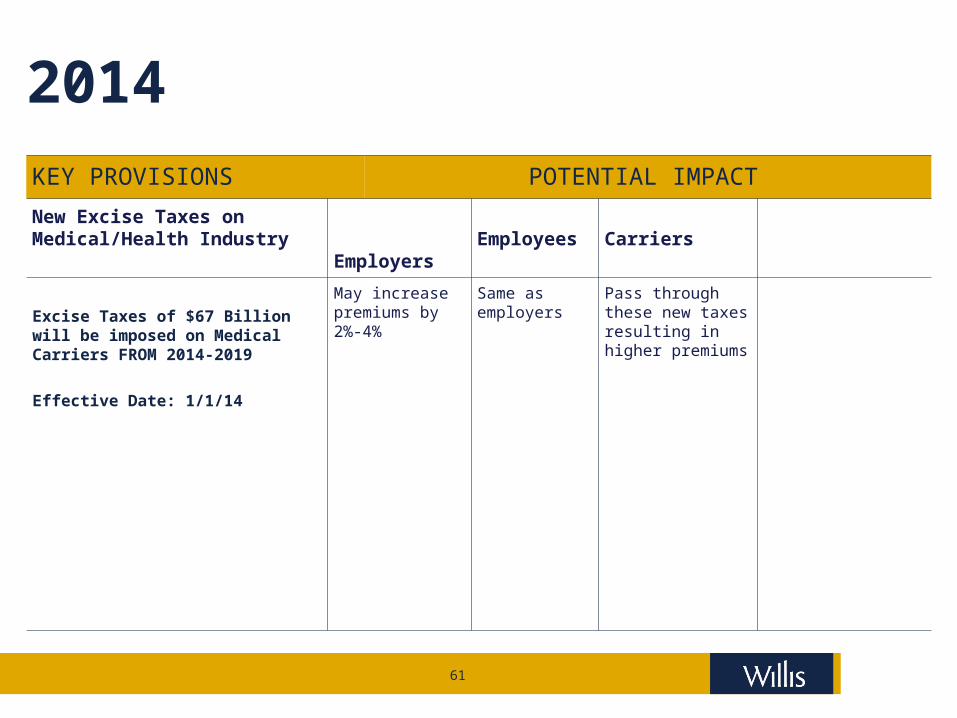
2014KEY PROVISIONS POTENTIAL IMPACT
New Excise Taxes on Medical/Health Industry
Employers Employees Carriers
Excise Taxes of $67 Billion will be imposed on Medical Carriers FROM 2014-2019
Effective Date: 1/1/14
May increase premiums by 2%-4%
Same as employers
Pass through these new taxes resulting in higher premiums

62
2014 (continued)
KEY PROVISIONS POTENTIAL IMPACT
Establishment of State-Based Insurance Exchanges
Employers Employees Carriers
State-based Insurance Exchanges will be established for individuals and small groups under 101 employees (In 2017, this access ceiling could be increased by each state). These exchanges will likely become the only market for these individuals and small Employers
Effective Date: 1/1/14
Could create lower cost options
Same as employers
May squeeze carrier pricing/ profitability further, but also provides access to newly covered enrollees
63
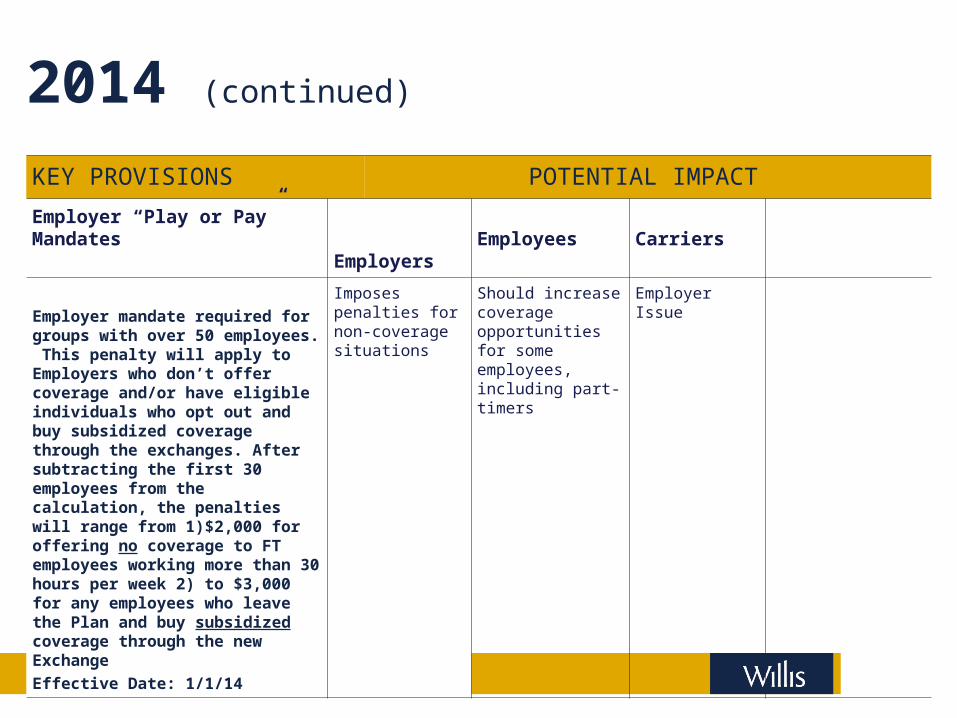
2014 (continued)
KEY PROVISIONS POTENTIAL IMPACT
Employer “Play or Pay” Mandates
Employers Employees Carriers
Employer mandate required for groups with over 50 employees. This penalty will apply to Employers who don’t offer coverage and/or have eligible individuals who opt out and buy subsidized coverage through the exchanges. After subtracting the first 30 employees from the calculation, the penalties will range from 1)$2,000 for offering no coverage to FT employees working more than 30 hours per week 2) to $3,000 for any employees who leave the Plan and buy subsidized coverage through the new Exchange
Effective Date: 1/1/14
Imposes penalties for non-coverage situations
Should increase coverage opportunities for some employees, including part-timers
Employer Issue
64
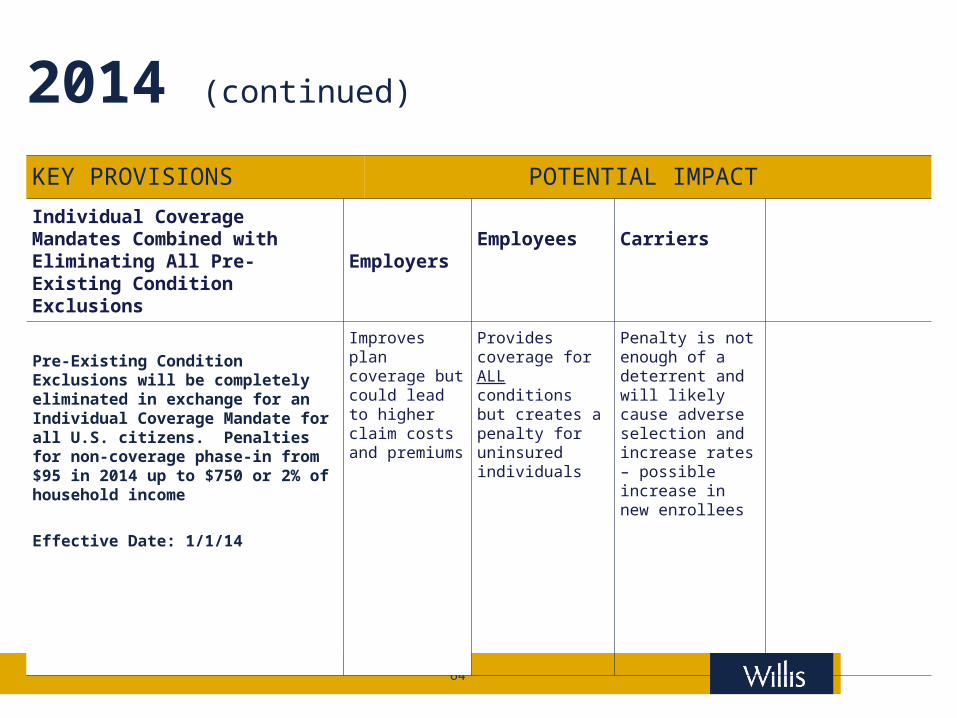
2014 (continued)
KEY PROVISIONS POTENTIAL IMPACT
Individual Coverage Mandates Combined with Eliminating All Pre-Existing Condition Exclusions
Employers Employees Carriers
Pre-Existing Condition Exclusions will be completely eliminated in exchange for an Individual Coverage Mandate for all U.S. citizens. Penalties for non-coverage phase-in from $95 in 2014 up to $750 or 2% of household income
Effective Date: 1/1/14
Improves plan coverage but could lead to higher claim costs and premiums
Provides coverage for ALL conditions but creates a penalty for uninsured individuals
Penalty is not enough of a deterrent and will likely cause adverse selection and increase rates – possible increase in new enrollees
65
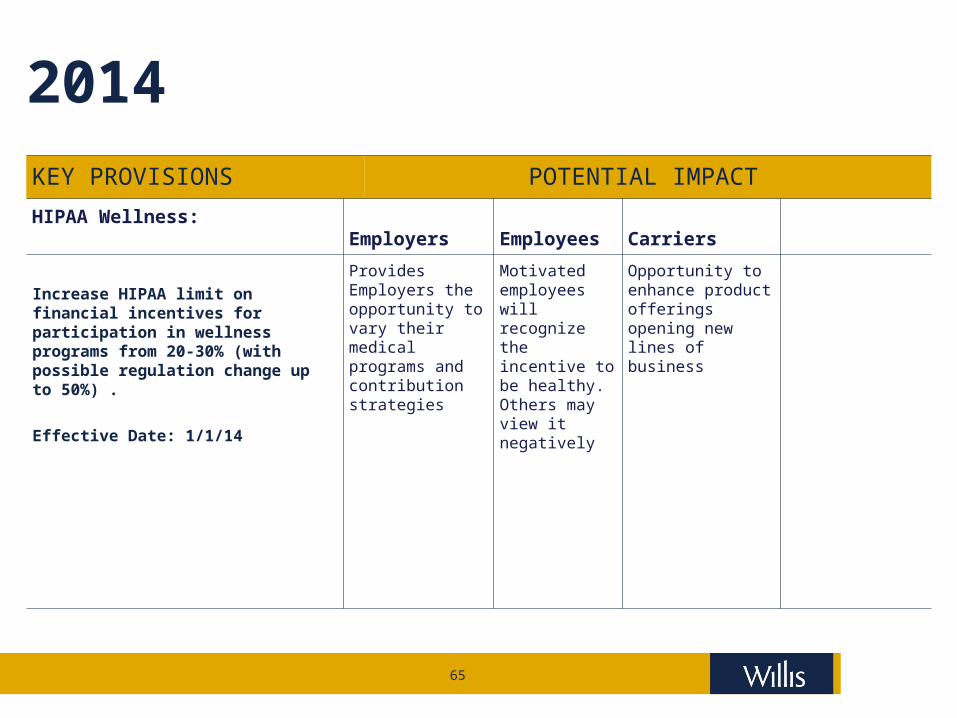
2014KEY PROVISIONS POTENTIAL IMPACT
HIPAA Wellness: Employers Employees Carriers
Increase HIPAA limit on financial incentives for participation in wellness programs from 20-30% (with possible regulation change up to 50%) .
Effective Date: 1/1/14
Provides Employers the opportunity to vary their medical programs and contribution strategies
Motivated employees will recognize the incentive to be healthy. Others may view it negatively
Opportunity to enhance product offerings opening new lines of business
66
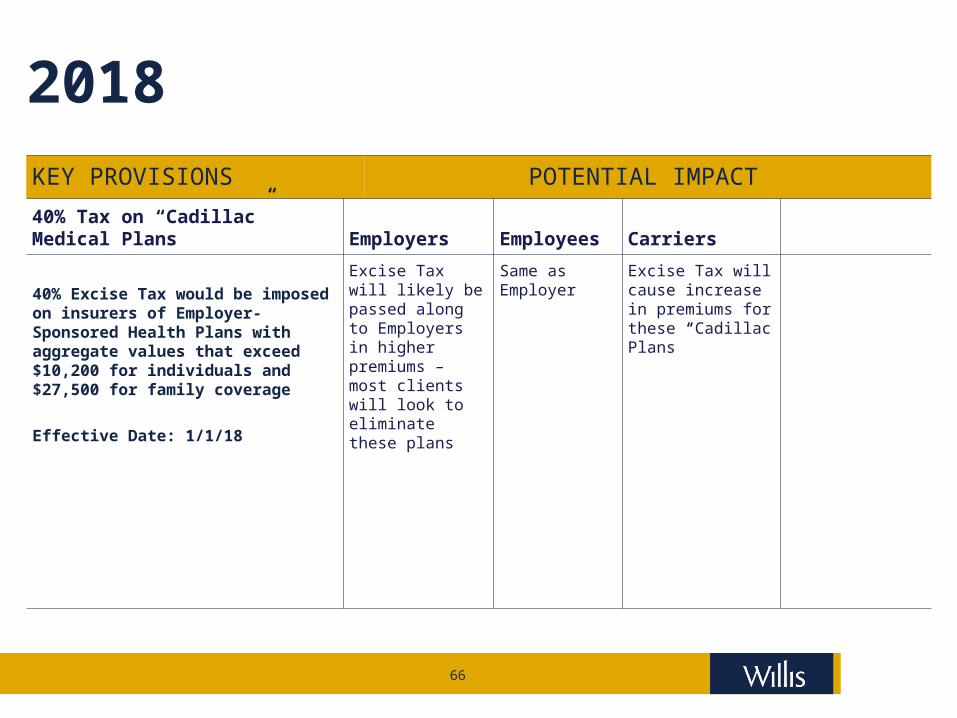
2018KEY PROVISIONS POTENTIAL IMPACT
40% Tax on “Cadillac” Medical Plans
Employers Employees Carriers
40% Excise Tax would be imposed on insurers of Employer-Sponsored Health Plans with aggregate values that exceed $10,200 for individuals and $27,500 for family coverage
Effective Date: 1/1/18
Excise Tax will likely be passed along to Employers in higher premiums – most clients will look to eliminate these plans
Same as Employer
Excise Tax will cause increase in premiums for these “Cadillac Plans”
67
MANDATED DISCLOSURE AND 1099 REQUIREMENT2012 Mandated disclosure requirement – HHS will issue format
Uniform explanation of coverage documents as of March 23, 2012‒ No more than 4 pages, using 12 point font‒ Culturally and linguistically appropriate manner‒ Information on covered benefits, exclusions, cost sharing, continuation‒ Notify of material coverage changes no less than 60 days in advance of
effective date 1099 Mandate
1099s for all corporate (health) service providers receiving more than $600
68
FUTURE ISSUES AFFECTING EMPLOYRS AND PLANS2013 FSA contributions capped at $2,500
Indexed to CPI Subsidy for retiree drug coverage eliminated
Allowable deduction reduced by tax-free subsidy Employer notice informing employees of State Exchange
If plan’s share of total allowed costs of benefits is less than 60% Availability of tax credit Availability of free choice voucher Current employees as of March 1, 2013 and subsequent new
hires
69
TAX CHANGES
2013 – Tax Changes Payroll tax increase
To .9% on earnings over $200,000 for individualsand joint filers over $250,000
Adds 3.8% tax on same individuals’ net investment income over $200,000/$250,000
‒ interest, dividends, royalties, rents, gross income from trade or business involving passive activities, and
net gain from disposition of property (other than property held in trade or business) - reduced by properly allocable deductions
Participant fee for comparative effectiveness research $1 per participant for first plan year ending after September 30, 2012 $2 per participant following year Not applicable to HIPAA exempt benefits Sunsets 1/1/2020
70
ADDITIONAL MANDATES
2014 Employer reports to IRS to enforce individual mandates
Coverage offered employees, length of waiting period, lowest cost option, actuarial value
Auto enrollment mandated for employer plans with 200 or more employees
Prohibits waiting periods greater than 90 days Wellness Programs will be able to increase incentives to 30% or up
to 50% if HHS approves
71
PAY OR PLAY MANDATE
Effective in 2014 Nondeductible penalty on some employer plans with 50 or more FT
(30 hours/week or more) employees Part time employee equivalents used to determine FT number First 30 FT employees excluded from tax Tax is $2,000 per FT employee if no coverage at all and at least
one employee receives tax credit for coverage on an exchange Tax is $3,000 per FT employee if employer DOES offer coverage
but employee receives tax credit for coverage on an exchange but no more than $2,000 X all employees
Seasonal employees are NOT excluded For the penalty, are to determine size of employer
72
VOUCHERS AND INDIVIDUAL MANDATEEffective in 2014 Vouchers
Employer must offer vouchers to permit certain employees‒ eligible under plan AND‒ required premium is between 8% and 9.8% of income AND‒ total household income does not exceed 400% of FPL
Voucher can be used to purchase coverage outside of employer plan and retain any excess tax free
Must equal the largest portion the employer provides toward type of coverage
No free rider penalty for employees receiving vouchers Individual mandate commences – fines for failure to purchase:
‒ $95 in 2014‒ $325 in 2015‒ $695 in 2016
Or‒ 1.0% of taxable income in 2014‒ 2.0% of taxable income in 2015‒ 2.5% of taxable income in 2016 and thereafter
73
INSURANCE REFORM MANDATESEffective in 2014 – Affects on all plans (grandfathered until
effective date) Mandated benefit package – determined by HHS Clinical trials for life threatening diseases (grandfathered plans
exempt) No discrimination of provider acting within scope of license No pre-existing condition exclusion No annual limits on essential benefits Cost sharing limitations-OOP does not exceed qualified HDHP coverage and deductibles do exceed $2,000/4,000 (grandfathered plans exempt) State insurance exchanges commence for individuals and small
businesses
74
INSURANCE EXCHANGES
Commence in 2017 State insurance exchanges commence for employers with more
than 100 employees
75
HIGH COST PLAN EXCISE TAX
Effective in 2018 Excise taxes on “Cadillac” plans
40% nondeductible tax Value of all employer – sponsored medical benefits in excess of:
‒ $10,200 for individual coverage‒ $27,500 for more than individual coverage
High risk occupations* and retirees‒ $11,850 individual‒ $30,950 more than individual
Indexed at CPI + 1% in 2019, CPI thereafter Active and retired employees
* Longshoremen, repair or install electrical or telecommunications lines, law enforcement, fire protection, EMT, construction, mining, agriculture (except not food processing), forestry and fishing
76
HIGH COST PLAN EXCISE TAX
2018 – Cadillac Plans – cont. Value includes
All medical coverage‒ Group medical‒ EAP‒ HSAs, FSAs, HRAs‒ Employer paid‒ Employee paid‒ Pre-tax‒ After-tax
Not disability or life
77
HIGH COST PLAN EXCISE TAX
Effective in 2018 – Cadillac Plans – cont. Excise tax on an individual basis
Threshold and tax calculated monthly Paid by the employer Based on COBRA determination amount Intent to keep employer plans under threshold so consider -
Reduce benefits? Reduce account based plans? Eliminate ancillary coverage?
78
QUESTIONS AND COMMENTS
Federal Healthcare Reform – What’s Next?Willis Human Capital PracticeLegislative and Regulatory Update
Jay M. Kirschbaum, JD, LLM, FLMIPractice LeaderNational Legal & Research Group
This material and any accompanying remarks are provided for informational purposes only and nothing contained in either should be taken as a legal opinion or as legal advice Copyright 2010 All rights reserved