evaluation of the greater saphenous vein with classification c2 e (ceap...
TRANSCRIPT

ORIGINAL ARTICLE
J Vasc Bras. 2012;11(3):187-193.
Amélia Cristina Seidel1, Leandro Pablos Rossetti2, Yara Juliano3, Neil Ferreira Novo3, Fausto Miranda Jr4
AbstractBackground: With the presence of venous reflux, there is need to evaluate the clinical severity by quantifying the hemodynamic effect of venous incompetence and definition of their anatomical distribution.Objective: To determine and correlate the degree of reflux of the greater saphenous vein (insufficiency) in a clinical CEAP C2/C3 by air plethysmography and color Doppler ultrasonography.Methods: We prospectively investigated 87 limbs with reflux of the greater saphenous vein as ascertained by Doppler ultrasonography and 32 limbs without signs or symptoms of the venous disease. All patients underwent clinical examinations using air plethysmography and Doppler ultrasonography of the lower limbs. The parameters used with the Doppler ultrasound were: the diameter of the saphenous vein (seven levels) and the speed and time of reflux. In the plethysmography, the venous filling index, ejection fraction and residual volume fraction were also considered.Results: Of the 119 limbs, 61 were class C2. In comparing the diameters of the vein of the control group with the study group there were statistically significant differences. There was an exception at the malleolus level. Using the Spearman correlation to analyze the indices for the plethysmography and Doppler ultrasound it showed some differences, but the coefficient of determination (r2) showed that they were weak.Conclusions: The parameters of the plethysmography did not correlate with the degree of reflux in the greater saphenous vein. There was a very weak correlation between their values, time and speed of reflux. Only the venous filling index correlated with venous reflux. The ejection fraction and residual volume fraction were not important for discrimination of clinical severity.
Keywords: saphenous vein; Ultrasonography, Doppler; plethysmography; varicose veins.
ResumoContexto: Com a presença de refluxo venoso, há necessidade de avaliar a gravidade clínica da doença pela quantificação do efeito hemodinâmico da incompetência venosa e definição de sua distribuição anatômica.Objetivo: Determinar a correlação da pletismografia a ar com o grau de refluxo pelo eco-Doppler na insuficiência da veia safena magna no quadro clínico C2 e C3 da CEAP.Métodos: Foram examinados, prospectivamente, 87 membros com refluxo da veia safena magna determinado pelo eco-Doppler e 32 membros sem sinais ou sintomas de doença venosa. Todos foram submetidos ao exame clínico, pletismografia e eco-Doppler de membros inferiores. Do eco-Doppler foram utilizados os parâmetros: diâmetro da veia safena em sete níveis, velocidade e tempo de refluxo. Da pletismografia foram considerados o índice de enchimento venoso, a fração de ejeção e a fração de volume residual.Resultados: Dos 119 membros, 61 pertenciam à classe C2. Na comparação do diâmetro da veia nos grupos controle e estudo houve diferença estatisticamente significante, exceto ao nível do maléolo. Utilizando-se a Correlação de Spearman para análise dos índices da pletismografia e eco-Doppler foram observadas algumas significâncias, porém o coeficiente de explicação (r2) mostrou que foram fracas.Conclusões: Os parâmetros da pletismografia não se correlacionam com o grau de refluxo na veia safena magna, pois houve uma correlação muito fraca entre seus valores e o tempo e a velocidade do refluxo. Somente o índice de enchimento venoso tem correlação com refluxo venoso. A fração de ejeção e de volume residual não se mostraram importantes na discriminação da gravidade clínica.
Palavras-chave: veia safena; ultrassonografia Doppler; pletismografia; varizes.
Evaluation of the greater saphenous vein with classification C2 e C3 (CEAP) by air plethysmography and color Doppler ultrasonographyAvaliação da insuficiência da veia safena magna com classificação C2 e C3 (CEAP) pela pletismografia a ar e pelo eco-Doppler colorido
From the Universidade Estadual de Maringá (UEM) Medical School – Maringá (PR), Brazil; and the Post-graduation Program of the Universidade Federal de Paulo (UNIFESP-EPM) – São Paulo (SP), Brazil.Paper presented at the VIII Panamerican Congress on Vascular and Endovascular Surgery, I Panamerican Venous Forum, V Symposium on Vascular Echo-color-Doppler, em 2004; e no 15th World Congress of the Union Internationale de Phebologie, 2005. Peter Gloviczki Award (2st place).1 Vascular Ultrasonographist from Brazilian Society of Angiology and Vascular Surgery (SBACV) and Colégio Brasileiro de Radiologia e Diagnóstico por Imagem (CBR); Adjunct Professor of Angiology and Vascular Surgery at UEM – Maringá (PR), Brazil.
2 Medical student at UEM – Maringá (PR), Brazil.3 Adjunct Professor of Biostatistics at the Department of Preventive Medicine of UNIFESP-EPM; Full Professor of Public Health at Universidade de Santo Amaro (UNISA) – São Paulo (SP), Brazil.4 Vascular Ultrasonographist from SBACV and CBR; Full Professor of Vascular Surgery at UNIFESP-EPM – São Paulo (SP), Brazil.Financial support: noneConflict of interest: nothing to declareSubmitted on: 26.07.11. Accepted on: 15.03.12.

APG and color Doppler ultrasound in GSV insufficiency - Seidel AC et al.J Vasc Bras 2012, Vol. 11, Nº 3188
Introduction
Chronic venous insufficiency is a common disease in medical practice1,2 that is characterized by a set of changes that may affect the skin and subcutaneous tissue, and is determined by valvular insufficiency and/or failure of the calf muscle pump3. This disease has a significant socioeconomic impact because its complications are an important cause of morbidity4. Several risk factors are associated with the development of chronic venous insufficiency, such as obesity, sex and age5.
Varicose veins represent only part of the spectrum of venous disease, which ranges from asymptomatic valvar incompetence to leg ulcer, which is severe in most cases6. Reflux is the leading cause of the disease, but its minimal occurrence to produce symptoms is not well known7.
The presence of venous reflux requires evaluation of the disease clinical severity, quantification of hemodynamic effect of the venous incompetence and definition of its anatomical distribution8.
Color Doppler ultrasonography allows accurate detection and quantification of the reflux in individual veins8, and the introduction of accelerated air plethysmography (APG) has provided a quantitative assessment of the severity of the chronic venous insufficiency (CVI) by non-invasive means6,9,10.
This paper aims to investigate the value of APG in the diagnosis of greater saphenous veins insufficiency and to determine its correlation with the anatomic distribution of the reflux identified by the color Doppler ultrasonographyin cases classified as C2 and C3 (CEAP).
Methods
In a four-month period, 352 patients with complaints compatible with venous disease were seen in a vascular laboratory. After clinical assessment, they were submitted to color Doppler ultrasonography and to APG of the lower limbs. Out of those 352 patients, 71 had GSV insufficiency classified as C2 and C3.
All participants signed the informed consent form, and the protocol was approved by the Ethics Committee (n. 0832/02).
This is a cross-sectional prospective study. Patients without history of venous surgery, deep vein thrombosis or phlebitis were included in Group E (study), and those who had limitation in the movements of the ankle, knee or other musculoskeletal changes that could interfere in the calf
venous emptying during exercises at APG were excluded. The study group was formed by 87 lower lims (56 females and 15 males), with ages ranging from 24 to 78 years.
Following the same inclusion and exclusion criteria of Group E, 16 subjects with no signs of current venous insufficiency were allocated in Group C (control). There were 14 females and 2 males, with ages ranging from 21 to 57.
CEAP classification11 was used for clinical evaluation of the venous disease. In Group E, patients presented reflux of primary etiology in the superficial system, being classified as C2-3EpAs2-3 Pr. Patients from Group C were classified as C0.
Color Doppler ultrasonography (Hewlett-Packard Image Point - Hewlett-Packard Co, Andover, Mass., USA) was performed to confirm the patency of the deep venous system of the lower limbs of patients and controls in the supine position. Then they were assessed in the standing position as to the presence of perforating veins, diameter of the GSV and the presence or absence of reflux in the superficial veins. Measurement of the GSV diameter was performed at seven different levels, and the first was considered in the inguinal region, 2 cm distal to the saphenofemoral junction, where the vein could be seen without any curvature. The fourth level was marked on the medial aspect of the knee at the interarticular line; the second and the third levels were located in the thigh, equidistant to the above-mentioned. The seventh level was close to the medial tibial malleolus and the fifth and sixth were located in the leg, also equidistant to the others.
We used the classification of the GSV reflux pattern described by Engelhorn et al.12, which is characterized by type I - perijunction reflux; II - reflux in the proximal segment (thigh); III - reflux in the distal segment (leg); IV - segmental reflux, and V – full-length reflux (thigh and leg). At spectral analysis, the retrograde flow of GSV was defined as reflux lasting longer than 0.5 second13 and systolic velocities greater than 25 cm/s.
In another room with temperature at 22-24 °C, APG (SDV 3000 appliance; Angiotec®) was performed based on the method described by Christopoulos et al.14, which provided record of venous filling index (VFI), ejection fraction (EF) and residual volume fraction (RVF) for the hemodynamic evaluation of the limb. Normal values were VFI <2 mL/s, EF> 60%, and RVF <40%.
Statistical analysis was performed using the Student’s t test for independent data to assess sample homogeneity, and the Spearman correlation was used to verify the results of APG and color Doppler ultrasound. The value is referred to as zero when two variables are totally independent, that is, there is no correlation between them; the maximum value of +1 is
APG and color Doppler ultrasound in GSV insufficiency - Seidel AC et al. J Vasc Bras 2012, Vol. 11, Nº 3 189
considered when the association is positive and “stronger” as possible, and the maximum value of –1 when negative and “weaker”. Significance level was set at 5%.
Results
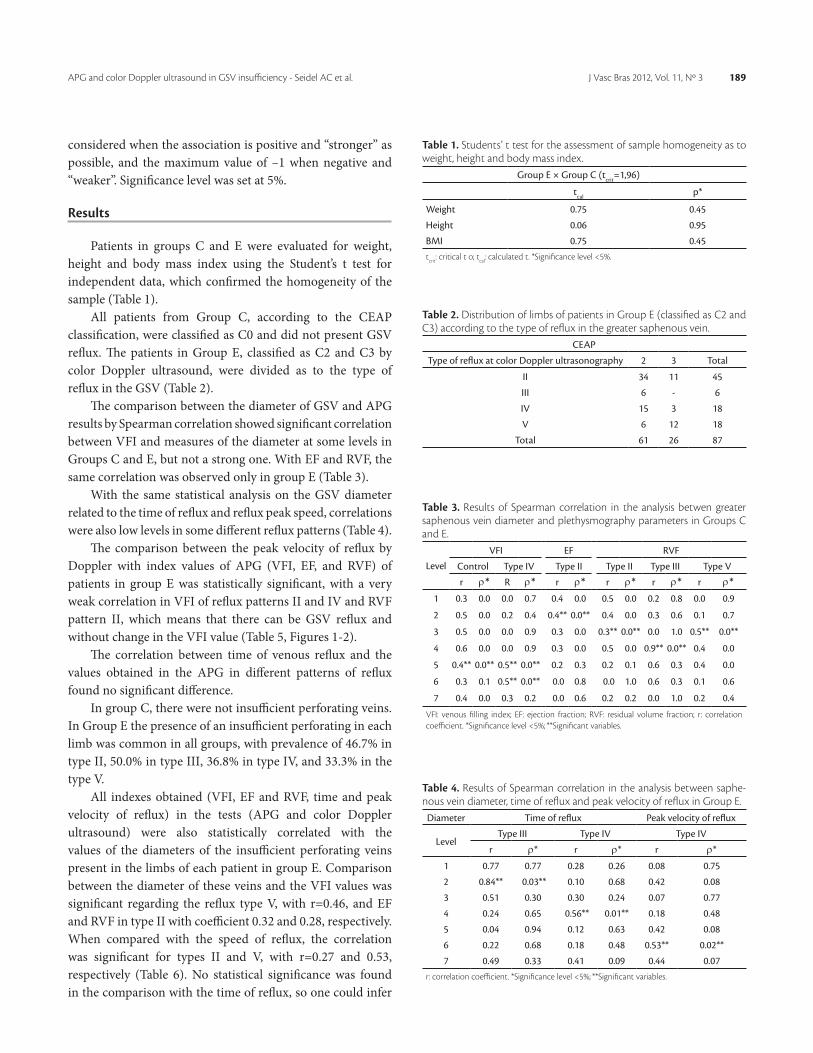
Patients in groups C and E were evaluated for weight, height and body mass index using the Student’s t test for independent data, which confirmed the homogeneity of the sample (Table 1).
All patients from Group C, according to the CEAP classification, were classified as C0 and did not present GSV reflux. The patients in Group E, classified as C2 and C3 by color Doppler ultrasound, were divided as to the type of reflux in the GSV (Table 2).
The comparison between the diameter of GSV and APG results by Spearman correlation showed significant correlation between VFI and measures of the diameter at some levels in Groups C and E, but not a strong one. With EF and RVF, the same correlation was observed only in group E (Table 3).
With the same statistical analysis on the GSV diameter related to the time of reflux and reflux peak speed, correlations were also low levels in some different reflux patterns (Table 4).
The comparison between the peak velocity of reflux by Doppler with index values of APG (VFI, EF, and RVF) of patients in group E was statistically significant, with a very weak correlation in VFI of reflux patterns II and IV and RVF pattern II, which means that there can be GSV reflux and without change in the VFI value (Table 5, Figures 1-2).
The correlation between time of venous reflux and the values obtained in the APG in different patterns of reflux found no significant difference.
In group C, there were not insufficient perforating veins. In Group E the presence of an insufficient perforating in each limb was common in all groups, with prevalence of 46.7% in type II, 50.0% in type III, 36.8% in type IV, and 33.3% in the type V.
All indexes obtained (VFI, EF and RVF, time and peak velocity of reflux) in the tests (APG and color Doppler ultrasound) were also statistically correlated with the values of the diameters of the insufficient perforating veins present in the limbs of each patient in group E. Comparison between the diameter of these veins and the VFI values was significant regarding the reflux type V, with r=0.46, and EF and RVF in type II with coefficient 0.32 and 0.28, respectively. When compared with the speed of reflux, the correlation was significant for types II and V, with r=0.27 and 0.53, respectively (Table 6). No statistical significance was found in the comparison with the time of reflux, so one could infer
Table 3. Results of Spearman correlation in the analysis betwen greater saphenous vein diameter and plethysmography parameters in Groups C and E.
Level
VFI EF RVF
Control Type IV Type II Type II Type III Type V
r ρ* R ρ* r ρ* r ρ* r ρ* r ρ*1 0.3 0.0 0.0 0.7 0.4 0.0 0.5 0.0 0.2 0.8 0.0 0.9
2 0.5 0.0 0.2 0.4 0.4** 0.0** 0.4 0.0 0.3 0.6 0.1 0.7
3 0.5 0.0 0.0 0.9 0.3 0.0 0.3** 0.0** 0.0 1.0 0.5** 0.0**
4 0.6 0.0 0.0 0.9 0.3 0.0 0.5 0.0 0.9** 0.0** 0.4 0.0
5 0.4** 0.0** 0.5** 0.0** 0.2 0.3 0.2 0.1 0.6 0.3 0.4 0.0
6 0.3 0.1 0.5** 0.0** 0.0 0.8 0.0 1.0 0.6 0.3 0.1 0.6
7 0.4 0.0 0.3 0.2 0.0 0.6 0.2 0.2 0.0 1.0 0.2 0.4
VFI: venous filling index; EF: ejection fraction; RVF: residual volume fraction; r: correlation coefficient. *Significance level <5%; **Significant variables.
Table 4. Results of Spearman correlation in the analysis between saphe-nous vein diameter, time of reflux and peak velocity of reflux in Group E.
Diameter Time of reflux Peak velocity of reflux
LevelType III Type IV Type IV
r ρ* r ρ* r ρ*
1 0.77 0.77 0.28 0.26 0.08 0.75
2 0.84** 0.03** 0.10 0.68 0.42 0.08
3 0.51 0.30 0.30 0.24 0.07 0.77
4 0.24 0.65 0.56** 0.01** 0.18 0.48
5 0.04 0.94 0.12 0.63 0.42 0.08
6 0.22 0.68 0.18 0.48 0.53** 0.02**
7 0.49 0.33 0.41 0.09 0.44 0.07r: correlation coefficient. *Significance level <5%; **Significant variables.
Table 1. Students’ t test for the assessment of sample homogeneity as to weight, height and body mass index.
Group E × Group C (tcrit=1,96)
tcal p*
Weight 0.75 0.45
Height 0.06 0.95
BMI 0.75 0.45tcrit: critical t o; tcal: calculated t. *Significance level <5%.
Table 2. Distribution of limbs of patients in Group E (classified as C2 and C3) according to the type of reflux in the greater saphenous vein.
CEAP
Type of reflux at color Doppler ultrasonography 2 3 Total
II 34 11 45
III 6 - 6
IV 15 3 18
V 6 12 18
Total 61 26 87

APG and color Doppler ultrasound in GSV insufficiency - Seidel AC et al.J Vasc Bras 2012, Vol. 11, Nº 3190
Table 5. Results of Spearman correlation for the analysis of reflux velo-city and plethysmography parameters in Group E, in which the coefficient showed correlation.
Velocity
VFI RVF
Type II Type IV Type II
r ρ* r ρ* r ρ*
>25 cm/s 0.37 0.01 0.52 0.02 0.32 0.03r: correlation coefficient. *Significance level <5%; VFI: venous filling index; RVF: residual vol-ume fraction.
Table 6. Results of Spearman correlation of the diameter of perforating veins, plethysmography parameters, time and velocity of the reflux in dif-ferent patterns of greater saphenous vein ultrasonography.
Diameter of the perforating veins
VariableII V
r ρ* r ρ*
VFI 0.38 0.00 0.46** 0.04**
EF 0.32** 0.02** 0.04 0.87
RVF 0.28** 0.05** 0.00 0.99
Time 0.22 0.10 0.11 0.63
Velocity 0.27** 0.05** 0.53** 0.02**VFI: venous filling index; EF: ejection fraction; RVF: residual volume fraction; r: correlation coefficient. *Significance level <5%; **Significant variables.
VFI: venous filling index; EF: ejection fraction; RVF: residual volume fraction.
Figure 1. Graph obtained from the plethysmography in patient with greater saphenous vein reflux type V, with venous filling index of 1.73 mL/s (normal).
Figure 2. Color Doppler ultrasound in patient with greater saphenous vein reflux type V with velocity of 52.9 cm/s and time of 4.32 s. Same patient from Figure 1.
of the patient and the results of the color Doppler ultrasound of the lower limbs was performed. The study was directed to C2 and C3 classifications (CEAP), for these patients were more commonly referred for treatment of varicose vein of the lower limbs, that is, patients with venous disease of the superficial venous system and insufficient perforating veins presenting varicosities with no other signs or symptoms of complications.
In the present study, the distribution of the classification of reflux, the type II (55%) was predominant, followed by types V (20%), IV (19%) and III (6%). Engelhorn et al.12 found as type IV (38.4%) the most common, followed by type II (13.8%), III (7.4%), V (6.6%) and I (0,8%). In the study by Luccas et al.15, 45.2% of patients had normal GSV, 13.6% had failure in the entire length of the GSV, 17.0% presented reflux from the groin to the knee region, 11.1% had failure of the groin to the upper or medium third of the thigh, 3.4% had only groin insufficiency and its collateral veins, and 9.4% presented with segmental pattern of insufficiency between the medium third of the thigh and the upper third of the leg. We believe that the difference between values is explained by the type of patient each service receives.
Considering that clinical examination may fail to determine the source of reflux, color Doppler ultrasonography is currently the method of choice for the diagnosis in reflux in individual veins13,16-21.
The literature lacks comparative parameters for the discussion of peak reflux velocity at the insufficient GSV segment, for the measurement of the velocity in various segments of the venous system offers difficulty in the calculation of the total reflux index. The multiplicity of the veins and the intrinsic errors that occur in this calculation makes this e measurement difficult and offers it little credibility22.
In the APG analysis, the indexes (VFI, EF) are a reliable method to distinguish the presence or absence of chronic
that the diameter of the insufficient perforating veins also had little influence on the results of APG.
Discussion
To assess the importance of APG in the quantification of GSV insufficiency, a comparative analysis of clinical evaluation

APG and color Doppler ultrasound in GSV insufficiency - Seidel AC et al. J Vasc Bras 2012, Vol. 11, Nº 3 191
clinical classifications aiming at a complete evaluation of the limb with CVI22. However, van Bemmelen et al.25 cited that the parameters of APG do not distinguish limbs with CVI from those presenting non-complicated varicose veins. Thus, they suggested that a discrepancy was found between the examinations because they did not measure the same reflux, so the arterial flow effect was found in the measurement of APG.
This paper presents results similar to those presented by Yamaki et al.22, who concluded that a longer reflux do not correlate with VFI. Nevertheless, there is a significant correlation between VFI and peak velocity in the sapheno-femoral and sapheno-popliteal junctions, and a moderate correlation of reflux in GSV. EF and RVF present a weak correlation with parameters from color Doppler ultrasonography. The length of time of reflux in individual veins was shown to be weakly related to APG variables and the clinical severity of CEAP in patients with isolated superficial venous insufficiency.
The clinical picture of venous insufficiency worsens depending on the number and diameter of incompetent perforating veins36,37, but, according to Labropoulos et al.36, other factors must be taken into account, which makes this association hard to be proven.
In the sample studied, the statistical results also presented a weak correlation between the diameter of perforating veins, the results from APG (only EF and RVF), and the velocity of reflux in the GSV reflux type II and V.
Data from literature indicate that color Doppler ultrasonography in an effective method to assess the deep and superficial venous systems isolated, but APG can help quantifying the degree of superficial incompetence, identifying the flow obstruction and determining whether the varicose veins contribute with the increase in venous pressure or are channels needed to the outflow of the obstructed deep veins22,25,38.
Conclusion
APG is not a reliable method for the assessment of greater saphenous vein insufficiency in cases classified as CEAP C2 and C3.
References
1. França LHG, Tavares V. Insuficiência venosa crônica: uma atualização. J Vasc Bras. 2003;2(4):318-28.
2. Castro e Silva M, Cabral ALS, Barros Junior N, Castro AA, Santos MERC. Diagnóstico e tratamento da doença venosa crônica. J Vasc Bras. 2005;4(3):S185-94.
venous insufficiency23,24, although they do not determine well the limbs with non-complicated varicose veins in patients presenting ulcers or stasis dermatitis. The VFI, on its turn, correlated poorly with the presence of incompetent veins and their diameters25.
The EF may not correlate with the clinical degree of the disease. RVF, VFI and the time of valvar closure have shown a tendency to the worsening of the venous hemodynamics as IVC progresses, with a significant superposition between groups in all variables tested, except when compared to the Control Group and those with venous disease26.
In theory, VFI and the efficacy of the calf pump (EF) should be related to the IVC manifestations. However, in the present paper, this correlation was not observed.
Christopoulos et al.14 found RVF of 2 to 35% in normal limbs, and 35 to 65% in limbs with varicose veins. In the present paper, the mean value for RVF was 28,2% for normal limbs and 32%, 26%, 30.4% and 36.1% for GSV reflux types II, III, IV and V, respectively, with a clear superposition of values.
The functional information found in the various phases of the test is important for clinical evaluation and treatment decisions27,28. However, when studying the variation in the parameters of AGP for chronic venous disease in back-test situations, the authors concluded that it is not likely that APG can detect small alterations in the parameters of assessment of venous reflux and of the calf pump, unless the sample studied is large enough29. Some studies have shown that APG is not sensitive enough to detect small hemodynamic alterations either21,25,26,30,31, but VFI is a diagnosis parameter that is useful in the assessment of chronic venous insufficiency23,32.
Results of the relation between APG and color Doppler ultrasound indexes showed that VFI correlates significantly with the total time of reflux in the limb and the time of reflux in the deep venous system, which means that the information obtained by both examinations complement each other, for they provide detailed hemodynamic and anatomical data in the segment studied33,34.
Unlike the above-mentioned paper, some authors have not found a correlation between the time of valvar closure and the flow volume, or between the time of valvar closure and peak velocity of reflux in any segment studied. No correlation was found between the time of valvar closure and VFI or between total flow volume and RVF either35. Correlation between VFI and peak velocity of reflux was observed only in patients presenting reflux type II and V, and the intensity was low, presenting coefficients of 0.37 and 0.52, respectively.
Color Doppler ultrasonography and APG are recommended for the assessment of patients in different

APG and color Doppler ultrasound in GSV insufficiency - Seidel AC et al.J Vasc Bras 2012, Vol. 11, Nº 3192
19. Szendro G, Nicolaides AN, Zukowski AJ, et al. Duplex scanning in the assessment of deep venous incompetence. J Vasc Surg. 1986;4(3):237-42. http://dx.doi.org/10.1016/0741-5214(86)90192-8
20. Neglén P, Raju S. A rational approach to detection of significant reflux with duplex Doppler scanning and air plethysmography. J Vasc Surg. 1993;17:590-5. http://dx.doi.org/10.1016/0741-5214(93)90160-N
21. Welch HJ, Faliakou EC, McLaughlin RL, Umphrey SE, Belkin M, O’Donnell Junior TF. Comparison of descending phlebography with quantitative photoplethysmography, air plethysmography, and duplex quantitative valve closure time in assessing deep venous reflux. J Vasc Surg. 1992;16(6):913-9. http://dx.doi.org/10.1016/0741-5214(92)90054-C
22. Yamaki T, Nozaki M, Sasaki K. Quantitative assessment of superficial venous insufficiency using duplex ultrasound and air plethysmography. Dermatol Surg. 2000;26(7):644-8. http://dx.doi.org/10.1046/j.1524-4725.2000.00025.x
23. Nishibe T, Kudo F, Miyazaki K, Kondo Y, Nishibe M, Dardik A. Relationship between air-plethysmographic venous function and clinical severity in primary varicose veins. Int Angiol. 2006;25(4):352-5. PMid:17164740.
24. Oliveira RA, Barros Junior N, Miranda Junior F. A variabilidade hemodinâmica venosa detectada pelos parâmetros da pletismografia a ar nas classes clínicas da classificação CEAP. J Vasc Bras. 2007;6(4):359-65.
25. van Bemmelen PS, Mattos MA, Hodgson KJ, et al. Does air plethysmography correlate with duplex scanning in patients with chronic venous insufficiency? J Vasc Surg. 1993;18(5):796-807. http://dx.doi.org/10.1016/0741-5214(93)90334-I
26. Lafrati MD, Welch H, O’Donnell TF, Belkin M, Umphrey S, McLaughlin R. Correlation of venous noninvasive tests with the Society for Vascular Surgery / International Society for Cardiovascular Surgery clinical classification of chronic venous insufficiency. J Vasc Surg. 1994;19(6):1001-7. http://dx.doi.org/10.1016/S0741-5214(94)70211-X
27. Comerota AJ, Harada RN, Eze AR, Katz ML. Air plethysmography: a clinical review. Int Angiol. 1995;14(1):45-52. PMid:7658103.
28. Evangelista SSM. Pletismografia no estudo das doenças venosas. In: Maffei FHA, Lastória S, Yoshida WB, Rollo HA, organizadores. Doenças vasculares periféricas. 3 ed. Rio de Janeiro: Medsi; 2002. p. 479-92.
29. Yang D, Vandongen YK, Stacey MC. Variability and reliability of air plethysmographic measurements for the evaluation of chronic venous disease. J Vasc Surg. 1997;26(4):638-42. http://dx.doi.org/10.1016/S0741-5214(97)70063-6
30. Payne SP, Thrush AJ, London NJ, Bell PR, Barrie WW. Venous assessment using air plethysmography: a comparison with clinical examination, ambulatory venous pressure measurement and duplex scanning. Br J Surg. 1993;80(8):967-70. http://dx.doi.org/10.1002/bjs.1800800808
31. Araki CT, Back TL, Padberg Junior FT, Thompson PN, Duran WN, Hobson RW 2nd. Refinements in the ultrasonic detection of popliteal vein reflux. J Vasc Surg. 1993;18(5):742-8. http://dx.doi.org/10.1016/0741-5214(93)90326-H
32. Engelhorn CA, Beffa CV, Bochi G, Pullig RC, Cassou MF, Cunha SS. A pletismografia a ar avalia a gravidade da insuficiência venosa crônica? J Vasc Bras. 2004;3:311-6.
3. Vasdekis SN, Clarke GH, Nicolaides AN. Quantification of venous reflux by means of duplex scanning. J Vasc Surg. 1989;10(6):670-7. http://dx.doi.org/10.1016/0741-5214(89)90011-6
4. Ting AC, Cheng SW, Wu LL, Cheung GC. Air plethysmography in chronic venous insufficiency: clinical diagnosis and quantitative assessment. Angiology. 1999;50(10):831-6. PMid:10535722.
5. Seidel AC, Mangolim AS, Rossetti LP, Gomes JR, Miranda Junior F. Prevalência de insuficiência venosa superficial dos membros inferiores em pacientes obesos e não obesos. J Vasc Bras. 2011;10(2):124-30. http://dx.doi.org/10.1590/S1677-54492011000200006
6. Antignani PL. Classification of chronic venous insufficiency: a review. Angiology. 2001;52(Suppl 1):S17-26.
7. Christopoulos D, Nicolaides AN, Szendro G. Venous reflux: quantification and correlation with the clinical severity of chronic venous disease. Br J Surg. 1988;75(4):352-6. PMid:3359149.
8. Criado E, Farber MA, Marston WA, Daniel PF, Burnham CB, Keagy BA. The role of air plethysmography in the diagnosis of chronic venous insufficiency. J Vasc Surg. 1998;27(4):660-70. http://dx.doi.org/10.1016/S0741-5214(98)70231-9
9. Dezotti NRA, Joviliano EE, Toma MK, Moriya T, Piccinato CE. Estudo da hemodinâmica venosa por meio da pletismografia a ar no pré e pós-operatório de varizes dos membros inferiores. J Vasc Bras. 2009;8(1):21-8.
10. Saliba Junior OA, Giannini M, Rollo HA. Métodos de diagnóstico não-invasivos para avaliação da insuficiência venosa dos membros inferiores. J Vasc Bras. 2007;6(3):266-75.
11. Eklöf B, Rutherford RB, Bergan JJ, et al. Revision of the CEAP classification for chronic venous disorders: consensus statement. J Vasc Surg. 2004;40(6):1248-52. http://dx.doi.org/10.1016/j.jvs.2004.09.027
12. Engelhorn CA, Picheth FS, Castro Junior N, Dabul Junior NM, Gomes CS. Estudo do sistema venoso superficial com o duplex scan a cores. Cir Vasc Angiol. 1996;12:12-4.
13. van Bemmelen PS, Bedford G, Beach K, Strandness DE. Quantitative segmental evaluation of venous valvular reflux with duplex ultrasound scanning. J Vasc Surg. 1989;10(4):425-31. http://dx.doi.org/10.1016/0741-5214(89)90417-5
14. Christopoulos DG, Nicolaides AN, Szendro G, Irvine AT, Bull ML, Eastcott HH. Air-plethysmography and the effect of elastic compression on venous hemodynamics of the leg. J Vasc Surg. 1987;5(1):148-59. http://dx.doi.org/10.1016/0741-5214(87)90205-9
15. Luccas GC, Nagase Y, Menezes FH, et al. Cirurgia de varizes dos membros inferiores. Avaliação pré-operatória do sistema venoso com mapeamento duplex. Cir Vasc Angiol. 1996;12:15-20.
16. Cavezzi A, Labropoulos N, Partsch H, et al. Duplex ultrasound investigation of the veins in chronic venous disease of the lower limbs – UIP consensus document. Part II. Anatomy. Eur J Vasc Endovasc Surg. 2006;31(3):288-99.
17. Labropoulos N, Leon Junior LR. Duplex evalution of venous insufficiency. Semin Vasc Surg. 2005;18(1):5-9. http://dx.doi.org/10.1053/j.semvascsurg.2004.12.002
18. Delis KT, Ibegbuna V, Nicolaides AN, Lauro A, Hafez H. Prevalence and distribution of incompetent perforating veins in chronic venous insufficiency. J Vasc Surg. 1998;28(5):815-25. http://dx.doi.org/10.1016/S0741-5214(98)70056-4

APG and color Doppler ultrasound in GSV insufficiency - Seidel AC et al. J Vasc Bras 2012, Vol. 11, Nº 3 193
38. Hanrahan LM, Araki CT, Fisher JB, et al. Evaluation of the perforating veins of the lower extremity using high resolution duplex imaging. J Cardiovasc Surg. 1991;32(1):87-97. PMid:2010459.
Correspondence: Amélia Cristina Seidel
Rua Dr. Gerardo Braga, 118 – Jardim Vila Rica CEP: 87050-610 – Maringá (PR), Brazil
E-mail: [email protected]
Authors’ contributionsStudy conception and design: ACS, FMJ.
Data analysis and interpretation: ACS, LPR, FMJ. Data collection: ACS.
Writing: ACS, LPR. Critical analysis: ACS, LPR, FMJ.
Final approval*: ACS, FMJ. Statistical analysis: YJ, NFN. Overall responsibility: ACS
*All authors have read and approved the final version of the paper submitted to J Vasc Bras.
33. Weingarten MS, Czeredarczuk M, Scovell S, Branas CC, Mignogna GM, Wolferth Junior CC. A correlation of air plethysmography and color-flow-assisted duplex scanning in the quantification of chronic venous insufficiency. J Vasc Surg. 1996;24(5):750-4. http://dx.doi.org/10.1016/S0741-5214(96)70008-3
34. Navarro TP, Delis KT, Ribeiro AP. Clinical and hemodynamic significance of the greater saphenous vein diameter in chronic venous insufficiency. Arch Surg. 2002;137(11):1233-7. PMid:12413308.
35. Rodriguez AA, Whitehead CM, McLaughlin RL, Umphrey SE, Welch HJ, O’Donnell TF. Duplex-derived valve closure times fail to correlate with reflux flow volumes in patients with chronic venous insufficiency. J Vasc Surg. 1996;23(4):606-10. http://dx.doi.org/10.1016/S0741-5214(96)80039-5
36. Labropoulos N, Tassiopoulos AK, Bhatti AF, Leon L. Development of reflux in the perfurator veins in limbs with primary venous disease. J Vasc Surg. 2006;43(3):558-62. http://dx.doi.org/10.1016/j.jvs.2005.11.046
37. Krnic A, Vucic N, Sucic Z. Correlation of perforating vein incompetence with extent of great saphenous insufficiency: cross sectional study. Croat Med J. 2005;46(2):245-51. PMid:15849846.