early vas reduction speed predicts the treatment outcome
TRANSCRIPT

Original ArticlePAIN RESEARCH 30 (2015) 148–157
148PAIN RESEARCH Vol.30 2015
Early VAS reduction speed predicts the treatmentoutcome in acute low back pain
Yuzuru Takahashi1,2
1Sannoh Orthopedic Clinic2Department of Orthopedic Surgery, Sannoh Hospital
AbstractThe speed of change in pain intensity as measured by the visual analog
scale (VAS) was investigated in patients with acute low back pain (LBP).Each patient was initially treated with oral nonsteroidal anti–inflammatorydrugs (NSAIDs). Clinical outcome was determined by patient self–assess-ment on the day of the last visit and classified into four groups : healed,improved, marginal, and unidentified. Data were analyzed for 131 cases inthe healed (n=55), improved (n=62), and marginal (n=14) groups. VASvalues at the first and last visits were denoted as VAS–f and VAS–l,respective ly. ∆VAS, the speed of change in the VAS value per day wascalculat ed by dividing the change in the VAS value by the number of dayselapsed. The initial ∆VAS (∆VAS–i) and the ∆VAS throughout the study(∆VAS–t) were calculated between the first and second visits and betweenthe first and last visits, respective ly. VAS–f was not relevant to outcome,while VAS–l was strongly cor related with outcome, as expected. Both∆VAS–i and ∆VAS–t were significantly correlated with outcome. Patients inthe healed and improved groups showed higher ∆VAS–i values as comparedwith those in the marginal group. A ∆VAS–i over 5 mm/day predictedfavorable outcomes. The ∆VAS–i can be regarded as a predictor of outcomein acute LBP. Speedy pain relief should be planned for patients with acuteLBP with a low ∆VAS–i to prevent a change to chronic LBP.
KeywordsAcute low back pain; Visual analog scale (VAS); Speed of change in VAS (∆VAS);
Treatment outcome; Prognosis ; Predictor
Received: 8 July 2014Accepted: 12 February 2015

Introduction
Most cases of acute low back pain (LBP) arebenign. The majority of patients with acuteLBP recover within three months 7,9). A fewpatients, however, complain of persistent pain,resulting in chronic LBP. The cutoff time pointthat demarcates acute and chronic LBP has notbeen established 11). There are several criteriafor chronic LBP that relate to pain duration.Currently, chronic LBP is a common diseasethat causes social and medico–financialproblems in industrial countries. An importantrole of primary care physicians is to preventacute LBP from progressing to chronic LBP 10).
Authorized questionnaires for LBP such asthe Roland–Morris Disability Questionnaire(RDQ) 17) and the Oswestry Questionnaire 4)
reveal physical and psychological conditionsunderlying chronic LBP 12,15). In Japan, theJapanese Orthopaedic Association Back PainEvaluation Questionnaire (JOABPEQ) wasrecently established (2007–2009) after a large–scale pilot study 6). It is now not only adomestic standard LBP questionnaire 1,2), but itis also used abroad 3). Screening instruments toidentify prognostic factors of LBP have beenreported 14). Factors leading to chronic LBPthat can be found at the first examination or inthe early stages have been investigated 10,14).Previous studies have indicated that psycholog-ical factors, emotional distress, and work statusare strongly associated with chronicity 7,8,14).However, none has been clarified as a cardinalrisk factor.
The orthopedic department of our hospitaland its satellite clinic to which the presentauthor reports, serve as local orthopedicprimary care institutions. One orthopedistspecialized in treating LBP, the author of the
present study, examines a maximum of 10 newpatients with LBP every day. LBP question-naires and the JOABPEQ can be completed atthe first visit, but they are difficult to incorpo-rate into every visit. Furthermore, a recentstudy revealed that the JOABPEQ score at thefirst visit is not prognostic in acute LBP 19).Simple and reliable clinical findings thatidentify early–stage patients at risk for unfavor-able outcomes are desired 14).
Pain is the chief complaint, and often theonly sign in patients with LBP, so pain intensitydata are the most important in the assessmentof LBP. The visual analog scale (VAS) is awidely used, universal, standard tool for themeasurement of pain intensity 5,13,16). However,the author reported that pain intensity repre-sented by the VAS score and the degree of dis-ability and quality of life were weakly correlatedwith each other either at the first visit and 15days later 11). This suggested that the VASvalue in the early stage cannot predict outcome.
The change in the value of the VAS frombefore to after treatment is an efficacy indicatorin clinical and basic studies of pain. The differ-ence in the change in VAS between a study groupand a control group is a standard measure inpain studies. However, this measure cannotpredict treatment outcome. We measured theVAS value value of our patients with LBP atevery visit. We noticed that patients withfavorable outcomes tended to report quickreduc tions in VAS values in the early stage,regard less of the initial VAS value. We hypo -thesized that the speed of reduction in the VASvalue (∆VAS), not the VAS value itself, is cor -related with clinical outcome. LBP was definedas pain perceived on the body surface arearostro caudally between the thoracolumbarboundary (T ⁄ L) line and the gluteal fold anddorso ventrally between the right and left dorsal
149
VAS reduction speed in acute LBP
PAIN RESEARCH Vol.30 2015

and ventral boundary (D ⁄ V) lines in the back.Pain per ceived in this area is caused by disordersin the lumbar spine and sacrum and relatedmuscles and ligaments, and is not of radicularorigin. The scientific basis of this concept wasdescribed in a book published recently 18).
Materials and Methods
Subjects
VAS data from patients with LBP who metthe following criteria were investigated retro-spectively : 1) Pain persisting less than onemonth from the onset of pain at the first visit.2) Patients who visited more than one time:This criterion was included because the calcula -tion of ∆VAS requires two VAS values recordedat different visits. 3) Patients with bone tumors,osteo porotic vertebral fractures, and infectiousconditions were excluded. 4) Patients were alsoexcluded if they could not understand writtenJapanese sentences. Consequently, VAS data of148 patients who met the criteria were analyzed.
Patients were given options for the day oftheir next visit. Accordingly, intervals betweenvisits were irregular for each patient. Thenumber of visits differed among patients,ranging from a minimum of one (the first re–examination only) to a maximum of 14.
VAS and ∆VAS
Patients were asked to rate their pain intensitywith the VAS at every visit. We used a handystandard 100-mm horizontal bar VAS scale onwhich the left border (0 mm) was denoted as“no pain” and the right (100 mm) as “worstpain imaginable”. The speed of change in theVAS value (∆VAS) between the two visits was
calculated by dividing the change in VAS valueby the number of days elapsed. A positive ∆VASrepresents a reduction in the VAS value. Twotypes of ∆VAS values, ∆VAS–i and ∆VAS–t,were calculated. Here ∆VAS–i, the initial ∆VAS,was calculated as the ∆VAS between the first andthe second visits. ∆VAS–t, the ∆VAS through-out the study, was caluculated as the ∆VASbetween the first and last visits. ∆VAS–i re -presents the change in VAS values in the earlyperiod of treatment.
Treatments
Every patient who met the inclusion criteriawas prescribed oral and externally appliedNSAIDs at the first visit, regardless of diagnosis,VAS–f value, and JOABPEQ score. Othertreatments, such as vitamins and pregabalin,trigger point injections, nerve blocks, andphysical therapies, were considered after thesecond visit when the initial treatments withNSAIDs were clearly insufficient for painreduction.
Judgment of treatment outcome
There are no uncontroversial criteria regardingto the efficacy of treatment. The only criterion,that could be widely accepted is a VAS of 0 = nopain. We routinely ask patients their self–evalua tion of pain relief at every visit. In thisstudy, the patient–based evaluation was classifiedinto four groups : healed, improved, marginal,and unidentified. Clinical outcome was deter-mined by the last medical record. Patients whoreported that they had healed and did not needfurther examinations and treatments wereclassifi ed into the healed group. Those whoexpressed that their pain was reduced from thefirst visit were classified into the improvedgroup. Patients who expressed that their painhad not changed or deteriorated from the first
150
Y. Takahashi
PAIN RESEARCH Vol.30 2015

visit were classified in the marginal group.When no information on pain reduction wasobtained, patients were classified into theunidentified group. Statistical analyses wereperformed for the data in the healed, improved,and marginal groups.
JOABPEQ
The JOABPEQ contains five categories : lowback pain, lumbar function, walking ability,social life function, and mental health. Patientsare asked to answer 25 questions relating tothese categories. Each category is scored on ascale ranging from 0 (representing the worstcondition) through 100 (representing the bestcondition) 6).
Statistical analysis
VAS and ∆VAS values between the treatmentoutcome groups were statistically analyzed withthe Mann–Whitney U test. Gender was analyzedwith the chi–square test. Age was analyzedwith a one–way analysis of variance (ANOVA).Differences in JOABPEQ scores were analyzedwith the Kruskal–Wallis test. P values less than0.05 were considered to be significant. Statisticalanalyses were performed with StatMate III forMacintosh (ver. 3.14, ATMS, Tokyo).
151
VAS reduction speed in acute LBP
PAIN RESEARCH Vol.30 2015
Table 1 Demographic characteristics of the 148 patients
healed improved marginal unidentified
Number of subjects 55 62 14 17
Gender (male : female) 31 : 24 34 : 28 10 : 4 9 : 8
Age (mean ± S.D.) 43.4 ± 16.6 44. 8 ± 15.1 47.8 ± 19.5 40.9 ± 14.9
Duration of visit (days) <min – med – max> 2 – 9 – 106 1 – 7 – 110 3 – 17 – 93 1 – 7 – 42
S.D. : standard deviation; min: minimum; med: median; max: maximum.No statistical difference in gender or age was noted among the healed, improved, and marginal groups.
Table 2 JOABPEQ score in the 131 patients (mean ± S.D.)
healed (n=55) improved (n=62) marginal (n=14) Kruskal–Wallis test
Low back pain 46.1 ± 31.9 37.0 ± 25.5 45.9 ± 32.2 NS
Lumbar function 38.0 ± 33.1 33.4 ± 28.0 58.3 ± 28.2 p<0.05
Walking ability 53.2 ± 31.9 51.2 ± 31.6 76.6 ± 28.0 p<0.05
Social life function 45.2 ± 27.7 39.0 ± 21.9 56.9 ± 25.0 NS
Mental health 53.5 ± 16.4 49.8 ± 18.0 54.7 ± 16.9 NS
S.D. : standard deviation; NS: not significant

Results
Demographic data
Demographic data for the 148 patients whomet the inclusion criteria are summarized inTable 1. Out of these 148 patients, treatmentoutcome was unclear in 17. VAS data for theremaining 131 patients were classified into thehealed, im proved, and marginal groups to beinvestigated in further statistical analyses.Statistical analyses revealed no significant dif-ferences in gender and age among the healed,improved, and marginal groups.
JOABPEQ
There were no statistical differences in thescores for pain, social life function and mentalhealth on the JOABPEQ among the healed,improv ed, and marginal groups. The lumbarfunction and walking ability scores showed astatistical difference among the groups. Scoreswere greater in the marginal group (Table 2).
VAS
Changes in VAS values throughout the studyfor each of the 131 patients in the three groupsare shown in Fig.1. VAS values at the first visit(VAS–f), VAS values at the last visit (VAS–l),and number of visits were conspicuously dif -ferent among patients. Fig.2 shows the changesin VAS values in the first five weeks. The VAS–fwas statistically higher in the healed andimprov ed groups than in the marginal group(Fig.3), implying that the severity of the VASvalue at the first examination did not cor -respond with prognosis. The VAS–l was statis-tically lower in the healed group than in theimproved and marginal groups (Fig.4).
∆VAS
The ∆VAS–i and ∆VAS–t values were statis-tically higher in the healed and improved groupsthan in the marginal group (Fig.5 and Fig.6).The median of ∆VAS–i was 8.8 (mm/day) for thehealed group and 6.7 for the improved group,whereas it was 1.6 for the marginal group.
152
Y. Takahashi
PAIN RESEARCH Vol.30 2015
Fig.1 Changes in VAS values in the 131 patients in the healed, improved, and marginal groups through-out the study.The circle (●), triangle (▲), and cross (×) symbols represent the healed, improved, and marginal groups,respective ly. Unfilled and filled symbols represent the VAS values at the first visit and the last visit, respectively.

153
VAS reduction speed in acute LBP
PAIN RESEARCH Vol.30 2015
Fig.2 Early changes in VAS values during the 5 weeks after the first visit.A: the healed group (n=55), B: the improved group (n=62), and C: the marginal group (n=14). Unfilled andfilled symbols represent VAS values at the first visit and the last visit, respectively.
A
B
C
154
Y. Takahashi
PAIN RESEARCH Vol.30 2015
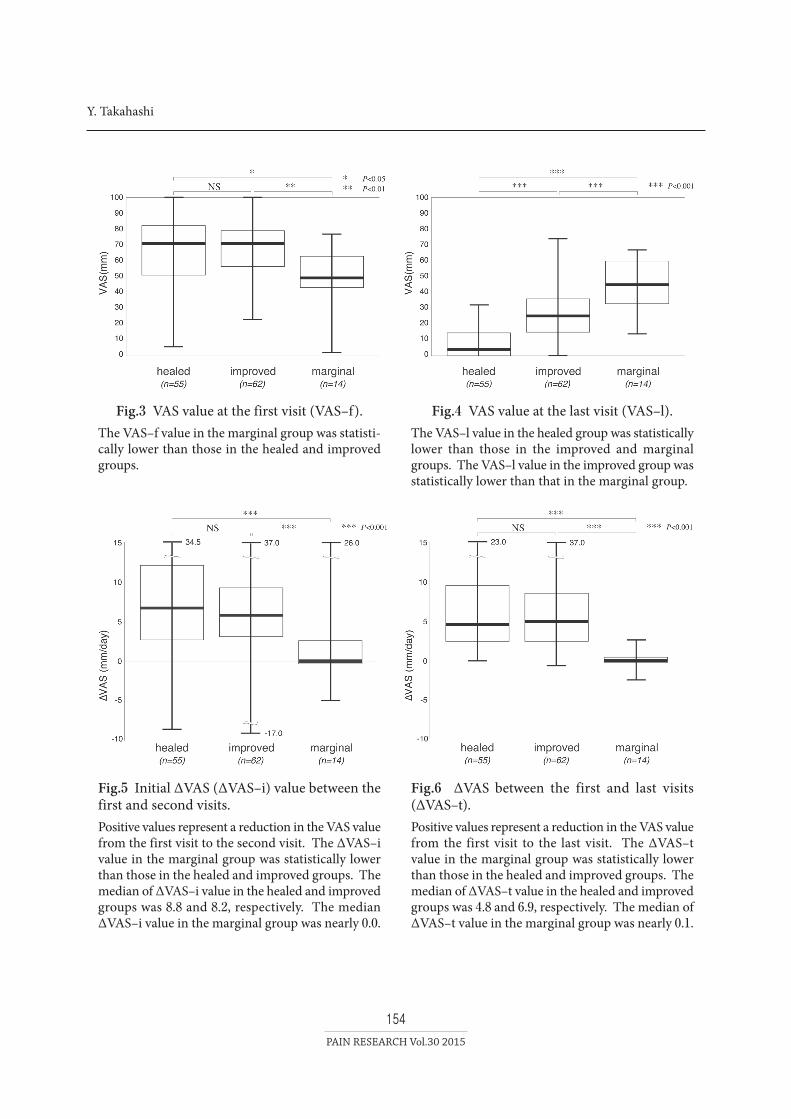
Fig.3 VAS value at the first visit (VAS–f).The VAS–f value in the marginal group was statisti-cally lower than those in the healed and improvedgroups.
Fig.4 VAS value at the last visit (VAS–l).The VAS–l value in the healed group was statisticallylower than those in the improved and marginalgroups. The VAS–l value in the improved group wasstatistically lower than that in the marginal group.
Fig.6 ∆VAS between the first and last visits(∆VAS–t).Positive values represent a reduction in the VAS valuefrom the first visit to the last visit. The ∆VAS–tvalue in the marginal group was statistically lowerthan those in the healed and improved groups. Themedian of ∆VAS–t value in the healed and improvedgroups was 4.8 and 6.9, respectively. The median of∆VAS–t value in the marginal group was nearly 0.1.
Fig.5 Initial ∆VAS (∆VAS–i) value between thefirst and second visits.Positive values represent a reduction in the VAS valuefrom the first visit to the second visit. The ∆VAS–ivalue in the marginal group was statistically lowerthan those in the healed and improved groups. Themedian of ∆VAS–i value in the healed and improvedgroups was 8.8 and 8.2, respectively. The median∆VAS–i value in the marginal group was nearly 0.0.

Discussion
When healed and improved cases were
regarded as favorable, 89% (117 out of 131cases) of patients with acute LBP had a
favorable outcome within 100 days. Thus, the
present study also confirmed the notion that
acute LBP usually subsides as previous studies
have reported 7,9).
It is quite natural that the ∆VAS–t was
strongly correlated with treatment outcome.
The ∆VAS–t should be correspond with treat -
ment out come, as it is another expression of
treat ment outcome. In contrast, the ∆VAS–i
obtained in the early stage can be used as a
predictor of treatment outcome. Previous
studies of the factors leading to progression of
acute LBP to chronic LBP have focused on
static data obtained from physical findings and
questionnaires 10,14). To our knowledge, this
study is the first to focus on data regarding the
chronological change in the patient’s condition.
Patients with acute LBP with a ∆VAS–i over
5 mm/day, in other words, those who show an
early VAS value reduction of over 35 mm/week,
would have a favorable outcome.
The present study did not reveal factors that
influence treatment outcome. There were no
statistical differences in age and gender among
the groups. The VAS–f, the VAS value at the first
visit, was significantly lower in the marginal
group. This seems counterintuitive at first
glance. However, it is not uncommon in our
experience. Some patients in the healed and
improved groups suffered from severe acute
LBP at the first visit, complaining of serious
disability in moving and walking, with
remarkab ly high VAS values. Such cases often
report a speedy pain reduction. VAS values in
the healed and improved groups showed a fast
pain reduction, with a speed of around 5 mm/day.
Patients with sprains and contusions often
report a speedy reduction in pain intensity, sug-
gesting that the pathogenesis of acute LBP is
minor injury of the lumbar soft tissue or
motion segments (intervertebral disc and facet
joint). If this is the case, pain reduction may be
achieved mainly by spontaneous repair of
injured tissues with rest, not only by the effect
of NSAIDs.
Factors causative for chronicity were not
elucidat ed. Social and psychological factors
have been suggested for chronicity 7,8,14).
However, social life functions and mental
condi tions as scored by the JOABPEQ did not
differ among groups. Patients who reported
severe (VAS > 80 mm) and persisting pain were
rare in the present population of patients with
LBP with possible degenerative pathology.
Possible factors under lying chronicity may be
the duration and past history of LBP from its
onset to the first visit. Patients in the marginal
groups may have had chronic LBP before the
first visit. This estimation will be examined in
the next study.
The present results suggest another vision for
the treatment of pain : a “virtuous or vicious
cycle” hypothesis. Patients who undergo a fast
pain reduction would be healed spontaneously
due to relief from disease and confidence in
medicine. However, regardless of its intensity
155
VAS reduction speed in acute LBP
PAIN RESEARCH Vol.30 2015

pain that does not change would result inpatients falling into a chronic condition due tofear of disease and distrust of medicine. Thisvirtuous or vicious cycle mechanism may betrue for disaster and crime victims. Earlyresolu tion may be cardinal for people withanxiety.
A problem of the present study is that the“final” outcome was unclear in patients in theimproved and marginal groups. Patients in thosetwo groups terminated their visits halfwaythrough the study by their own decision.Whether those patients eventually healed ordeteriorated is not known. Another problem isthe existence of patients with acute LBP whohad only one visit. They were excluded fromthe present study because a ∆VAS could not beobtained. They may have healed within a fewdays, or conversely, they may have consultedanother hospital. The conclusions of the presentstudy would be verified by a complete follow–upstudy for all patients.
In conclusion, the early speed of change inthe VAS value predicted treatment outcome.Patients with ∆VAS–i over 5 mm/day werehealed or improved, whereas those with∆VAS–i around 0 mm/day were not healed.The ∆VAS–i may be a reliable predictor oftreatment outcome in acute LBP. Patients witha ∆VAS–i over 5 mm/day would heal sponta-neously within a month. In contrast, thosewith a ∆VAS–i around 0 mm/day would notreport pain reduction with only NSAIDs.Various therapeutic interventions should beplanned for such patients as early as possible toprevent progression to chronic LBP.
References1) Akagi, R., Aoki, Y., Ikeda, Y., Nakajima, F.,
Ohtori, S., Takahashi, K., Yamagata, M.,Comparison of early and late surgical inter-vention for lumbar disc herniation: is earlierbetter ?, J. Orthop. Sci., 2010 (2010) 294–298.
2) Arai, Y., Okawa, A., Kawabata, S., Kato, T.,Shinomiya, K., Surgical outcomes in patientswith lumbar canal stenosis assessed by JOAscore and JOABPEQ. A prospective compara-tive study of two different types of minimallyinvasive surgery, J. Jpn. Soc. Spine Surg. R.Res., 20 (2009) 724–729.
3) Azimi, P., Shahzadi, S., Montazeri, A., TheJapanese Orthopedic Association Back PainEvaluation Questionnaire (JOABPEQ) for lowback disorders: a validation study from Iran, J.Orthop. Sci., 17 (2012) 521–525.
4) Fairbank J.C.T., Couper, J., Davis, J.B., O’Brien,J.P., The Oswestry low back pain disabilityquestionnaire, Physiotherapy, 66 (1980) 271–273.
5) Ferreira–Valente, M.A., Pais–Ribeiro, J.L.,Jensen, M.P., Validity of four pain intensityrating scales, Pain, 152 (2011) 2399–2404.
6) Fukui, M., Chiba, K., Kawakami, M., Kikuchi,S., Konno, S., Miyamoto, M., Seichi, A.,Shimamura, T., Shirado, O., Taguchi, T.,Takahashi, K., Takeshita, K., Tani, T., Toyama,Y., Yonenobu, K., Wada, E., Tanaka, T., Hirota,Y., JOA Back pain evaluation questionnaire(JOABPEQ) ⁄ JOA cervical myelopathy evalua-tion questionaire (JOACMEQ). The report onthe development of revised versions April 16,2007, J. Orthop. Sci., 14 (2009) 348–365.
7) Grotle, M., Brox, J.I., Veierod, M.B., Glomsrod,B., Lonn, J.H., Vollestad, N.K., Clinical courseand prognostic factors in acute low back pain:patients consulting primary care for the firsttime, Spine, 30 (2005) 976–982.
8) Grotle, M., Brox, J.I., Glomsrod, B., Lonn, J.H.,Vollestad, N.K., Prognostic factors in first–time care seekers due to acute low back pain,Eur. J. Pain, 11 (2007) 290–298.
9) Gurcay, E., Bal, A., Eksioglu, E., Hasturk, A.,Gurcay, A., Cakci, A., Acute low back pain:clinical course and prognostic factors, Disabil.Rehabil., 31 (2009) 840–845.
10) Heneweer, H., van Woudenberg, N., vanGenderen, F., Vanhees, L., Wittink, H.,Measuring psychosocial variables in patientswith (sub) acute low back pain complaints, atrisk for chronicity: a validation study of the
156
Y. Takahashi
PAIN RESEARCH Vol.30 2015

Acute Low Back Pain Screening Questionnaire–Dutch Language Version, Spine, 35 (2010)447–452.
11) Kovacs, F., Abraira, V., Zamora, J., Teresa Gildel Real, M., Llobera, J., Fernández, C., Bauza,J., Bauza, K., Coll, J., Cuadri, M., Duro, E., Gili, J.,Gestoso, M., Gómez, M., González, J., Ibañez,P., Jover, A., Lázaro, P., Llinás, M., Mateu, C.,Mufraggi, N., Muriel, A., Nicolau, C., Olivera,M., Pascual, P., Perelló, L., Pozo, F., Revuelta,T., Reyes, V., Ribot, S., Ripoll, J., Ripoll, J.,Rodríguez, E., Correlation between pain, dis-ability, and quality of life in patients with com-mon low back pain, Spine, 29 (2004) 206–210.
12) Linton, S., A review of psychological risk fac-tors in back and neck pain, Spine, 25 (2000)1148–1156.
13) Matamalas, A., Ramirez, M., Mojal, S.,Biostatistics, L., De Frutos, A.G., Molina, A.,Salo, G., Llado, A., Caceres, E., The visualanalo g scale and a five–item rating scale arenot interchangeable for back pain assessmentin lumbar spine disorders, Spine, 35 (2010)E1115–1119.
14) Melloh, M., Elfering, A., Presland, C.E.,Roeder, C., Barz, T., Salathé, C.R., Tamcan, O.,Mueller, U., Theis, J.C., Identification of prog-nostic factors for chronicity in patients withlow back pain: a review of screening instru-ments, Int. Orthop., 33 (2009) 301–313.
15) Pincus, T., Burton, A., Vogel, S., Field, A., Asystemic review of psychological factors as pre-dictors of chronicity/disabillty in prospectivecohorts of low back pain, Spine, 27 (2002)109–120.
16) Price, D.D., Patel, R., Robinson, M.E., Staud,R., Characteristics of electronic visual analogueand numerical scales fro rating of experimen-tal pain in healthy subjects and fibromyalgiapatients, Pain, 140 (2008) 158–166.
17) Roland, M., Morris, R., A study of the naturalhistory of back pain. Part I, Spine, 8 (1983)141–144.
18) Takahashi, Y., Visible low back pain: a hypo-thetic somatosensory structure map for thediagnosis of muscloskeletal pain. 1st ed.,Tokyo: Nankodo, 2012.
19) Takahashi, Y., Clinical significance of theJapanese Orthopaedic Association Back PainEvaluation Questionnaire (JOABPEQ) inprima ry medicine, Bessatsu Seikeigeka, 63(2013) 55–59.
Address for correspondence:Yuzuru TakahashiSannoh Orthopedic Clinic160-1 Sannoh-cho, Inage-ku, Chiba City, Chiba 263-0002, JapanFAX: +81-43-422-1700E-mail: [email protected]
157
VAS reduction speed in acute LBP
PAIN RESEARCH Vol.30 2015