denis raccah, md, phd professor of medicine university
TRANSCRIPT
The basal plus strategy
Denis Raccah, MD, PhDProfessor of Medicine
University Hospital Sainte MargueriteMarseilleFRANCE

7
Check A1C every3 months until <7%. Change treatment if
A1C is ? 7%
Step 3
ADA/EASD guidelines recommend use of basal insulin as early as the second step in type 2 diabetes management
a Sulfonylureas other than glybenclamide or chlorpropamide.b Insufficient clinical safety data; CHF, congestive heart failure
Tier 1: Well-validated core therapies
At diagnosis:
Lifestyle+
Metformin
Lifestyle + Metforminplus
Basal Insulin
Lifestyle + Metforminplus
Sulfonylureaa
Lifestyle + Metforminplus
Intensive Insulin
Step 1 Step 2
Lifestyle + Metforminplus
PioglitazoneNo hypoglycemia
Oedema / CHFBone Loss
Lifestyle + Metforminplus
GLP-1 agonistbNo hypoglycemia
Weight lossNausea / vomiting
Tier 2: Less well-validated therapiesLifestyle + Metformin
plusPioglitazone
plusSulfonylureaa
Lifestyle + Metforminplus
Basal Insulin
ADA/EASD Guidelines. Diabetes Care 2008;31(12):1–11

The concept of basal insulin therapy

Postprandial hyperglycemia persists despite treatment of FBG using basal insulin
Yki-Järvinen H, et al. Diabetologia 2006;49:442-51.
Bloo
d gl
ucos
e (m
mol
/l)
4
12
8
16
Baseline
Weeks 25-36
Insulin glargine + metformin
Beforebreakfast
22:00 04:00Afterbreakfast
Beforelunch
Afterlunch
Beforedinner
Afterdinner
Basal insulin therapy reduces the entire 24-hour blood glucose profile, but postprandial hyperglycaemia persists — LANMET study data
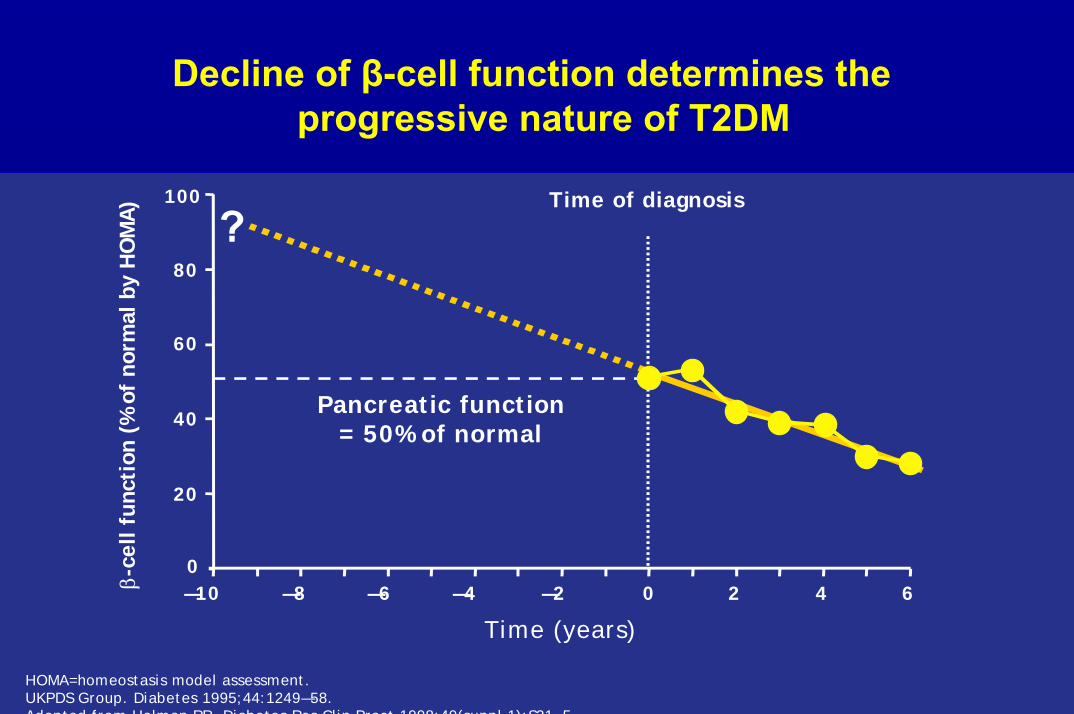
Decline of β-cell function determines the progressive nature of T2DM
HOMA=homeostasis model assessment.UKPDS Group. Diabetes 1995;44:1249―58. Adapted from Holman RR Diabetes Res Clin Pract 1998;40(suppl 1):S21 5
β-ce
ll fu
ncti
on (
% o
f no
rmal
by
HO
MA
)
Time (years)
0
20
40
60
80
100
―10 ―8 ―6 ―4 ―2 0 2 4 6
Time of diagnosis
?
Pancreatic function= 50% of normal
Insufficiency of basal insulin + OAD
Definition
– FBG < 100mg/dl,
– with HbA1c > 7% and/or PPG > 140-160 mg/dl,
– Suggesting that OAD (insulin secretagogues) loose their capability to control PPG, and that prandial insulin supplementation must be considered.
Insufficiency of basal insulin + OADdifferent situations
• 30 to 50% of patients treated by basal insulin do not reach theHbA1c target, at initiation, and despite optimisation of the dose (basal insulin is not enough)
Riddle M et al. Treat To Target. Diabetes Care 2005
• Natural history of the pancreatic disease in type 2 diabetes (basal insulin is no longer enough with time)
• Hypoglycemic risk during the titration of basal insulin making difficult to reach the FBG target
• Very high dose of basal insulin without significant effect on FBG, and weight gain ( severe insulin resistance)
Monnier et coll. Diab Metab 2006

What options are available when basal insulin therapyis no longer sufficient for glycemic control ?
Insulin intensification
1- Premix insulin
2- Basal Bolus regimen
3- The Basal Plus strategy

23
Lifestyle changes plus metformin (± other agents)
BasalAdd basal insulin and titrate
Basal PlusAdd prandial insulin at main meal
Basal BolusAdd prandial insulin before each meal
Progressive deterioration of β-cell function
Adapted from Raccah D, et al. Diabetes Metab Res Rev 2007; 23(4):257? 64
Type 2 diabetes: matching treatment to disease progression using a stepwise approach
Basal Plus: once-daily basal insulin plus once daily* rapid-acting insulin
*As the disease progresses, a second daily injection of prandial insulin may be added

• PPG is correlated to HbA1c
• The PPG is not the same according to the meals of the day, and vary from one patient to another, and from one country to another ( the highest being after breakfast in France, and after dinner in USA)
• The control of the highest PPG could influence the rest of the day.
Rationale for the « basal plus » strategy
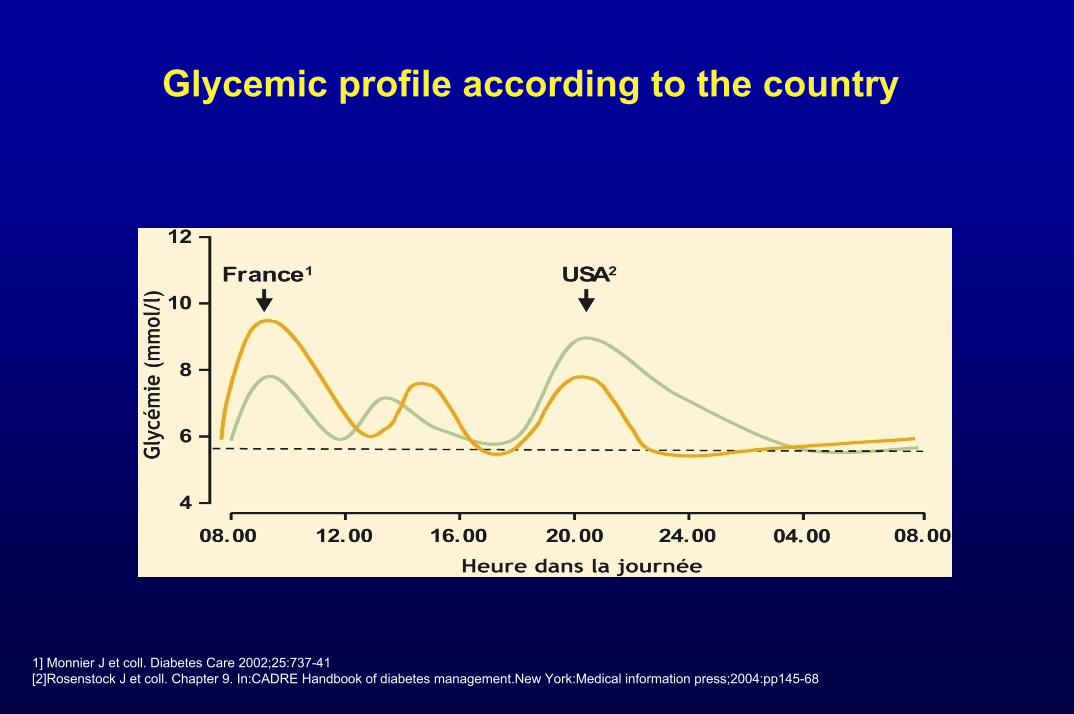
Glycemic profile according to the country
1] Monnier J et coll. Diabetes Care 2002;25:737-41[2]Rosenstock J et coll. Chapter 9. In:CADRE Handbook of diabetes management.New York:Medical information press;2004:pp145-68
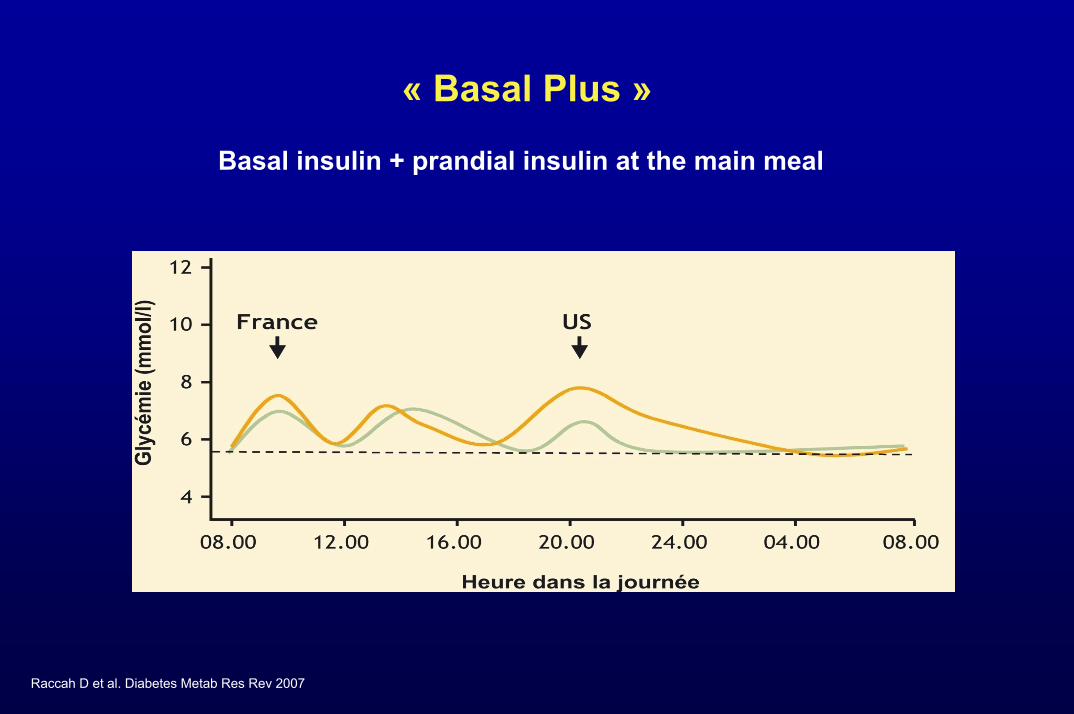
Raccah D et al. Diabetes Metab Res Rev 2007
« Basal Plus »
Basal insulin + prandial insulin at the main meal

Basal Plus: general considerations for treatment with once-daily basal insulin plus once daily rapid
prandial insulin
• Fix fasting first• Titrate basal insulin to control fasting BG
• For some patient candidates, basal will not be enough• Intensify treatment
• Add prandial insulin to control postprandial BG for efficacy and safety in patient candidates with: • HbA1c >7% to <9% despite optimal titration of basal insulin1
• And FBG control close to or at target2
Raccah D, et al. Diabetes Metab Res Rev 2007;23:257−64
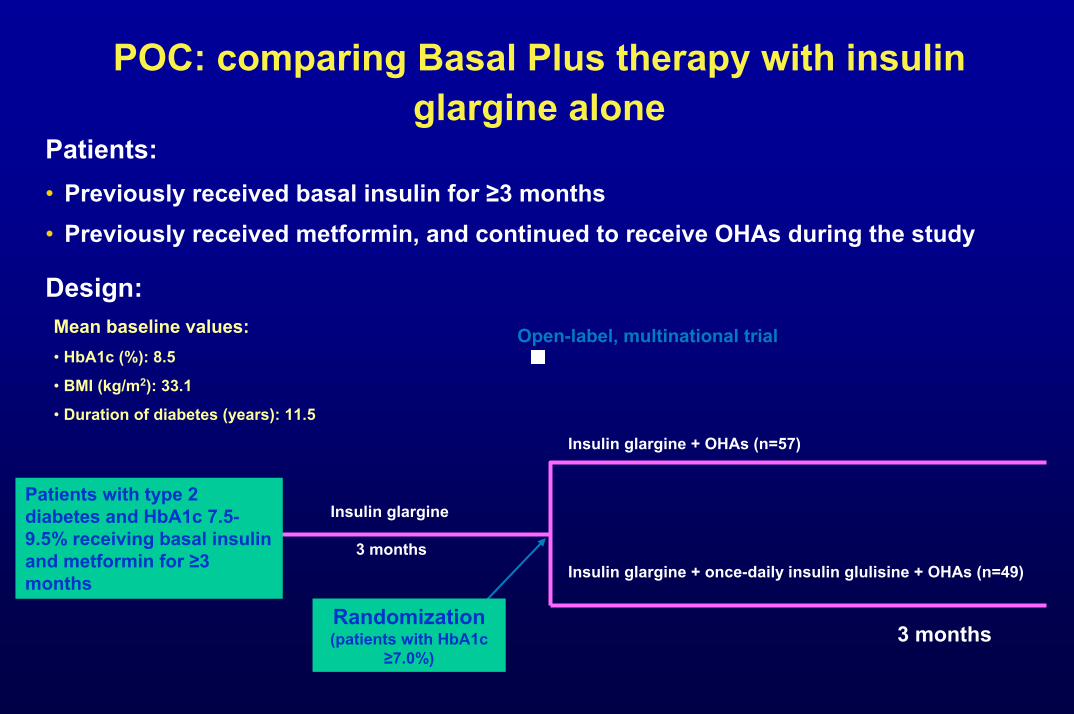
POC: comparing Basal Plus therapy with insulin glargine alone
Patients:• Previously received basal insulin for ≥3 months• Previously received metformin, and continued to receive OHAs during the study
Design:
Randomization (patients with HbA1c
≥7.0%)
Patients with type 2 diabetes and HbA1c 7.5-9.5% receiving basal insulin and metformin for ≥3 months
3 months
Insulin glargine
3 months
Insulin glargine + OHAs (n=57)
Insulin glargine + once-daily insulin glulisine + OHAs (n=49)
Mean baseline values:• HbA1c (%): 8.5
• BMI (kg/m2): 33.1
• Duration of diabetes (years): 11.5
Open-label, multinational trial

POC: adding glulisine to glargine increases efficacy and improves glycemic control
Glargine Glargine + glulisine6.06.57.07.58.08.59.09.5
10.0Randomisation
Endpoint
HbA
1c (%
)
Glargine Glargine + glulisine0
10
20
30
40
Patie
nts
achi
evin
g H
bA1c
<7
(%)
7.8
24.4
p=0.025
8.07.87.8
7.4
p=0.024
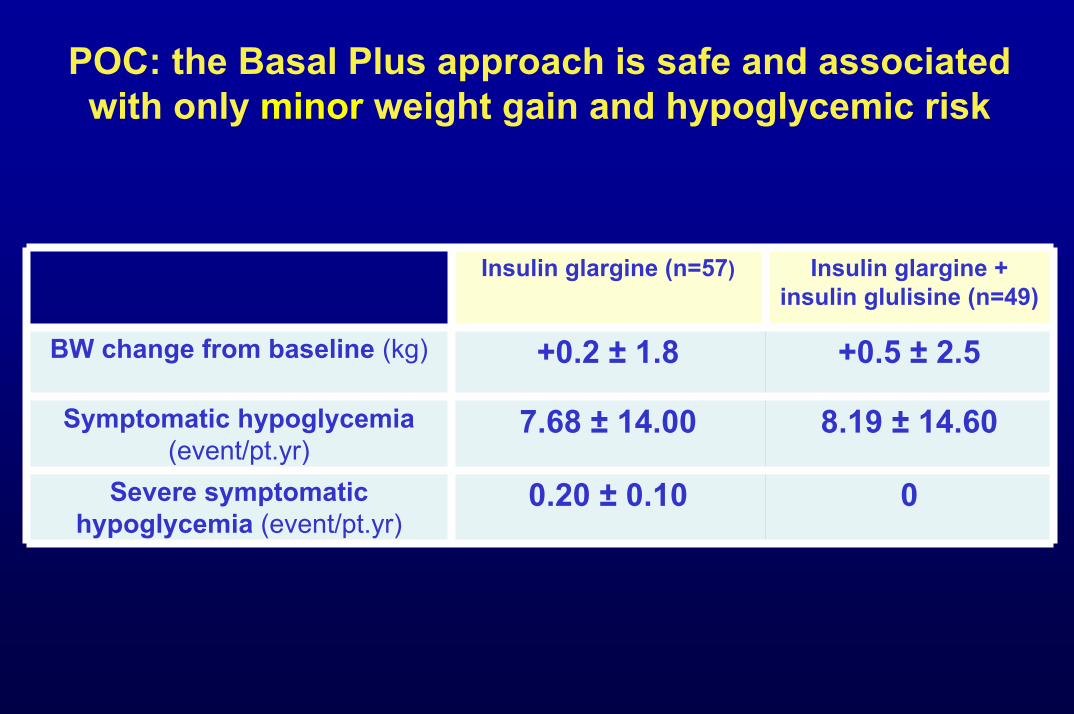
POC: the Basal Plus approach is safe and associated with only minor weight gain and hypoglycemic risk
Insulin glargine (n=57) Insulin glargine + insulin glulisine (n=49)
BW change from baseline (kg) +0.2 ± 1.8 +0.5 ± 2.5
Symptomatic hypoglycemia (event/pt.yr)
7.68 ± 14.00 8.19 ± 14.60
Severe symptomatic hypoglycemia (event/pt.yr)
0.20 ± 0.10 0
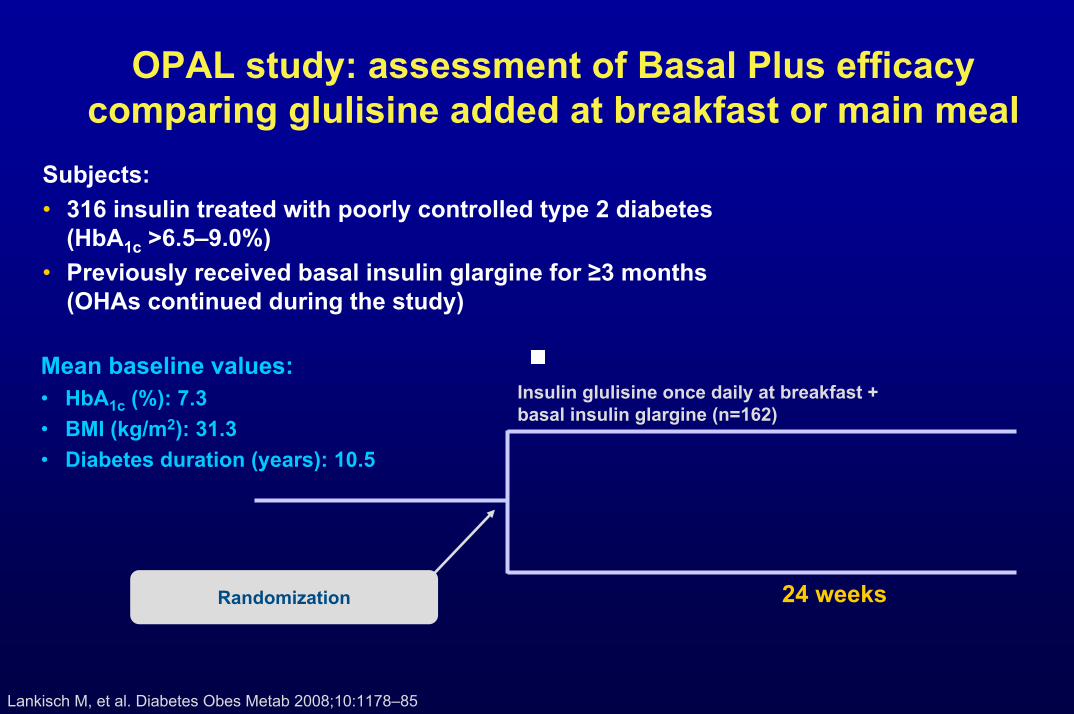
OPAL study: assessment of Basal Plus efficacy comparing glulisine added at breakfast or main meal
Subjects:• 316 insulin treated with poorly controlled type 2 diabetes
(HbA1c >6.5–9.0%) • Previously received basal insulin glargine for ≥3 months
(OHAs continued during the study)
Mean baseline values:• HbA1c (%): 7.3• BMI (kg/m2): 31.3• Diabetes duration (years): 10.5
24 weeksRandomization
Insulin glulisine once daily at breakfast + basal insulin glargine (n=162)
Lankisch M, et al. Diabetes Obes Metab 2008;10:1178–85
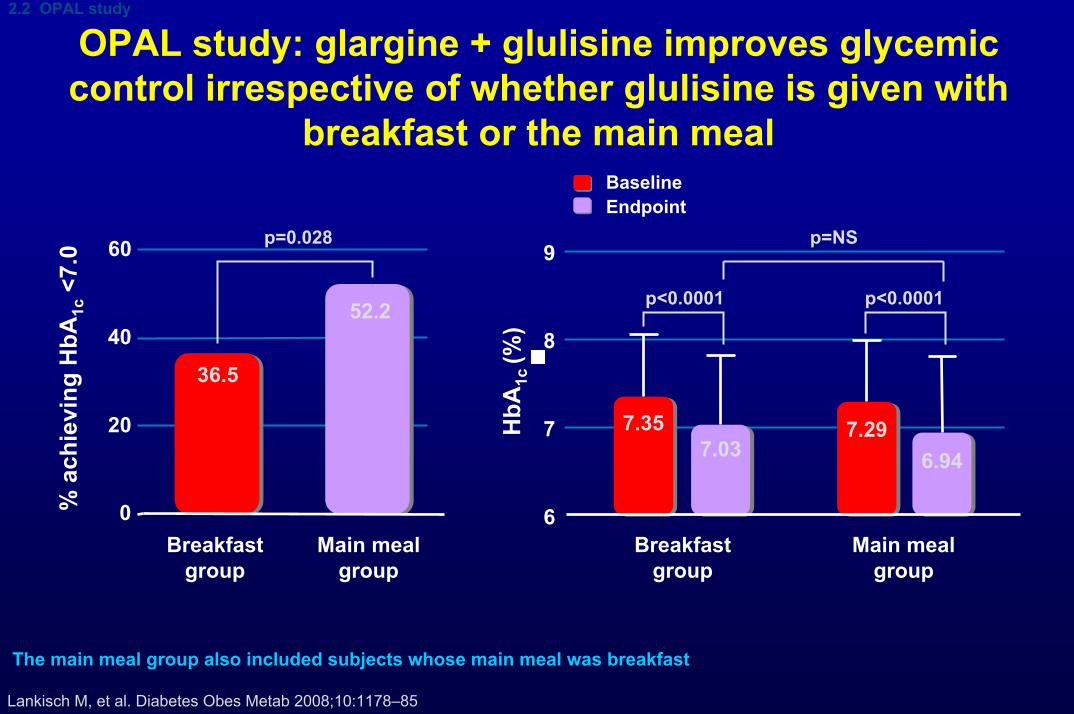
OPAL study: glargine + glulisine improves glycemic control irrespective of whether glulisine is given with
breakfast or the main meal
2.2 OPAL study
BaselineEndpoint
Breakfastgroup
Main mealgroup
0
20
40
60
% a
chie
ving
HbA
1c<7
.0
36.5
52.2
p=0.028 p=NS
p<0.0001
HbA
1c (%
)6
7
8
9
7.357.03
7.296.94
Breakfastgroup
Main mealgroup
p<0.0001
The main meal group also included subjects whose main meal was breakfast
Lankisch M, et al. Diabetes Obes Metab 2008;10:1178–85

OPAL study: the timing of glulisine addition to glargine does not affect safety or weight gain
2.2 OPAL study
p=NS
Breakfastgroup
Mainmeal
0.0
0.2
0.4
0.6
0.8
1.0
1.2
Mea
n bo
dy w
eigh
t cha
nge
from
bas
elin
e (k
g)
1.00.9
0
1
2
3
4
2.72
3.69
Con
firm
ed h
ypo
(eve
nt/p
atie
nt-y
ear)
Breakfastgroup
Mainmeal
p=NS
0.00
0.01
0.02
0.03
0.04
0.05
Breakfastgroup
Mainmeal
Seve
re h
ypo
(eve
nt/p
atie
nt-y
ear)
0.01
0.04
p=NS
Lankisch M, et al. Diabetes Obes Metab 2008;10:1178–85
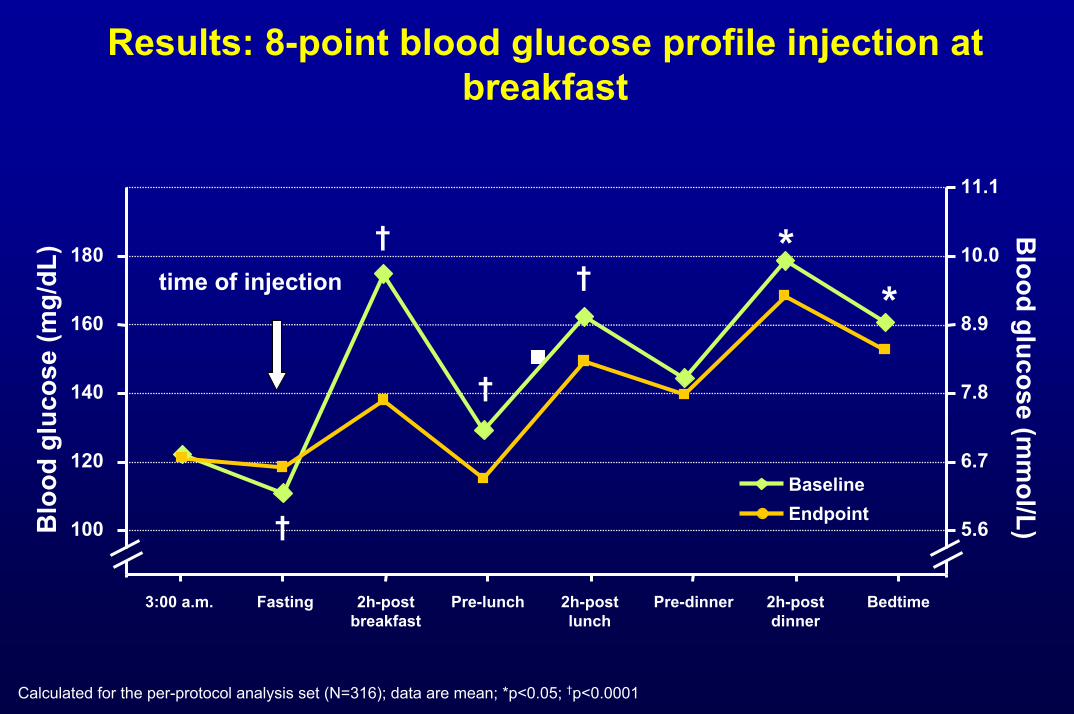
Results: 8-point blood glucose profile injection at breakfast
Calculated for the per-protocol analysis set (N=316); data are mean; *p<0.05; †p<0.0001
2h-postbreakfast
2h-postlunch
2h-postdinner
3:00 a.m. Fasting Pre-lunch Pre-dinner Bedtime
100
120
140
160
180
Blo
od g
luco
se (m
g/dL
)
5.6
6.7
7.8
8.9
10.0
11.1
Blood glucose (m
mol/L)
BaselineEndpoint
time of injection
†
*†
†
†*
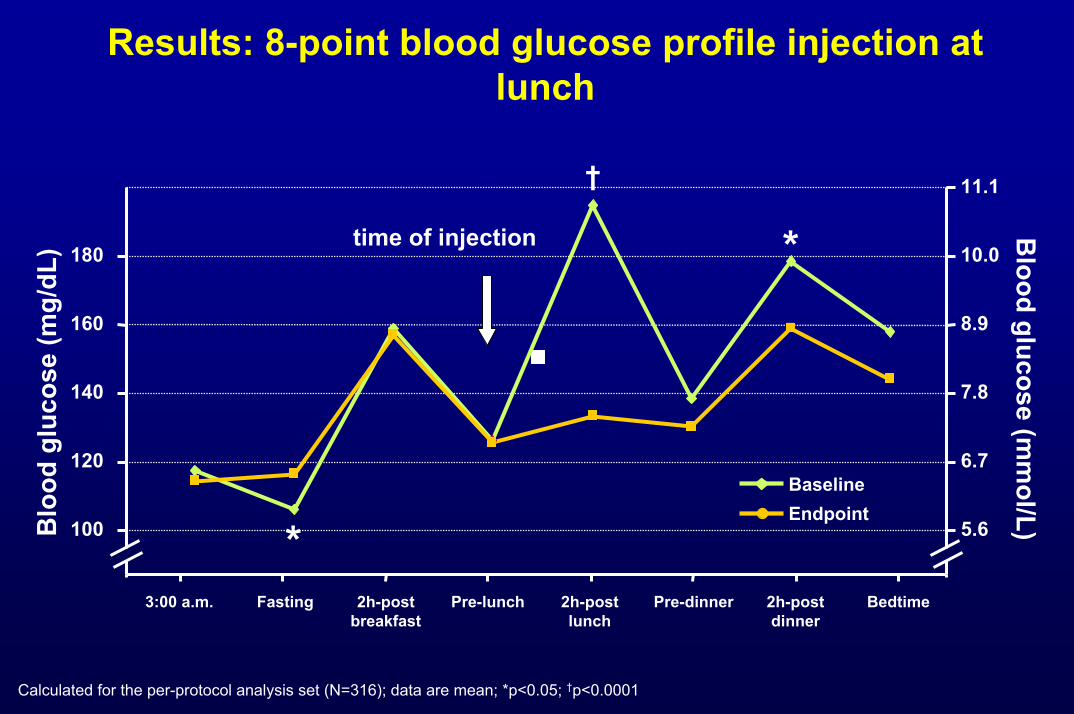
Results: 8-point blood glucose profile injection at lunch
Calculated for the per-protocol analysis set (N=316); data are mean; *p<0.05; †p<0.0001
2h-postbreakfast
2h-postlunch
2h-postdinner
3:00 a.m. Fasting Pre-lunch Pre-dinner Bedtime
100
120
140
160
180
Blo
od g
luco
se (m
g/dL
)
5.6
6.7
7.8
8.9
10.0
11.1
Blood glucose (m
mol/L)
BaselineEndpoint
time of injection
†
*
*

Results: 8-point blood glucose profile injection at dinner
Calculated for the per-protocol analysis set (N=316); data are mean; *p<0.05; †p<0.0001
2h-postbreakfast
2h-postlunch
2h-postdinner
3:00 a.m. Fasting Pre-lunch Pre-dinner Bedtime
100
120
140
160
180
Blo
od g
luco
se (m
g/dL
)
5.6
6.7
7.8
8.9
10.0
11.1
Blood glucose (m
mol/L)
BaselineEndpoint
time of injection
†
*
*†
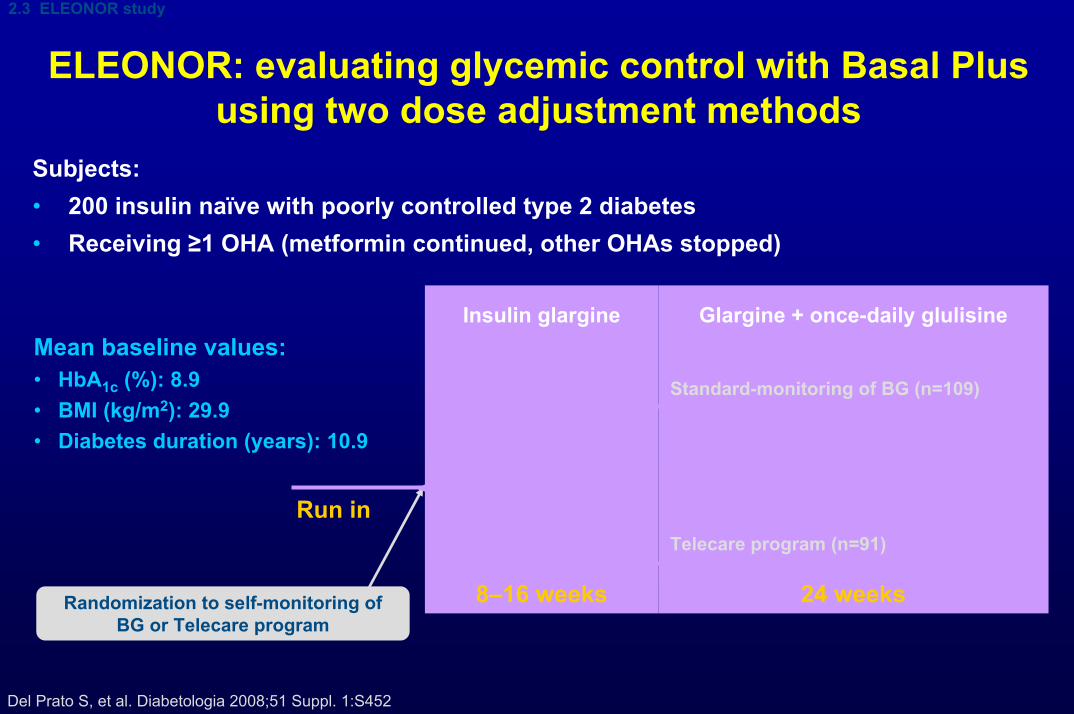
ELEONOR: evaluating glycemic control with Basal Plus using two dose adjustment methods
Subjects:• 200 insulin naïve with poorly controlled type 2 diabetes • Receiving ≥1 OHA (metformin continued, other OHAs stopped)
Randomization to self-monitoring of BG or Telecare program
Glargine + once-daily glulisine
8–16 weeks
Insulin glargine
Standard-monitoring of BG (n=109)
Telecare program (n=91)
Run in
2.3 ELEONOR study
Del Prato S, et al. Diabetologia 2008;51 Suppl. 1:S452
Mean baseline values:• HbA1c (%): 8.9• BMI (kg/m2): 29.9• Diabetes duration (years): 10.9
24 weeks
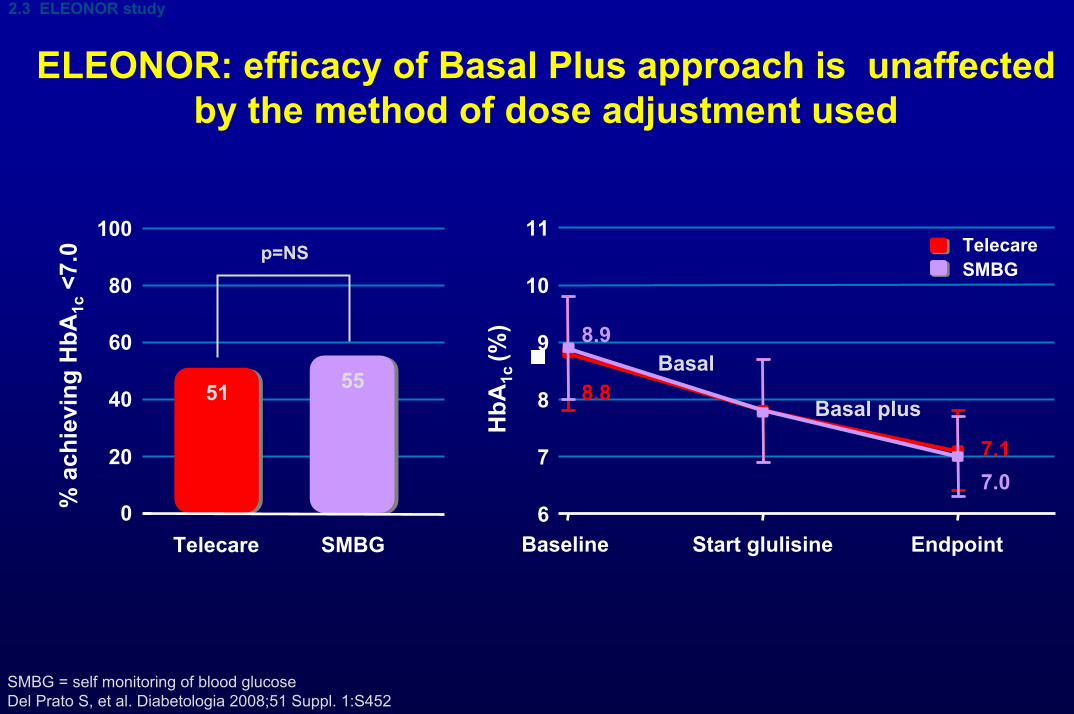
ELEONOR: efficacy of Basal Plus approach is unaffected by the method of dose adjustment used
2.3 ELEONOR study
SMBG = self monitoring of blood glucoseDel Prato S, et al. Diabetologia 2008;51 Suppl. 1:S452
20
40
60
80
100
51 55
0% a
chie
ving
HbA
1c<7
.0
Telecare SMBG
p=NS
Baseline Start glulisine Endpoint
8.9
8.8
7.17.0
Basal
Basal plus
TelecareSMBG
6
7
8
9
10
11
HbA
1c (%
)
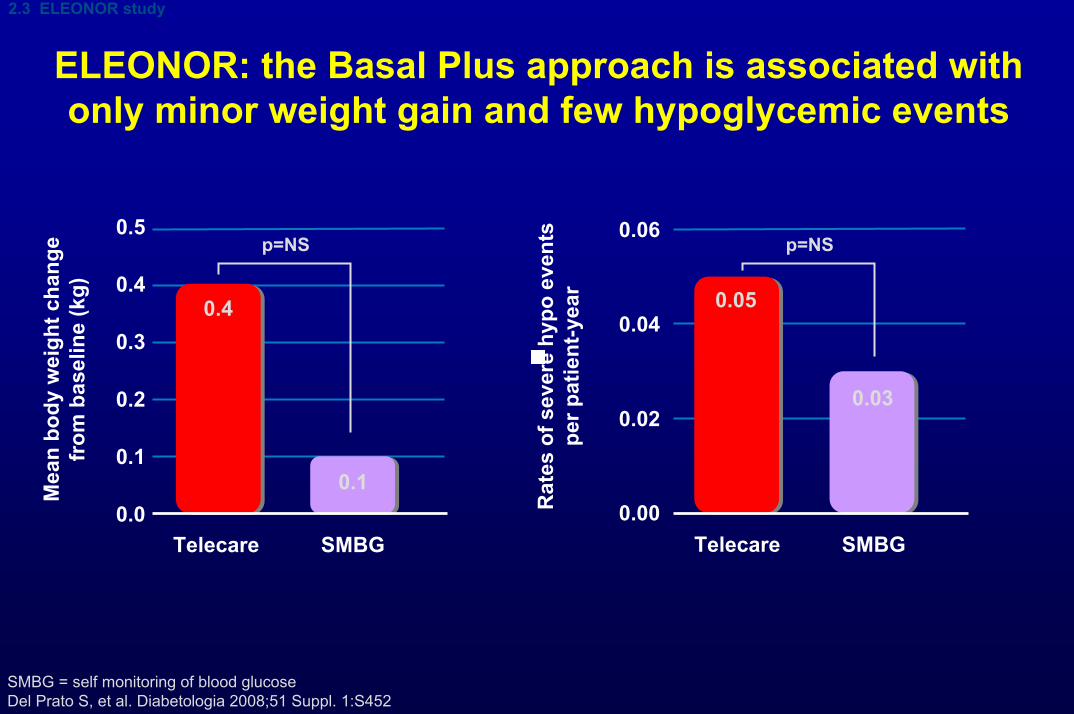
ELEONOR: the Basal Plus approach is associated with only minor weight gain and few hypoglycemic events
2.3 ELEONOR study
SMBG = self monitoring of blood glucoseDel Prato S, et al. Diabetologia 2008;51 Suppl. 1:S452
0.0
0.1
0.2
0.3
0.4
0.5
Mea
n bo
dy w
eigh
t cha
nge
from
bas
elin
e (k
g)
0.4
0.1
Telecare SMBG
p=NS
0.00
0.02
0.04
0.06
Rat
es o
f sev
ere
hypo
eve
nts
per p
atie
nt-y
ear 0.05
0.03
Telecare SMBG
p=NS

1.2.3 study: insulin glargine with addition of one, two or three daily doses of glulisine
Subjects:• Insulin naïve (785 entered study, 343 randomized) with type 2 diabetes
(HbA1c ≥8.0%)• Receiving 2 or 3 OHAs for ≥3 months (OHAs continued except sulfonylurea)
Randomization (subjects with HbA1c >7.0%, n=343)
24 weeks
Insulin glargine(n=785)
14 weeks
Additional insulin glulisine once daily (n=115)
Additional insulin glulisine twice daily (n=113)
Additional insulin glulisine three times daily (n=115)
2.4 1.2.3 study
Sanofi-aventis data on file (1.2.3 study)
Mean study entry values:• HbA1c (%): 10.1• BMI (kg/m2): 35.0

1.2.3 study: intensification of Basal insulinwith mealtime glulisine injections
improves glycemic control
2.4 1.2.3 study
Sanofi-aventis data on file (1.2.3 study)
Run in Randomization Wk 8 Wk 16 Wk 24
7.40
7.0
HbA
1c (%
)
10.1910.19
10.16
7.44
7.29
8.0
9.0
10.0Glulisine 1xGlulisine 2xGlulisine 3x
Responders in the whole population (n=785)
Evolution of HbA1c in the randomized population (n=343)
0
20
40
60
80
Subjects who achieved HbA1c<7.0% with glargine during run in
Additional subjects who achievedHbA1c <7.0%with glulisine added toglargine
All subjects(n=785)
% a
chie
ving
HbA
1c<7
.0
23%
37%
Glargine(alone)
Glargine plus glulisine(patients with HbA1c >7%)

1.2.3 study: The Basal Plus strategy is associated with a reduced level of hypoglycaemia
p=NS for all other pairwise comparisons
2.4 1.2.3 study
Sanofi-aventis data on file (1.2.3 study)
x1 x2 x30
1
2
3
4
5
Mea
n bo
dy w
eigh
t cha
nge
from
bas
elin
e (k
g)
3.7 3.8 3.9
Glulisine
0
5
10
15
20
x1 x2 x3Glulisine
Con
firm
ed s
ympt
omat
ic h
ypo
(eve
nt/p
atie
nt-y
ear)
12.2 12.9
17.1
p=0.043
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
Seve
re o
r ser
ious
hyp
o(e
vent
/pat
ient
-yea
r)
x1 x2 x3Glulisine
0.10
0.300.26

« Basal Plus » in clinical practice
Initiation • 6 point glycemic profile during 3 consecutive days• Identification of the main meal ( highest PPG, greatest glycemic delta)• Add one injection of rapid-acting insulin analog at this main meal: initial dose:0,05 U / Kg
Titration
What’s about the OAD?• Some patients may stop or decrease the insulin-secretagogues (based on glycemic profile)• Continuation of metforminWhat’s about the basal insulin dose?• No change
Mean PPG> 140 mg/dl Increase 2 U
Mean PPG between 100 and 140 mg/dl No changeMean value of PPG at this meal for the two previous days
Mean PPG < 100 mg/dl Decrease 2 U
2. La stratégie "basale plus" : résumé
1Del Prato S et coll. Diabetologia 2008 ; 51 Suppl. 1 : S452, et Sanofi-aventis, données internes ; 2Nathan DM et coll. Diabetes Care 2008 ; 31 : 1–11 ; 3Raccah D et coll. Diabetes Metab Res Rev 2007 ; 23 : 257–64 ; 4Halbron M et coll. Diabetes Metab 2007 ; 33 : 316–20

Basal Plus – Conclusion 1
• Basal Plus is once-daily basal insulin plus once-daily rapid-acting insulin (before the main meal)
• Adding once-daily rapid insulin to basal insulin gives a significant improvement in HbA1c
• Further reductions in HbA1c concentrations• Additional patients able to achieve HbA1c <7.0% goal
(between 30 and 50 % according to the studies)
• When added to once-daily basal insulin, giving prandial insulin before breakfast is as effective as giving it before the main meal
• Basal Plus is the first intensification step to consider after optimization of the basal insulin dose
• Basal plus strategy is safe in terms of hypoglycemic risk
Basal Plus – Conclusion 2
When basal insulin is no longer enough
• Basal Plus will be compared to premix insulin ( ALL TO TARGET study)
• Stepwise addition of rapid acting insulin will be compared to full basal-bolus regimen (OSIRIS study)

The basal plus strategy
Denis Raccah, MD, PhDProfessor of Medicine
University Hospital Sainte MargueriteMarseilleFRANCE