december 2005 vol 13 no 4 issn 1681-5552 - squarepharma.com.bdsquarepharma.com.bd/thesquare/the...
TRANSCRIPT
DECEMBER 2005 VOL 13 NO 4 ISSN 1681-5552
Published as a service to medical professionals by
h e a l t h c a r e b u l l e t i n
TelemedicineNeuropathic PainHepatitis CInauguration of SQUARE Cephalosporins Ltd.MSD Activities 2005- Few HighlightsProduct Profile- Vertina®
Medical Breakthrough
Dear Doctor:
We are very happy to present you the fourth issue of "the SQUARE" healthcare
bulletin, 2005!.
In this issue we have concentrated on "Telemedicine" which allows health
care professionals to use "connected" medical devices in the evaluation,
diagnosis and treatment of patients in other locations. Telemedicine is
utilized by health providers in a growing number of medical specialties,
including, but not limited to: dermatology, oncology, radiology, surgery,
cardiology, psychiatry and home health care. We have a special feature on
"Neuropathic Pain", which is a complex "chronic pain" state that can be
puzzling and frustrating for people who have it and for doctors who treat
it. We also bring you all the details on "Hepatitis C", an epidemic for
anyone! Without rapid intervention to contain the spread of the disease,
the death rate from hepatitis C will surpass that from AIDS by the turn
of the century and will only get worse.
Moreover, we have focused on the "Inauguration of SQUARE
Cephalosporins Ltd.", the dedicated and state-of-the-art
Cephalosporin manufacturing facility at Kaliakoir, Gazipur. We have
also highlighted a few "Activities of MSD in 2005" in this issue!
In our regular features, we have one of our "Product Profile" and
some fascinating news in the "Medical Breakthrough" section.
We believe you will enjoy reading this publication!
On behalf of the "SQUARE family", we wish you and your
family a very joyful, healthy and peaceful life!
From the Desk of Managing Editor
Managing EditorOmar Akramur RabMBBS, FCGP, FIAGP, FRSH
PG Dip. Business Management (India)
Executive Editor
Latifa NishatMBBS
Associate Editors
Md. Mahfuzur Rahman SikderMBBS
Md. Mahbubur RahmanMBBS
Members of the Editorial BoardMuhammadul Haque
MBA
A. H. Mahbub AlamM Pharm, PhD
Product InformationProduct Management Department
International BussinessInternational Marketing Department
The views expressed in this publication do not necessarily reflect those of its editor or SQUAREPharmaceuticals Ltd. Information in “the SQUARE” may be reprinted or translated to otherlanguages without permission but proper credit must be given to “the SQUARE”.
D E C E M B E R 2 0 0 5 V O L 1 3 N O 4 IN THIS ISSUE:Telemedicine ... Page 1
Neuropathic Pain ... Page 5
Hepatitis C ... Page 11
Inauguration of SQUARECephalosporins Ltd. ... Page 16
MSD Activities 2005-Few Highlights ... Page 17
Product Profile-Vertina® ... Page 19
Medical Breakthrough ... Page 20
ISSN 1681-5552Key title: The SQUARE (Dhaka)Abbreviated key title: SQUARE (Dhaka)
“the SQUARE”
Omar Akramur Rab
orldwide, people living in rural and remote areasstruggle to access timely, quality specialty medical care.For more than 30 years, clinicians, health servicesresearchers, and others have been investigating the use ofadvanced telecommunications and computertechnologies to improve health care. Because ofinnovations in computing and telecommunicationstechnology, many elements of medical practice can beaccomplished when the patient and health care providerare geographically separated. At the intersection of manyof these efforts is telemedicine–a combination ofmainstream and innovative information technologies.And so telemedicine could define as the use of electronic
information and communications technologies to provideand support health care when distance separates theparticipants. Telemedicine allows health care profession-als to use "connected" medical devices in the evaluation,diagnosis and treatment of patients in other locations.
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
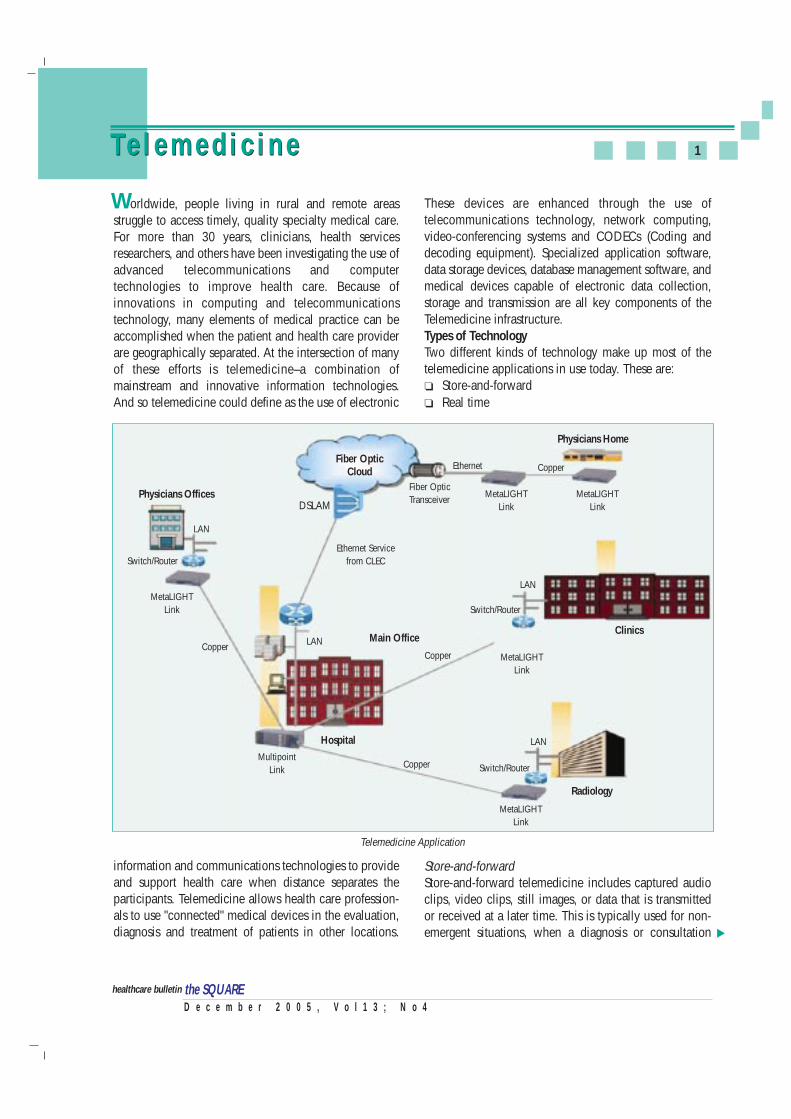
These devices are enhanced through the use oftelecommunications technology, network computing,video-conferencing systems and CODECs (Coding anddecoding equipment). Specialized application software,data storage devices, database management software, andmedical devices capable of electronic data collection,storage and transmission are all key components of theTelemedicine infrastructure.Types of TechnologyTwo different kinds of technology make up most of thetelemedicine applications in use today. These are:❏ Store-and-forward❏ Real time
Store-and-forwardStore-and-forward telemedicine includes captured audioclips, video clips, still images, or data that is transmittedor received at a later time. This is typically used for non-emergent situations, when a diagnosis or consultation
1Te l e m e d i c i n eTe l e m e d i c i n e
▲
W
Telemedicine Application
Fiber OpticCloud
Physicians Home
DSLAM
LAN
LAN
LAN
LAN
Switch/Router
Switch/Router
Switch/Router
MetaLIGHTLink
Copper
MultipointLink
MetaLIGHTLink
MetaLIGHTLink
MetaLIGHTLink
Fiber OpticTransceiver
Ethernet Servicefrom CLEC
MetaLIGHTLink
Hospital
Radiology
Main OfficeClinics
Copper
Copper
CopperEthernet
Physicians Offices

D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
2Te l e m e d i c i n e
may be made in the next 24 - 48 hours and sent back.Store-and-forward applications enable asynchronouscommunication, with the advantage of not needingconcurrent participant involvement.
Teleradiology, the sending of x-rays, CT scans, or MRIs isthe most common application of this technology. Manyradiologists are installing appropriate computertechnology in their homes, so they can have images sentdirectly to them for diagnosis, instead of making an off-hours trip to a hospital or clinic.
Telepathology is another common use of this technology.Images of pathology slides may be sent from one locationto another for diagnostic consultation. Dermatology is alsoa natural for store and forward technology (althoughpractitioners are increasingly using interactive technologyfor dermatological exams). Digital images may be taken ofskin conditions, and sent to a dermatologist for diagnosis.
Real timeReal time, another widely used technology, is the livepresence of both patient and provider in an interactiveenvironment so that the patient is actually seen by theprovider and two way communications (both visually andaudibly) can take place. Two-way interactive television(IATV), is used when a 'face-to-face' consultation isnecessary. The patient and sometimes their provider, ormore commonly a nurse practitioner or telemedicinecoordinator (or any combination of the three), are at theoriginating site. The specialist is at the referral site, mostoften at an urban medical center. Videoconferencingequipment at both locations allow a 'real-time' consulta-tion to take place. The technology has decreased in priceand complexity over the past five years, and manyprograms now use desktop videoconferencing systems.There are many configurations of an interactive consulta-tion, but most typically it is from an urban-to-rurallocation. It means that the patient does not have to travelto an urban area to see a specialist, and in many cases,provides access to specialty care when none has beenavailable previously. Almost all specialties of medicinehave been found to be conducive to this kind ofconsultation, including psychiatry, internal medicine,rehabilitation, cardiology, pediatrics, obstetrics andgynecology and neurology. There are also many periphe-ral devices which can be attached to computers whichcan aid in an interactive examination. For instance, an
otoscope allows a physician to 'see' inside a patient's ear;a stethoscope allows the consulting physician to hear thepatient's heartbeat.
Many health care professionals involved in telemedicineare becoming increasingly creative with availabletechnology. For instance, it's not unusual to use store-and-forward, interactive, audio, and video still images in avariety of combinations and applications. Use of the Webto transfer clinical information and data is also becomingmore prevalent. Wireless technology is being used forinstance, in ambulances providing mobile telemedicineservices.
Classification of Clinical Applications of TelemedicineClinical applications of telemedicine involve care forparticular individuals, although any given transactionmay also serve educational, administrative, or researchpurposes.
Clinical applications of telemedicine can be classifiedinto six general categories:
1. Initial urgent evaluation of patients for triage, stabili-zation, and transfer decisions;
2. Supervision of primary care by nonphysician provi-ders when a physician is not available locally;
3. One-time or continuing provision of specialty carewhen a specialist is not available locally;
4. Consultation, including second opinions;
5. Monitoring and tracking of patient status as part offollow-up care or management of chronic problems;and
6. Use of remote information and decision analysisresources to support or guide care for specific patients.
Services Provide by TelemedicineTelemedicine encompasses a broad variety of medicaland health services:❏ Specialist referral services typically involves of a
specialist assisting a general practitioner in renderinga diagnosis. This may involve a patient "seeing" aspecialist over a live, remote consult or thetransmission of diagnostic images and/or video alongwith patient data to a specialist for viewing later.Radiology continues to make the greatest use oftelemedicine with thousands of images "read" byremote providers each year. Other major specialty
▲
The Multi-Technology SolutionTelemedicine program requires the melding of a numberof different technologies into a seamless telemedicinesystem. In planning telemedicine system, it is essential tohave a completely integrated, fully operational solutionset. Often, a single system integrator is selected to installthe system and assure its functionality.
The following major areas of technology integration thatmay be appropriate for review and assessment as part ofthe planning process.
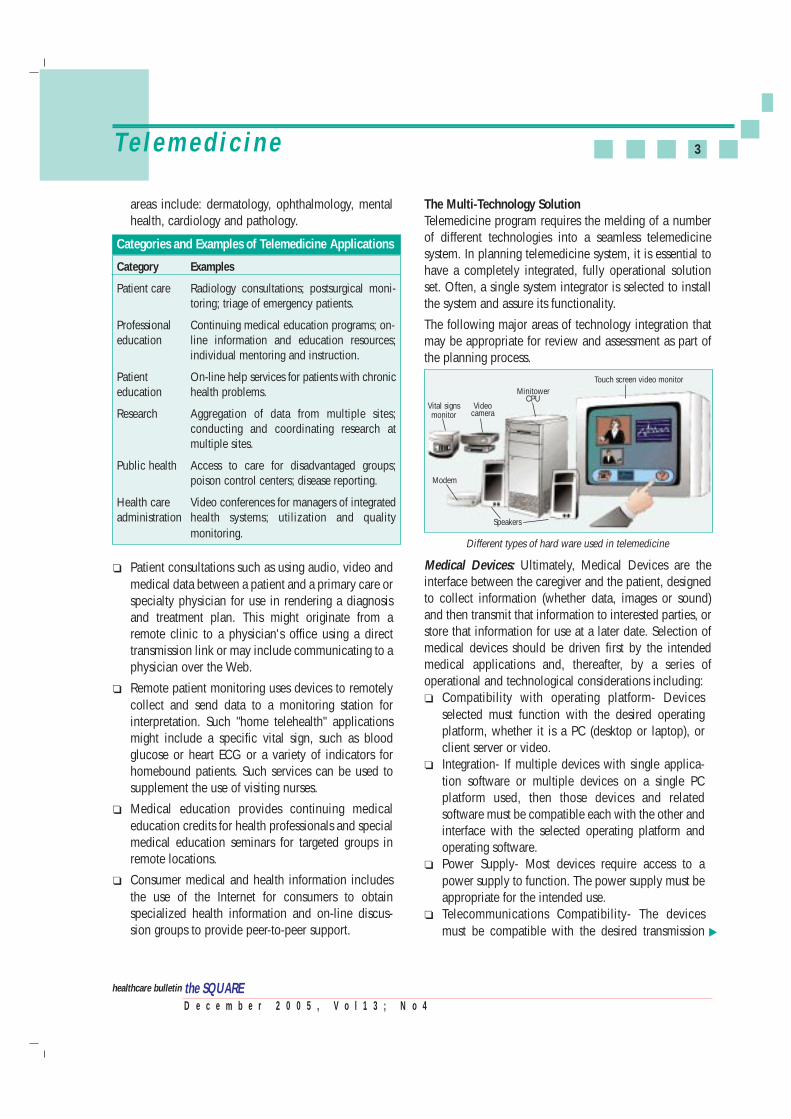
Medical Devices: Ultimately, Medical Devices are theinterface between the caregiver and the patient, designedto collect information (whether data, images or sound)and then transmit that information to interested parties, orstore that information for use at a later date. Selection ofmedical devices should be driven first by the intendedmedical applications and, thereafter, by a series ofoperational and technological considerations including: ❏ Compatibility with operating platform- Devices
selected must function with the desired operatingplatform, whether it is a PC (desktop or laptop), orclient server or video.
❏ Integration- If multiple devices with single applica-tion software or multiple devices on a single PCplatform used, then those devices and relatedsoftware must be compatible each with the other andinterface with the selected operating platform andoperating software.
❏ Power Supply- Most devices require access to apower supply to function. The power supply must beappropriate for the intended use.
❏ Telecommunications Compatibility- The devicesmust be compatible with the desired transmission
Vital signsmonitor
Videocamera
Modem
Speakers
MinitowerCPU
Touch screen video monitor
Different types of hard ware used in telemedicine
areas include: dermatology, ophthalmology, mentalhealth, cardiology and pathology.
Categories and Examples of Telemedicine Applications
Category Examples
Patient care Radiology consultations; postsurgical moni-toring; triage of emergency patients.
Professional Continuing medical education programs; on- education line information and education resources;
individual mentoring and instruction.
Patient On-line help services for patients with chroniceducation health problems.
Research Aggregation of data from multiple sites;conducting and coordinating research atmultiple sites.
Public health Access to care for disadvantaged groups;poison control centers; disease reporting.
Health care Video conferences for managers of integratedadministration health systems; utilization and quality
monitoring.
❏ Patient consultations such as using audio, video andmedical data between a patient and a primary care orspecialty physician for use in rendering a diagnosisand treatment plan. This might originate from aremote clinic to a physician's office using a directtransmission link or may include communicating to aphysician over the Web.
❏ Remote patient monitoring uses devices to remotelycollect and send data to a monitoring station forinterpretation. Such "home telehealth" applicationsmight include a specific vital sign, such as bloodglucose or heart ECG or a variety of indicators forhomebound patients. Such services can be used tosupplement the use of visiting nurses.
❏ Medical education provides continuing medicaleducation credits for health professionals and specialmedical education seminars for targeted groups inremote locations.
❏ Consumer medical and health information includesthe use of the Internet for consumers to obtainspecialized health information and on-line discus-sion groups to provide peer-to-peer support.
3Te l e m e d i c i n e
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
▲

method (e.g. "live" or "store and forward") and theavailable telecommunications platforms. For exam-ple, if the program desires to transmit "live" IP sound,then analog sound must be converted to a digitalformat, interfaced with a PC and software applicationfor transmission. Similar procedures must befollowed on the receiving end to decode the sound.
Network Computing: Network computing relates to thecompu-ting devices which drive functionality, permit thestorage of data (whether temporary or permanent, andlocal or on a central server), and facilitate the transfer ofthe desired data from the medical device to the availablecommunications platform for distribution to otherprofessionals or for storage.
Video-conferencing: Parties desiring "live" transmission ofvideo select video-conferencing equipment to displayimages and to transmit sound and data on a real timebasis. Fortunately, newergeneration video-conferencingsystems operate on a standardsbasis and connection of users ofdifferent video-conferencingsystems can be readily achieved.Even with standards basedsystems, however, there arelimited situations in whichdevices will not easily interfacedwith video-conferencing sys-tems.
Software Requirements: Generally, development of anintegrated telemedicine system involves a number ofsoftware issues. ❏ Applications Software- Telemedicine programs often
use business or clinical applications software tomanage program operations. This software often associates data with a particularpatient, and then manages transmission of data tovarious parties.
❏ Device interfaces- Frequently, devices are designedusing proprietary software or systems which do notreadily interface to applications software. Deviceinterfaces may be required to assure the flow ofinformation.
❏ Interface to database/other applications- Quite
4Te l e m e d i c i n e
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
often, the telemedicine system sponsor would like theprogram applications to interface with the sponsor'sdatabase systems or with other specific applications(e.g. finan-cial reporting, billing, physicianscheduling). Because the goal is to mainstreamtelemedicine, operating software must interface toother software systems customarily used in the opera-tion of health care providers.
Telecommunications Options: The telecommunicationsoptions at the Originating Site often dictate thetransmission method (live vs. store and forward).Generally, transmission of live images, data or sound, orthe transmission of extremely large data files, requireshigh bandwidth telecommunication options.
Consideration must also be given to two way data transferand transfer in synchronous or asynchronous modes.Understanding of available telecommunications options
may dramatically affect theselection of devices.
ConclusionSuccessful telemedicine programis the result of thoughtfulplanning, skillful management,adequate funding and thededication of participatingprofessionals. They reflect acommitment to teamwork tomeld technical and operationalcomplexities into a fully integra-
ted and efficiently functioning program.
In the end, the rewards of a successful telemedicineprogram are many. But few moments are as rewarding asreceiving an anxious look from a patient in need, andgiving reassurances that access to the best medical care isonly a moment away.
Reference:● Telemedicine: A Guide to Assessing Telecommunications for
Health Care (1996).● Telemedicine Reimbursement Handbook California Telemedi-
cine and e-Health Center, 2005.● AMD Telemedicine 2005.● Nancy Brown, Telemedicine Coming of Age, January 13, 2005.● Nancy Brown, A Brief History of Telemedicine, May 30, 1995.● American Telemedicine Association 2005.
the SQUARE
Video conference

ain is usually the natural consequence of tissue injuryand it is one of the most common reasons for a patient toseek medical care. In general, as the healing processcommences, the pain and tenderness associated with theinjury will resolve. Unfortunately some individualsexperience pain without an obvious injury or sufferprotracted pain that persists for months or years after theinitial insult. This pain condition is usually neuropathic innature and accounts for a large number of patientspresenting with chronic, non–malignant pain. Rather thanthe nervous system functioning properly to sound analarm regarding tissue injury, in neuropathic pain (NP) theperipheral or central nervous systems are malfunctioningand become the cause of the pain. Neuropathic pain, isdescribed as "burning", "electric", "tingling", and"shooting" in nature. It can be continuous or paroxysmalin presentation. The pain is produced by damage to, orpathological changes in the peripheral or central nervoussystems.
Epidemiology and EtiologyNeuropathic pain is a world wide chronic disability. Itaffects the social, economic and health sector of nearly allcountries of the world. Disorders of the brain or spinalcord can lead to “central pain,” such as that encounteredin multiple sclerosis, after a stroke, and in spondylotic andposttraumatic myelopathy. Peripheral nervous systemdisorders include diseases of the spinal nerve roots, dorsalroot ganglia, and peripheral nerves. Focal lesions of theperipheral nervous system that occur, for example, afteramputation and with radiculopathy, carpal tunnelsyndrome, and other entrapment neuropathies are usuallydistinguishable from diffuse disorders such as diabeticpolyneuropathy, human immunodeficiency virus (HIV)sensory neuropathy, and idiopathic small-fiber sensoryneuropathy.
Diabetic Peripheral Neuropathy (DPN): DPN occurs inpersons with diabetes at a rate of 11.6% in those who areinsulin dependent and 32.1% in those who are insulinnon-dependent. The most common form of painful DPNcauses spontaneous burning pain, numbness, andallodynia in the lower extremities. There may beconcomitant carpal tunnel syndrome or meralgiaparesthetica, pain in the distribution of the lateral femoralcutaneous nerve. Loss of small-fiber sensation in the
stocking-glove distribution usually is present in patientswith diabetes who have pain. Nocturnally exacerbatedsymptoms are extremely common; they may preventrestorative sleep and lead to secondary fatigue, irritability,and myofascial dysfunction. Glycemic control currently isemphasized to delay onset and progression of DPN.
Post Herpetic Neuropathy (PHN): Approximately 9% -24% of patients with herpes zoster infection will developPHN. After acute herpes zoster infection, PHN developsin 50% of persons olderthan 70 years and maylead to disability, dep-ression, and social isola-tion. Frequently, back-ground burning oraching pain is accom-panied by paroxysmalstabbing or itching andsevere, evoked allodynia and hyperalgesia. Bothperipheral and central mechanisms are responsible for thevariable manifestations of PHN. Promising strategies forprevention of PHN pain include early treatment withagents specific for NP, antiviral medications, and varicellazoster alloimmunization.
Low Back Pain and Neck Pain: Low back and neck painare among the most common reasons for physician visits.Although the percentage of patients with low back andneck pain of solely NP origin is unknown, chronicradicular pain develops in more than 20% of thoserequiring spinal surgery. In addition to axial pain, patientswith chronic radiculopathy usually experience activity-dependent aching, burning, and lancinating or stabbingpain in the sensory distribution of a nerve root.Occasionally, spontaneous burning or lancinating painpredominates, especially in patients with other evidenceof neurologic dysfunction such as sensory loss, weakness,and/or loss of deep tendon reflexes. The degree ofreported pain intensity or disability may not correlate withthe physical examination or radiographic findings.Superimposed myofascial, inflammatory, and skeletalnociceptive pain generators often coexist. Opportunitiesfor prevention of long-term disability may include earlymobilization and physical therapy facilitated byaggressive symptomatic management, patient education,
5
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
N e u r o p a t h i c P a i nN e u r o p a t h i c P a i n
P
▲
Shingles

and psychological interventions in high-risk patients.Pharmacotherapy alone is rarely effective, andinterdisciplinary management strategies may be required.
Complex Regional Pain Syndrome (CRPS): Formerlyknown as reflex sympathetic dystrophy, CRPS type I ischaracterized by the development of neuropathic painafter tissue trauma such as surgery or bone fracture. InCRPS type II, formerly known as causalgia, neuropathicpain results from an injury to a peripheral nerve with painthat extends beyond the distribution of the injured nerve.In both types, hallmark features of CRPS such asasymmetric sweating, changes in skin texture, diminishedskin temperature, and fluctuating degrees of swelling mayaccompany more universal symptoms of neuropathicpain such as burning, allodynia, and motor dysfunction.By definition, these symptoms outlast the period ofnormal tissue healing. Neuropathic pain in CRPS isconsidered sympathetically maintained when it isreduced by sympatholytics or sympathetic nerve blocks.Sympathetic-independent pain may emerge in the laterstages of the illness.
Trigeminal Neuralgia (TN): An uncommon condition,idiopathic trigeminal neuralgia (TN) is characterized byparoxysmal, lancinating, and evoked pain in thedistribution of 1 or more divisions of the trigeminal nerve.Patients who have sensory loss or other neurologicsymptoms need to be evaluated for a primary nervoussystem structural lesion or an inflammatory disorder suchas multiple sclerosis. The symptoms of TN can bedebilitating. For example, speaking or chewing maybecome incapacitating.
Carcinoma: Neuropathic pain is a common andimportant source of morbidity in patients with cancer.Neuropathic symptoms often coexist with nociceptivepain generators such as bone metastases and visceralpain. The most common cancer-related etiologies of NPinclude tumor-related neural compression, radiation-induced neural injuries, and neuropathies related toparaneoplastic disorders and chemotherapeutic agents.Although the mainstay of pharmacological treatment ofcancer-related pain is opioids, referral to a painmanagement center for neurolytic blocks or othermedical management may be required to optimizequality of life.
6N e u r o p a t h i c P a i n
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
Human Immunodeficiency Virus (HIV) Infection: Inpatients with HIV, neuropathic pain may have multiplemanifestations. In moderately advanced disease (CD4 cellcount, 0.200-0.500 x 109/L), concomitant infection withhepatitis C or human T-lymphotropic virus 1 can lead topainful peripheral neuropathy. In advanced HIV-1 disease(CD4 cell count, <0.200 x 109/L), distal symmetricalsensory polyneuropathy can present with paresthesias,cramps, and disabling burning and lancinating pain in thefeet. Cytomegalovirus infection occurs in 2% of patientswith advanced HIV-1 disease and may cause debilitatinglow back pain, radicular pain, and myelopathy. Severalantiretroviral agents, including lamivudine andsaquinavir, can cause patients to develop acute toxicneuropathy, with 50% of patients presenting with pain astheir first symptom.
Clinical ManifestationThe hallmark of neuropathic pain is the experience ofboth paresthesias (nonpainful abnormal sensations) anddysesthesias (unpleasant abnormal sensations).Spontaneous pain qualities such as burning, tingling,itching, and aching often coexist with evoked painqualities such as shooting, stabbing, or electric pains.Hyperalgesia is an exaggerated response to a painfulstimulus, whereas allodynia, pain after an innocuousstimulus, is common and often disabling. Hypoesthesia oranesthesia (reduction or loss, respectively, of normalsensation) in an area of NP is known as anesthesiadolorosa. Symptoms of neuropathic pain from variousetiologies are remarkably similar (e.g. 2 individuals withpostherpetic neuralgia [PHN] and diabetic peripheralneuropathy [DPN] may both experience burning pain).
Transmission of PainThe spinothalamic tract transmits input encoded for painand temperature, and the dorsal column transmits inputencoded for light touch. The free nerve ending of an Adelta fiber or a C fiber senses pain and temperature and hasits cell body in the dorsal root ganglion. This synapses inthe dorsal horn with a second-order neuron thatimmediately crosses the midline and ascends on thecontralateral side in the spinothalamic tract. The axons ofthe second-order neuron terminate in the hypothalamusand thalamus. In the thalamus, some projections are madedirectly to the primary sensory cortex, whereas others go to
▲

7N e u r o p a t h i c P a i n
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
the limbic system, which includes the insula, amygdala,and cingulate cortex. The Pacinian corpuscle is a first-order neuron that senses pressure. This neuron’s cell bodyis also in the dorsal horn, and the axon ascends a fewlevels, crosses the midline, and ascends in thecontralateral dorsal column/ medial lemniscus, throughthe medulla and midbrain, and terminates in the thalamus.There, the neuron synapses with a second-order neuron,which projects to the primary sensory cortex.
Pathophysiology of Neuropathic PainThe mechanisms involved in neuropathic pain arecomplex and the underlying dysfunction may involvedeafferentation within the peripheral nervous system (e.g.neuropathy), deafferentation within the central nervoussystem (e.g. post–thalamic stroke) or an imbalancebetween the two (e.g. phantom limb pain).
Central deafferentation: Overactivity of a second-orderneuron in the dorsal horn leads to enhanced paintransmission. In some individuals, central sensitizationresults after a peripheral nerve injury induces changes inpain processing within the dorsal horn. It is characterizedby a lowered threshold for activation and expandedreceptive fields, leading to the activation of key excitatory
amino acid receptors such as the N-methyl-D-aspartate(NMDA) receptor.
Disinhibition: Reduced activation of key central inhibitoryinputs from the dorsolateral fasciculus throughendogenous opioid, serotonin, and norepinephrinepathways may result in neuropathic central pain.Disinhibition also may result from loss of local inhibitorypathways from an interneuron.
Sympathetic activation: Sympathetic nerve endingssprout from a nearby blood vessel toward the site of injuryand can enhance signal transmission in the dorsal rootganglion. Catecholamine release and up-regulation ofadrenergic receptors on free nerve endings and neuromasalso contribute to sympathetically mediated pain.
Abnormal electrical connections can occur betweenadjacent demyelinated axons. These are referred to asephapses. "Ephaptic cross talk" may result in the transferof nerve impulses from one axon to another. Cross talkbetween A and C fibers develops in the dorsal rootganglion. Nerve growth trophic factors may be importantin the elaboration of these changes. A similar eventreferred to as "crossed afterdischarge" has also beendescribed whereby "the sprouts of primary afferents withdamaged axons can be made to discharge at highfrequencies by the discharge of other afferents. It is alsotheorized that injured nerves may contain ephapsesbetween sensory and sympathetic fibers, and suchcross–connections may play a role in the pathogenesis ofsympathetically mediated pain.
Peripheral defferentation: Injury to peripheral nerves maylead to the hyperexcitability of peripheral nerve terminals,or nociceptors, normally responsible for the transductionof painful stimuli. Formation of ectopic neuronalpacemakers can occur at various sites along the length ofthe nerve. This may be a result of altered expression ofsodium channels, calcium channels, and adrenergicreceptors in peripheral nerves and dorsal root ganglia.
Neurogenic inflammation may cause pain andhyperalgesia. Inflammatory neuropeptides (substance P)and prostaglandins (PGE2) are released from primaryafferent nociceptors and sympathetic postganglionicneurons respectively, activating nearby receptors andtriggering a process of spreading activation. These
▲
Normal sensory tracts
Primary sensorycortex
Cingulatecortex
Thalamus
Hypothalamus
Periaqueductalgray matter
Dorsolateral fasciculus(descending inhibition)
Dorsal rootganglion
A beta fibers
A delta fibers and C fibers
Free nerveending
Pacinian corpuscle
Spinothalamic tract
Dorsal horn
Dorsal columns}
Lissauer tract
Fasciculus gracilis
Medial lemniscus
AmygdalaInsula
Fasciculus cuneatus
mechanisms may explain the clinical response of someneuropathic pain patients to topical nonsteroidalanti–inflammatory drugs, lidocaine, and capsaicin.
The connective tissue sheath around peripheral nerves isinnervated by the nervi nervorum. Injury, compression,and inflammation of the sheath may cause pain. In cancerpatients, pain associated with tumor compression ofneural structures is clinically indistinguishable fromnon–malignant neuropathic pain. This nervi nervorumrelated pain may resolve following tumor resection ortreatment of tumor induced inflammation.
Management of Neuropathic PainInitial evaluation of the patients entails detailed review ofthe diagnosis and previous treatments. Patients needreassurance that disease-based treatments are optimized.Educating patients about pain mechanisms diminishestheir fears of undiagnosed disease.
Assessment and evaluation: A detailed history of the onsetand nature of pain is important. Individual painassessment remains primarily subjective. The visual
analog scale and numeric rating scales allow pain to berated from “no pain” to “worst pain imaginable.” Paindiaries reviewed periodically by the physician encouragepatient involvement and are useful for outcomeassessments.
Neurological and musculoskeletal examination: adetailed neurologic and musculoskeletal examinationshould be performed.
Electromyography and nerve conduction test:Electromyography and nerve conduction studies are usefulin assessing large-fiber involvement and the presence ofaxonal loss and reinnervation. Assessments of small-fiberpathology with dermal biopsies or quantitative sensorytesting remain principally research tools. Referrals toappropriate specialists for help in pinpointing a diagnosisallow for use of disease-based therapies, when available.
Psychological screening: Finally, for patients in whomconcomitant psychological dysfunction is suspected,psychological screening for depression and anxiety shouldbe performed.
PharmacotherapyNeuropathic pain clearly can impact a patient’s ability tocarry out his or her activities of daily living (ADLs).Increased pain during the night interferes with sleep. Thepatient may have difficulty ambulating without feelingpain. Handling eating utensils or tools may cause pain.The patient may guard an affected painful limb, limitsocial activities, or develop depression. Pain relief isimportant to improve the patient’s quality of life.
Complete pain relief may not be achieved with treatment.Despite improvements with pharmacotherapy, up to 30%of patients may have intractable pain. Previous medicalregimens, including dosing, escalation, and reasons forfailure, should be reviewed. A more realistic goal is todecrease pain to a tolerable level. Effective treatmentusually combines nonpharmacologic methods withmedication. Patients should understand the goals of eachstep and need to know that effects are not immediate.Serum levels are generally unpredictive of response andshould be monitored if maximal doses are achievedwithout toxicity or benefit. Medications are not necessarilylifelong therapy, and tapering should be considered after aperiod of sustained relief and improved function.
8N e u r o p a t h i c P a i n
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
▲
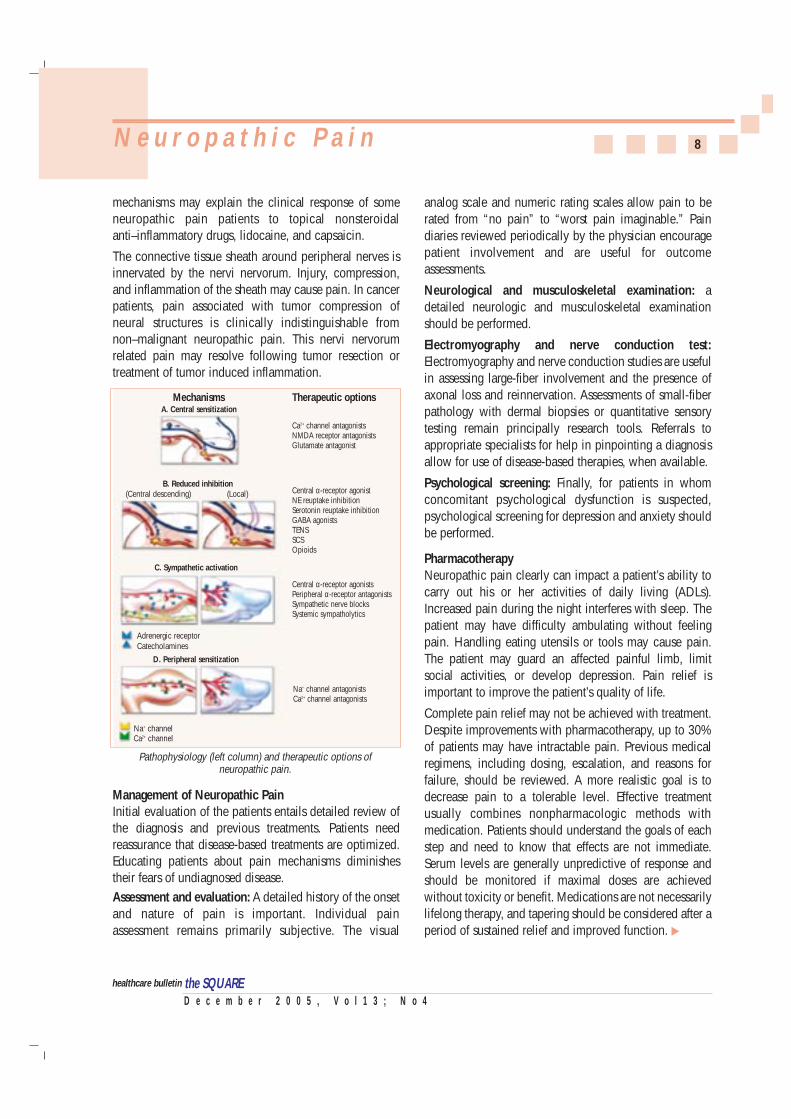
Pathophysiology (left column) and therapeutic options ofneuropathic pain.
A. Central sensitization
B. Reduced inhibition
C. Sympathetic activation
D. Peripheral sensitization
Ca2+ channel antagonistsNMDA receptor antagonistsGlutamate antagonist
Central α-receptor agonistNE reuptake inhibitionSerotonin reuptake inhibition GABA agonists TENSSCSOpioids
Central α-receptor agonists Peripheral α-receptor antagonists Sympathetic nerve blocksSystemic sympatholytics
Na+ channel antagonistsCa2+ channel antagonists
(Local)(Central descending)
Adrenergic receptorCatecholamines
Na+ channelCa2+ channel
Mechanisms Therapeutic options

Many patients, especially those with localized symptoms,may respond to initial therapy with topical lidocaine. Indiffuse syndromes, pharmacotherapy begins at the lowestavailable dose of a single drug, followed by gradualtitration to efficacy and tolerability. Initial systemictherapy may begin with gabapentin or nortriptyline.Tricyclic antidepressants (TCA) should be used withcaution in patients with a history of cardiac conductiondisturbances. The tertiary amines, such as amitriptyline,should be avoided in elderly persons because of theirincreased risk of falling. To best evaluate efficacy andpossible adverse effects, it is advisable to avoidsimultaneous adjustments of an existing regimen and theaddition of new agents. Incomplete or partial responses todrugs with minimal risk such as topical lidocaine oftencan be augmented by the addition of a drug with adifferent mechanism of action (such as gabapentin).Although many patients respond favorably to 2 or 3 drugswith synergistic profiles, careful attention must be given tothe use of more than 3 drugs when incremental benefitdoes not occur. Improving the activities of daily living isan important goal from the outset of therapy but is alsoimportant when a ceiling of analgesic efficacy has beenreached with a pharmacological regimen.
Tramadol can be considered a treatment option forpatients in whom a TCA or gabapentin fails or is onlypartially effective, especially when nociceptive pain (eg,from osteoarthritis or cancer) coexists. Many of theseindividuals will require more potent opioids, andindividual tolerability varies widely. Rotation to a differentopioid may be useful in patients with poor tolerability toan initial agent. Patients who may benefit from opioid usecan be identified with a trial of a short-acting agent suchas hydrocodone, oxycodone, or morphine, depending onthe severity of the problem. If the trial is effective, long-term therapy with a sustained-release or long-actingpreparation is advisable. A dosing schedule at regularintervals is preferable to use of “breakthrough”medications for patients with chronic pain. Use ofnonpharmacological options, such as psychologicaltechniques, TENS (Transcutaneous Electric NerveStimulation), and local modalities (heat, ice, massage)should be encouraged instead of “as needed” or“breakthrough” medications when a stable dose of opioidhas been achieved.
Non Pharmacological ManagementRefractory pain leads to depression, anxiety, impairedproductivity, declining social functioning, and diminishedquality of life. Characterized by the escalating use ofhealth care, affective disorders, and physicaldeconditioning, the chronic pain syndrome requires acomprehensive treatment strategy incorporatinginterdisciplinary management. Nonpharmacologicalmanagement plays an important role in restoring functionand reducing disability. Every effort should be made tonormalize the patient’s sleep schedule. Reviewing goodsleep hygiene, limiting caffeine intake, and encouragingexercise can prevent dependence on a nightly sedative.Psychological referral for biofeedback, cognitive-behavioral techniques, group therapy, and counseling iswarranted early in patients with psychosocial impairment.Physical therapy referral should be made for neuro-muscular rehabilitation, gait and prosthetic deviceassessment, therapeutic exercise instruction, desensiti-zation (especially in patients with severe allodynia andhyperalgesia), and TENS trials. A structured program withstepwise advancement is imperative in many disorders,especially CRPS and chronic radiculopathy. Occupationaltherapy and vocational rehabilitation may help the patienttransition to functional independence. The network ofcare completed by mental health providers and physicaland occupational therapists often helps sustain patientoptimism and participation.
Interventional TherapyInterventional therapy (diagnostic or therapeutic nerveblocks or implantable technologies) may be considered inpatients with continuing pain and dysfunction who areunresponsive to conservative approaches. Techniquessuch as local anesthetic and corticosteroidal nerve blocksgenerally are used to hasten return of function while long-term strategies are identified. Although evidence for theefficacy of epidural injections is limited, in some casessuccess rates are higher than with conservative therapy.Patients with acute neck or back pain with a radicularpattern may derive the greatest benefit from epiduralcorticosteroid injection. Interventional strategies such asepidural corticosteroid injections may be considered inacute radiculopathy if symptoms persist despite physicaltherapy and use of oral analgesics.
9N e u r o p a t h i c P a i n
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
▲
In CRPS, early physical rehabilitation of the affected limbis crucial for recovery. If the patient is unable to undergophysical therapy despite adequate medication trials,referral to a pain clinic is appropriate. Nerve blocks suchas a lumbar sympathetic block (lower extremity), stellate
ganglion block (upper extremity), or somatic nerve blockmay provide sufficient analgesia for participation inphysical therapy and remobilization. The duration andextent of analgesia should be considered whendetermining the need for subsequent nerve blocks andescalation of physical therapy.
After multiple medication trials have been ineffective,referral to a pain clinic is warranted for additional medicalmanagement and appropriate interventions by the painspecialist. A trial of spinal cord stimulation (SCS) may beindicated for certain NP diagnoses. The positive results ofSCS for patients in whom other therapies have failed forlow back pain syndrome and CRPS have led to the use ofSCS in other neuropathic disorders. Intrathecal opioids,clonidine, baclofen, and local anesthetics (alone or invarious combinations) have been used long term inselected patients with refractory pain. For example,intrathecal morphine has been used successfully in
patients who respond to oral opioids but haveunmanageable adverse effects. Intrathecal drug deliveryshould be considered early in patients with NP and cancerin whom systemic analgesics are poorly tolerated.
Conclusion
Neuropathic pain remains a clinical challenge fortreatment. Any medication used to treat neuropathy mustbe weighed for benefits and risks before using. It may takeseveral trials to find an effective medication orcombination of medications. Patients may need supportthroughout the process. Neuropathic pain often requires acombination of medication and nonpharmacologicmodalities in order to achieve adequate pain relief.
References:❏ Review: Contemporary Management of Neuropathic Pain for the
Primary Care Physician. Mayo Clinic Proceedings, 2004; 79(12):1533-45.
❏ Steven Richeimer, MD. Understanding Neuropathic Pain. Obtainedfrom: USC Pain Management, USC Medical Center atwww.helpforpain.com on November 10, 2005.
❏ Jacintha S. Cauffield, Pharm.D., BCPS. Treatment Options inNeuropathic Pain. US Pharmacist, 25:6.
10N e u r o p a t h i c P a i n
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
the SQUARE
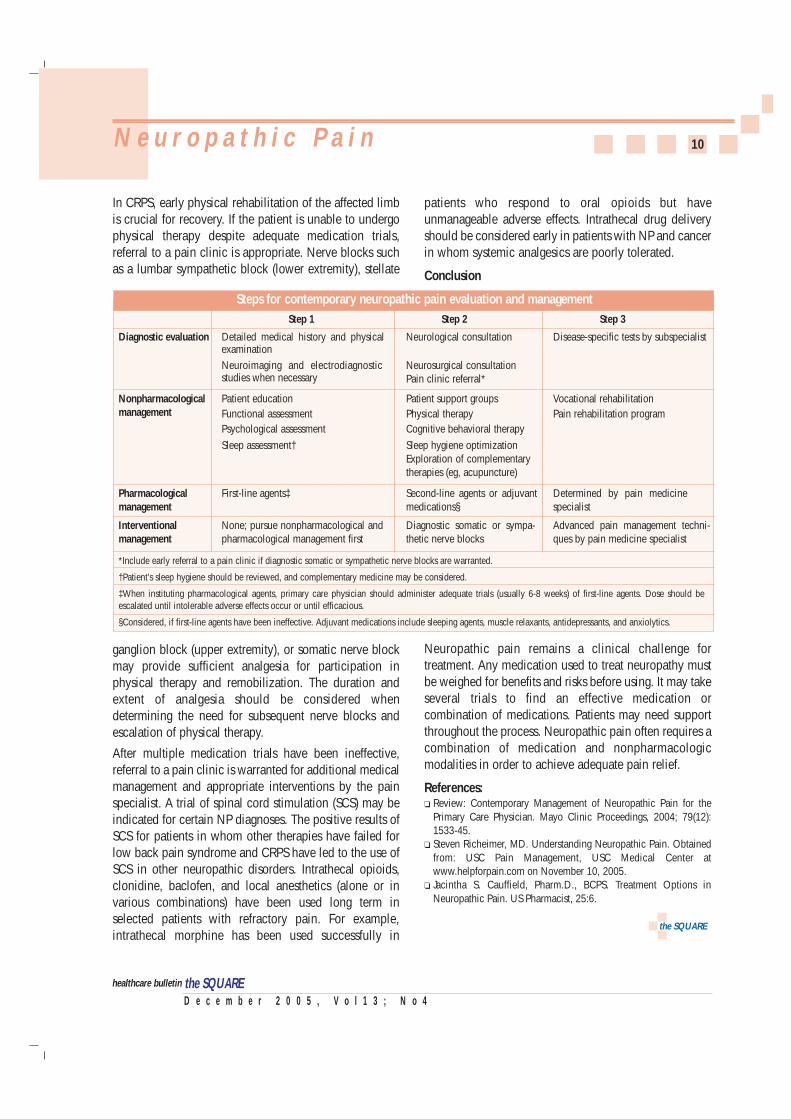
Steps for contemporary neuropathic pain evaluation and managementStep 1 Step 2 Step 3
Detailed medical history and physicalexamination
Neurological consultation Disease-specific tests by subspecialist
Neurosurgical consultationPain clinic referral*
Diagnostic evaluation
Patient educationFunctional assessmentPsychological assessment
Sleep assessment†
Patient support groupsPhysical therapyCognitive behavioral therapy
Sleep hygiene optimizationExploration of complementarytherapies (eg, acupuncture)
Vocational rehabilitationPain rehabilitation program
Nonpharmacologicalmanagement
First-line agents‡ Second-line agents or adjuvantmedications§
Determined by pain medicinespecialist
Pharmacologicalmanagement
None; pursue nonpharmacological andpharmacological management first
Diagnostic somatic or sympa-thetic nerve blocks
Advanced pain management techni-ques by pain medicine specialist
Interventionalmanagement
Neuroimaging and electrodiagnosticstudies when necessary
*Include early referral to a pain clinic if diagnostic somatic or sympathetic nerve blocks are warranted.
†Patient’s sleep hygiene should be reviewed, and complementary medicine may be considered.
‡When instituting pharmacological agents, primary care physician should administer adequate trials (usually 6-8 weeks) of first-line agents. Dose should beescalated until intolerable adverse effects occur or until efficacious.
§Considered, if first-line agents have been ineffective. Adjuvant medications include sleeping agents, muscle relaxants, antidepressants, and anxiolytics.
epatitis C is a viral infection of the liver which had beenreferred to as parenterally transmitted "non A, non Bhepatitis" until identification of the causative agent in1989 by molecular cloning. The discovery andcharacterization of the hepatitis C virus (HCV) led to theunderstanding of its primary role in post-transfusionhepatitis and its tendency to induce persistent infection.HCV is a major cause of acute hepatitis and chronic liverdisease, including cirrhosis and liver cancer. Globally, anestimated 170 million persons are chronically infectedwith HCV and 3 to 4 million persons are newly infectedeach year. HCV is spread primarily by direct contact withhuman blood. Most HCV-infected persons might not beaware of their infec-tion because they arenot clinically ill.Infected persons serveas a source of trans-mission to others andare at risk for chronicliver disease or otherHCV-related chronicdisease.
The major causes of HCV infection worldwide are use ofunscreened blood transfusions, and re-use of needles andsyringes that have not been adequately sterilized.Although its means of transmission are well documented,the hepatitis C virus itself still remains an enigma.No vaccine is currently available to preventhepatitis C and treatment for chronic hepatitis C istoo costly for most persons in developing countriesto afford. Thus, from a global perspective, thegreatest impact on hepatitis C disease burden willlikely be achieved by focusing efforts on reducingthe risk of HCV transmission from nosocomialexposures (e.g. blood transfusions, unsafe injectionpractices) and high-risk behaviors (e.g. injectiondrug use).
Pathogen
The hepatitis C virus is an enveloped RNA virus with adiameter of about 50 nm, classified as a separate genus(Hepacivirus) within the Flaviviridae family whichappears to have a narrow host range. Humans andchimpanzees are the only known species susceptible to
infection, with both species developing similar disease.An important feature of the virus is the relative mutabilityof its genome, which in turn is probably related to thehigh propensity (80%) of inducing chronic infection. HCVis highly heterogeneous. HCV is clustered into severaldistinct genotype, eleven HCV genotypes with severaldistinct subtypes have been identified throughout theworld, which may be important in determining theseverity of the disease and the response to treatment.Moreover, such heterogeneity hinders the development ofvaccines, since vaccine antigens from multiple serotypeswill probably be necessary for global protection. The virusis inactivated by-❏ Exposure to lipid solvents or detergents❏ Heating at 60˚C for 10 hours or 100˚C for 2 minutes
in aqueous solution ❏ Formaldehyde (1:2000) at 37˚C for 72 hours❏ β-propriolactone❏ Ultra violet irradiation
HCV is relatively unstable to storage at room temperatureor repeated freezing and thawing.
Epidemiology
HCV infection occurs throughout the world, and up untilthe introduction of anti-HCV screening test for blooddonors, introduced in 1990/1991 in Europe and theUnited States, it has represented the major causetransfusion associated hepatitis.
The incidence of HCV on a global scale is not wellknown, because acute infection is generallyasymptomatic. About 150,000 new cases occur annuallyin the US and in Western Europe, and about 350,000 inJapan. Of these, about 25% are asymptomatic, but 60 to
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
11H e p a t i t i s CH e p a t i t i s C
H
▲
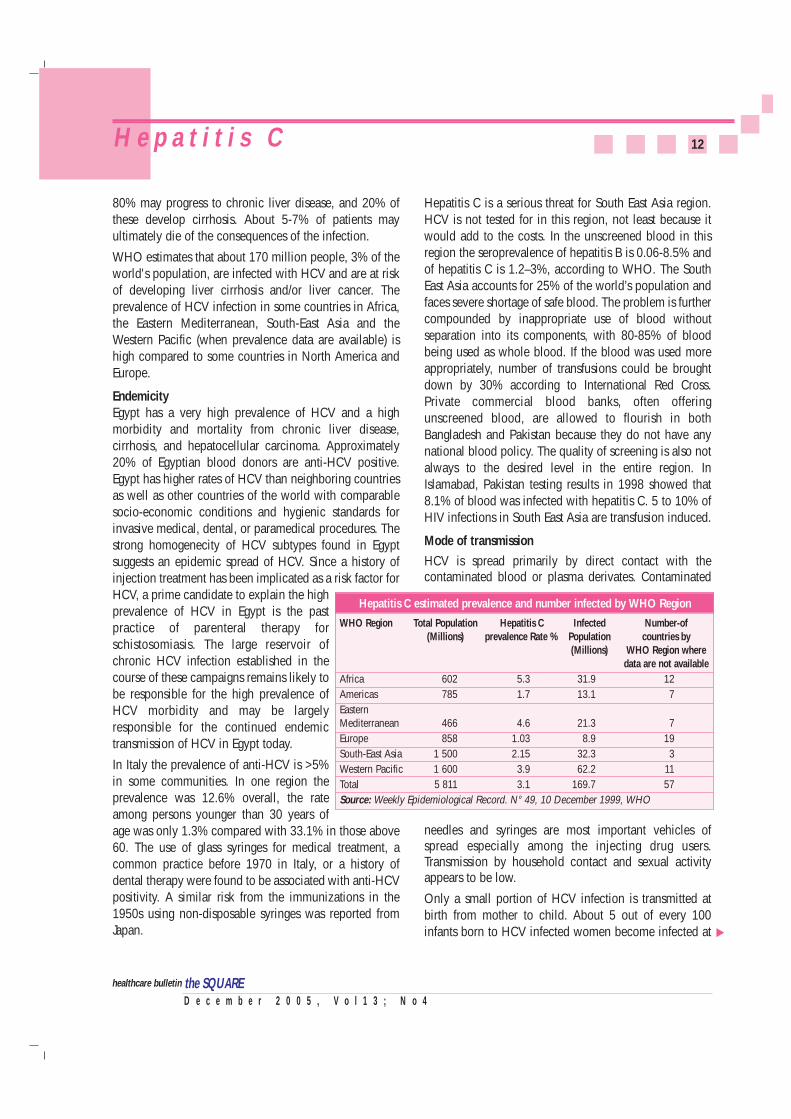
Hepatitis C global infection ratesCountry Population Residents with Percent of population
HCV infections infected with HCV
Bangladesh 150,589,000 3,614,136 2.4%India 1,041,543,000 18,747,774 1.8%Pakistan 162,409,000 3,897,816 2.4%Nepal 24,409,000 144,504 0.6%Sweden 8,560,000 257 0.003%United Kingdom 58,393,000 11,679 0.02%United States 266,096,000 4,789,728 1.8%Egypt 64,210,000 11,622,010 18.1%
Source: World Health Organization c. 1999.
Hepatitis C virus
80% may progress to chronic liver disease, and 20% ofthese develop cirrhosis. About 5-7% of patients mayultimately die of the consequences of the infection.
WHO estimates that about 170 million people, 3% of theworld's population, are infected with HCV and are at riskof developing liver cirrhosis and/or liver cancer. Theprevalence of HCV infection in some countries in Africa,the Eastern Mediterranean, South-East Asia and theWestern Pacific (when prevalence data are available) ishigh compared to some countries in North America andEurope.
EndemicityEgypt has a very high prevalence of HCV and a highmorbidity and mortality from chronic liver disease,cirrhosis, and hepatocellular carcinoma. Approximately20% of Egyptian blood donors are anti-HCV positive.Egypt has higher rates of HCV than neighboring countriesas well as other countries of the world with comparablesocio-economic conditions and hygienic standards forinvasive medical, dental, or paramedical procedures. Thestrong homogenecity of HCV subtypes found in Egyptsuggests an epidemic spread of HCV. Since a history ofinjection treatment has been implicated as a risk factor forHCV, a prime candidate to explain the highprevalence of HCV in Egypt is the pastpractice of parenteral therapy forschistosomiasis. The large reservoir ofchronic HCV infection established in thecourse of these campaigns remains likely tobe responsible for the high prevalence ofHCV morbidity and may be largelyresponsible for the continued endemictransmission of HCV in Egypt today.
In Italy the prevalence of anti-HCV is >5%in some communities. In one region theprevalence was 12.6% overall, the rateamong persons younger than 30 years ofage was only 1.3% compared with 33.1% in those above60. The use of glass syringes for medical treatment, acommon practice before 1970 in Italy, or a history ofdental therapy were found to be associated with anti-HCVpositivity. A similar risk from the immunizations in the1950s using non-disposable syringes was reported fromJapan.
Hepatitis C is a serious threat for South East Asia region.HCV is not tested for in this region, not least because itwould add to the costs. In the unscreened blood in thisregion the seroprevalence of hepatitis B is 0.06-8.5% andof hepatitis C is 1.2–3%, according to WHO. The SouthEast Asia accounts for 25% of the world’s population andfaces severe shortage of safe blood. The problem is furthercompounded by inappropriate use of blood withoutseparation into its components, with 80-85% of bloodbeing used as whole blood. If the blood was used moreappropriately, number of transfusions could be broughtdown by 30% according to International Red Cross.Private commercial blood banks, often offeringunscreened blood, are allowed to flourish in bothBangladesh and Pakistan because they do not have anynational blood policy. The quality of screening is also notalways to the desired level in the entire region. InIslamabad, Pakistan testing results in 1998 showed that8.1% of blood was infected with hepatitis C. 5 to 10% ofHIV infections in South East Asia are transfusion induced.
Mode of transmissionHCV is spread primarily by direct contact with thecontaminated blood or plasma derivates. Contaminated
needles and syringes are most important vehicles ofspread especially among the injecting drug users.Transmission by household contact and sexual activityappears to be low.
Only a small portion of HCV infection is transmitted atbirth from mother to child. About 5 out of every 100infants born to HCV infected women become infected at
12H e p a t i t i s C
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
▲
Hepatitis C estimated prevalence and number infected by WHO Region
WHO Region Total Population Hepatitis C Infected Number-of (Millions) prevalence Rate % Population countries by
(Millions) WHO Region where data are not available
Africa 602 5.3 31.9 12
Americas 785 1.7 13.1 7
Eastern Mediterranean 466 4.6 21.3 7
Europe 858 1.03 8.9 19
South-East Asia 1 500 2.15 32.3 3
Western Pacific 1 600 3.9 62.2 11
Total 5 811 3.1 169.7 57
Source: Weekly Epidemiological Record. N° 49, 10 December 1999, WHO
the time of birth. Unfortunately, no treatment can preventthis from happening. The risk of mother to infanttransmission of HCV increases dramatically if the motheris co-infected with HIV possibly due to an increase inHCV titer as a result of immunosuppression. The risk ofmother-baby transmission correlates with the titer ofmaternal HCV viremia. For women found to be HCVpositive, there are no recommendations againstpregnancy or breast-feeding, nor is a special methodrecommended to deliver the baby. However, invasive fetalmonitoring (e.g. using scalp electrodes) should beavoided. HCV-positive mothers should considerabstaining from breast-feeding if their nipples are crackedor bleeding.
Other modes of transmission such as social, cultural, andbehavioral practices using percutaneous procedures (e.g.ear and body piercing, circumcision, tattooing) can occurif inadequately sterilized equipment is used. HCV is notspread by sneezing, hugging, coughing, food or water,sharing eating utensils, or casual contact.
Risk groupsGroups at risk of contracting an HCV infection:
❏ Recipients of previously unscreened blood, bloodproducts and organs (blood transfusion or solid organtransplant before 1992, coagulation factorconcentrates before 1987)
❏ Patients and employees in hemodialysis centers(nosocomial infections)
❏ Hemophiliacs
❏ Injecting drug users sharing contaminated needlesand/or injection materials
❏ People exposed to unsterile medical or dentalequipment
❏ Occupational exposure to blood
❏ People administrating or receiving acupunctureand/or tattooing with unsterile medical devices
❏ Health care workers
❏ Sexual, household and perinatal transmission ispossible.
❏ Infants born to infected mothers
A number of cases, 10% to 40%, have no identifiable riskfactor.
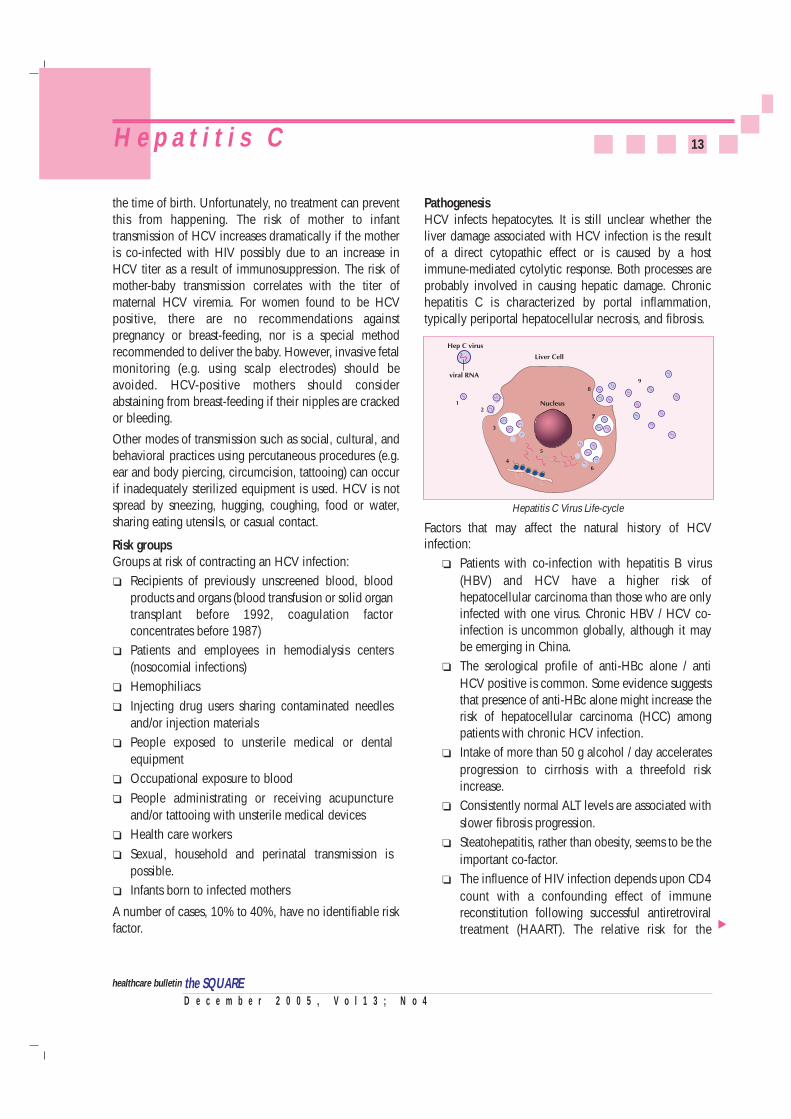
PathogenesisHCV infects hepatocytes. It is still unclear whether theliver damage associated with HCV infection is the resultof a direct cytopathic effect or is caused by a hostimmune-mediated cytolytic response. Both processes areprobably involved in causing hepatic damage. Chronichepatitis C is characterized by portal inflammation,typically periportal hepatocellular necrosis, and fibrosis.
Factors that may affect the natural history of HCVinfection:
❏ Patients with co-infection with hepatitis B virus(HBV) and HCV have a higher risk ofhepatocellular carcinoma than those who are onlyinfected with one virus. Chronic HBV / HCV co-infection is uncommon globally, although it maybe emerging in China.
❏ The serological profile of anti-HBc alone / antiHCV positive is common. Some evidence suggeststhat presence of anti-HBc alone might increase therisk of hepatocellular carcinoma (HCC) amongpatients with chronic HCV infection.
❏ Intake of more than 50 g alcohol / day acceleratesprogression to cirrhosis with a threefold riskincrease.
❏ Consistently normal ALT levels are associated withslower fibrosis progression.
❏ Steatohepatitis, rather than obesity, seems to be theimportant co-factor.
❏ The influence of HIV infection depends upon CD4count with a confounding effect of immunereconstitution following successful antiretroviraltreatment (HAART). The relative risk for the
13H e p a t i t i s C
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
▲
Hepatitis C Virus Life-cycle
development of cirrhosis among HIV and HCV co-infected patients is around two.
❏ Preliminary evidence suggests that smoking mayinfluence the development of HCC.
Viral load or genotypes do not influence disease severityor progression. The size of the viral inoculum receivedmay determine the course of disease: post-transfusioncases may proceed more aggressively than infectionsassociated with injecting drug use (IDU). Diseaseexpression is related to viral expression: low levels ofcirculating HCV RNA are generally found inasymptomatic patients with normal ALT levels.Experiments carried out with chimpanzees have shownthat the administration of powerful immunosuppressantsbefore and after virus inoculation prevents thedevelopment of acute hepatitis despite viremia in theanimal and viral expression in the liver. Removal of theimmunosuppressant triggered an immune response whichresulted in the onset of acute hepatitis followed by viruselimination
Clinical features of acute infectionThe incubation period for acute hepatitis C averages 6 to10 weeks. Most persons who develop acute hepatitis Chave no symptoms. The onset of disease is usuallyinsidious, with anorexia, vague abdominal discomfort,nausea and vomiting, fever and fatigue, progressing tojaundice in about 25% of patients, less frequently thanhepatitis B. Rapid, fulminant liver failure associated withHCV infection is a rare event. Probably as many as 70%-90% of infected people fail to clear the virus during theacute phase of the disease and become chronic carriers.
Chronic infection and consequencesAn important clinical feature of infection with HCV is thehigh rate of chronic hepatitis and slowly progressivelifelong infection, which may lead to cirrhosis and liverfailure in about 10%-20% of persons with chronichepatitis C. HCV-associated cirrhosis leads to liver failureand death in about 20%-25% of cirrhotic cases. HCV-associated cirrhosis now represents a leading indicationfor liver transplantation. Chronic HCV infection appearsto be associated with the development of hepatocellularcarcinoma (HCC) in 1%-5% of persons with chronichepatitis C. Development of HCC is rare in patients withchronic hepatitis C who do not have cirrhosis. Chronic
infection is often not symptomatic, until evidence of liverfailure becomes clinically apparent. The rate ofprogression to cirrhosis is usually slow, with 20 or moreyears elapsing between infection and the development ofserious complications. The period of communicabilityspans from one or more weeks before onset of the firstsymptoms and may persist in most persons indefinitely.HCV infection does not cause fulminant hepatic failure,but, occurring in the setting of another chronic liverdisease such as chronic HBV infection, may precipitateliver failure. Persons who have chronic liver disease are atincreased risk for fulminant hepatitis A. Most of theserious liver disease associated with HCV is aconsequence of the chronic, persistent nature of theinfection. Even in the asymptomatic carrier, a decrease inquality of life has been reported. Histopathology gradeand stage of liver damage is not reflected by serumALT/AST levels or serological status.
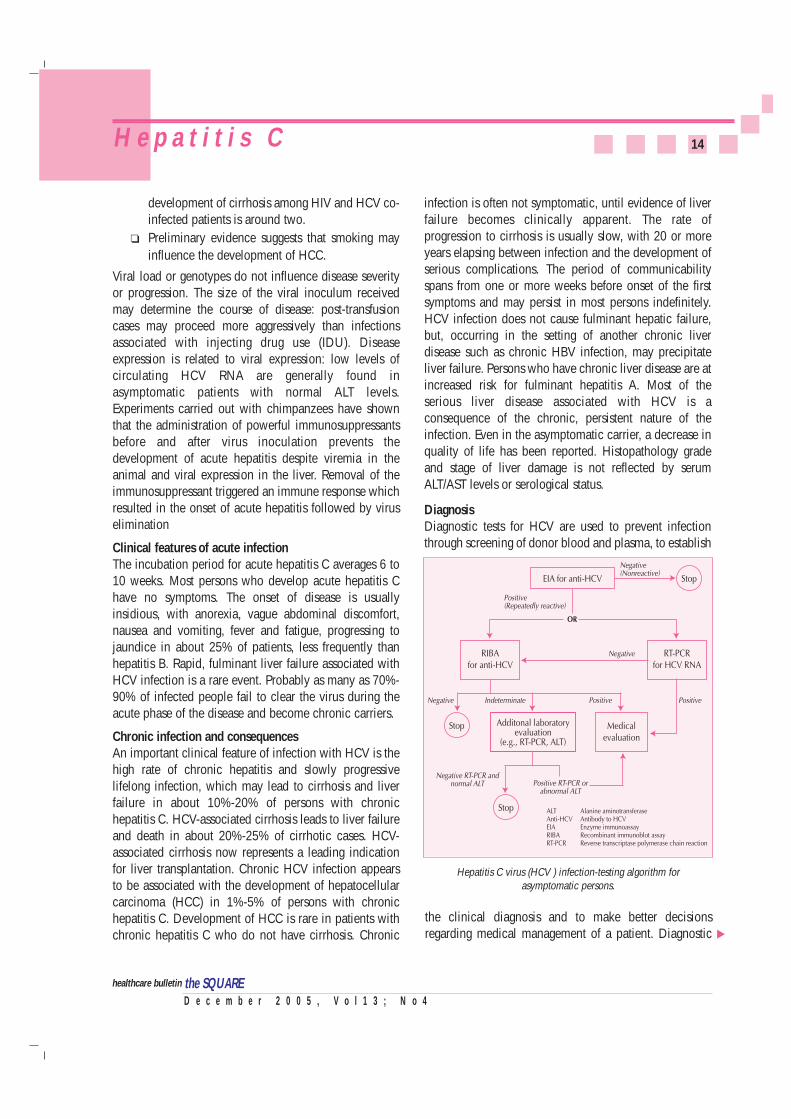
DiagnosisDiagnostic tests for HCV are used to prevent infectionthrough screening of donor blood and plasma, to establish
14H e p a t i t i s C
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
▲
Hepatitis C virus (HCV ) infection-testing algorithm forasymptomatic persons.
the clinical diagnosis and to make better decisionsregarding medical management of a patient. Diagnostic

tests commercially available are based on Enzymeimmunosorbant assays (EIA) for the detection of HCVspecific antibodies. EIAs can detect more than 95% ofchronically infected patients but can detect only 50% to70% of acute infections. A recombinant immunoblotassay (RIBA) that identifies antibodies which react withindividual HCV antigens is often used as a supplementaltest for confirmation of a positive EIA result. Testing forHCV circulating by amplification tests RNA (e.g.polymerase chain reaction or PCR, branched DNA assay)is also being utilized for confirmation of serological resultsas well as for assessing the effectiveness of antiviraltherapy. A positive result indicates the presence of activeinfection and a potential for spread of the infection andor/the development of chronic liver disease.
TreatmentAntiviral drugs such as interferon taken alone or incombination with ribavirin, can be used for the treatmentof persons with chronic hepatitis C, but the cost oftreatment is very high. Treatment with interferon alone iseffective in about 10% to 20% of patients. Interferoncombined with ribavirin is effective in about 30% to 50%of patients. Ribavirin does not appear to be effective whenused alone.
PreventionThere is no vaccine against HCV. Research is in progressbut the high mutability of the HCV genome complicatesvaccine development. Lack of knowledge of anyprotective immune response following HCV infection alsoimpedes vaccine research. It is not known whether theimmune system is able to eliminate the virus. Somestudies, however, have shown the presence of virus--neutralizing antibodies in patients with HCV infection.
In the absence of a vaccine, all precautions to preventinfection must be taken including:
❏ Screening and testing of blood, plasma, organ,tissue, and semen donors;
❏ Virus inactivation of plasma derived products;
❏ Implementation and maintenance of infectioncontrol practices in health care settings, includingappropriate sterilization of medical and dentalequipment;
❏ Promotion of behavior change among the generalpublic and health care workers to reduce overuseof injections and to use safe injection practices;and Risk reduction counseling for persons withhigh-risk drug and sexual practices.
Routine precautions for the care of all hemodialysispatients-
◆ Patients should have specific dialysis stationsassigned to them, and chairs and beds shouldbe cleaned after each use.
◆ Sharing among patients of ancillary suppliessuch as trays, blood pressure cuffs, clamps,scissors, and other nondisposable items shouldbe avoided.
◆ Nondisposable items should be cleaned ordisinfected appropriately between uses.
◆ Medications and supplies should not be sharedamong patients, and medication carts shouldnot be used.
◆ Medication should be prepared and distributedfrom a centralized area.
◆ Clean and contaminated areas should beseparated.
Postexposure follow-up of health-care, emergencymedical, and public safety workers for HCV infection
❏ For the source, baseline testing for anti-HCV.❏ For the person exposed to an HCV-positive
source, baseline and follow-up testing including-◆ Baseline testing for anti-HCV and ALT activity;
and◆ Follow-up testing for anti-HCV (at 4-6 months)
and ALT activity.❏ Confirmation by supplemental anti-HCV testing
of all anti-HCV results reported as positive byenzyme immunoassay (EIA).
Reference:❍ World Health Organization, 2002❍ Centers for Disease Control & Prevention, December 17, 2004❍ National Center for Complementary and Alternative Medicine,
2003❍ Mayo Foundation for Medical Education and Research, February
18, 2004.❍ News. BMJ; Volume 320; 15 April 2000.
15H e p a t i t i s C
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
the SQUARE

16Inauguration of SQUARE Cephalosporins Ltd.Inauguration of SQUARE Cephalosporins Ltd.
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
Yet another milestone in Pharmaceutical manufacturing was set by Square onSeptember 27, 2005 when the company launched its dedicated and state of theart Cephalosporin Manufacturing facility at Kaliakor, Gazipur.
Dr. Khandaker Mosharraf Hossain, MP, Hon’ble Minister for Health and FamilyWelfare inaugurated the facility built as per US, FDA and UK, MHRA cGMPspecifications. Mr. Mizanur Rahman Sinha, MP Hon’ble State Minister for Healthand family Welfare also graced the occasion.
This world class facility is housed in a 95,000 sq. feet of covered area and willmanufacture Cephalosporin antibiotics in tablets, Capsules, Dry Syrup andInjectable preparations. The annual capacity per shift of the plant is 64 million
tablets, 47 million capsules, 3.32 million bottle of dry syrps and 10.58 million ofinjectables. The facility was built by Telstar S.A. of Spain, a world renownedpharmaceutical manufacturing facility, on a turn key basis.
The facility will add new era in Pharmaceutical export from Bangladesh. Patientsin the country will also now get developed country standard Cephalosporinsfrom the facility.
Presidents and Secretary Generals of Bangladesh Medical Association (BMA) andBangladesh Pharmaceutical Manufacturers Association (BAPI) along with manydignitaries from Home and Abroad attended the inauguration.

17MSD Activities 2005- Few HighlightsMSD Activities 2005- Few Highlights
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
SQUARE Pharmaceuticals Ltd. sponsored the scientific seminar on“Post Stroke Rehabilitation” organized by Rotary Health Care and
Physiotherapy Centre in Association of CRP Savar, Dhaka at Khulna.
The distinguished guests of the International Scientific Seminar at HotelAgrabad, Chittagong. The program was organized by OGSB and
sponsored by MSD, SQUARE Pharmaceuticals Ltd.
Medical Services Dept. (MSD) of SQUARE Pharmaceuticals Ltd. organized the scientific seminar on “Osteoporosis andIts Management” at the Gynae & Obstetrics Dept. of BSMMU, Dhaka.
MSD of SQUARE sponsored the “Annual Scientific Seminar” ofChittagong Medical College Teachers Association at Chittagong.
MSD of SQUARE Pharmaceuticals Ltd. sponsored a scientific seminar on “RenalMycosis” organized by Teachers’ Association of RMCH. Prof. K. L. Gupta from
Post-Graduate Institute of Nephrology, Chandigarh, India was the keynote speaker.
18
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
T e s t Y o u r s e l fT e s t Y o u r s e l f
Test YourselfTest Yourself
Correct answers of the 'Test Yourself - 20’1. b & c 2. a & c 3. a & d 4. a & d 5. b & c 6. a & c
1. All the following regarding "Neuropathic Pain" iscorrect except:a. It is described as 'burning', 'electric', 'tingling' and
'shooting' in nature.b. It is "continuous" in presentation.c. It is a worldwide acute disability. d. Multiple sclerosis, post-traumatic myopathy can
lead to 'central pain'.
2. The following points are true for "Telemedicine"except:a. It helps in remote patients monitoring.b. Patient transfer is possible through this.c. Consumers' medical and health information can
be transferred.d. Specialist referral services can be achieved.
3. The below mentioned points are true for"Neuropathic Pain" except:a. DPN occurs in diabetic persons at a rate of 11% in
those who are insulin dependent. b. About 9% - 24% of the patients with herpes zoster
infection will develop PHN.c. Complete pain relieve may not be achieved with
treatment.d. TCA should be used with caution in persons with
a history of cardiac conduction disturbances.
4. All the following points are true except:a. Vertina® has CNS depressant, antiemetic,
anticholinergic, antispasmodic and antihistaminicproperties.
b. Vertina® is only indicated for the prevention andtreatment of nausea and vomiting.
c. Vertina® is chewable tablet.d. Use of Vertina® is not recommended for the
children under 12 years of age.
5. All the following are correct regarding clinicalapplications of "Telemedicine" except:a. Consultation, including second opinion.b. Monitoring and tracking the patients status. c. Supervision of primary care by the physician only.d. Continuous provisions of specialty care by a local
specialist.
6. All the following points are true for "Hepatitis C"except:a. Globally, an estimated 170 million persons are
chronically infested with HCV. b. Sneezing, coughing, food or water spreads HCV. c. The incubation period for acute hepatitis C
averages 6-10 weeks. d. HCV is spread primarily by contaminated blood or
plasma derivatives.
The following are the 10 winners of the “Test Yourself -20”; they have been selected through lottery.
Congratulations from “the SQUARE” Editorial BoardDr. A. E. M. Mazharul IslamAsst. Professor, CardiologyNICVD, Dhaka
Dr. Debasish Ghose, MBBSMedical OfficerUpazila Health ComplexLohagara, Chittagong
Dr. Md. Anwar HussainMBBS, MCPS (ENT), DLOConsultant, ENTSadar HospitalBrahmanbaria
Dr. Md. Arifur Rahman, MBBSInternee Doctor, Surgery Unit – IIISher-E-Bangla Medical College Hospital,Barisal
Dr. Md. Liaquat Ali Mollah, FCPS (Paed)Consultant, PaediatricsGeneral HospitalNarayanganj
Dr. Md. Maruful IslamMBBS, FCPS(P-II)A/R, Surgery Unit-IIRangpur Medical College Hospital
Dr. Md. Najmul Karim (Robin), MBBSHouse No. 471, Road No. 1/5G. L. Roy RoadRangpur
Dr. Sayeed Ahmed, MBBSRoom No. 309Dr. Milon Internee HostelBakshi Bazar, Dhaka
Dr. Syed Amanul Islam, MBBSEMOKhulna Medical College HospitalKhulna
Dr. Tangina, MBBSRoom No. 107, Rumana Smriti HostelSir Salimullah Medical College &Mitford HospitalDhaka
Soon our officials will be
visiting you with a token of our appreciation
ertina®
Composition Vertina® Tablet : Each chewable tablet contains Meclizine
HCl USP 50 mg.
Chemical Structure
PharmacologyVertina® (Meclizine hydrochloride) is an antihistaminewhich shows marked protective activity against nebulizedhistamine and lethal doses of intravenously injectedhistamine in guinea pigs. It has a marked effect inblocking the vasodepressor response to histamine, butonly a slight blocking action against acetylcholine. Itsactivity is relatively weak in inhibiting the spasmogenicaction of histamine on isolated guinea pig ileum.
Mechanism of ActionMeclizine has CNS depressant, antiemetic,anticholinergic, antispasmodic and antihistaminicproperties. Meclizine depress labyrinth excitability andconduction in vestibular-cerebellar pathways. Theantiemetic and antimotion sickness action of meclizineresult from its central anticholinergic and CNS depressantproperties.
IndicationVertina® (Meclizine hydrochloride) is indicated for theprevention and treatment of nausea and vomiting, anddizziness associated with motion sickness. It is alsoindicated in the management of vertigo associated withdiseases affecting the vestibular system.
Dosage and AdministrationVertigoFor the control of vertigo associated with diseasesaffecting the vestibular system, the recommended dose ofVertina® (Meclizine hydrochloride) is 25 to 100 mg daily,in divided dosage, depending upon clinical response.
19
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
P r o d u c t P r o f i l e - V e r t i n a ®P r o d u c t P r o f i l e - V e r t i n a ®
V Motion SicknessThe initial dose of 25 to 50 mg of Vertina® (Meclizinehydrochloride) should be taken one hour prior toembarkation for protection against motion sickness.Thereafter, the dose may be repeated every 24 hours forthe duration of the journey.
Contraindication and PrecautionMeclizine HCl is contraindicated in individuals who haveshown a previous hypersensitivity to it.
Since drowsiness may, on occasion, occur with use of thisdrug, patients should be warned of this possibility andcautioned against driving a car or operating dangerousmachinery.
Patients should avoid alcoholic beverages while takingthis drug. Due to its potential anticholinergic action, thisdrug should be used with caution in patients with asthma,glaucoma, or enlargement of the prostate gland.
Side EffectDrowsiness, dry mouth and on rare occasions, blurredvision have been reported.
Use in Pregnancy and LactationPregnancy Category B. Epidemiological studies inpregnant women, do not indicate that Meclizine increasesthe risk of developmental anomalies or any abnormalitieson fetus when administered during pregnancy.Nevertheless, Meclizine, or any other medication, shouldbe used during pregnancy only if clearly necessary.
Usage in ChildrenClinical studies establishing safety and effectiveness inchildren have not been done; therefore, usage is notrecommended in children under 12 years of age.
Storage ConditionStore in a cool and dry place, protect from light andmoisture. Keep all medication out of reach of children.
How SuppliedVertina® Tablet : Each box contains 5x10 chewable
tablets in blister pack.
the SQUARE
CI N N CH2
CH3
● 2HCI ● H2O
HC

20M e d i c a l B r e a k t h r o u g hM e d i c a l B r e a k t h r o u g h
New Revolutionary CT Scanner!
A new generation of imaging technology is wowingdoctors and patients alike. This speedy, pinpoint-accuratemachine is changing how doctors view the body.
Like older models, this CT scanner takes cross-sectionalpictures of the body using X-rays and detectors. What'sdifferent is its speed. In the 70s, it used to take fiveminutes to take one rotation. In the early 90s, it wentdown to one second per one rotation, and towards the late1990s, it went to about half a second for four slices in onerotation.
With this new scanner,doctors can now take 64slices every half second.The new scanner is so fastthat it can basically freezethe motion of the heart.The other advantage forthem is the diagnosis ismuch more accurate. Doctors say the speed of thescanner will help them unravel more medical mysteries-one scan at a time.
SOURCE: Ivanhoe Broadcast News
Blood Test Predicts Heart Disease Deaths
A simple blood test may help determine who is more atrisk of dying from cardiovascular disease. The testmeasures gamma-glutamyl transferase (GGT), an enzymeproduced primarily by the liver. The enzyme is elevated insome forms of liver disease. Now, researchers in Austriafound the higher the blood level of GGT, the greater therisk of cardiovascular death. Researchers say that peoplewith high GGT have 1.5-fold more risk of dying fromcardiovascular diseases in comparison to people withnormal low levels of GGT.
The study also shows the risk of cardiovascular death is28-percent higher for men with moderately high GGTcompared to those with normal levels of the enzyme. Itwent up to 64-percent for men with highly elevated GGT.In women, the increase in risk ranged from 35 percent to51 percent.
Researchers cite two reasons GGT can predict the risk ofcardiovascular death: High levels of GGT show thepresence of atherosclerosis, and the enzyme is related to
the harmful effects of heavy drinking on blood vessels.
Researchers analyzed data on more than 160,000Austrian adults. They were age 19 or older when the studybegan. Researchers followed them for an average of 11years to 12 years.
SOURCE: Circulation, 2005; 11 2.
“Good Bye” to Cataracts and Glasses!
A cataract clouds the eye's natural lens, making it hard tosee clearly. Now, some patients can get rid of cataractsand their glasses or contacts at the same time.
A new lens doesdouble duty. The"new lens" is a lensthat has differentzones of focus builtinto the plastic of thelens. When this lens isplaced into the eye, itallows the patient tofocus distant, interme-diate and close-up. Once it is unfolded, It has pretty muchthe consistency of a stick of gum. In clinical trials, 80percent of patients who got the "new lens" no longerneeded glasses.
SOURCE: Ivanhoe Broadcast News
Implanted Device for Depression!
The FDA has approved a first-of-its-kind implantableelectrical nerve stimulator device to treat severedepression. The device, called the Vagus NerveStimulation (VNS) System, was approved for adult patientswith long-term or recurrent major depression that has notresponded adequately to four or more antidepressanttreatments.
VNS consists of a stopwatch-sized device that's surgicallyimplanted in the upper chest. Tiny wires attach the deviceto the vagus nerve, which runs from the neck to the brainThe eiectrical stimulation is thought to alter the chemicaltransmitters that carry messages between nerve cellsinvolved in regulating mood.
More than 32,000 patients worldwide have used the VNSTherapy System.
SOURCE: WebMD Medical News
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
the SQUARE
New Lens for Cataract
New CT Scanner
… from bacterial infectious diseases.
USFDA approved
Broad spectrum
Highly effective against typhoid fever in children
Effective option for switch therapy
Covers most patient groups (15 days to geriatric patients)
100 & 200 mg capsule
Dry powder for suspension
Paediatric drops
Cefpodoxime proxetil
Vanprox¤
Ensures ideal coverage in anorectal disorders
Erian®ointmentCinchocaine HCl BP 0.5% + Hydrocortisone BP 0.5% +
Framycetin Sulphate BP 1% + Esculin 1%
Relievesall symptoms of anorectal disorders
Ensuressynergistic activity
Ensures comfort & compliance
Welltolerated
Treats Ulcer Truly
Pantoprazole 20 mg & 40 mg Tablet
TrupanTrupan¤
More specific site-binding capability with proton pump
Truly once daily
Least side effects
Lack of unfavorable drug interactions
US FDA pregnancy category B
D e c e m b e r 2 0 0 5 , V o l 1 3 ; N o 4the SQUAREhealthcare bulletin
Production PharmaScope
Medical Services Department, SQUARE PHARMACEUTICALS LTD. Corporate Headquarters, SQUARE CENTRE 48, Mohakhali Commercial Area, Dhaka-1212, Tel : 8827729 - 38, 8817729 - 38, Fax : 880 -2-882 8608 / 882 8609E-mail : [email protected], Web Page : http://www.squarepharma.com.bd, Omar Akramur Rab <[email protected]>