cysts & sinuses of the neck
TRANSCRIPT

CONGENITAL CYSTS & CONGENITAL CYSTS & SINUSES OF THE NECKSINUSES OF THE NECK

Development . . . .Development . . . .
Head & neck is formed predominantly by Head & neck is formed predominantly by bars of mesenchyme adjacent to most bars of mesenchyme adjacent to most cranial part of foregut.cranial part of foregut.
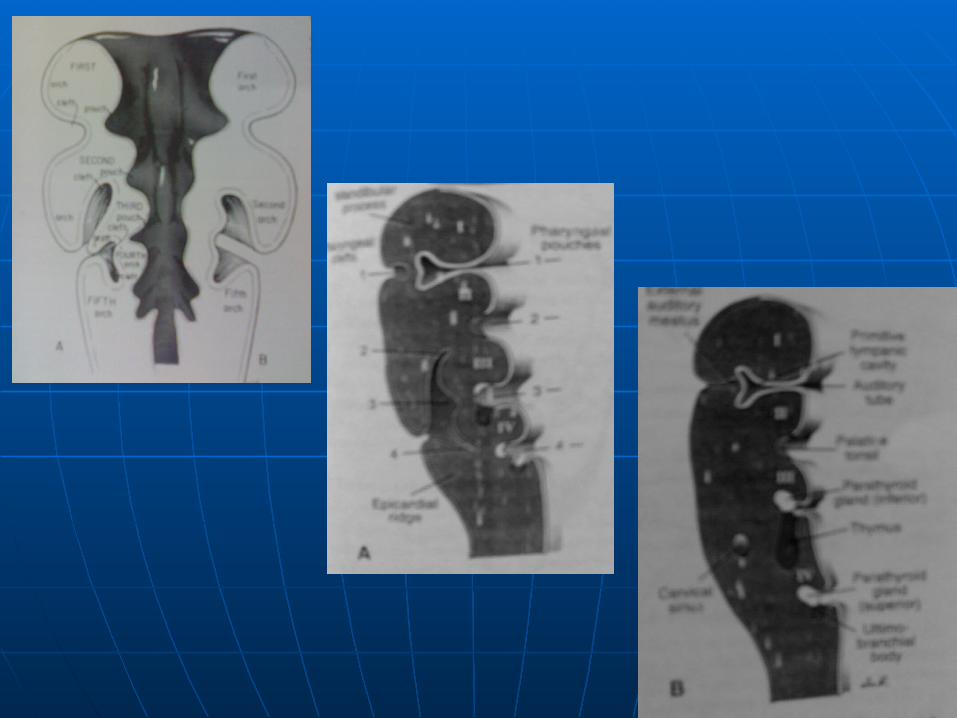
Pharyngeal / Branchial arches.Pharyngeal / Branchial arches.
Appear in the 4th & 5th week.Appear in the 4th & 5th week.
There are potentially 6 Branchial arches.There are potentially 6 Branchial arches.

Separated from the outside by deep Separated from the outside by deep clefts called branchial clefts.clefts called branchial clefts.
Outpouchings occur in the lateral Outpouchings occur in the lateral wall of the pharynx called branchial wall of the pharynx called branchial pouches.pouches.
Clefts meet corresponding pouch at Clefts meet corresponding pouch at the closing membrane.the closing membrane.
Open communication in amphibians Open communication in amphibians to form gills ( Branchia = gills ).to form gills ( Branchia = gills ).

Each arch consists of a core of Each arch consists of a core of mesenchymal tissue & neural crest mesenchymal tissue & neural crest cells cells
Each arch is characterized by its own Each arch is characterized by its own muscular component. These muscular component. These muscular components of each arch muscular components of each arch have their own cranial nerve & have their own cranial nerve & arterial supply.arterial supply.


First (Mandibular) archFirst (Mandibular) arch Maxillary process - premaxilla, maxilla, Maxillary process - premaxilla, maxilla,
zygomatic & temporal bone.zygomatic & temporal bone.
Mandibular process - Meckel’s cartilage - Mandibular process - Meckel’s cartilage - mandible, malleus & incus.mandible, malleus & incus.
Musculature: muscles of mastication,ant Musculature: muscles of mastication,ant belly of Digastric, Mylohyoid, Tensor belly of Digastric, Mylohyoid, Tensor tympani & palatini.tympani & palatini.
Nerve: mandibular branch of Trigeminal Nerve: mandibular branch of Trigeminal nerve.nerve.
Artery: maxillary arteryArtery: maxillary artery

Second (Hyoid) archSecond (Hyoid) arch Skeletal : Stapes, Styloid process of Skeletal : Stapes, Styloid process of
Temporal bone, Stylohyoid ligament, Temporal bone, Stylohyoid ligament, lesser horn & upper part of body of lesser horn & upper part of body of hyoid.hyoid.
Muscles - Stapedius, Stylohyoid, Muscles - Stapedius, Stylohyoid, posterior belly of Digastric, Auricular, posterior belly of Digastric, Auricular, muscles of facial expression.muscles of facial expression.
Nerve – Facial nerve.Nerve – Facial nerve. Artery – Stapedial artery.Artery – Stapedial artery.

3rd arch:3rd arch: Skeletal: lower part of body & greater Skeletal: lower part of body & greater
horn of hyoid.horn of hyoid. Muscle: Stylopharyngeus.Muscle: Stylopharyngeus. Nerve: Glossopharyngeal.Nerve: Glossopharyngeal. Artery: Common carotid bifurcation, Artery: Common carotid bifurcation,
proximal internal carotid.proximal internal carotid.
4th & 6th arches4th & 6th arches Skeletal: Thyroid, Cricoid, Arytenoids, Skeletal: Thyroid, Cricoid, Arytenoids,
Corniculate & Cuneiform cartilages.Corniculate & Cuneiform cartilages.

Muscles :Muscles :
4th – Cricothyroid, Levator palitini & 4th – Cricothyroid, Levator palitini & constrictors of pharynx.constrictors of pharynx.
6th – intrinsic muscles of the larynx. 6th – intrinsic muscles of the larynx.
Nerve:Nerve:
4th – superior laryngeal branch of 4th – superior laryngeal branch of the Vagus.the Vagus.
6th– recurrent laryngeal branch of 6th– recurrent laryngeal branch of Vagus.Vagus.


POUCHESPOUCHES
1st – Tubotympanic recess.1st – Tubotympanic recess. 2nd – Palatine tonsil. Part of pouch 2nd – Palatine tonsil. Part of pouch
remains as tonsillar fossaremains as tonsillar fossa 3rd – Dorsal wing forms inferior 3rd – Dorsal wing forms inferior
parathyroid & ventral forms thymus.parathyroid & ventral forms thymus. 4th – Superior parathyroid gland. 4th – Superior parathyroid gland. 5th – Ultimobranchial body5th – Ultimobranchial body


CLEFTSCLEFTS Dorsal part of 1st cleft forms external Dorsal part of 1st cleft forms external
auditory meatus.auditory meatus. Mesenchyme of 2nd arch actively Mesenchyme of 2nd arch actively
proliferates to overlap 3 & 4th arches proliferates to overlap 3 & 4th arches to merge with the epicardial ridge in to merge with the epicardial ridge in the lower part of the neck.the lower part of the neck.
This forms a cavity lined by This forms a cavity lined by ectodermal epithelium – cervical ectodermal epithelium – cervical sinus – which eventually disappears.sinus – which eventually disappears.

THYROIDTHYROID Epithelial proliferation in the floor of the Epithelial proliferation in the floor of the
pharynx between the Tuberculum impar pharynx between the Tuberculum impar & Copula indicated by foramen Caecum. & Copula indicated by foramen Caecum.
Descends in front of the pharynx as a Descends in front of the pharynx as a bilobed diverticulum. bilobed diverticulum.
During this migration it remains During this migration it remains connected to the tongue by a narrow connected to the tongue by a narrow canal – Thyroglossal duct. canal – Thyroglossal duct.

Thyroid descends in front of the Thyroid descends in front of the hyoid & laryngeal cartilages. hyoid & laryngeal cartilages.
Reaches its final position in front of Reaches its final position in front of trachea by 7th wk. It acquires a small trachea by 7th wk. It acquires a small median isthmus & two lateral lobes. median isthmus & two lateral lobes.
Starts functioning by 4th month.Starts functioning by 4th month.

Branchial anomaliesBranchial anomalies
More than 90% of branchial cleft More than 90% of branchial cleft anomalies are second arch anomalies are second arch anomaliesanomalies
M:F equalM:F equal When sinus is present most Branchial When sinus is present most Branchial
anomalies are diagnosed in the first anomalies are diagnosed in the first decade of life, when there is no decade of life, when there is no external sinus diagnosis may not be external sinus diagnosis may not be made until adulthood made until adulthood

Branchial CystBranchial Cyst
Cyst presents as a soft mass deep to Cyst presents as a soft mass deep to the Sternomastoid muscle on its the Sternomastoid muscle on its upper third. upper third.
Sudden appearance of a painful mass Sudden appearance of a painful mass in this location may be the first sign.in this location may be the first sign.
Cysts usually between 5 – 10 cms in Cysts usually between 5 – 10 cms in size. size.

Protrudes from beneath the anterior Protrudes from beneath the anterior border of sternomastoid. border of sternomastoid.
Round to oval with long axis running Round to oval with long axis running forwards & downwards, cannot be forwards & downwards, cannot be reduced or compressedreduced or compressed
Usually not transilluminant. Usually not transilluminant.
Branchiogenic carcinoma in 1% Branchiogenic carcinoma in 1% remnants. remnants.

ManagementManagement
Because of likelihood of infection excision Because of likelihood of infection excision is generally recommended.is generally recommended.
Complete excision to avoid recurrence.Complete excision to avoid recurrence.
Surgery done after the age of 3 months.Surgery done after the age of 3 months.
In presence of infection excision is In presence of infection excision is delayed. Antibiotics and needle delayed. Antibiotics and needle aspiration is advised.aspiration is advised.

Incision is made parallel to Incision is made parallel to Langers lines.Langers lines.
Cyst may extend between the Cyst may extend between the origins of internal & external origins of internal & external carotid arteries upto pharyngeal carotid arteries upto pharyngeal wall.wall.
Hypoglossal, Glossopharyngeal Hypoglossal, Glossopharyngeal nerves lie deep to the cyst.nerves lie deep to the cyst.

Branchial FistulaBranchial Fistula Tiny pit in the skin at the lower third of ant Tiny pit in the skin at the lower third of ant
border of Sternomastoid muscle which may border of Sternomastoid muscle which may discharge.discharge.
Sinus b/l in 30% cases.Sinus b/l in 30% cases.
Cord may be palpable running upward in the Cord may be palpable running upward in the neck from the ostium, milking the tract neck from the ostium, milking the tract provides a mucoid discharge.provides a mucoid discharge.
Swallowing will cause the fistula to be tucked Swallowing will cause the fistula to be tucked in causing prominent dimpling. in causing prominent dimpling.
Course of the fistulaCourse of the fistula
From opening, passes subcutaneously to From opening, passes subcutaneously to level of upper border of thyroid cartilage.level of upper border of thyroid cartilage.
Pierces deep fascia & passes through Pierces deep fascia & passes through bifurcation of common carotid. bifurcation of common carotid.
All structures of second arch will be All structures of second arch will be superficial & 3rd arch will be deep. superficial & 3rd arch will be deep.
It passes deep to post belly of digastric & It passes deep to post belly of digastric & Stylohyoid.Stylohyoid.
Superficial to IJV, Hypoglossal & Superficial to IJV, Hypoglossal & Glossopharyngeal n & Stylopharyngeus Glossopharyngeal n & Stylopharyngeus muscle. muscle.
Pierces superior constrictor & opens on the Pierces superior constrictor & opens on the posterior pillar of tonsillar fossa.posterior pillar of tonsillar fossa.


ManagementManagement
Excision of the fistula.Excision of the fistula. Surgery done after the age of 3 Surgery done after the age of 3
months.months. Placement of probe into the sinus.Placement of probe into the sinus. In a child Branchial fistula can be In a child Branchial fistula can be
excised through a single incision excised through a single incision incorporating the sinus opening, incorporating the sinus opening, whereas in adolescents two stepladder whereas in adolescents two stepladder incisions may be required. incisions may be required.

Thyroglossal Duct Cyst:Thyroglossal Duct Cyst:
Course of Thyroglossal duct: Course of Thyroglossal duct:
Down from foramen Caecum between Down from foramen Caecum between the Genioglossi, then in midline either in the Genioglossi, then in midline either in front or through the hyoid, or hooks front or through the hyoid, or hooks below & behind the hyoid & then below & behind the hyoid & then descends downwards in the midline to descends downwards in the midline to upper border of thyroid cartilage. Then upper border of thyroid cartilage. Then moves slightly to the left & ends in moves slightly to the left & ends in pyramidal lobe of thyroid.pyramidal lobe of thyroid.

Most common congenital neck mass.Most common congenital neck mass.
More than 50% diagnosed in first two More than 50% diagnosed in first two decades of life.decades of life.
A draining sinus is always the result of A draining sinus is always the result of spontaneous or surgical drainage.spontaneous or surgical drainage.
60% are adjacent to hyoid, 24% above 60% are adjacent to hyoid, 24% above the hyoid, 13% below & 8% the hyoid, 13% below & 8% intralingual.intralingual.

Painless midline swelling, draining sinus or a Painless midline swelling, draining sinus or a tender mass.tender mass.
Occasionally may decompress into the mouth Occasionally may decompress into the mouth producing bad taste.producing bad taste.
Swelling moves with swallowing.Swelling moves with swallowing.
Pulled up & fixed on protrusion of tongue.Pulled up & fixed on protrusion of tongue.
Fluctuant, occasionally transilluminant.Fluctuant, occasionally transilluminant.
Can be moved sideways but not vertically. Can be moved sideways but not vertically.

Incidence of ectopic thyroid Incidence of ectopic thyroid misdiagnosed as Thyroglossal cyst is misdiagnosed as Thyroglossal cyst is 1 – 2%.1 – 2%.
? Thyroid scan to r/o Ectopic thyroid.? Thyroid scan to r/o Ectopic thyroid.
If there are s/o hypothyroidism.If there are s/o hypothyroidism.
USG of neck to demonstrate thyroid at USG of neck to demonstrate thyroid at its normal site.its normal site.

ManagementManagement Infected cyst – antibiotics & needle Infected cyst – antibiotics & needle
aspirationaspiration Incidence of malignancy – 1%Incidence of malignancy – 1% Excision of cyst along with complete Excision of cyst along with complete
thyroglossal tract upto the tongue, thyroglossal tract upto the tongue, with excision of 0.5 cm of healthy with excision of 0.5 cm of healthy tissue cuff around the tract. tissue cuff around the tract.
May necessitate excision of segment May necessitate excision of segment of hyoid in the midline. This is called of hyoid in the midline. This is called Sistrunk’s operationSistrunk’s operation


Thyroglossal FistulaThyroglossal Fistula
Generally fistula appears off and on due to Generally fistula appears off and on due to recurrent infection & rupture of cystrecurrent infection & rupture of cyst
Usually midlineUsually midline Hood or semi lunar fold of skin above the Hood or semi lunar fold of skin above the
fistulafistula Excision – SistrunkExcision – Sistrunk
Other cysts – Cystic Hygroma, Dermoid Other cysts – Cystic Hygroma, Dermoid cysts, Preauricular cysts & Thymic cysts cysts, Preauricular cysts & Thymic cysts

Cystic HygromaCystic Hygroma
Aggregation of cysts containing clear Aggregation of cysts containing clear lymphlymph
Sites – Posterior triangle of neckSites – Posterior triangle of neck
Cheek, Axilla, Mediastinum, Cheek, Axilla, Mediastinum,
Groin Groin Earliest swelling seen in the neckEarliest swelling seen in the neck Lower third of neck in the posteior Lower third of neck in the posteior
triangle triangle

Occasionally very large.Occasionally very large. Soft, cystic, smooth / lobulated Soft, cystic, smooth / lobulated
surface, compressible.surface, compressible. Brilliant Transillumination.Brilliant Transillumination. May cause respiratory distressMay cause respiratory distress Infection.Infection. Complete excision in single or staged Complete excision in single or staged
manner.manner. Monoclonal antibody – OK-432 Monoclonal antibody – OK-432
extracted from Streptococcus extracted from Streptococcus pyogenes.pyogenes.