copyright © cisst erc, 2004 nsf engineering research center for computer integrated surgical...
Post on 20-Dec-2015
215 views
TRANSCRIPT
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
Medical Robotics and Computer-Integrated Surgery
Russell H. TaylorDept. of Computer Science/Radiology/Mechanical EngineeringDirector, Center for Computer-Integrated Surgical Systems and TechnologyThe Johns Hopkins University3400 N. Charles Street; Baltimore, Md. [email protected]
NSF Engineering Research Center for Computer-Integrated Surgical Systems and Technology

Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
Disclosures• Russell Taylor is a member of the Scientific
Advisory Board of Integrated Surgical Systems and of Image Guide, Inc., and he consequently has (an exceedingly small) financial interest in these companies, and he may join other Advisory Boards.
• Some of Dr. Taylor’s patents have been licensed by Image Guide, Incorporated, and he consequently has a small financial interest in IG,
• Other of Dr. Taylor’s patents have been licensed by Intuitive Surgical Systems.
• ISS, IG, GE, Intuitive Surgical, Siemens, Medtronic, Burdette Medical, and several other companies whose systems were discussed in this talk are affiliates of the NSF CISST ERC, of which Dr. Taylor is the Director.
• Dr. Taylor also enjoys fishing
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
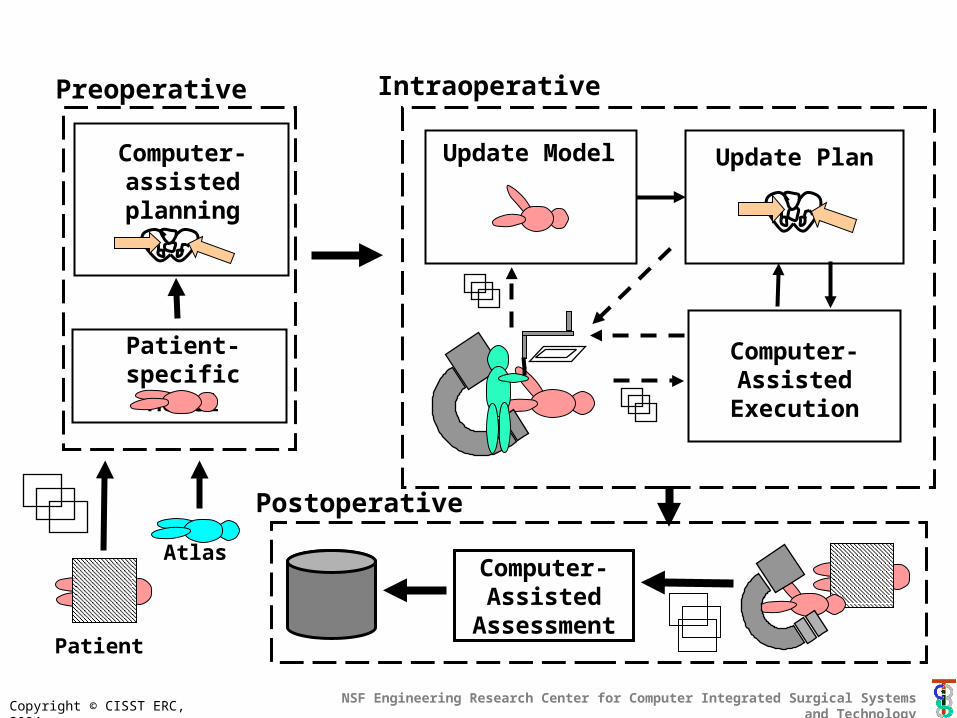
Computer-assisted planning
Patient-specific Model
Update Model
Computer- Assisted
Execution
Update Plan
Computer- Assisted
Assessment
Preoperative Intraoperative
Atlas
Postoperative
Patient

Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
Computer-assisted planning
Patient-specific Model
Update Model
Computer- Assisted
Execution
Update Plan
Computer- Assisted
Assessment
Preoperative Intraoperative
Atlas
PostoperativePatient
Surgical “CAD”
Surgical “TQM”
Surgical “CAM”

Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
Computer-assisted planning
Patient-specific Model
Update Model
Computer- Assisted
Execution
Update Plan
Computer- Assisted
Assessment
Preoperative Intraoperative
Atlas
Postoperative
Patient
Surgical
Assistants

Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
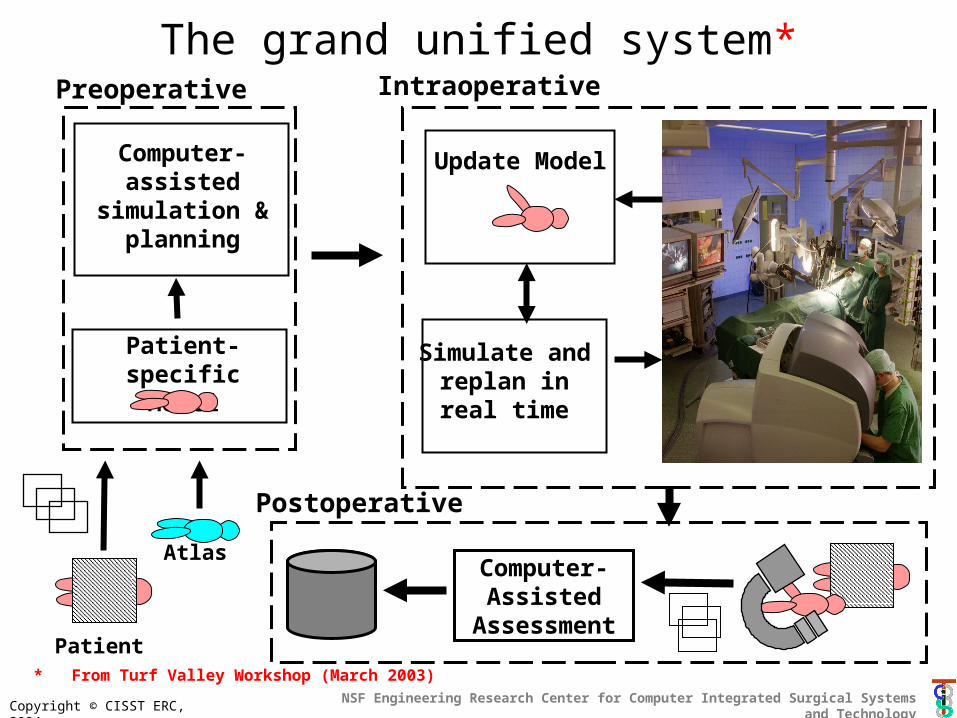
Computer-assisted
simulation & planning
Patient-specific Model
Update Model
Simulate and replan in real
time
Computer- Assisted
Assessment
Preoperative Intraoperative
Atlas
Postoperative
Patient
The grand unified system*
* From Turf Valley Workshop (March 2003)
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
Drivers for adoption• Error-free surgery
– Designs & systems to make things safer– Integration of imaging, computer assistance, etc.
• Enablers for otherwise infeasible interventions– Superhuman capabilities (access, precision, …)– Delivery systems for novel image-guided therapies
• Enablers for research & development– Consistency, capability & data gathering
• Capture of information about cases• Use of robots as training tools
– Mentoring– Simulation integrated with robotics
* From Turf Valley Workshop (March 2003)

Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
Research and technology barriers
Modeling & analysis• Segmentation• Registration• Atlases• Optimization• Visualization• Task characterization• etc.
Interface Technology• Sensing• Robotics• Human-machine
interfacesSystems• Safety & verifiability• Usability & maintainability• Performance and validation
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
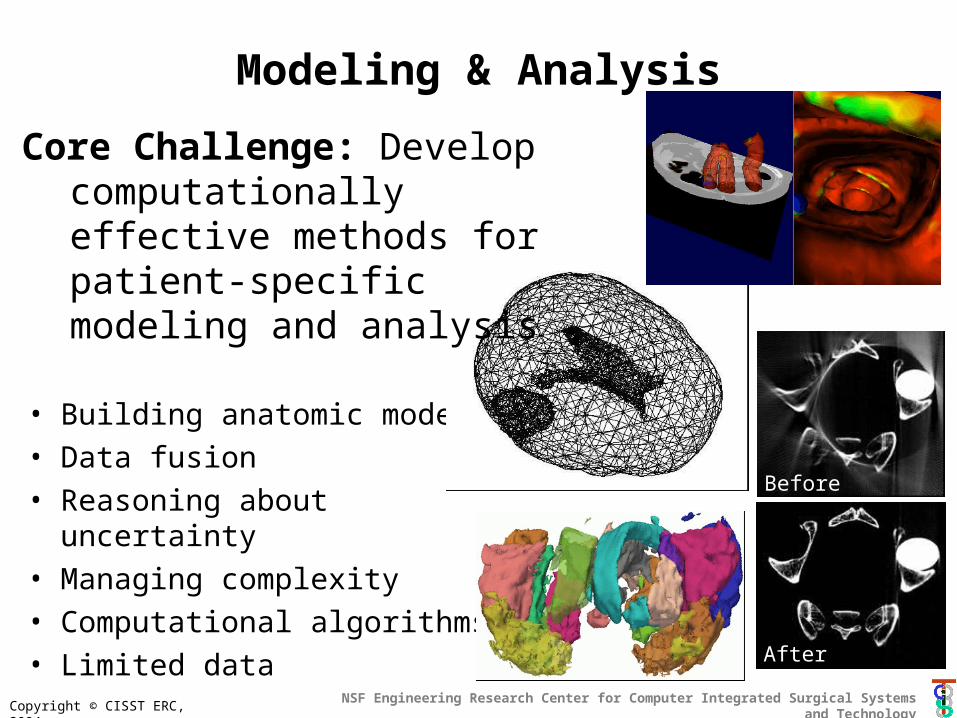
• Building anatomic models• Data fusion• Reasoning about uncertainty• Managing complexity• Computational algorithms• Limited data
Modeling & Analysis
Core Challenge: Develop computationally effective methods for patient-specific modeling and analysis
Before
After

Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
Modeling and Analysis Highlights
• Explosion of 3D imaging modalities
– MRI, CT, Ultrasound, etc.• Patient-specific models
based on images• Statistical atlases and
deformable models are emerging as crucial enabling technologies within CIS
• Beginning to see application of real-time computer vision methods
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
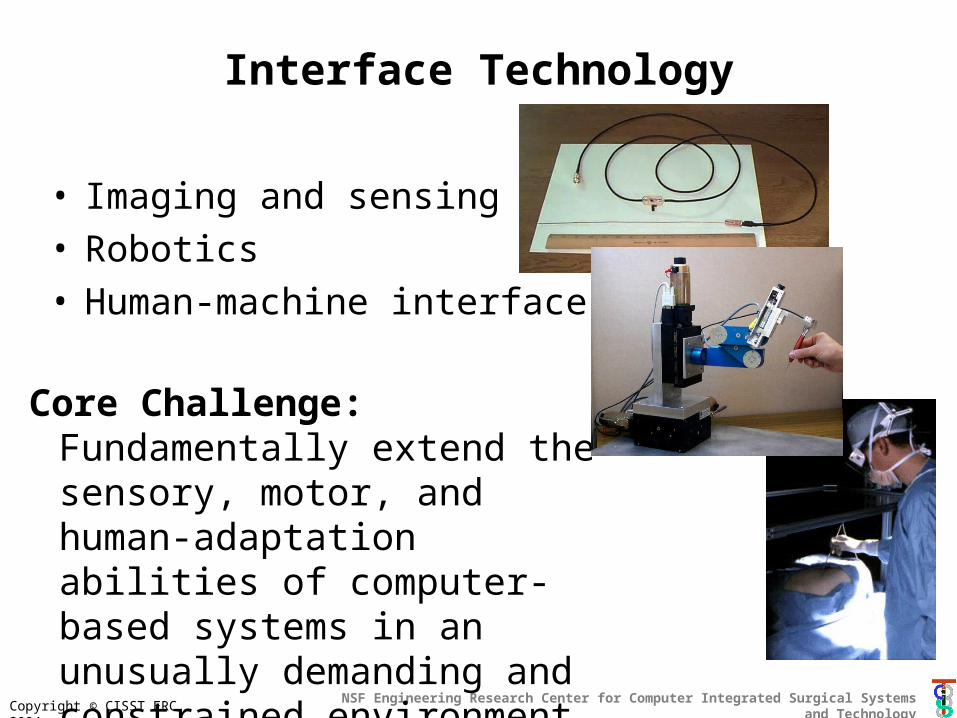
Interface Technology
• Imaging and sensing• Robotics• Human-machine interfaces
Core Challenge: Fundamentally extend the sensory, motor, and human-adaptation abilities of computer-based systems in an unusually demanding and constrained environment
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
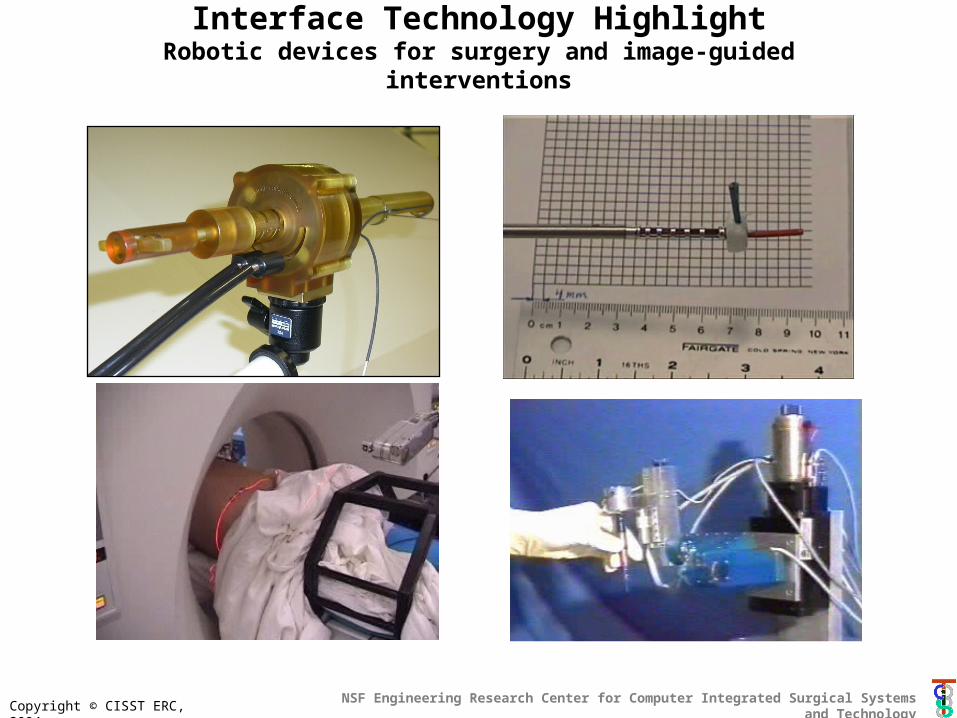
Interface Technology HighlightRobotic devices for surgery and image-guided interventions
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
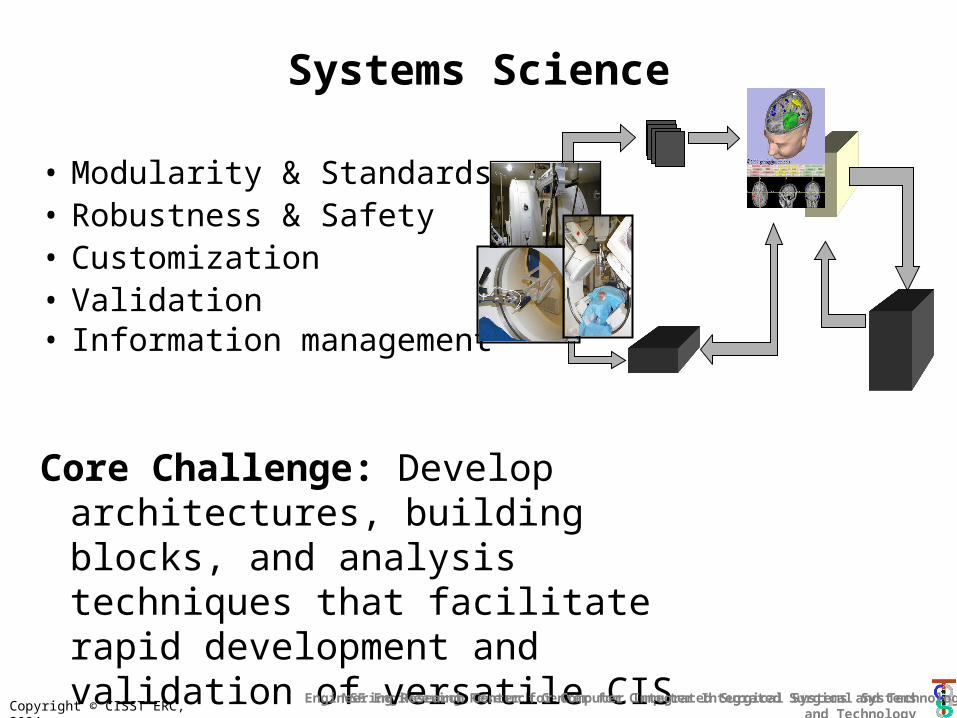
Systems Science
• Modularity & Standards• Robustness & Safety• Customization• Validation • Information management
Core Challenge: Develop architectures, building blocks, and analysis techniques that facilitate rapid development and validation of versatile CIS systems & processes with predictable performance
Engineering Research Center for Computer Integrated Surgical Systems and Technology
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
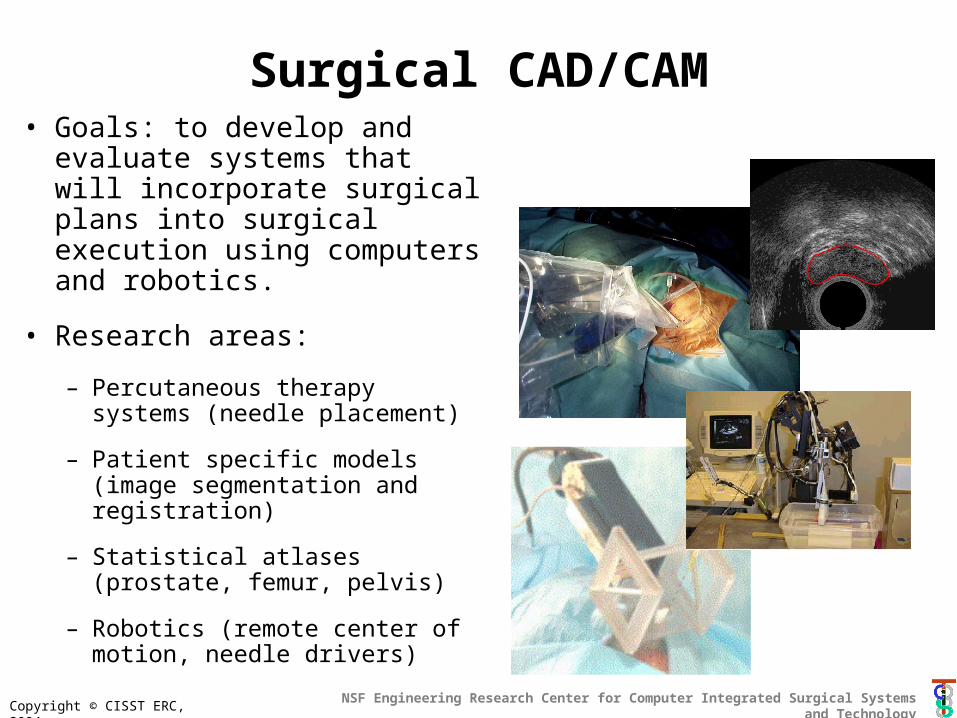
Surgical CAD/CAM• Goals: to develop and
evaluate systems that will incorporate surgical plans into surgical execution using computers and robotics.
• Research areas:
– Percutaneous therapy systems (needle placement)
– Patient specific models (image segmentation and registration)
– Statistical atlases (prostate, femur, pelvis)
– Robotics (remote center of motion, needle drivers)
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
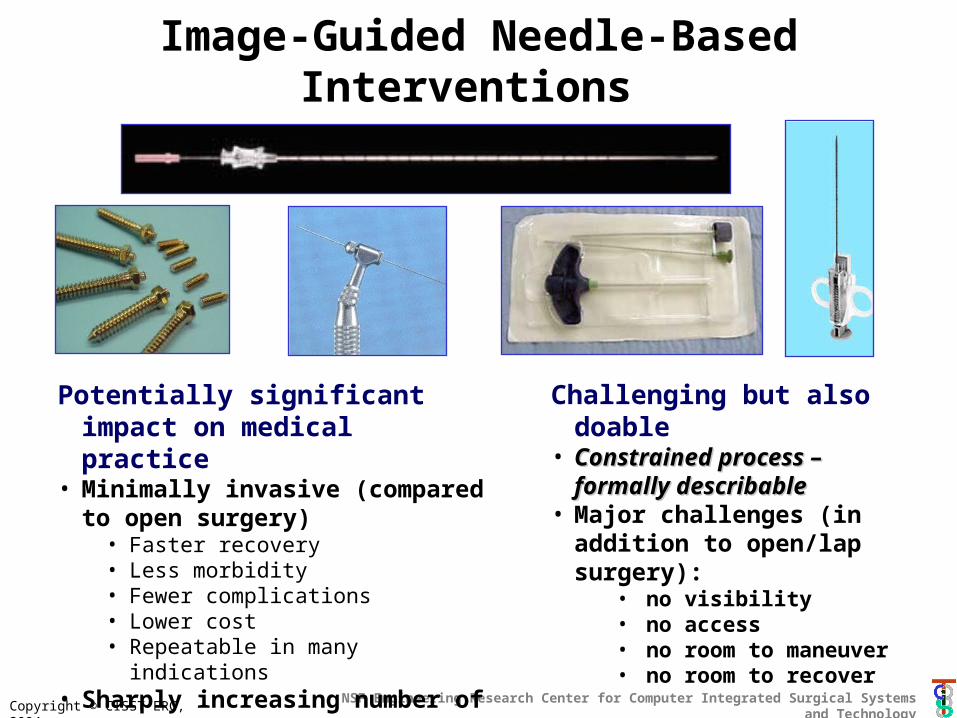
Image-Guided Needle-Based Interventions
Potentially significant impact on medical practice
• Minimally invasive (compared to open surgery)
• Faster recovery• Less morbidity• Fewer complications• Lower cost• Repeatable in many indications
• Sharply increasing number of procedures
Challenging but also doable• Constrained process – Constrained process –
formally describableformally describable• Major challenges (in addition
to open/lap surgery):• no visibility• no access• no room to maneuver• no room to recover
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
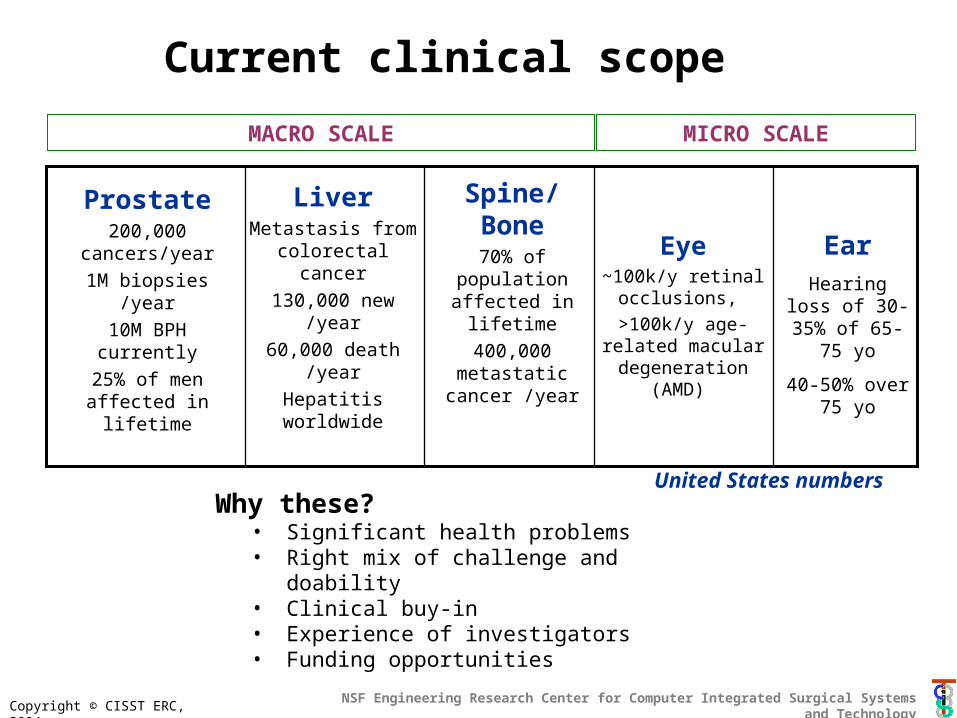
Current clinical scope
Spine/Bone70% of population affected in lifetime
400,000 metastatic
cancer /year
LiverMetastasis from colorectal cancer
130,000 new /year
60,000 death /year
Hepatitis worldwide
Prostate200,000 cancers/year
1M biopsies /year
10M BPH currently
25% of men affected in lifetime
Why these?• Significant health problems• Right mix of challenge and doability• Clinical buy-in• Experience of investigators• Funding opportunities
United States numbers
Eye~100k/y retinal
occlusions,
>100k/y age-related macular degeneration
(AMD)
EarHearing loss of 30-35% of 65-
75 yo
40-50% over 75 yo
MACRO SCALE MICRO SCALE
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
Why these organ systems?
Humanitarian reasons• Significant health problems in US
and worldwide
Opportunistic reasons• Right mix of challenge and doability• Clinical buy-in• Funding opportunities• Experience of investigators• Publishing opportunities
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
Engineering Goals
1. “One-Stop Shopping”•Plan, Do, and Verify – in one sitting
2. “Plug & Play Surgery”•Rapidly configure for target organ,
imaging modality, and therapy•Predictable performance
3. Critical Mass of Components
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
-0.3
-0.2
-0.1
0
0.1
0.2
0.3
0 2 4 6 8 10
Dis
tanc
e (m
m)
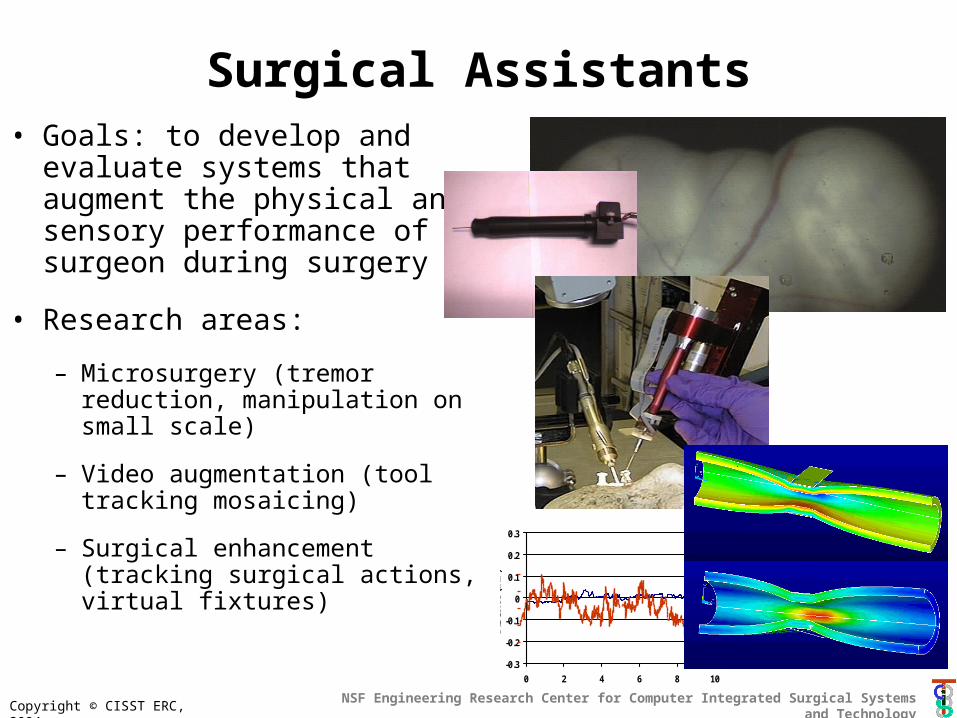
Surgical Assistants• Goals: to develop and evaluate
systems that augment the physical and sensory performance of a surgeon during surgery
• Research areas:
– Microsurgery (tremor reduction, manipulation on small scale)
– Video augmentation (tool tracking mosaicing)
– Surgical enhancement (tracking surgical actions, virtual fixtures)
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
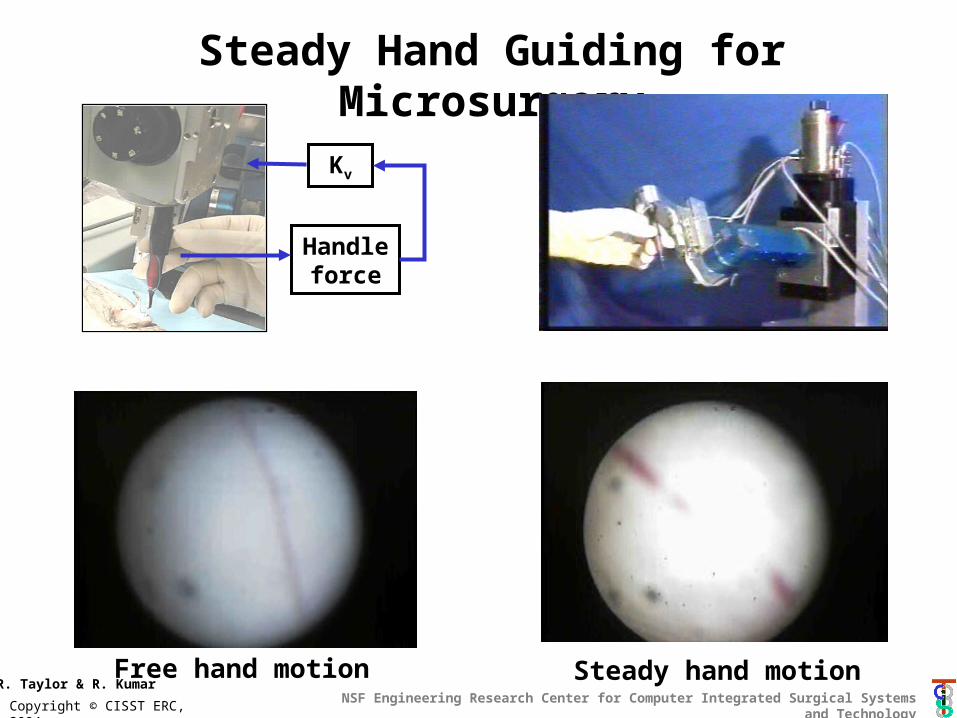
Handle force
Kv
Steady Hand Guiding for Microsurgery
R. Taylor & R. KumarFree hand motion Steady hand motion
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
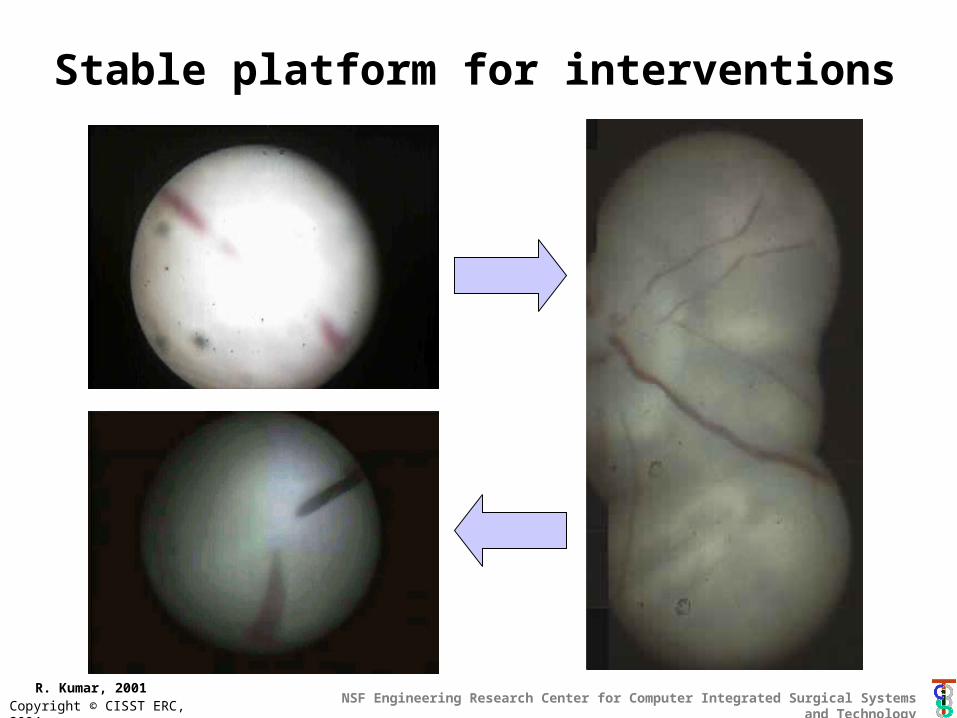
Stable platform for interventions
R. Kumar, 2001
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
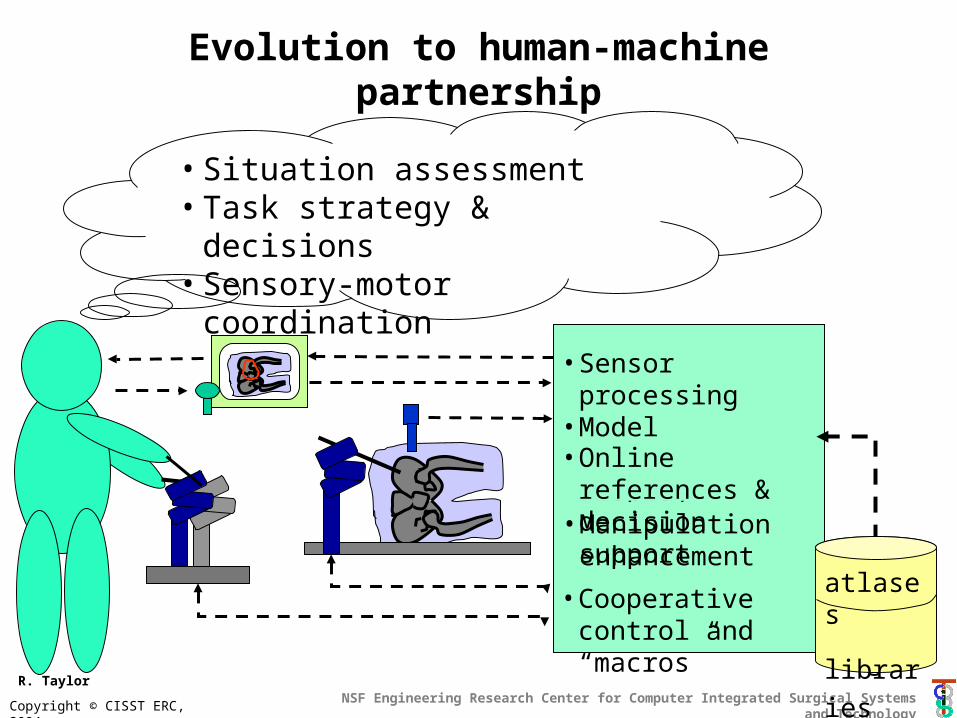
Evolution to human-machine partnership
• Situation assessment• Task strategy & decisions• Sensory-motor coordination
Augmentation System
• Sensor processing• Model interpretation• Display
atlases
• Manipulation enhancement
• Online references & decision support
• Cooperative control and “macros”
atlases
libraries
R. Taylor
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
Computer-assisted
simulation & planning
Patient-specific Model
Update Model
Simulate and replan in real
time
Computer- Assisted
Assessment
Preoperative Intraoperative
Atlas
Postoperative
Patient
The grand unified system*
* From Turf Valley Workshop (March 2003)

Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
System barriers• Safety & verifiability
• “The usual”• No fly zones• Information-based supports
• Usability & maintainability• “The usual”• Surgical performance
analysis• Recording information
• Performance and validation• “The usual”• Accuracy propogation• Analysis-based generation
of test plans • Standards
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
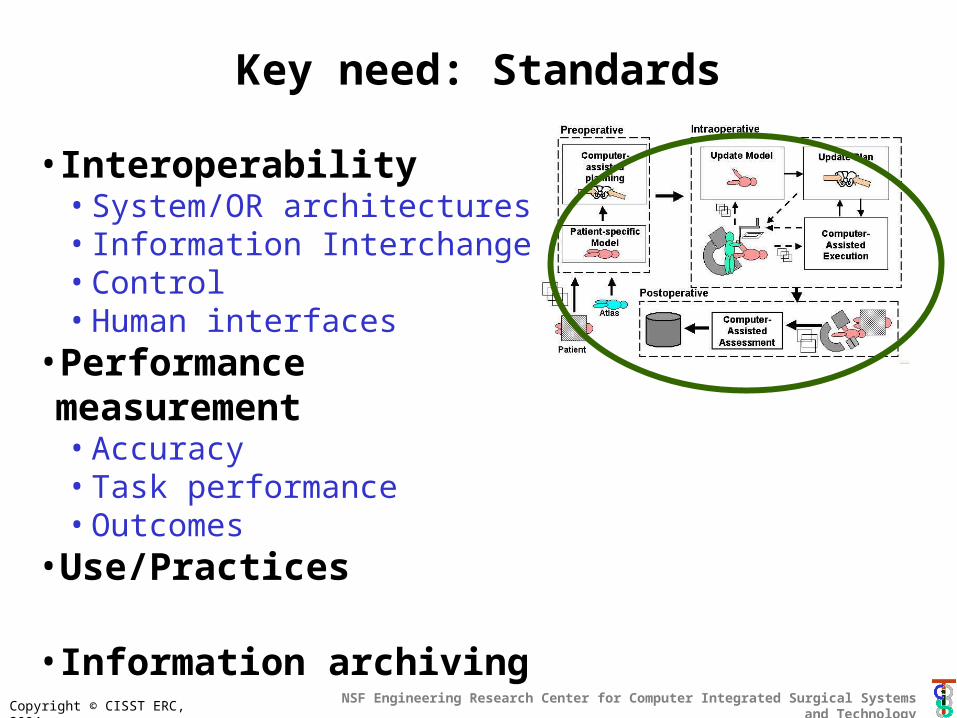
Key need: Standards
• Interoperability• System/OR architectures• Information Interchange• Control• Human interfaces
•Performance measurement• Accuracy• Task performance• Outcomes
•Use/Practices
• Information archiving
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
A few “grand challenge” areas
• Grand Unified System – Real-time patient-specific models– Surgical total information management– Active human-machine partnerships– Correlate performance to outcome
• “Fanstastic Voyage”*– Micro-invasive interventions on tiny structures
• Surgery on cells & microstructures
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
Surgical Total Information Management
• Real time sensing & modeling of surgical situation– Patient-specific models– Surgical tools & tool-tissue interations– Surgeon movements– Etc.
• Application drivers– Assistance (robots & information support)– Outcomes assessment
• Technology drivers– Imaging, computer vision, image analysis– Sensors, sensor networks– Biomechanics, statistical modeling– Human-machine interfaces, haptics– Performance/task modeling
Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
How can we get there?
Strong and committed teams
– Surgeons– Engineers– Industry
Focus on systems that address important needs
Rapid iteration with measurable goals
Have fun!

Copyright © CISST ERC, 2004NSF Engineering Research Center for Computer Integrated Surgical Systems and Technology
Bio
Russell H. Taylor has a B.E.S. from Johns Hopkins, and a Ph.D. in Computer Science from Stanford. He joined IBM Research, where he developed the Agent Markup Language (AML) robot language. Following an assignment in Boca Raton, he managed robotics and automation technology research activities at IBM Research until returning to full-time technical work, when he became a manager of Computer Assisted Surgery. Taylor then moved to Johns Hopkins University as a Professor of Computer Science. He is currently a Professor of Computer Science, with joint appointments in Radiology and Mechanical Engineering, and is the Director of the NSF Engineering Research Center for Computer-Integrated Surgical Systems and Technology at Johns Hopkins. Research interests include robot systems, programming languages, model-based planning, and the use of imaging, model-based planning, and robotic systems to augment human performance in surgical procedures. He is Editor Emeritus of the IEEE Transactions on Robotics and Automation, Fellow of the IEEE, and a member of various honorary societies, panels, editorial boards, and program committees.