comorbidity, distress, coping and social support in asthma...
TRANSCRIPT

Comorbidity, Distress, Coping
and Social Support in Asthma
and Allergy
Nina Lind
Department of psychology Umeå 2015

This work is protected by the Swedish Copyright Legislation (Act 1960:729) ISBN: 978-91-7601-183-6 Electronic version available at http://umu.diva-portal.org/ Printed by: Print & Media Umeå, Sweden 2014 Cover: Niklas Schmidt

To mom, I love you

Acknowledgement
So how do you thank for an experience like this? First of all, I want to send the greatest of thanks to my wonderful supervisors, without you, this thesis wouldn’t exist. Steven Nordin, words cannot describe how grateful I am. You have taught me that no question is too simple or too small, and that one can never be too curious. Thank you for always keeping your door open and letting me learn more and more each day. Anna-Sara Claeson, thanks for your support and guidance in helping me in find my own way into what was previously unknown. Eva Millqvist, without your knowledge in the field of asthma and allergy, I would have been in deep water, thank you for letting me lean on your expertise. I also want to send a special thanks to the Swedish Asthma and Allergy Association Research Fund (2010019-K and 2012030-K), for funding this thesis.
I would like to send the warmest thanks to you, Maria Nordin, what would I have done without you? Thanks for all the moments we shared, both at work and during travels. Linus Andersson, for always thinking outside the box, thanks for all your valuable comments and ideas. I would also like to thank my co-author, Eva Palmquist and Anna Söderholm, and a special thanks to Eva for all the help with the database.
My most humble gratitude goes to those who spent time reading this thesis at an early stage, Bernt Lindahl, Bo Molander, Kristina Westerberg, Petra Sandberg and Olle Löwhagen. With a combination of your knowledge, comments and ideas, you helped me making this thesis better.
Thanks to everyone who believed in me, Mikael Henningsson, Kristina Westerberg, Anna Stigsdotter-Neely, and the rest of you who have been involved, thanks for giving me this opportunity.
A special thanks goes to my colleagues in Betula Air, thank you for giving me the chance to be part of your group, I have enjoyed these years and learned a lot. I would also like to thank my colleagues at the Department of Psychology at Umeå University, the PhD-students and the AD-group. Markus Nyström, thank you for being there for much needed lunch breaks, discussions and support from time to time. Hanna Malmberg Gavelin, Robert Lundmark and Johan Paulin, my distant roomies, thanks for letting me be part of your group. Elisabeth Åström, if there will be a competition, you are my forever first choice of team-mate. Fredrik Sjödin, thanks for all the tips and tricks, I can assure you that this thesis have never looked so great.
Last but not least, I would like to thank my friends and family for being there, both in good times and in bad. Far away or not, Ida Åberg, Angeliki Kourtopoulos and Isabel

Agerbjörk, thank you for being only a call away, even during times when I've been distant. Christopher Schmidt, you are the best friend a girl can ever have. Niklas Schmidt, thank you for helping me with the cover of this thesis, and for all the stories that made me smile for days, if not weeks. Linus, thank you for being my brother and helping me to see the happy things in life and what is important, you are amazing. Thanks to my parents, Mom and Per, for your endless support.
My biggest supporter in life, mom, you have always been there by my side, always strong and always supportive. I would like to dedicate this thesis to you, I love you.
Dad, if you were here with us today, I know you would have been proud.
Nina Lind Umeå, 2014-12-18

i
Table of Contents
Table of Contents i Abstract iii List of abbrevations iv List of studies v Sammanfattning (Summary in Swedish) vi Definitions viii Introduction 1
Prevalence and characteristics of asthma and allergy 2 Asthma 3 Allergic rhinitis 3 Atopic dermatitis 4 Comorbidity within asthma and allergy 4 Risk factors and trigger factors 6
Comorbidity 7 Distress 10 Coping and social support 12 General aims of the thesis 14 General methods 15
The Västerbotten Environmental Health Study 15 Participants 19 Ethical approval 23 Data management 23 Statistical analysis 23 Study-specific group categorization and statistical analysis 24
Study I 24 Study II 24 Study III 25
Overview of the empirical studies 25 Study I – Co- and multimorbidity between asthma and allergy and intolerance to
chemicals and certain buildings 25 Aims and specific methods 25 Results and discussion 26
Study II – Psychological distress in asthma and allergy 28 Aims and specific methods 28 Results and discussion 29
Study III – Coping and social support in asthma and allergy 31 Aims and specific methods 31 Results and discussion 32

ii
General discussion 35 Co- and multimorbidity between asthma and allergy and intolerances to
chemicals and certain buildings 35 Psychological distress in asthma and allergy 36 Coping and social support in asthma and allergy 38 A metaperspective on the studies 40 Strengths and limitations of the thesis 43 Implications 45 Future perspectives 47 Concluding remarks 47
References 49 Appendix 62
Study I
Study II
Study III

iii
Abstract
Asthma and allergies are some of the most common illnesses worldwide that almost everybody will come in contact with. This thesis studied persons with allergic asthma, non-allergic asthma, allergic rhinitis and atopic dermatitis in a population-based sample. At an early stage, these illnesses were regarded as psychosomatic. Over time, as knowledge about asthma/allergy has increased more of a biomedical perspective was taken by the research field. In considering early documentations well as contemporary research, a psychobiosocial perspective was taken in this thesis when conducting the three studies. Thus, as psychological factors may affect the illness and be a result of the illness, it is important to incorporate these factors to better understand asthma and allergy.
Study I examined the co- and multimorbidity in asthma/allergy with the environmental intolerances in the form of chemical and building-related intolerance. Study II investigated psychological distress in the four forms of asthma and allergy. Psychological distress was in this study defined as stress, burnout, anxiety, depression and environmental health worries. Study III examined usage of problem and emotion focused coping strategies and perceived social support from the surrounding in high and low asthma/allergy severity. All studies were performed using data from the Västerbotten Environmental Health Study, a questionnaire-based survey with focus on various environmental hypersensitivities and asthma and allergy.
The result showed that the co-and multimorbidity with the environmental intolerances in asthma/allergy was larger than what was statistically excepted. Those with allergic asthma and atopic dermatitis experienced more stress, burnout and anxiety than those with non-allergic asthma, allergic rhinitis and non-asthma/allergy. Moreover, the most common way of coping with asthma and allergy was found to be strategies such as avoiding environments that are believed to affect health, and trying to accept the situation, independent of asthma/allergy severity. Finally, in general, those with asthma and allergy reported receiving most support from their partner, other family members and health care, and least support was perceived by those with low asthma/allergy severity.
The findings suggest that co- and multimorbidity with environmental intolerances is relatively common in asthma and allergy, and should therefore be included in the clinical anamnesis for this patient group. The elevated level of distress in allergic asthma and atopic dermatitis evokes the question of use of therapies such as mindfulness may be beneficial in certain afflicted persons. The results on coping and social support provide a foundation for further research regarding informing the asthma/allergy patient and family members about effective coping strategies and the importance of adequate social support. A metaperspective is taken in which interrelations between important variables in the thesis are discussed.
Keywords: atopy, asthma, allergy, allergic rhinitis, atopic dermatitis, environmental intolerance, chemical intolerance, building intolerance, psychological distress, stress, anxiety, depression, burnout, coping, social support

iv
List of abbrevations
ANOVA Analysis of variance BI Building intolerance CBT Cognitive behavioral therapy CI Chemical intolerance EI Environmental intolerance HADS Hospital and Anxiety Scale HRQoL Health-related quality of life IgE Immunoglubulin E MCS Multiple chemical sensitivity NBRS Non-specific building-related symptoms PNI Psychoneuroimmunology QoL Quality of life SD Standard deviation SE Standard error SHR Sensory hyperreactivity VEHS Västerbotten Environmental Health Study WHO World Health Organization

v
List of studies
I. Lind, N., Söderholm, A., Palmquist, E., Andersson, L., Millqvist, E., &
Nordin, S. (2014) Co- and Multimorbidity of Asthma and Allergy and Intolerance to Chemicals and Certain Buildings. Manuscript.
II. Lind, N., Nordin, M., Palmquist, E., & Nordin, S. (2014). Psychological Distress in Asthma and Allergy: The Västerbotten Environmental Health Study. Psychology, Health & Medicine, 19(3), 316-323.
III. Lind, N., Nordin, M., Palmquist, E., Claeson, A-S., Millqvist, E., & Nordin, S. (2014) Coping and Social Support in Asthma and Allergy: The Västerbotten Environmental Health Study. Journal of Asthma, Advance online publication.
Paper II and III have been reproduced with permission from the copyright holders.

vi
Sammanfattning (Summary in Swedish)
Astma och allergi hör till de vanligaste sjukdomarna i världen som nästan alla kommer att komma i kontakt med på något sätt. Denna avhandling studerar personer med allergisk astma, icke-allergisk astma, allergisk rinit och atopiskt eksem. Dessa former av astma och allergi har alla en tidig historia inom psykosomantiken, där man ansåg att sjukdomen i sig var ett resultat av den psykiska hälsan. Med tiden, samtidigt som kunskapen om astma/allergi har ökat, har forskningsfältet tagit ett mer biomedicinskt perspektiv som förklaringsmodell för sjukdomen. Med tanke på den tidiga dokumenteringen samt den aktuella forskningen, har ett psykobiosocialt perspektiv tagits i denna avhandling med tre studier. Eftersom psykologiska faktorer kan påverka sjukdomen och samtidigt vara ett resultat av sjukdomen i sig, är det viktigt att inkorporera dessa faktorer för att bättre förstå astma och allergi.
I avhandlingen genomfördes tre delstudier, där Studie I undersökte sam- och multisjuklighet i astma/allergi med två typer av miljöintoleranser, kemisk och byggnadsrelaterad intolerans, både som läkardiagnostiserad och självrapporterad. Studie II undersökte psykiskt lidande bland de fyra formerna av astma och allergi. Psykologisk lidande var i denna studie definierad som stress, utbrändhet, ångest, depression och miljöhälsooro. Studie III undersökte användningen av problem- och känslofokuserade hanteringsstrategier och upplevd socialt stöd från den närmsta omgivningen bland astmatiker och allergiker med hög och låg svårighetsgrad av sjukdomen. Alla tre studier utfördes med data från Miljöhälsostudien i Västerbotten, vilket är en populationsbaserad enkätundersökning med fokus på olika miljööverkänsligheter och astma och allergi bland invånarna i Västerbotten, Sverige.
Resultaten visade att sam- och multisjuklighet med de olika typerna av miljöintoleranser vid astma/allergi var större än vad som statistiskt var förväntat, oberoende om intoleranserna var läkardiagnostiserade eller självrapporterade. De med allergisk astma och atopiskt eksem rapporterade mer stress, utbrändhet och ångest än de med icke-allergisk astma, allergisk rinit och utan någon av dessa diagnoser. De vanligaste strategierna för att hantera sin astma och allergi var att undvika miljöer som ansågs påverka hälsan, och att försöka acceptera sin situation, vilket var oberoende av svårighetsgrad av sjukdomen. Slutligen, i allmänhet upplevde de med astma och allergi att de får mest stöd från sin partner, andra familjemedlemmar och hälsovården, och minst stöd från myndigheter och förenings-/stödgrupper. Generellt upplevde de med låg svårighetsgrad av astma/allergi mer stöd i jämförelse med de som hade högre svårighetsgrad.
Sammanfattningsvis ger resultaten stöd för att sam- och multisjuklighet med miljöintolerans är relativt vanligt bland astmatiker och allergiker, och bör därför inkluderas i den kliniska anamnesen för denna patientgrupp. Den förhöjda nivån av

vii
psykologiskt lidande vid allergisk astma och atopisk eksem väcker frågan om möjliga hälsoeffekter av terapier så som mindfullness hos speciellt utsatta individer. Resultaten beträffande hantering och socialt stöd ger en grund för framtida forskning samt behov av information till patienter med astma och allergi och dess familjemedlemmar om effektiva hanteringsstrategier och vikten av socialt stöd. Ett metaperspektiv diskuteras om samspelet mellan viktiga variabler i avhandlingen.

viii
Definitions
Atopy
Atopy was first introduced in the 1920’s by Coca and Cooke (1923) as a term for the sensitivity phenomenon which is hereditary and limited to a small group. Originally the term was referring to asthma and allergy caused by an allergic reaction, Immunoglobulin E (IgE) mediated allergy, which appears due to predisposition toward developing a certain allergy or an individual and/or hereditary tendency. The term atopy is not to be confused with allergy as atopic individuals may or may not have symptoms of allergy. Allergy is a sensitivity reaction caused by immunologic mechanism.
Asthma
Asthma is defined as a chronic inflammatory illness of the airways, caused by an inflammation of the airways or airway hyperresponsiveness (an exaggerated airway narrowing in response to triggers, such as allergens and exercise). Common symptoms are sporadic breathing problems, such as wheezing and coughing when being exposed to typical allergens. Clinically, both allergic and non-allergic asthma are used as forms of diagnosis.
Allergic rhinitis
Allergic rhinitis is caused by an inflammation of the nasal airway due to an IgE-mediated response to an allergen which leads to swelling of the nasal mucosa. Common symptoms are nasal congestion, nasal itch, rhinorrhea and sneezing. Nasal symptoms of rhinitis, such as a runny nose can also be accompanied by symptoms in the ears, eyes and throat such as runny and itchy eyes and itching of the palate and pharynx.
Atopic dermatitis
Atopic dermatitis is a chronic, inflammatory skin illness, characterized by symptoms such as burning skin sensation, intense itching and skin lesion. It is common for atopic dermatitis to first occur in childhood and later reoccur in adulthood or adult life. In adolescence and adulthood, symptoms of dermatitis can be found on the flexural surfaces of the extremities, hands and feet, which are commonly affected areas of the body. Atopic dermatitis may, just like asthma, be of allergic or non-allergic nature.

1
Introduction
Asthma and allergy are common conditions that almost everybody in society will come in contact with. Historically, both asthma and allergy have been viewed as purely psychosomatic illnesses thought to be due to being emotionally upset or mentally agitated (Rosner, 1997). Others have suggested that asthma and eczema are primarily nervous disorders, which are attributed to emotional disturbances rooted in the mother and child relationship (Daruna, 2012). In the 1900’s the view on asthma changed towards being understood as an organic illness in which treatment with corticosteroids radically improved life of the afflicted individual, which together changed the understanding for both asthma and allergy in general. Although acknowledged as life threatening, before the 1960’s asthma was partly viewed as an illness limited to the socially and educated elite, whereas it was later recognized to be affecting all groups of society and a serious threat to both overall health and life, especially in the deprived sections of society (Jackson, 2009). Later, in 1968 the annunciation of the fifth immunoglobulin, IgE, confirmed what previously had been expected, thus, that atopic illness is caused by an allergic reaction. This annunciation leads to increased understanding and to the development of more beneficial treatments and changed the view of allergic illness towards what we know today (Ishizaka, Ishizaka, & Menzel, 1967; Stanworth, Humphrey, Bennich, & Johansson, 1967).
This thesis concerns psychological aspects ranging from co- and multimorbidity in asthma/allergy with intolerances to chemicals and certain buildings, to the experience of various types of distress in different asthma and allergy diagnoses, and to degrees of usage of coping strategies and experience of social support. A broad view was taken by studying four of the most common forms of asthma and allergy diagnoses.
Asthma and allergy has for centuries interested scientists regarding aspects ranging from underlying causes to prevention. Early documentations ranging back to 2500 BC have been found for different forms of allergic illness. The clinical description of asthma dates back to ancient times (Walter & Holtzman, 2005) in which early theories suggested that asthma attacks could be prevented by self-regulation of anger (Douwes, Brooks, van Dalen, & Pearce, 2011). Maimonides (1135-1204), a Jewish rabbi, physician, and philosopher living in Egypt suggested asthma to be a psychosomatic illness. On the one hand, he argued, a deranged psyche may affect the somatic or physical wellbeing of an individual. On the other hand, joy could have positive effects as it was believed to gladden the heart, and stimulate the blood and mental activity. Over time, allergic illness has developed into being understood as syndromes with multiple pathophysiology. One of the essential aspects includes inflammation that can be more or less localized and occur in response to relatively innocuous external irritants such as allergens.

2
It has been suggested that the shift in the perception of asthma and allergy over the last few decades can be mirrored in the way it has been treated (Bjermer, 2007). During the second half of the 19th century, asthma was predominantly viewed as a psychosomatic illness in which emotional stress and imbalances in the nervous system were seen as its key factors in its etiology. As a result of this, relief of anxiety was considered the main therapeutic intervention for asthma (Jackson, 2009). This can be compared to the view of asthma/allergy today, which are predominantly viewed as inflammatory illnesses in which both the inflammation and allergic reaction is treated with medications such as corticosteroids and histamine (Daruna, 2012).
Once the IgE was recognized as a mediator in inflammatory illness (Berg & Johansson, 1969) the development of beneficial treatments, such as corticosteroids and inhaled formulations, helped people control their illness caused by allergies, and thereby improve their everyday life (Holgate, 2011). During the early 1970’s inhaled corticosteroids improved the treatment of asthma, and especially in the non-allergic form. By administering inhaled corticosteroids one could now avoid adverse effects of orally administered cortisone. Later in the 1990’s asthma was confirmed as an inflammatory illness which can explain the positive effects of the anti-inflammatory substances. The link between immunology and psychology can be referred to as psychoneuroimmunology (PNI), which focuses on the links between psychologically and biologically plausible explanations for how psychological factors might influence immunity and immune system-mediated illness. These issues have been the motivation for this thesis as there are more to an illness than what a biomedical perspective will include.
Prevalence and characteristics of asthma and allergy
Although contradicting results exist (Lötvall et al., 2009), an increasing number of persons appears to suffer from asthma and allergy worldwide, especially in the industrialized countries (Subbarao, Mandhane, & Sears, 2009; von Mutius, 2000). Ekerljung and colleagues (2010) concluded that this increased prevalence might indicate a change in diagnostic practices rather than an actual increase in prevalence, as the prevalence of asthmatic symptoms has not changed over recent time. In Europe it is estimated that 5-10% have asthma, with the lowest prevalence in the Mediterranean and highest in Great Britain and Scandinavia (Janson et al., 2001). It is further estimated that approximately 300 million of the world’s population are affected by asthma, and that the number will have increased to 400 million at year 2025 (Bateman et al., 2008). Both asthma and allergy have been reported to affect aspects ranging from quality of life (QoL) (Leynaert, Neukirch, Liard, Bousquet, & Neukirch, 2000) to psychological distress (Chida, Hamer, & Steptoe, 2008), which, in turn, can create a negative loop where stress can lead to atopy outcome (Rand et al., 2012), but also to higher risk for morbidity (Weiss, 2012). Taken together, the negative aspects of the illness can result in decreased financial safety for the individual due to missed work/school days as well as

3
limitations in everyday social life (Barnes et al., 1996). Asthma and allergy is also costly for society (Bahadori et al., 2009) due to need of medical help and hospitalization. It has been suggested that lost productivity due to sick days of allergic rhinitis and the common cold to be estimated to a yearly cost of €2.7 billion in Sweden alone (Hellgren, Cervin, Nordling, Bergman, & Cardell, 2010). This suggest that the illnesses, both asthma and allergy, benefit from being illuminated from various points of view to find variations to reduce sick days as well as improve QoL in these individuals.
Asthma
Asthma is defined as a chronic inflammatory illness. The typical clinical signs of asthma are sporadic breathing problems, such as wheezing and coughing when being exposed to triggers, i.e. allergens, cold air and exercise. It has a varying complexity between individuals as well as within the individual. When asthma is caused by an immunologic reaction towards an allergen, it is referred to as allergic asthma, whereas when it is caused, for example, by physical exercise it is referred to as non-allergic asthma (see Table 1 for diagnostic criteria). In many cases the asthma attack is initiated by IgE-antibodies and the release of histamines, but it can also be the case that the attack is initiated by a non-allergic reaction as a result of cold temperature, although both types have a presence of an inflammation of the airways. Clinically, both allergic and non-allergic asthma are used as diagnostic forms of asthma, and among those with allergic asthma it is also common that they experience a non-asthmatic reactions triggered, for example, by stress (Johansson, Millqvist, Nordin, & Bende, 2006). Some studies have suggested that non-allergic asthma is more severe than the allergic form (Romanet-Manent et al., 2002) due to the lowered controllability. The definition of asthma comprises four domains, of which none constitute a necessary criterion for the diagnosis: symptoms, airway obstruction, airway hyperresponsiveness and airway inflammation (Reddel et al., 2009). In Sweden it is estimated that around 8.3-12% of the population is affected (Lötvall et al., 2009).
Allergic rhinitis
Allergic rhinitis is an chronic inflammation of the nasal airways in response to an allergen (Skoner, 2001) in which the reaction is caused by an IgE-mediated response (see Table 1 for diagnostic criteria). Common symptoms of rhinitis include nasal congestion, nasal itch, rhinorrhea and sneezing (see Table 1 for diagnostic criteria). Nasal symptoms of rhinitis can also be accompanied by symptoms in the ears, eyes and throat such as runny and itchy eyes and itching of the palate and pharynx. Rhinitis is one of the most common illnesses all over the world, with as many as 40% of certain populations being affected (Small & Kim, 2011). The most common form of rhinitis, allergic rhinitis (caused by an IgE-mediated reaction), affects about 10-20% of the population, and there are studies suggesting an increase in prevalence over time (Lee &

4
Mace, 2009). It has been found that severe rhinitis not only causes symptoms in the nasal area, but also limited QoL, sleep and work performance (Dykewicz & Hamilos, 2010). Around 14-15% of the Swedish population is believed to be afflicted (Nihlén et al., 2006).
Atopic dermatitis
Atopic dermatitis (also known as atopic eczema), is a chronic, inflammatory skin illness, characterized by intense itching and skin lesion. It is common for atopic dermatitis to first occur in childhood and later reoccur in adulthood or adult life (Beasley, 1998; Williams, 2005). During early childhood, infants are mostly affected in areas such as the scalp, face, neck and trunk, whereas in older children it is more common in the flexural surfaces of extremities such as fold/back of elbow and back of knee together with neck, wrist and ankles. In adolescence and adulthood, the flexural surfaces of the extremities, hands and feet, are usually the affected areas of the body (see Table 1 for diagnostic criteria). Common for all ages is that the itching is present throughout the day and worsens at night, which in turn leads to sleep impairment and reduced QoL (McKenna & Doward, 2008). Atopic dermatitis may, just like asthma, be of allergic or non-allergic nature. In some countries, as many as 10-20% of children (Beasley, 1998; Bjorksten et al., 1998) but only 1-3% of adults are believed to be affected (Larsen & Hanifin, 2002). In a recent study it has been suggested that the prevalence of atopic dermatitis is as high as 15% in Sweden (Rönmark et al., 2012).
Comorbidity within asthma and allergy
It has previously been suggested that atopic dermatitis is a risk factor for developing other atopic illnesses such as allergic asthma and allergic rhinitis. In a study by Akdis and colleagues (Akdis et al., 2006) it was reported that among children that developed atopic dermatitis during their first two years, 50% developed asthma within the coming years. It was also suggested that those who later developed asthma or allergic rhinitis would develop a more severe illness. Others have suggested that there is a link between the different atopic diagnoses such as between asthma and allergic rhinitis, which is referred to the similarities between asthma and rhinitis, and illustrated by the strong epidemiologic, pathogenic and immunologic association (Bjermer, 2007). It has in previous studies been discussed whether or not to divide these two atopies into different illnesses, or whether one should see them as one and the same, although having different localizations. This relationship has been described as the integrated airways illness hypothesis (Meltzer, Szwarcberg, & Pill, 2004) and allergic airway illness (Braunstahl, 2005). Accordingly, asthma and rhinitis are considered to be manifestations of an inflammatory process within a continuous airway rather than separate pathologies.

5
Table 1. Diagnostic criteria for the asthma/allergy diagnoses used in the thesis. Diagnosis Diagnostic criteria Source Asthma (adults)
Symptom: Wheeze of the bronchi, spontaneously or triggered by allergens or physical exertion and β2-reversibility ≥12 percent after e.g. salbutamol 0.8 mg or terbutaline 1.0 mg or PEF variability ≥20 percent over 1-2 weeks (difference between lowest and highest value) The diagnosis of asthma is supported by a. Positive methacholine or histamine test b. Positive steroid test. FEV-percent increase ≥15 after prednisolone
30 mg × 1 for 2 weeks c. Positive subjective effect of deposited asthma medications
Global Initiative for Asthma, 2014; Löwhagen, 2005
Allergic rhinitis
Intermittent: symptoms are present <4 days a week or for <4 consecutive weeks Persistent: symptoms are present >4 days a week and for >4 consecutive weeks Mild: none of the following conditions
• Sleep disturbance • Impairment of daily activities, leisure, and/or sport • Impairment of school or work • Troublesome symptoms
Moderate/severe: one or more of the following conditions
• Sleep disturbance • Impairment of daily activities, leisure, and/or sport • Impairment of school or work • Troublesome symptoms
Brożek et al., 2010
Atopic dermatitis (children)
Must have: An itchy skin condition in the last 12 months Plus three or more of:
• Onset below age 2* • History of flexural involvement • History of generally dry skin • Personal history of other atopic disease** • Visible flexural dermatitis as per photographic protocol
Williams et al., 1994
* Not used in children under 4 years ** In children under 4 years, history of atopic disease in a first degree relative may be included

6
Studies have shown that rhinitis is an independent risk factor for asthma in both atopic and non-atopic individuals. The airways, both the upper and lower (pharynx, nasal cavity and the trachea, bronchi and bronchioles), differ between the two conditions but do also have many similarities (Leynaert, Bousquet, Neukirch, Liard, & Neukirch, 1999). It has therefore been suggested that asthma should be regarded as a systemic illness as it is sharing features with other parts of the body such as the nose, skin and bone marrow. This is illustrated by the difficulties to achieve optimal asthma control in a patient with asthma and rhinitis without also treating the upper airways. This probably applies to concomitant manifestations in other parts of the body. This view of asthma as a potential systemic disorder supports the use of systemic therapeutic modalities (Durham, Till, & Corrigan, 2000).
Risk factors and trigger factors
A risk factor is regarded as something that may increase the risk of developing, for example, asthma and allergy, whereas a trigger factor is regarded as something that will cause symptom exacerbation in already sensitized/affected individuals. However, there is some overlap between risk and trigger factors. For example, smoking increases the risk for developing asthma (Ghosh, Pahwa, Rennie, & Janzen, 2009; Thomsen, Duffy, Kyvik, & Backer, 2010), and both first- or second-hand smoking may trigger acute worsening of exacerbation (Avila, Soto-Martínez, Soto-Quirós, & Celedón, 2005; Gupta et al., 2005; Hastert, Babey, Brown, & Meng, 2007). In this context, trigger factors can be defined as environmental factors, substances or events that increase the risk for an individual to experience severe worsening of asthma symptoms or that leads to an acute onset or worsening of asthma symptoms lasting several hours or days (Araujo, Ferraz, Borges Mde, Filho, & Vianna, 2007; Bateman et al., 2008; De Vries et al., 2005). Risk factors for developing asthma has in previous studies been identified as types of allergies (e.g. atopic dermatitis and allergic rhinitis), obesity, low socioeconomic status, urbanization, hereditary, and sex which is believed to be depending on age (Thomsen et al., 2010).
Several explanations have been given for the development of different forms of asthma and allergy. One of the most common theories of why asthma and allergy occur is the hygiene hypothesis. It states that a lack of early childhood exposure to infectious agents, symbiotic microorganisms (e.g., gut flora or probiotics), and parasites increases susceptibility to allergic illness by suppressing the natural development of the immune system. In particular, the lack of exposure is thought to lead to defects in the establishment of immune tolerance (Brooks, Pearce, & Douwes, 2013).
As risk and trigger factors in some cases may work as one and the same, there are some triggers that are more commonly reported than others. In a recent study, it was found that patients with asthma were able to recognize a wide selection of frequent trigger

7
factors found in their closest environment. This includes indoor/outdoor allergens, environmental pollutants/irritants, strong odors, different kinds of foods, weather, exercise, sinusitis/respiratory infections, stress, medications, and strong emotions that are perceived to contribute to the frequency and severity of asthma symptoms (Vernon, Bell, Wiklund, Dale, & Chapman, 2013). Other factors that are likely to trigger non-allergic reactions include exposure to cold air, anxiety and stress (Global Initiative for Asthma, 2014).
Comorbidity
Parallel to the high prevalence of asthma and allergy, a substantial proportion of the population report that they become ill by low levels of environmental exposures which are assumed to be harmless. These persons commonly experience symptoms that are similar to those due to asthma/allergy, but they do not respond to the traditional medical treatment for allergies (Heaney & Horne, 2012). One explanation may be the fact that these symptoms are signs of different forms of environmental intolerance (EI) as well as other illnesses. In many ways, EIs share defining characteristics with asthma and allergies, where the afflicted person reports symptoms, often in the forms of airway and skin symptoms, after being exposed to environmental factors previously tolerated by the person or commonly tolerated by the general population. EIs are, however, considered medically unexplained symptoms, whereas asthma and allergies generally are not. It may therefore be of relevance to study EIs in asthma and allergy as they can decrease QoL (Söderholm, Söderberg, & Nordin, 2011). In a recent study by Claeson, Palmquist, Lind and Nordin, (2014) it was reported that persons with asthma and persons with more than one asthma/allergy diagnosis, compared to a reference group, reported odorous/pungent and building-related environmental factors to trigger symptoms to a larger extent than did those without asthma/allergy.
It is likely that individuals complaining of symptoms from perfume or other sensory irritating substances do not have an IgE-mediated reaction, which is the cause of an allergic reaction, even though the symptoms may be misinterpreted as allergic (Millqvist, 2008). The origin of symptoms in intolerances have been suggested to be differentiated from those that are due to asthma/allergy, although some suggest that both occupational asthma and multiple chemical sensitivity (MCS) can occur due to exposure to toxic substances (Caress & Steinemann, 2009). Symptoms due to EI are in the general population commonly attributed to chemicals (e.g., perfumed products) and biological materials (e.g., mold) that generate odor and sensory irritation (e.g., pungency). These symptoms are commonly considered as medically unexplained (Henningsen & Priebe, 2003) since the etiology is unknown and since there is no known effective medical treatment. For example, as for asthma/allergy, airway, mucosae and general symptoms (e.g., fatigue) are common also in MCS and non-specific building related symptoms (NBRS; Andersson, Andersson, Bende, Millqvist, &

8
Nordin, 2009; Edvardsson et al., 2008). Meggs and Dunn (1996) reported runny/stuffy nose, eye irritation, sinus symptoms, and shortness of breath to be common in both allergy and self-reported chemical (odor) intolerance. As asthma, allergy and intolerances share similar symptomology it may be an increased risk for an over-diagnosis, or miss-diagnosis of asthma and allergy in actual cases of EI, which may be followed by wrong and too much medication without major effect.
Chemical intolerance (CI) is a form of EI for which symptoms are attributed to low levels of (typically odorous) chemicals such as perfume, cleaning products and fragrant flowers. CI is commonly categorized as either self-reported (i.e., affirmative answers to questions such as “do you get symptoms from odorous exposure”) or given by a physician. The most common clinical definition, physician-diagnosis, of CI is MCS, but other labels such as idiopathic environmental intolerance and sensory hyperreactivity (SHR; Millqvist, 2008) are also used. The estimated prevalence of self-reported CI is surprisingly high, falling between 9 and 33% (Berg, Linneberg, Dirksen, & Elberling, 2008; Caress & Steinemann, 2004; Carlsson, Karlson, Ørbæk, Österberg, & Östergren, 2005; Hausteiner, Bornschein, Zilker, Henningsen, & Förstl, 2007; Johansson, Brämerson, Millqvist, Nordin, & Bende, 2005; Kreutzer, Neutra, & Lashuay, 1999), and between 0.5 and 6.3% fulfill criteria for physician-diagnosed CI (Caress & Steinemann, 2004; Johansson et al., 2005; Kreutzer et al., 1999; Park & Knudson, 2007), see Table 2 for diagnostic criteria for physician-diagnosed EI.
Another form of EI regards individuals who attribute symptoms to certain buildings, here called building intolerance (BI), which is an affliction referred to as NBRS when physician-diagnosed (also called “sick building syndrome”; (Hodgson & Addorisio, 2005). Similar to CI, BI is often categorized as either self-reported or physician-diagnosed. The prevalence for BI has been reported to be 4.3-5.0%, and 2.5% for self-reported and physician-diagnosed intolerance, respectively (Eriksson & Stenberg, 2006; Nordin, 2012).
CI and BI, or for that matter other EIs such as hypersensitivity to sound and symptoms attributed to electromagnetic fields, are often regarded as closely related conditions. They are described as medically unexplained symptoms, possibly with a common underlying mechanism (Yunus, 2008). There is also a large co- and multimorbidity between different EIs (Palmquist, Claeson, Neely, Stenberg, & Nordin, 2014).
Meggs and Dunn (1996) reported an overlap between self-reported CI and allergy in the general population, with as many as 16.9% having both illnesses. Kreutzer and colleagues (1999) found that 19% of asthmatics, compared with 5% of non-asthmatics, were diagnosed by a physician with MCS or EI. It was reported from a Japanese study that as many as 84% of patients with MCS had an allergy to pollen, house dust or drugs (Hojo, Ishikawa, Kumano, Miyata, & Sakabe, 2008). Similar results have been obtained

9
Table 2. Diagnostic criteria for the three intolerances, multiple chemical sensitivity (MCS), sensory hyperreactivity (SHR), and non-specific building-related symptoms (NBRS). Diagnosis Definition Source MCS 1. The symptoms are reproducible with exposure Nethercott,
Davidoff, Curbow, & Abbey, 1993
2. The condition is chronic (>6 months)
3. Low levels of exposure result in manifestations of
the syndrome
4. The symptoms improve or resolve when the
incitants are removed
5. Responses occur to multiple chemically unrelated
substances 6. Symptoms involve multiple organ systems
SHR 1. Reproducible respiratory symptoms Johansson, Millqvist, Nordin, & Bende, 2006
2. Symptoms are triggered by scents or chemicals
3. Positive cough provocation with inhaled capsaicin
4.
Affective reactions and impact on the behavior of odorous/pungent substances
5. The condition is chronic (>6 months)
NBRS A.
General, mucosal, and skin symptoms weekly during the last 3 months
World Health Organization, 1983
B. 1. People in the building complain of symptoms of acute discomfort
2. The cause of the symptoms is unknown
3.
Most of the complainants report relief soon after leaving the building
in other studies, in which symptoms of allergy and BI were difficult to distinguish (Menzies & Bourbeau, 1997).
The fact that prevalence of EI has been reported to overlap with asthma and allergy (Kreutzer et al., 1999; Meggs & Dunn, 1996; Wang et al., 2008) motivates a broader perspective when investigating asthma and allergy from a psychological perspective. Comorbid intolerance, such as CI and BI, in asthma and allergy may be a factor that can increase stress and social isolation as well as decrease QoL. Such a perspective may increase the understanding for possible factors that might play a role in asthma and allergy and contribute to increased understanding for the processes of PNI. One aspect would be the relation between illness and prolonged stress which can increase the risk for both physical and psychiatric disorders (McEwen, 1998) which may be involved in asthma and allergy together with EI. EI has previously been reported to affect individuals in multiple negative ways. In addition to health symptoms and social

10
isolation, these individuals are typically not being taken seriously by health professionals (e.g. Söderholm et al., 2011). This may worsen QoL for persons with comorbid asthma and allergy and lead to increased stress.
Distress
A linkage between asthma and allergy, on the one hand, and psychological factors, on the other, has evoked scientific interest for decades. The early introduced concept of ‘psychogenic asthma’ illustrates the belief that psychological factors may trigger illness symptoms, and the impact of asthma and allergy symptoms on QoL provides further illustration of such a linkage. Apart from the fact that the symptoms of asthma, allergic rhinitis, and atopic dermatitis are aggravating, patients with these conditions often report other symptoms than those typical for that condition, such as disturbed sleep (Goral, Lipsitz, Muhsen, & Gross, 2012; Hanifin & Rajka, 1980; Juniper, 1997) and stress. As a result, these conditions are associated with poor health-related quality of life (HRQoL). This includes adverse impact on physical, emotional, and social functioning, and concentration difficulties at home, work and school, contributing to, for example, decreased productivity (Blanc et al., 2001; Bousquet et al., 1994; Bousquet et al., 1996; Juniper, 1997; Marshall & Colon, 1993; Meltzer, Nathan, Seiner, & Storms, 1997). This may lead to worsening of the illness itself and to increased negative affect in the afflicted individual.
Poor mental health, or psychological distress, has previously been shown to be related to atopy. Indeed, in a meta-analysis, Chida and collaborators (2008) demonstrated a bidirectional relationship between psychological distress and atopy. This study suggested a potential negative loop, such that atopy may lead to psychological distress, which, in turn, may reinforce the atopy outcome. Relevant aspects of psychological distress in this context are stress, burnout (mental and physical exhaustion), anxiety, depression, and health worries. The association between stress, on the one hand, and atopy in the form of allergic asthma (Rand et al., 2012; Yonas, Lange, & Celedón, 2012; Lekander, 2008), allergic rhinitis (Mösges & Klimek, 2007) and atopic dermatitis (Mitschenko, Lwow, Kupfer, Niemeier, & Gieler, 2008), on the other hand, is well documented. However, conflicting results exist, suggesting that stressors do not have a significant adverse impact on atopic illness (Chida et al., 2008). In addition, mechanisms underlying stress as a mediator of atopy have carefully been described (Rand et al., 2012; Wright, 2005; Wright, Cohen, & Cohen, 2005; Yonas et al., 2012). Thus, psychological distress may be related to atopy in two ways; directly with distress being a result of atopy as the illness may increase anxiety or depression due to the medical state, and indirectly with distress being a mediator between atopy and symptoms where stress can trigger an allergic reaction.

11
The definition of psychological distress used in this thesis is based on previous findings showing that stress can have a negative effect on immunology (Cohen, Janicki-Deverts, & Miller, 2007) and lead to depression and anxiety (Aneshensel, Rutter, & Lachenbruch, 1991; Nolen-Hoeksema, 2001; Schmaus, Laubmeier, Boquiren, Herzer, & Zakowski, 2008), all which are believed to affect the immunological status (Kiecolt-Glaser & Glaser, 2002). Long-term stress, which may be a cause of chronic illness, might lead to burnout in terms of both mental and physical exhaustion (Ptacek et al., 2013), and both stress and burnout are believed to negatively affect mental health status, such as depression (Schaufeli & Greenglass, 2001). Health worries for environmental pollution may be of relevance in this context since asthmatics have previously reported outdoor pollution to be a common trigger factor (Vernon et al., 2013), and thus is believed to be a factor that may lead to increased stress. Based on this reasoning, these five aspects are believed to be closely related, such that one aspect might lead to another.
Considering the close relation between stress and various forms of negative affect (Karasek & Theorell, 1990; Rusli, Edimansyah, & Naing, 2008), it is reasonable to expect that other aspects of psychological distress, such as exhaustion, anxiety, depression and health worries, also would be associated with atopy. However, the picture is not clear regarding these associations. Since stress is associated with atopy, burnout (a result of prolonged stress) would be expected to also be associated with atopy, but no such studies have to my knowledge been documented. Regarding anxiety and depression some studies support a relation with some forms of atopy. Early work suggests that both anxiety and depression are associated with atopy (Bell, Jasnoski, Kagan, & King, 1991) as well as asthma (Vamos & Kolbe, 1999). In a study by Wainwright, Surtees, Wareham, and Harrison (2007) it was reported that anxiety or depressive disorders were associated with increased rate of hospital admissions due to asthma. Other studies have reported that prolonged worry is known to reinforce the development of immunological, endocrine, cardiovascular and neurovascular illness (Brosschot, Gerin, & Thayer, 2006; Verkuil, Brosschot, Meerman, & Thayer, 2012), and it is most likely that hypersensitivity to environmental allergens will evoke health worries for such environmental exposure. Based on this, such worry would possibly also generalize to health worries for environmental pollution. However, no such studies have been found for any of the asthma/allergy diagnosis used in this thesis, but in food intolerance, which has been shown to be associated with a global measure of worry for environmental and technological aspects of modern life (Petrie et al., 2001). Of relevance would be to specifically investigate the relation between atopy and aspects of modern life that refer to environmental pollution.
No previous study has compared different diagnoses of asthma and allergy with respect to stress, burnout, anxiety, depression and health worries, nor has a comparison been made with persons without asthma/allergy who are drawn from the same population-based sample. Such a procedure would increase the generalizability and comparability.
12
Taken together, distress may affect asthma and allergy in various ways. The fact that the illness is chronic might increase the level of distress, which may further increase the need of help and understanding from the social surrounding.
Coping and social support
A high level of distress may lead to reduced QoL as well as decrease in other aspects of psychological well-being. Although medical treatment such as desensitization, a method for preventing the onset of symptoms of IgE-mediated allergic illness by reducing sensitivity to allergens, may be useful for some patients, there is no easily administrated treatment for asthma and allergy. Due to this, most patients are limited to medication such as corticosteroids and antihistamines to help them control the symptoms. With this in mind, the illness itself is a stressful factor that will increase the need and usage of coping strategies (Tijhuis, Flap, Foets, & Groenewegen, 1995) and social support (Cobb, 1976).
Coping is defined as realistic and flexible thoughts and actions to solve problems, but also to handle emotions and thereby reduce stress (Lazarus & Folkman, 1984). It can also be explained as the process of handling or managing specific demands, which are appraised as exceeding available resources, were the accompanying emotions are referred to as coping (Lazarus & Folkman, 1984). Coping can be divided into strategies that are focused either on emotions or on problems. On one hand, emotion focused coping includes acknowledging, understanding and expressing the emotion, and is more likely to occur when the environment or an event is perceived as taxing, unpredictable or uncontrollable, which are appraised as unchangeable, and can be used as an emotional reaction to avoid and prevent depression. Problem-focused coping, on the other hand, includes analyzing, reducing or eliminating stressors, and is more likely in situations that are perceived as threatening or dangerous, and are valued as susceptible to change either by solving or altering the source of stress (Lazarus & Folkman, 1984; Snyder, 1999). An appropriate coping strategy can in a stressful situation relieve the individual from stress, and reduce the emotional suffering induced by the situation (Lazarus & Folkman, 1984). It is therefore important to have a set of strategies that work in different situations and are able to adapt to the specific needs. In summary, one can say that problem-focused coping tends to dominate when the person feels that something constructive can be done, and emotion focused coping tends to dominate when the person feels that the stressor is uncontrollable or unchangeable (Lazarus & Folkman, 1984).
Social support is defined as the aid, comfort, and confirmation given by, for example, family, friends, and coworkers that makes the individual feel cared for, loved, esteemed, and part of the community (Cobb, 1976). The support itself can be divided into different types, such as emotional (e.g., comfort, understanding and appreciation),

13
instrumental (practical assistance) and informative (help with information; Lakey & Cohen, 2000) support. The support is believed to buffer against stressors (Cohen & Wills, 1985), but in order to be stress-reducing the support must match the stressor (Cutrona & Russell, 1990). Specific needs, especially in chronic illness, should be met by specific types of social support, meaning that also the sources of the support must be specific to the stressor. For instance, information about the illness and its treatment is presumably best provided by healthcare professionals, whereas information about societal resources and rights is best provided by association and support groups, and emotional support by family and friends (Dakof & Taylor, 1990; Masters, Stillman, & Spielmans, 2007). Studies examining depression indicate that instrumental support protects more against depression in functionally disabled patients (Fitzpatrick et al., 1991), whereas emotional support protects against depression in patients with a life-threatening illness (Ell, Nishimoto, Mediansky, Mantell, & Hamovitch, 1992). Regarding overall well-being, social support has been suggested to be related to better psychological (Turner, 1981) and physical health (Uchino, 2006).
There are theories regarding how we seek social support and from whom we receive it. One theory, ‘the social comparison theory’, suggests that individuals turn to those who are similar to themselves. This refers not only to those with the same personality and attitudes, but also to those who have experienced a similar situation, for example an illness. The received support is believed to have a relatively calming effect when it comes to stress (Cohen & Wills, 1985). Cohen and Willis (1985) have proposed two hypotheses regarding how social support can improve health. First, they suggest that social support will strengthen overall health for everyone (the buffering hypothesis). Secondly, social support only enhances health in those who experience a stressful situation (the direct effect hypothesis).
Studies have suggested that an individual’s way of coping may be affected by social support (Baum, Revenson, & Singer, 2012). In chronic illness, such as asthma and allergy, social support has been suggested to have beneficial effects on coping (Cohen, Gottlieb, & Underwood, 2000) as well as enhancing effects on health promoting behavior (Cohen & Wills, 1985). Both social support and coping strategies are believed to affect each other, and may enhance the person’s ability to cope with difficult situations overall. It is also believed to have a positive effect on problem solving and in reducing the effects of stress (Lakey & Cohen, 2000; Snyder, 1999; Taylor & Stanton, 2007). In general, one can explain coping as being performed by the individual him- or herself, whereas social support is provided by others in the closest surrounding. Social support may affect coping according to the main-effect hypothesis, suggesting that the individual with strong perception of social support has a feeling of being loved and cared for, which has a permanent positive effect on the individual’s general health (Frey & Röthlisberger, 1996). In that sense the support may serve as a resource of coping by influencing the choice of coping strategy in a stressful situation (Schreurs & de Ridder, 1997).

14
Regarding coping, some types of strategies are important in order to avoid and prevent depression, which has been found to be associated with asthma (Vamos & Kolbe, 1999). Social support, in contrast, when being perceived as high has been found to buffer against asthma incidence (Loerbroks, Apfelbacher, Bosch, & Sturmer, 2010) whereas low support has been found to elevate the risk of hospital admittance with 30% (Wainwright et al., 2007). Furthermore, studies have reported that low social support or burdensome relationships have been linked to markers for pro-inflammatory activity, whereas high social support has been suggested to be associated with lower pro-inflammatory activity (Ford, Loucks, & Berkman, 2006).
Clark and Nothwher (1997) reported that patients with asthma experience both positive and negative aspects regarding social support from family members, friends and co-workers. Several of the patients felt that those closest to them did not understand how it was to live with asthma. One way to cope with this was being less sensitive, and reducing contact with those who they felt were less supportive. A secure individual was in that study found to be more likely to receive social support not only from a partner, but also from other family members and friends, compared to a more insecure individual. Regarding coping, Sexton and colleagues (1999) found differences in coping strategies between patients with mild and severe asthma symptoms, such that those with severe disorders used larger number of coping strategies. Taken together, many patients with asthma might see the illness as a cause of loss in personal health and self-esteem, for which both coping and social support are important factors for managing and reducing the emotions. Thus, for increasing well-being and QoL, but also the feeling of being seen and loved from those in the closest surrounding.
General aims of the thesis
The overall aim of this thesis is to better understand asthma and allergy from different psychological perspectives, ranging from comorbidity with intolerances to chemicals and certain buildings, to experienced distress, and to coping strategies and perceived social support. These aims were addressed with three studies, all which were conducted within the Västerbotten Environmental Health Study (VEHS). The specific research questions were:
1. What is the overlap in prevalence between asthma/allergy diagnosis, intolerance to odorous/irritating chemicals, and intolerance to certain buildings in the general population? Do these overlaps differ from what would be expected by chance?
2. Are there differences between persons with allergic asthma, non-allergic asthma, allergic rhinitis, atopic dermatitis, and non-asthma/allergy (referents) in the general population with respect to different aspects of psychological
15
distress such as perceived stress, burnout (mental and physical exhaustion), anxiety, depression, and health worries for environmental pollution?
3. To what extent are different types of problem and emotion focused coping used in asthma and allergy, and is degree of symptom exacerbation of asthma and allergy associated with usage of coping strategies?
4. To what extent are different types of social support (instrumental, emotional and informative) perceived to be received from different sources (partner, other family members, friends, co-workers, healthcare, authorities and association/support groups), and is degree of symptom exacerbation of asthma and allergy associated with social support?
General methods
The Västerbotten Environmental Health Study
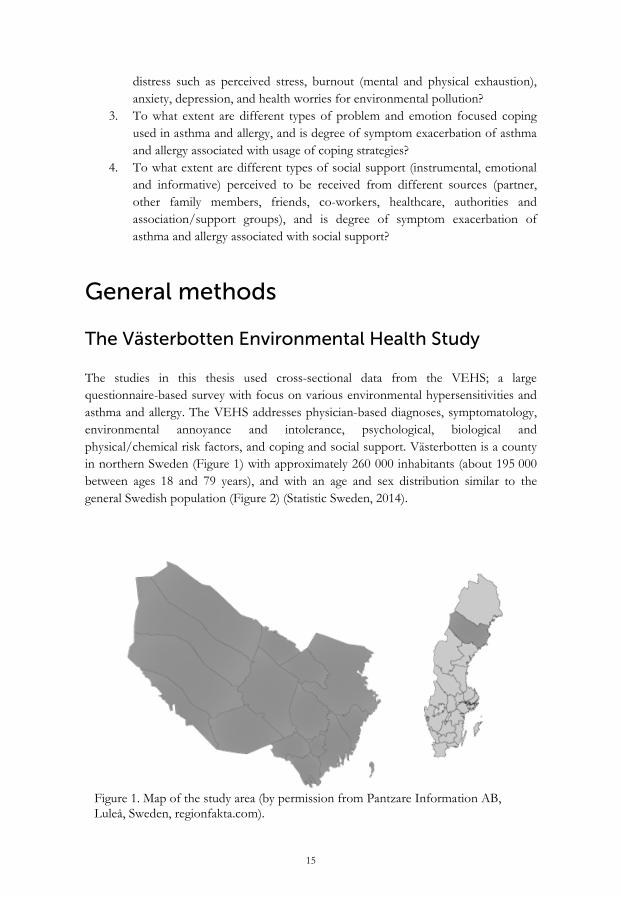
The studies in this thesis used cross-sectional data from the VEHS; a large questionnaire-based survey with focus on various environmental hypersensitivities and asthma and allergy. The VEHS addresses physician-based diagnoses, symptomatology, environmental annoyance and intolerance, psychological, biological and physical/chemical risk factors, and coping and social support. Västerbotten is a county in northern Sweden (Figure 1) with approximately 260 000 inhabitants (about 195 000 between ages 18 and 79 years), and with an age and sex distribution similar to the general Swedish population (Figure 2) (Statistic Sweden, 2014).
Figure 1. Map of the study area (by permission from Pantzare Information AB, Luleå, Sweden, regionfakta.com).

16
Figure 2. Distribution of the population of Sweden (dark bars) and Västerbotten (light bars) for each age strata.
To obtain a representative sample of the population, 8600 adults (aged 18–79 years) from the county of Västerbotten were randomly selected from the population registry after stratification according to sex and six age strata: 18–29 years (n = 1990; men = 1035, women = 955), 30–39 years (n = 1377; men = 717, women = 660), 40–49 years (n = 1452; men = 741, women = 711), 50–59 years (n = 1467; men = 746, women = 721), 60–69 years (n = 1395; men = 702, women = 693) and 70–79 years (n = 919; men = 426, women = 493).
Eighty persons were excluded from the sample because they were identified as unknown by the postal service, resulting in a sample of 8520 persons. The sample size was based on the lowest expected prevalence for a specific EI by sex, which was EI to electromagnetic fields for men (1.1%; Hillert, Berglind, Arnetz, & Bellander, 2002). Precision was set to 0.55% (Naing, Winn, & Rusli, 2006), and with a level of confidence of 95% the sample size was calculated according to Daniel (1995) to 1382 men.
Since the sex distribution in Västerbotten was nearly equally distributed (50.3% men) in 2010 (Statistic Sweden, 2014) the number of women needed was rounded up to the same number as for men. With an expected response rate of 60% the sample size was estimated to 4607 participants. The present studies were based on the first part of an ongoing longitudinal study. Thus, the sample size was estimated to fully 8530 participants which was rounded up to 8600. Among the 8520 who could be reached, 3406 (40.0%) volunteered to participate. The highest non-response rate is found among men aged 18-29 years, whereas highest response rate is found among old men (Table 3).

17
The questionnaire was sent by mail together with written information concerning confidentiality, intended use of the data, and that participation was voluntary. A reminder was sent to non-responders after fully three weeks. An additional reminder and a new copy of the questionnaire were sent after another three weeks. The present study was conducted between March and April 2010 (before the allergy season in the northern part of Sweden).
Data from the VEHS questionnaire consisted of various sections, see Table 4. Section (i) was used for all studies in the thesis to acquire demographic information, and section (ii) for the asthma and allergy diagnoses. In Study I sections (ii) and (iii) were used for physician-diagnosed and self-reported EI. In Study II section (vi) was used to assess perceived stress, burnout (mental and physical exhaustion), anxiety, depression, and modern health worries. In Study III section (iii) was used regarding background information concerning asthma and allergy, and section (ix) concerning coping strategies and social support.
Table 3. Numbers of respondents (and response percentages of those invited) across age and sex strata and for the entire sample.
Age strata (years) Women Men
18-29 307 (32.1) 179 (17.3)
30-39 266 (40.3) 177 (24.7)
40-49 288 (40.5) 230 (31.0)
50-59 369 (50.9) 295 (39.5)
60-69 405 (58.4) 356 (50.7)
70-79 265 (53.8) 271 (63.6)
18-79 1898 (44.8) 1508 (34.5)

18
Table 4. Contents of the VEHS and sections used for the three studies in this thesis.
Study
Section Content I II III
i Demographic inquiries ii Inventory on diagnosed cases of disease iii Questions on self-reported intolerance and symptoms
attributed to asthma/allergy and environmental factors
(odorous/pungent chemicals, certain buildings, sounds
and EMFs)
iv Inquiries on affective and behavioral consequences of
noise, odorous/pungent chemicals and EMFs
v Inventories on somatic symptoms and symptoms
associated with EIs
vi Questionnaire instruments for assessing selected aspects
of mental health problems (perceived stress, burnout
syndrome, anxiety, depression, hopelessness and
helplessness, modern health worries)
vii Questions concerning sleep viii Inquiries on certain environments and sources eliciting
problems
ix Section, only answered by those with self-reported EI
and asthma/allergy containing questions on coping and
social support

19
Participants
A total of 530 responders reported having been given at least one of the diagnoses allergic asthma, non-allergic asthma, allergic rhinitis or atopic dermatitis by a physician. In total, 2876 respondents reported not to have an asthma or allergy diagnosis, and constituted a reference group. The entire sample consisted of 3406 individuals. The responders with and without asthma or allergy, and the entire sample are described in Table 5 with respect to demographics, health-related life style, and diagnoses of asthma and allergy.
All responders where asked whether they had been given a physician-based diagnosis from a list of 33 diagnoses. It is important to note that the diagnoses used for these studies have not been obtained through health examinations or register search, and are therefore being referred to as self-reported physician diagnoses.
In Study I all individuals who reported to have one or more asthma/allergy diagnoses were combined into an asthma and allergy group: (i) allergic asthma, (ii) non-allergic asthma, (iii) allergic rhinitis, and (iv) and atopic dermatitis. In Study II those who reported to have one of the asthma and allergy diagnoses (i−iv) were selected for analysis in comparison to the referents (none asthma/allergy). Those with more than one diagnosis were excluded from the analysis, as the aim was to compare specific diagnoses of asthma and allergy with those who did not have asthma or allergy. The individuals selected for Study III had one or several of the diagnoses (i−iv). If they had a diagnosis of EI they were included only if they reported that their asthma/allergy was more disturbing than their EI. Additional inclusion criteria in Study III were having responded to questions in the questionnaire about frequency of asthma/allergy exacerbations, coping strategies and social support. Flow charts for participation are presented in Figures 3−6.

20
Table 5. Demographics, health-related life-style, perceived health, and specific physician-based diagnoses of asthma and allergy in the participants with any diagnosis of asthma and/or allergy (asthma/allergy), without asthma/allergy (referents) and in the entire sample.
Asthma/allergy n=530
Referents n=2876
Entire sample n=3406
Age (mean±SD) 48.8±17.0 51.7±16.8 51.2±16.9 Women (%) 57.7 55.4 55.7 University education 44.7 41.2 41.2 Married/partner (%) 71.1 74.6 74.6 Smoking regularly (%) 7.6 9.0 8.8 Physical exercise > twice a week (%) 66.1 67.3 67.1 Alcohol consumption > twice a week (%) 13.7 12.4 12.6 Perceived general health (%) Excellent/very good 35.6 40.9 40.0 Good 32.9 34.4 34.2 Fairly good/poor 31.5 24.7 25.8 Asthma/allergy diagnoses (%) Allergic asthma 30.9 0 4.8 Non-allergic asthma 24.3 0 3.8 Allergic rhinitis 56.2 0 8.7 Atopic dermatitis 16.6 0 2.6

21
Total sample n=3406
Total sample n=3406
Physician-diagnosed asthma and allergy n=530
Physician-diagnosed asthma and allergy n=530
Excluded: multiple asthma/allergy diagnosis n=132
Single diagnosis of asthma/allergy n=298
Healthy control group n=2786
Allergic asthma n=76
Non-allergic asthma n=86
Allergic rhinitis n=190
Atopic dermatitis
n=46
Figure 3. Flow chart showing the participants in Study I.
Figure 4. Flow chart showing the participants in Study II.

22
Total sample n=3406
Total sample n=3406
Physician-diagnosed asthma and allergy n=530
Physician-diagnosed asthma and allergy n=530
Excluded: other main sensitivity n=145
Excluded: other main sensitivity n=145
Excluded: missing data on coping n=198
Asthma/allergy sample n=187
High severity n=63
Low severity n=124
Excluded: missing data on coping n=291
Asthma/allergy sample n=94
High severity n=37
Low severity n=57
Figure 5. Flow chart showing the participants in Study III: coping strategies.
Figure 6. Flow chart showing the participants in Study III: social support.

23
Ethical approval
The study was conducted in accordance with the Helsinki Declaration and approved by the Umeå Regional Ethics Board (Dnr 09-171M). All participants gave their informed consent to participate.
Data management
Filled-out questionnaires were scanned, and a database was created. A data-entry verification test was per-formed to check the accuracy of the scanning procedure. Each randomly selected questionnaire of 35 (∼1% of all filled-out questionnaires) were compared with the entries in the database, revealing an error rate of 0.11%, which was considered insignificant. Several quality control checks (e.g. range checks and logical checks) were performed to test the accuracy of the data before analysis (Palmquist et al., 2014). Missing data in the database was replaced by using the method of multiple imputation (Graham, 2008; Schafer & Graham, 2002; Sinharay, Stern, & Russell, 2001).
Statistical analysis
The Statistical Package for the Social Sciences (SPSS, IBM Corp., IBM SPSS Statistics for Windows, Version 22.0, Armonk, NY, USA) was used to analyze the data. Chi-square analysis where performed in Study I, and Kruskal-Wallis one-way analysis of variance in Study II. In Study III a two-way mixed model analysis of variance (ANOVA) was conducted separately for problem-focused and emotion-focused strategies, with type of strategy (four levels for both problem- and emotion-focused strategies) as a within group factor, and symptom frequency (two levels: low and high frequency of asthma/allergy exacerbation) as a between group factor. A three-way mixed model ANOVA was conducted for support type (three levels: understanding, practical help, and help with information) and support source (seven levels: one’s partner, other family members, friends, coworkers, the healthcare system, authorities, and patient associations/support groups) as within group factors, and symptom frequency (two levels: low and high frequency of asthma/allergy exacerbation) as a between group factor. Greenhouse-Geisser correction was applied in all ANOVAs. The α-level was set at 0.05, except for post-hoc analyses and the one- and two-way ANOVAs that compared pairs of support sources, for which an α-level of 0.01 was chosen due to a large number of pairwise comparisons.

24
Study-specific group categorization and statistical analysis
Study I
In Study I, individuals with intolerance to chemicals and certain buildings were identified by answering affirmatively to one of the questions in section (iii) in the questionnaire regarding self-reported intolerance to odorous/pungent chemicals or certain buildings. For self-reported intolerance participants were asked to answer “yes” or “no” to the questions “Are you getting symptoms from odorous/pungent chemicals (not limited to certain buildings), such as perfumes and cleaning agents, in doses that you were not getting symptoms from before or that you believe most other people are not getting symptoms from? “for self-reported CI, and “Are you getting symptoms from residing in certain buildings (non-specific building related symptoms) that you were not getting symptoms from before or that you believe most other people are not getting symptoms from?” for self-reported BI. Cases diagnosed with asthma and allergy were identified by answering affirmatively to having been diagnosed by a physician with asthma due to allergy, asthma without allergy as known cause, allergic rhinitis and atopic dermatitis. For diagnosed EI, participants reporting to have been given a diagnosis by a physician of SHR or MCS were referred to as physician-diagnosed CI. Participants reporting to have been given a diagnosis by a physician of NBRS were referred to as physician-diagnosed BI. Self-reported and diagnosed cases did partially overlap, and may be considered as different criteria for EI. As the aim was to examine comorbidity in asthma and allergy with EI, the observed prevalence rates were compared with corresponding expected prevalence rates in a sample of non-asthma/allergy by means of chi-square analysis. For all comparisons an α-level of 0.05 was used.
Study II
In Study II, participants reporting to have a diagnosis of either (i) allergic asthma, (ii) non-allergic asthma, (iii) allergic rhinitis, or (iv) atopic dermatitis were included in the analysis. The aim was to investigate differences between each of the asthma and allergy groups as well as between these groups and referents with no asthma/allergy. Participants with more than one asthma/allergy diagnosis were excluded in the analyses. The five groups were compared with respect to five measures of psychological distress. Since the five groups were very different in sample size and not normally distributed on the measures of psychological distress, the non-parametric test Kruskal-Wallis one-way analysis of variance was chosen. For all analyses α=0.05 was used, except for post hoc-analyses for which an α-level of 0.01 was chosen due to a large number of comparisons.
25
Study III
In Study III, those participants were included who (i) had been diagnosed by a physician with asthma due to allergy, asthma without allergy as known cause, allergic rhinitis and/or atopic dermatitis, (ii) reported that their asthma/allergy was the most severe health problem if they also had an EI, and (iii) responded to questions about coping strategies and social support. Missing data on coping strategy were imputed (see below for further description) based on multiple imputation technique. This was not possible for the social support section as not all sources may be applicable. It the latter case it was not possible to know whether a non-response to questions about social support from, for example, a partner or co-workers was a true missing value, or whether the question was not applicable due to not having a partner or co-workers. Therefore, the group sizes are different in the two sub-studies in Study III. The statistical analyses tested differences in the usage of coping strategies as well as perception of social support from seven sources in groups of high and low asthma/allergy symptom exacerbation. As the data on coping and support were normally distributed, ANOVAs were chosen in both sub-studies. A two-way ANOVA (type of coping strategy by level of symptom exacerbation) was conducted in the first sub-study, and a three-way ANOVA (support type by support source by level of symptom exacerbation) was conducted in the second sub-study. For all analyses α=0.05 was used, except for post hoc-analysis for which an α-level of 0.01 was chosen due to a large number of comparisons.
Overview of the empirical studies
Study I – Co- and multimorbidity between asthma and allergy and intolerance to chemicals and certain buildings
Aims and specific methods
Based on prior studies of associations between conditions of asthma/allergy, chemical- and building-related conditions and on the assumption that they share substantial symptomology, the hypothesis of Study I was that the comorbidity in asthma/allergy with EI would be larger than by chance. Overlaps were examined both as EI within asthma and allergy and asthma and allergy within EI. For the examined overlaps see Table 6. Overlaps between BI and CI have been presented elsewhere (Palmquist et al., 2014). Assessment of physician-diagnosed asthma/allergy and physician-diagnosed and

26
self-reported CI and BI is described in the section “Study-specific group categorization and statistical analysis.”
Table 6. Overlaps examined among the different groups. Among persons with physician-diagnosed asthma/allergy Physician-diagnosed chemical intolerance only Physician-diagnosed building-related intolerance only Both physician-diagnosed chemical intolerance and physician-diagnosed building-
related intolerance Self-reported chemical intolerance only Self-reported building-related intolerance only Both self-reported chemical and building-related intolerance Among persons with physician-diagnosed chemical intolerance Both physician-diagnosed asthma/allergy and physician-diagnosed building-related
intolerance Among persons with self-reported chemical intolerance Both physician-diagnosed asthma/allergy and self-reported building-related
intolerance Among persons with physician-diagnosed building-related intolerance Both physician-diagnosed asthma/allergy and physician-diagnosed chemical
intolerance Among persons with self-reported building-related intolerance Both physician-diagnosed asthma/allergy and self-reported chemical intolerance
Results and discussion
In this section, only the results from perspective of having asthma/allergy and non-asthma/allergy are commented on (see Study I in Appendix for all overlaps, including those from the EI perspective). Overlaps are presented as observed numbers of physician-diagnosed asthma/allergy, CI only, BI only, and CI and BI in combination. Observed frequencies are presented in Figure 7, separately for the sample with asthma/allergy and the referents, and separately for physician-diagnosed and self-reported intolerance.

27
All observed overlaps showed to differ statistically significant in frequency from what would be expected by chance which was the case for all possible comparisons. Thus, both the prevalence of co- and multimorbidity were higher than what would be expected statistically. Analysis suggested odds ratios (ORs) between 3 and 11 for having either a chemical-related or a building-related intolerance among persons who also have asthma/allergy. The OR for the multiples, having both chemical and building intolerance if the person also has asthma/allergy, were even larger, showing ORs of 6-22 (see Appendix for Study I and Table 2), suggesting that the observed prevalence is larger than the entity. All OR are statistically significant.
448 51
20
11
36
5
11
PDAsthma/allergy PD Chemical
PD Building
350
209
47
109
49
22
47
SR Chemical
SR Building
PDAsthma/allergy
109
4947
47 22SR Building
SR Chemical
Referents
2092573
530530
2876
414
165
112
47
414
165
PD A
sthm
a/al
lerg
y
Physician-diagnosed Self-reported
Refe
rent
s 109
22
49
PD Chemical
Referents
365
112051
11
2824
PD Building
2876
47
11251
2011
Figure 7. Venn-diagrams of case groups representing comorbidity of asthma/allergy, chemical and building intolerance both in forms of physician-diagnosed (PD; left diagram) and self-re-ported (SR; right diagram) intolerance. Referents without asthma/allergy for comparison. The numbers in the figures refer to number of participants with the condition. Note that the circle areas for the asthma/allergy and referent group are set equal to enhance direct comparison of proportions.

28
The comorbidity was indeed high for both physician-diagnosed and self-reported intolerance within asthma/allergy. This may indicate a large proportion of persons with asthma/allergy being more bothered by other sources and triggers than what would be considered as common asthmatic or allergic trigger factors. Considering that asthma and allergy possibly share common ground with CI and BI on symptomology and environmental factors that trigger symptoms, it is not surprising that these two conditions seem to be more prevalent in asthma/allergy than in the general population. With the assumption that CI is a common underlying condition in building-related intolerance, similarities between allergy and CI may be of interest for understanding the high comorbidity in asthma/allergy. In asthma/allergy, but most likely also in CI, protective defense mechanism explain the symptoms. In allergy, allergens that are not invasive to most people are identified by the immune system in the afflicted person as threats that evoke defensive mechanisms that, in turn, trigger health symptoms. In a similar vein, in CI, chemical substances that are not invasive to most people are identified by the olfactory and chemosomatosensory systems in the afflicted person as threats that evoke defensive mechanisms that, in turn, trigger health symptoms. The symptoms may, in both allergy and CI, develop in order to signal the individual to avoid the particular environment, irrespective of whether the threat in fact is hazardous or not. Memory plays a critical role in both types of hypersensitivity; it is involved in identifying the allergen/chemical substance, in categorizing it as a threat, and in retrieving appropriate biological, behavioral and emotional reactions. In speculating, it is possible that the learned reaction with symptoms in response to one type of threat (e.g., an allergen) generalizes over time to another type of threat (e.g., odorous/pungent substances) which could possibly explain some the comorbidity between CI and asthma/allergy, but also between asthma/allergy and BI and between CI and BI.
Study II – Psychological distress in asthma and allergy
Aims and specific methods
The aim was to better understand stress, burnout, anxiety, depression, and health worries for environmental pollution in allergic asthma, non-allergic asthma, allergic rhinitis and atopic dermatitis. This was investigated by comparing each of these four diagnosis groups with each other and with a referent group with no asthma/allergy. It was hypothesized that the five aspects of psychological distress would be higher in allergic asthma, allergic rhinitis, and atopic dermatitis, but not in non-allergic asthma, when compared to persons with no asthma or allergy, and that depression would have a weaker association than anxiety with the three forms of atopy.

29
Various questionnaire instruments were used for assessing psychological distress. The questionnaire used included Swedish versions of the Perceived Stress Scale (Cohen, Kamarck, & Mermelstein, 1983) for measuring stress, the Shirom-Melamed Burnout Questionnaire (Melamed, Kushnir, & Shirom, 1992) for measuring burnout in the form of mental and physical exhaustion, the Hospital Anxiety and Depression Scale (HADS; Zigmond & Snaith, 1983) for measuring anxiety and depression, and the Environmental Pollution subscale of the Modern Health Worries Scale (Petrie et al., 2001) for measuring health worries about environmental pollution.
Results and discussion
The analysis yielded significant group differences for stress, burnout and anxiety for allergic asthma and atopic dermatitis, meaning that these two diagnosis groups reported higher on these measures in comparison to the other groups. There was a strong tendency (p < .07) for higher scores in the allergic asthma and atopic dermatitis groups regarding depression and health worries for environmental pollution. The groups with allergic asthma and atopic dermatitis did not differ from each other, but these two groups had significantly higher scores than the groups with non-allergic asthma, allergic rhinitis, and the referents. The latter three groups did not differ significantly from each other, see Figure 8.
The hypothesis that psychological distress would be higher than normal in allergic asthma, allergic rhinitis and atopic dermatitis, but not in non-allergic asthma, was partly supported by the data. Thus, stress, exhaustion and anxiety were found to be more extensive than normal in allergic asthma and atopic dermatitis, but not in non-allergic asthma or allergic rhinitis, whereas there was only a tendency of such abnormalities regarding depression and health worries for environmental pollution. However, the result of depression being less prominent than anxiety in allergic asthma and atopic dermatitis was in accordance with the hypothesis. The high degree of burnout may be a result of the high stress level, indicated by high scores in allergic asthma and atopic dermatitis in this study, as burnout is likely to be a result from long-term stress, which can be a cause of the illness itself being presented for a long period of time, resulting in burnout in forms of both mental and physical exhaustion.
The high scores on the Anxiety subscale of the HADS in allergic asthma may to some extent be referred to panic attacks. It is well known that panic attacks are associated with asthma (Goodwin & Eaton, 2003; Goodwin, Pine, & Hoven, 2003). Regarding the high anxiety and stress scores in atopic dermatitis, a review from Hashizume and Takigawa (2006) suggests a psychoneuroimmunological mechanism of interest in this context. Atopic patients with emotional problems may develop a vicious cycle between anxiety and symptoms. Stress, both acute and chronic can affect these patients by increasing the level of anxiety. Anxiety, in turn, may increase the risk for respiratory symptoms as a result of the stress induction itself whereas the anxiety and symptoms in
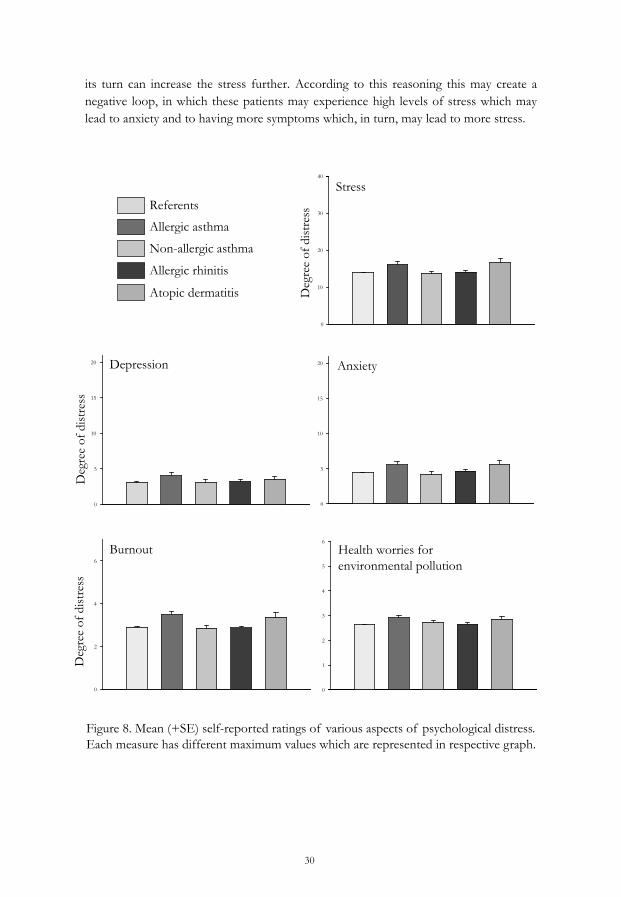
30
its turn can increase the stress further. According to this reasoning this may create a negative loop, in which these patients may experience high levels of stress which may lead to anxiety and to having more symptoms which, in turn, may lead to more stress.
Anxiety
0
5
10
15
20Depression
0
5
10
15
20
Health worries for environmental pollution
0
1
2
3
4
5
6
Burnout
0
2
4
6
Stress
0
10
20
30
40
Deg
ree
of d
istre
ss
Deg
ree
of d
istre
ss
Referents
Allergic asthma
Non-allergic asthma
Allergic rhinitis
Atopic dermatitis
Deg
ree
of d
istre
ss
Figure 8. Mean (+SE) self-reported ratings of various aspects of psychological distress. Each measure has different maximum values which are represented in respective graph.

31
Study III – Coping and social support in asthma and allergy
Aims and specific methods
The aim was to better understand how individuals with different degree of asthma/allergy severity use (i) problem-focused and emotion-focused coping strategies to cope with their illness, and (ii) perceive having received different types of social support (instrumental, emotional and informational) from different sources (partner, other family members, friends, coworkers, the healthcare system, authorities, and patient associations/support groups). Severity was operationalized as symptom exacerbation frequency, where monthly symptom exacerbation was considered as low, and was compared with daily/weekly exacerbation which was considered as high. Frequency of asthma/allergy symptom exacerbation was assessed with the question “How often do you in general have asthma/allergy exacerbations?” (daily / once or a few times per week / once or a few times per month).
Coping strategies were assessed with four statements about problem-focused strategies and four statements about emotion-focused strategies (Table 7). Social support was assessed with the three questions “To what extent do you perceive that you receive (1) understanding for…, (2) help with information about…, and (3) practical help with… …your asthma/allergy?” Thus, the questions referred to emotional support (operationalized as understanding), instrumental support (practical help), and informative support (help with information). For each question the participant was instructed to respond with respect to each of seven social support sources (partner, other family members, friends, co-workers, health care, authorities and association/support groups). As for the assessment of coping, an almost identical version of this instrument has been used previously to study coping strategies and social support in CI (Nordin, Andersson, & Nordin, 2010).

32
Table 7. Problem- and emotion-focused statements about coping strategies
Problem-focused coping strategies
You ask others to explore the environment before you go to a place you suspect will affect your asthma and/or allergy. You seek information about asthma and/or allergies. You seek health care for you asthma and/or allergy. You avoid environments you know will affect your asthma and/or allergies.
Emotion-focused coping strategies
You try to accept your situation with asthma and/or allergies and make the best of it. You try to re-prioritize how important different things are to you.
You try not to think about your asthma/allergy. You make yourself feel better by eating, drinking or smoking.
Results and discussion
Mean ratings of usage of problem-focused or emotion-focused coping strategies are presented in Figure 9. Regarding coping strategies, no difference due to severity was found. In asthma/allergy the most used problem-focused strategies were avoiding environments that might affect one’s health and seek health care, and the most used emotion-focused strategies were accepting the situation and trying not to think about the illness.
Regarding avoiding environments that might affect one’s health, which was rated highest in the present study, previous studies have found that avoidance-oriented strategies can affect health in a negative way. This may result in more effective coping strategies not being used (Taylor & Stanton, 2007). Accepting the situation, which was the highest rated emotion-focused strategy, can be a much better way of handling the illness compared to avoiding environments, which can lead to isolation. However, other studies have found that usage of emotional coping strategies can decrease control of the illness and also decrease HRQoL (Barton, Clarke, Sulaiman, & Abramson, 2003; Hesselink et al., 2004).
For social support, differences were found between the three support types, which suggest that persons with asthma/allergy perceive more support regarding understanding than practical help and help with information. In general, the degree of emotional support varied from moderate to fairly high, whereas instrumental and informational support varied from fairly low to moderate. Most support was given from the partner, family members and health care, and least support was received from

support groups and authorities. In this study, authorities were not defined although considered to be referring to, for example, the social insurance which is a Swedish government agency that is responsible for large parts of the public welfare system. A difference was found in symptom exacerbation frequency, which can be referred to higher social support being perceived in those who reported low frequency asthma/allergy exacerbation in comparison to those with high frequency of exacerbation (see Figure 10). This could, on the one hand be a result of the social surrounding not being able and having stamina to maintain efficient support. On the other, the low exacerbation may also be a result of high support that is received from the surrounding.
Problem-focused coping
High Low0
2
4
6
Ask others to explore Seek information Seek healthcare Avoid environments
Emotion-focused coping
High Low
Deg
ree
of u
sage
of c
opin
g
0
2
4
6
Try to accept Re-prioritize Try not to think about Eat, drink and smoke
Figure 9. Mean (+SD) self-reported degree of usage of coping strategies, separate for problem- and emotion-focused in high (daily/weekly) and low (monthly) symptom exacerbation.
33

34
Deg
ree
of p
erce
ived
soc
ial s
uppo
rtUnderstanding
High Low0
2
4
6
33
Help with information
High Low0
2
4
6
Partner Family members Friends Co-workers Health care Authorites Support groups
Practical help
High Low0
2
4
6
Figure 10. Mean (+SD) self-reported degree of perceived social support for three support types and seven support sources in high (daily/weekly) and low (monthly) symptom frequency exacerbation.

35
General discussion
The general aim of this thesis was to examine different psychological aspects in common forms of asthma and allergy. The specific questions examined regarded comorbidity with environmental intolerance, psychological distress, and coping and social support, all which were examined in a group of participants with asthma and allergy participating in the VEHS. The four asthma and allergy diagnoses (i) allergic asthma, (ii) non-allergic asthma, (iii) allergic rhinitis and (iv) atopic dermatitis were chosen as they are the most common allergic and non-allergic illnesses.
In Study I and Study III a decision was made to combine the four asthma/allergy groups into one group. This was made predominantly to obtain sufficient statistical power. A second reason for this was based on previous findings of strong relationships between the four diagnoses (e.g. being risk factors for each other and showing high comorbidity). The reason for the groups being separated in Study II was based on the research question, as the aim was to study differences between single diagnoses of asthma and allergy as well as with a referent group.
Co- and multimorbidity between asthma and allergy and intolerances to chemicals and certain buildings
Clear relationship have been reported in previous studies between various forms of asthma/allergy (Akdis et al., 2006; Bjermer, 2007; Meltzer et al., 2004), various forms of EIs (Palmquist et al., 2014), and between asthma/allergy and EIs (Caress & Steinemann, 2004; Caress & Steinemann, 2009; Wang et al., 2008). The comorbidity with asthma/allergy and intolerance to chemicals and certain buildings is likely to negatively affect the immune system as it increases stress in the individual (McEwen, 1998), which may worsen health in general.
Study I showed that all possible overlaps between asthma/allergy, physician-diagnosed and self-reported CI and BI was larger than what was expected by chance, suggesting that a substantial part of those with asthma/allergy also have either physician-diagnosed or self-reported EI, either as a single or a multiple overlap. One possible reason for this overlap might be explained by the overlap in diagnostic criteria’s as the two forms of EI are not exclusive, and in this specific sample there are persons who meet the criteria for both forms, (see Table 2 for definitions of these criteria). However, use of both types of criteria, physician-diagnosed and self-reported, provides broader understanding and thus stronger support for EI being common in asthma and allergy.
Persons with allergy have been reported to be more sensitive than normal to sensory irritating stimuli (Elberling et al., 2005; Hodgson & Addorisio, 2005). This enhanced

36
sensitivity in allergic patients is believed to increase the reactions to other stimuli in the environment, leading to more frequent reporting of symptoms (Grivel & Candas, 1991). This may also lead persons with atopic illness to be prone to report symptoms at an earlier stage than non-atopic persons. This may in turn lead to over reporting of symptoms, even though the person may not actually react strongly. This increased sensitivity to irritants might affect them in negatively regarding everyday chemicals. Studies have reported that asthmatics frequently report feeling ill due to perfume and cleaning agents (Baldwin, Bell, & O'Rourke, 1999).
Although it is possible that those with both asthma/allergy and EI respond fairly well to traditional asthma/allergy treatment such as corticosteroids or antihistamines, the result of this study may suggest that they are attributing their symptoms to other sources such as everyday chemicals or that they have an increased sensitivity. Even though this could partly explain some of the overlap between asthma/allergy and the intolerance, it also questions whether the multiple diagnoses reflect the seriousness of the patient’s symptoms and actual problem and in what way it affects their psychological well-being. Moreover, the multiple overlap might be a sign of a knowledge gap regarding medically unexplained illnesses.
Psychological distress in asthma and allergy
Asthma and allergy are regarded as stressful factors that will increase the need for medical help and understanding from society. The illnesses can lead to decreased QoL which may have an overall negative effect on both the psyche and physical illness.
Previous studies have suggested an association between atopy and psychological distress (Chida et al., 2008; Rand et al., 2012), which the results found in Study II partly support. The results suggest that persons with allergic asthma and atopic dermatitis experience more stress, anxiety and burnout compared to non-allergic asthma, allergic rhinitis and non-asthma/allergy. The hypothesis of those with an atopic (IgE-mediated) asthma/allergy experiencing more distress was therefore not completely confirmed, as this was not found in allergic rhinitis. Although, some studies have previously reported that asthma is associated with depression (Chida et al., 2008; Wright et al., 2005), it may be the case that the association between depression and asthma is mediated by anxiety. Other studies have suggested the association between atopy and depression to be relatively weak. Thus, Slattery and Essex (2011) found no significant associations of depression with either asthma, allergic rhinitis, or atopic dermatitis, whereas associations were found for anxiety in asthma and allergic rhinitis, but not atopic dermatitis. Furthermore, they found that having both asthma and allergic rhinitis strengthened the association with anxiety compared to having either atopy alone. Others have reported that anxiety and depression are associated with asthma-related symptoms but not between with diagnosis of asthma (Janson, Björnsson, Hetta, & Boman, 1994). This finding is partly supported by the result in Study II, as the level of

37
depression was not found to be statistically higher in any of the two forms of asthma compared to the other diagnoses, although a tendency was found for allergic asthma. Whereas distress in other studies has been defined as a combination of anxiety and depression (Wright et al., 2005), others have defined this concept as anxiety, depression, stress-related personality and immature coping skills (Chida et al., 2008). We chose to combine various aspects that are related and that may affect each other.
Stress has been found to have a direct effect on the immune system, and short-term stress can lead to increased immune protection. However, when stress is prolonged the protection is lowered, and the risk of illness increases (McEwen, 1998). Others have suggested that stress due to chronic illness increases the risk for symptoms of anxiety and depression (Centanni et al., 2000). It is therefore not surprising that the three measures, which are strongly related, are all associated with atopy (except for allergic rhinitis in this case). It is perhaps surprising though that depression, which correlates highly with anxiety and may lead to reduced asthma control (Di Marco, Santus, & Centanni, 2011), could not be identified as being significantly associated with asthma/allergy. Furthermore, it has been suggested that asthma and rhinitis are the same illness, since the systemic nature of asthma is associated with rhinitis in term of epidemiology, pathology and immunology (Bjermer, 2007). Despite this, allergic rhinitis was not found to be significantly associated with distress. However, this result may suggest that depression is not as strongly related as anxiety in triggering the body’s defense system. Other studies have reported that among asthmatic patients a rather high prevalence have an undiagnosed psychiatric morbidity of depression (Heaney, Conway, Kelly, & Gamble, 2005). The results further suggest a tendency for increased worries for environmental pollution among asthmatics and allergics. This could be a result of environmental pollution being a factor that in general can increase the stress level due to worry affecting health (Brosschot et al., 2006).
PNI is of interest in the context of psychological aspects since it is somewhat of a common nominator of each of the three studies. Stress, anxiety and depression appears to play important roles in both asthma and allergy, but also in EI (Study I), various measures of distress were key output variables in Study II, and such measures are important determinants for coping and social support, which was the focus of Study III. Accordingly, the field of PNI provides substantial evidence for factors such as stress (Cohen et al., 2007), depression (Kiecolt-Glaser & Glaser, 2002), social support (Uchino, 2006) and negative emotions (Kiecolt-Glaser, McGuire, Robles, & Glaser, 2002) influencing both cellular and humoral indicators of immune status and function. It has been suggested that there is a potential negative loop, such that atopy may lead to psychological distress, which, in turn, may reinforce the atopy outcome (Chida et al., 2008).
Prolonged stress leads to repeated activation of the hypothalamic-pituitary-adrenocortical (HPA) axis and the sympathetic and adrenomedullary (SAM) system

38
which can result in increased risk of both physical and psychiatric disorders (McEwen, 1998). In illness, such as asthma and allergy, disturbed balance may be occurring in these systems. Di Marco and collaborators (2011) propose that stress may induce hyporesponsiveness of the HPA axis, resulting in reduced cortisol secretion in patients with asthma. An unbalance may lead to negative emotional responses to environmental stressors, which can disturb the regulation of the HPA axis and the SAM system, making it difficult to maintain normal homeostasis. The imbalance may lead other immune mediators to overreact and increase the risk of autoimmune and inflammatory disorders.
In a recent study by Tsiakiris, Neely, Lind and Nordin (2014) it was reported that psychiatric conditions and functional somatic syndromes increased from having a certain single atopy, to having a certain atopy, irrespective of additional atopies, to having multiple atopies. Based on these results, it is likely that these associations may also be found in psychological distress in which differences can be found, which should be of focus in future studies.
Coping and social support in asthma and allergy
Coping and social support has been found to have positive effects in chronic illness (S. Cohen et al., 2000; S Cohen & Wills, 1985). It has been suggested that appropriate coping strategies can help in asthma management whereas an inappropriate strategy may increase the risk for loss of control over the illness (Barton et al., 2003). Social support, on the other hand, has been reported to have positive effects on the health outcome as well as in the reduction of stress (Ell et al., 1992; Ford et al., 2006) whereas low or insufficient support has been associated with increased risk for hospital admission (Wainwright et al., 2007). Relatively high distress was found in allergic asthma and atopic dermatitis in Study II, and previous studies have reported that long-term distress may lead to immunological changes (Ader, Cohen, & Felten, 1995) which can result in decreased control and worsening of asthma/allergy.
The results in Study II showed no difference between those with high and low symptom frequency of asthma/allergy regarding usage of coping strategies. Previous studies have suggested that those with severe asthma use a greater number of coping strategies than those with mild and moderate asthma (Sexton et al., 1999). This difference in outcome may be explained by the difference definition of severity between studies and the fact that the present study did not have access to medical records. Sexton and colleagues (1999) used medical records as well as a specialist nurse to categorize the participants into the groups based on their anamnesis and medical examination. The categorization in the present study was based on the self-reported question of how frequent they had symptoms due to their illness as well as self-reported physician-diagnosis. The symptom frequency was regarded as one possible aspect of severity.

39
In Study III differences between the four asthma/allergy diagnoses were not examined due to the groups being too small for enough statistical power. Even though symptom exacerbation may be an aspect of severity, there may be a difference between the diagnoses that enables direct comparison. Thus, the difference between the symptom frequency of atopic dermatitis and asthma might not be comparable as an asthma exacerbation may very well be life-threatening even though not experienced every day. Atopic dermatitis may, on the other hand, occur daily and decrease QoL to a large extent (McKenna & Doward, 2008) by affecting aspects such as sleep quality, but not being life-threatening.
The identified variation between support types depend partly on support source and symptom frequency of asthma/allergy exacerbation. In general, moderate to fairly high support was perceived to be received from the partner, other family members, and the healthcare system; moderate support from friends and coworkers; fairly low to moderate support from authorities; and low support from patient associations/support groups. Moderate to fairly high social support was perceived among those with low symptom frequency of asthma/allergy exacerbation, and fairly low to moderate support among those with low symptom frequency. Previous studies of asthmatics have reported that the partner and family members are the foremost provider of social support, although they also report that those closest to them did not understand how it is to live with the illness (Clark & Nothwehr, 1997). This result is partly in line with what was found in the present study, as the main support source was found to be the partner and family members. A positive result in this study is that the persons with asthma and allergy experience that they get most support from health care, in addition to the family, which earlier was found not to be the case in MCS (Nordin et al., 2010). This may be explained by the fact that asthma/allergy is an illness that is more socially accepted, leading to more social support. The difference between the two studies might be due to asthma and allergy being accepted in the medical community (Bjermer, 2007; Daruna, 2012), whereas EI may be more dependent on the physician’s beliefs (Palmquist et al., 2014). At date, no general agreement exists in treatment of EI. Instead the afflicted persons are being sent around to different medical specialist in search for more knowledge, usually without being given help.
Studies have also suggested that stress increases when support is perceived not to be sufficient. Since social support buffers against stress (Cohen & Wills, 1985), there is reason to believe that the atopic mechanisms underlying allergic rhinitis and atopic dermatitis, as well as asthma, may be related to social support through mediation of stress, although, this was not studied in the present study.
Regarding social support in general, it has been suggested that women and men seek support from different sources (Aukett, Ritchie, & Mill, 1988; Shumaker & Hill, 1991). Further analysis on the same sample in Study III, with sex as a grouping variable, revealed no main effect of sex on social support. However, interactions were found

40
between sex and type of social support, and between sex and support sourc, where men reported more support in to way of understanding than help with information and practical help. Similar analysis for coping strategies was also performed, and the results suggest that sex differences are associated with type of strategy, such that women report more usage of emotion focused coping strategies in comparison to men, whereas no sex difference was found for problem-focused strategies. The two most used problem-focused strategies were avoiding environments and seeking health care, and the two most used emotion focused were accepting and trying not to think about it.
A metaperspective on the studies
As previously reported, several aspects brought up in this thesis are related to each other. Stress may be seen as a key aspect, which can have a negative effect on health by affecting both the immune system and psychological distress. To validate the studies, a factor analysis was performed with the variables used in Study II and Study III, see Table 11. An eigenvalue above one was used to identify the number of factors. For the analysis the principal axis functioning method was chosen with oblique rotation as the variables were found to correlate with each other. The variables for EI (Study I) were not included in the analysis, as they were rather seen as factors that will increase the level of distress (Study II) and affect the ability to perform and receive buffering support (Study III).
Table 11. Factor loadings for three major factors. The strongest factor loadings for each item is given in bold.
Factor 1 Factor 2 Factor 3
Anxiety 0.919 0.076 0.106 Stress 0.841 -0.045 0.072 Burnout 0.805 -0.038 -0.147 Depression 0.794 -0.023 -0.088 Informational1 0.039 0.909 -0.039 Practical1 -0.047 0.861 -0.101 Understanding1 -0.123 0.730 -0.073 Emotion-focused2 0.058 0.433 0.018 Problem-focused2 -0.039 0.226 0.138 Health worries -0.014 -0.050 0.796 1Social support, 2coping strategies
According to the factor analysis, the data consisted of three factors of which Factor 1 consisted of the variables used in Study II, except for the modern health worries variable, and Factor 2 consisted of the variables used in Study III, although problem-focused coping had a rather low loading (Table 11). According to the analysis, the third

41
factor consists of the modern health worries variable, suggesting that it may not be a valid variable within the concept of distress. This is also in accordance with the theoretical view, as worries and distress, per se may affect each other, but worries may be a result of distress rather than an aspect of distress.
The three studies in this thesis cover a substantial part of a psychobiosocial perspective on asthma and allergy, although more research is needed. In Figure 11 I have proposed a metaperspective on the studies that is further described with examples as follows. (1) Psychological distress and EI may affect each other such that distress increases the risk for developing EI and intensifies symptoms associated with EI, and EI may, due to poor QoL, increase the level of distress. (2) EI and asthma/allergy may have a mutual impact on severity due to shared symptomology. (3) Distress can negatively affect asthma and allergy outcome, supposedly due to strengthened defense reactions, resulting in symptoms. Asthma and allergy may increase distress (stress, anxiety and depression), which in the long run can lead to burnout, thus causing a negative loop. (4) EIs may have a general negative impact on the psychological buffer of coping strategies and social support due to the disbelief the afflicted individuals often experience, whereas high social support and efficient coping strategies may help persons with EI. (5) Sufficient psychological buffers may lead to increased control of the asthma/allergy, whereas insufficient buffers may lead to limited social contact with those they experience as non-supporting, with consequences for QoL, likely to lead to higher illness severity. (6) Psychological buffers may decrease distress (e.g. buffering hypothesis), whereas distress may increase use of coping strategies and seeking of social support. Overall, the relation between psychological distress and asthma/allergy can be described as being direct as well as being mediated by EI and a psychological buffer.

42
Psyc
holo
gica
l dist
ress
Psyc
holo
gica
l buf
fer
Env
ironm
enta
l in
tole
ranc
e
Ast
hma
and
alle
rgy
Stre
ss
Anx
iety
Dep
ress
ion
Burn
out
Hea
lth
wor
ries
Cop
ing
stra
tegi
es
Prob
lem
focu
sed
Em
otio
n fo
cuse
d
Soci
al su
ppor
tE
mot
iona
l
Inst
rum
enta
lIn
form
ativ
e
Che
mic
al in
tole
ranc
eBu
ildin
g in
tole
ranc
e
Stud
y I
Stud
y II
Stud
y II
I
Seve
rity
Self-
repo
rted
Phys
icia
n-di
agno
sed
(1)
(2)
(4)
(5)
(3)
(6)
Figu
re 1
1. T
heor
etic
al m
odel
of
the
met
aper
spec
tive
show
ing
the
rela
tions
hip
betw
een
the
thre
e st
udie
s on
asth
ma
and
alle
rgy

43
Strengths and limitations of the thesis
There are some strengths and limitations of the studies that need to be mentioned. The inhabitants in the county of Västerbotten in Northern Sweden have an age and sex distribution that is very similar to that of Sweden in general (Statistics Sweden 2014). Furthermore, the VEHS investigates a population-based sample that was stratified for both sex and age. These two aspects enhance the possibility of generalizing the results to asthmatics and allergics in the general Swedish population and to other similar populations. In 2009, Västerbotten, had 258 548 inhabitants (Statistic Sweden, 2014) which means that the population included in the study represents around only 2.8% of the Swedish population as a whole. This may somewhat limit the generalizability. One strength with this thesis is the fact that all three studies have been performed using the same sample in various combinations, which includes four of the most common forms of asthma and allergy. This further enhances the comparability between the three studies as they are studying the same population.
Among the randomly selected individuals, 40% volunteered to participate. This has may have consequences for the representativeness. Decreasing participation and low response rate is an ongoing issue in all areas of research worldwide (Groves, 2004), and some have suggested that the steady decrease in participation in studies is caused by our society being ”over surveyed” (Galea & Tracy, 2007). Other reasons may be the contradictory messages of scientific studies to the public that may increase the disbelief (Beilin & Puddey, 2006; Patrick, 2000). Although, it has been argued that participation rates ranging between 30% and 70% are associated with little bias (Galea & Tracy, 2007), two identical surveys with 36% and 61% respectively in response rate found few significant differences (Keeter, Miller, Kohut, Groves, & Presser, 2000).
Information on age and gender was available for those who declined participation in this study, and the largest proportion of non-responders was found among young men. Assuming that young men to a relatively similar degree are bothered by asthma and allergy, in comparison to other age groups, the data may have somewhat lower mean scores on some of the measures as well as prevalence of various illnesses than otherwise would have been the case. Previous studies have not found any consistent evidence with regard to study participation and age. The VEHS consisted of a large number of sections and questionnaire instruments in order to capture a large number of aspects of environmental health. This may be one limitation as usage of more extensive measurements which might have been more appropriate was not chosen due to a question of space.
For all three studies, one can assume that some participants may have reported a physician-diagnosis of asthma/allergy from which they are no longer is troubled by. Assuming that this is the case, it may, for example, for Study II suggests that the results

44
are somewhat conservative, supposing that those who are no longer affected would report similar to the referents.
One of the reasons for the low participation in responding to questions about social support may be due to the fact that some of the sources were not applicable to all participants, such as partner, coworkers and so on, as they might not be in a relationship or have a job or one that includes co-workers. It may also be a result of asthmatic and allergic persons purposely limiting their contact with those who they perceive as non-supporting (Clark & Nothwehr, 1997). Moreover, regarding coping strategies and social support, the participants were not asked how frequently they use each strategy or perceive them to function, or how they perceive the support to work. For example, there are no questions regarding usage of medicine as a way of handling the illness, though asthma and allergy are in most cases treated with medicine to enable the patients to handle their problems on daily basis. It has been reported that coping strategies may work differently between persons, although the stressor is the same (J. T. Ptacek, Smith, & Dodge, 1994). There is also a limitation in studying coping strategies as we do not know if they are using other types of coping strategies than those assessed, which is important to take into consideration in further research in an asthmatic and allergic population.
Other limitations regard the fact that the questions concerning coping strategies and social support have not been validated, although they are likely to have good face validity. However, this is not seen as an evident criterion for validity. Thus, certain caution should be taken when interpreting those results. Other limitations for both measures of coping strategies and social support are that they were primary developed to be used for in groups of patients with MCS. However, it was considered to be suitable for the participants of Study III, as there are similarities in diagnoses regarding symptomology and possible sources that elicit symptoms, although the support might be dependent on how accepted the illnesses are.
Another caution that is important to mention is the timing of the study. The questionnaire was sent out before the onset of the pollen season suggesting that some of the participants are answering questions about health when off allergy season which would result in under-reporting of experienced symptoms in accordance to their diagnosis. For example, allergic rhinitis and asthma is strongly bound to a season depending on what allergen the person is reacting towards (Henriksen, Sue-Chu, Lingaas Holmen, Langhammer, & Bjermer, 1999; Madonini et al., 1987) whereas persons with atopic dermatitis has been found to experience worsening of symptoms during the colder months (Vocks et al., 2001).

45
Implications
Previous research might already have acknowledged that persons with asthma and allergy have a decreased QoL yet there are important aspects to consider when studying the illnesses. The results from this thesis may have important clinical implications for diagnosing and working towards preventing asthma and allergy exacerbation and gaining more control over the illness. The aim of this thesis has been to explore asthma and allergy from different psychological perspectives which are assumed to have an effect on the illness. As asthma and allergy are commonly viewed from the biomedical perspective, and although it in its early history was believed to be purely psychosomatic there is reason to believe that looking at asthma and allergy from a psychological perspective can increase the understanding for the afflicted individual as well as for the illness in general. This thesis also aims at contributing to the literature as a broad view was taken with four of the most common asthma and allergy diagnoses. Although the results of this thesis need to be confirmed in future research, there are a number of implications to be mentioned.
Based on the findings in this thesis and on what previously has been reported one can conclude that asthmatic and allergic persons to a larger extent than non-asthmatic/allergics suffer from intolerance towards chemical emissions. This implies that there is a need in clinical severe cases to question what the patient is reacting towards and experiences to be sensitive to, as it may be that there are other allergens or chemicals which are not commonly thought of. With support from the data, there may be cases where the asthma/allergy patient has an overlapping CI but also BI, to which traditional medical treatment does not respond, even though he/she exhibits typical symptoms. Even though the study did not focus on the separate diagnoses of asthma and allergy, these results imply an increased risk in asthma and allergy in general, also with the high comorbidity between the asthma and allergy diagnoses in mind. The identified comorbidity is consistent with findings in previous studies.
Distress may be a factor which negatively affects individuals in general, leading to both a decrease in QoL and decreased financial and social safety as it may increase the likelihood for worsening of the illness. As previous studies have shown, stress is a factor that increases the risk of worsening of the illness due to immunological changes and increased symptoms. The results from this thesis suggest that those with allergic asthma and atopic dermatitis experience more stress, burnout and anxiety. The distress may be a cause of the illness as well as the source of illness outcome (Chida et al., 2008). Regarding Study I and medical treatment, the results from Study 2 may imply that there is an advantage in having a wide view when examining asthmatics/allergics also in cases where medication is helping, as there may be positive outcomes from stress reduction methods, for example mindfulness.
46
The fact that the comorbidity of intolerance towards chemicals and certain buildings was statistically larger than expected by chance implies that a substantial part of those with high distress have comorbid intolerance and asthma/allergy diagnosis as they are part of the same sample. This comorbidity is likely to cause decreased QoL since those with intolerance in a previous study have been reported to experience lack of understanding and respect from others, as well as being limited in participating in society, and being dependent on others (Söderholm et al., 2011). The usage of coping strategies helps in handling everyday situations. The strategies with highest rating of usage found for this thesis were seeking information and avoiding environments, which imply room for improvements as there may be need for more information from health care on strategies that can improve the overall health in illness. One example can be more active coping in the form of accepting or planning which has been found to have positive effects as it makes it part of everyday life but also increase the control over the illness. As there is a strong relationship between coping strategies and social support, which is believed to buffer against stress, it is likely that avoidance coping may lead to social isolation which in turn can lead to less opportunities for social support which may increase risk for illness.
Research has found improvements in comorbid asthma based on psychological interventions. The aim of using psychological techniques on asthma is to reduce negative emotions such as panic and fear, but also to improve QoL (Affleck et al., 2000; Hyland, Finnis, & Irvine, 1991). Ross and colleagues (Ross et al., 1999) reported that cognitive behavioral therapy (CBT) and asthma education in women with comorbid asthma and panic disorder had an improved, on morning peak-flow expiratory rate and on asthma-related QoL, although not sustained effect over time. This may function as an illustration of how treatment of comorbid conditions in asthma and allergy can be useful for these patients.
Studies have found beneficial effects on both asthma and allergy when using appropriate coping strategies. Since the appropriate strategy depends on the situation and it is important to develop different strategies in order to adapt to different situations. Social support on the other hand can be helpful when improving the set of coping strategies used as well as to help establish new ones. Support from others can help either in solving a problem that a stressor poses, or to comfort and help dealing with the emotions that the stressor elicits. The persons with asthma and allergy investigated in Study III can be considered as relative experienced regarding the illness as the mean duration of the illness is 20 years. Even though they are considered as experienced, it is likely that there is still room for improvements both in the way they seek support and how they cope with everyday life. Patients with asthma and allergy and their significant others can benefit from being informed about effective coping strategies and how to best give social support.

47
Future perspectives
The results from Study I emphasize that there is common ground in asthma/allergy and EI. Previous findings have shown that psychological interventions, such as CBT, have positive, although not permanent, effects on asthma with comorbid panic attacks (Ross et al., 1999). Similar results have been found by Steen and Binkley (1998) who in a pilot study reported that persons with MCS experienced improvement in symptoms when undergoing CBT .This motivates future research regarding this kind of psychological treatment in patients with these comorbidities. Thus, future studies should investigate the effects of CBT in persons with asthma/allergy who experience high levels of distress, and in particular in those with comorbid EI. These patients are likely to be particularly vulnerable as they may have difficulties controlling their illness.
Moreover, longitudinal studies are needed in which severe clinical cases of asthma/allergy are treated with mindfulness to investigate its effect on high levels of distress. Mindfulness may play a crucial role in how to handle and maintain health in severe cases. Other questions for longitudinal studies regard how different types of coping and social support affect stress and asthma/allergy severity,and whether coping and social support change due to seasonal changes in asthma/allergy.
Future studies should also aim at developing an asthma/allergy-specific questionnaire instrument for coping and social support. Up to date there are no, to my knowledge, such a specific instrument for this patient group. If one aims at measuring coping strategies, as was the case in Study III, measures need to be adapted to the specific population as the strategies should be adapted to the specific situations that persons with asthma and allergy experience. In addition, future large-scale studies are needed for investigating coping strategies and social support in different types of asthma/allergy as well longitudinal studies to understand differences over time.
Concluding remarks
Asthma and allergy are some of the most commonly occurring illnesses, and have been suggested to increase in prevalence. As there is no easily conducted treatment for these illnesses that can offer complete recovery, patients are left with pharmacological and mediational treatments to gain control or relief of their symptoms. It is important to consider the person as a whole, incorporating both body and mind by a holistic approach.
To summarize, the results from the studies in this thesis suggest that: 1. The overlap in prevalence between asthma/allergy diagnoses, intolerance to
odorous/irritating chemicals, and intolerance to certain buildings in the

48
general population is found to be larger than by chance, regarding both physician-diagnosed and self-reported chemical and building intolerance.
2. Persons with allergic asthma and atopic dermatitis show more perceived stress, burnout (mental and physical exhaustion), and anxiety than do persons with non-allergic asthma, allergic rhinitis, and without asthma/allergy.
3. Persons with asthma and allergy use the same type of coping strategies to cope with their illness, independent of illness severity. Most used problem and emotion focused strategies are avoiding environments and trying to accept, respectively.
4. More social support in asthma and allergy is perceived in the form of understanding than help with information and practical help. Most support is received from the partner, other family members and healthcare whereas least support is received from authorities and association/support groups. Persons with low severity of asthma/allergy report to perceive more support from the surrounding in comparison to those with high illness severity.

49
References Ader, R., Cohen, N., & Felten, D. (1995). Psychoneuroimmunology: interactions
between the nervous system and the immune system. Lancet, 345(8942), 99-103. doi: http://dx.doi.org/10.1016/S0140-6736(95)90066-7
Affleck, G., Apter, A., Tennen, H., Reisine, S., Barrows, E., Willard, A., . . . ZuWallack, R. (2000). Mood States Associated With Transitory Changes in Asthma Symptoms and Peak Expiratory Flow. Psychosomatic Medicine, 62(1), 61-68.
Akdis, C. A., Akdis, M., Bieber, T., Bindslev-Jensen, C., Boguniewicz, M., Eigenmann, P., . . . Immunology, P. C. G. (2006). Diagnosis and treatment of atopic dermatitis in children and adults: European Academy of Allergology and Clinical Immunology/American Academy of Allergy, Asthma and Immunology/PRACTALL Consensus Report. Allergy, 61(8), 969-987. doi: 10.1111/j.1398-9995.2006.01153.x
Andersson, M. J., Andersson, L., Bende, M., Millqvist, E., & Nordin, S. (2009). The idiopathic environmental intolerance symptom inventory: development, evaluation, and application. Journal of Occupational and Environmental Medicine, 51(7), 838-847. doi: 10.1097/JOM.0b013e3181a7f021
Aneshensel, C. S., Rutter, C. M., & Lachenbruch, P. A. (1991). Social Structure, Stress, and Mental Health: Competing Conceptual and Analytic Models. American Sociological Review, 56(2), 166-178. doi: 10.2307/2095777
Araujo, A. C., Ferraz, E., Borges Mde, C., Filho, J. T., & Vianna, E. O. (2007). Investigation of factors associated with difficult-to-control asthma. Journal Brasileiro de Pneumologia, 33(5), 495-501.
Aukett, R., Ritchie, J., & Mill, K. (1988). Gender differences in friendship patterns. Sex Roles, 19(1-2), 57-66. doi: 10.1007/BF00292464
Avila, L., Soto-Martínez, M. E., Soto-Quirós, M., & Celedón, J. C. (2005). Asthma, Current Wheezing, and Tobacco Use Among Adolescents and Young Adults in Costa Rica. Journal of Asthma, 42(7), 543-547. doi: 10.1080/02770900500214791
Bahadori, K., Doyle-Waters, M., Marra, C., Lynd, L., Alasaly, K., Swiston, J., & FitzGerald, J. M. (2009). Economic burden of asthma: a systematic review. BMC Pulmonary Medicine, 9(1), 24.
Baldwin, C. M., Bell, I. R., & O'Rourke, M. K. (1999). Odor sensitivity and respiratory complaint profiles in a community-based sample with asthma, hay fever, and chemical odor intolerance. Toxicology and Industrial Health, 15(3-4), 403-409. doi: 10.1177/074823379901500314
Barton, C., Clarke, D., Sulaiman, N., & Abramson, M. (2003). Coping as a mediator of psychosocial impediments to optimal management and control of asthma. Respiratory Medicine, 97(7), 747-761. doi: http://dx.doi.org/10.1016/S0954-6111(03)00029-5
Bateman, E. D., Hurd, S. S., Barnes, P. J., Bousquet, J., Drazen, J. M., FitzGerald, M., . . . Zar, H. J. (2008). Global strategy for asthma management and prevention:

50
GINA executive summary. European Respiratory Journal, 31(1), 143-178. doi: 10.1183/09031936.00138707
Baum, A., Revenson, T. A., & Singer, J. E. (2012). Hanbook of health psychology. New York: Psychology Press.
Beasley, R. (1998). Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. Lancet, 351(9111), 1225-1232. doi: http://dx.doi.org/10.1016/S0140-6736(97)07302-9
Beilin, L. J., & Puddey, I. B. (2006). Alcohol and Hypertension: An Update. Hypertension, 47(6), 1035-1038. doi: 10.1161/01.HYP.0000218586.21932.3c
Bell, I. R., Jasnoski, M. L., Kagan, J., & King, D. S. (1991). Depression and Allergies: Survey of a Nonclinical Population. Psychotherapy and Psychosomatics, 55(1), 24-31.
Berg, T., & Johansson, S. G. O. (1969). IgE Concentrations in Children with Atopic Diseases. International Archives of Allergy and Immunology, 36(3), 219-232.
Berg, N. D., Linneberg, A., Dirksen, A., & Elberling, J. (2008). Prevalence of self-reported symptoms and consequences related to inhalation of airborne chemicals in a Danish general population. International Archives of Occupupational and Environmental Health, 81(7), 881-887. doi: 10.1007/s00420-007-0282-0
Bjermer, L. (2007). Time for a paradigm shift in asthma treatment: From relieving bronchospasm to controlling systemic inflammation. Journal of Allergy and Clinical Immunology, 120(6), 1269-1275. doi: http://dx.doi.org/10.1016/j.jaci.2007.09.017
Bjorksten, B., Dumitrascu, D., Foucard, T., Khetsuriani, N., Khaitov, R., Leja, M., . . . Riikjarv, M. (1998). Prevalence of childhood asthma, rhinitis and eczema in Scandinavia and Eastern Europe. European Respiratory Journal, 12(2), 432-437.
Blanc, P. D., Trupin, L., Eisner, M., Earnest, G., P Katz, P., Israel, L., & Yelin, E. H. (2001). The work impact of asthma and rhinitis: Findings from a population-based survey. Journal of Clinical Epidemiology, 54(6), 610-618. doi: http://dx.doi.org/10.1016/S0895-4356(00)00349-8
Bousquet, Bullinger, Fayol, Marquis, Valentin, & Burtin. (1994). Assessment of quality of life in patients with perennial allergic rhinitis with the French version of the SF-36 Health Status Questionnaire. Journal of Allergy and Clinical Immunology, 94(2), 182-188. doi: 10.1053/ai.1994.v94.a54939
Bousquet, J., Duchateau, J., Pignat, J. C., Fayol, C., Marquis, P., Mariz, S., . . . Burtin, B. (1996). Improvement of quality of life by treatment with cetirizine in patients with perennial allergic rhinitis as determined by a French version of the SF-36 questionnaire. Journal of Allergy and Clinical Immunology, 98(2), 309-316. doi: http://dx.doi.org/10.1016/S0091-6749(96)70155-0
Braunstahl, G.-J. (2005). The unified immune system: Respiratory tract–nasobronchial interaction mechanisms in allergic airway disease. Journal of Allergy and Clinical Immunology, 115(1), 142-148. doi: http://dx.doi.org/10.1016/j.jaci.2004.10.041

51
Brooks, C., Pearce, N., & Douwes, J. (2013). The hygiene hypothesis in allergy and asthma: an update. Current Opinion in Allergy and Clinical Immunology, 13(1), 70-77 10.1097/ACI.1090b1013e32835ad32830d32832.
Brosschot, J. F., Gerin, W., & Thayer, J. F. (2006). The perseverative cognition hypothesis: A review of worry, prolonged stress-related physiological activation, and health. Journal of Psychosomatic Research, 60(2), 113-124. doi: http://dx.doi.org/10.1016/j.jpsychores.2005.06.074
Brożek, J. L., Bousquet, J., Baena-Cagnani, C. E., Bonini, S., Canonica, G. W., Casale, T. B., . . . Schünemann, H. J. (2010). Allergic Rhinitis and its Impact on Asthma (ARIA) guidelines: 2010 Revision. Journal of Allergy and Clinical Immunology, 126(3), 466-476. doi: http://dx.doi.org/10.1016/j.jaci.2010.06.047
Caress, S., & Steinemann, A. (2004). Prevalence of Multiple Chemical Sensitivities: A Population-Based Study in the Southeastern United States. American Journal of Public Health, 94(5), 746-747.
Caress, S., & Steinemann, A. (2009). Asthma and chemical hypersensitivity: prevalence, etiology, and age of onset. Toxicology and Industrial Health, 25(1), 71-78. doi: 10.1177/0748233709102713
Carlsson, F., Karlson, B., Ørbæk, P., Österberg, K., & Östergren, P. O. (2005). Prevalence of annoyance attributed to electrical equipment and smells in a Swedish population, and relationship with subjective health and daily functioning. Public Health, 119(7), 568-577. doi: http://dx.doi.org/10.1016/j.puhe.2004.07.011
Centanni, S., Di Marco, F., Castagna, F., Boveri, B., Casanova, F., & Piazzini, A. (2000). Psychological issues in the treatment of asthmatic patients. Respiratory Medicine, 94(8), 742-749. doi: http://dx.doi.org/10.1053/rmed.1999.0766
Chida, Y., Hamer, M., & Steptoe, A. (2008). A Bidirectional Relationship Between Psychosocial Factors and Atopic Disorders: A Systematic Review and Meta-Analysis. Psychosomatic Medicine, 70(1), 102-116 110.1097/PSY.1090b1013e31815c31811b31871.
Claeson, A.-S., Palmquist, E., Lind, N., & Nordin, S. (2014). Symptom-trigger factors other than allergens in asthma and allergy [Manuscript].
Clark, N. M., & Nothwehr, F. (1997). Self-management of asthma by adult patients. Patient Education and Counseling, 32, Supplement 1(0), S5-S20. doi: http://dx.doi.org/10.1016/S0738-3991(97)00092-X
Cobb, S. (1976). Social Support as a Moderator of Life Stress. Psychosomatic Medicine, 38(5), 300-314.
Coca, A. F., & Cooke, R. A. (1923). On the Classification of the Phenomena of Hypersensitiveness. The Journal of Immunology, 8(3), 163-182.
Cohen, S., Gottlieb, B. H., & Underwood, L. G. (2000). Social Relationships and Health (N. Cohen, L. G. Underwood & B. H. Gottlieb Eds.): Oxford University Press.
Cohen, S., Janicki-Deverts, D., & Miller, G. E. (2007). PSychological stress and disease. JAMA, 298(14), 1685-1687. doi: 10.1001/jama.298.14.1685

52
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A Global Measure of Perceived Stress. Journal of Health and Social Behavior, 24(4), 385-396. doi: 10.2307/2136404
Cohen, S., & Wills, T. A. (1985). Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98(2), 310-357. doi: 10.1037/0033-2909.98.2.310
Cutrona, C. E., & Russell, D. W. (1990). Type of social support and specific stress: Toward a theory of optimal matching. In B. R. Sarason, I. G. Sarason & G. R. Pierce (Eds.), Social support: An interactional view (pp. 319-366). Oxford, England: John Wiley & Sons.
Dakof, G. A., & Taylor, S. E. (1990). Victims' perceptions of social support: What is helpful from whom? Journal of Personality and Social Psychology, 58(1), 80-89. doi: 10.1037/0022-3514.58.1.80
Daniel, W. W. (1995). Biostatistics : a foundation for analysis in the health sciences. New York [etc.]: Wiley.
Daruna, J. H. (2012). Introduction to Psychoneuroimmunology: Academic Press. De Vries, M. P., van Den Bemt, L., Lince, S., Muris, J. W. M., Thoonen, B. P. A., & van
Schayck, C. P. (2005). Factors Associated with Asthma Control. Journal of Asthma, 42(8), 659-665. doi: 10.1080/02770900500264903
Di Marco, F., Santus, P., & Centanni, S. (2011). Anxiety and depression in asthma. Current Opinion in Pulmonary Medicine, 17(1), 39-44.
Douwes, J., Brooks, C., van Dalen, C., & Pearce, N. (2011). Importance of Allergy in Asthma: An Epidemiologic Perspective. Current Allergy and Asthma Reports, 11(5), 434-444. doi: 10.1007/s11882-011-0215-6
Durham, S. R., Till, S. J., & Corrigan, C. J. (2000). T lymphocytes in asthma: Bronchial versus peripheral responses. Journal of Allergy and Clinical Immunology, 106(5, Supplement), S221-S226. doi: http://dx.doi.org/10.1067/mai.2000.110154
Dykewicz, M. S., & Hamilos, D. L. (2010). Rhinitis and sinusitis. Journal of Allergy and Clinical Immunology, 125(2, Supplement 2), S103-S115. doi: http://dx.doi.org/10.1016/j.jaci.2009.12.989
Edvardsson, B., Stenberg, B., Bergdahl, J., Eriksson, N., Lindén, G., & Widman, L. (2008). Medical and social prognoses of non-specific building-related symptoms (Sick Building Syndrome): a follow-up study of patients previously referred to hospital. International Archives of Occupational and Environmental Health, 81(7), 805-812. doi: 10.1007/s00420-007-0267-z
Ekerljung, L., Andersson, Å., Sundblad, B. M., Rönmark, E., Larsson, K., Ahlstedt, S., . . . Lundbäck, B. (2010). Has the increase in the prevalence of asthma and respiratory symptoms reached a plateau in Stockholm, Sweden? The International Journal of Tuberculosis and Lung Disease, 14(6), 764-771.
Elberling, J., Linneberg, A., Dirksen, A., Johansen, J. D., Frølund, L., Madsen, F., . . . Mosbech, H. (2005). Mucosal symptoms elicited by fragrance products in a population-based sample in relation to atopy and bronchial hyper-reactivity. Clinical and Experimental Allergy, 35(1), 75-81. doi: 10.1111/j.1365-2222.2005.02138.x

53
Ell, K., Nishimoto, R., Mediansky, L., Mantell, J., & Hamovitch, M. (1992). Social relations, social support and survival among patients with cancer. Journal of Psychosomatic Research, 36(6), 531-541. doi: http://dx.doi.org/10.1016/0022-3999(92)90038-4
Eriksson, N. M., & Stenberg, B. G. T. (2006). Baseline prevalence of symptoms related to indoor environment. Scandinavian Journal of Public Health, 34(4), 387-396. doi: 10.1080/14034940500228281
Fitzpatrick, M. F., Engleman, H., Whyte, K. F., Deary, I. J., Shapiro, C. M., & Douglas, N. J. (1991). Morbidity in nocturnal asthma: sleep quality and daytime cognitive performance. Thorax, 46(8), 569-573. doi: 10.1136/thx.46.8.569
Ford, E. S., Loucks, E. B., & Berkman, L. F. (2006). Social Integration and Concentrations of C-Reactive Protein Among US Adults. Annals of Epidemiology, 16(2), 78-84. doi: http://dx.doi.org/10.1016/j.annepidem.2005.08.005
Frey, C., & Röthlisberger, C. (1996). Social support in healthy adolescents. Journal of Youth and Adolescence, 25(1), 17-31. doi: 10.1007/BF01537378
Galea, S., & Tracy, M. (2007). Participation Rates in Epidemiologic Studies. Annals of Epidemiology, 17(9), 643-653. doi: http://dx.doi.org/10.1016/j.annepidem.2007.03.013
Ghosh, S., Pahwa, P., Rennie, D. C., & Janzen, B. (2009). Gender-Related Interactive Effect of Smoking and Rural/Urban Living on Asthma Prevalence: A Longitudinal Canadian NPHS Study. Journal of Asthma, 46(10), 988-994. doi: 10.3109/02770900903301278
Global Initiative for Asthma. (2014). Global Strategy for Asthma Management and Prevention. Retrieved from www.ginasthma.org. [Accessed December 4, 2014].
Goodwin, R. D., & Eaton, W. W. (2003). Asthma and the risk of panic attacks among adults in the community. Psychological Medicine, 33(05), 879-885. doi: doi:10.1017/S0033291703007633
Goodwin, R. D., Pine, D. S., & Hoven, C. W. (2003). Asthma and Panic Attacks Among Youth in the Community. Journal of Asthma, 40(2), 139.
Goral, A., Lipsitz, J. D., Muhsen, K., & Gross, R. (2012). Depressive symptoms, risk factors and sleep in asthma: results from a national Israeli health survey. General Hospital Psychiatry, 34(1), 17-23. doi: http://dx.doi.org/10.1016/j.genhosppsych.2011.09.007
Graham, J. W. (2008). Missing Data Analysis: Making It Work in the Real World. Annual Review of Psychology, 60(1), 549-576. doi: 10.1146/annurev.psych.58.110405.085530
Grivel, F., & Candas, V. (1991). Ambient temperatures preferred by young European males and females at rest. Ergonomics, 34(3), 365-378. doi: 10.1080/00140139108967320
Groves, R. M. (2004). Survey errors and survey costs. Hoboken (NJ): John Wiley & Sons. Gupta, D., Aggarwal, A. N., Chaudhry, K., Chhabra, S., D'Souza, G., Jindal, S., . . .
Vijayan, V. K. (2005). Household environmental tobacco smoke exposure,

54
respiratory symptoms and asthma in non-smoker adults: a multicentric population study from India. The Indian Journal of Chest Diseases and Allied Sciences, 48(1), 31-36.
Hanifin, J. M., & Rajka, G. (1980). Diagnostic Features of Atopic Dermatitis. Acta Dermatol Venereolgica, 60(92), 44-47.
Hashizume, H., & Takigawa, M. (2006). Anxiety in allergy and atopic dermatitis. Current Opinion in Allergy and Clinical Immunology, 6(5), 335-339.
Hastert, T. A., Babey, S. H., Brown, E. R., & Meng, Y.-Y. (2007). Pets and Smoking in the Home Associated with Asthma Symptoms and Asthma-Like Breathing Problems. UCLA Center for Health Policy Research.1-8.
Hausteiner, C., Bornschein, S., Zilker, T., Henningsen, P., & Förstl, H. (2007). Dysfunctional cognitions in idiopathic environmental intolerances (IEI)—An integrative psychiatric perspective. Toxicology Letters, 171(1–2), 1-9. doi: http://dx.doi.org/10.1016/j.toxlet.2007.04.010
Heaney, L. G., Conway, E., Kelly, C., & Gamble, J. (2005). Prevalence of psychiatric morbidity in a difficult asthma population: Relationship to asthma outcome. Respiratory Medicine, 99(9), 1152-1159. doi: http://dx.doi.org/10.1016/j.rmed.2005.02.013
Heaney, L. G., & Horne, R. (2012). Non-adherence in difficult asthma: time to take it seriously. Thorax, 67(3), 268-270. doi: 10.1136/thoraxjnl-2011-200257
Hellgren, J., Cervin, A., Nordling, S., Bergman, A., & Cardell, L. O. (2010). Allergic rhinitis and the common cold – high cost to society. Allergy, 65(6), 776-783. doi: 10.1111/j.1398-9995.2009.02269.x
Henningsen, P., & Priebe, S. (2003). New Environmental Illnesses: What Are Their Characteristics? Psychotherapy and Psychosomatics, 72(5), 231-234.
Henriksen, A. h., Sue-Chu, M., Lingaas Holmen, T., Langhammer, A., & Bjermer, L. (1999). Exhaled and nasal NO levels in allergic rhinitis: relation to sensitization, pollen season and bronchial hyperresponsiveness. European Respiratory Journal, 13(2), 301-306. doi: 10.1034/j.1399-3003.1999.13b14.x
Hesselink, A. E., Penninx, B. W. J. H., van der Windt, D. A. W. M., van Duin, B. J., de Vries, P., Twisk, J. W. R., . . . van Eijk, J. T. M. (2004). Effectiveness of an education programme by a general practice assistant for asthma and COPD patients: results from a randomised controlled trial. Patient Education and Counseling, 55(1), 121-128. doi: http://dx.doi.org/10.1016/j.pec.2003.08.007
Hillert, L., Berglind, N., Arnetz, B. B., & Bellander, T. (2002). Prevalence of self-reported hypersensitivity to electric or magnetic fields in a population-based questionnaire survey. Scandinavian Journal of Work, Environment and Health, 28(1), 33-41.
Hodgson, M. J., & Addorisio, M. R. (2005). Chapter 50 - Exposures in Indoor Environments. In L. Redlich, M. R. Rosenstock, C. A. Cullen, C. A. Brodkin & C. A. Redlich (Eds.), Textbook of Clinical Occupational and Environmental Medicine (2nd ed., pp. 1133-1142). Edinburgh: W.B. Saunders.

55
Hojo, S., Ishikawa, S., Kumano, H., Miyata, M., & Sakabe, K. (2008). Clinical characteristics of physician-diagnosed patients with multiple chemical sensitivity in Japan. International Journal of Hygiene and Environmental Health, 211(5–6), 682-689. doi: http://dx.doi.org/10.1016/j.ijheh.2007.09.007
Holgate, S. T. (2011). Pathophysiology of asthma: What has our current understanding taught us about new therapeutic approaches? Journal of Allergy and Clinical Immunology, 128(3), 495-505. doi: http://dx.doi.org/10.1016/j.jaci.2011.06.052
Hyland, M. E., Finnis, S., & Irvine, S. H. (1991). A scale for assessing quality of life in adult asthma sufferers. Journal of Psychosomatic Research, 35(1), 99-110. doi: http://dx.doi.org/10.1016/0022-3999(91)90011-C
Ishizaka, K., Ishizaka, T., & Menzel, A. E. O. (1967). Physicochemical Properties of Reaginic Antibody: VI. Effect of Heat on γE-, γG- and γA-Antibodies in the Sera of Ragweed Sensitive Patients. The Journal of Immunology, 99(3), 610-618.
Jackson, M. (2009). Asthma: the biography: Oxford University Press. Janson, C., Anto, J., Burney, P., Chinn, S., de Marco, R., Heinrich, J., . . . II, o. b. o. t. E.
C. R. H. S. (2001). The European Community Respiratory Health Survey: what are the main results so far? European Respiratory Journal, 18(3), 598-611.
Janson, C., Björnsson, E., Hetta, J., & Boman, G. (1994). Anxiety and depression in relation to respiratory symptoms and asthma. American Journal of Respiratory and Critical Care Medicine, 149(4), 930-934. doi: 10.1164/ajrccm.149.4.8143058
Johansson, A. k., Millqvist, E., Nordin, S., & Bende, M. (2006). Relationship between self-reported odor intolerance and sensitivity to inhaled capsaicin*: Proposed definition of airway sensory hyperreactivity and estimation of its prevalence. Chest, 129(6), 1623-1628. doi: 10.1378/chest.129.6.1623
Johansson, Å., Brämerson, A., Millqvist, E., Nordin, S., & Bende, M. (2005). Prevalence and risk factors for self-reported odour intolerance: the Skövde population-based study. International Archives of Occupational and Environmental Health, 78(7), 559-564. doi: 10.1007/s00420-005-0616-8
Juniper, E. F. (1997). Quality of life in adults and children with asthma and rhinitis. Allergy, 52(10), 971-977. doi: 10.1111/j.1398-9995.1997.tb02416.x
Karasek, R. A., & Theorell, T. (1990). Healthy work. New York: Basic Books. Keeter, S., Miller, C., Kohut, A., Groves, R., M., & Presser, S. (2000). Consequences of
Reducing Nonresponse in a National Telephone Survey. Public Opinion Quarterly, 64(2), 125-148. doi: 10.1086/317759
Kiecolt-Glaser, J. K., & Glaser, R. (2002). Depression and immune function: Central pathways to morbidity and mortality. Journal of Psychosomatic Research, 53(4), 873-876. doi: http://dx.doi.org/10.1016/S0022-3999(02)00309-4
Kiecolt-Glaser, J. K., McGuire, L., Robles, T. F., & Glaser, R. (2002). Psychoneuroimmunology: Psychological influences on immune function and health. Journal of Consulting and Clinical Psychology, 70(3), 537-547. doi: 10.1037/0022-006X.70.3.537

56
Kreutzer, R., Neutra, R. R., & Lashuay, N. (1999). Prevalence of People Reporting Sensitivities to Chemicals in a Population based Survey. American Journal of Epidemiology, 150(1), 1-12.
Lekander, M. (2008). Stress och allergi. Allergi i praxis, 3, 30-36. Lakey, B., & Cohen, S. (2000). Social support theory and measurement. In S. Cohen, L.
G. Underwood & B. H. Gottlieb (Eds.), Social support measurement and intervention: A guid for health and social scientist. (pp. 29-52). Oxford University Press.
Larsen, F. S., & Hanifin, J. M. (2002). Epidemiology of atopic dermatitis. Immunology and Allergy Clinics of North America, 22(1).
Lazarus, R. S., & Folkman, S. (1984). Stress, Appraisal and Coping. New York: Springer Publishing Company LLC.
Lee, P., & Mace, S. (2009). An approach to allergic rhinitis. Allergy Rounds, 1. Leynaert, B., Bousquet, J., Neukirch, C., Liard, R., & Neukirch, F. (1999). Perennial
rhinitis: An independent risk factor for asthma in nonatopic subjects: Results from the European Community Respiratory Health Survey. Journal of Allergy and Clinical Immunology, 104(2), 301-304. doi: http://dx.doi.org/10.1016/S0091-6749(99)70370-2
Leynaert, B., Neukirch, C., Liard, R., Bousquet, J., & Neukirch, F. (2000). Quality of Life in Allergic Rhinitis and Asthma. American Journal of Respiratory and Critical Care Medicine, 162(4), 1391-1396. doi: 10.1164/ajrccm.162.4.9912033
Loerbroks, A., Apfelbacher, C. J., Bosch, J. A., & Sturmer, T. (2010). Depressive symptoms, social support, and risk of adult asthma in a population-based cohort study. Psychosomatic Medicine, 72(3), 309-315. doi: 10.1097/PSY.0b013e3181d2f0f1
Lotvall, J., Ekerljung, L., Ronmark, E., Wennergren, G., Linden, A., Ronmark, E., . . . Lundback, B. (2009). West Sweden Asthma Study: Prevalence trends over the last 18 years argues no recent increase in asthma. Respiratory Research, 10(1), 94.
Madonini, E., Briatico-Vangosa, G., Pappacoda, A., Maccagni, G., Cardani, A., & Saporiti, F. (1987). Seasonal increase of bronchial reactivity in allergic rhinitis. Journal of Allergy and Clinical Immunology, 79(2), 358-363. doi: http://dx.doi.org/10.1016/0091-6749(87)90156-4
Marshall, P. S., & Colon, E. A. (1993). Effects of allergy season on mood and cognitive function. Ann Allergy, 71(3), 251-258.
Masters, K., Stillman, A., & Spielmans, G. (2007). Specificity of Social Support for Back Pain Patients: Do Patients Care Who Provides What? Journal of Behavioral Medicine, 30(1), 11-20. doi: 10.1007/s10865-006-9078-z
McEwen, B. S. (1998). Stress, Adaptation, and Disease: Allostasis and Allostatic Load. Annals of the New York Academy of Sciences, 840(1), 33-44. doi: 10.1111/j.1749-6632.1998.tb09546.x
McKenna, S. P., & Doward, L. C. (2008). Quality of life of children with atopic dermatitis and their families. Current Opinion in Allergy and Clinical Immunology, 8(3), 228-231. doi: 10.1097/ACI.0b013e3282ffd6cc

57
Meggs, W. J., & Dunn, K. A. (1996). Prevalence and nature of allergy and chemical sensitivity in a general population. Archives of Environmental Health, 51(4), 275.
Melamed, S., Kushnir, T., & Shirom, A. (1992). Burnout and Risk Factors for Cardiovascular Diseases. Behavioral Medicine, 18(2), 53-60. doi: 10.1080/08964289.1992.9935172
Meltzer, E. O., Nathan, R. A., Seiner, J. C., & Storms, W. (1997). Quality of life and rhinitic symptoms: Results of a nationwide survey with the SF-36 and RQLQ questionnaires. Journal of Allergy and Clinical Immunology, 99(6, Part 2), S815-S819. doi: http://dx.doi.org/10.1016/S0091-6749(97)80041-3
Meltzer, E. O., Szwarcberg, J., & Pill, M. W. (2004). Allergic rhinitis, asthma, and rhinosinusitis: diseases of the integrated airway. Journal of Managed Care Pharmacy, 10(4), 310-317.
Menzies, D., & Bourbeau, J. (1997). Building-Related Illnesses. New England Journal of Medicine, 337(21), 1524-1531. doi: doi:10.1056/NEJM199711203372107
Millqvist, E. (2008). Mechanisms of increased airway sensitivity to occupational chemicals and odors. Current Opinion in Allergy and Clinical Immunology, 8(2), 135-139. doi: 10.1097/ACI.0b013e3282f647ec
Mitschenko, A. V., Lwow, A. N., Kupfer, J., Niemeier, V., & Gieler, U. (2008). Neurodermitis und Stress. Der Hautarzt, 59(4), 314-318. doi: 10.1007/s00105-008-1525-z
Mösges, R., & Klimek, L. (2007). Today’s allergic rhinitis patients are different: new factors that may play a role. Allergy, 62(9), 969-975. doi: 10.1111/j.1398-9995.2007.01440.x
Naing, L., Winn, T., & Rusli, B. N. (2006). Practical issues in calculating the sample size for prevalence studies. Archives of orofacial science, 1(1), 9-14.
Nihlén, U., Greiff, L., Montnémery, P., Löfdahl, C. G., Johannisson, A., Persson, C., & Andersson, M. (2006). Incidence and remission of self-reported allergic rhinitis symptoms in adults. Allergy, 61(11), 1299-1304. doi: 10.1111/j.1398-9995.2006.01166.x
Nolen-Hoeksema, S. (2001). Gender Differences in Depression. Current Directions in Psychological Science, 10(5), 173-176. doi: 10.1111/1467-8721.00142
Nordin, M., Andersson, L., & Nordin, S. (2010). Coping strategies, social support and responsibility in chemical intolerance. Journal of Clinical Nursing, 19(15-16), 2162-2173. doi: 10.1111/j.1365-2702.2010.03264.x
Nordin, S. (2012). Individfaktorers betydelse för ospecifik byggnadsrelaterad ohälsa. Paper presented at the Inomhusklimat Universitetssjukhuset Örebro.
Palmquist, E., Claeson, A.-S., Neely, G., Stenberg, B., & Nordin, S. (2014). Overlap in prevalence between various types of environmental intolerance. International Journal of Hygiene and Environmental Health, 217(4–5), 427-434. doi: http://dx.doi.org/10.1016/j.ijheh.2013.08.005
Park, J., & Knudson, S. (2007). Medically unexplained physical symptoms. Health Reports, 18(1), 43-47.

58
Patrick, L. (2000). Beta-carotene: the controversy continues. Alternative medicine review : a journal of clinical therapeutic, 5(6), 530-545.
Petrie, K. J., Sivertsen, B., Hysing, M., Broadbent, E., Moss-Morris, R., Eriksen, H. R., & Ursin, H. (2001). Thoroughly modern worries: The relationship of worries about modernity to reported symptoms, health and medical care utilization. Journal of Psychosomatic Research, 51(1), 395-401. doi: http://dx.doi.org/10.1016/S0022-3999(01)00219-7
Ptacek, J. T., Smith, R. E., & Dodge, K. L. (1994). Gender Differences in Coping with Stress: When Stressor and Appraisals Do Not Differ. Personality and Social Psychology Bulletin, 20(4), 421-430. doi: 10.1177/0146167294204009
Ptacek, R., Stefano, G. B., Kuzelova, H., Raboch, J., Harsa, P., & Kream, R. M. (2013). Burnout syndrome in medical professionals: a manifestation of chronic stress with counterintuitive passive characteristics. Neuro-Endocrinology Letters, 34(4), 259-264.
Rand, C. S., Wright, R. J., Cabana, M. D., Foggs, M. B., Halterman, J. S., Olson, L., . . . Taggart, V. (2012). Mediators of asthma outcomes. Journal of Allergy and Clinical Immunology, 129(3, Supplement), S136-S141. doi: http://dx.doi.org/10.1016/j.jaci.2011.12.987
Reddel, H. K., Taylor, D. R., Bateman, E. D., Boulet, L.-P., Boushey, H. A., Busse, W. W., . . . Wenzel, S. E. (2009). An Official American Thoracic Society/European Respiratory Society Statement: Asthma Control and Exacerbations. American Journal of Respiratory and Critical Care Medicine, 180(1), 59-99. doi: 10.1164/rccm.200801-060ST
Romanet-Manent, S., Charpin, D., Magnan, A., Lanteaume, A., Vervloet, D., & and the, E. C. G. (2002). Allergic vs nonallergic asthma: what makes the difference? Allergy, 57(7), 607-613. doi: 10.1034/j.1398-9995.2002.23504.x
Rosner, F. (1997). The Medical Legacy of Moses Maimonides. Ktav Pub Inc. Ross, S., Grant, A., Counsell, C., Gillespie, W., Russell, I., & Prescott, R. (1999).
Barriers to Participation in Randomised Controlled Trials: A Systematic Review. Journal of Clinical Epidemiology, 52(12), 1143-1156. doi: http://dx.doi.org/10.1016/S0895-4356(99)00141-9
Rusli, B., Edimansyah, B., & Naing, L. (2008). Working conditions, self-perceived stress, anxiety, depression and quality of life: A structural equation modelling approach. BMC Public Health, 8(1), 48.
Rönmark, E. P., Ekerljung, L., Lötvall, J., Wennergren, G., Rönmark, E., Torén, K., & Lundbäck, B. (2012). Eczema among adults: prevalence, risk factors and relation to airway diseases. Results from a large-scale population survey in Sweden. British Journal of Dermatology, 166(6), 1301-1308. doi: 10.1111/j.1365-2133.2012.10904.x
Schafer, J. L., & Graham, J. W. (2002). Missing data: Our view of the state of the art. Psychological Methods, 7(2), 147-177. doi: 10.1037/1082-989X.7.2.147

59
Schaufeli, W. B., & Greenglass, E. R. (2001). Introduction to special issue on burnout and health. Psychology and Health, 16(5), 501-510. doi: 10.1080/08870440108405523
Schmaus, B. J., Laubmeier, K. K., Boquiren, V. M., Herzer, M., & Zakowski, S. G. (2008). Gender and stress: Differential psychophysiological reactivity to stress reexposure in the laboratory. International Journal of Psychophysiology, 69(2), 101-106. doi: http://dx.doi.org/10.1016/j.ijpsycho.2008.03.006
Schreurs, K. M. G., & de Ridder, D. T. D. (1997). Integration of coping and social support perspectives: Implications for the study of adaptation to chronic diseases. Clinical Psychology Review, 17(1), 89-112. doi: http://dx.doi.org/10.1016/S0272-7358(96)00050-5
Sexton, D. L., Calcasola, S. L., Bottomley, S. R., & Funk, M. (1999). Adults' experience with asthma and their reported uncertainty and coping strategies. Clinical Nurse Specialist, 13(1), 8-14.
Shumaker, S. A., & Hill, D. R. (1991). Gender differences in social support and physical health. Health Psychology, 10(2), 102-111. doi: 10.1037/0278-6133.10.2.102
Sinharay, S., Stern, H. S., & Russell, D. (2001). The use of multiple imputation for the analysis of missing data. Psychological Methods, 6(4), 317-329. doi: 10.1037/1082-989X.6.4.317
Skoner, D. P. (2001). Allergic rhinitis: Definition, epidemiology, pathophysiology, detection, and diagnosis. Journal of Allergy and Clinical Immunology, 108(1, Supplement), S2-S8. doi: http://dx.doi.org/10.1067/mai.2001.115569
Slattery, M. J., & Essex, M. J. (2011). Specificity in the Association of Anxiety, Depression, and Atopic Disorders in a Community Sample of Adolescents. Journal of psychiatric research, 45(6), 788-795. doi: 10.1016/j.jpsychires.2010.11.003
Small, P., & Kim, H. (2011). Allergic rhinitis. Allergy, Asthma and Clinical Immunology, 7(Suppl 1), S3.
Snyder, C. R. (1999). Coping: The psychology of what works: Oxford University Press. Stanworth, D. R., Humphrey, J. H., Bennich, H., & Johansson, S. G. O. (1967). Specific
inhibition of the prausnitzküstner reaction by an atypical human myeloma protein. Lancet, 290(7511), 330-332. doi: http://dx.doi.org/10.1016/S0140-6736(67)90171-7
Statistic Sweden. (2014). Population by sex, age, marital status by county Dec. 31, 2009 according to the administrative subdivisions of January 1, 2010. Retreived from:http://www.scb.se/statistik/_publikationer/BE0101_2009A01_BR_BE0110TAB.pdf. [Accessed December 1, 2014].
Stenn, P., & Binkley, K. (1998). Successful Outcome in a Patient With Chemical Sensitivity: Treatment With Psychological Desensitization and Selective Serotonin Reuptake Inhibitor. Psychosomatics, 39(6), 547-550. doi: http://dx.doi.org/10.1016/S0033-3182(98)71289-7

60
Subbarao, P., Mandhane, P. J., & Sears, M. R. (2009). Asthma: epidemiology, etiology and risk factors. CMAJ : Canadian Medical Association Journal, 181(9), E181-E190. doi: 10.1503/cmaj.080612
Söderholm, A., Söderberg, A., & Nordin, S. (2011). The Experience of Living With Sensory Hyperreactivity—Accessibility, Financial Security, and Social Relationships. Health Care for Women International, 32(8), 686-707. doi: 10.1080/07399332.2011.585727
Taylor, S. E., & Stanton, A. L. (2007). Coping Resources, Coping Processes, and Mental Health. Annual Review of Clinical Psychology, 3(1), 377-401. doi: 10.1146/annurev.clinpsy.3.022806.091520
Thomsen, S. F., Duffy, D. L., Kyvik, K. O., & Backer, V. (2010). Genetic influence on the age at onset of asthma: A twin study. Journal of Allergy and Clinical Immunology, 126(3), 626-630. doi: http://dx.doi.org/10.1016/j.jaci.2010.06.017
Tijhuis, M. A. R., Flap, H. D., Foets, M., & Groenewegen, P. P. (1995). Social support and stressful events in two dimensions: Life events and illness as an event. Social Science and Medicine, 40(11), 1513-1526. doi: http://dx.doi.org/10.1016/0277-9536(94)00276-Y
Tsiakiris, G., Neely, G., Lind, N., & Nordin, S. (2014). Comorbidity in atopy: Psychiatric conditions and functional somatic syndromes [Manuscript].
Turner, R. J. (1981). Social Support as a Contingency in Psychological Well-Being. Journal of Health and Social Behavior, 22(4), 357-367. doi: 10.2307/2136677
Uchino, B. (2006). Social Support and Health: A Review of Physiological Processes Potentially Underlying Links to Disease Outcomes. Journal of Behavioral Medicine, 29(4), 377-387. doi: 10.1007/s10865-006-9056-5
Wainwright, N. W. J., Surtees, P. G., Wareham, N. J., & Harrison, B. D. W. (2007). Psychosocial factors and incident asthma hospital admissions in the EPIC-Norfolk cohort study. Allergy, 62(5), 554-560. doi: 10.1111/j.1398-9995.2007.01316.x
Walter, M. J., & Holtzman, M. J. (2005). A Centennial History of Research on Asthma Pathogenesis. American Journal of Respiratory Cell and Molecular Biology, 32(6), 483-489. doi: 10.1165/rcmb.F300
Vamos, M., & Kolbe, J. (1999). Psychological factors in severe chronic asthma. Australian and New Zealand Journal of Psychiatry, 33(4), 538-544.
Wang, B.-L., Takigawa, T., Yamasaki, Y., Sakano, N., Wang, D.-H., & Ogino, K. (2008). Symptom definitions for SBS (sick building syndrome) in residential dwellings. International Journal of Hygiene and Environmental Health, 211(1–2), 114-120. doi: http://dx.doi.org/10.1016/j.ijheh.2007.03.004
Weiss, S. T. (2012). New approaches to personalized medicine for asthma: Where are we? Journal of Allergy and Clinical Immunology, 129(2), 327-334. doi: http://dx.doi.org/10.1016/j.jaci.2011.12.971
Verkuil, B., Brosschot, J. F., Meerman, E. E., & Thayer, J. F. (2012). Effects of momentary assessed stressful events and worry episodes on somatic health

61
complaints. Psychology and Health, 27(2), 141-158. doi: 10.1080/08870441003653470
Vernon, M. K., Bell, J. A., Wiklund, I., Dale, P., & Chapman, K. R. (2013). Asthma Control and Asthma Triggers: The Patient Perspective. Journal of Asthma and Allergy Educators, 4(4), 155-164. doi: 10.1177/2150129713483307
Williams, H. C., Jburney, P. G., Hay, R. J., Archer, C. B., Shipley, M. J., Ahunter, J. J., . . . David, T. J. (1994). The U.K. Working Party's Diagnostic Criteria for Atopic Dermatitis. British Journal of Dermatology, 131(3), 383-396. doi: 10.1111/j.1365-2133.1994.tb08530.x
Williams, H. C. (2005). Atopic Dermatitis. New England Journal of Medicine, 352(22), 2314-2324. doi: 10.1056/NEJMcp042803
Vocks, E., Busch, R., Fröhlich, C., Borelli, S., Mayer, H., & Ring, J. (2001). Influence of weather and climate on subjective symptom intensity in atopic eczema. International Journal of Biometeorology, 45(1), 27-33. doi: 10.1007/s004840000077
von Mutius, E. (2000). The environmental predictors of allergic disease. Journal of Allergy and Clinical Immunology, 105(1, Part 1), 9-19. doi: http://dx.doi.org/10.1016/S0091-6749(00)90171-4
Wright, R. J. (2005). Stress and atopic disorders. Journal of Allergy and Clinical Immunology, 116(6), 1301-1306. doi: http://dx.doi.org/10.1016/j.jaci.2005.09.050
Wright, R. J., Cohen, R. T., & Cohen, S. (2005). The impact of stress on the development and expression of atopy. Current Opinion in Allergy and Clinical Immunology, 5(1), 23-29.
Yonas, M. A., Lange, N. E., & Celedón, J. C. (2012). Psychosocial stress and asthma morbidity. Current Opinion in Allergy and Clinical Immunology, 12(2), 202-210. doi: 10.1097/ACI.0b013e32835090c9
Yunus, M. B. (2008). Central Sensitivity Syndromes: A New Paradigm and Group Nosology for Fibromyalgia and Overlapping Conditions, and the Related Issue of Disease versus Illness. Seminars in Arthritis and Rheumatism, 37(6), 339-352. doi: http://dx.doi.org/10.1016/j.semarthrit.2007.09.003
Zigmond, A. S., & Snaith, R. P. (1983). The Hospital Anxiety and Depression Scale. Acta Psychiatrica Scandinavica, 67(6), 361-370. doi: 10.1111/j.1600-0447.1983.tb09716.x
Appendix
Study 1
Study 2
Study 3
62