community pbf in rwanda chd 2013. structure moh mch desk nutrition desk community health desk fp...
TRANSCRIPT

Community PBF in Rwanda
CHD 2013

STRUCTURE
Introduction In 2005, MOH has reinforced 3 major
stratagies to improve the health quality services: CBHI(Community Based Health
Insurance) Performance based financing Quality assurance The Community PBF started in January
2006, in all districts of Rwanda, with funding throught the local administration

Selected indicators 2006-2008 Number of members of CBHI(Community
Based Health Insurance) , Mobilisation of assisted delivery, Mobilisation in using LLIN(Long Lasting
Insecticide Nets) Treatment of dehydration of children
under 5 years, Hygiene Report of Community Activities.

Challenges of this model of Community PBF 2006-2008 Use of funds for other priorities of the
districts Delay in reporting indicators Delay in transfering funds by the districts Lack of motivation to supervise the
community activities Lack of tools in data collaction No reports from the districts to MOH Lack of mechanisms for data verification
New model CPBF : 2009 Designed in 2009 to change the challenges of
the old model: Trought the TWG of CPBF (MOH and
parteners WB, USAID/MSH, HDP etc…) In december 2007: first draft of
Community PBF The new model proposed in different
Health Centers for review and considerations (MOH department of policies ; Senior Management; Health Financing Unit ; Technical Working Group of Community PBF etc)

Making decision Results from the evaluation of selected HCs on the
impact of CPBF show that MOH has reached : Increasing of utilization of health services – Assisted
delivery, Preventive of Health care of children under 5 years Increasing health quality – Post natal care and immunization
Results also show that expanding of PBF at the Community level can reduce the difficult to realize the MCH indicators: Nutritional status Timely prenatal care utilization Institutional delivery Timely postnatal care utilization Modern contraceptive use

INDICATORS REMUNERATED:
Nutrition Monitoring: % of children monitored for nutritional status
ANC : Women accompanied/referred to Health Center for prenatal care within first 4 months of pregnancy
Deliveries: Women accompanied/referred to HC for assisted deliveries
Family Planning: new users referred by CHWs for modern family planning methods
Family Planning: % of regular users using long term methods (IUD, Norplant, Surgical/NSV contraception)
Number of TB suspects referred to the health center by the CHW’s
Number of TB patients receiving DOTS at home Number of couples referred to a health center for PMTCT Number of households referred to a health center for VCT CHW’s Reports

Signing Contracts of Community PBF: Improves
performance
Payments made when proof of the agreed level of performance
The Sector Steering Committee signed the community contracts
Data entered at district level web-based database

www.pbfrwanda.org.rw/siscom

Mécanisme contractuel entre acteurs
Financement forfaitaire d’un seul résultat trimestriel: Rapport des ASC avec suivi spécifique de 5 indicateurs (Modèle national)
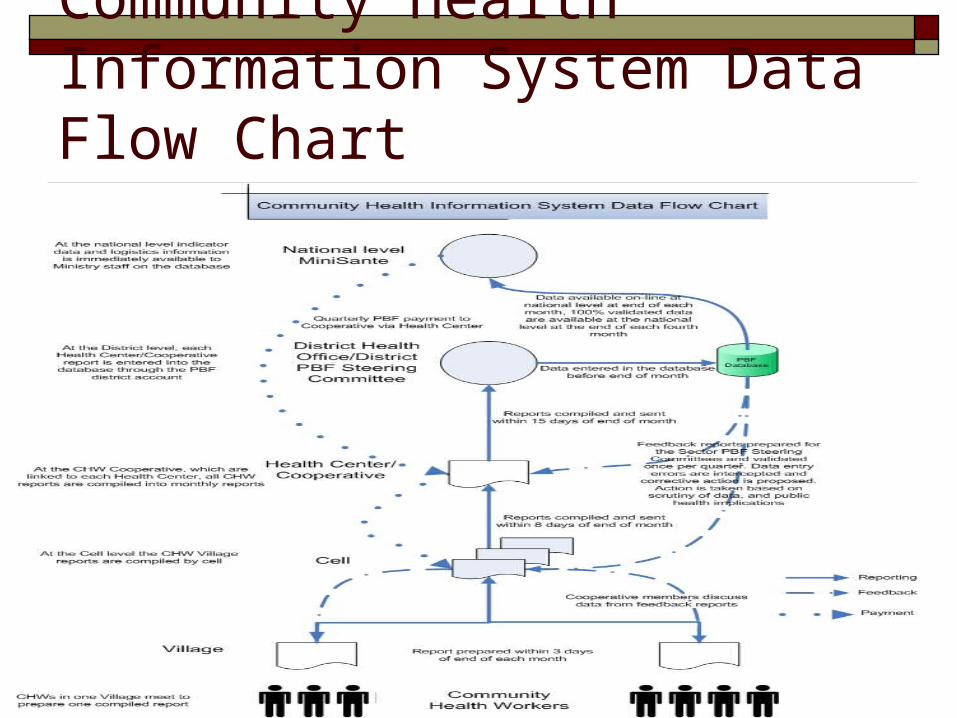
Community Health Information System Data Flow Chart


CHWs MotivationCHWs Motivation• Trust and respect from community
members, leaders etc…
• Support from Supervisors and implementation partners help improve work;
• Regular trainings, meetings supervision
• In-country study tours to learn from peers in other districts
• Distance learning
• Community performance-based financing (PBF);
• Membership in cooperatives for income generation

CHWs’ Cooperatives
- Community Health Workers’ (CHWs) cooperatives were initiated in late 2007
• - The model was introduced through a transformation process from CHWs non profit making associations
• - Previously, they had associations that were no more than a forum to receive and share funds from MOH, and after each member would do as they wished with that money
• - Up to-date, 449 cooperatives exist country wide• - However, more are being formed as there are new health centers
emerging• 100% are operational with approximately 42% CHWs cooperatives
legally registered at national level• - Objective is to have all cooperatives with a legal certificate by end of
first quarter 2012 because of the importance of registration• - This shall be possible through close collaboration between MOH,
district authorities and RCA

Achievements for CPBF Program Implementation of Com PBF in all districts CHW’S are remunerated by quarter(449 CHWs cooperatives) Sector Steering Committee are trained on reporting and on
all tools used in reporting and counter verification data New revised CPBF Contracts in KINYARWANDA are signed
between the SSC and HC;SSC and CHW’s Cooperatives CHW’s cooperatives data reports are validated by Sector
Steering Committees and submitted to the Community PBF Health centers and SSC are the principal evaluators in data
reported by the CHW’S and data entered by HC District Steering Committee and DH are the second
evaluators before sending the reports to the Central level Central level make analysis on the data reported by the
CHW’s before the payment

Achievements for CPBF Program Monthly CPBF Subcommittee meeting Monthly Extend Team PBF meeting Community PBF Audit system is done and the
report available Community PBF Counter verification data, audit
is done and the report is available Results dissemination for Community PBF
counter verification data presented in coordination meeting with the districts
Program Challenges Training: CHWs need training in essential service
delivery, data reporting, and income generation; Robust verification mechanisms to ensure that minimum
package of community health services has been delivered;
The logistics to deliver the minimum package of community health services;
Data verification mechanisms on reported indicators; Communication issues: cell phones for reporting and
sharing information regarding the community-based activities;
Issues related to the design and management of community health workers’ income generating activities (cooperatives)

PRIORITIES
Reinforce and increase the data reports provided by the CHW’s
Reinforce counter verification data at all levels
Reinforce the data analysis reports from CHW’s by the Sector Steering Committee and Districts Steering Committee
Reinforce keeping all reports from villages to cells and to be analysed by the Sector Steering Committees
Regular supervision by Central Level in data collection by Sector Steering Committee and District Steering Committee

HE Paul KAGAME with all CHWs

Merci