introduction to mch (and mch-b) lend orientation...
TRANSCRIPT
Introduction to MCH (and MCH-B) LEND Orientation 2013
Colleen E Huebner PhD, MPH
MCH Program School of Public Health
What is MCH?
“the professional and academic field that focuses on the determinants, mechanisms and systems that promote and maintain the health, safety, well being and appropriate development of children and their families in communities and societies in order to enhance the future health and welfare of society and subsequent generations.”
(Alexander, 2004)
Objectives
• History of federal support for Maternal and Child Health (housed in MCH “B”)
• MCH now
• MCH in the near future
• MCH and you
Henry Bergh, Founder Am Soc for Prevention of Cruelty to Animals (1866) Am Soc for Prevention of Cruelty to Children (1875)
Mary Ellen Wilson
1874
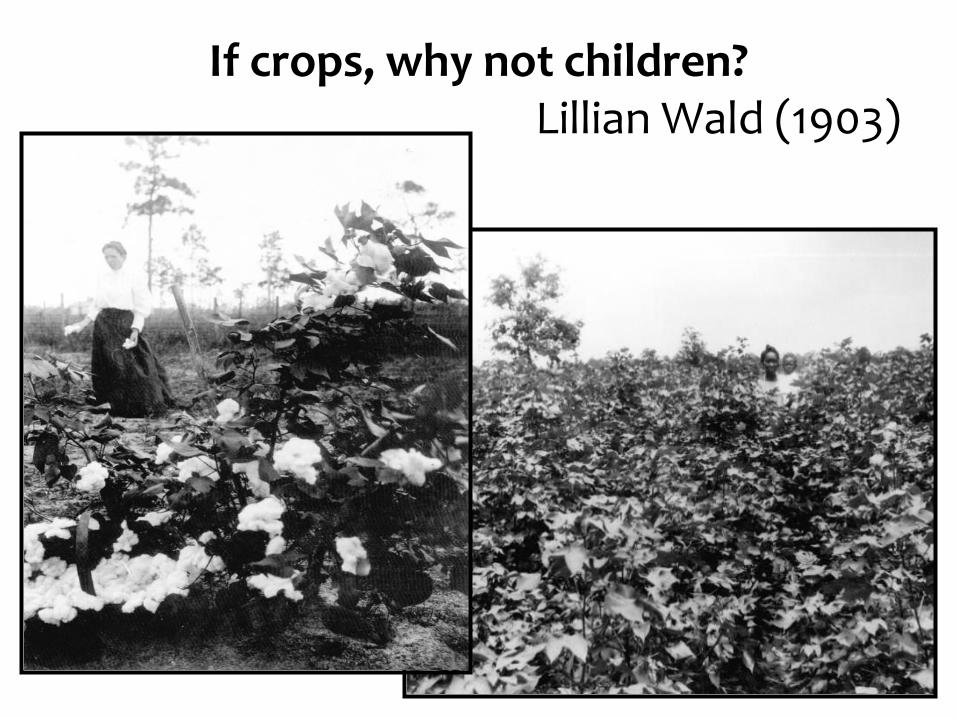
If crops, why not children? Lillian Wald (1903)

Children’s Bureau: Mission Statement
“Investigate and report …. upon all matters pertaining to the welfare of children and child life among all classes of our people and shall especially investigate the questions of infant mortality, the birth rate, orphanage, juvenile courts, desertion, dangerous occupations, accidents and diseases of children, employment, legislation affecting children in the several states and Territories.”
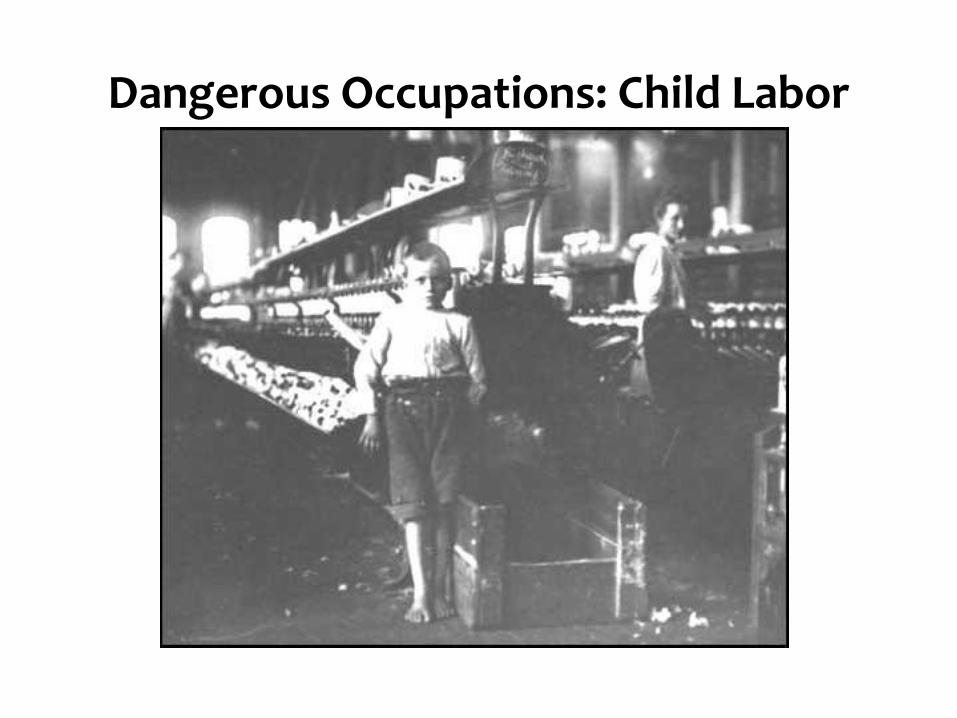
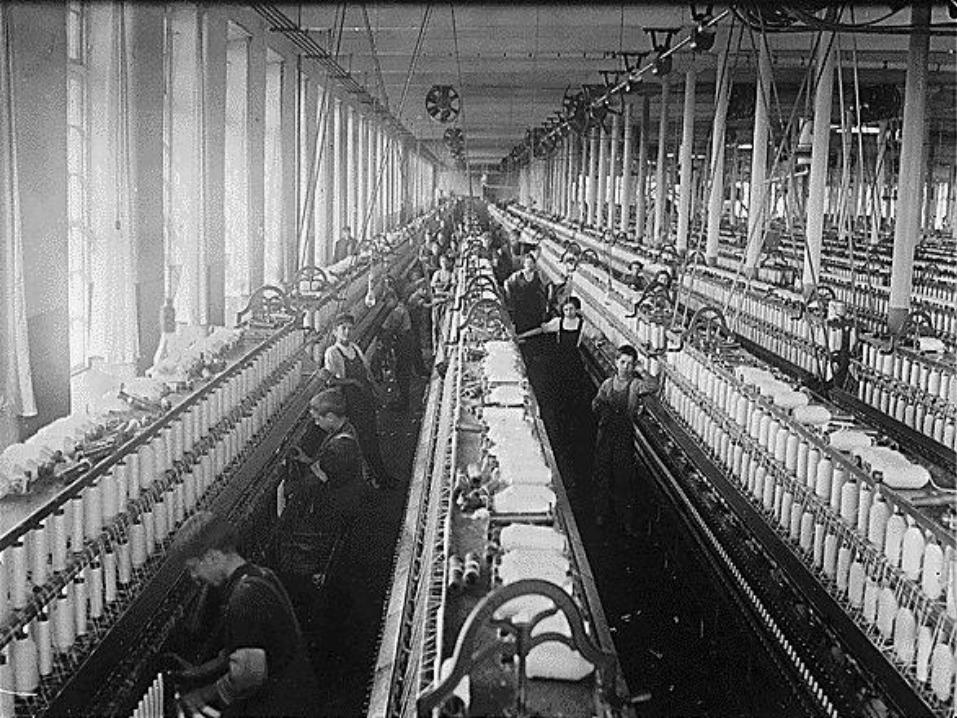
Dangerous Occupations: Child Labor
Infant Care (1914)
Johnstown, PA: Infant Mortality Study
Birth Certificates
Federal Maternal and Child Health Legislation Past …
• Role of the Children’s Bureau evolved to include direct assistance to States to help them improve conditions for infants and women during childbearing.
• These grants-in-aid were authorized by Congress in 1921 as part of the Maternity and Infancy Act (also known as the Sheppard-Towner Act).
Sheppard-Towner Act
• Enacted,1921
• Allowed to expire,1929
• Why?
A Blueprint for Title V
• Although the Sheppard-Towner Act expired in 1929, its existence established the expectation and acceptance that the people of the United States, through their Federal and State governments, share a responsibility for the health and welfare of children.
• This belief provided a blueprint for Title V of the Social Security Act of 1935 (Public Law 74-271) to support mothers and children left destitute during the Great Depression.

FDR in Seattle, 1932
… Federal Maternal and Child Health
Legislation Present - Title V • Title V of the Social Security Act of 1935 created Federal-
State partnerships to: – ensure the health of mothers and children
– promote care for “crippled children”
• Administration of Title V was assigned to the Children’s Bureau in 1935; by June 1937, all States and Territories had MCH divisions
Emergency Maternity and Infant Care (EMIC) Program
• When the U.S. entered WW II, millions of military wives were dislocated from their homes
• In 1943, Congress passed the EMIC program to provide health services to wives of service men in the lowest 4 pay grades
• Services included prenatal care, delivery and 6 weeks postpartum, and infant care to age 12 months
Who is MCH Today?
• The historical phrase “maternal and child health” (MCH) refers to women, infants, children of all ages, adolescents, and families.
• Today, priority for services supported by federal Maternal and Child Health funds is given to 3 groups:
– Mothers of infants and children < 21 years of age
– Pregnant women and women of child-bearing age
– Children with special health care needs (CSHCN)
Legislative Basis for MCHB • Title V is the chief financial foundation and the primary
legislative authorization for MCHB, “the Bureau”
• Title V provides the majority of the funding sources for all Bureau programs. Under Title V, MCHB administers Formula Grants, including the Block Grant to the States and competitive Discretionary Grants
• Services and activities are not protected as “entitlements;” Congress determines the funding level
• MCHB is responsible also for administering several categorical programs
• State and local Title V initiatives are organized within the 10 PHS regions of the U.S.
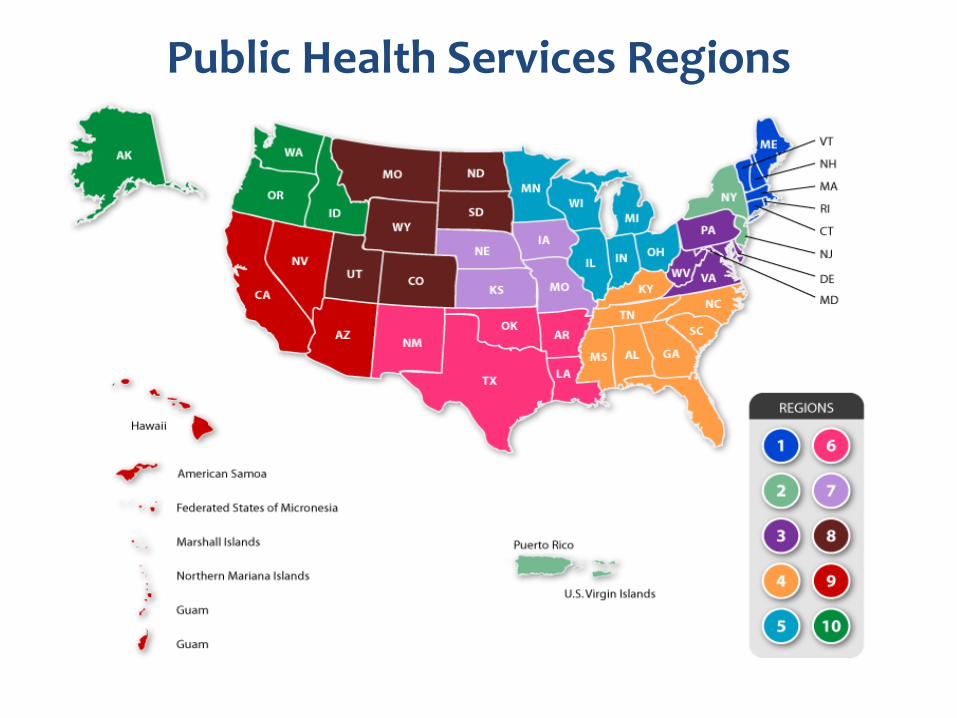
Public Health Services Regions
What’s a “block?”
Requirements of the Title V Block Grant
• The purpose of the MCH Services Block Grant is to improve the health of all mothers and children in the Nation
• Every $4 of Federal Title V money must be matched by at least $3 of State and local money
• At least 30% of Title V Federal funds is earmarked for services for Children and Youth with Special Health Care Needs (CYSHCN)

Changes in the Block as of 1989
States’ applications required:
•needs assessment and priorities
•measurable objectives
•budget accountability
•documentation of matching funds
•public input

Functions of MCH: The Pyramid
What’s been happening lately?
Legislative Authority
• Section 2951 of the Affordable Care Act of 2010 (P.L. 111-148) ….
• amends Title V of the Social Security Act to add Section 511: Maternal, Infant, and Early Childhood Home Visiting Programs (MIECHV)
• $1.5 billion over 5 years • $100M FY2010 • $250M FY2011 • $350M FY2012 • $400M FY2013 • $400M FY2014
31
MIECHV Goals
Provide voluntary, evidence-based home visiting services (in period from prenatal to age 6 yrs) to improve: – Prenatal, maternal, and newborn health – Child health and development, including the
prevention of child injuries and maltreatment – Parenting skills – School readiness and child academic achievement – Family economic self-sufficiency – Referrals for and provision of other community
resources and supports
32
Priority Populations • Families in at-risk communities
• Low-income families
• Pregnant women under age 21
• Families with a history of child abuse or neglect
• Families with a history of substance abuse
• Families that have users of tobacco in the home
• Families with children with low ac achievement
• Families with children with developmental delays or disabilities
• Families with individuals serving or have served in the Armed Forces
33
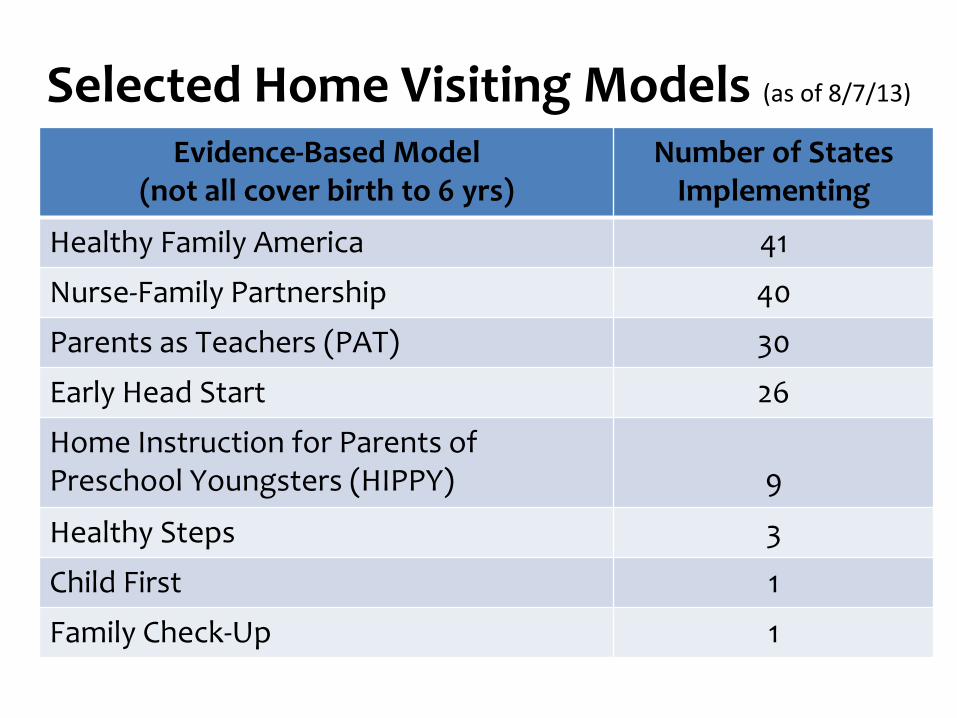
Selected Home Visiting Models (as of 8/7/13)
Evidence-Based Model (not all cover birth to 6 yrs)
Number of States Implementing
Healthy Family America 41
Nurse-Family Partnership 40
Parents as Teachers (PAT) 30
Early Head Start 26
Home Instruction for Parents of Preschool Youngsters (HIPPY)
9
Healthy Steps 3
Child First 1
Family Check-Up 1
34
Where’s the Population Health or the “Infrastructure”?
• National evaluation of Maternal, Infant and Early Childhood Home Visiting (MIECHV)
• Required by legislation; grantees (states and their subcontractors) required to participate
• $40m over 9 years, transferred annually from HRSA to ACF/OPRE
• Secretary’s Advisory Committee (SAC) on the MIECHV evaluation met 3 times to discuss design and design received comment from OMB, SAC, Counselors to the Secretary
MIHOPE: Mother and Infant Home Visiting Program Evaluation
September 13, 2013
• Analysis of the needs assessments • Effectiveness study • Subgroup analysis, including both populations
and programs • Study of effects on the health care system • No later than March 31, 2015, the Secretary
shall submit a report to Congress on the results of the evaluation conducted
• And shall make the report publicly available
ACA specifies 4 main components of the national evaluation
September 13, 2013
• Evaluation must use a rigorous design • Conduct a thorough implementation study • Produce results that will inform program-
level decision-making and strengthen the program in the future
• Random assignment and baseline data collection at the time of enrollment and a follow up assessment when the child is approximately 15 months old.
• Cost data for cost and cost effectiveness analysis
Evaluation (HHS’) GoalsIHOPE: Design
September 13, 2013
• Four models selected by 10 or more states
• Early Head Start
• Healthy Families America
• Nurse Family Partnership
• Parents as Teachers • Sample of 5,100 families in approximately 85
local sites across 12 states • Contractor and multiple contractors
Evaluation includes …MIHOPE
September 13, 2013
What’s happening now?
Affordable Care Act
• Signed into law March 23, 2010
• Goal to decrease number of uninsured Americans
– Requires nearly all to have health insurance
– Expands Medicaid eligibility to all at or below 133% of the FPL ($19,530 for family of 3)*
– Creates new health insurance marketplaces where individuals and small businesses can obtain coverage
Medicaid Expansion
• Optional for states (Supreme Court)
• 25 states “yes,” 22 “no,” 4 “undecided”
• Region X?
– WA and OR “yes”; AK and ID “no”
ACA: 10 Essential Health Benefits • Ambulatory services
• Emergency services and Hospitalization
• Maternity and newborn care
• Mental health and substance use disorder services, including behavioral health treatment
• Prescription drugs
• Rehabilitative and habilitative services and devices
• Laboratory services
• Preventive & wellness services; chronic disease mgmt
• Pediatric services, including oral and vision care
My patients are covered by Medicaid already …
what changes might this bring for me?
What’s happening next in MCH?
Recall “Changes in the Block as of 1989”
States’ applications required to include:
•needs assessment and priorities
•measurable objectives
•budget accountability
•documentation of matching funds
•public input
Title V Performance and Outcome Measures
18 national health performance measures
7-10 state negotiated performance measures
6 health outcome measures - 1 state (optional)
Population Health Monitoring The Title V Information System
6 national outcome measures reported from each of the states and jurisdictions of the U.S.
• Infant mortality rate per 1,000 live births
• Ratio of black infant mortality rate to the rate for whites
• Neonatal mortality rate per 1,000 live births
• Postneonatal mortality rate per 1,000 live births
• Perinatal mortality rate per 1,000 live births plus fetal deaths
• Child death rate per 100,000, ages 1 through 14

National (Core) Performance Measures
Examples of 18 PM’s:
• Children with special health care needs age 0 to 18 who receive coordinated, ongoing, comprehensive care within a medical home
• % third grade children who have received protective sealants on at least one permanent molar tooth
• Rate of deaths to children aged 14 years and younger caused by motor vehicle crashes per 100,000 children
• Rate (per 100,000) of suicide deaths among youths ages 15 through 19 (PM #16)
But are these the best measures for today? tomorrow?
In addition,
Title V authorizes funds to …
“provide for special projects (SPRANS), research, and training for MCH and CSHCN, for genetic disease testing, counseling, and information, for grants relating to hemophilia, and for the screening of newborns for sickle cell anemia, and other genetic disorders and follow-up services.”

What is MCH Leadership?
“An MCH leader inspires and bring people
together to achieve sustainable results to
improve the lives of the MCH population”
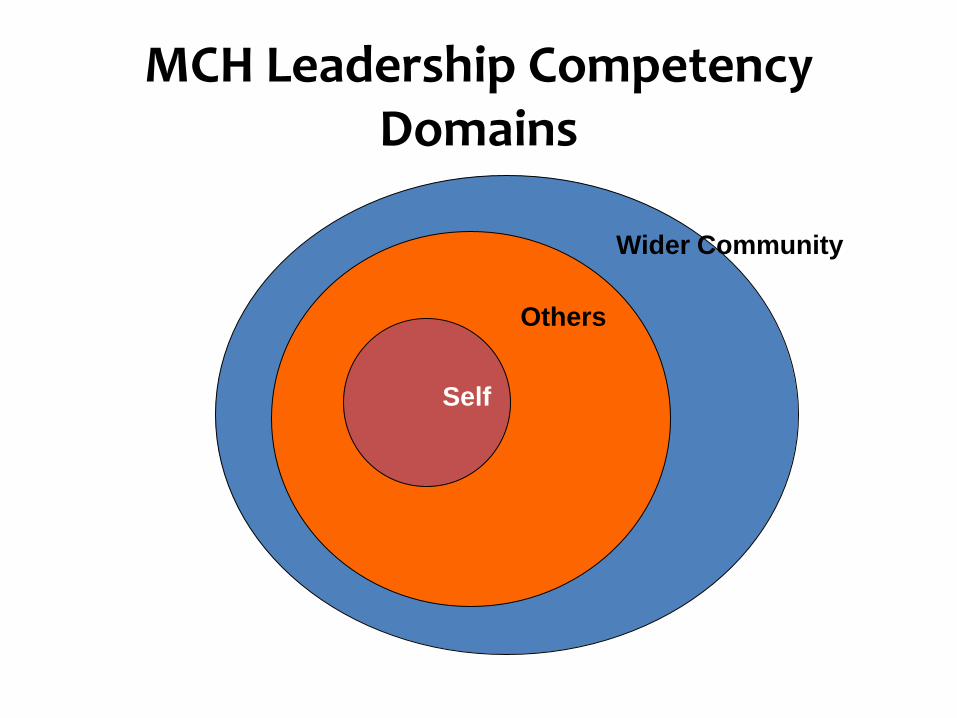
MCH Leadership Competency Domains
Self
Others
Wider Community
MCH Field Leadership
• Academia
• Clinical Settings
• Public Health and Policy
• MCH Advocacy
Grace Abbott 1878-1939
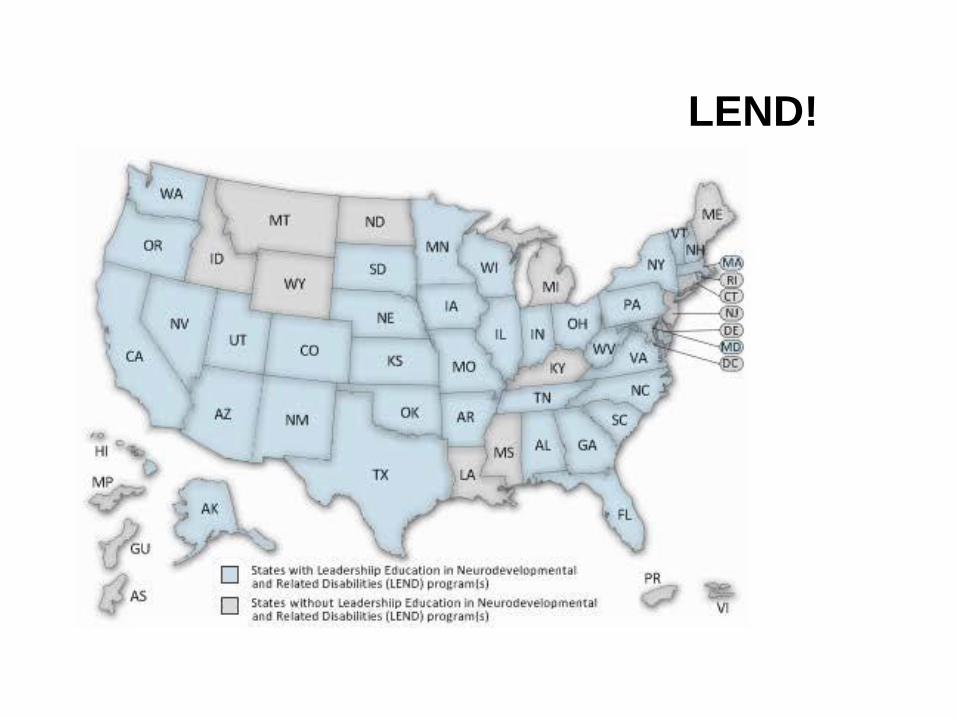
LEND!
Resources Commonwealth Fund (U.S. Health Care)
http://www.commonwealthfund.org
AMCHP (MCH, National)
http://www.amchp.org
Northwest Bulletin (MCH, Region X)
http://depts.washington.edu/mchprog
[email protected] to subscribe
MCH UW SPH Course Fall 2013
Drop in! M/W 12:30-1:50, see Sally for syllabus