communicate with confidence-printstatic.aapc.com/3b7310d0-2751-4c51-8dd2-4cc34d8103... ·...
TRANSCRIPT
Communicate With Confidence to Physicians:
Coding as a Second Language
Written by:Dr. Joseph J. Sivak MD and Ms. Lorraine J. Sivak

Communicate with Confidence Copyright © AAPC 2009 Page 2
DISCLAIMER
This course was current at the time it was published. This course was prepared as a tool to
assist the participant in effective communication. Although every reasonable effort has been
made to assure the accuracy of the information within these pages the ultimate responsibility
for clear communication and the correct submission of claims or response to any remittance
advice lies with the provider of services. The American Academy of Professional Coders (AAPC)
employees, agents, and staff make no representation, warranty or guarantee that this
compilation of information is error-free and will bear no responsibility, or liability for the
results or consequences of the use of this course. This guide is a general summary that
explains commonly accepted aspects of effective communication but it is not a legal or medical
document. All information is intended for general knowledge only and is not a substitute for
medical advice or treatment for specific medical conditions. We cannot and do not give medical
including mental health advice.
NOTICES
Current Procedural Terminology (CPT®) is copyright © 2008 American Medical Association. All
Rights Reserved. CPT® is a registered trademark of the American Medical Association (AMA).
COMMUNICATE WITH CONFIDENCE TO PHYSICIANS:CODING AS A SECOND LANGUAGE
Written by:Dr. Joseph J. Sivak MD and Ms. Lorraine J. Sivak
Editorial contributions by:Stephanie L. Jones, CPC, CEMC
Communicate with Confidence Copyright © AAPC 2009 Page 3
Contents
FORWARD ..............................................................................................................................................................4
INTRODUCTION ....................................................................................................................................................5
CODER-SELF-AWARENESS ................................................................................................................................6
Exercise One: Locus of Control. ...................................................................................................................6
Exercise Two: Styles of Communication ......................................................................................................9
Exercise Three: Learning and Personality Styles .......................................................................................16
THE MIND OF A PHYSICIAN ............................................................................................................................21
Stereotypical Physician Personalities .........................................................................................................21
Appreciating Physician Development ........................................................................................................22
Understanding How a Physician Thinks .....................................................................................................22
THE CODER-PHYSICIAN WORKING ALLIANCE ................................................................................................23
Top 10 Coder Mantras for a Successful Coder-Physician Working Alliance ............................................23
Communication that “Works” .....................................................................................................................24
CONCLUSION ......................................................................................................................................................30
Communicate with Confidence Copyright © AAPC 2009 Page 4
FORWARD
Physician coding education is vital to payment-compliant medical
documentation and proper reimbursement. Often the delivery of this
information falls to the coder, who is responsible for correctly coding per the
medical record while also leaving no payable, rendered service unreported.
Coders are required to explain detailed coding models, which require a solid
understanding of medical terminology and anatomy that often does not equal
the physician’s.
Compounding the issue, the personality and style of varied physicians may
cause some coders to fear communicating unpopular coding concepts:
- What if I mispronounce that medical term?
- What if she erupts and I sit there speechless?
- What if he does not find me creditable?
- What if I am asked a question and I do not know the answer?
- What if I am unable to get my point across?
Level of education, experience, and talent aside — the best coders and billers
have also mastered the art of communicating with physicians in ways that
almost always produce positive results. A certified professional coder is one of
the physician’s best tools in proper reimbursement, and is often an important
key to the financial success of the medical practice.
This course addresses persuasive communication skills necessary to manage
challenging situations with physicians and turn them into a catalyst for positive
change. A key to effective communication is in understanding your own
unconscious motivations and needs. For this reason it will begin with a Self
Assessment. The remainder of the course is designed to help a coder better
understand and respond to physicians with the end goal being…
Flawless documentation that promotes proper payment for all rendered
services!
Communicate with Confidence Copyright © AAPC 2009 Page 5
INTRODUCTION
Communication between a
professional coder and a
physician are vital to the
correct payment process. When
a provider understands the
rules around documentation,
coding and compliance are
optimized. To make the best
business decisions a physician
needs clear and trusted
communication from the
coders who are helping to assure his or her proper payment. Sometimes the
lines of communication are muddied by frustrations making communication
more difficult. No one likes to be told there are rules when those rules result in
lowered income or being told that services are worth less than expected. This
communication barrier between a coder and a physician can be overcome by
three Cornerstones of Effective Coder Communication.
Cornerstones for Effective Coder Communication
¸ CODER-SELF-AWARENESS
¸ UNDERSTANDING THE MIND OF A PHYSICIAN
¸ THE CODER-PHYSICIAN WORKING ALLIANCE
It may not be possible to convince someone that the sky is blue if they believe it
is purple. Challenging the beliefs of a person can result in lost communication
because one or both parties feel the other is arrogant, ignorant or both. The
real question is:
How important is the color of the sky if the story is about birds in flight?
“To effectively communicate we must
realize that we are all different in the
way we perceive the world and use this
understanding as a guide to our
communication with others.”
~ Anthony Robbins
Communicate with Confidence Copyright © AAPC 2009 Page 6
CODER-SELF-AWARENESS
The ability to see beyond communication obstacles and focus on desired
actions or outcomes begins with a complete understanding of your own
strengths and weaknesses. Increasing your awareness to your natural listening
and response styles enables you to better modify responses, if need be, for
best results. This is the first step in effective communication.
The following self assessment exercises will give you a good point of personal
perspective.
Exercise One: Locus of Control. Based on J.B. Rotter (1966) Generalized
expectancies for internal versus external control of reinforcement Psychological
Monographs 80 (1 Whole No. 609).
Answer the questions below truthfully as possible. Check the box A. ˛ or B. ˛
according to the statement you most agree with:
A B Question
A. People's misfortunes result from the mistakes they make.
B. Many of the sad things in people's lives are partly due to bad luck
A. One of the major reasons why we have wars is because people
don't take enough interest in politics.
B. There will always be wars no matter how hard people try to prevent
them.
A. In the long run people get the respect they deserve in this world.
B. Unfortunately an individual's worth often passes unrecognized no
matter how hard he tries.
A. The idea that Physicians are unfair to Coders is nonsense.
B. Most Coders don't realize the extent to which their credibility is
Communicate with Confidence Copyright © AAPC 2009 Page 7
influenced by accidental happenings.
A. Capable people who fail to become leaders have not taken
advantage of their opportunities.
B. Without the right breaks one cannot be an effective leader.
A. People who can't get others to like them don't understand how to
get along with others.
B. No matter how hard you try some people just don't like you.
A. Trusting to fate has never turned out as well for me as making a
decision to take a definite course of action.
B. I have often found that what is going to happen will happen.
A. In the case of the well prepared Coder there is rarely if ever such a
thing as an unfair test of their coding ability.
B. Many times coding tends to be so unrelated to billing that accuracy
is really next to impossible.
A. Becoming a success is a matter of hard work; luck has little or
nothing to do with it.
B. Getting a good job depends mainly on being in the right place at
the right time.
A. The average citizen can have an influence in government decisions.
B. This world is run by the few people in power and there is not much
the little guy can do about it.
A. When I make plans I am almost certain that I can make them work.
B. It is not always wise to plan too far ahead because many things
turn out to be a matter of luck anyway.
A. In my case getting what I want has little or nothing to do with luck.
B. Many times we might just as well decide what to do by flipping a
coin.
A. What happens to me is my own doing.
B. Sometimes I feel that I don't have enough control over the direction
my life is taking.
Communicate with Confidence Copyright © AAPC 2009 Page 8
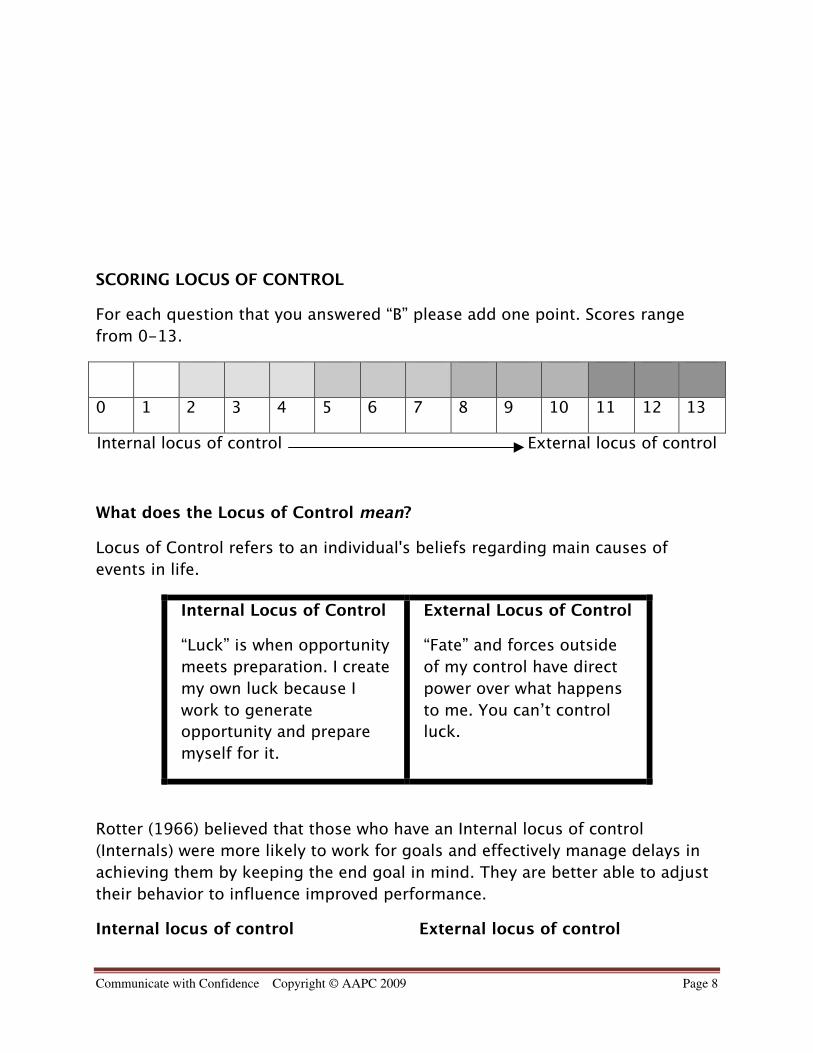
SCORING LOCUS OF CONTROL
For each question that you answered “B” please add one point. Scores range
from 0-13.
0 1 2 3 4 5 6 7 8 9 10 11 12 13
Internal locus of control External locus of control
What does the Locus of Control mean?
Locus of Control refers to an individual's beliefs regarding main causes of
events in life.
Internal Locus of Control
“Luck” is when opportunity
meets preparation. I create
my own luck because I
work to generate
opportunity and prepare
myself for it.
External Locus of Control
“Fate” and forces outside
of my control have direct
power over what happens
to me. You can’t control
luck.
Rotter (1966) believed that those who have an Internal locus of control
(Internals) were more likely to work for goals and effectively manage delays in
achieving them by keeping the end goal in mind. They are better able to adjust
their behavior to influence improved performance.
Internal locus of control External locus of control
Communicate with Confidence Copyright © AAPC 2009 Page 9
More Likely to… More Likely to…
• Tolerate vague situations
• Learn from their mistakes
• Prefer games based on skill
• Prefer “Black and White” rules
• Suffer from depression
• Prefer games based on chance
Studies show that Internals tend to be less “stressed out” because they control
their choices and their circumstances. Those with an external locus of control
feel more at the mercy of outside events and have less (or no) control over their
situation. Because Internals tend to be healthier and happier the following tips
can help those with external tendencies feel better about daily situations,
including communicating effectively with those around them.
“Life is 1% what happens to you and 99% how you choose to feel aboutit.”
When you feel caught up in frustrating situations in your life, surprise yourself
with the number of options you have:
• Write down every option open to you in your current situation.• Even if you don’t like the choices available, remember that you have
choices• Evaluate your list and decide on the best course of action to meet your
goals• Practice expanding your mind to all open possibilities• Replace “I HAVE to…” or “I NEED to…” with “I CHOSE to…”
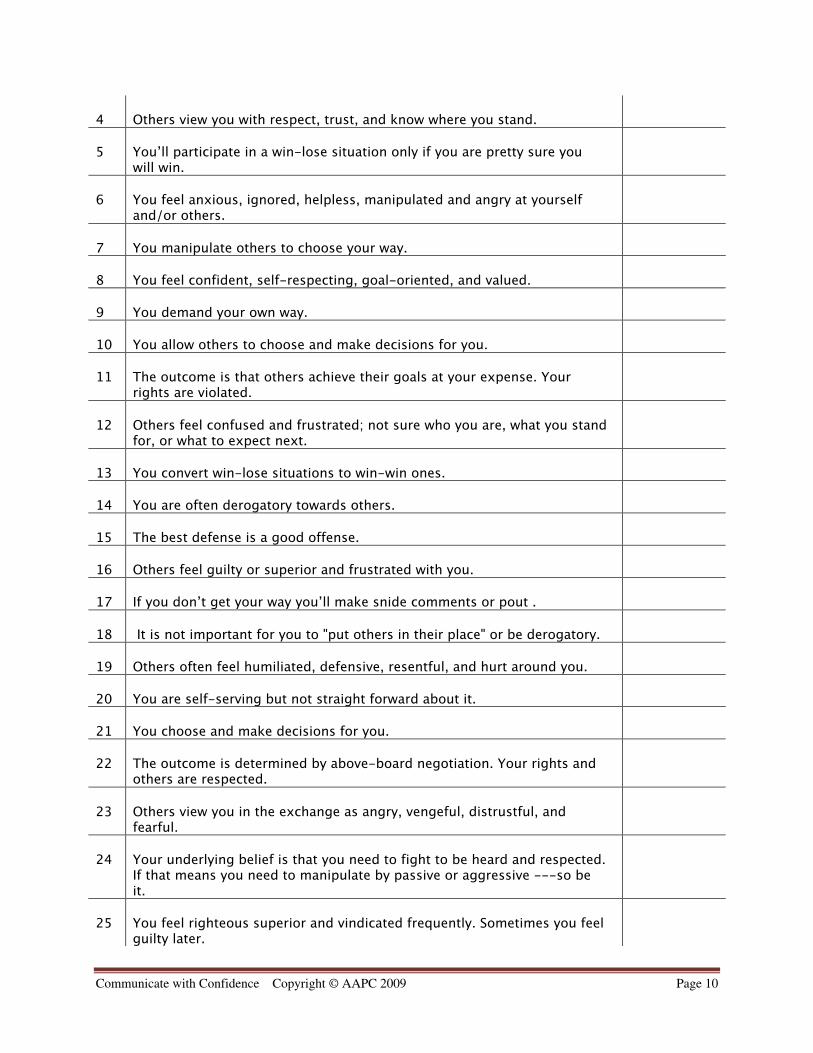
Exercise Two: Styles of Communication
There are four generally recognized communication styles that influence every
message we attempt to convey. They are “Assertive,” “Aggressive,” “Passive”
and “Passive-Aggressive.” The following exercise can help you to determine
your prominent style.
Statement True orFalse
1 If you get your own way it is by chance or so it seems.
2 You tend towards indirectness with the air of being direct.
3 You end up in many situations where you must stand up for yourself andothers must be put in their place by you.
Communicate with Confidence Copyright © AAPC 2009 Page 10
4 Others view you with respect, trust, and know where you stand.
5 You’ll participate in a win-lose situation only if you are pretty sure youwill win.
6 You feel anxious, ignored, helpless, manipulated and angry at yourselfand/or others.
7 You manipulate others to choose your way.
8 You feel confident, self-respecting, goal-oriented, and valued.
9 You demand your own way.
10 You allow others to choose and make decisions for you.
11 The outcome is that others achieve their goals at your expense. Yourrights are violated.
12 Others feel confused and frustrated; not sure who you are, what you standfor, or what to expect next.
13 You convert win-lose situations to win-win ones.
14 You are often derogatory towards others.
15 The best defense is a good offense.
16 Others feel guilty or superior and frustrated with you.
17 If you don’t get your way you’ll make snide comments or pout .
18 It is not important for you to "put others in their place" or be derogatory.
19 Others often feel humiliated, defensive, resentful, and hurt around you.
20 You are self-serving but not straight forward about it.
21 You choose and make decisions for you.
22 The outcome is determined by above-board negotiation. Your rights andothers are respected.
23 Others view you in the exchange as angry, vengeful, distrustful, andfearful.
24 Your underlying belief is that you need to fight to be heard and respected.If that means you need to manipulate by passive or aggressive ---so beit.
25 You feel righteous superior and vindicated frequently. Sometimes you feelguilty later.
Communicate with Confidence Copyright © AAPC 2009 Page 11
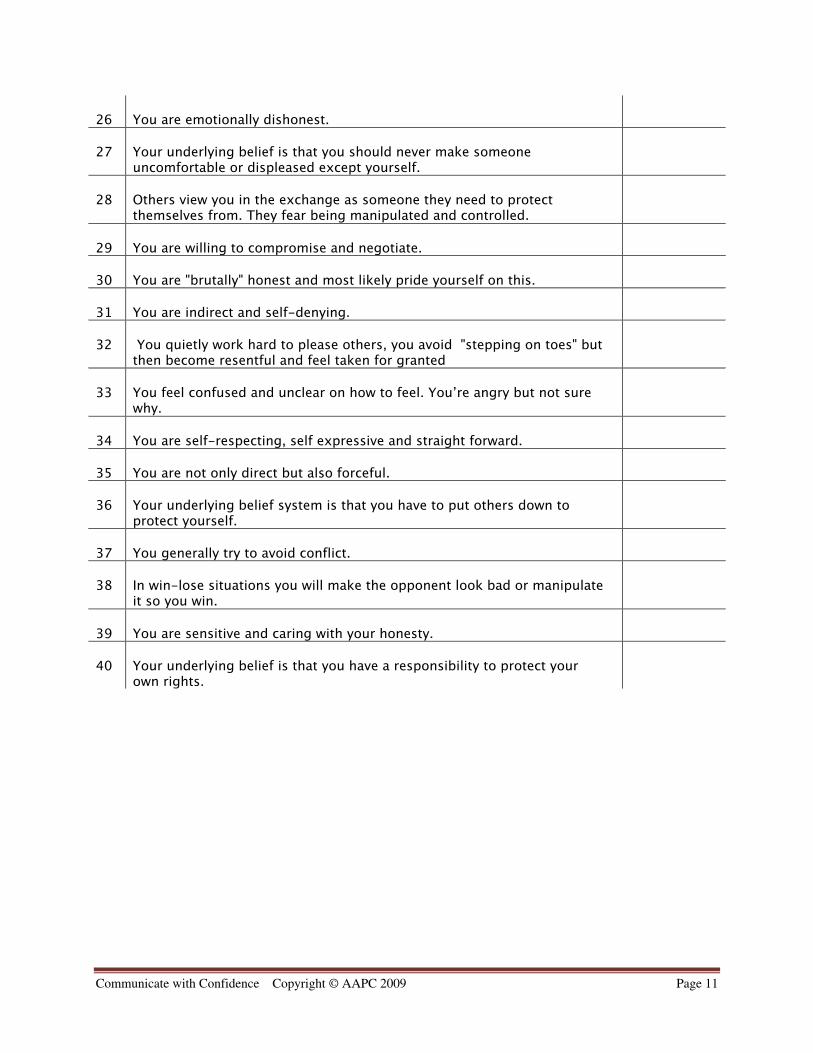
26 You are emotionally dishonest.
27 Your underlying belief is that you should never make someoneuncomfortable or displeased except yourself.
28 Others view you in the exchange as someone they need to protectthemselves from. They fear being manipulated and controlled.
29 You are willing to compromise and negotiate.
30 You are "brutally" honest and most likely pride yourself on this.
31 You are indirect and self-denying.
32 You quietly work hard to please others, you avoid "stepping on toes" butthen become resentful and feel taken for granted
33 You feel confused and unclear on how to feel. You’re angry but not surewhy.
34 You are self-respecting, self expressive and straight forward.
35 You are not only direct but also forceful.
36 Your underlying belief system is that you have to put others down toprotect yourself.
37 You generally try to avoid conflict.
38 In win-lose situations you will make the opponent look bad or manipulateit so you win.
39 You are sensitive and caring with your honesty.
40 Your underlying belief is that you have a responsibility to protect yourown rights.
Communicate with Confidence Copyright © AAPC 2009 Page 12
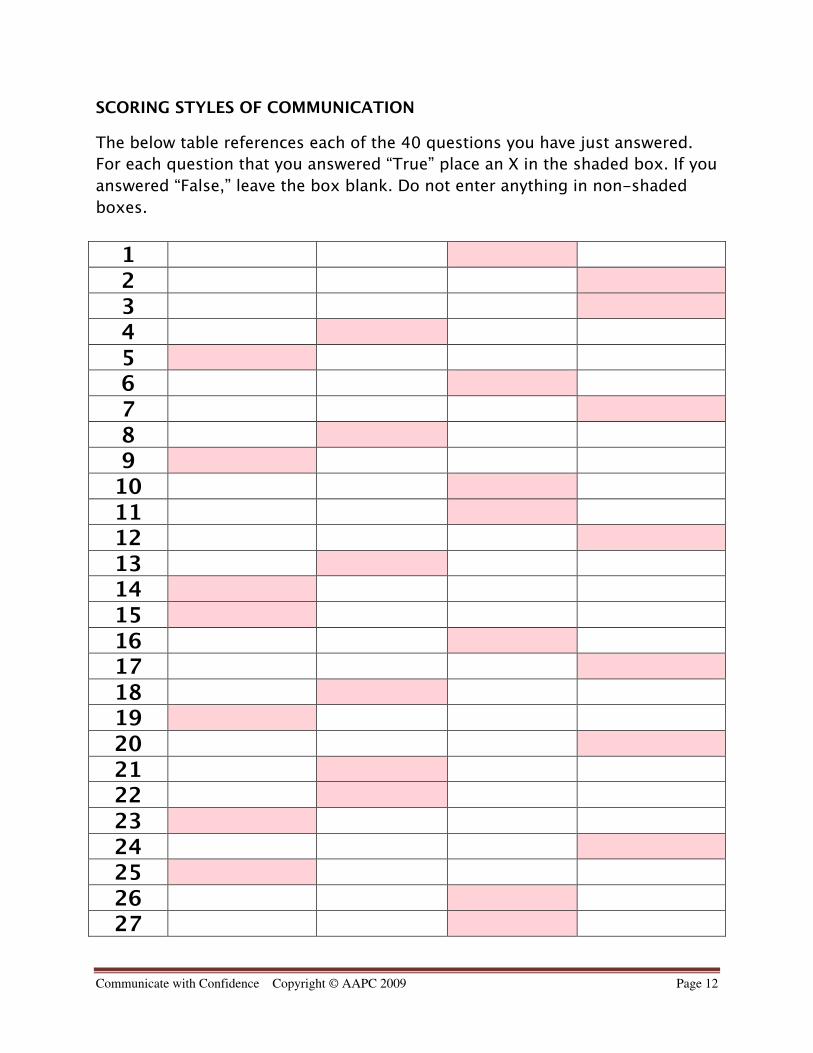
SCORING STYLES OF COMMUNICATION
The below table references each of the 40 questions you have just answered.
For each question that you answered “True” place an X in the shaded box. If you
answered “False,” leave the box blank. Do not enter anything in non-shaded
boxes.
1 2 3 4 56789
101112131415161718192021222324252627
Communicate with Confidence Copyright © AAPC 2009 Page 13
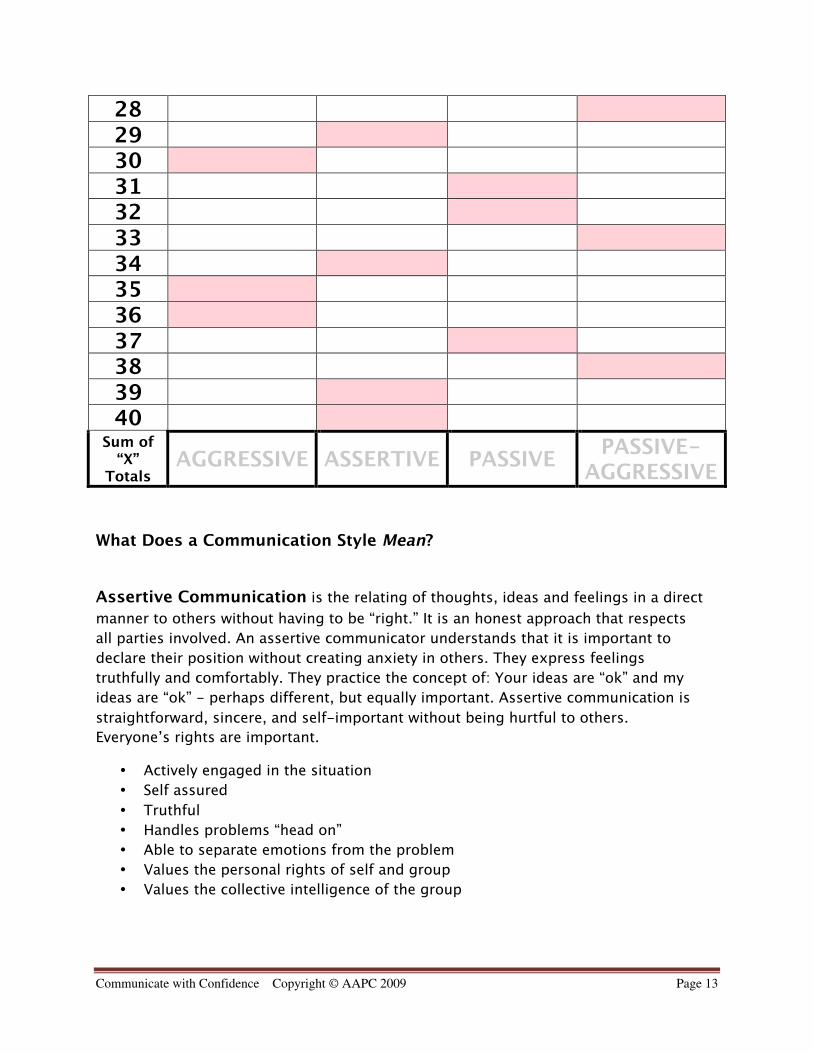
28293031323334353637383940
Sum of“X”
TotalsAGGRESSIVE ASSERTIVE PASSIVE
PASSIVE-AGGRESSIVE
What Does a Communication Style Mean?
Assertive Communication is the relating of thoughts, ideas and feelings in a direct
manner to others without having to be “right.” It is an honest approach that respects
all parties involved. An assertive communicator understands that it is important to
declare their position without creating anxiety in others. They express feelings
truthfully and comfortably. They practice the concept of: Your ideas are “ok” and my
ideas are “ok” - perhaps different, but equally important. Assertive communication is
straightforward, sincere, and self-important without being hurtful to others.
Everyone’s rights are important.
• Actively engaged in the situation
• Self assured
• Truthful
• Handles problems “head on”
• Able to separate emotions from the problem
• Values the personal rights of self and group
• Values the collective intelligence of the group
Communicate with Confidence Copyright © AAPC 2009 Page 14
Aggressive Communication is the relating of thoughts, ideas, and feelings in an
indirect manner to others while having to be “right.” It often incorporates the use of
antagonistic language, including name-calling and mockery. Aggressive
communication is insincere and self-important without regard to being hurtful to
others. Only the aggressor’s rights are important.
• Emotionally engaged in the situation - Angry when faced by problems
• Antagonistic
• Argumentative about opinion
• Self serving
• Demands personal rights
• Does not believe in a collective intelligence
Passive Communication is the act of not relating thoughts, ideas and feelings to
avoid dealing with direct confrontation. The passive communicator’s rights are
personally forfeited because they think that they do not have the right to an opinion or
they are not strong enough to assert one.
• Intentionally disengaged from the situation
• Unworthy
• Unconfident
• Avoids problems
• Forfeits personal rights
• Does not feel part of the collective intelligence
Passive-Aggressive Communication is the relating of thoughts, ideas, and
feelings in an indirect manner to others in order to be proven “right.” Like the Passive
communicator, Passive Aggressive communicators often say nothing to protect their
rights while employing less obvious Aggressive communication to demand those rights
returned to them. They often show resentment in non-verbal ways (i.e. procrastination,
pouting, complaining, and blaming others). Only the Passive Aggressor’s rights are
important, but they are taken in a roundabout way.
• Seems unengaged in the situation
• Calculating
• Self serving
• Demands personal rights by “showing” someone they are wrong
• Deals with problems in a roundabout manner
• Conniving
• Elects to side-line the collective intelligence
Communicate with Confidence Copyright © AAPC 2009 Page 15
What does this mean about me?
Very few people are all one or another style. Communication styles cannot
usually be based on one snap shot self assessment. A cumulative and honest
look at typical responses will help you to better recognize natural patterns. It is
not important to label a personality type as “bad” or “good.”
For example:
Aggressive style can work when:
• a quick decision has to be made• an emergency is happening• being right is crucial to an important fact• evoking a sense of competition on a team
Passive style can work when:
• the issue is inconsequential• the conflict will not change an outcome already in progress• the boss is not right - but is still the boss• the differing core belief has no impact on your own (i.e.: religion)
Passive Aggressive style can work when:
• a decision needs to be delayed• it makes sense to wait until tempers cool down
Communicate with Confidence Copyright © AAPC 2009 Page 16
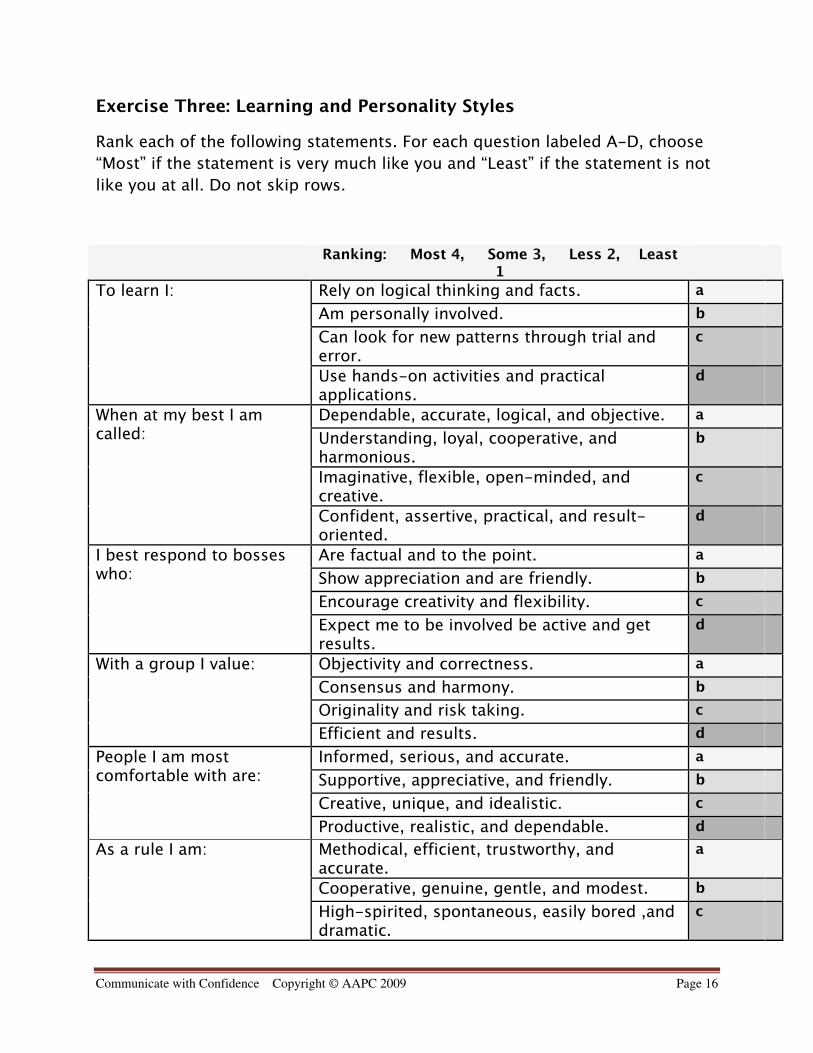
Exercise Three: Learning and Personality Styles
Rank each of the following statements. For each question labeled A-D, choose
“Most” if the statement is very much like you and “Least” if the statement is not
like you at all. Do not skip rows.
Ranking: Most 4, Some 3, Less 2, Least1
Rely on logical thinking and facts. a
Am personally involved. b
Can look for new patterns through trial anderror.
c
To learn I:
Use hands-on activities and practicalapplications.
d
Dependable, accurate, logical, and objective. a
Understanding, loyal, cooperative, andharmonious.
b
Imaginative, flexible, open-minded, andcreative.
c
When at my best I amcalled:
Confident, assertive, practical, and result-oriented.
d
Are factual and to the point. a
Show appreciation and are friendly. b
Encourage creativity and flexibility. c
I best respond to bosseswho:
Expect me to be involved be active and getresults.
d
Objectivity and correctness. a
Consensus and harmony. b
Originality and risk taking. c
With a group I value:
Efficient and results. d
Informed, serious, and accurate. a
Supportive, appreciative, and friendly. b
Creative, unique, and idealistic. c
People I am mostcomfortable with are:
Productive, realistic, and dependable. d
Methodical, efficient, trustworthy, andaccurate.
a
Cooperative, genuine, gentle, and modest. b
As a rule I am:
High-spirited, spontaneous, easily bored ,anddramatic.
c
Communicate with Confidence Copyright © AAPC 2009 Page 17
Straightforward, conservative, responsible. d
Collection of acts to determine the rightsolution.
a
Finding the solution that will please othersand me.
b
Brainstorming creative solutions that feelright.
c
When decision-making Ibelieve in:
Quickly choosing the most practical andrealistic solution.
d
Analytical. a
Caring. b
Innovative. c
In one word I am:
Productive. d
Reaching accurate and logical solutions. a
Being cooperative and respecting people’sfeelings.
b
Finding hidden connections and creativeoutcomes.
c
I "shine" when:
Making realistic practical and timely decisions. d
Gathering technical information and beingobjective.
a
Making personal connections and working ingroups.
b
Exploring possibilities creative tasks beingflexible.
c
When learning new thingsI like:
Producing results solving problems andmaking decision.
d
Sum of a:
Sum of b:
Sum of c:
Sum of d:
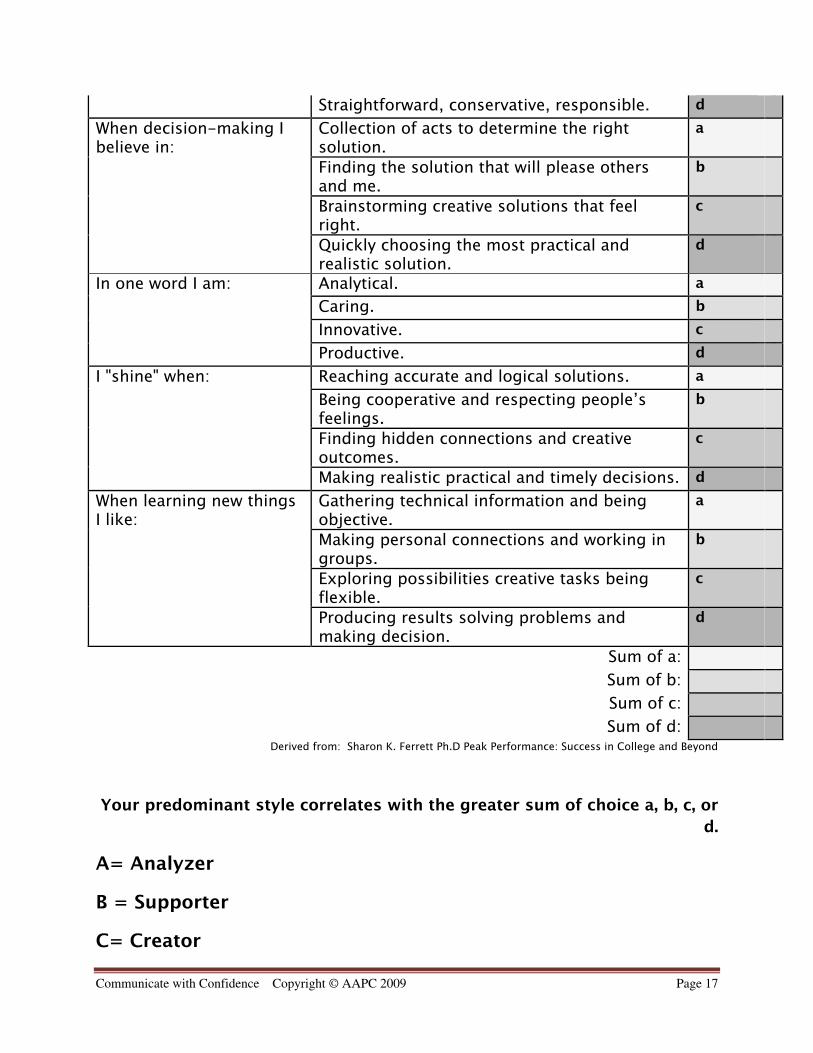
Derived from: Sharon K. Ferrett Ph.D Peak Performance: Success in College and Beyond
Your predominant style correlates with the greater sum of choice a, b, c, or
d.
A= Analyzer
B = Supporter
C= Creator

Communicate with Confidence Copyright © AAPC 2009 Page 18
D= Director
Learning and Personality Styles indicate your preference in working with others
in making decisions and in learning new information. Understanding your own
preference and the preferences of others can be most valuable in improving the
likelihood of effective communication.
Point to Ponder: Moving beyond your personal Learning and Personality Styles
what style does your physician display?
Communicate with Confidence Copyright © AAPC 2009 Page 19
Analyzers: “Let me examine that working.”
Common Traits Communication with Physician
Analyzers often requires Coders to:
• Careful
• Commonsensical
• Detached
• Detailed-Oriented
• Exact
• Hesitant
• Methodical
• Restricted
• Sudden
• Undemonstrative
• Unimaginative
• Use facts
• Show the source document on
rules
• Use rationales
• Be organized detached and calm
• Be professionally impersonal
• State facts concisely
Supporters: “ Why does that work?”
Common Traits Communication with Physician
Supporters often requires Coders to:
• Easy going
• Faithful
• Helpful
• Kind
• Naïve
• Passive
• Sensitive
• Slower acting
• Sympathetic
• Tactful
• Thankful
• Be genuine
• Be personable
• Be pleasant
• Create a calm environment
• Create familiarity
• Focus on personal values
• Listen with caring
Communicate with Confidence Copyright © AAPC 2009 Page 20
Creators: “ What if it worked like ….this?”
Common Traits Communication with Physician
Creators often requires Coders to:
• Artistic
• Contradictory
• Disjointed
• Eager
• Imaginative
• Impractical
• Intolerant
• Original
• Pioneering
• Romantic
• Spontaneous
• Undependable
• Be engaged
• Be excited
• Be flexible
• Embrace change
• Focus on imaginative ideas
• Talk about potential
Directors: “I have taken that apart to see how it works.”
Common Traits Communication with Physician
Directors often requires Coders to:
• Antagonistic
• Controlling
• Dynamic
• In charge
• Overwhelming
• Persistent
• Results driven
• Self-assured
• Self-confident
• Focus on accomplishment
• Focus on outcome
• Forfeit control
• Make no excuses
• Set milestones and timelines
• Take responsibility
Communicate with Confidence Copyright © AAPC 2009 Page 21
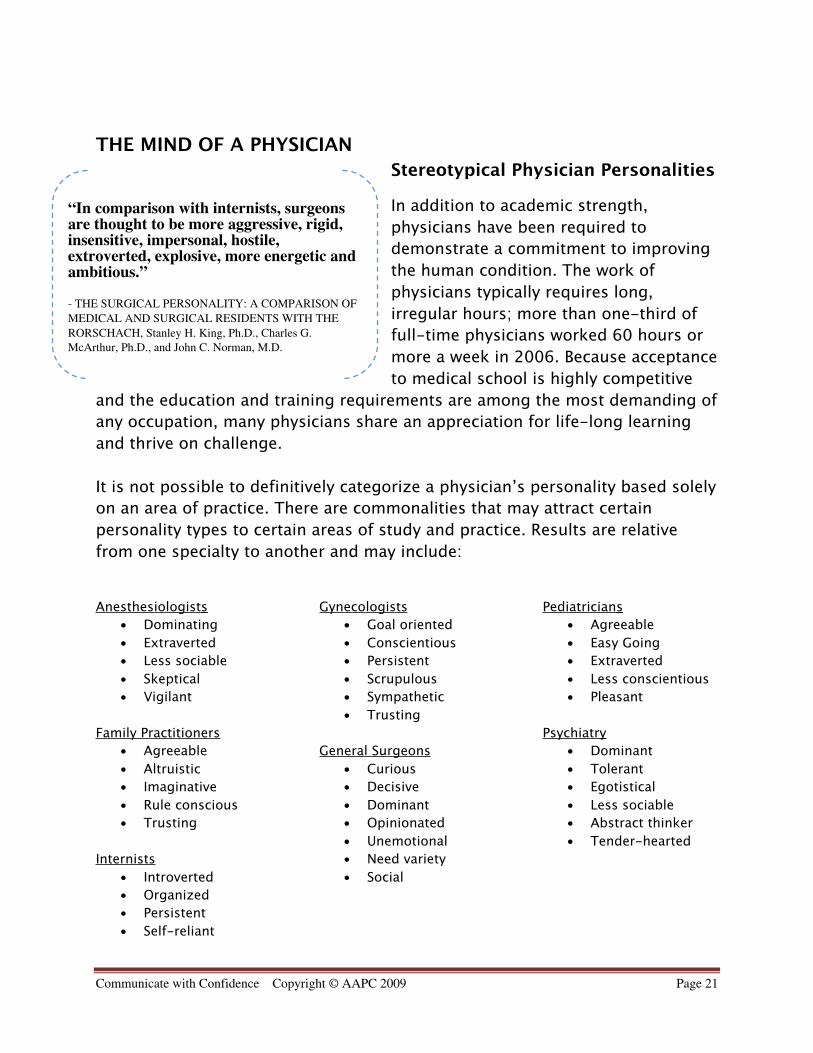
THE MIND OF A PHYSICIAN
Stereotypical Physician Personalities
In addition to academic strength,
physicians have been required to
demonstrate a commitment to improving
the human condition. The work of
physicians typically requires long,
irregular hours; more than one-third of
full-time physicians worked 60 hours or
more a week in 2006. Because acceptance
to medical school is highly competitive
and the education and training requirements are among the most demanding of
any occupation, many physicians share an appreciation for life-long learning
and thrive on challenge.
It is not possible to definitively categorize a physician’s personality based solely
on an area of practice. There are commonalities that may attract certain
personality types to certain areas of study and practice. Results are relative
from one specialty to another and may include:
Anesthesiologists
• Dominating
• Extraverted
• Less sociable
• Skeptical
• Vigilant
Family Practitioners
• Agreeable
• Altruistic
• Imaginative
• Rule conscious
• Trusting
Internists
• Introverted
• Organized
• Persistent
• Self-reliant
Gynecologists
• Goal oriented
• Conscientious
• Persistent
• Scrupulous
• Sympathetic
• Trusting
General Surgeons
• Curious
• Decisive
• Dominant
• Opinionated
• Unemotional
• Need variety
• Social
Pediatricians
• Agreeable
• Easy Going
• Extraverted
• Less conscientious
• Pleasant
Psychiatry
• Dominant
• Tolerant
• Egotistical
• Less sociable
• Abstract thinker
• Tender-hearted
“In comparison with internists, surgeonsare thought to be more aggressive, rigid,insensitive, impersonal, hostile,extroverted, explosive, more energetic andambitious.”
- THE SURGICAL PERSONALITY: A COMPARISON OF
MEDICAL AND SURGICAL RESIDENTS WITH THE
RORSCHACH, Stanley H. King, Ph.D., Charles G.
McArthur, Ph.D., and John C. Norman, M.D.
Communicate with Confidence Copyright © AAPC 2009 Page 22
Derived from: Borges NJ Osman WR . 2000 J Vocational Behavior 58: 22-35 Borges NJ Savickas MI. 2002 J Career
Assessment 10: 362-380
Appreciating Physician Development
In order to better understand and communicate with physicians, coders must
appreciate the dedication, sacrifice and time spent in their professional
development.
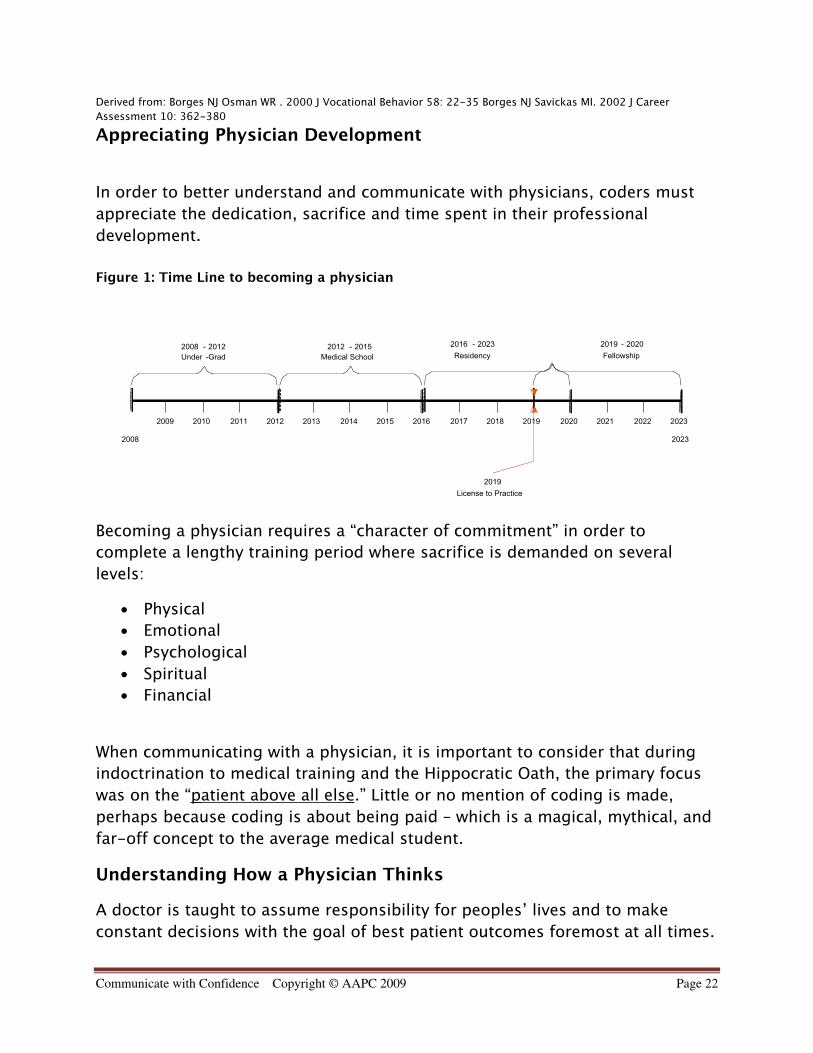
Figure 1: Time Line to becoming a physician
2008 2023
2009 2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021 2022 2023
2008 - 2012
Under -Grad
2012 - 2015
Medical School
2019 - 2020
Fellowship
2016 - 2023
Residency
2019
License to Practice
Becoming a physician requires a “character of commitment” in order to
complete a lengthy training period where sacrifice is demanded on several
levels:
• Physical
• Emotional
• Psychological
• Spiritual
• Financial
When communicating with a physician, it is important to consider that during
indoctrination to medical training and the Hippocratic Oath, the primary focus
was on the “ patient above all else .” Little or no mention of coding is made,
perhaps because coding is about being paid – which is a magical, mythical, and
far-off concept to the average medical student.
Understanding How a Physician Thinks
A doctor is taught to assume responsibility for peoples’ lives and to make
constant decisions with the goal of best patient outcomes foremost at all times.
Communicate with Confidence Copyright © AAPC 2009 Page 23
The mind of a physician constantly classifies information; prioritizing,
reclassifying and reprioritizing in an effort to make the best decision -- often
under extreme intellectual pressure. Doctors often don’t see coding as having
an effect on the patient outcome, making it almost always classified as a very
low priority in everyday existence. Physicians often believe there is no margin
for error in caring for their patients; all patients expect perfection, which
physicians strive for. Many are already under a greater than average level of
stress - before a coder drops the following bomb:
“Doc--Your total effort may never be paid.”
Ouch!
For many physicians, learning that no matter how hard they work, how hard
they try, how much effort they have given for the patient may not correlate with
the coding and payment is difficult. This can lead to a barriers in the coder-
physician working relationship and translate to communication problems if the
coder is unaware of the conflict. The personality style of the physician may
cause him or her to react to a coder in an unpleasant manner. A coder must
remember that a physician is not there to build or tear down the coder’s self-
esteem, and usually has no actual investment in doing either. At different
times, a physician will not always consider or recognize the work of a coder as a
major priority. It should not represent a blow to a coder’s personal self-esteem.
It is never about you, unless YOU make it about you!
THE CODER-PHYSICIAN WORKING ALLIANCE
Top 10 Coder Mantras for a Successful Coder-Physician Working
Alliance
1. I know my job and prepare myself with the facts in all coding situations.
2. My confidence is based on my choice to feel confident. I am confident.
3. I know my personality strengths/weakness. I temper my delivery and
response.
4. Coding is healthcare business and is not “personal.” I don’t get my
feelings hurt.
5. Physicians are often overworked. I ask for their time wisely.
Communicate with Confidence Copyright © AAPC 2009 Page 24
6. I make coding rules easy for physicians so their focus stays on patient
care.
7. Physicians don’t have time to see what I do. I self-start & do not need
praise.
8. I am pleasant, calm and in control of my feelings. No one can “make” me
upset.
9. Asking a question does not undermine my value. When I don’t know I
ask.
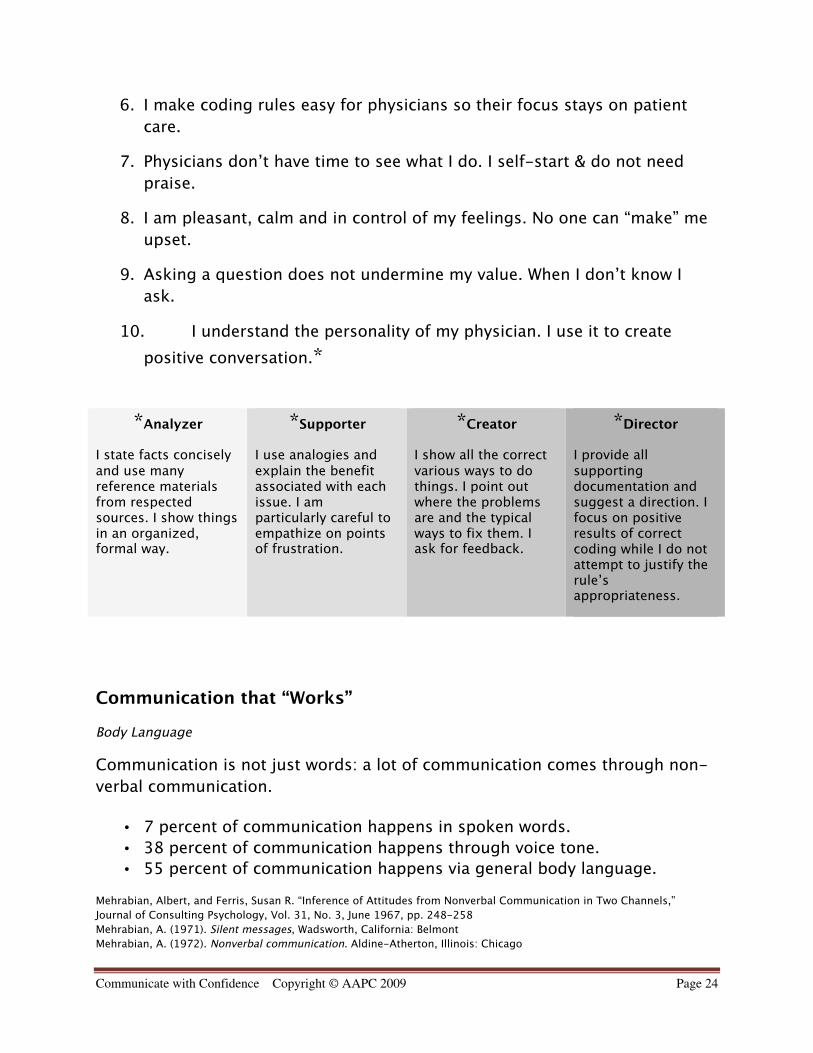
10. I understand the personality of my physician. I use it to create
positive conversation.*
*Analyzer
I state facts conciselyand use manyreference materialsfrom respectedsources. I show thingsin an organized,formal way.
*Supporter
I use analogies andexplain the benefitassociated with eachissue. I amparticularly careful toempathize on pointsof frustration.
*Creator
I show all the correctvarious ways to dothings. I point outwhere the problemsare and the typicalways to fix them. Iask for feedback.
*Director
I provide allsupportingdocumentation andsuggest a direction. Ifocus on positiveresults of correctcoding while I do notattempt to justify therule’sappropriateness.
Communication that “Works”
Body Language
Communication is not just words: a lot of communication comes through non-
verbal communication.
• 7 percent of communication happens in spoken words.
• 38 percent of communication happens through voice tone.
• 55 percent of communication happens via general body language.
Mehrabian, Albert, and Ferris, Susan R. “Inference of Attitudes from Nonverbal Communication in Two Channels,”
Journal of Consulting Psychology, Vol. 31, No. 3, June 1967, pp. 248-258
Mehrabian, A. (1971). Silent messages, Wadsworth, California: Belmont
Mehrabian, A. (1972). Nonverbal communication. Aldine-Atherton, Illinois: Chicago
Communicate with Confidence Copyright © AAPC 2009 Page 25
Controlling your body language can help to ensure effective communication.
There is some study to suggest that mimicking the body stance and pose of the
person you are conversing with may subconsciously put them at ease. Example:
If you notice that the physician is sitting with legs crossed, resting elbows on
the table with head resting on palms, you may try sitting across the table with
legs crossed, elbows on table and arms flat or folded on the table. If you notice
that the physician is standing with hands on hips you may try doing the same.
As a note of caution, it is important to not make an overt gesture or to
unnaturally position your body because this may have a reverse affect - making
you appear manipulative or insincere, or at least: uncomfortable. The following
body language mistakes to avoid are:
• Arms crossed: You are defensive.
• Constant eye contact: You are aggressive.
• Fidgeting: You are bored or impatient
• Hunched Posture: You lack confidence.
• Little eye contact: You have low interest or lack confidence.
• Rubbing your nose or mouth: You are lying.
• Tapping: You are impatient or nervous.
• Touching your face or hair: You are timid.
• Watching the time: You are anxious to move on to something else.
Tips for tricky communication situations:
Verbal Attack:
The key to bridging this gap is to not accelerate the situation. Breathe.
Remember that it is rarely YOU being yelled at, it is the situation. Do not allow
yourself to become upset, you have a choice to steer the conversation in a
better direction or to make it worse! If a physician is upset and angry, yelling
may be their learned method of reacting to these emotions –their way of
“letting it out.” Empathizing with someone like this can help move the direction
of the conversation to a move positive arena.
• “I understand that you are upset.”
• “I’d want to yell too if I worked as hard as you do and this was happening
to me.”
• “This is an upsetting situation for you. I’m sorry you feel this way.”

Communicate with Confidence Copyright © AAPC 2009 Page 26
• “I know this is distressing. Would you prefer to have this conversation
later?”
Note: Do not allow yourself to become verbally abused. In some situations your
best reaction is no reaction and ending the conversation.
- “What you have to say is important to me, but I can’t hear past your
yelling. I feel afraid. May we continue this later when you feel less angry?”
Sometimes, this honest response is enough to sober the situation immediately.
If not, it will often set the stage for a better conversation in the future.
Communicate with Confidence Copyright © AAPC 2009 Page 27
Defusing Verbal Attacks:
Listen. Whenever you are verbally attacked let the physician know that you arenot going to fight them and that you are trying to understand how they arefeeling.
Example:Physician – “You can’t be serious! This is too a CONSULTATION! Howon earth can you tell me otherwise?”
Less Effective Coder Response – “Let me tell you why it is! A consultrequires….”
Effective Coder Response – “Tell me why you feel this way. I’minterested in your thought process on this.”
Don’t need to hear you are “right.” Some people have a natural inclination towant to “win” if an argument arises. If you find yourself in a confrontation,remember that any “counterattack” you launch serves only your ego. It isunlikely that you will often hear the words: “You are right.” Reactingemotionally will not change the situation or help you achieve your goal from theconversation.
Example:Physician – “You can’t be serious! This is too a CONSULTATION! Howon earth can you tell me otherwise?”
Less Effective Coder Response – “Well, it IS wrong. It is FRAUD if youkeep marking these visits as consults.”
Effective Coder Response – “I agree with you that it is confusing.Sometime the verbiage used in reimbursement rules is very differentfrom how the same term is used clinically. Let me show you how tocode these so that you can bill for a consultation every time thecoding rules allow it.”
Have thick skin. A simple and effective method to diffuse a verbal attack is topay no attention to it. By showing no response, the likelihood of continuance isdiminished.
Example:
Communicate with Confidence Copyright © AAPC 2009 Page 28
Physician – “You are ridiculous! This is a consultation!”
Less Effective Coder Response – “I am not ridiculous! Your coding isincorrect.”
Effective Coder Response – “Unfortunately the rules on billingconsultations can seem a bit ridiculous. Let me show you the rulehere in the book…”
Be Kind. One of the most powerful tactics for defusing an aggressor is a sincere“I’m sorry.” This is not always easy to do when you are being confronted oversomething that is not directly your doing.
Example:Physician – “You can’t be serious! This is too a CONSULTATION! Howon earth can you tell me otherwise?”Less Effective Coder Response – “I didn’t make the rules! I just followthem.”
Effective Coder Response – “I’m sorry this is confusing. Iunderstand why you feel this way.”
Agree. It is very difficult to continue yelling at something when they use threesimple words: “You are right.”
Example:Physician – “You can’t be serious! This is too a CONSULTATION! Howon earth can you tell me otherwise?”
Less Effective Coder Response – “You are not correct on this, Dr.”
Effective Coder Response – “I agree with you. The coding rules aredifferent from clinical rules; what do you suggest we do to keep youout of harm’s way? ”
Give away “control.” Physicians are trained to be in complete control duringcrisis situations. It is a difficult thing to feel as if they have no control. It can behelpful to re-word statements from absolutes to phases that put them incontrol of their own actions.
Example:Physician – “You can’t be serious! This is too a CONSULTATION!How on earth can you tell me otherwise?”
Communicate with Confidence Copyright © AAPC 2009 Page 29
Less Effective Coder Response – “This is the way that it is. You haveto do it this way.”
Effective Coder Response – “You can keep yourself out of harm’sway if you want to and code according to rules or we couldchallenge the rules if you would like to. Would you suggest that wewrite a letter to the medical association about this or to theinsurance companies we contract with?”
Divert Negativity. Redistributing the tension between you and the physician canallow the physician to place the “blame” elsewhere, which allows you to moreeffectively come to mutual resolution and agreement.
Example:Physician – “You can’t be serious! This is too a CONSULTATION! Howon earth can you tell me otherwise?”
Less Effective Coder Response – “I am telling you the right way to dothis.”
Effective Coder Response – “The people who make these rules mustnever have practiced the art of medicine! They make us comply withthem, though. The good news is that I think I can explain this so thatyou confidently bill for a consultation every time they will allow it.”
Initiating a difficult conversation:
The following steps are a good guide to follow when initialing a conversation
that you believe will not be received favorably.
- Ask. Is this is a good time to talk?
- Be direct. Prepare a short statement in advance that gets right to thepoint.
- Be quiet and listen. Allow the physician to respond completely, even ifdefensively.
- Sympathize. Try to understand the physician’s perspective and makeeffort to show it.
- Empathize. Express that you realize how hard this is; that it is hard foryou too.

Communicate with Confidence Copyright © AAPC 2009 Page 30
- Assess. Is the physician is ready for you to expand on your openingstatement?
1. A sincere (“Tell me more”), non-angry question (“How can you saythat?”)
2. Ask: Are you ready for me to expand on this? No: wait. Yes:continue
- Commence the conversation with detail. Explain the rationale, reward,and risk.
CONCLUSION
Level of education, experience and talent aside — the best coders and billers
have also mastered the art of communicating with physicians in ways that
almost always produce positive results. Your physician needs coders. Your
performance is often an important key to the financial success of the medical
practice. The purpose this course has been to provide the framework for
persuasive communication skills that allow a coder manage challenging
situations with physicians and turn them into a catalyst for positive change.
From understanding yourself, to understanding the physician, the coder can
communicate coding concepts that are, for many physicians, a foreign language
- with confidence.
About the Authors:
Lorraine J. Sivak has over twenty four years of experience as a medical coder.
She is the former AAPC Local Chapter President of the Ft Lauderdale chapter
and currently manages her husband’s outpatient psychiatric practice in Duluth,
Minnesota.
Dr. Joseph J. Sivak MD is a board certified General Psychiatrist with seventeen
years experience treating patients. He is an assistant professor at the University
of Minnesota at Duluth College of Pharmacy and School of Medicine and
currently operates a psychiatric outpatient practice in the Twin Ports area of
Duluth and Superior WI.
1/15/2009
1
Communicate With Confidence to Physicians:
Coding as a Second Language
Add Presenter Name Here
Agenda
9:00 – 10: 45 am
Lecture and Coder Self Assessment
10:45 – 11: 00 am
Break
11:00 – 12:00 pm
Lecture and Group Exercises
Communication Cornerstones
Effective Communication between a coder and a physician:
Coder-Self-Awareness What can I learn about me? Locus of Control Style of Communication Learning and Personality Style
Understanding the Mind Of a Physician Typical personality The making-of a physician Why a physician thinks as he/she does
The Coder-physician Working Alliance Mantras for success Communication that WORKS
1/15/2009
2
Coder-Self-Awareness
Understanding your strengths and weaknesses.
Increased awareness:
Of natural listening and response styles
Ability to see beyond communication obstacles
Modify responses as needed for the desired results
Coder-Self-Awareness: Locus of Control
Turn to the Locus of Control Worksheet in your workshop book.
!10 minutes. Please read each question carefully.
Choose A. or B. for each question.
Chose your answer by your first impression.
Do not “over think” the questions.
Locus of Control: Self Assessment
For each question you answered “B” give yourself one point.
0 1 2 3 4 5 6 7 8 9 10 11 12 13
Internal Locus of Control
“Luck” is when opportunity
meets preparation. I create
my own luck because I work
to generate opportunity and
prepare myself for it.
External Locus of Control
“Fate” and forces outside of
my control have direct power
over what happens to me.
You can’t control luck.
1/15/2009
3
Locus of Control: What does it mean?
Internal locus of control
More Likely to…
External locus of control
More Likely to…
• Tolerate vague situations • Prefer “Black & White” rules
• Learn from their mistakes
• Prefer games based on skill
• Suffer from depression
• Prefer games based on chance
Internalizing the External Locus of Control
Life is 1% what happens to you & 99% how you
choose to feel about it.
Write down every option in your current situation.
Even if you don’t like the choices, remember you have them
Decide on the best course of action to meet your goals y g
Practice expanding your mind to all open possibilities
Replace “I HAVE to…” or “I NEED to…” with: “I CHOSE to…”
Coder-Self-Awareness: Style of Communication
Turn to the Styles of Communication Worksheet in your workshop book.
!10 minutes. Please read each question carefully.
Choose True or False for each question.
Chose your answer by your first impression.
Do not “over think” the questions.
1/15/2009
4
Style of Communication: Self Assessment
For each question that is True place an “X” in the shaded
box on the row that correlates with the number of the question.
If you answered False leave the row blank.
Count the number of “X” marks you have in each column.
The column with the largest number is your dominant Style of Communication
Sum of
“X”
Totals
5AGGRESSIVE
7ASSERTIVE
2PASSIVE
1PASSIVE!AGGRESSIVE
What does this assessment mean?
Very few people are all one or another style.
Communication styles cannot be based on one self assessment.
A cumulative look and awareness allow a person to better recognize natural patterns of communication.
Let’s take a closer Look…
Communication Style: Assertive
Assertive Communication is the relating of thoughts,
ideas and feelings in a direct manner to others without
having to be “right”. I’m ok. You’re ok.
Actively engaged in the situation
Self assured
Truthful
Handles problems “head on”
Able to separate emotions from the problem
Values the personal rights of self and group
Values the collective intelligence of the group
1/15/2009
5
Aggressive Communication is the relating of thoughts, ideas and feelings in an indirect manner to others while having to be “right”. Only the aggressor’s rights are important.
Emotionally engaged in the situation
Antagonistic
Communication Style: Aggressive
g
Argumentative about opinion
Self serving
Demands personal rights
Does not believe in a collective intelligence
Communication Style: Passive
Passive Communication is the act of not relating
thoughts, ideas and feelings to avoid dealing with direct
confrontation. The passive communicator’s rights are
personally forfeited.
Intentionally disengaged from the situation
Unworthy
Unconfident
Avoids problems
Forfeits personal rights
Does not feel part of the collective intelligence
Passive-Aggressive Communication is the relating of
thoughts, ideas and feelings in an indirect manner to others
in order to be proven “right”. Only the Passive Aggressor’s
rights are important, but they are taken in a roundabout
way.
Communication Style: Passive!Aggressive
Seems unengaged in the situation
Calculating
Self serving
Demands rights by “showing” someone else wrong
Deals with problems in a roundabout manner
Conniving
Elects to side-line the collective intelligence
1/15/2009
6
Styles: Not "Good" or "Bad"
Aggressive style can work when:
a quick decision has to be made
an emergency is happening
being right is crucial to an important fact
evoking a sense of competition on a team
Passive style can work when:
the issue is inconsequential
the conflict will not change an outcome already in progress
the boss is not right---but is still the boss
the differing core belief has no impact on your own (i.e.: religion)
Passive Aggressive style can work when:
a decision needs to be delayed
it makes sense to wait until tempers cool down
Coder-Self-Awareness: Learning and Personality Styles
Turn to the Learning and Personality Styles Worksheet in your workshop book.
!10 minutes. Please read each question carefully.
Choose “4- Most” if the statement is very much like you. y y
Choose “1- Least” if the statement is not like you at all.
Do not skip rows.
Chose your answer by your first impression.
Do not “over think” the questions.
Add together the total sum for each “a” choice, each “b” choice, each “c” choice and each “d” choice.
Your predominant style correlates with the greater sum
of choice a, b, c, or d.
Learning and Personality Style: Self Assessment
A= Analyzer
B = Supporter
C= Creator
D= Director
1/15/2009
7
What does this assessment mean?
Very few people are all one or another style.
Very few people are equally all styles.
Personality styles cannot be based on one self y yassessment.
A cumulative look and awareness allow a person to better recognize natural personality traits.
Let’s take a closer Look…
Analyzers:
“Let me examine that working.”
Common Traits Physician Analyzers require Coders to:
Careful
Commonsensical
Detached
Detailed-Oriented
Use facts
Show the source document on rules
Use rationales
Be organized detached and calm Detailed Oriented
Exact
Hesitant
Methodical
Restricted
Sudden
Undemonstrative
Unimaginative
Be organized detached and calm
Be professionally impersonal
State facts concisely
Supporters:
“Why does that work?”
Common Traits Physician Supporters requires coders to:
Easy going
Faithful
Helpful
Be genuine
Be personable
Be pleasant
Kind
Naïve
Passive
Sensitive
Slower acting
Sympathetic
Tactful
Thankful
Create a calm environment
Create familiarity
Focus on personal values
Listen with caring
1/15/2009
8
Creators:
“What if it worked like ….this?”
Common Traits Physician Creators require Coders to:
Artistic
Contradictory
Disjointed
Eager
I i ti
Be engaged
Be excited
Be flexible
Embrace change
F i i ti id Imaginative
Impractical
Intolerant
Original
Pioneering
Romantic
Spontaneous
Undependable
Focus on imaginative ideas
Talk about potential
Directors:
“I have taken that apart to see how it works.”
Common Traits Physician Directors require Coders to:
Antagonistic
Controlling
Dynamic
In charge
Focus on accomplishment
Focus on outcome
Forfeit control
Make no excusesg
Overwhelming
Persistent
Results driven
Self-assured
Self-confident
Set milestones and timelines
Take responsibility
The Mind of a Physician
Committed to improving the human condition
Typically work long, irregular hours
More than 1/3 of full-time physicians work 60+ hours a week
Training is among the most demanding of any occupation
Appreciate life-long learning
D t t “ h t f it t” h Demonstrates a “character of commitment” wheresacrifice is demanded on several levels:
Physical
Emotional
Psychological
Spiritual
Financial
1/15/2009
9
Sterotypical Personality Traits
Anesthesiologists
Dominating
Extraverted
Less sociable
Skeptical
Vigilant
Family Practitioners
Agreeable
Gynecologists
Goal oriented
Conscientious
Persistent
Scrupulous
Sympathetic
Trusting
Pediatricians
Agreeable
Easy Going
Extraverted
Less conscientious
Pleasant
Psychiatry
Important note: It is not possible to categorize a personality based solely on an area of practice.
Altruistic
Imaginative
Rule conscious
Trusting
Internists
Introverted
Organized
Persistent
Self-reliant
General Surgeons
Curious
Decisive
Dominant
Opinionated
Unemotional
Need variety
Social
y y
Dominant
Tolerant
Egotistical
Less sociable
Abstract thinker
Tender-hearted
• Derived from: Borges NJ Osman WR . 2000 J Vocational Behavior 58: 22-35 Borges NJ Savickas MI. 2002 J Career Assessment 10: 362-380
Patient Above All Else (…even coding)
I swear by Apollo, Asclepius, Hygieia, and Panacea, and I take to witness all the gods, all the goddesses, to keep according
to my ability and my judgment, the following Oath.
To consider dear to me, as my parents, him who taught me this art; to live in common with him and, if necessary, to share my goods with him; To look upon his children as my own brothers, to teach them this art.
I will prescribe regimens for the good of my patients according to my ability and my judgment and never do harm to anyone.
I will not give a lethal drug to anyone if I am asked, nor will I advise such a plan; and similarly I will not give a woman a pessary to cause an abortion.
B t I ill pr r th p rit f lif nd rtBut I will preserve the purity of my life and my arts.
I will not cut for stone, even for patients in whom the disease is manifest; I will leave this operation to be performed by practitioners, specialists in this art.
In every house where I come I will enter only for the good of my patients, keeping myself far from all intentional ill-doing andall seduction and especially from the pleasures of love with women or with men, be they free or slaves.
All that may come to my knowledge in the exercise of my profession or in daily commerce with men, which ought not to be spread abroad, I will keep secret and will never reveal.
If I keep this oath faithfully, may I enjoy my life and practice my art, respected by all men and in all times; but if I swerve from it or violate it, may the reverse be my lot.
- HIPPOCRATIC OATH- HIPPOCRATES- FATHER OF MEDICINE, c460-c367 b.c. Greek Physician
Physican Development
High school and Undergrad: needs outstanding grades to get accepted for further training
70-90% of those in pre-med will not be accepted to medical school and will change career gpaths
Medical School: Financial sacrifice becomes apparent, still secondary to the commitment
Must memorize, process and integrate thousands of facts and concepts every 4-6 weeks
Typically none of those facts or concepts involve coding
Typically there is no orientation to the coding process in medical or pre-medical education
Medical school:
Average student financial debt in 2007 was $139,517
75.5% of students graduate with debt of at least $100,000
87.6% of graduating students have outstanding loans
1/15/2009
10
“Pssst….Doc--Your total effort may never be paid.”
Doctors don’t see coding as having an effect on the patient outcome, making it classified as a very low priority
Learning that no matter how hard they work, how hard they try, how much effort they have given for the patient may not correlate with coding and payment is difficultmay not correlate with coding and payment is difficult.
This can lead to a barriers in the coder-physician working relationship
Top 10 Coder Mantras for a Successful Coder Physician
Working Alliance
I know my job and prepare myself with the facts in all coding situations.
My confidence is based on my choice to feel confident. I am confident.
I know my personality strengths/weakness. I temper my delivery and response.
Coding is healthcare business and is not “personal”. I don’t get my feelings hurt.
Physicians are often overworked. I ask for their time wisely.
I make coding rules easy for physicians so their focus stays on patient care. I make coding rules easy for physicians so their focus stays on patient care.
Physicians don’t have time to see what I do. I self-start & do not need praise.
I am pleasant, calm and in control of my feelings. No one can “make” me upset.
Asking a question does not undermine my value. When I don’t know I ask.
I understand the personality of my physician. I use it to create positive conversation.*
Personality and Positive Communication
I understand the personality of my physician. I use it to create positive conversation.
*Analyzer
I state facts concisely and
usemany reference
*Supporter
I use analogies and
explain the benefit
*Creator
I show all the correct
various ways to do things
*Director
I provide all supporting
documentation anduse many reference
materials from respected
sources. I show things in
an organized, formal way.
explain the benefit
associated with each
issue. I am particularly
careful to empathize on
points of frustration.
various ways to do things
and I point out where the
problems are and the
typical ways to fix them.
I ask for feedback.
documentation and
suggest a direction. I
focus on positive results
of correct coding and do
not attempt to justify the
rule’s appropriateness.
1/15/2009
11
Body Language
Communication is not just words
7% of communication happens in spoken words.
38% of communication happens through voice tone.
55% of communication happens via general body language.
“There is something about you I like…”
Mimicking the body stance of a person may subconsciously put them at ease
Physician is sitting with legs crossed, resting elbows on the table with head resting on palms, you may try sitting across the table with legs crossed, elbows on table and arms flat or folded on the table.
Physician is standing with hands on hips you may try doing the same.
Must not feel or look unnatural or it may appear insincere
Body Language Mistakes
Arms crossed: You are defensive.
Constant eye contact: You are aggressive.
Fidgeting: You are bored or impatient
Hunched Posture: You lack confidence.
Little eye contact: You have low interest or lack confidence.
R bbi th Y l i Rubbing your nose or mouth: You are lying.
Tapping: You are impatient or nervous.
Touching your face or hair: You are timid.
Watching the time: You are anxious to move on to something else.
Verbal Attack
Words to soften the situation: “I understand that you are upset”
“I’d want to yell too if I worked as hard as you do and this was happening to me”
“This is an upsetting situation for you. I’m sorry you feel this way.”
“I know this is distressing. Would you prefer to have this conversation later?”
Do not allow yourself to become verbally abused.
In some situations your best reaction is no reaction and ending the conversation.
“What you have to say is important to me, but I can’t hear past your yelling. I feel afraid. May we continue this later when you feel less angry?”
1/15/2009
12
Defusing Verbal Attacks
Listen. Whenever you are verbally attacked let the physician know that you are
not going to fight them and that you are trying to understand how they are feeling.
Physician – “You can’t be serious! This is too a CONSULTATION! How on earth can you tell me otherwise?” y
Less Effective Coder Response – “Let me tell you why it is! A consult requires….”
Effective Coder Response – “Tell me why you feel this way. I’m interested in your thought process on this.”
Defusing Verbal Attacks
Don’t need to hear you are “right”. Some people have a natural inclination to want to “win” if an argument
arises. If you find yourself in a confrontation, remember that any “counterattack” serves only your ego.
Physician – “You can’t be serious! This is too a CONSULTATION! How on earth can you tell me otherwise?” y
Less Effective Coder Response – “Well, it IS wrong for coding. It is FRAUD if you keep marking these visits as consults.”
Effective Coder Response – “I agree with you that it is confusing. Sometime the verbiage used in reimbursement rules is very different from how the same term is used clinically. Let me show you how to code these so that you can bill for a consultation every time the coding rules allow it.”
Defusing Verbal Attacks
Have thick skin. A simple and effective method to diffuse a verbal attack is to pay no
attention to it. By showing no response, the likelihood of continuance is diminished.
Physician – “You are ridiculous! This is a consultation!”
Less Effective Coder Response – “I am not ridiculous! Your coding is incorrect.”
Effective Coder Response – “Unfortunately the rules on billing consultations seem a bit ridiculous until you go over them completely. Let me show you…”
1/15/2009
13
Defusing Verbal Attacks
Be Kind. One of the most powerful tactics for defusing an aggressor is a sincere
“I’m sorry.” This is not always easy to do when you are being confronted over something that is not directly your doing.
Physician – “You can’t be serious! This is too a CONSULTATION! How on earth can you tell me otherwise?” y
Less Effective Coder Response – “I didn’t make the rules! I just follow them.”
Effective Coder Response – “I’m sorry this is confusing. I understand why you feel this way.”
Defusing Verbal Attacks
Agree. It is very difficult to continue yelling at something when they use three
simple words: “You are right.”
Physician – “You can’t be serious! This is too a CONSULTATION! How on earth can you tell me otherwise?”
Less Effective Coder Response – “You are not correct on this, Dr.”
Effective Coder Response – “I agree with you. The coding rules are different from clinical rules; what do you suggest we do to keep you out of harm’s way? ”
Defusing Verbal Attacks
Give away “control”. Physicians are trained to be in complete control during crisis situations. It
is a difficult thing to feel as if they have no control. It can be helpful to re-word statements from absolutes to phases that put them in control of their own actions.
Physician – “You can’t be serious! This is too a CONSULTATION! How on earth can you tell me otherwise?”
Less Effective Coder Response – “This is the way that it is. You have to do it this way.”
Effective Coder Response – “You can keep yourself out of harm’s way if you want to and code according to rules or we could challenge the rules if you would like to. Would you suggest that we write a letter to the medical association about this or to the insurance companies we contract with?”
1/15/2009
14
Defusing Verbal Attacks
Divert Negativity. Deflecting the tension between you and the physician can allow the
physician to place the “blame” elsewhere, which allows you to more effectively come to mutual resolution and agreement.
Physician – “You can’t be serious! This is too a CONSULTATION! How on earth can you tell me otherwise?”y
Less Effective Coder Response – “I am telling you the right way to do this.”
Effective Coder Response – “The people who make these rules must never have practiced the art of medicine! They make us comply with them, though. The good news is that I think I can explain this so that you confidently bill for a consultation every time they will allow it.”
Initiating a Difficult Conversation Ask. Is this is a good time to talk?
Be direct. Prepare a short statement in advance that gets to the point.
Be quiet and listen. Allow the physician to respond completely.
Sympathize. Try to understand the physician’s perspective and show it.
Empathize. Express you realize how hard this is; it’s hard for you too.
Assess. Is the physician is ready for you to expand on your statement?
A sincere question (i.e. “Tell me more.”)
Not an angry question (i.e. “How can you say that!?”)
“Dr., are you ready for me to expand on this”? No: wait. Yes: continue
Commence the conversation with detail Rationale reward and risk
Group Exercises
Using scenarios presented, come up with a best response.
Remember: Conversation Initiation
Respect the physician's time
Be Direct
Sympathize/Empathize
Remember: Defusing Verbal Attack
Listen Listen
Don’t need to be right
Have thick skin
Be Kind
Agree
Give away “control”
Divert Negativity
We will present suggestions and discuss the results for each.
1/15/2009
15
Group Exercise One
Turn to the person next to you Consider together the following:
! 5 minutes.
The Coder performs an Audit of E/M codes. This audit finds the
Physician consistently under documents the medical decision
making of his exam. After the audit the Coder would like to show
the Physician what he has done wrong and “set him straight”.
What approach may be most successful?
Conversation Initiation
Is this is a good time to talk?
I’ve found a problem that could result in a payer under-coding your claims
Session Discussion: Exercise One
under-coding your claims.
I know that documentation rules are time consuming, but I want you to be paid properly for your work.
Listen.
“Tell me why you feel this way. I’m interested in your thought process on this.”
Don’t need to be right.
“You are right. This is confusing and makes no clinical sense.”
Have thick skin.
“It is ridiculous but we need to make sure you are fully & correctly paid.”
Be Kind.
“I’m sorry this is confusing. I understand why you feel this way.”
Session Discussion: Exercise One
y g y y y
Agree.
“I agree with you. What do you suggest we do to keep you out of harm’s way? ”
Give away “control”.
“We could write a letter to the Plan’s medical director about this.”
Divert Negativity.
“The payer must not understand how hard you work!”
1/15/2009
16
Turn to your partner Consider together the following:
! 5 minutes.
The Coder is reviewing an operative report in a specialty she has
f S ff
Group Exercise Two
never coded before. She is having a difficult time understanding
the procedure. The Coder would like to ask the Physician to
explain the procedure, but she doesn’t want to look bad. This is
a busy surgeon’s office and the Physician is always in a hurry. He
seems to hate to slow down and answer questions.
What approach may be most successful?
Conversation Initiation
Is this is a good time to talk?
I have researched this but don’t fully understand what you did. I want you to be paid properly could you walk me through it so that I can code everything you did?
Session Discussion: Exercise Two
that I can code everything you did?
I know you are busy but explain this to me once I can make sure you get properly paid.
Listen.
“Tell me when a better time is for you?”
Don’t need to be right.
“I wish I knew this. I don’t want to guess with your $”
Have thick skin.
“Your payment is more important to be than my embarrassment over asking.”
Be Kind.
“I’m sorry that I am taking your time. I understand why you feel this way.”
Session Discussion: Exercise Two
y g y y y y
Agree.
“I agree with you. I need to know this. ”
Give away “control”.
“I could leave my code book with you to review and highlight.”
Divert Negativity.
“If coding school taught more surgical anatomy and med school taught more coding we would both be happier!”
1/15/2009
17
Turn to your partner Consider together the following:
! 5 minutes. The Coder is auditing records for an office to understand why
every E/M code with a -25 modifier is being denied. He finds that
the Physician documents “patient returns to the office today to
Group Exercise Three
the Physician documents patient returns to the office today to
receive injection.” Clearly each patient is coming in with the intent
of receiving the injection and it appears from the documentation
this Physician is abusively billing the insurance companies. He
has to tell the Physician that this is incorrect and she can no
longer bill this way. You confront the Physician about her use of
this modifier and she says “the last biller told me to do this at
every visit.” I’m just following the rules.
What approach may be most successful?
Session Discussion: Exercise Three
Conversation Initiation
Is this is a good time to talk?
You have been given bad advice. We’ll need to modify things a bit to keep you out of harm’s way.
It must be frustrating to hear different things from different people. It is hard to know what to trust.
Session Discussion: Exercise Three Listen.
“I’d like to hear more about what you were told.”
Don’t need to be right.
“You are right. All coders should say and do the same thing.”
Have thick skin.
“I’d yell too if I were you. I can show you the correct way to do this.”
Be Kind.
“I’m sorry that you have been misled.” y y
Agree.
“I agree with you. You should never have to waste your time or effort. ”
Give away “control”.
“Would you like to read the official rules? Perhaps you’ll see something we could use.”
Divert Negativity.
“I am sure the previous coder was just trying to get you paid. She must not have realized how dangerous it was for you.”
1/15/2009
18
Turn to your partner Consider together the following:
! 5 minutes.
While with the patient, the physician documents only brief
C
Group Exercise Four
statements. He uses a short hand that system the Coder has
never seen before. He usually goes back and documents the full
record at the end of the day but sometimes does not get back to
the record for several days or even a week. The compliance
department is concerned that the documentation is not timely
enough and has asked the coder to make sure services are
documented fully.
What approach may be most successful?
Session Discussion: Exercise Four
Conversation Initiation
Is this is a good time to talk?
The your method of documenting may cause us to under code your services.
I know you are very busy and this is not your highest priority. I don’t want to see you get unpaid.
Session Discussion: Exercise Four Listen.
“I’m interested in your short hand system. Will you tell me more about it?”
Don’t need to be right.
“You are right. Documentation is time consuming.”
Have thick skin.
“I understand you are frustrated. Let’s talk about documentation short-cuts that code well for busy physicians.
Be Kind.
“I’m sorry that you have so few free moments in your day.”
Agree.
“I agree with you. You should only have to concentrate on patient care. ”
Give away “control”.
“Will you recommend a solution that will work better.”
Divert Negativity.
“I wish our compliance department could fully appreciate how hard this is for you.”
1/15/2009
19
Turn to your partner Consider together the following:
! 5 minutes.
A new biller entered charges incorrectly, which resulted in many
C
Group Exercise Five
more denials than usual. The Coder usually enters charges and is
responsible. She also loads the system with the fee schedule and
contract rates. She needs to tell the physician why revenue is
down this month and tell him that new rates will cause him a 6%
cut this year.
What approach may be most successful?
Session Discussion: Exercise Five
Conversation Initiation
Is this is a good time to talk?
Payment is going to be delayed on $1500 this month and there are changes in the fee schedule that I need to warn you of.
You are working harder than ever and I know this is the last thing you want to hear.
Session Discussion: Exercise Five Listen.
“It helps me to hear your thoughts on this.”
Don’t need to be right.
“You are right. You are working harder for less money.”
Have thick skin.
“It is important that I prevent mistakes and help prepare for changes.”
Be Kind.
“I’m sorry that your patient care is not more properly rewarded ” I m sorry that your patient care is not more properly rewarded.
Agree.
“I agree with you. Billing mistakes are not allowable. ”
Give away “control”.
“Would you like to see a financial forecast?”
Divert Negativity.
“I can’t believe that they are cutting payment like this and expect good physicians to stay in practice.”