collusive behaviour in healthcare and impact on consumers
TRANSCRIPT

1
ww
w.c
uts
-cc
ier.
org
/CO
HE
D
Background
The right to health is recognised in a number ofinternational legal instruments and enshrinedthrough constitutional commitments in India(Article 21, Indian Constitution). According torecent government estimates, India�s overallperformance in terms of life expectancy, childsurvival and maternal mortality has improvedsteadily over the recent years.1 However, thereare wide divergences in achievements across thecountry vis-à-vis health indicators. If, as a country,India is to achieve improvements vis-à-vis universalhealth coverage2 and come close to achieving the2015 healthcare-related targets of the MillenniumDevelopment Goals (MDGs), there is an urgentneed to highlight policy areas that would requirerefinements and immediate (and effective)implementation.
Healthcare services in the country are characterisedby a profound contrast in performance between theprivate and the public sectors. While the upsurge inprivate participation in this sector would continueto meet the demand of the increasing populace, thegovernment needs to assess and adjust its role inthis emerging environment. Through the initiationof the National Rural Health Mission (NRHM)in 2005, a number of states have made progresswith provision of quality healthcare services to itscitizens.
However, a number of challenges remain in thesector, especially since a large number of Indiansstill remain outside the reach of healthcare services(WHO, 2008).3 Over the process of implementingits �Support for India�s Health Sector Programme�,the World Bank has observed, based on theNational Sample Survey (60th round) in 2004, that63 million individuals, or 12 million households,fell into poverty due to health expenditure. Themajority of these households (79 percent) becameimpoverished due to spending on outpatient care,including drugs, and the remainder (21 percent)fell into poverty due to hospital care.
The Annual Report to the People on Health,Ministry of Health and Family Welfare (MoHFWSeptember 2010) reveals that the health indicatorsof the country have lagged behind the impressiveeconomic progress over the past two decades. Itreiterates the need to adopt a national public healthpolicy urgently, for reconfiguring the health systemin the country � making it more efficient andequitable. One of the recommendations in thisreport is to raise public finance on healthcare tothree percent of the gross domestic product (GDP).
The other extremely important point touchesaccess to medicines. Private (out-of-pocket)expenditure in healthcare constitutes 80 percentof the total healthcare expenses in India. Expenses
Collusive Behaviour inHealthcare and Impact on Consumers
Evidence from Assam
COHED No. 1/2011
This FactSheet produced under the COHED project highlights findings of the research andinvestigation undertaken in three towns in the state of Assam (India), to gather evidence aboutcollusive behaviour among healthcare providers. It was revealed from the analysis that certain practicesexisted in both public and private healthcare that reduced the availability of medicine and healthcareservices for a large number of citizen consumers. Prevalence of such practices in public healthcarehas huge implications especially for the poor. This document urges the state government and otherrelevant authorities to investigate the origin of such practices and take immediate remedial actions.
2
ww
w.c
uts
-ccie
r.org
/CO
HE
D
made for buying medicines comprise 72 percentof the total out-of-pocket expenses on healthcarein India.4
The MoHFW issued an order nearly a year ago(Order SS-11025/45/10-MH-1, May 26, 2010)that government hospitals should prescribe onlygood quality generic medicines to the patients.However, it is evident that such practices havenot been picked up by most state governments,yet.
Despite policy recommendations for greatercoordination between the Department ofPharmaceuticals (Ministry of Chemical andFertilisers) and the MoHFW, there seems to be alack of coherence in the process of policyformulation and adoption � which ultimatelyaffects the efficacy of healthcare services. Lack ofappropriate regulatory oversight of the healthcaresector remains a huge challenge, especially giventhe role that private providers play in the healthcaredelivery in the country. Whether the concern isover cost, quality and availability of healthcareinfrastructure/facilities/services or the nexusbetween various players in the healthcare valuechain, consumers continue to remain at the mercyof providers and have little say or choice whileseeking healthcare services in the country.
CUTS Project (COHED)
Various imperfections in the market for healthcareservices remain due to the combination of anumber of factors, including huge informationasymmetry between consumers and providers,lack of coherence in policy formulation andimplementation between the Centre and State,absence of proper regulatory oversight, etc. Theseimperfections have led to proliferation of marketmalpractices, which give huge commercial benefitsto providers, to the detriment of the consumers.
It is, therefore, logical to assume that curbing suchmarket malpractices would be beneficial forconsumers, not only in terms of monetary benefits(reduced costs of healthcare services) but also inenabling greater access to quality healthcareservices.
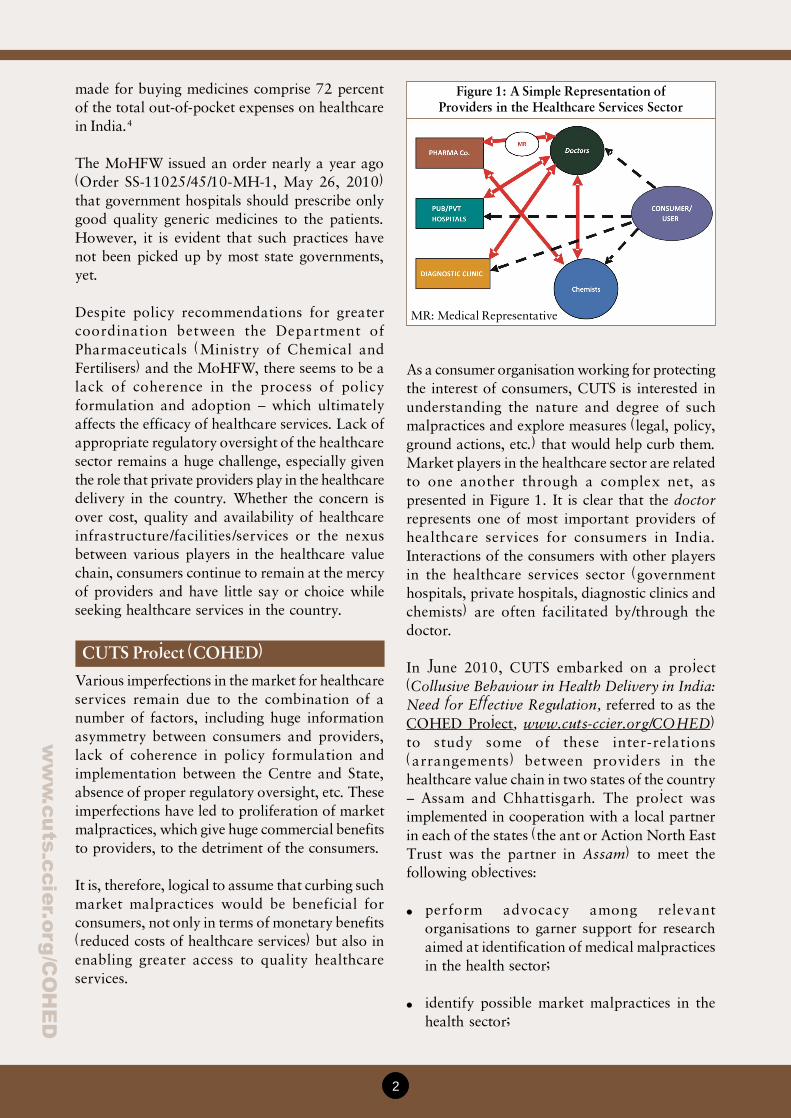
As a consumer organisation working for protectingthe interest of consumers, CUTS is interested inunderstanding the nature and degree of suchmalpractices and explore measures (legal, policy,ground actions, etc.) that would help curb them.Market players in the healthcare sector are relatedto one another through a complex net, aspresented in Figure 1. It is clear that the doctorrepresents one of most important providers ofhealthcare services for consumers in India.Interactions of the consumers with other playersin the healthcare services sector (governmenthospitals, private hospitals, diagnostic clinics andchemists) are often facilitated by/through thedoctor.
In June 2010, CUTS embarked on a project(Collusive Behaviour in Health Delivery in India:Need for Effective Regulation, referred to as theCOHED Project, www.cuts-ccier.org/COHED)to study some of these inter-relations(arrangements) between providers in thehealthcare value chain in two states of the country� Assam and Chhattisgarh. The project wasimplemented in cooperation with a local partnerin each of the states (the ant or Action North EastTrust was the partner in Assam) to meet thefollowing objectives:
� perform advocacy among relevantorganisations to garner support for researchaimed at identification of medical malpracticesin the health sector;
� identify possible market malpractices in thehealth sector;
Figure 1: A Simple Representation ofProviders in the Healthcare Services Sector
MR: Medical Representative
3
ww
w.c
uts
-cc
ier.
org
/CO
HE
D
The Indian Constitution has madehealthcare services largely a responsibility ofstate governments and, thus, it primarilybecomes the responsibility of the state toprovide healthcare to all people in equalmeasure. Since health is influenced by anumber of factors, such as adequate food,housing, basic sanitation, healthy lifestyles,protection against environmental hazards andcommunicable diseases, the term�healthcare� embraces a multitude of servicesprovided to individuals or communities byagents of the health services or profession forthe purpose of promoting, maintaining,monitoring or restoring health.
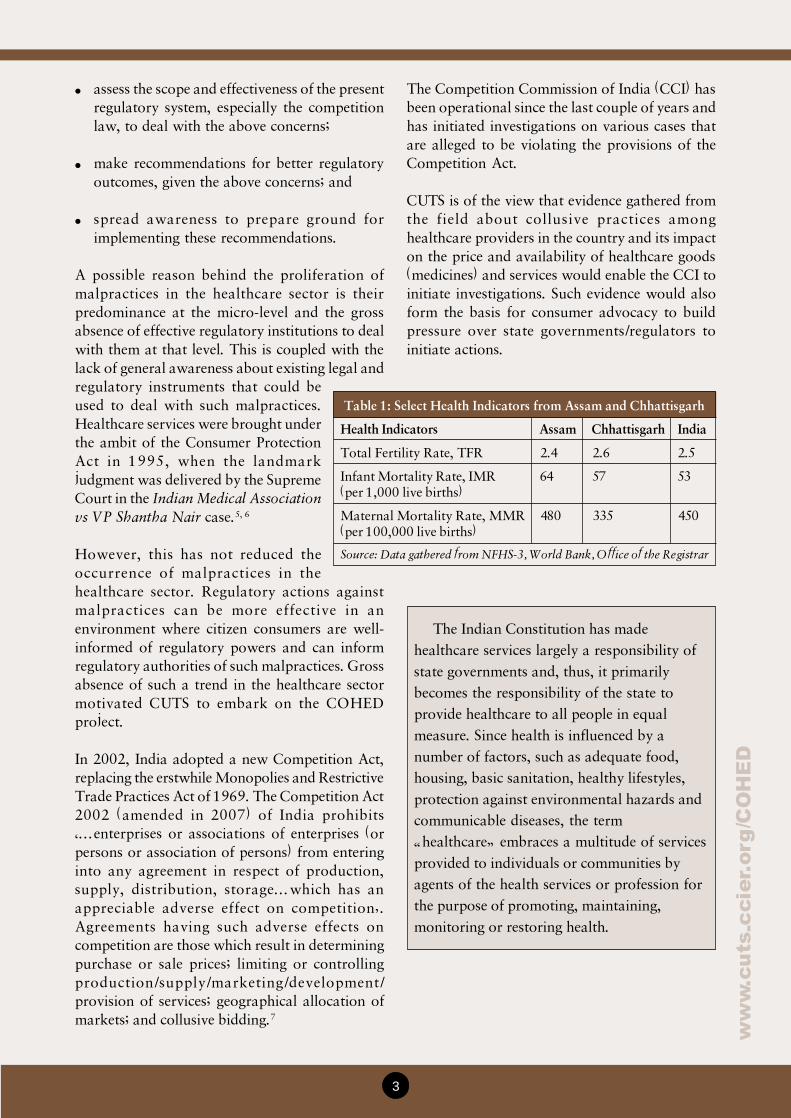
Table 1: Select Health Indicators from Assam and Chhattisgarh
Health Indicators Assam Chhattisgarh India
Total Fertility Rate, TFR 2.4 2.6 2.5
Infant Mortality Rate, IMR 64 57 53(per 1,000 live births)
Maternal Mortality Rate, MMR 480 335 450(per 100,000 live births)
Source: Data gathered from NFHS-3, World Bank, Office of the Registrar
� assess the scope and effectiveness of the presentregulatory system, especially the competitionlaw, to deal with the above concerns;
� make recommendations for better regulatoryoutcomes, given the above concerns; and
� spread awareness to prepare ground forimplementing these recommendations.
A possible reason behind the proliferation ofmalpractices in the healthcare sector is theirpredominance at the micro-level and the grossabsence of effective regulatory institutions to dealwith them at that level. This is coupled with thelack of general awareness about existing legal andregulatory instruments that could beused to deal with such malpractices.Healthcare services were brought underthe ambit of the Consumer ProtectionAct in 1995, when the landmarkjudgment was delivered by the SupremeCourt in the Indian Medical Associationvs VP Shantha Nair case.5, 6
However, this has not reduced theoccurrence of malpractices in thehealthcare sector. Regulatory actions againstmalpractices can be more effective in anenvironment where citizen consumers are well-informed of regulatory powers and can informregulatory authorities of such malpractices. Grossabsence of such a trend in the healthcare sectormotivated CUTS to embark on the COHEDproject.
In 2002, India adopted a new Competition Act,replacing the erstwhile Monopolies and RestrictiveTrade Practices Act of 1969. The Competition Act2002 (amended in 2007) of India prohibits��enterprises or associations of enterprises (orpersons or association of persons) from enteringinto any agreement in respect of production,supply, distribution, storage�which has anappreciable adverse effect on competition�.Agreements having such adverse effects oncompetition are those which result in determiningpurchase or sale prices; limiting or controllingproduction/supply/marketing/development/provision of services; geographical allocation ofmarkets; and collusive bidding.7
The Competition Commission of India (CCI) hasbeen operational since the last couple of years andhas initiated investigations on various cases thatare alleged to be violating the provisions of theCompetition Act.
CUTS is of the view that evidence gathered fromthe field about collusive practices amonghealthcare providers in the country and its impacton the price and availability of healthcare goods(medicines) and services would enable the CCI toinitiate investigations. Such evidence would alsoform the basis for consumer advocacy to buildpressure over state governments/regulators toinitiate actions.

4
ww
w.c
uts
-ccie
r.org
/CO
HE
D
Table 3: Financial Burden of Healthcare forDifferent Consumer Classes (Assam)
Income Average Percentage of TotalClasses Monthly Health Monthly Income
Expense (M) (in percent)
Low 902 2.56
Middle 1687 8.95
High 2055 4.43
Table 2: Healthcare Institutions in Assam
Health Institutions Number
Medical Colleges 4
State-level Hospitals 1
District Hospitals 21
Sub-divisional Hospitals 13
Community Health Centres 108
Public Health Centres 844
Sub-centres 4592
B.Sc. Nursing Colleges 1
GNM Training Centres 15
ANM Training Centres 18
Source: National Rural Health Mission, Department ofHealth and Family Welfare, Government of Assam, atwww.nrhmassam.in
Figure 2: Choice of Providers (Assam)
� Choice of Provider: 44 percent of therespondents visited public hospitals fortreatment, while 37 percent of them preferredprivate healthcare. Nearly a fifth (19 percent)of the surveyed population preferred visiting
Health Sector in Assam
Poor literacy rate, low per capita income which ismainly due to the high density of population, wideurban-rural disparity, improper water and sanitationfacilities, etc., are seen to have contributed towardsthe under developed health sector in the state.8 Inorder to address challenges facing the state vis-à-vishealthcare issues, certain reform measures have beenadopted by the state as enumerated below:
� Assam Public Health Act 2010: Assam is apioneer state in the country to enact AssamPublic Health Act 2010, which seeks toguarantee people�s right to appropriate andefficacious healthcare � especially towardseffective measures for prevention, treatmentand control of epidemic and endemic diseases.
� Drug Procurement Policy: Assam has draftedProcurement Guideline, in line with WorldBank guideline, for procurement and logisticmanagement of drugs and equipments. Underthe guidelines, drugs are procured by theirgeneric name.
� Essential Drug List: In 2007, the government(under the aegis of the NRHM) developed theState List of Essential Medicines andformulary based on common aliments.
The current status of the healthcare infrastructurein the state is summarised in Table 2:9
Results and Discussion
A multiple-stage survey and analysis methodologywas developed by CUTS, along with its partner(the ant), and the same was employed for arrivingat the following results.
I. Survey of Consumers (visiting Public healthcareInstitutions)In the first stage survey, the information wasgathered from consumers on the basis of aquestionnaire from three towns in each of the twostates. In Assam, the information was gatheredfrom 301 consumers from Guwahati, Bongaigaonand Nagaon. The results are enumerated below.
� Financial Burden of Healthcare: It was clearthat households belonging to the low-incomeclass in the sample spent a much larger share(20.56 percent) of their monthly income onhealthcare, as compared to people from theother economic classes. In monetary terms, itwas M902 for the respondents.
5
ww
w.c
uts
-cc
ier.
org
/CO
HE
D
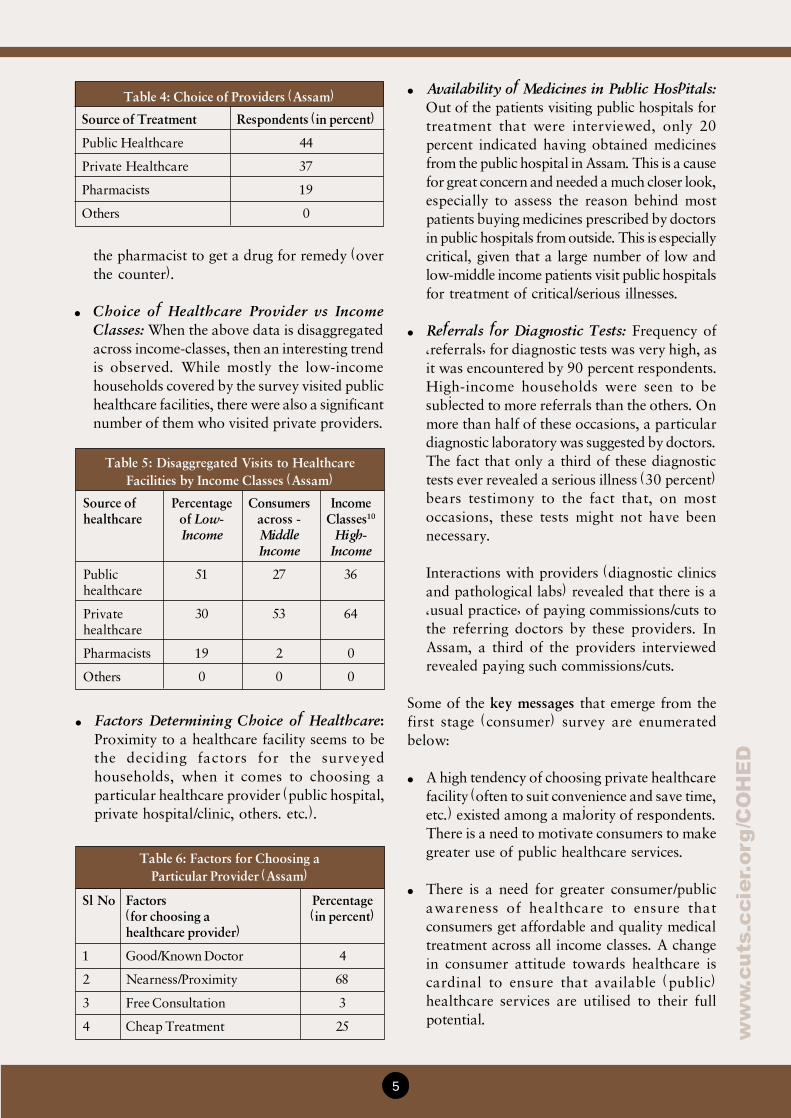
� Availability of Medicines in Public Hospitals:Out of the patients visiting public hospitals fortreatment that were interviewed, only 20percent indicated having obtained medicinesfrom the public hospital in Assam. This is a causefor great concern and needed a much closer look,especially to assess the reason behind mostpatients buying medicines prescribed by doctorsin public hospitals from outside. This is especiallycritical, given that a large number of low andlow-middle income patients visit public hospitalsfor treatment of critical/serious illnesses.
� Referrals for Diagnostic Tests: Frequency of�referrals� for diagnostic tests was very high, asit was encountered by 90 percent respondents.High-income households were seen to besubjected to more referrals than the others. Onmore than half of these occasions, a particulardiagnostic laboratory was suggested by doctors.The fact that only a third of these diagnostictests ever revealed a serious illness (30 percent)bears testimony to the fact that, on mostoccasions, these tests might not have beennecessary.
Interactions with providers (diagnostic clinicsand pathological labs) revealed that there is a�usual practice� of paying commissions/cuts tothe referring doctors by these providers. InAssam, a third of the providers interviewedrevealed paying such commissions/cuts.
Some of the key messages that emerge from thefirst stage (consumer) survey are enumeratedbelow:
� A high tendency of choosing private healthcarefacility (often to suit convenience and save time,etc.) existed among a majority of respondents.There is a need to motivate consumers to makegreater use of public healthcare services.
� There is a need for greater consumer/publicawareness of healthcare to ensure thatconsumers get affordable and quality medicaltreatment across all income classes. A changein consumer attitude towards healthcare iscardinal to ensure that available (public)healthcare services are utilised to their fullpotential.
Table 6: Factors for Choosing aParticular Provider (Assam)
Sl No Factors Percentage(for choosing a (in percent)healthcare provider)
1 Good/Known Doctor 4
2 Nearness/Proximity 68
3 Free Consultation 3
4 Cheap Treatment 25
Table 5: Disaggregated Visits to HealthcareFacilities by Income Classes (Assam)
Source of Percentage Consumers Incomehealthcare of Low- across - Classes10
Income Middle High-Income Income
Public 51 27 36healthcare
Private 30 53 64healthcare
Pharmacists 19 2 0
Others 0 0 0
the pharmacist to get a drug for remedy (overthe counter).
� Choice of Healthcare Provider vs IncomeClasses: When the above data is disaggregatedacross income-classes, then an interesting trendis observed. While mostly the low-incomehouseholds covered by the survey visited publichealthcare facilities, there were also a significantnumber of them who visited private providers.
� Factors Determining Choice of Healthcare:Proximity to a healthcare facility seems to bethe deciding factors for the surveyedhouseholds, when it comes to choosing aparticular healthcare provider (public hospital,private hospital/clinic, others. etc.).
Table 4: Choice of Providers (Assam)
Source of Treatment Respondents (in percent)
Public Healthcare 44
Private Healthcare 37
Pharmacists 19
Others 0
6
ww
w.c
uts
-ccie
r.org
/CO
HE
D
� Private healthcare suffers from a high degreeof variation (from hi-tech hospitals to theprivate practitioner in the neighbourhood) inas far as quality is concerned and there is hardlyany regulation on maintaining a minimumstandard of treatment.
� An extremely high frequency of referral (todiagnostic clinics), combined with theprevalence of �cuts� for referring doctors, wasnoted. This is an extremely perniciousarrangement � and measures should be takenat the local/micro-levels to curb/eliminate sucharrangements.
� In spite of having received medical treatmentat a public hospital, consumers are buyingmedicines from private sources. This raises thecost of healthcare for consumers further.Whether this is due to sheer unavailability ofdrugs in the hospital (implies that publicprocurement of medicines is something that thestates should consider very seriously) or due tocollusive arrangements between providers inthe public healthcare system and the privatepharmacists (whose shops are mostly justoutside the public hospitals) was an issue thatrequired further investigation in the secondstage of the survey.
II. Prescribing Pattern and Analysis (in Publichealthcare institutions)
A. Respondent�s Feedback on Public HealthcareSystem
Information gathered from 210 respondentsvisiting public healthcare institutions in the secondstage (prescription analysis) revealed the findingsas mentioned in the following bullets. Thefollowing public healthcare institutions werecovered:
- Guwahati Medical College and Hospital- Civil Hospital, Nagaon- Urban Health Centre, Nagaon- Civil Hospital and Primary Health Centre,
Bongaigaon
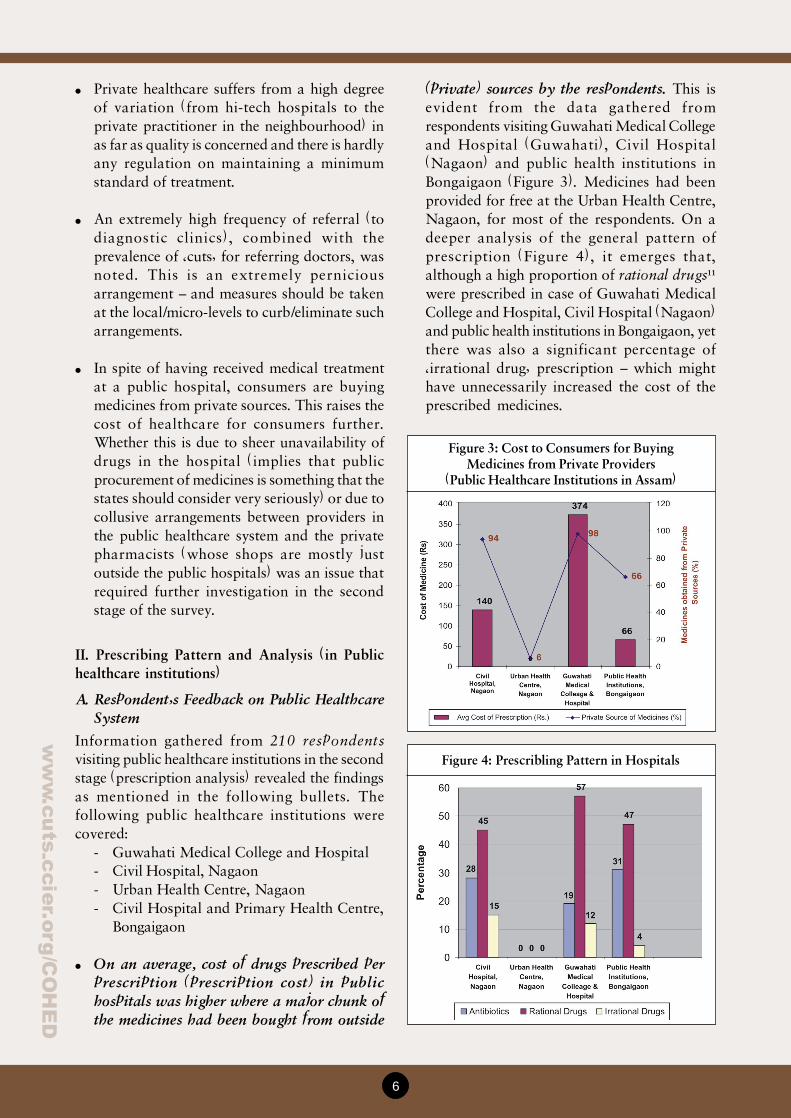
� On an average, cost of drugs prescribed perprescription (prescription cost) in publichospitals was higher where a major chunk ofthe medicines had been bought from outside
(private) sources by the respondents. This isevident from the data gathered fromrespondents visiting Guwahati Medical Collegeand Hospital (Guwahati), Civil Hospital(Nagaon) and public health institutions inBongaigaon (Figure 3). Medicines had beenprovided for free at the Urban Health Centre,Nagaon, for most of the respondents. On adeeper analysis of the general pattern ofprescription (Figure 4), it emerges that,although a high proportion of rational drugs11
were prescribed in case of Guwahati MedicalCollege and Hospital, Civil Hospital (Nagaon)and public health institutions in Bongaigaon, yetthere was also a significant percentage of�irrational drug� prescription � which mighthave unnecessarily increased the cost of theprescribed medicines.
Figure 3: Cost to Consumers for BuyingMedicines from Private Providers
(Public Healthcare Institutions in Assam)
Figure 4: Prescribling Pattern in Hospitals
7
ww
w.c
uts
-cc
ier.
org
/CO
HE
D
policies for medicines in the state. Only a smallfraction of respondents who have been visitingthe Urban Health Centre, Nagaon, indicatedthat they bought medicines from privatesources. If distribution of medicine in a publichealth institution has been so efficiently
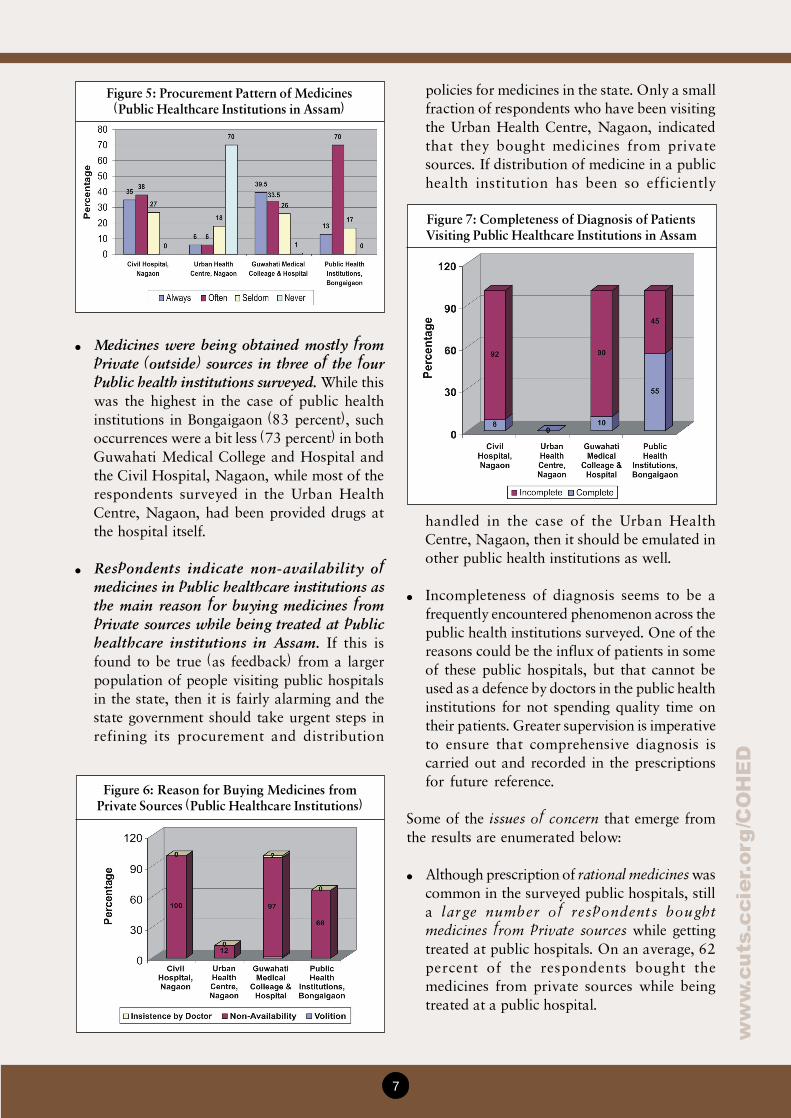
Figure 5: Procurement Pattern of Medicines(Public Healthcare Institutions in Assam)
� Medicines were being obtained mostly fromprivate (outside) sources in three of the fourpublic health institutions surveyed. While thiswas the highest in the case of public healthinstitutions in Bongaigaon (83 percent), suchoccurrences were a bit less (73 percent) in bothGuwahati Medical College and Hospital andthe Civil Hospital, Nagaon, while most of therespondents surveyed in the Urban HealthCentre, Nagaon, had been provided drugs atthe hospital itself.
� Respondents indicate non-availability ofmedicines in public healthcare institutions asthe main reason for buying medicines fromprivate sources while being treated at publichealthcare institutions in Assam. If this isfound to be true (as feedback) from a largerpopulation of people visiting public hospitalsin the state, then it is fairly alarming and thestate government should take urgent steps inrefining its procurement and distribution
Figure 6: Reason for Buying Medicines fromPrivate Sources (Public Healthcare Institutions)
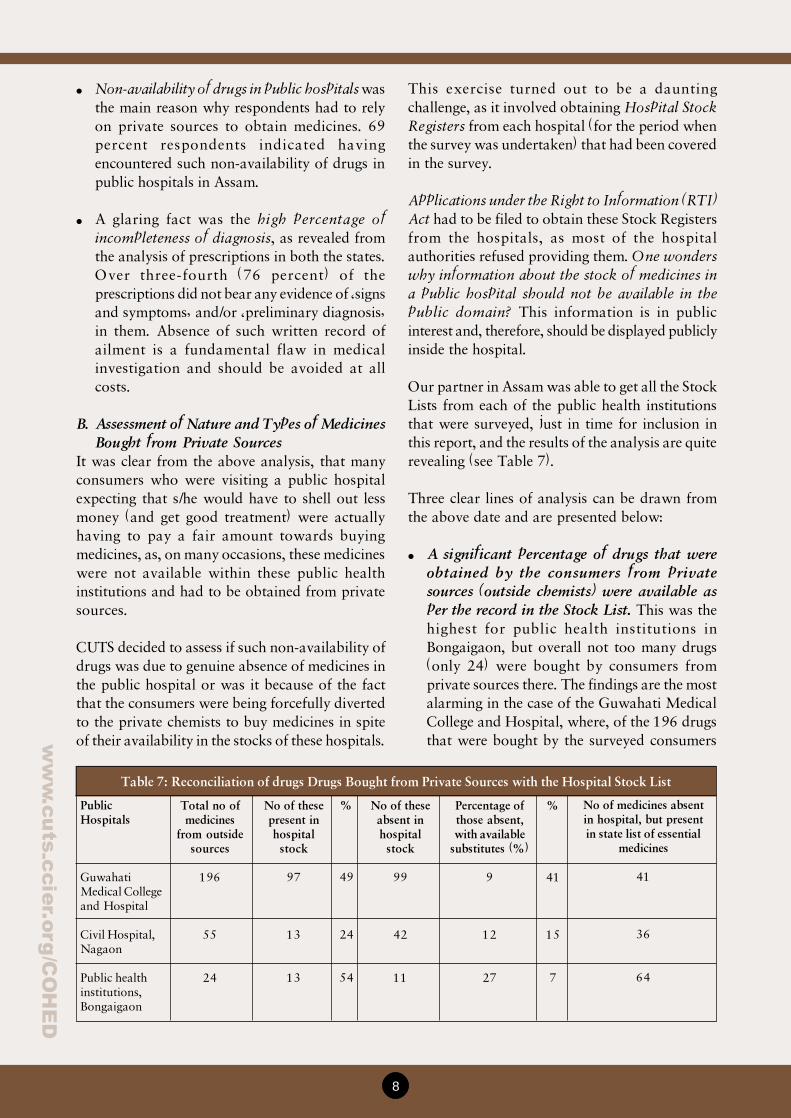
Figure 7: Completeness of Diagnosis of PatientsVisiting Public Healthcare Institutions in Assam
handled in the case of the Urban HealthCentre, Nagaon, then it should be emulated inother public health institutions as well.
� Incompleteness of diagnosis seems to be afrequently encountered phenomenon across thepublic health institutions surveyed. One of thereasons could be the influx of patients in someof these public hospitals, but that cannot beused as a defence by doctors in the public healthinstitutions for not spending quality time ontheir patients. Greater supervision is imperativeto ensure that comprehensive diagnosis iscarried out and recorded in the prescriptionsfor future reference.
Some of the issues of concern that emerge fromthe results are enumerated below:
� Although prescription of rational medicines wascommon in the surveyed public hospitals, stilla large number of respondents boughtmedicines from private sources while gettingtreated at public hospitals. On an average, 62percent of the respondents bought themedicines from private sources while beingtreated at a public hospital.
8
ww
w.c
uts
-ccie
r.org
/CO
HE
D
� Non-availability of drugs in public hospitals wasthe main reason why respondents had to relyon private sources to obtain medicines. 69percent respondents indicated havingencountered such non-availability of drugs inpublic hospitals in Assam.
� A glaring fact was the high percentage ofincompleteness of diagnosis, as revealed fromthe analysis of prescriptions in both the states.Over three-fourth (76 percent) of theprescriptions did not bear any evidence of �signsand symptoms� and/or �preliminary diagnosis�in them. Absence of such written record ofailment is a fundamental flaw in medicalinvestigation and should be avoided at allcosts.
B. Assessment of Nature and Types of MedicinesBought from Private Sources
It was clear from the above analysis, that manyconsumers who were visiting a public hospitalexpecting that s/he would have to shell out lessmoney (and get good treatment) were actuallyhaving to pay a fair amount towards buyingmedicines, as, on many occasions, these medicineswere not available within these public healthinstitutions and had to be obtained from privatesources.
CUTS decided to assess if such non-availability ofdrugs was due to genuine absence of medicines inthe public hospital or was it because of the factthat the consumers were being forcefully divertedto the private chemists to buy medicines in spiteof their availability in the stocks of these hospitals.
This exercise turned out to be a dauntingchallenge, as it involved obtaining Hospital StockRegisters from each hospital (for the period whenthe survey was undertaken) that had been coveredin the survey.
Applications under the Right to Information (RTI)Act had to be filed to obtain these Stock Registersfrom the hospitals, as most of the hospitalauthorities refused providing them. One wonderswhy information about the stock of medicines ina public hospital should not be available in thepublic domain? This information is in publicinterest and, therefore, should be displayed publiclyinside the hospital.
Our partner in Assam was able to get all the StockLists from each of the public health institutionsthat were surveyed, just in time for inclusion inthis report, and the results of the analysis are quiterevealing (see Table 7).
Three clear lines of analysis can be drawn fromthe above date and are presented below:
� A significant percentage of drugs that wereobtained by the consumers from privatesources (outside chemists) were available asper the record in the Stock List. This was thehighest for public health institutions inBongaigaon, but overall not too many drugs(only 24) were bought by consumers fromprivate sources there. The findings are the mostalarming in the case of the Guwahati MedicalCollege and Hospital, where, of the 196 drugsthat were bought by the surveyed consumers
Table 7: Reconciliation of drugs Drugs Bought from Private Sources with the Hospital Stock List
PublicHospitals
GuwahatiMedical Collegeand Hospital
Civil Hospital,Nagaon
Public healthinstitutions,Bongaigaon
Total no ofmedicines
from outsidesources
196
55
24
No of thesepresent inhospital
stock
97
13
13
%
49
24
54
No of theseabsent inhospital
stock
99
42
11
Percentage ofthose absent,with available
substitutes (%)
9
12
27
%
41
15
7
No of medicines absentin hospital, but presentin state list of essential
medicines
41
36
64

9
ww
w.c
uts
-cc
ier.
org
/CO
HE
D
from private sources, 49 percent were availablein the hospital stock register.
� Of the medicines that were absent in thehospital stock list, some had substitutes thatwere available in the hospital stock but werenot prescribed. These were nine percent and12 percent, respectively, in Guwahati MedicalCollege and Hospital and Civil Hospital,Nagaon. In public healthcare institutions inBongaigaon this was 27 percent.
� A consistently high percentage of medicinesfrom the State List of Essential Medicines wasabsent in the hospitals. This was highest in caseof the Bongaigaon (64 percent), but alsoconsiderably high in Guwahati (41 percent) andCivil Hospital, Nagaon (36 percent).
CUTS urges the state government to initiateinvestigations in these healthcare institutions toclearly find out the reason why medicines thatwere present in the hospital stock list were notbeing offered to a large number of consumers?
As noted earlier, the Competition Act 2002 ofIndia prohibits ��enterprises or associations ofenterprises (or persons or association of persons)from entering into any agreement in respect ofproduction, supply, distribution, storage...whichhas an appreciable adverse effect on competition�.
Agreements having such adverse effects oncompetition are those which result in determiningpurchase or sale prices; limiting or controllingproduction/supply/marketing/development/provision of services; geographical allocation ofmarkets; and collusive bidding.
Given that the Competition Commission of Indiais sufficiently empowered, as above, it shouldinvestigate if supply and distribution of medicinesin these public hospitals have been restricted dueto agreements between the various playersinvolved and necessary corrective measures shouldbe taken.
III. Prescribing Pattern and Analysis (in PrivateHealthcare)
A random sample of private prescriptions wasgathered from Bongaigaon (Assam) during the
survey in order to get a snapshot of the visibletrends in private healthcare. From the analysis, thefollowing results emerged:
� The average amount paid for medicines by thepeople covered under the survey each time theyvisited a private healthcare institution wasM336.
� Incompleteness of diagnosis was rampantamong the private practitioners (67 percent) inthe prescriptions of private healthcareproviders. This was also quite high (45 percent)in public healthcare institution covered inBongaigaon.
� Polypharmacy (prescription of four or moredrugs) was encountered in only half (52percent) of the prescriptions collected fromprivate providers. It was even higher among thepublic healthcare providers surveyed inBongaigaon (63 percent).
� Irrational drug prescription was observed in 18percent of the prescriptions gathered from theprivate providers, which was almost identicalto its occurrence (17.5 percent) among thepublic healthcare institutions in Bongaigaon.
IV. Discussions with Medical Representatives
It proved quite a challenging task to gatherinformation about the nature and extent of theallegiance between doctors and pharmaceuticalcompanies in the two states. Only one suchmeeting/interview has been possible and a briefaccount of the same is presented here. The nameof the town/state from where this evidence wasgathered has not been mentioned intentionally.
While categorically denouncing such malpractices(allegiances between doctors and pharmaceuticalcompanies) and asking for help in forcing thegovernment to clean up the system, the medicalrepresentatives themselves flayed the unethicalpractices of doctors and listed out various systemsin practices. These depended on various factors,including the pharmaceutical company, the product,bargaining capacity of the doctors, etc. Thesepractices can broadly be classified under threeheads: (i) reminders, (ii) inducements, and (iii) cashpayments or bribes, as is elucidated below:
10
ww
w.c
uts
-ccie
r.org
/CO
HE
D
i. Reminders
� Small gifts like pens, paper pads, calendars� Medicine samples
ii. Inducements
� Gifts in the form of medical equipment likestethoscope, torches, scopes, BP instrument,etc.
� Vacations for doctor and his family� Paper reading at seminars in foreign
countries for doctors identified as KeyOpinion Leaders
� Sponsorship of Seminars and ContinuingMedical Education Programmes for doctors
iii. Cash Payments and Bribes
� Gifts like cars, ACs, etc.� Equated Monthly Instalments (EMI) for
home appliances, cars, etc.� Life insurance premiums� School fees for their children� Cash payments � doctors call companies and
their managers promise X amount of theirproduct sales and ask for commissionsbetween 10 to 25 percent
There were also a number of ways in which thepharmaceutical companies kept track of thevolume of products being sold through a particulardoctor. Some of the popular tracking techniquesto determine the amount payable to these doctorsas cash for sales are presented below:
� Sales of products supplied by stockist topharmacies where a doctor sits is attributed tothe doctor; and
� Vials of costly injectables, etc., are manuallyverified on a day-to-day basis to ascertain the
amount that is payable and cash payments aremade on a daily basis.
� Some pharmaceutical companies providespecial prescription pads to the doctors, whichhave carbonless self-copying chemicals thatallow the doctor to maintain a copy of everyprescription with him. The doctor would thenproduce each of these prescription copies forcash payments at already negotiated rates.
Some of the other issues that were revealed fromthese discussions were that:
� These practices are considered as usual andpracticed by most of the doctors, barring a few.
� After the Medical Council of Indiaannouncement (2009) barring doctors fromaccepting gifts, etc., there was a temporarystoppage, but things soon returned to normal(even got worse).
� The situation in the hinterland is much worse,as compared to cities and towns.
� �Free samples� of medicines are also sold.
� Doctors in both public and private healthcareinstitutions indulge in these practices.
Conclusion and the Way Forward
On the basis of the review and the field workundertaken, certain conclusions have been derivedand recommendations made to ensure that a moreconsumer-friendly healthcare system is evolved.These are segregated into two specific categories:(i) issues for policy, and (ii) issues for consumerawareness and action.
Issues for policy that emerge from this study havebeen expanded in this section into the followingsub-areas:
� Procurement and distribution of drugs � Thestate government should urgently ensure thatmedicines are available in public hospitals. Forthis, state level policies and �action programmes�should be developed and implemented urgently.
Illustration: Injection Ceftriaxone thatmay be sold as low as for M50 per vial isalso available at M200. The doctor wouldtypically offer to sell this more expensivebrand only on a daily cash basis, so thatthe medical representative would have tocome every evening to make cash pay-ments.

11
ww
w.c
uts
-cc
ier.
org
/CO
HE
D
� Public display of hospital stock of medicines� A small step that can make a huge impact isthat the state government should make itmandatory for public hospitals to publiclydisplay their stock of medicines and the figures(of current stock) should be updated on a day-to-day basis and displayed in a prominentlocation in the hospital.
� Periodic scrutiny of prescription patterns �A periodic exercise should be initiated by thestate government and implemented incooperation with local civil societyorganisations to scrutinise prescriptionpatterns, especially in public hospitals.
� Monitoring of chemist/pharmacist shops inclose proximity of public hospitals � The stategovernment authorities should undertakeperiodic (and �unannounced�) visits to privatechemists and pharmacist shops outside publichospitals and also get feedback from consumersvisiting them.
� Greater attention towards patients � Doctorsneed to spend more time on the consumer whois seeking healthcare service and document (inthe prescription) �signs/symptoms� and a�preliminary diagnosis�, or face action.
� Identify �good practices� within the state andreplicate them � The study reveals that thereare �good practice� hospitals that are existentin each of the two states. It is necessary todevelop a system of �performance evaluation�of public healthcare institutions and recognisethose which have been doing their job well.Efforts should also be made to explore thepossibility of emulating such �good practicecases� in the other public healthcare institutions.
� Adoption of the Clinical Establishment Act2010 � This Act should be adopted at theearliest and effectively implemented to ensurea minimum standard of healthcare forconsumers.
Issues for consumer awareness and action arepresented below:
� Need to be more cautious in choosinghealthcare providers � Consumers seem to bevery casual in choosing healthcare providers andoften visit those providers who are locatednearby. It is important that they chooseproviders who have an established goodperformance.
� Approach Consumer Forum for redressal �Consumers are unaware that they can complainagainst unfair and deceptive practices of doctorsto the State Consumer Forum and get redressal.
� Raise demand for generic drugs � It ismandatory for doctors in public hospitals (runby the Central Government) to prescribe onlygeneric drugs and the consumer should demandthese from them. When they visit pharmacistswith prescriptions with generic drugs writtenon them, they should ask the pharmacists toprovide them 3-4 brands for each of thesegenerics and then make a choice based onseveral criteria (company, price, advice ofpharmacists, etc.).
� Demand discounts from pharmacists � Likeany other consumer good/services, consumersshould ask for discount on the price ofmedicines (MRP) from the pharmacists. It is apractice to sell medicines at MRP only.
CUTS encourages civil society organisations acrossthe state of Assam also to take up these issueswith the state government to ensure that healthcareservices for consumers become cheaper and thatthey are not fleeced by commercially motivatedproviders in the healthcare value chain.
12
ww
w.c
uts
-ccie
r.org
/CO
HE
D
Endnotes
1 Annual Report to the People on Health, Ministry of Health and Family Welfare, Government of India, 2010,New Delhi.
2 Universal Coverage - Member States of the World Health Organisation (WHO) committed in 2005 to developtheir health financing systems so that �all people have access to services and do not suffer financial hardshippaying for them�. This goal was defined as universal coverage, sometimes called universal health coverage(World Health Report 2010, WHO).
3 According to a 2008 WHO estimate, 65 percent Indians do not have access to modern healthcare.
4 Shiva Kumar, A. K. et al., �India: Towards Universal Health Coverage�, LANCET Journal, January 2011(www.thelancet.com).
5 Nihajwan, S. B., National Commission and Supreme Court on Consumer Cases 1986-96, Part II, InternationalLaw Book Company, 1996, New Delhi.
6 ��Services rendered to a patient by a medical practitioner would fall within the ambit of �services� as definedunder the Section 2(1)(o) of the Consumer Protection Act, 1986�.
7 Section 3 of The India Competition Act 2002 (amended in 2007).
8 Dutta, Indrani & Bawari, S. �Health and healthcare in Assam � A Status Report�, CEHAT, 2007, Mumbai.
9 http://www.nrhmassam.in/health_facilities.php
10 For the purpose of this study, a classification of the respondents into income classes was done on the basis of thefollowing measurements: (a) Lowincome households were those with a total monthly household income of lessthan M10,000; (b) Middle-income households were those with a total monthly household income of betweenM10,000 to 40,000; and (c) Highincome households were those with an average monthly household income ofabove M40,000. The average household size was considered to be five individuals for this study.
11 Analysis of the rational use of drugs for this study was undertaken in line with its definition provided by theWHO, i.e., �Rational use of drugs requires that patients receive medications appropriate to their clinicalneeds, in doses that meet their own individual requirements for an adequate period of time, and the lowestcost to them and their community.� (Report of the Conference of Experts on Rational Use of Drugs, WHO,Nairobi, 1985)
This Factsheet has been prepared by CUTS Centre for Competition, Investment & Economic Regulation (CUTS CCIER) as part of theproject entitled, �Collusive Behaviour in Health Delivery in India: Need for Effective Regulation� (COHED) with support from Oxfam,India.
CUTS CCIER Factsheets are to inform, educate and provoke debate on specific issues. Readers are encouraged to quote orreproduce material from this paper for their own use, but CUTS International requests due acknowledgement and a copy of thepublication.
© CUTS International 2011. CUTS International, D-217, Bhaskar Marg, Bani Park, Jaipur 302016, India. Ph: +91.141.2282821,Fx: +91.141.2282485, E-mail: [email protected], Website: www.cuts-international.org