chemical eye trauma, by dr. safaa refaat
TRANSCRIPT

Chemical Eye Injury
ByDr. Safaa Refaat
FRCSG Ophth, MSc , MBBS.

ن� حم� الر� الله� ب�سم�
يم� ح� الر� “ العالمين” رب� لله� الحمد� وقيل�

In Chemical Eye InjuryWASH
Is Every Thing!
Chemical Eye InjuryChemical injuries are among the most destructive of all traumatic insults suffered by the eye .
They may occur in domestic, industrial, and military settings.
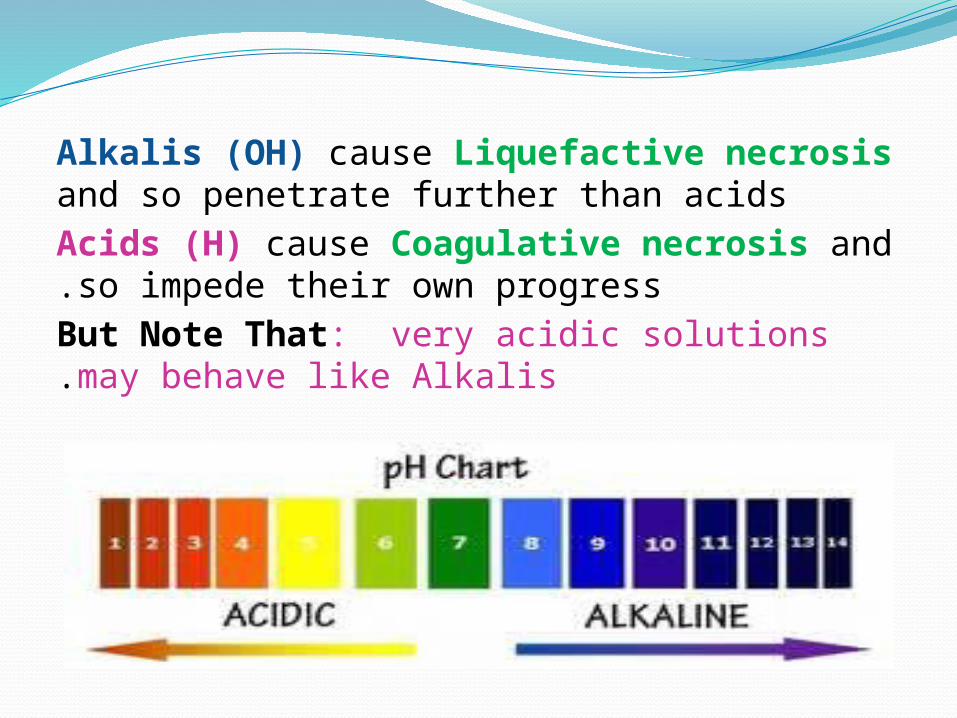
Alkalis (OH) cause Liquefactive necrosis and so penetrate further than acidsAcids (H) cause Coagulative necrosis and so impede their own progress.But Note That: very acidic solutions may behave like Alkalis.

PH 7.4
CornealInvolveme
nt
Durationof Contact
Prognostic factors

*PH *Duration of Contact
*Extent of Corneal Involvement*Limbal Involvement: Re-
epithelialization relies on migration of the limbal stem cells.
*Associated nonchemical injury: blunt trauma, thermal injury.
Prognostic factors

Clinical features -Conjunctival injection or
blanching, chemosis, hemorrhage, epithelial defects
-Corneal epitheliopathy, punctate to complete loss, corneal edema; perilimbal ischemia, anterior chamber reaction
-Intra Ocular Pressure raise -Necrotic Retinopathy.
-Eye Lids Burn and associated Facial Burn.

Alkali Burn
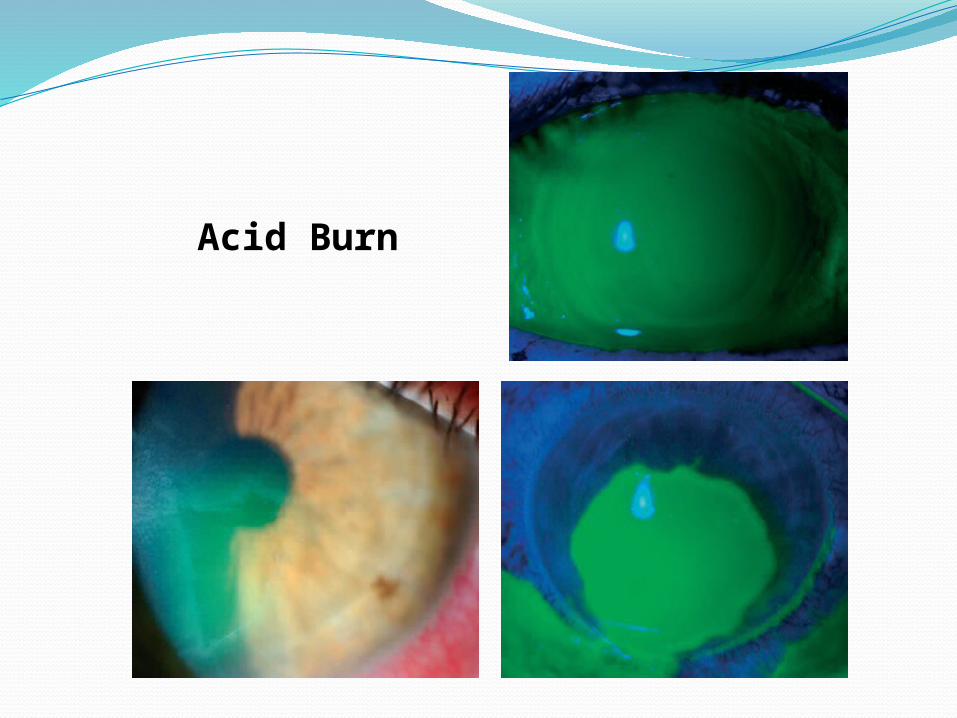
Acid Burn

Complications• Conjunctival
scarring, symblepharon, & keratoconjunctivitis sicca (Dry Eye)
•Significant limbal ischemia: conjunctivalization, vascularization, Corneal opacification
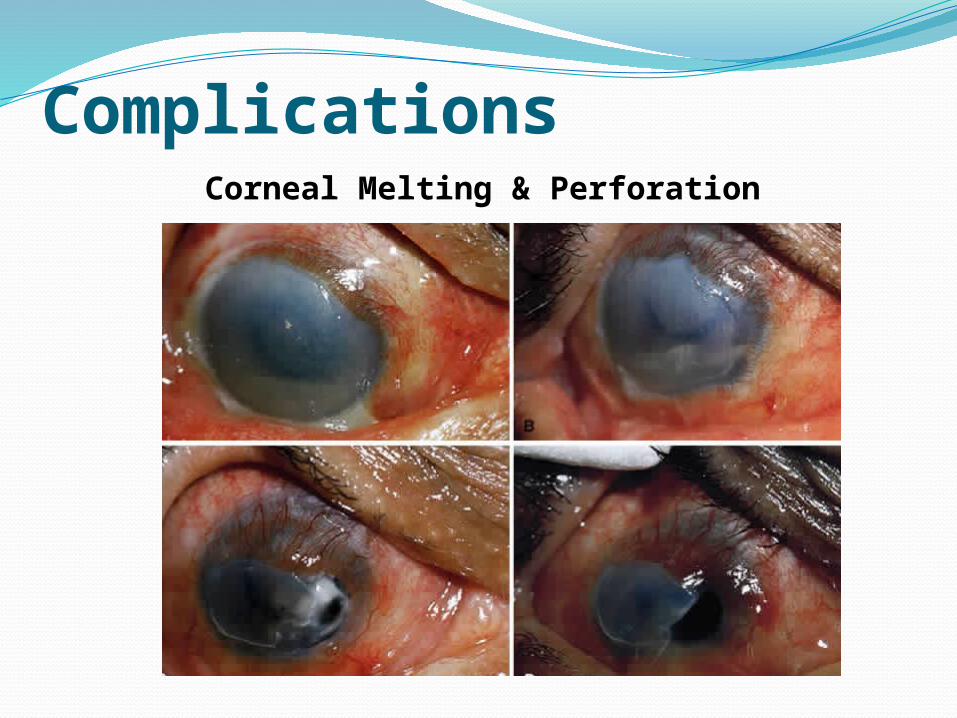
ComplicationsCorneal Melting & Perforation

•Full-thickness burns: hypotony, iris, ciliary, and lenticular damage; may progress to phthisis bulbi; very poor prognosi
•Periorbital burns :first-, second-, or third-degree chemical burns of periorbital tissues
Complications

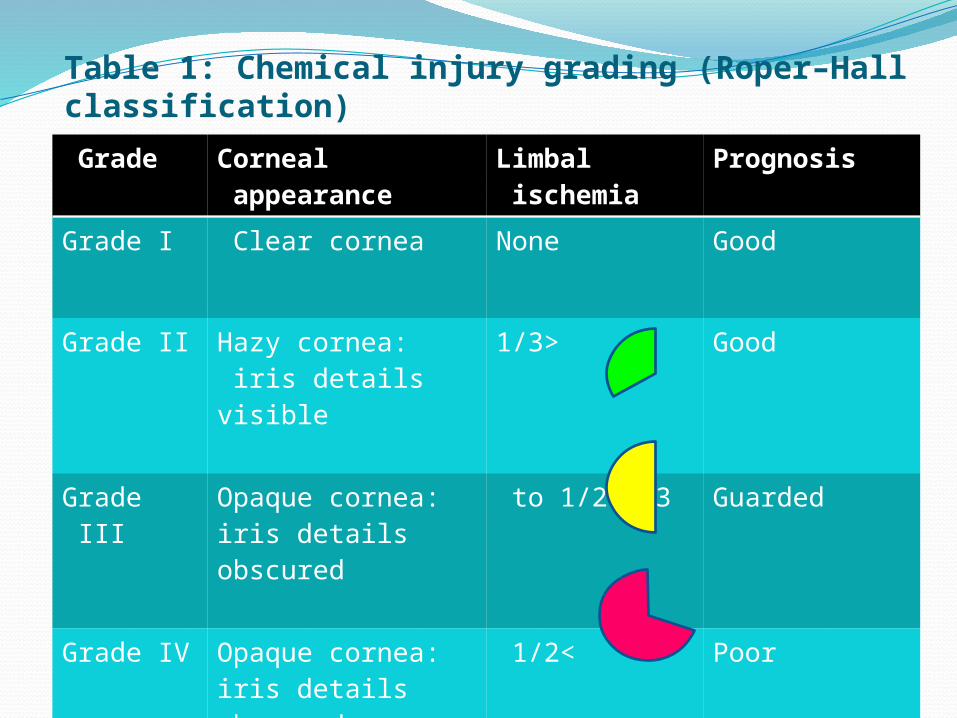
Table 1: Chemical injury grading (Roper–Hall classification)Grade Corneal
appearance Limbal ischemia
Prognosis
Grade I Clear cornea None Good
Grade II Hazy cornea: iris details visible
<1/3 Good
Grade III Opaque cornea: iris details obscured
1/3 to 1/2 Guarded
Grade IV Opaque cornea: iris details obscured
>1/2 Poor

Table 2: Strong Alkalis in common use
Common alkalisSubstance
Chemical PH
Oven cleaning fluid
Sodium hydroxide
14
Drain cleaning fluid
Sodium (or potassium) hydroxide
14
Plaster Calcium hydroxide
14
Fertilizers (some)
Ammonium hydroxide
13

Common acidsSubstance
Chemical PH
Battery fl uid
Sulfuric acid 1
Lavatory cleaning fluid
Sulfuric acid 1
Bleach Sodium hypochlorite
1
Pool cleaning fluid
Sodium (or calcium) hypochlorite
1
Table 2: Strong Acids in common use
Chemical Eye Burn: Managment
Early•Minutes counts against your patient!
Don’t wait for the Ophthalmologist to Reach
Effective•To achieve Neutral pH,
Avarage from 2 to 8 liter is needed
IrrigationEffectiveEarly
Chemical Eye Burn: First Aid At Home
Wash under running water for 20 to 45 minutes

Chemical Eye Burn: First Aid At work Bath Station at our
lab

Chemical Eye Burn: Immediate treatmentNeutralization of pH by irrigation
*Even before a full history or detailed examination is conducted
*Copious Irrigation in cycles of 2 litre then rest 10 min. check pH & Repeat until neutral or near-neutral pH is confirmed by
pH/ litmus paper.*Evert the lids to remove retained
particulate matter in fornices (e.g., lime, cement).

IrrigationEffectiveEarly

IrrigationEffectiveEarly

1
9876
5
3
4
2

Record & Document:
-Time started & Time Ended Irrigation -Amount & Type of fluid used
-pH records and times they measured- Visual Acuity- Date & Signature of care giver
-Send to ophthalmic Department !

Chemical Eye Burn -Further treatment:
•Topical antibiotics prophylaxis. •Topical cycloplegia for comfort/AC activity
•Topical lubricants per hour. •Oral analgesia.
Topical medication should be preservative-free when possible.
• Topical steroids• Topical & Oral ascorbic acid: essential for
collagen formation and is an effective scavenger of damaging free radicals. (Not in acid burn)
• Systemic Tetracycline: (proteinease inhibitor & anti-inflamatory properties)
. Antiglaucoma medications: if raised IOP:Give acetazolamide ± topical B-blocker
Chemical Eye Burn -Further treatment for severe injury:

Long-term—complicated casesPoor corneal healing:
-conjunctival graft,-limbal stem cell graft,-amniotic membrane graft .
Corneal opacifi cation:-Penetrating keratoplasty: wait 6 months, Rejection Risk.
Keratoprosthesis : for severely damaged eyes.

In Chemical Eye InjuryEarly & Effective
Irrigation Is Crucial In Saving Vision!

THANK YOU