casos clinico-radiológicos
TRANSCRIPT

JAVIER E. PACHECO PATERNINA
RADIOLOGIA E IMÁGENES DIAGNOSTICASFACULTAD DE MEDICINA
UNIVERSIDAD DE CARTAGENAAÑO 2014
CASO CLÍNICO

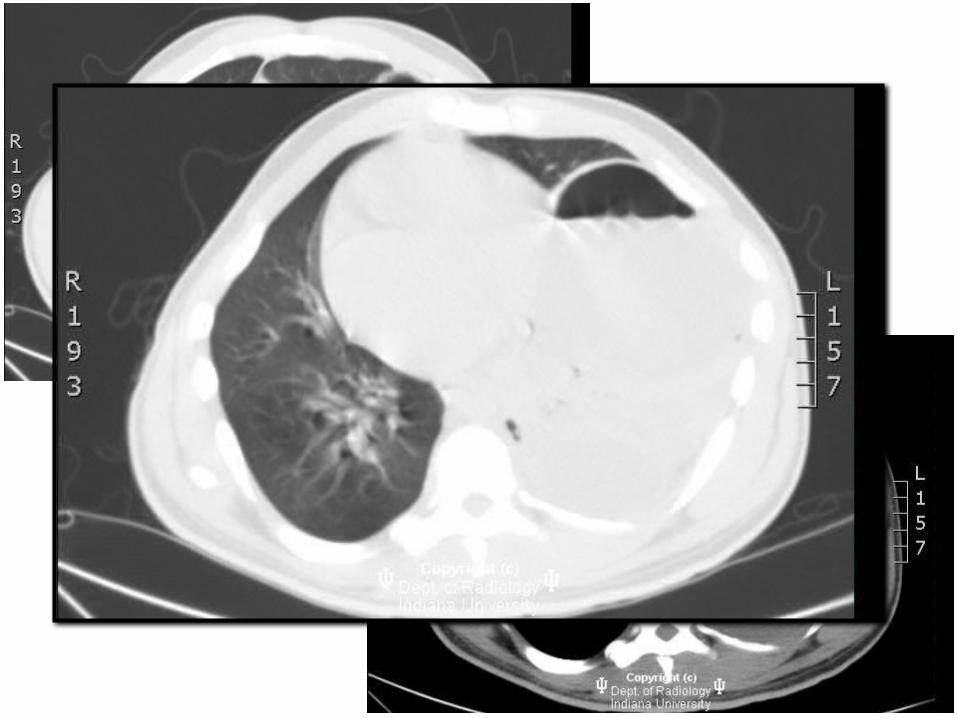
History: Cough. Otherwise asymptomatic.
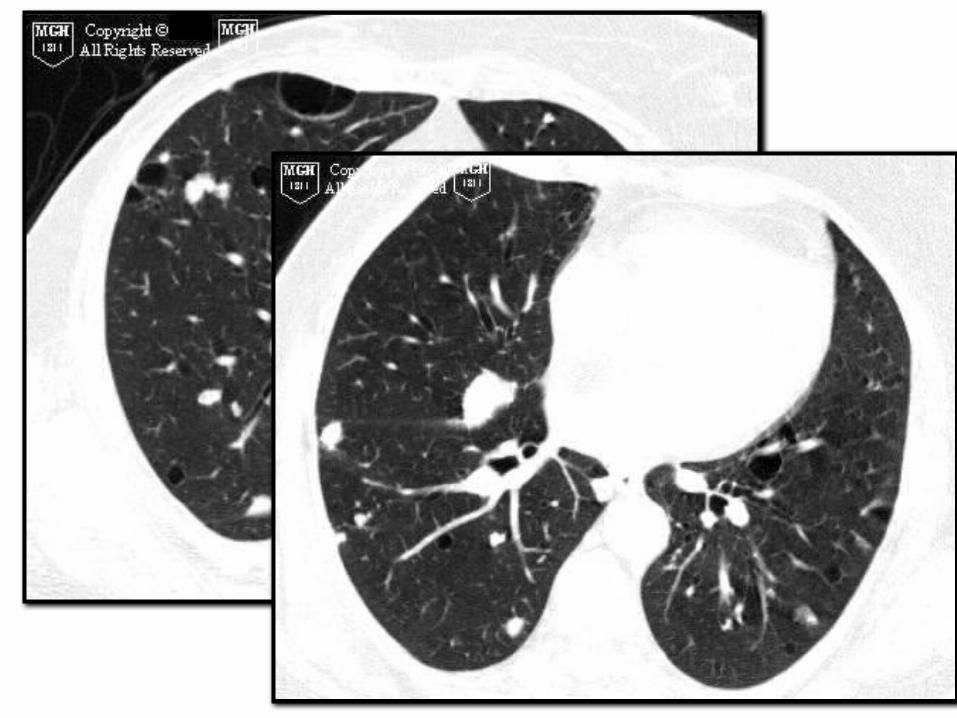

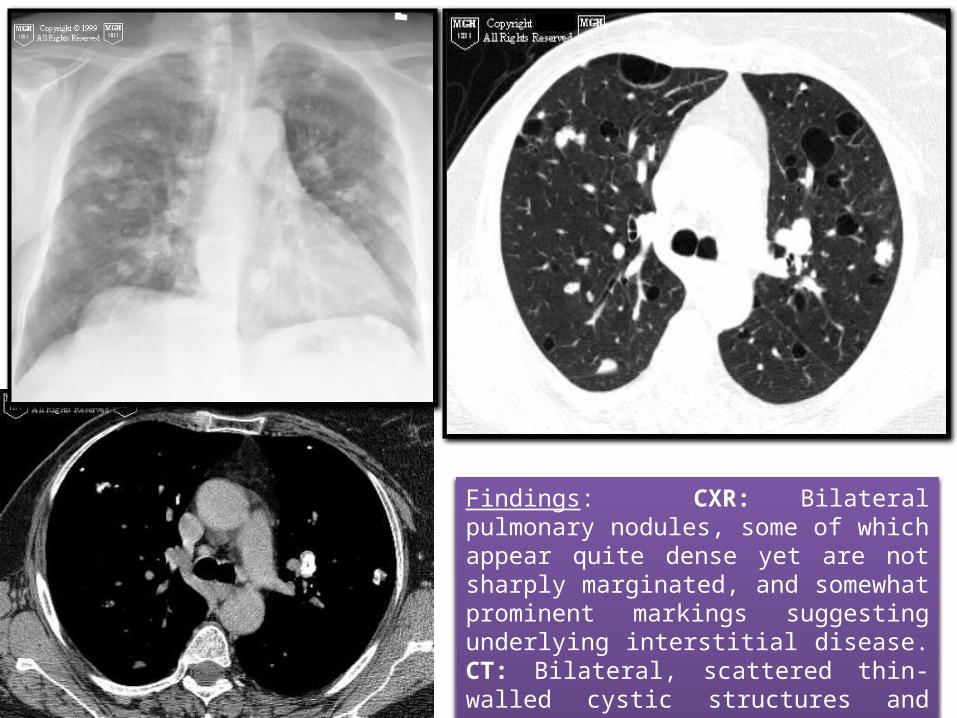
Findings: CXR: Bilateral pulmonary nodules, some of which appear quite dense yet are not sharply marginated, and somewhat prominent markings suggesting underlying interstitial disease. CT: Bilateral, scattered thin-walled cystic structures and numerous nodules, some of which contain abundant calcium.
DX: Pulmonary Manifestations of Amyloidosis
Amyloid is manifested by the extracellular deposition of an insoluble protein that characteristically stains with Congo red and produces a green birefringence when viewed under a polarizing microscope.
The disorder can be localized (10-20% of cases) in which there are focal discrete depositions of amyloid, or systemic (80-90% of cases).
In systemic disease the respiratory system is involved in 50% of cases and involvement is usually characterized by a diffuse interstitial pattern.
Various forms of pulmonary disease can be seen, including: diffuse parenchymal disease, nodular parenchymal disease, or tracheobronchial involvement. Isolated mediastinal nodal involvement/mediastinal amyloid masses are rare in the absence of pulmonary involvement, but have been reported. Calcification can be seen in up to 50% of such cases.
Patients with systemic amyloid and pulmonary involvement frequently experience dyspnea and have a poor long term prognosis with a median survival of 16 months. [1,4] Despite their poor prognosis, the pulmonary is disease is responsible for the patients death in only about 10% of cases

GRACIAS
CASO CLÍNICO N 2

History: Man with difficulty breathing.


Findings: The heart and mediastinum are displaced to the right due to a large mass or masses in the left lung. There is a large air-fluid level in the superior aspect of the mass. The mass appears to make acute angles with the pleural surface.
Differential diagnosis:Lung abscessPleural empyemaPneumatocelesInfected bullae
Diagnosis: Large lung abscessCT: fluidos de aire indican comunicación bronquial. La pared de la cavidad es variable de 4-15mm favoreciendo el extremo más grueso del espectro. No puede haber patron de vidrio deslustrado. A menudo hay adenopatía mediastínica e hiliar.Abscesos pulmonares son complicaciones de las infecciones microbianas no tratadas. Se encuentran en los mismos lugares que la infección subyacente.
Absceso periféricos puede ser difícil de diferenciar de empiemas pleurales base. Los abscesos suelen ser tan alto como ellos son anchas y forman ángulos agudos con la pleura.
Los abscesos se tratan con antibióticos y siguieron con RX de tórax de la resolución. Curan con bronquiectasias, cambio quística, y la cicatrización.Abscesos no reciben tratamiento tienen una mortalidad del 30%.