cardiovascular system disorders 2€™s pathophysiology: concepts of altered health states from...
TRANSCRIPT

Cardiovascular System Disorders 2
Lecture 20
Pathology and Clinical
Science 1 (BIOC211)
Department of BioscienceText Reference:
Porth’s Pathophysiology: Concepts of Altered Health States
Sheila C. Grossman & Carol Mattson Porth.
Ninth Edition.
Copyright © 2014 Lippincott, Williams & Wilkins Publishers, Inc.
© endeavour.edu.au

© Endeavour College of Natural Health endeavour.edu.au 2
Session Learning Outcomes
The aim of this session is to :
o Comprehend the pathophysiology of atherosclerosis
o Identify the risk factors and understand how to prevent
the atherosclerosis and Coronary Heart Disease (CHD)
o Describe the clinical features, investigations and
management of CHDs.

© Endeavour College of Natural Health endeavour.edu.au 3
ATHEROSCLEROSIS
Introduction
oMay manifest as CAD (angina, MI,
sudden death), cerebrovascular
disease (stroke and TIA) or peripheral
vascular disease (claudication and
limb ischemia)

© Endeavour College of Natural Health endeavour.edu.au 4
ATHEROSCLEROSIS
o Complex inflammatory process.
o Vascular endothelium is critical for maintaining
vascular integrity & homeostasis
o Atherogenesis thought to be triggered by initial
endothelial injury or dysfunction:
• Mechanical shear stresses
• Biochemical abnormalities
• Immunological factors
• Inflammation
• Genetic alteration

© Endeavour College of Natural Health endeavour.edu.au 5
RISK FACTORSTraditional Risk Factors
• Age
– Increases with age
• Gender
– M > F (premenopausal)
– M = F (postmenopausal)
• Family History
– Other risk factors can be familial
– ? independent
• Smoking
– Proportional to quantity
– Decrease in risk (almost to normal) after 10yrs abstinence

© Endeavour College of Natural Health endeavour.edu.au 6
RISK FACTORSo Diet and Obesity
• High fat, low antioxidants
o Hypertension
• Systolic & diastolic
o Hyperlipidaemia
– High LDL
– Low HDL
– Decreased cholesterol = reduced progression +
regression of coronary artery disease (CAD)
– Lipid lowering Rx = decreased mortality
o Diabetes mellitus
• Also magnifies the effect of other risk factors

© Endeavour College of Natural Health endeavour.edu.au 7
LIPID TRANSPORT Schematic
representation
of the
exogenous and
endogenous
pathways for
triglyceride and
cholesterol
transport.
From Porth’s Pathophysiology: Concepts of Altered Health States. (9th ed., p. 744), by
Sheila C. Grossman & Carol Mattson Porth.
Philadelphia, U.S.A. Walters Kluwer Health - Lippincott, Williams & Wilkins

© Endeavour College of Natural Health endeavour.edu.au 8
RISK FACTORSNewer risk factors
o Sedentary life style
• Lack of exercise
o Psychological well-being
• Work stress, lack of social support, depression & personality
o Alcohol
o Genetic factors
o Lipoprotein (a)
o Coagulation factors
• Serum fibrinogen, homocysteine
o C-reactive protein (CRP)
© Endeavour College of Natural Health endeavour.edu.au 9
RISK FACTOR MANAGEMENT
o Primary prevention
• modification of risk factors that reduce the development of coronary atheroma
o Secondary prevention
• modification of risk factors that slow the progression of established disease
o Smoking
• ↓ amount
• complete cessation
o Hypertension
• Control HT

© Endeavour College of Natural Health endeavour.edu.au 10
RISK FACTOR MANAGEMENT
oLipids
• any decrease is beneficial
• Lipid lowering agents (statins)
oExercise

© Endeavour College of Natural Health endeavour.edu.au 11
RISK FACTOR MANAGEMENT
o Weight
• Maintain ideal body weight
o Diabetes Mellitus (DM)
• Optimise BGL
o Diet
• Reduce saturated fat
• Increase vegetables + grains
• Fish, lean meat
• Limit take-away, snack food, cakes etc
• Avoid high cholesterol foods + offal

© Endeavour College of Natural Health endeavour.edu.au 12
DEVELOPMENT OF
ATHEROSCLEROSIS
o Follows endothelial dysfunction
o Accumulation of oxidized lipoproteins
o Lipoproteins are taken up by macrophages
o Macrophages become lipid-laden foam cells
o Fatty streaks appear & progress
o Plaque formation
o Cytokine release further damages endothelium

© Endeavour College of Natural Health endeavour.edu.au 13
DEVELOPMENT OF ATHEROSCLEROSIS
From Porth’s Pathophysiology: Concepts of Altered Health States. (9th ed., p. 750),
by Sheila C. Grossman & Carol Mattson Porth.
Philadelphia, U.S.A. Walters Kluwer Health - Lippincott, Williams & Wilkins
Endothelial Cell Injury Migration of Inflammatory
Cells
© Endeavour College of Natural Health endeavour.edu.au 14
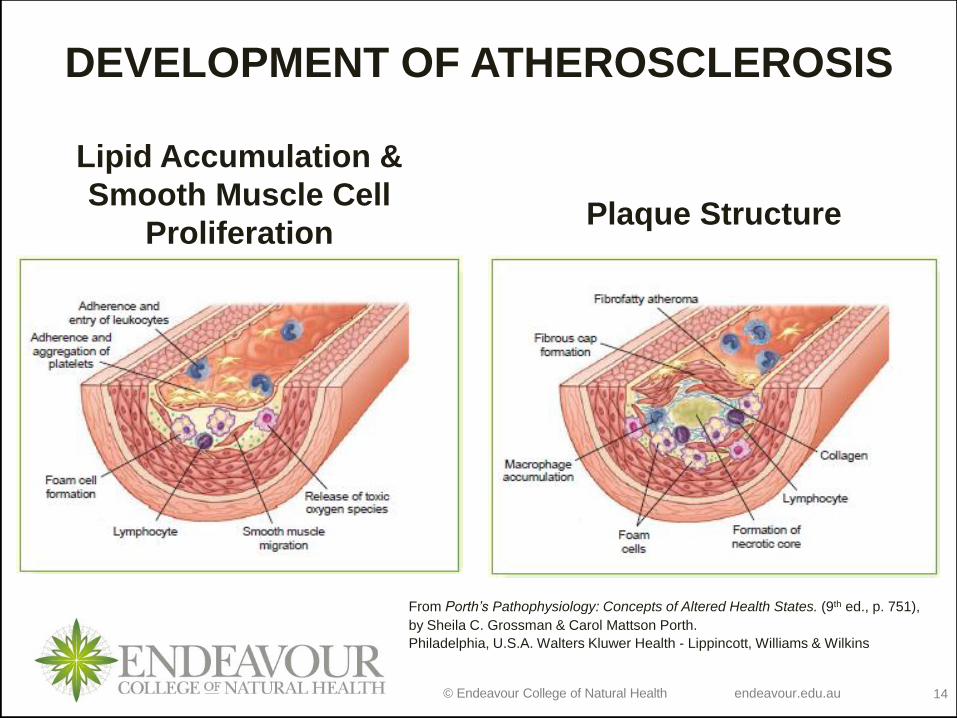
DEVELOPMENT OF ATHEROSCLEROSIS
Lipid Accumulation &
Smooth Muscle Cell
ProliferationPlaque Structure
From Porth’s Pathophysiology: Concepts of Altered Health States. (9th ed., p. 751),
by Sheila C. Grossman & Carol Mattson Porth.
Philadelphia, U.S.A. Walters Kluwer Health - Lippincott, Williams & Wilkins

© Endeavour College of Natural Health endeavour.edu.au 15
DEVELOPMENT OF ATHEROSCLEROSIS
Porth’s Pathophysiology: Concepts of Altered Health States
From Porth’s Pathophysiology: Concepts of Altered Health States. (9th ed., p. 749), by
Sheila C. Grossman & Carol Mattson Porth.
Philadelphia, U.S.A. Walters Kluwer Health - Lippincott, Williams & Wilkins

© Endeavour College of Natural Health endeavour.edu.au
DEVELOPMENT OF ATHEROSCLEROSIS
From Pathology. (2nd ed., p. 161), by A. Stevens & J. Lowe. 2000, London. Mosby,
Harcourt Publishers Ltd.

© Endeavour College of Natural Health endeavour.edu.au
ATHEROSCLEROSIS
http://www.portalesmedicos.com/imagenes/publicaciones_10/1009_modelo_animal_arterio
sclerosis/arteria_coronaria_aterosclerosis.jpg

© Endeavour College of Natural Health endeavour.edu.au 18
DEVELOPMENT OF
ATHEROSCLEROSIS
oCollagen produced by smooth muscle cells = advanced/raised fibrolipidplaque
oAdvanced plaque can grow slowly (encroaching on lumen) or become unstable (thrombosis with obstruction = complicated plaque)

© Endeavour College of Natural Health endeavour.edu.au 19
DEVELOPMENT OF
ATHEROSCLEROSIS
o Plaque thrombosis caused by:
• Superficial endothelial injury exposing connective tissue
with platelet adhesion = superficial thrombus
• Deep endothelial fissuring of advanced plaque allowing
blood to enter inside the plaque (highly thrombogenic
environment) = thrombus within plaque
o 50% reduction in luminal diameter results in
haemodynamically significant stenosis
• Smaller distal arteries/arterioles become maximally
dilated
• Any increase in myocardial demand = ischaemia

© Endeavour College of Natural Health endeavour.edu.au 20
COMPLICATIONS
From Pathophysiology for the Health Professions (2nd ed., p. 274), by B Gould, 2002. Philadelphia. W B Saunders Company.

© Endeavour College of Natural Health endeavour.edu.au 21
ATHEROSCLEROSIS
From Porth’s Pathophysiology: Concepts of Altered Health States.
(9th ed., p. 747), by Sheila C. Grossman & Carol Mattson Porth.
Philadelphia, U.S.A. Walters Kluwer Health - Lippincott, Williams &
Wilkins

© Endeavour College of Natural Health endeavour.edu.au 22
CORONARY HEART DISEASE
CHD is the most common form of heart disease
o Epidemiology
• Single most important cause of
premature death in Europe, South
America, Australia and New Zealand
• In UK 1 in 3 men and 1 in 4 women die
from CHD

© Endeavour College of Natural Health endeavour.edu.au 23
CORONARY HEART DISEASE
CAD results in variety of clinical situations
• Stable angina pectoris (AP)
• Unstable AP (UAP)
• Myocardial Infarction (MI) = advanced plaque with total occlusive thrombus
• Heart failure
• Arrhythmia
• Sudden death

© Endeavour College of Natural Health endeavour.edu.au 24
STABLE ANGINA
Angina Pectoris
Symptom complex of chest pain, discomfort due to transient myocardial ischaemia
o Causes
• Coronary atheroma is the most common cause
• Aortic valve disease
• Hypertrophic cardiomyopathy
© Endeavour College of Natural Health endeavour.edu.au 25
STABLE ANGINA
Clinical features
• Central chest pain, discomfort or
breathlessness precipitated by exertion
or stress
• Promptly relieved by rest
Investigation
• Resting ECG, exercise ECG
• Coronary arteriography

© Endeavour College of Natural Health endeavour.edu.au 26
STABLE ANGINA
Management
• Careful assessment
• Risk factors management
• Control symptoms
– Antiplatelet therapy - Low dose aspirin
– Antianginal drugs – nitrates, beta-blockers
– Percutaneous coronary interventions (PCI) - Stents
– Percutaneous trans-coronary arteriogram (PTCA)
– Coronary artery bypass graph (CABG)
Prognosis
• Depends on number of diseased vessels, degree of left ventricular dysfunction
• Single vessel and good LV function ( 5 yr survival > 90%)
© Endeavour College of Natural Health endeavour.edu.au 27
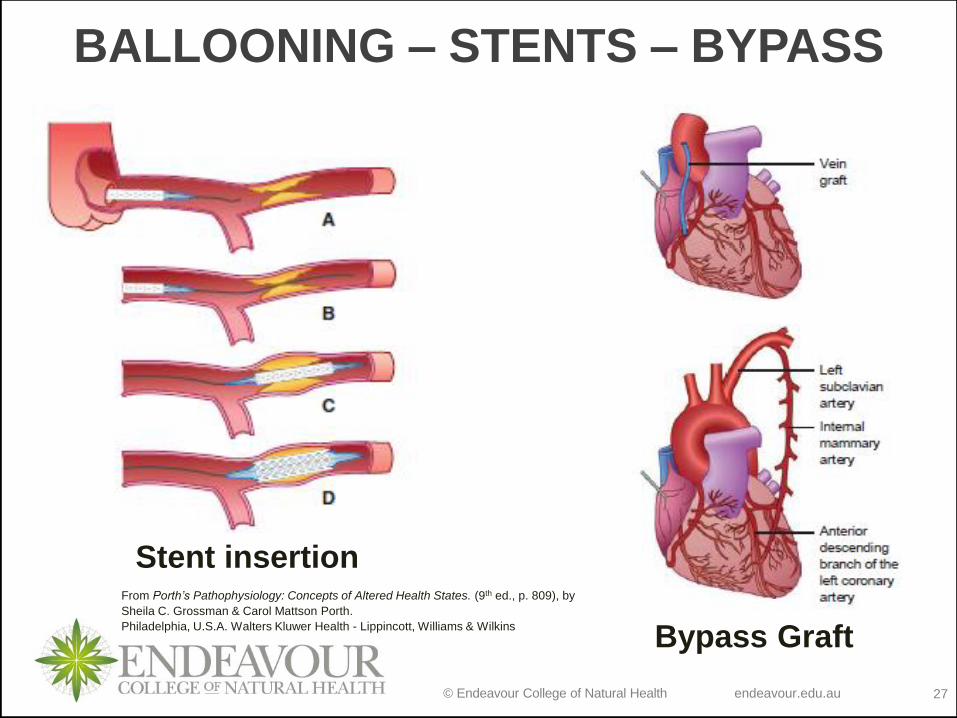
BALLOONING – STENTS – BYPASS
Stent insertion
Bypass Graft
From Porth’s Pathophysiology: Concepts of Altered Health States. (9th ed., p. 809), by
Sheila C. Grossman & Carol Mattson Porth.
Philadelphia, U.S.A. Walters Kluwer Health - Lippincott, Williams & Wilkins

© Endeavour College of Natural Health endeavour.edu.au 28
ANGIOPLASTY
http://www.vascular.co.nz/angioplastyrev%20copy.jpg

© Endeavour College of Natural Health endeavour.edu.au 29
UNSTABLE ANGINA
Characterised by new onset or rapidly worsening angina, angina on minimal exertion or angina at
rest
Diagnosis
• Evaluation of ECG
• Biochemical markers for cardiac damage
Management
• Admission to hospital due to risk of myocardial infarction (MI)
• Bed rest, antiplatelet therapy
• Same as for stable angina

© Endeavour College of Natural Health endeavour.edu.au 30
ANGINA
PAIN
From Porth’s Pathophysiology: Concepts of Altered Health States. (9th ed., p. 812), by
Sheila C. Grossman & Carol Mattson Porth.
Philadelphia, U.S.A. Walters Kluwer Health - Lippincott, Williams & Wilkins

© Endeavour College of Natural Health endeavour.edu.au 31
MYOCARDIAL INFARCTION
Definition
o Result of sudden decrease or interruption to arterial blood flow to the myocardium
Pathophysiology
o Coronary atheroma with plaque rupture + superimposed thrombus
o Myocardial necrosis = permanent myocardial damage
Causes
o Atheroma (predominantly) as above

© Endeavour College of Natural Health endeavour.edu.au 32
MYOCARDIAL INFARCTION
Clinical Features
o Key CF= chest pain
• severe, constant pain, unrelieved with
rest/nitrates
o Nausea/vomiting/sweating/breathlessness
o Anxiety and fear of impending death
o Collapse and syncope
o Sudden death

© Endeavour College of Natural Health endeavour.edu.au 33
MYOCARDIAL INFARCTION
Investigations
o ECG
o Biochemical markers – Creatine Kinase (CK); Troponin
o Chest X ray
o Echocardiography
Treatment
o Immediate access to medical care and defibrillation facility
o Emergency Rx (aspirin, thrombolysis, pain relief (morphine)
o CCU, bed rest
o Identify & Correct Risk Factors
o Subsequent Medical Rx – aspirin, B-blockers, ACEI, statins)
o Ongoing assessment

© Endeavour College of Natural Health endeavour.edu.au 34
MYOCARDIAL INFARCTIONComplications
• Arrhythmias
• Post infarct ischaemia
• Acute circulatory failure
• Mechanical complications
–Papillary muscle damage – valve lesions
–Rupture of interventricular septum – VSD
–Rupture of ventricle
• Embolism
• Heart failure
• Ventricular aneurysm

© Endeavour College of Natural Health endeavour.edu.au 35
MYOCARDIAL INFARCTION
Prognosis
o Mortality 25% without medical care
o 50% of death from MI occur within 24 hrs
o 40% die within 1 month
o Those survive an acute attack – 5 yr survival 75%
Differential Diagnosis
o As by main symptoms
o Cardio/pulmonary (CP) (CVS vs. other)
o MI vs. Upper abdominal pathologies

© Endeavour College of Natural Health endeavour.edu.au 36
Readings and ResourcesResources:
o Set Textbooks:
Colledge, N.R., Walker, B.R. & Ralston S.H. (2014). Davidson’s Principles and Practice of Medicine, (22nd ed.). Edinburgh.
Churchill Livingstone.
Grossman, S.C. & Porth, C.M. (2014). Porth’s Pathophysiology: concepts of altered health states, (9th ed.). Philadelphia,
U.S.A. Walters Kluwer Health - Lippincott, Williams & Wilkins.
o Additional textbooks:
Davies, A. & Moores, C. (2010). The respiratory system: basic science and clinical conditions, (2nd ed.). Edinburgh. Churchill,
Livingstone, Elsevier.
Field, M., Pollock, C., Harris, D. (2010). Systems of the Body: The Renal System; Basic Science and Clinical Conditions. (2nd
ed.). United Kingdom: Churchill Livingstone.
Jamison, J.R. (2006) Differential Diagnosis for Primary Care: a handbook for health care practitioners. (2nd ed.). Edinburgh.
Churchill Livingstone.
Lee, G. & Bishop, P. (2013). Microbiology and Infection Control for Health Professionals, (5th ed.). Frenchs Forest, NSW.
Pearson Education.
McCance, K.L. & Huether, S.E. (2014). Pathophysiology: the biological basis for disease in adults and children, (7th ed.). St.
Louis, MO. Elsevier.
Murphy, K. (2011). Janeway’s immunobiology, (8th ed.). New York. Garland Science.
Noble, A., Johnson, R. & Bass, P. (2010). The cardiovascular system: basic science and clinical conditions, (2nd ed.).
Edinburgh. Churchill, Livingstone, Elsevier.
Pagana, K.D. & Pagana, T.J. (2013). Mosby’s diagnostic and laboratory test reference, (11th ed.). St. Louis, MO. Elsevier.
Smith, M.E. & Morton, D.G. (2010). The digestive system: basic science and clinical conditions, (2nd ed.). Edinburgh.
Churchill, Livingstone, Elsevier.
VanMeter, K.C. & Hubert, R. (2014). Gould’s pathophysiology for health professions, (5th ed.). St. Louis, MO. Elsevier.

© Endeavour College of Natural Health endeavour.edu.au 37
COMMONWEALTH OF AUSTRALIA
Copyright Regulations 1969
WARNING
This material has been reproduced and
communicated to you by or on behalf of
the Endeavour College of Natural Health pursuant to
Part VB of the Copyright Act 1968 (the Act).
The material in this communication may
be subject to copyright under the Act.
Any further reproduction or
communication of this material by you
may be the subject of copyright
protection under the Act.
Do not remove this notice.