cardio pulmonary resuscitation
TRANSCRIPT

CPR GUIDELINES 2010
• Gordon –artificial ventilation• Elam and Safar-rescue breathing• Beck and Zoll-AC defibrillator• Lown-DC defibrillator• Kouwenhoven Knickerboker,jude-chest
compressions• CPR endorsed-1963• CPR guidelines-1966, 1973, 1979, 1985,
1992, 2000, 2005,2010

Actions linking the adult victim of sudden cardiac arrest with survival are called the adult Chain of Survival.
Epidemiology and Recognition of Cardiac Arrest-most common victim is a man between 50 and 75 years of age –with r/f
Incidence of cardiac arrest is lowest during sleep and begins to rise rapidly soon after awakening
Greater than 80% of patients -initiating event is a ventricular tachyarrhythmia (ventricular tachycardia) degenerating rapidly to ventricular fibrillation in 62% of cases, torsades de pointes in 13%, and primary ventricular fibrillation in 8%
Most important determinant of survival from sudden cardiac arrest is the presence of a trained lay rescuer who is ready, willing, and able to act.
As a rule of thumb, the American Heart Association recommends that at least 20% of the adult population should be trained in basic CPR to reduce mortality from out-of-hospital cardiac arrest
Each minute that a patient remains in ventricular fibrillation, the odds of survival decrease by 7% to 10%
Survival is highest when CPR is started within the first 4 minutes of arrest and advanced cardiac life support (ACLS), including defibrillation and drug therapy, is started within the first 8 minutes
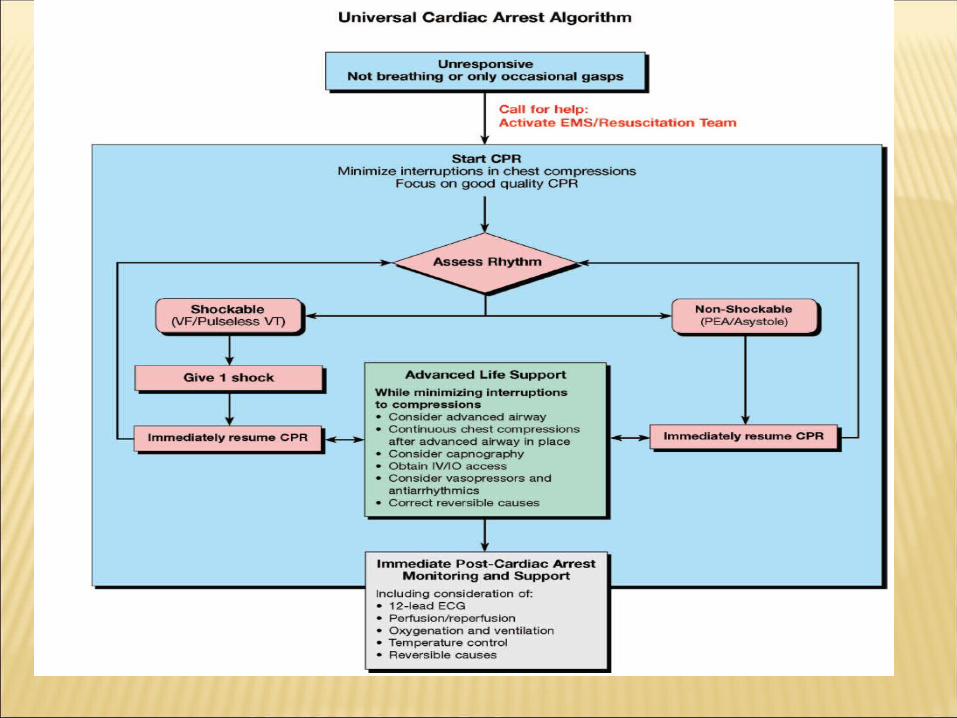
• Rescuers should begin CPR if an adult is unresponsive and not breathing normally
• Do not delay in an attempt to recognise a pulse
• Pulse Check-lay rescuers ,even healthcare providers perceived a pulse when it was nonexistent
• Breathing Assessment-agonal gasps are mistaken for regular breathing
• Circulatory assessment-non specific

Combination of absent breathing with unresponsiveness
Pulse alone not a good criterion Agonal gasps should not be mistaken
for breathing

For lay rescuers, interrupting chest compressions to perform a pulse check is not recommended.
For healthcare professionals, it is reasonable to check a pulse if an organized rhythm is visible on the monitor at the next rhythm check
Attempt to shorten the delay to first chest compressions for adult victims, experts came to the consensus that rescuers may consider starting CPR with chest compressions rather than ventilations (the sequence will then be “CAB”).

major determinant of neurologically intact survival from prolonged cardiac arrest because of VF -perfusion pressures generated by chest compressions rather than the blood gas composition, acid base balance, or the frequency or strength of defibrillation shocks

With sudden unexpected cardiac collapse from VF, the pulmonary veins, the left heart and the entire arterial system are filled with oxygenated blood and the recommended two ventilations do not increase arterial saturation

if chest compressions are initiated early and continued, many of these patients will continue to gasp, thereby providing physiologic ventilation that facilitates both oxygenation and venous return to the chest

• 241 patients randomly assigned to receive chest compression alone and 279 assigned to chest compression plus mouth-to-mouth ventilation
• Survival to hospital discharge was better among patients assigned to chest compression alone than among those assigned to chest compression plus mouth-to-mouth ventilation (14.6% vs. 10.4%), but the difference was not statistically significant (p = .18).
outcome after CPR with chest compression alone is similar to that after chest compression with mouth-to-mouth ventilation, and chest compression alone may be the preferred approach for bystanders

40% of 445 out-of-hospital cardiac arrests
46% of arrests caused by a cardiac etiology compared with 32% in other etiologies
Fifty-five percent of witnessed arrest patients had agonal activity compared with 16% of unwitnessed arrest patients

Agonal respirations occurred in 56% of arrests due to ventricular fibrillation compared with 34% of cases with a non ventricular fibrillation rhythm
Twenty-seven percent of patients with agonal respirations were discharged alive compared to 9% without them (p < .001).
Associated with increased survival

overall survival of out-of-hospital cardiac arrest ;
2.2 percent for those who were not receiving bystander CPR when the EMS arrived
4.2 percent for those who were receiving chest compressions plus mouth-to-mouth breathing
6.2 percent for those receiving chest-compression-only bystander CPR
Technique of closed-chest "cardiac massage" for cardiac arrest was first published in 1960-kouwenhoven, jude, and knickerbocker

Two models- Cardiac pump-younger,earlier
stages,normal chest walls,better survival
Thoracic pump-older,barrel chest,poorer survival

Hand position: The rescuer should compress the
lower half of the victim’s sternum-2005 guidelines
simplified way-Place the heel of your hand in the center of the chest with the other hand on top
Inter nipple line is not a relaible landmark.

chest compression rates 80/min were associated with ROSC in some studies.
chest compressions for adults at a rate of at least 100 compressions per minute.
There is insufficient evidence to recommend a specific upper limit for compression rate.
Pauses should be minimized to maximize the number of compressions delivered per minute
Chest Compression Depth measured compression depth during
adult human resuscitation is often less than 4 cm (1.5 inches)
Conflicting evidence regarding the utility of increasing depth of compression.
No improvement of myocardial blood flow with increased compression depth from 4 cm to 5 cm, although coronary perfusion pressure (CPP) improved from 7 to 14 mm Hg
Recommendation-reasonable to compress the sternum at least 2 inches/5 cm for all adult cardiac arrest victims
Insufficient evidence to recommend a specific upper limit for chest compression depth.

• Incomplete recoil during compressions is associated with reductions in mean arterial pressure, coronary perfusion pressure, cardiac output(LOE 4)
• Recommendation:allowing complete recoil of the chest after each compression may improve circulation, there is insufficient evidence to determine the optimal method to achieve the goal
Cough CPR:may be possible for a conscious, responsive person to cough forcefully and maintain enough blood flow to the brain to remain conscious for a few seconds until the arrhythmia disappears or is treated.
Blood flow is maintained by increased pressure in the chest that occurs during forceful coughs.
• Limited benefit of cough CPR during the initial seconds to minutes of cardiac arrest in patients who remained conscious in a controlled, monitored setting of electrophysiology testing
• Recommendation:only for patients maintaining consciousness during the initial seconds to minutes of VF or pulseless VT cardiac arrest in a witnessed, monitored, hospital setting (such as a cardiac catheterization laboratory).
• 3 prospective case series of VT in the electrophysiology laboratory-precordialthump by experienced cardiologists was of limited use (1.3% ROSC).
• Rhythm deterioration following precordial thump occurred in 3% of patients and was observed predominantly in patients with prolonged ischemia or digitalis-induced toxicity.
Precordial thump is ineffective for VF, and it should not be used for unwitnessed OHCA
Considered for patients with monitored, unstable VT if a defibrillator is not immediately available
Use of the precordial thump for witnessed onset of asystole –evidence equivocal

For patients in cardiac arrest, percussion (fist) pacing is not recommended

• Airway:head tilt– chin lift maneuver is feasible, safe, and effective
• Studies about jaw thrust are equivocal while studies about jaw lift with thumb in mouth are negative
• Recommendation:reasonable to open the airway using the head tilt– chin lift maneuver when assessing breathing or giving ventilations.

Each breath to be administered within 1 second, and delivered with enough volume to cause a visible rise in the anterior chest wall.
Administration of the two rescue breaths should be completed quickly, interrupting chest compression for only 10 seconds

Bystander reluctance inordinately long interruptions of
essential chest compressions Increases intrathoracic pressures,
thereby reducing the return of venous blood to the chest.

Compressions Only and Compressions Plus Ventilations:
Chest compressions alone -recommended for untrained laypersons
Chest compressions alone - trained laypersons if they are incapable of delivering airway and breathing maneuvers
Chest compressions with ventilations -trained laypersons who are capable of giving CPR with ventilations to cardiac arrest victims
Study based on 2005 guidelines-30:2 showed improvement of survival compared to survival with use of the previous 15:2 ratio
Animal studies (LOE 5) showed improved survival with a compression-ventilation ratio above 30:2
ratio of more than 100:2 was associated with a low ROSC rate and reduced arterial partial pressure of oxygen
Recommendation-ratio should be 30:2
Legitimate reasons for the interruption - Need to ventilate Need to assess the rhythm or to assess
ROSC Need to defibrillate.RECOMMENDATION:minimize
interruptions of chest compressions during the entire resuscitation attempt

Only an average of 5-15% of patients treated with standard CPR survive cardiac arrest and it is widely agreed that increasing the blood flow generated by chest compression will improve survival
Often done incorrectly, and incorrect chest compression can compromise survival.
Potentially better compression High quality chest compressions in a
moving ambulance Reduction in the number of emergency
medical systems (EMS) personnel needed to perform resuscitation

• Mimic intraaortic balloon counterpulsation.• Two rescuers are needed to perform this
technique: one compresses the sternum and the other interposes abdominal compressions between each pair of chest compressions
• Recommends -in-hospital resuscitation as an alternative to standard CPR whenever sufficient personnel trained in the technique are available
• maximize the force applied to the chest during compression
• By encircling the chest force can distributed over the chest, thereby reducing local stresses on the chest wall and allowing high forces to be safely applied.
• This distributed compression allows for large increases in intrathoracic pressure without the trauma inherent in applying force to a single point, as with standard chest compression
Typical inflation pressure is 250 mm Hg, and the chest compression rate is 60/minute.


Insufficient evidence to support or refute the use of IAC-CPR/ACD-CPR/Open chest-CPR/piston CPR
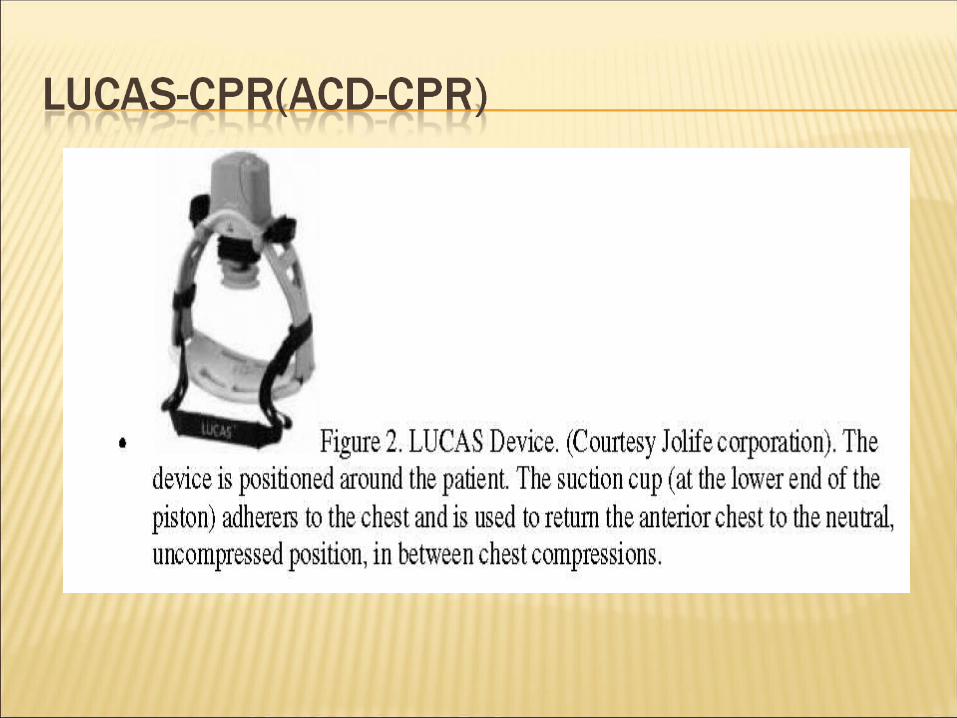
LUCAS/LDB-maintain continuous chest compression while undergoing CT scan or similar diagnostic studies, when provision of manual CPR would be difficult
BLS-CAB 3 GROUPS- VT/VF/PULSELESS ARREST BRADYASYSTOLE TACHYCARDIA WITH PULSES POST RESUCITATION CARE
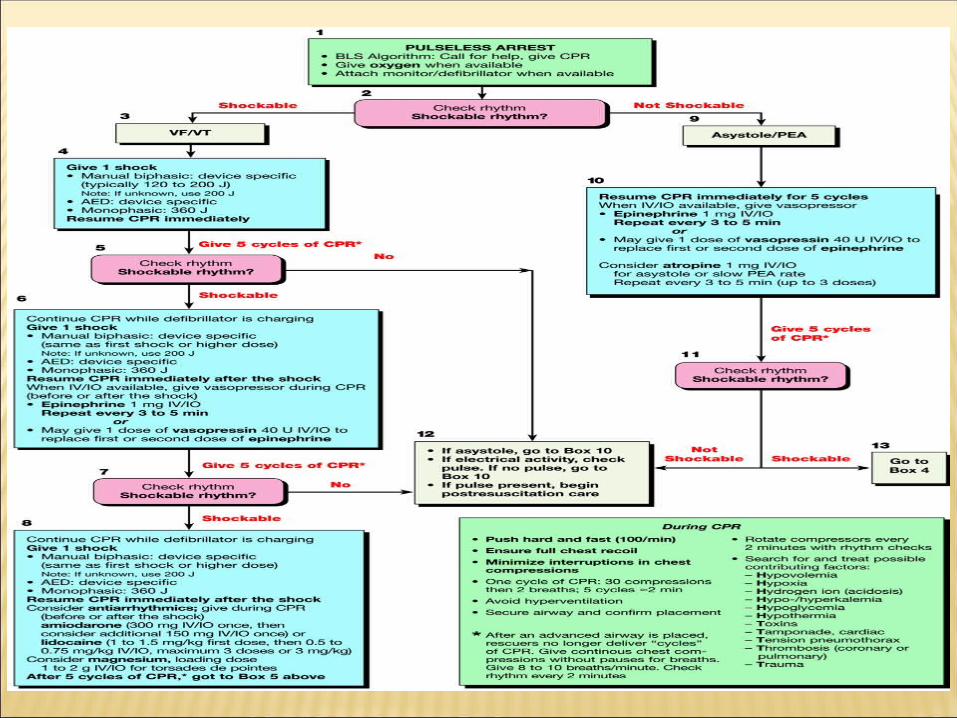
1. Electrical, phase of VF, lasts for about 4 to 5 minutes-defibrillation most effective in restoring rhythm
2. Circulatory, phase of untreated VF lasts for a variable period of time, but typically from about 5 to 15 minutes -defibrillation first during this "circulatory" phase –pulseless electrical activity

Metabolic phase of VF follows the circulatory phase-raely succseeful

Theoretical rationale for CPR before shock delivery is to improve coronary perfusion and thereby the chances of achieving sustained return of spontaneous circulation
Improvements in ROSC, survival to hospital discharge, neurologic outcome, and 1-year survival

Most crucial intervention -restoring myocardial blood flow by the generation of adequate coronary perfusion pressure with chest compressions prior to and immediately after defibrillation attempts
Chest compressions-improve the chances of restoring a perfusing rhythm following defibrillation

Recommendation:inconsistent evidence to support or refute delay in defibrillation to provide a period of CPR (90 seconds to 3 minutes) for patients in non EMS witnessed VF/pulseless VT cardiac arrest

Electrode-Patient Interface For both defibrillation and AF
cardioversion, when using biphasic defibrillators, self-adhesive defibrillation pads are safe and effective and are an acceptable alternative to standard defibrillation paddles
In AF cardioversion using monophasic defibrillators, hand-held paddles are preferable.

Reasonable to place paddles/pads on the exposed chest in an anterior-lateral position
The defibrillator paddle/pad should be placed on the chest wall ideally at least 8 cm from the generator position.
The anterior-posterior and anterior-lateral paddle/pad placements on the chest are acceptable in patients with a permanent pacemaker or icd

Reasonable to use a paddle/pad size 8 cm

Biphasic waveforms are more effective in terminating VF when compared with monophasic waveforms.
There is insufficient evidence to recommend any specific biphasic waveform.
In the absence of biphasic defibrillators, monophasic defibrillators are acceptable

It is reasonable to start at a selected energy level of 150 J to 200 J for a BTE waveform for defibrillation of pulseless VT/VF cardiac arrest.
monophasic defibrillation, initial and subsequent shocks using this waveform should be at 360 J.

For second and subsequent biphasic shocks the same initial energy level is acceptable.
It is reasonable to increase the energy level when possible

• Atrial fibrillation 100-200 (monophasic waveform)100-120 (biphasic waveform)Stepwise increase for subsequent shocks
• Atrial flutter 50-100Stepwise increase for subsequent shocks
• Supraventricular tachycardia due to reentry- 50-100Stepwise increase for subsequent shocks
• Ventricular tachycardia (VT) (monomorphic) 100Stepwise increase for subsequent shocks
• VT (polymorphic) 360 unsynchronized shock
• When defibrillation is required, a single shock should be provided with immediate resumption of chest compressions after the shock.
• Chest compressions should not be delayed for rhythm reanalysis or pulse check immediately after a shock.
• CPR should not be interrupted until rhythm reanalysis is undertaken.

High first-shock success rate of new defibrillators
Intervening chest compressions may improve oxygen and substrate delivery to the myocardium, making the subsequent shock more likely to result in defibrillation
Organised activity without effective circulation
Poor prognosis Treat reversible causes-
hypovolemia,pneumothorax Neck vein examination is helpful Proper CPR, Open massage in case of penetrating
trauma

Epinephrine:vasopressor of choice for use during resuscitation
improve cerebral blood flow by preventing arterial collapse and by increasing peripheral vasoconstriction
enhances coronary perfusion pressure, which is the major determinant of the ROSC after cardiac arrest

dose - 1 mg (10 mL of a 1:10,000 solution) every 3 to 5 minutes during resuscitation in adults
Continous infusion-1 mg of epinephrine hydrochloride to 250 mL of normal saline or dextrose 5% in water (D5W) to run at 1 µg/minute and increased to 3 to 4 µg/minute

Intracardiac injections increase the risk of coronary artery laceration, cardiac tamponade, and pneumothorax and cause interruption of external chest compression and ventilation-not advisable
Trials with doses of epinephrine >5mg showed no significant benefit
Vasopressin: recommended dose is 40 units IV in place of the first or second dose of epinephrine in the pulseless ventricular tachycardia/ventricular fibrillation algorithm.
last approximately 10 to 20 minutes No recommendation on optimal dose
Anoxic arrest of the heart causes a progressive increase in the concentration of PCO2 inside heart muscle cells that may reach very high levels (90 to 475 Torr)
Above an intramyocardial PCO2 of approximately 475 Torr, pulseless electrical activity is present and the heart cannot be resuscitated

Severe arterial acidosis –inadequate ventilation
Correct the inadequacy of CPR technique. Soda bicarb-if given will increase
intracellular Co2 and will cause further deterioration.
Can be given in cases of pre existing metabolic acidosis,renal failure,hyperkalemia


Amiodarone may be considered for those who have refractory VT/VF, defined as VT/VF not terminated by defibrillation, or VT/VF recurrence in out-of-hospital cardiac arrest or in-hospital cardiac arrest.
There is inadequate evidence to support or refute the use of lidocaine in the same settings

Monomorphic VT-w/o CHF/MI-procainamide With MI/CHF-amiodarone Sotalol can be considered in setting of MI

Amiodarone reduced the frequency of recurrent arrhythmias.
Magnesium –torsades de pointes

Vagal maneuvers, IV adenosine, verapamil, and diltiazem are recommended as first-line treatment strategies in the termination of narrow-complex tachycardias


Refers to a cardiac rhythm that has a ventricular rate below 60 beats per minute in adults and/or periods of absent heart rhythm (asystole)
Survival is poor (generally 1% to 3% or less)

• 1-mg dose of atropine IV and is repeated every 3 to 5 minutes if asystole persists.
• Three milligrams (0.04 mg/kg) given IV is a fully vagolytic dose in most patients
• The administration of a total vagolytic dose of atropine should be reserved for patients with bradyasystolic cardiac arrest.
• Endotracheal atropine produces a rapid onset of action similar to that observed with IV injection. The recommended adult dose of atropine for endotracheal administration is 1.0 to 2.0 mg diluted in 10 mL of sterile water
If not effective, then consider
epinephrine (2 to 10 g/min) or dopamine (2 to 10 g/kg/min).
Cardiac transplant, theophylline 100 to 200 mg slow injection IV(maximum 250 mg) may be given.

Use of pacing (eg, TC, TV, and needle) in cardiac arrest (in- or out-of-hospital) did not improve ROSC or survival.
no apparent benefit related to the time at which pacing was initiated (early or delayed in established asystole), location of arrest (out-of-hospital or in-hospital), or primary cardiac rhythm (asystole or PEA

Airway- Maintained by endo tracheal intubation Supraglottic airway is an alternative End tidal Pco2 is an useful adjunct

Percentage of carbon dioxide contained in the last few milliliters of gasexhaled from the lungs with each breath -end-tidal carbon dioxide concentration (PetCO2)
Measured by capnography-infrared device/colorimetry
Useful information on the anatomic location of an airway device
normal respiration and circulation, the PetCO2 averages 4% to 5%.
normal or elevated levels of cardiac output, ventilation is the rate-limiting factor
At low levels of cardiac output-ventilation is fixed -reflects change in cardiac output

Ventilation through an ET tube that has been properly inserted in the trachea yields a PetCO2 of 4% to 5% in a patient with a normal cardiac output and no significant ventilation/perfusion gradient
ventilation through an ET tube that has been inadvertently inserted into the esophagus results in a PetCO2 of less than 0.5%
Dramatic change from a low to a high PetCO2 due to venous carbon dioxide washout is often the first clinical indicator that ROSC has occurred
PetCO2 typically returns to normal (4% to 5%) within 2 to 5 minutes after ROSC if the patient maintains a good cardiac output.

• Resternotomy for patients with cardiac arrest following cardiac surgery should be considered in an appropriately staffed and equipped ICU
• Chest compressions should not be withheld while preparing for emergency resternotomy.
• Mechanical circulatory support may be considered in the setting of cardiac arrest following cardiac surgery.
Return of spontaneous circulation (ROSC) does not mean full recovery for the victim or even survival.
Postresuscitation deaths are highest in the first 24 hours after ROSC; therefore, postresuscitation care is critical for survival.

Assess adequacy of ventilationTitarate doses of medication-
ionotropesRepeat echo and ECGAssess for factors that could have led
to arrestCAD-early revascularisation







Avoid hyperthermia Seizure control Tight glucose control Organ specific evaluation and support

• 5 clinical signs that were found to strongly predict death or poor neurologic outcome, with 4 of the 5 predictors detectable at 24 hours after resuscitation:
• ● Absent corneal reflex at 24 hours• ● Absent pupillary response at 24 hours• ● Absent withdrawal response to pain at 24 hours• ● No motor response at 24 hours• ● No motor response at 72 hours• An electroencephalogram performed 24 to 48
hours after resuscitation has also been shown to provide useful predictive information and can help define prognosis
resuscitation efforts should be continued until "reliable criteria indicating irreversible death are present.”
This position leaves more latitude for the judgment of the medical personnel involved, but is more difficult to apply uniformly in practice.

CPR 2010 guidelines promote adherence to chain of survival principles
Importance of maintaining circulation by compressions is given priority changing the well known ABC to CAB.
Interruption of compressions to be minimised even for acts like pulse check,rescue breaths,rhythm analysis

Utility of 90 second CPR before defibrillation is not proven beyond doubt
End tidal CO2 is auseful guide for positioning ET tube as well as predicting success of CPR
Mechanical devices and alternate techniques can only be recommended in special situations
Induced hypothermia should be considered in comatose patients,especially post VF.