cardiac arrest registry to enhance survival - national …/media/files/activity files... · cardiac...
TRANSCRIPT

Bryan McNally, MD, MPH
Executive Director CARES
Associate Professor of Emergency Medicine
Emory University School of Medicine
Rollins School of Public Health
Atlanta, Georgia USA
Cardiac Arrest Registry to Enhance Survival
CARES Funding Partners
American Red Cross
American Heart Association
Emory University
Medtronic Philanthropy
Zoll Corporation
CDC (2004-2012)


CARES Mission Statement
To help communities determine standardized
outcome measures for out-of-hospital cardiac
arrest allowing for quality improvement efforts
and benchmarking capability to improve care
and increase survival.

CARES Vision Statement
To become the standard out-of-hospital
cardiac arrest registry for the United
States allowing for uniform data collection
and quality improvement in each state and
nationally.

Impact of the Links in the Chain of Survival
New England Journal of Medicine, 2004; 351(7): 647-656

Disparate outcomes are almost certainly due to timeliness and quality of
treatment.
What can we attribute the variation in survival to? Links in the “Chain of Survival”

You can’t manage what
you can’t measure!
The first step to improving survival rates is to begin
collecting data in order to better understand performance

“Most cities don’t measure their
performance effectively, if at all.
They don’t know how many lives
they are losing, so they can’t
determine ways to increase
survival rates.”
- Bob Davis, “Six Minutes to Live” USA Today, 2003

Institute of Medicine Report on EMS
“What is missing is a standard
set of measures that can be used
to assess the performance of the
emergency and trauma care
system within each community,
as well as the ability to
benchmark that performance
against statewide and national
performance metrics.”

Quality Improvement Elements of a
Resuscitation System
Developing a culture of high quality resuscitation. Travers AH, et al. (2010) Circulation;122:S676-S684

OHCA Registries
Danish Registry
OHCAR - Ireland
Swedish Registry
Japanese All Utstein Registry
EuReCa- Europe
PAROS – Asia
CARES - US
ROC-North America


Need for a registry CARES
Data collection mechanism
• Makes the data collection process more
efficient - linkage between EMS, Hospital
and dispatch outcome
• Benchmarking capabilities
• Measurement tool for effectiveness
CARES as a uniform data collection
system for OHCA
• Data collection into a registry at the regional,
state or national level enables providers or EMS
systems to benchmark their outcomes and
results with other communities
• Allows for identification of strengths and
weaknesses used to improve the quality of care
• Steps toward making cardiac arrest a
reportable disease
Sansio
Mainframe housed in Duluth, MN USA
Internet database system
https://mycares.net
HIPAA compliant security
Reporting features
Utstein Survival Reports
EMS/FR response time reports
Demographic reports
Excel Export
Unifies EMS, 911 dispatch, and hospital data
Any EMS system throughout US
CARES software is web based Allows for the consolidation of three separate silos of data
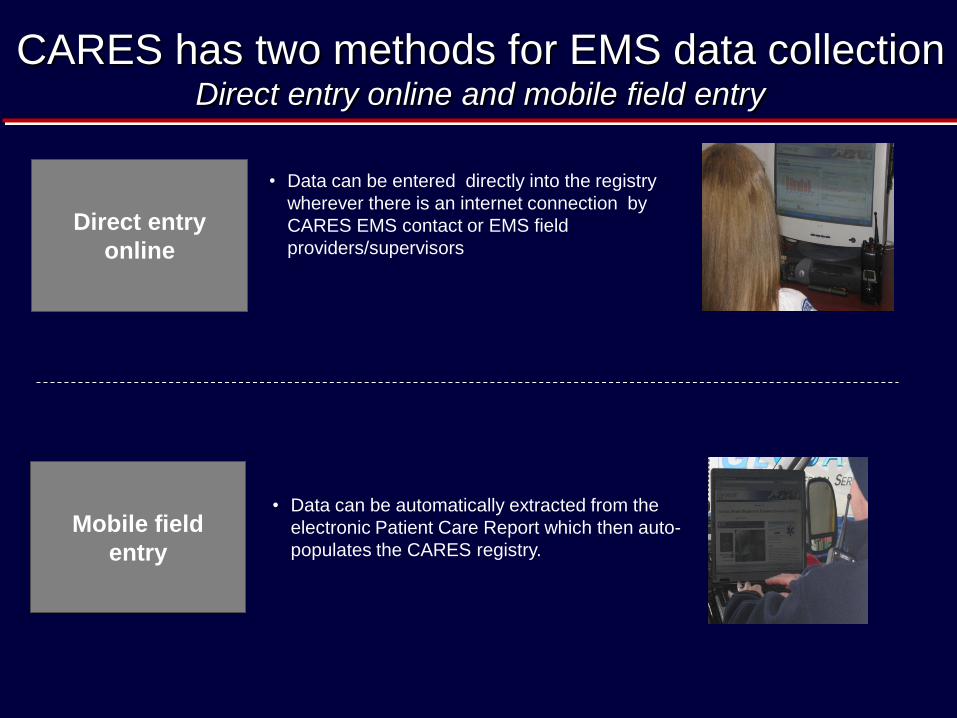
CARES has two methods for EMS data collection Direct entry online and mobile field entry
Direct entry
online
Mobile field
entry
• Data can be entered directly into the registry
wherever there is an internet connection by
CARES EMS contact or EMS field
providers/supervisors
• Data can be automatically extracted from the
electronic Patient Care Report which then auto-
populates the CARES registry.


Hospital component

CARES 2014 Site Map

CARES International Collaboration

CARES 2013 Catchment Area
The registry covers a population of over 75 million.
This represents more than 25% of the US population.
0
10,000,000
20,000,000
30,000,000
40,000,000
50,000,000
60,000,000
70,000,000
80,000,000
4th
-20
05
1st
-20
06
2n
d-2
00
6
3rd
-20
06
4th
-20
06
1st
-20
07
2n
d-2
00
7
3rd
-20
07
4th
-20
07
1st
-20
08
2n
d-2
00
8
3rd
-20
08
4th
-20
08
1st
-20
09
2n
d-2
00
9
3rd
-20
09
4th
-20
09
1st
-20
10
2n
d-2
01
0
3rd
-20
10
4th
-20
10
1st
-20
11
2n
d-2
01
1
3rd
-20
11
4th
-20
11
1st
-20
12
2n
d-2
01
2
3rd
-20
12
4th
-20
12
1st
-20
13
2n
d-2
01
3
3rd
-20
13
4th
-20
13
Po
pu
lati
on
Qtr/Year
Cumulative Catchment Area

CARES 2013 Registry Volume
0
5,000
10,000
15,000
20,000
25,000
30,000
35,000
40,000
Oct-Dec 2005 2006 2007 2008 2009 2010 2011 2012 2013
Annual Call Volume
Presumed cardiac etiology All etiologies
It is estimated that once all 2013 data is entered & audited, there will
be > 35,000 with >130,000 cumulative records in the registry.

2005-2012 N=73,075
*Presumed Cardiac Etiology
SUMMARY OF AGGREGATE
NATIONAL CARES DATA
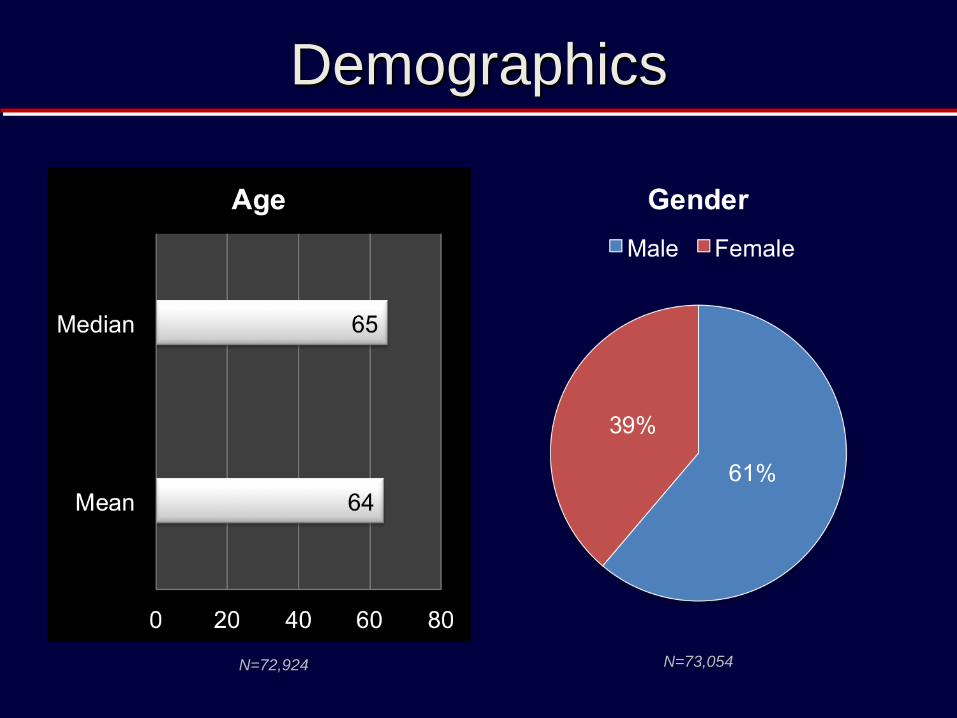
Demographics
N=72,924 N=73,054

Demographics
N=72,915
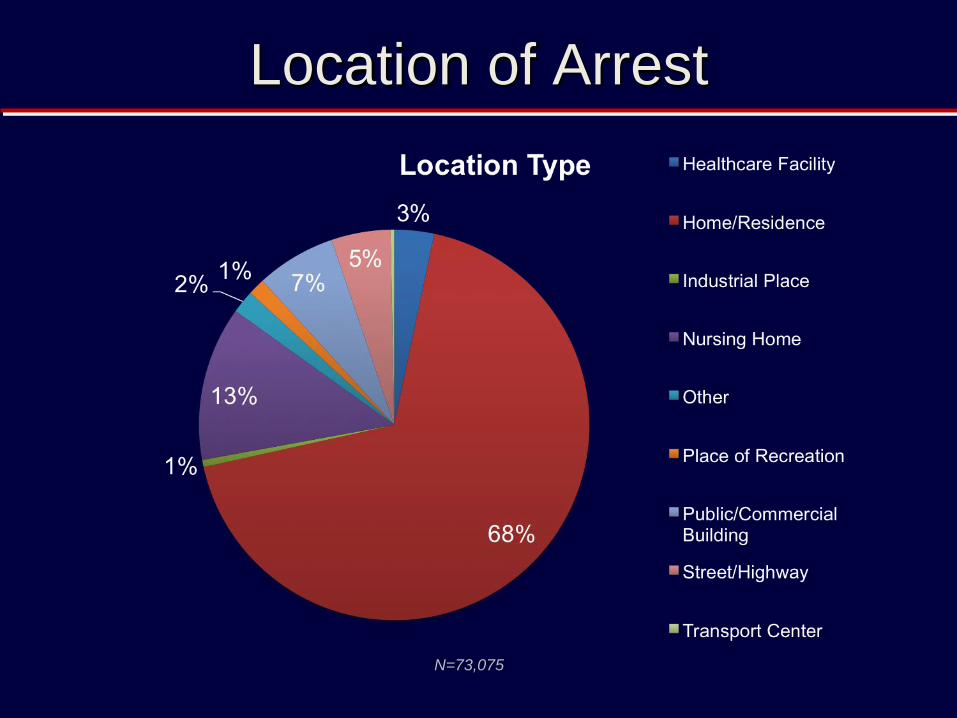
Location of Arrest
N=73,075

Witnessed Status & CPR Initiation
N=73,074 N=73,055

AED Application & First Defibrillation
N=72,259 N=34,706

First Arrest Rhythm & ROSC
N=73,060
N=72,570

Hypothermia & Pre-Hospital Outcome
N=50,179 N=73,073
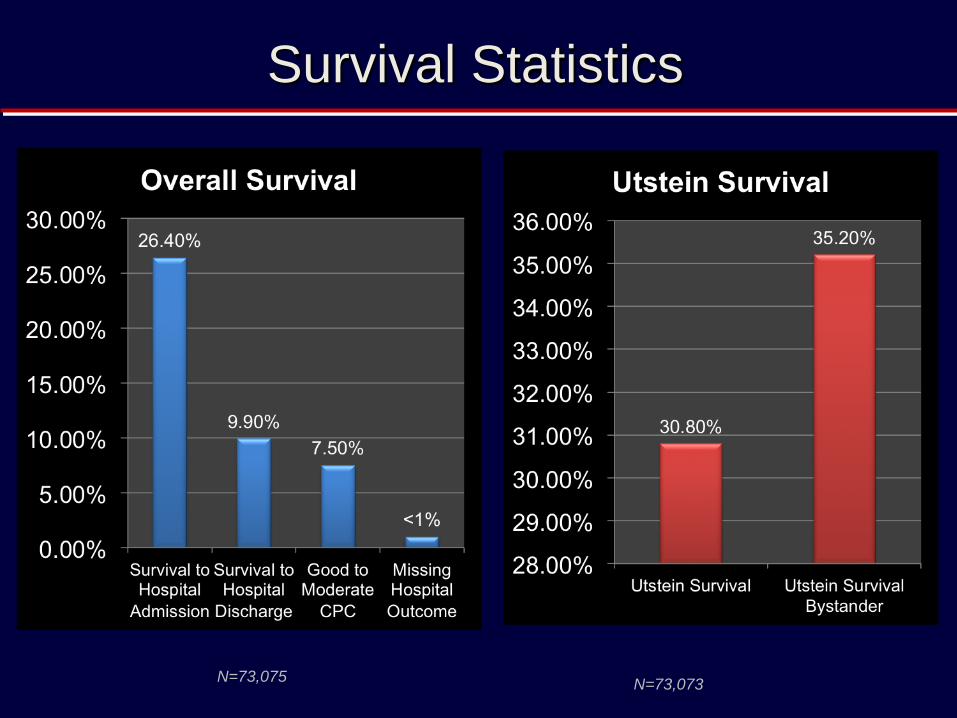
Survival Statistics
N=73,075 N=73,073
221
417
1403
3070 4388
4454 3659 2620 1774 1265
804 578
1322 120
231
819 1864 2674 2669 2153 1479 996 741 439
330
731
101 186
584
1206
1717
1782 1506 1141 778
524 365 248 591
45
70 261 477
695
672 562 401
264
165
115
74
176
0
5
10
15
20
25
30
35
40
45
0-1 1-2 2-3 3-4 4-5 5-6 6-7 7-8 8-9 9-10 10-11 11-12 >12
Su
rviv
al R
ate
(%
)
Response Time Interval (minutes)
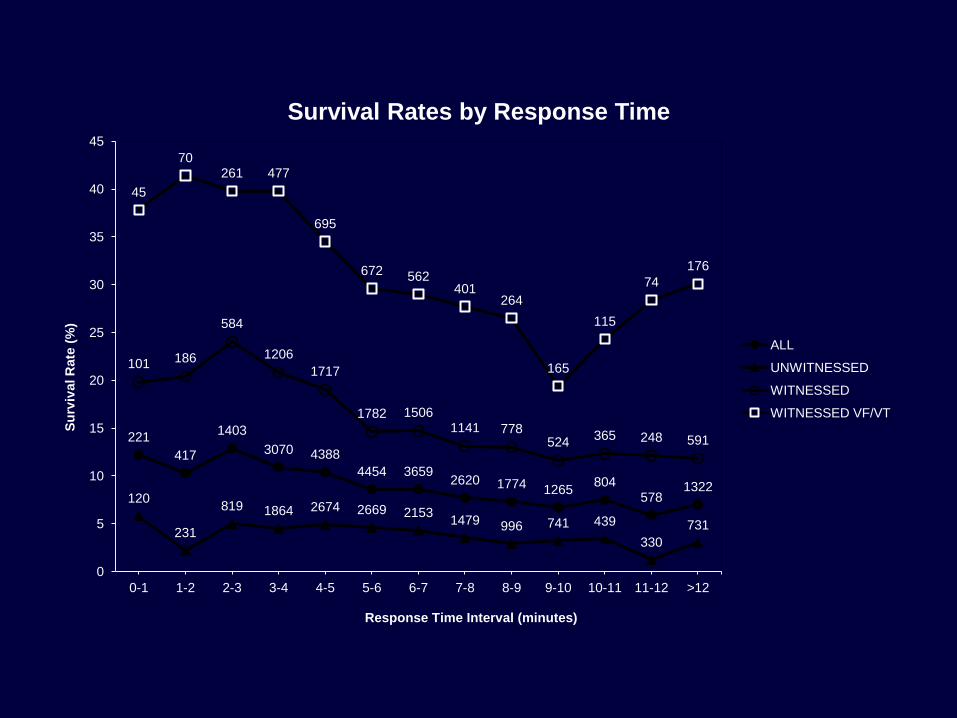
Survival Rates by Response Time
ALL
UNWITNESSED
WITNESSED
WITNESSED VF/VT

CARES 2005-2010 Summary Data

2010 Cohort – Who Initiated CPR?
2010 2011 2012
Communities Participating in 2010 Population of 26,688,033

2010 Cohort - Survival
2010 2011 2012

CARES Utstein Survival Report

CARES State Based Reports

CARES Hospital Report
Local
Local Your state
Your state Local

CARES - New England Journal of Medicine 2012
Predicted probability of Bystander Initiated
CPR

Linkage to Medicare Payment Data
Mean hospitalization cost twice national average
African American hospitalization cost almost double Caucasian.
Hospital payment for top male + female patient > CARES Budget

CARES AIRWAY DATA
Airway management and OHCA outcome in the CARES registry
Resuscitation February 2014 In Press. McMullen J, et al.

AIRWAY STUDY PROPOSAL

CARES Registry 2005-2012

Danish OHCA Registry JAMA November 2013

Japanese Utstein Registry

Dispatch Chain of Survival

https://mycares.net/sitepages/dispatchtraining.jsp
T-CPR

CARES Allows communities to determine OHCA
outcomes & identify high risk groups and neighborhoods
Enables clinical benchmarking to identify opportunities for improvement and track the diffusion of new therapies
Promotes accountability to improve the quality and impact of prehospital care
Observational data for effectiveness research
