breast cancer surgery in the elderly - samo-workshop.ch · breast cancer surgery in the elderly dr....
TRANSCRIPT
SAMO Interdisciplinary Workshop on Breast Tumors
Breast cancer surgery in the Elderly
Dr. med. Federica ChiesaBrustzentrum St. Gallen
SAMO Interdisciplinary Workshop on Breast Tumors
Summary
1. Population ageing
2. Definition of «elderly»
3. Geriatric assessments
4. Impact of breast cancer on survival
2
4. Impact of breast cancer on survival
5. Surgery yes or no?
6. Primary endocrine therapy
7. Conservative surgery vs. mastectomy
SAMO Interdisciplinary Workshop on Breast Tumors
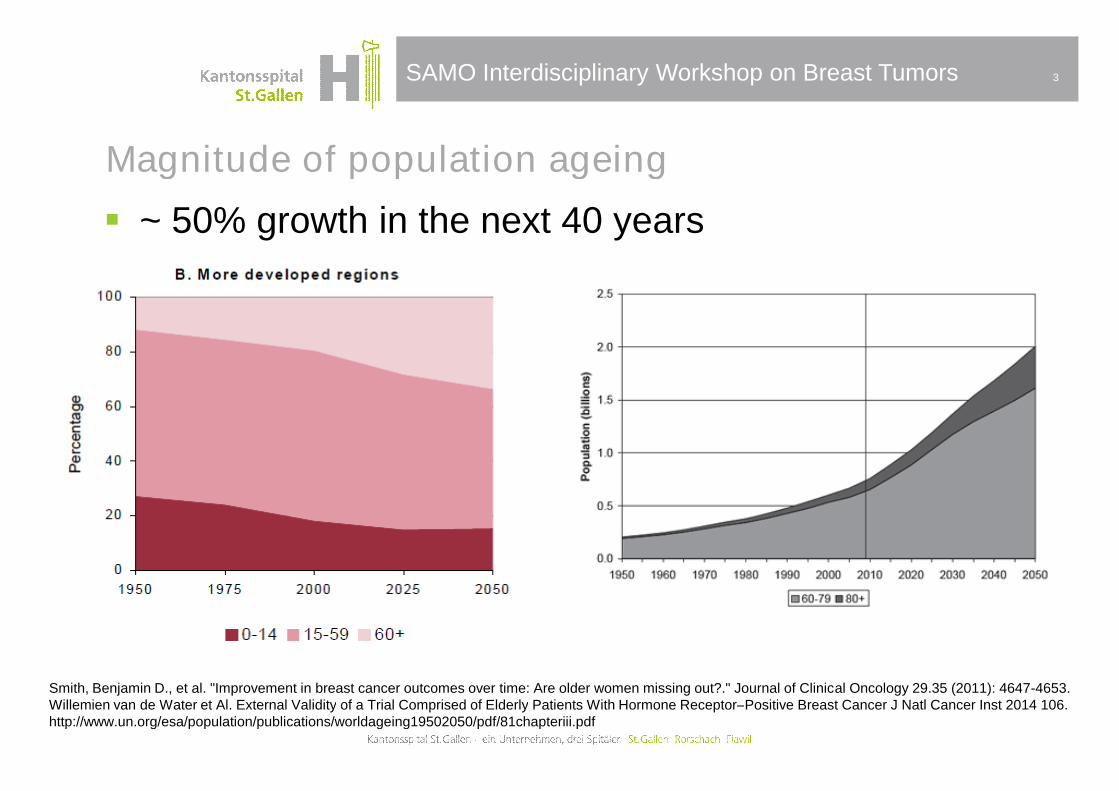
Magnitude of population ageing
3
~ 50% growth in the next 40 years
Smith, Benjamin D., et al. "Improvement in breast cancer outcomes over time: Are older women missing out?." Journal of Clinical Oncology 29.35 (2011): 4647-4653.Willemien van de Water et Al. External Validity of a Trial Comprised of Elderly Patients With Hormone Receptor–Positive Breast Cancer J Natl Cancer Inst 2014 106.http://www.un.org/esa/population/publications/worldageing19502050/pdf/81chapteriii.pdf
SAMO Interdisciplinary Workshop on Breast Tumors
Who is “old”?
biological age ≠ chronological age
Elderly is a controversial definition:
Chronological age of 65+ y.
4
Chronological age of 65+ y.
WHO: 60/50+ y.
Deutsches Konsensus: 70+ y. and multimorbidity
or 80+ y.
http://www.who.int/healthinfo/survey/ageingdefnolder/en/http://www.bv-geriatrie.de/presse/20070131.pdf
SAMO Interdisciplinary Workshop on Breast Tumors
Heterogeneous “elderly” population
Common elderly sub-populations:
young old: 65–74 years
older old: 75–84 years
oldest old: 85+ years
5
frailty
SAMO Interdisciplinary Workshop on Breast Tumors
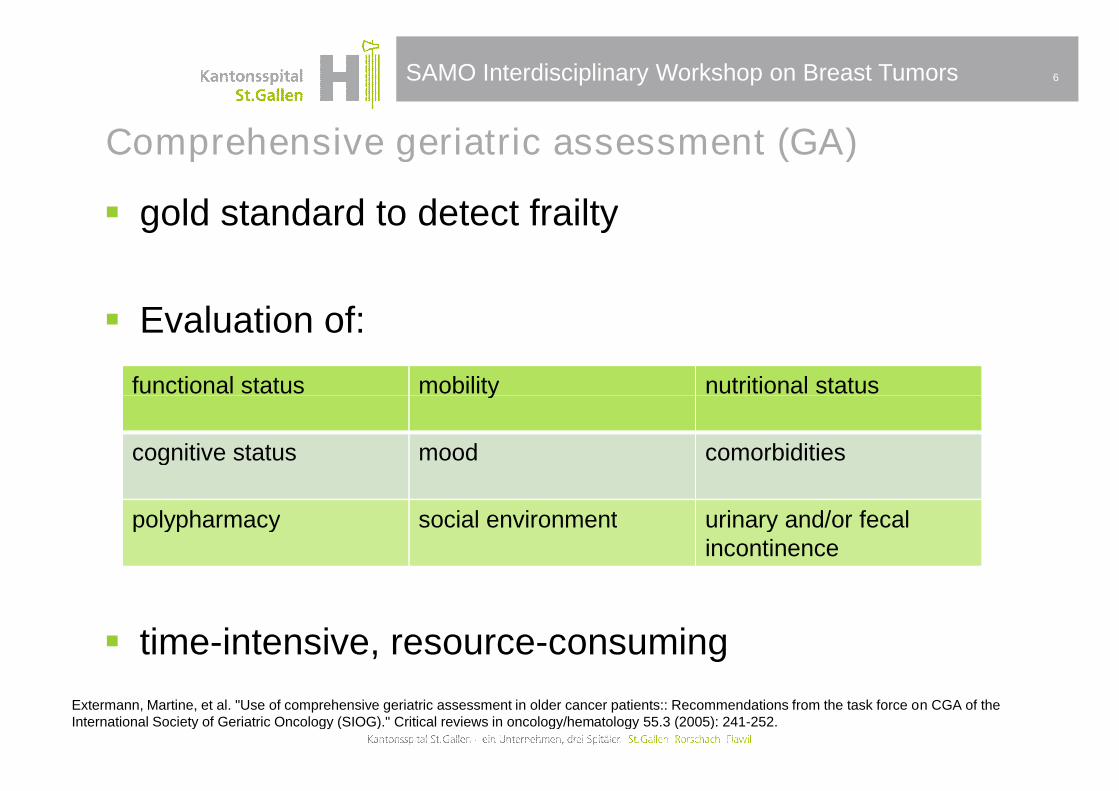
Comprehensive geriatric assessment (GA)
gold standard to detect frailty
Evaluation of:
6
functional status mobility nutritional status
time-intensive, resource-consuming
Extermann, Martine, et al. "Use of comprehensive geriatric assessment in older cancer patients:: Recommendations from the task force on CGA of theInternational Society of Geriatric Oncology (SIOG)." Critical reviews in oncology/hematology 55.3 (2005): 241-252.
functional status mobility nutritional status
cognitive status mood comorbidities
polypharmacy social environment urinary and/or fecalincontinence
SAMO Interdisciplinary Workshop on Breast Tumors
Cancer Specific Geriatric Screening Tools
feasible in busy oncology practices
easy & quick
prognostic
7
SAKK cancer-specific geriatric assessment: Charlson Comorbidity Index
G8 – Screening tool
Short geriatric depression scale (8-item)
Mini-Cog
Decoster, L., et al. "Screening tools for multidimensional health problems warranting a geriatric assessment in older cancer patients: an update on SIOGrecommendations." Annals of Oncology (2014): mdu210.Clough-Gorr, Kerri, et al. "The SAKK cancer-specific geriatric assessment (C-SGA): a pilot study of a brief tool for clinical decision-making in older cancerpatients." BMC Med. Inf. & Decision Making 13 (2013): 93.

SAMO Interdisciplinary Workshop on Breast Tumors
G8 Screening tool
Items Possible answers Score
A
Has food intake declined over the
past 3 months due to loss of
appetite, digestive problems,
chewing or swallowing difficulties?
0: severe reduction in food intake
1: moderate reduction in food
intake
2: normal food intake
………...
B
Weight loss during the last 3
months?
0: weight loss >3kg
1: does not know
2: weight loss between 1 and 3 kg
3: no weight loss
………...
C
Mobility 0: bed or chair bound
1: able to get out of bed/chair but
does not go out
2: goes out
………...
Neuropsychological problems 0: severe dementia or depression
8
Mini-Cog
E
Neuropsychological problems 0: severe dementia or depression
1: mild dementia or depression
2: no psychological problems
………...
F
Body Mass Index (weight in
kg/height in m2)
0: BMI less than 19
1: BMI 19 to less than 21
2: BMI 21 to less than 23
3: BMI 23 or greater
………...
HTakes more than 3 medications per
day
0: yes
1: no ………...
P
In comparison with other people of
the same age, how does the patient
consider his/her health status?
0: not as good
0,5: does not know
1: as good
2: better
………...
Age 0: >85
1: 80-85
2: <80
………...
Total score (0-17) A score of ≤14 is abnormal
………...
SAMO Interdisciplinary Workshop on Breast Tumors
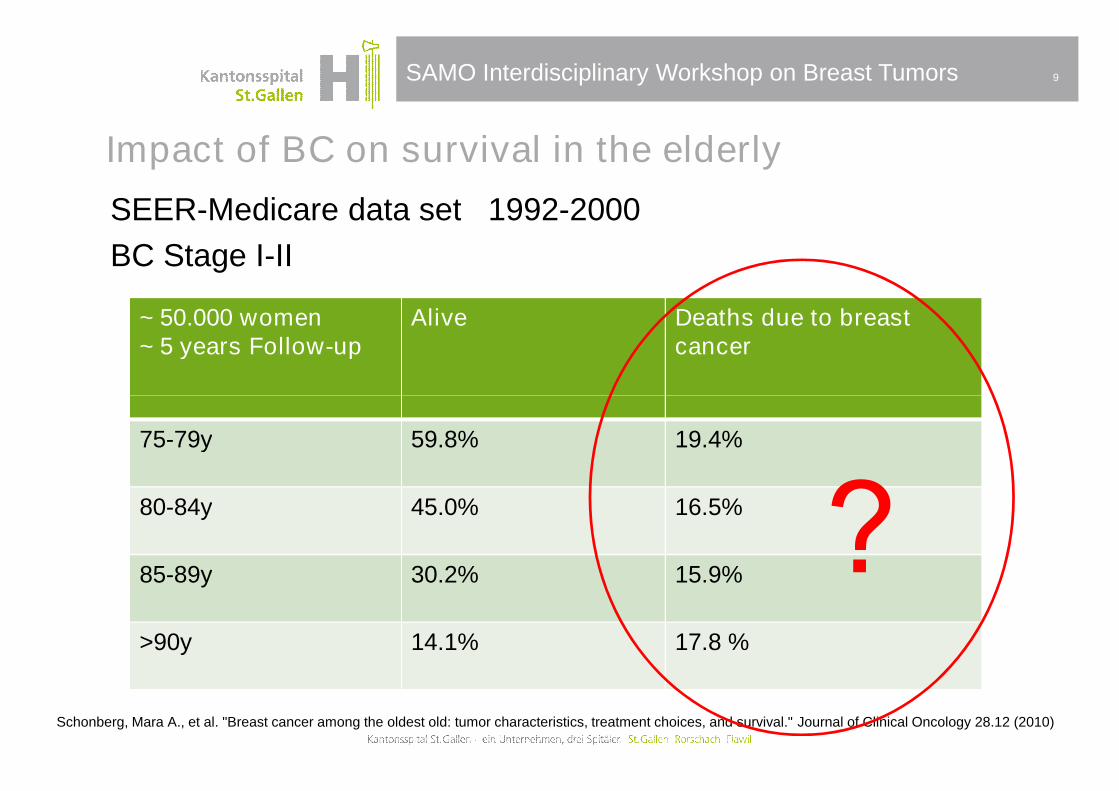
Impact of BC on survival in the elderly
SEER-Medicare data set 1992-2000
BC Stage I-II
9
~ 50.000 women~ 5 years Follow-up
Alive Deaths due to breastcancer
Schonberg, Mara A., et al. "Breast cancer among the oldest old: tumor characteristics, treatment choices, and survival." Journal of Clinical Oncology 28.12 (2010)
75-79y 59.8% 19.4%
80-84y 45.0% 16.5%
85-89y 30.2% 15.9%
>90y 14.1% 17.8 %
SAMO Interdisciplinary Workshop on Breast Tumors
Challenges of breast cancer treatment in the elderly
10
Comorbidities
Treatment-related toxicity
Patients and families wishes
Lack of evidence-based data Lack of evidence-based data
34-fold probability of non “state-of-the-art” treatment
Smith, Benjamin D., et al. "Improvement in breast cancer outcomes over time: Are older women missing out?." Journal of Clinical Oncology 29.35 (2011): 4647-4653.Willemien van de Water et Al. External Validity of a Trial Comprised of Elderly Patients With Hormone Receptor–Positive Breast Cancer J Natl Cancer Inst 2014 106.Lewis JH, Kilgore ML, Goldman DP, Trimble EL, Kaplan R, Montello MJ, Housman MG, Escarce JJ (2003) Participation of patients 65 years of age or older in cancerclinical trials. J Clin Oncol 21: 1383–1389Ess, S., et al. "Predictors of state-of-the-art management of early breast cancer in Switzerland." Annals of oncology (2010)

SAMO Interdisciplinary Workshop on Breast Tumors
Operable breast cancer
Schonberg M A et al. JCO 2010;28:2038-2045
Initial treatment by age at diagnosis

SAMO Interdisciplinary Workshop on Breast Tumors
Study proposal: Swiss elderly breast cancer study
Breast CancerStage I,II, operable
«standard» treatment
outcome
Medicalrecommendations
&Performed treatment
Stage I,II, operableIII80+y orFrail 70-79y
«tailored» treatment
outcome
follow-up

SAMO Interdisciplinary Workshop on Breast Tumors
Breast surgery in the elderly: yes or no?
13

SAMO Interdisciplinary Workshop on Breast Tumors
Surgery risks in the Elderly
Breast surgery mortality rate <1%
low specific risk surgery
anesthetic risk: related to co-morbidities not to age
14
→ Elderly tolerate breast surgery like younger patients
Moller, Jakob Trier, et al. "Long-term postoperative cognitive dysfunction in the elderly: ISPOCD1 study." The Lancet 351.9106 (1998): 857-861.Samain, Emmanuel, et al. "Anesthesia for breast cancer surgery in the elderly." Critical reviews in oncology/hematology 46.2 (2003): 115-120.Audisio, Riccardo A., et al. "Preoperative assessment of surgical risk in oncogeriatric patients." The Oncologist 10.4 (2005): 262-268.

SAMO Interdisciplinary Workshop on Breast Tumors
Primary endocrine therapy
Same OS Less local control
Johnston, S. J., et al. "A randomised trial of primary tamoxifen versus mastectomy plus adjuvant tamoxifen in fit elderly women with invasive breast carcinoma of highoestrogen receptor content: long-term results at 20 years of follow-up." Annals of oncology 23.9 (2012): 2296-2300.

SAMO Interdisciplinary Workshop on Breast Tumors
Response duration on primary Tamoxifen
time to best response ~ 5 mo
time to local relapse ~ 19 mo
Hind, Daniel, et al. "Surgery versus primary endocrine therapy for operable primary breast cancer in elderly women (70 years plus)." Cochrane Database Syst Rev1.1 (2006).O’Connor, Tracey, et al. "Managing Breast Cancer in the Older Patient." Clinical advances in hematology & oncology: H&O 11.6 (2013): 341
local progression
38% after 5 years
43% after 10 years
SAMO Interdisciplinary Workshop on Breast Tumors
Primary endocrine therapy (PET)
systematic review of the literature
Six RCT and 31 non-randomised studies
older patients with life expectancy >5 years: surgery better than PET for:
17
BC specific survival (90% vs 85% p< .01)
Overall survival (67% vs 49% p< .01)
aromatase inhibitors work better than Tamoxifen
PET: good for women unfit for surgery or who refuse surgery
Morgan, J. L., M. W. Reed, and L. Wyld. "Primary endocrine therapy as a treatment for older women with operable breast cancer–A comparison of randomisedcontrolled trial and cohort study findings." European Journal of Surgical Oncology (EJSO) 40.6 (2014): 676-684.

SAMO Interdisciplinary Workshop on Breast Tumors
Breast Conserving Surgery or Mastectomy?
If given a choice, older women prefer breastconservation over mastectomy
Better QOL after conservative treatment also for elderly
18
Better QOL after conservative treatment also for elderly
Old women do care!
Sandison, A. J. P., et al. "Breast conservation or mastectomy: treatment choice of women aged 70 years and older." British journal of surgery 83.7 (1996): 994-996.Di Maio, Massimo, and Francesco Perrone. "Quality of Life in elderly patients with cancer." Health and Quality of Life Outcomes 1.1 (2003): 44.

SAMO Interdisciplinary Workshop on Breast Tumors
Radiation after breast conserving surgery
Time to local or regional recurrence.
Smith, Benjamin D., and Thomas A. Buchholz. "Radiation treatments after breast-conserving therapy for elderly patients." Journal of Clinical Oncology 31.19(2013): 2367-2368.Hughes K S et al. JCO 2013;31:2382-2387
SAMO Interdisciplinary Workshop on Breast Tumors
Take home messagesSIOG and EUSOMA recommendations
Elderly tolerate surgery like younger patients
20
They should be offered the same surgical options
Standard of care is BCS and RT or mastectomy +/- RT
Biganzoli, Laura, et al. "Management of elderly patients with breast cancer: updated recommendations of the International Society of Geriatric Oncology(SIOG) and European Society of Breast Cancer Specialists (EUSOMA)." The lancet oncology 13.4 (2012): e148-e160.Wildiers, H. et al. "Management of breast cancer in elderly individuals: recommendations of the International Society of Geriatric Oncology." The lancetoncology 8.12 (2007): 1101-1115.