board meeting agenda - champlain lhin/media/sites/champlain/.../20160427brdpkg… · 2 agenda item...
TRANSCRIPT
1900 City Park Drive, Suite 204 Ottawa, ON K1J 1A3 Tel 613.747.6784 • Fax 613.747.6519 Toll Free 1.866.902.5446 www.champlainlhin.on.ca
1900, promenade City Park, bureau 204 Ottawa, ON K1J 1A3 Téléphone : 613 747-6784 • Télécopieur : 613 747-6519 Sans frais : 1 866 902-5446 www.rlisschamplain.on.ca
BOARD MEETING AGENDA
April 27, 2016
In-Camera meeting: 11:30 to 12:30 p.m. -- Public Meeting 13:00 to 17:35 p.m.
Champlain LHIN Office – 1900 City Park Drive, suite 500
(See page 3 for directions)
Agenda Item
&
Time
Documents
Attached,
Posted or Pre-
Circulated
Action
D= Decision
I = Information
S=Strategic Discussion
Strategic Plan
Reference(s)
(see legend
below)
1 11:30
Call to Order and Moment of Reflection
2
Conflict of Interest Declarations
3
Approval of Agenda D
4
12:30
In-Camera Session
Motion to move into closed session to receive
confidential information relating to:
4.1 Approval of confidential minutes: March 23, 2016
4.2 Chair’s Report
4.3 CEO Performance Evaluation and Compensation
Committee
4.4 CEO’s Report
D
I
D
I
1,2,3
12:30-13:00 BREAK
5
13:00
Welcome and Introduction
Chair’s Report and Report of In-Camera Session
1,2,3
6
13:10
CEO’s Report:
Approval of Attestations Fourth Quarter
No
D 1,2,3

2
Agenda Item
&
Time
Documents
Attached,
Posted or Pre-
Circulated
Action
D= Decision I = Information
S=Strategic
Discussion
Strategic Plan
Reference(s) (see legend
below)
7
13:20
Consent Agenda Items
7.1 Approval of draft minutes: March 23, 2016
Posted once
approved &
translated
D
1,2,3
8
13 :20
13 :45
14:20 – 14:35
14 :35
15 :05
15 :25
15 :35
15 :55
16 :05
16 :45
16:55-17 :15
Performance Accountability
8.1 Approval of Mississippi River Health Alliance
8.2 Approval of Third Quarterly Report on Performance
BREAK (15 minutes)
8.3.1 Approval of Annual Business Plan
8.3.2 Approval of Revised LHIN Scorecard Metrics
8.4 Overview of Service Accountability Agreements
8.5 Approval of Pre-Capital Proposal to Renovate the Mental
Health Program Space at the Queensway Carleton
8.6 Approval of Annual Attestation
8.7 Approval of Vision Care Plan - Timed item 4:00 p.m.
8.8 Update on Patients First Proposal
8.9 Update: Health System Funding Reform
Yes
Yes
Yes
Yes
Yes
Yes
No
Yes
No
Yes
D
D
D
D
I
D
D
D
I
I
1,2,3
9
17:15-17:35
Board Committee Stewardship Reports and Matters
Arising Therefrom
9.1 Community Nominations
9.2 French Language Services
9.3 Governance
9.4 CEO Performance Evaluation & Compensation
9.5 Finance & Audit
Yes
I
I
D
I
I
1,2,3
10
17:35
Other Business
10.1 Departure of Board Member
11
Round Table
12
Adjournment of Meeting
Strategic Plan References
1=Increase coordination and integration of services among hospitals
2=Build strong foundation of integrated primary and community care
3=Improve coordination and transitions of care
3
Directions: 1900 City Park Drive, Ottawa, ON.
Participants requiring accessibility supports or special accommodation
may contact [email protected] prior to the meeting.
Public documents and presentations distributed are be available on our website: Meeting Packages
1
Decision of the Champlain Local Health Integration Network issued pursuant to s.25(2)(a) of the Local Health System Integration Act,
2006 1. Date: April 27th, 2016
2. Subject Matter: Creation of the Mississippi River Health Alliance
3. Parties to the Decision:
Carleton Place & District Memorial Hospital (“CPDMH”)
CPDMH is a 22-bed fully accredited acute care facility located in Carleton Place, Ontario. It provides 24/7 Emergency Department coverage, as well as diagnostic, laboratory, rehabilitation therapy and telemedicine services. CPDMH has more than 60 clinics staffed by a wide range of medical specialists, and surgical services for both day patients and inpatients. CPDMH has entered into a hospital service accountability agreement with the Champlain LHIN and the Champlain LHIN provides CPDMH with funding for services.
Almonte General Hospital (“AGH”)
AGH is a 52-bed hospital located in Almonte, Ontario that has for generations, been providing an extensive range of services to local area residents, including 24-hour emergency services, a regional Obstetrics & Gynaecology programs well as Complex Continuing Care and Day Hospital programs serving the catchment areas of both AGH and CPDMH. AGH owns and operates Fairview Manor, a 112 bed long term care home, and operates Lanark County Paramedic Service under contract with the County of Lanark. AGH has entered into a hospital service accountability agreement with the Champlain LHIN and the Champlain LHIN provides AGH with funding for services.
4. Purpose and Nature of Integration:
The purpose of the proposed integration is to allow AGH and CPDMH to formally commit to advance collaborative efforts between the two hospitals, which includes sharing a Chief Executive Officer (“CEO”) and forming an Alliance Committee on the terms set forth in the attached Alliance Agreement entered into between AGH and CPDMH effective April 18th, 2016 (“Alliance Agreement”) (Attached as Appendix A).
2
5. Facts:
The Champlain LHIN facilitated the integration of services between AGH and CPDMH by providing advice to the hospitals as well as funding to support the analysis of options and the development of an approach to the integration of services as further described under section 6 of this decision. AGH and CPDMH have reached an agreement as set forth in the Alliance Agreement. Under s. 25 (2)(a) of the Local Health System Integration Act, 2006, the Champlain LHIN is required to issue an integration decision. The Boards of Directors of AGH and CPDMH have been discussing options to advance collaboration and coordination of services between the two hospitals for approximately two years and have now reached a written agreement about the form and nature of the partnership they wish to pursue. The Boards of Directors of CPDMH and AGH have kept their local communities informed about the fact that they were holding these discussions. In May 2015, they announced that they were taking their history of collaboration to a new level to improve accessibility and quality and to create a more inter-connected health care system. A column in the EMC, the local newspaper, reported on the establishment of a steering committee to guide discussions and recommend opportunities to enhance patient care. Since May 2015, the hospitals have used various communications methods such as columns in the local newspaper, a presentation to the Municipality of Mississippi Mills Council, the hospitals’ annual reports and public events such as hospital foundation donor events to share successes from their collaborative efforts. These successes include a new assess and restore program for the frail elderly, an automated referral for patients transferring from CPDMH to complex continuing care at AGH, coordination of the purchase of a new digital x-ray machine at each hospital and the sharing of pharmacy equipment to improve patient safety. In July 2015, a facilitator retained by the hospitals conducted interviews with 11 stakeholders representing primary care, acute care, community health care and municipal councils. The purpose of the consultations was to assess stakeholder perception about opportunities for collaboration between the two hospitals. The results of these consultations were shared with members of the Boards of Directors of both hospitals. The consultations revealed general support for the hospitals exploring opportunities for both clinical and administrative shared services. 6. Process In March 2015, the Champlain LHIN approved a request for funding, submitted by AGH on behalf of both hospitals via a Health System Improvement Proposal. The Champlain LHIN provided funding to off-set the costs incurred by the
3
hospitals during the 2014-15 fiscal year to secure the services of a facilitator. The facilitator supported the hospitals’ Board of Directors in the identification and analysis of options to enhance service delivery between the two hospitals. In January 2016, the Champlain LHIN approved a second request for funding, submitted by AGH on behalf of both hospitals via a Health System Improvement Proposal (“Proposal”). The Proposal outlined that the pending retirement of the CEO at CPDMH provided an opportunity for the hospitals to explore the option of sharing a CEO. Champlain LHIN funding was allocated to support the hospitals in developing an integrated leadership structure and governance oversight approach. As a condition of funding, the LHIN required that the hospitals provide it with a report detailing the proposed leadership structure and governance oversight approach by April 29th, 2016. On March 7th, 2016, the two hospital CEOs met with the CEO of the Champlain LHIN to provide an update on the status of the work funded by the LHIN. The hospital CEOs indicated that the hospitals wished to form an alliance and establish a committee to serve as a forum for discussion of ongoing opportunities to improve patient services and to oversee the performance of a shared CEO to provide senior leadership to both hospitals subject to approval by the Board of Directors of both hospital corporations. On April 18th, 2016, the Boards of Directors of both hospitals approved motions to establish the Mississippi River Health Alliance as outlined in the Alliance Agreement. 7. Analysis of Intended Integration The proposed integration is the outcome of approximately 2 years of dialogue and discussion between the AGH and CPDMH CEOs and Boards of Directors. The proposed integration will benefit both hospital corporations as well as the communities they serve. By securing joint leadership for the hospitals, the hospitals will see reduced administrative costs which will allow for the financial efficiencies to be used towards other cost pressures or priorities in the hospitals. The creation of a jointly formed Alliance Committee will ensure a formal means of ongoing dialogue between the two hospital corporations to identify further opportunities for integration. The communities will benefit from greater alignment in the provision of hospital services between the two corporations, a greater ability for the two hospitals to jointly recruit and retain staff, to share expertise and resources, and to preserve and grow existing hospital services.
4
The proposed integration is well aligned with the Champlain LHIN’s vision of Healthy people and healthy communities supported by a quality, accessible health system. The proposed integration supports the LHIN’s desire to ensure access to quality health care services, to create a more integrated health system and to ensure the sustainability of health services in the region. The LHIN is satisfied that the two hospitals have kept the community informed of their discussions about opportunities to advance collaboration between the two hospitals. The decision to establish the Mississippi River Health Alliance and enter into the Alliance Agreement is not contrary to the hospital service accountability agreements entered into separately by each hospital. The LHIN also recognizes that it is the responsibility of the Board of Directors of a hospital corporation to select a CEO to lead the corporation. AGH and CPDMH have advised the Champlain LHIN that they intend the Alliance Agreement to be effective on April 18th, 2016.
8. Decision Pursuant to subsection 25 (2)(a) of the Local Health System Integration Act, 2006, the Champlain LHIN finds that AGH and CPDMH have reached and entered into a binding agreement with respect to the integration described in this integration decision, and that pursuant to this decision, AGH and CPDMH will take the following actions:
Implement the Alliance Agreement by September 1st, 2016;
Develop a human resources adjustment plan in respect of this integration by May 30th, 2016;
Seek approval from the Champlain LHIN of any proposed changes to the Alliance Agreement and/or to the agreement to share a joint CEO; and
Should the work of the Alliance Committee result in further opportunities to integrate programs and services between the two hospitals, AGH and CPDMH will do so in accordance with applicable law and policy such as but not limited to the Local Health System Integration Act, 2006 and the Public Hospitals Act.
The Champlain Local Health Integration Network Per: _______________________________ __________________ Jean-Pierre Boisclair, Chair Date

Performance Report
for Q3 2015-16:
Highlights
Prepared by Vicky Walker, Senior Performance Specialist
Event Champlain LHIN Board Meeting
Date April 20, 2016
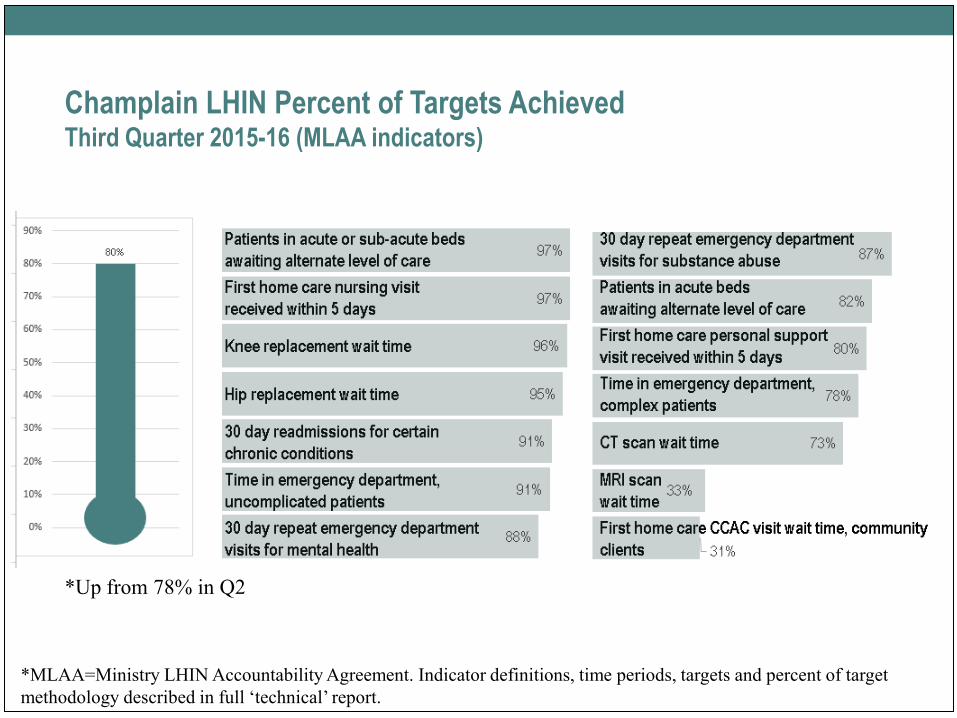
Champlain LHIN Percent of Targets Achieved Third Quarter 2015-16 (MLAA indicators)
*MLAA=Ministry LHIN Accountability Agreement. Indicator definitions, time periods, targets and percent of target
methodology described in full ‘technical’ report.
*Up from 78% in Q2
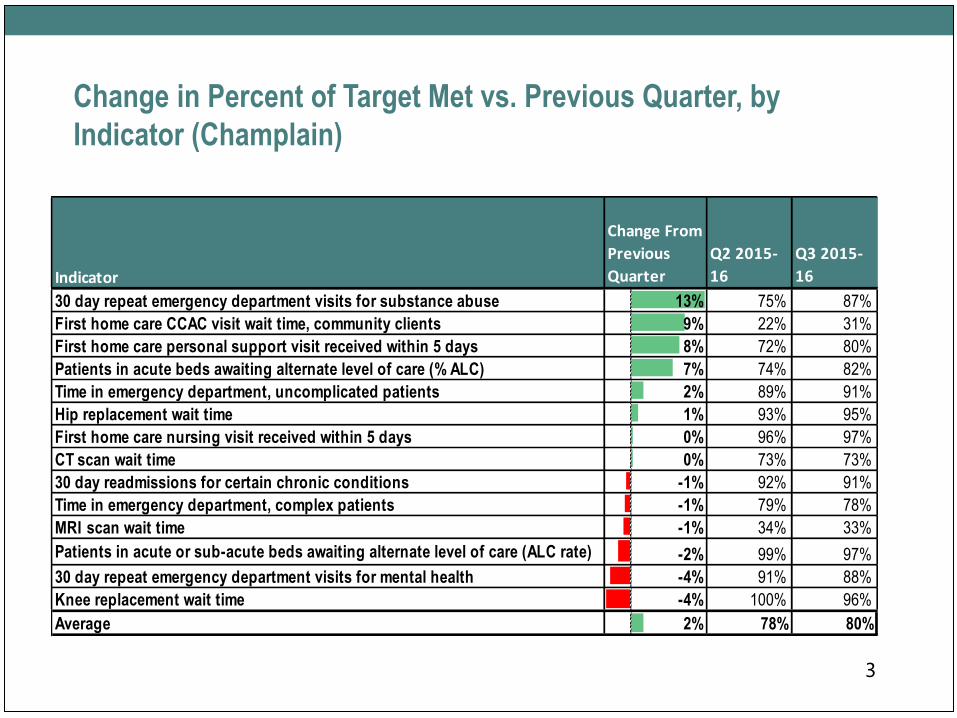
Change in Percent of Target Met vs. Previous Quarter, by
Indicator (Champlain)
3
Indicator
Change From
Previous
Quarter
Q2 2015-
16
Q3 2015-
16
30 day repeat emergency department visits for substance abuse 13% 75% 87%
First home care CCAC visit wait time, community clients 9% 22% 31%
First home care personal support visit received within 5 days 8% 72% 80%
Patients in acute beds awaiting alternate level of care (% ALC) 7% 74% 82%
Time in emergency department, uncomplicated patients 2% 89% 91%
Hip replacement wait time 1% 93% 95%
First home care nursing visit received within 5 days 0% 96% 97%
CT scan wait time 0% 73% 73%
30 day readmissions for certain chronic conditions -1% 92% 91%
Time in emergency department, complex patients -1% 79% 78%
MRI scan wait time -1% 34% 33%
Patients in acute or sub-acute beds awaiting alternate level of care (ALC rate) -2% 99% 97%
30 day repeat emergency department visits for mental health -4% 91% 88%
Knee replacement wait time -4% 100% 96%
Average 2% 78% 80%
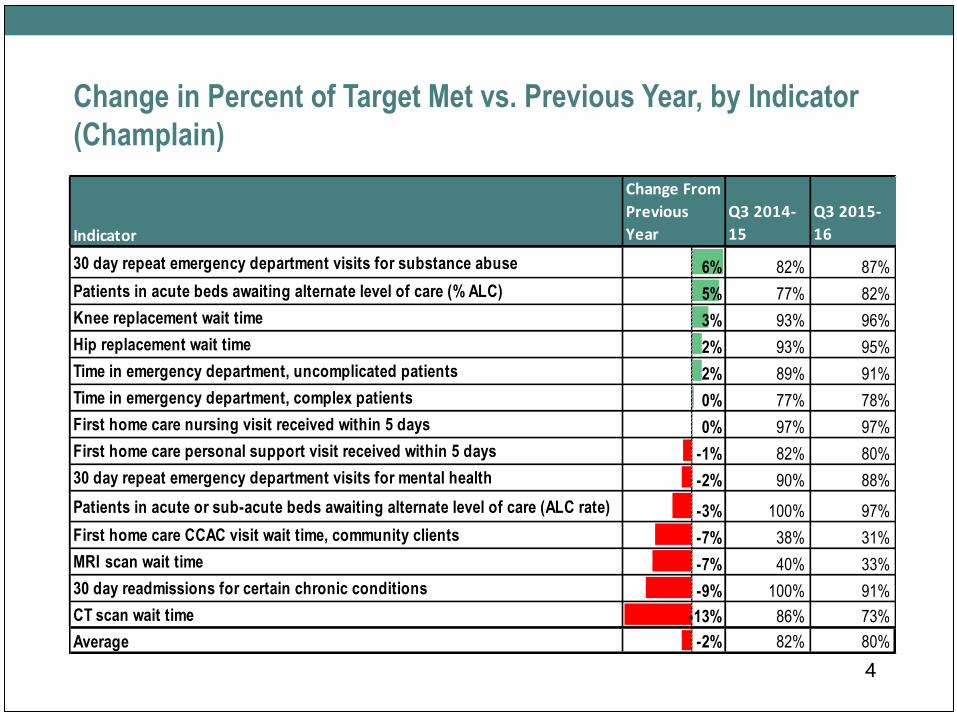
Change in Percent of Target Met vs. Previous Year, by Indicator
(Champlain)
4
Indicator
Change From
Previous
Year
Q3 2014-
15
Q3 2015-
16
30 day repeat emergency department visits for substance abuse 6% 82% 87%
Patients in acute beds awaiting alternate level of care (% ALC) 5% 77% 82%
Knee replacement wait time 3% 93% 96%
Hip replacement wait time 2% 93% 95%
Time in emergency department, uncomplicated patients 2% 89% 91%
Time in emergency department, complex patients 0% 77% 78%
First home care nursing visit received within 5 days 0% 97% 97%
First home care personal support visit received within 5 days -1% 82% 80%
30 day repeat emergency department visits for mental health -2% 90% 88%
Patients in acute or sub-acute beds awaiting alternate level of care (ALC rate) -3% 100% 97%
First home care CCAC visit wait time, community clients -7% 38% 31%
MRI scan wait time -7% 40% 33%
30 day readmissions for certain chronic conditions -9% 100% 91%
CT scan wait time -13% 86% 73%
Average -2% 82% 80%
Feature Section on LHIN Organizational Health
• Highlights include:
• Strong system partnerships and collaboration
• Very low administrative costs of LHIN relative to system
expenditures and other LHINs
• Effective internal management of resources as evidenced by
meeting objectives related to operational budget, achievement of
annual business plan objectives, and social media/
communications indicators
5
2016-17 Champlain LHIN
Annual Business PlanPresentation to the Champlain LHIN Board of Directors
April 27, 2016
James Fahey
Director, Health System Planning
What is the Annual Business Plan (ABP)?
• Outlines how the LHIN will use its various resources to achieve its
strategic directions and priorities
• Focuses on 2016/17 and projects out to 2018/19
• Follows Ministry of Health and Long Term Care (Ministry)
guidelines and pre-set format
• Highlights interventions where the LHIN is the main driver and plays
a significant role in the execution of the intervention
2
3
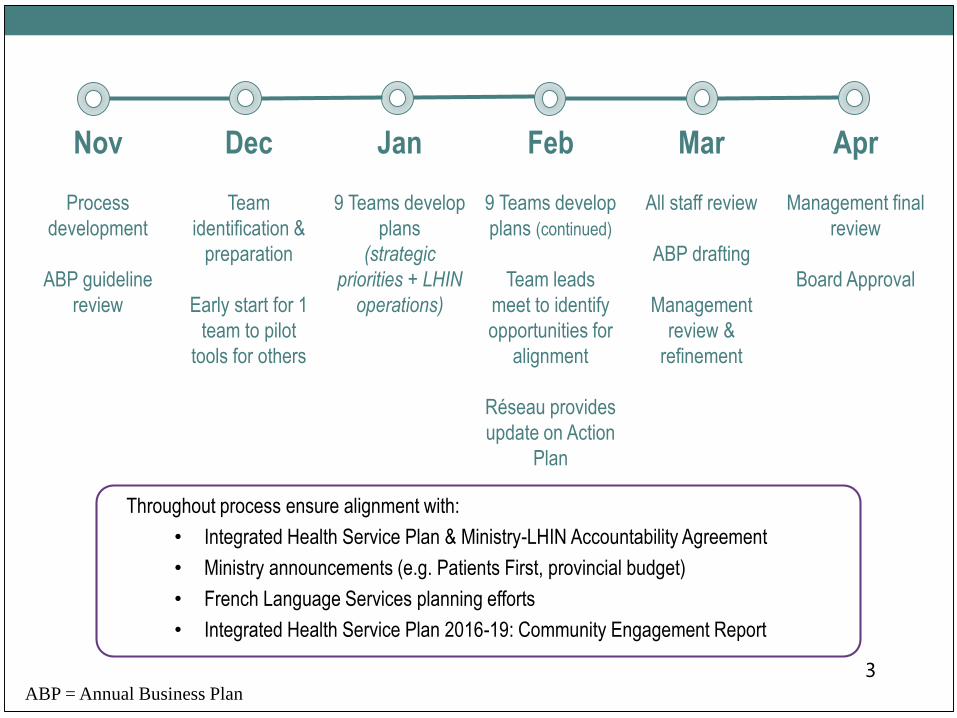
Nov Dec Jan Feb Mar Apr
Process
development
ABP guideline
review
Team
identification &
preparation
Early start for 1
team to pilot
tools for others
9 Teams develop
plans
(strategic
priorities + LHIN
operations)
9 Teams develop
plans (continued)
Team leads
meet to identify
opportunities for
alignment
Réseau provides
update on Action
Plan
All staff review
ABP drafting
Management
review &
refinement
Management final
review
Board Approval
Throughout process ensure alignment with:
• Integrated Health Service Plan & Ministry-LHIN Accountability Agreement
• Ministry announcements (e.g. Patients First, provincial budget)
• French Language Services planning efforts
• Integrated Health Service Plan 2016-19: Community Engagement Report
ABP = Annual Business Plan
4
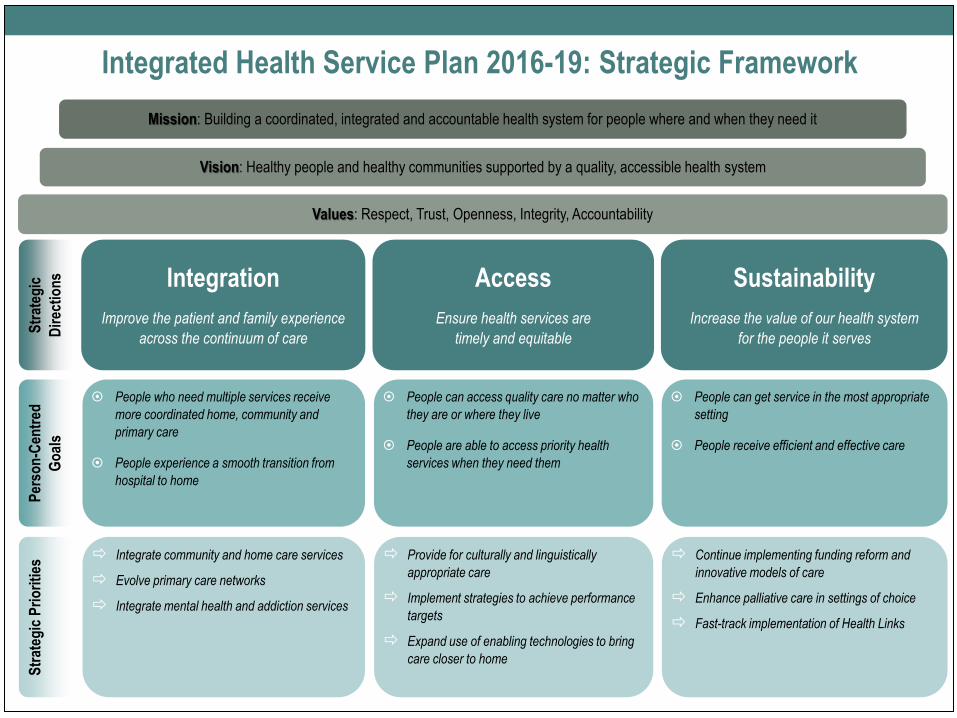
Sustainability
Increase the value of our health system
for the people it serves
Vision: Healthy people and healthy communities supported by a quality, accessible health system
Str
ateg
ic
Dir
ecti
on
s
Mission: Building a coordinated, integrated and accountable health system for people where and when they need it
Values: Respect, Trust, Openness, Integrity, Accountability
Integration
Improve the patient and family experience
across the continuum of care
Access
Ensure health services are
timely and equitable
People can get service in the most appropriate
setting
People receive efficient and effective care
Per
son
-Cen
tred
Go
als
People who need multiple services receive
more coordinated home, community and
primary care
People experience a smooth transition from
hospital to home
People can access quality care no matter who
they are or where they live
People are able to access priority health
services when they need them
Continue implementing funding reform and
innovative models of care
Enhance palliative care in settings of choice
Fast-track implementation of Health Links
Integrate community and home care services
Evolve primary care networks
Integrate mental health and addiction services
Provide for culturally and linguistically
appropriate care
Implement strategies to achieve performance
targets
Expand use of enabling technologies to bring
care closer to home
Str
ateg
ic P
rio
riti
es
Integrated Health Service Plan 2016-19: Strategic Framework
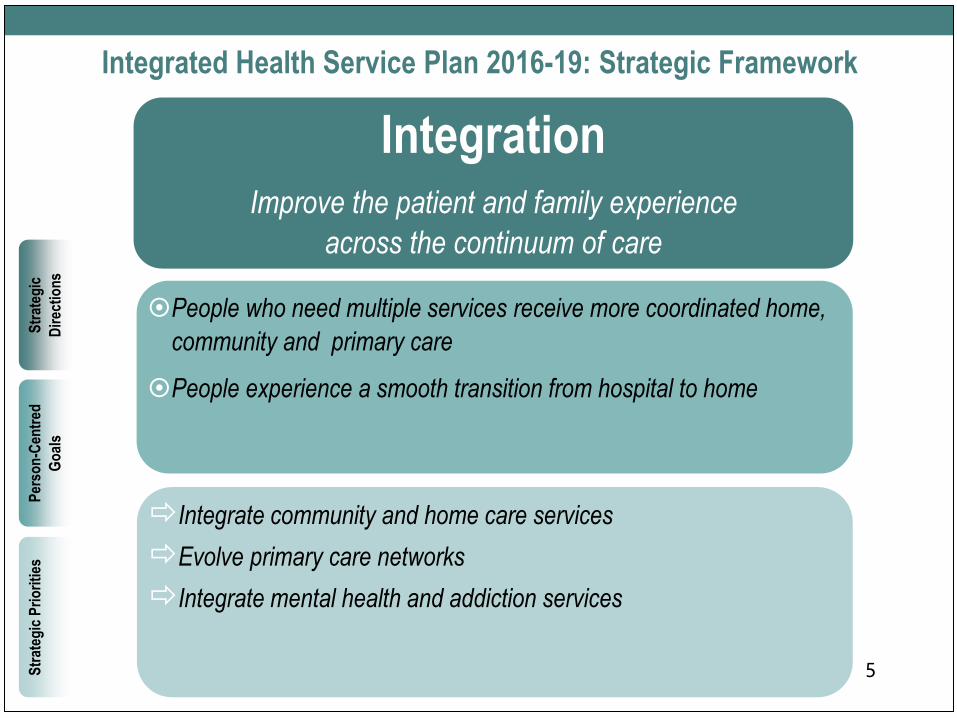
People who need multiple services receive more coordinated home,
community and primary care
People experience a smooth transition from hospital to home
Integrate community and home care services
Evolve primary care networks
Integrate mental health and addiction services
IntegrationImprove the patient and family experience
across the continuum of care
5
Str
ateg
ic
Dir
ecti
on
s
Per
son
-Cen
tred
Go
als
Str
ateg
ic P
rio
riti
es
Integrated Health Service Plan 2016-19: Strategic Framework
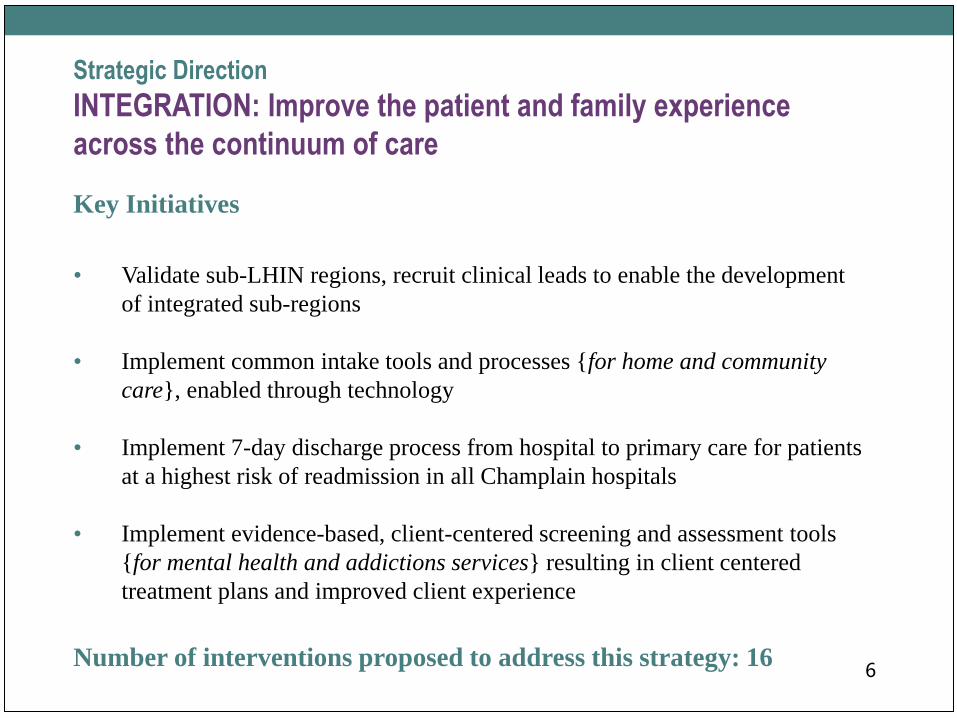
Strategic Direction
INTEGRATION: Improve the patient and family experience
across the continuum of care
Key Initiatives
• Validate sub-LHIN regions, recruit clinical leads to enable the development
of integrated sub-regions
• Implement common intake tools and processes {for home and community
care}, enabled through technology
• Implement 7-day discharge process from hospital to primary care for patients
at a highest risk of readmission in all Champlain hospitals
• Implement evidence-based, client-centered screening and assessment tools
{for mental health and addictions services} resulting in client centered
treatment plans and improved client experience
Number of interventions proposed to address this strategy: 166
AccessEnsure health services are
timely and equitable
People can access quality care no matter who they are or where they
live
People are able to access priority health services when they need
them
Provide for culturally and linguistically appropriate care
Implement strategies to achieve performance targets
Expand use of enabling technologies to bring care closer to home
7
Integrated Health Service Plan 2016-19: Strategic FrameworkS
trat
egic
Dir
ecti
on
s
Per
son
-Cen
tred
Go
als
Str
ateg
ic P
rio
riti
es
Strategic Direction
ACCESS: Ensure health services are timely and equitable
Key Initiatives:
• Address identified service gaps for Francophones within sub-regions, including
respite care, long-term care, sexual assault services and hospice palliative care
• Develop tools and resources to guide the LHIN and Health Service Providers in
the planning and delivery of culturally safe services to Indigenous people
• Increase health services for refugees, including assessing client needs at the
Ottawa Newcomer Health Centre
• Engage primary care and specialists to identify opportunities to simplify,
enhance, and integrate eConsult linked to referral flows
• Focus health service providers on achieving Ministry-LHIN accountability
performance targets through quality improvement plans, accountability
agreements and incentives
Number of interventions proposed to address this strategy: 188
9
SustainabilityIncrease the value of our health system
for the people it serves
People can get service in the most appropriate setting
People receive efficient and effective care
Continue implementing funding reform and innovative models of
care
Enhance palliative care in settings of choice
Fast-track implementation of Health Links
Str
ateg
ic
Dir
ecti
on
s
Per
son
-Cen
tred
Go
als
Str
ateg
ic P
rio
riti
esIntegrated Health Service Plan 2016-19: Strategic Framework
Strategic Direction
SUSTAINABILITY: Increase the value of our health system for
the people it serves
Key Initiatives:
• Implement the regional sub-acute care plan to achieve optimal utilization for
inpatient/outpatient rehabilitative care
• Develop a plan for a pilot health hub in a rural area including a detailed
implementation plan
• Enhance access to services through implementation of innovative palliative
and end of life care service delivery models
• Support all Health Links (10) across the region to increase the number of
people with complex care receiving coordinated care
Number of interventions proposed to address this strategy: 1010
Measures, Risks and Enablers
• Measures were selected that relate
to the interventions in the ABP
and our Strategic Priorities. Many
measures appear on the LHIN
Performance Scorecard.
11
• Risks – e.g. Financial/Economic, Project Complexity,
Technical Issues, Change Management. Mitigating
strategies for risks have been proposed.
• Enablers – e.g. collaboration with health service providers,
sub-regional planning, information/information technology,
system monitoring and performance management
LHIN Spending and Staffing Plans
LHIN Spending Plan
• Will be updated in June to reflect approved 16-17 LHIN Operating
budget and audited 2015/16 expenses
• Will include projections to 2018/19
LHIN Staffing Plan
• Provides overview of 2016-17 LHIN Staffing Plan and projections
until 2018/19
12
Communications and Community Engagement Plans
Communications Plan
• Details the measurable communications objectives for 2016/17
• Describes target audience, key messages and tactics
• Explains evaluation of communication strategy
Community Engagement Plan
• Explains the LHIN’s commitment to Community Engagement
• A more comprehensive detailing of community engagement
activities will be available in the 2016/17 Community Engagement
Plan that will be presented to the Board in June.
13

Board Motion
Be It Resolved that the Champlain LHIN
Board of Directors approves the 2016-17
Champlain LHIN Annual Business Plan
15
1900 City Park Drive, Suite 204 Ottawa, ON K1J 1A3 Tel 613.747.6784 • Fax 613.747.6519 Toll Free 1.866.902.5446 www.champlainlhin.on.ca
1900, promenade City Park, bureau 204 Ottawa, ON K1J 1A3 Téléphone : 613 747-6784 • Télécopieur : 613 747-6519 Sans frais : 1 866 902-5446 www.rlisschamplain.on.ca
Backgrounder
(Public information)
Subject Scorecard Indicators and Targets
Purpose of Discussion To consider revisions to indicators, targets and domains contained in the
Champlain LHIN scorecard and quarterly performance reports.
Background and Context Our scorecard and quarterly performance reports measure progress on
LHIN priorities, including those related to the Integrated Health Services
Plan (IHSP). With the new 2016-19 Integrated Health Services Plan
(IHSP) approved by the Board in January 2016, a process was initiated to
update the scorecard. The following approach was used:
Existing scorecard indicators were assessed in relation to the new IHSP’s strategic directions, person-centred goals and strategic priorities to identify gaps and mismatches.
Indicator options were compiled and a list of promising indicators was developed. Indicators related to LHIN operations were also included.
Internal working groups reviewed the indicators against a set of criteria, including:
o Alignment with the IHSP as well as the LHIN mandate and levers, the Ministry LHIN Accountability Agreement, Health Service Provider Accountability Agreements, the Patients First Action Plan and Health Quality Ontario indicators
o Indicator robustness (relevant, valid, easy to understand, reliable, objective, with good quality data, tested)
o Data availability, refresh frequency and timeliness o Indicator use/availability in other jurisdictions
All indicators contained in the Ministry LHIN Accountability Agreement were included by default.

2
This proposed indicator list (attachment A) was reviewed, revised and approved by the internal performance advisory group and by senior management.
To set targets for indicators, it is recommended that the approach used in
2015-16 be maintained:
Method A: Ministry LHIN Accountability Agreement (MLAA) indicators –
These targets are set provincially by the Ministry. It is expected that
progress towards meeting these targets will be demonstrated over the 3-
year term of the 2015-18 MLAA. The Champlain LHIN’s approach is to
set our targets to achieve the MLAA targets by the end of 2017/18. In
some cases, it is recommended that the LHIN aim to reach the full MLAA
target in 2016/17. In other cases, the gap between the current
performance and the MLAA target is so significant, a progressive (“2-
step”) approach is recommended. In these cases, the LHIN would plan to
achieve the MLAA target by the end of the 2017/18.
Method B: Indicators with sufficient historical data/information – If
sufficient information is available, the target is set based on the previous
year’s average as the baseline for the Champlain LHIN. If Champlain’s
performance is among the top 7 ranked LHINs, the target will be set to
the 7th best LHIN’s performance for the previous year. If performance is
among the bottom 7 LHINs, the target will be set to improve performance
to a level determined by a natural log formula.
Method C: Indicators with partial data – For indicators with partial data
available, targets have been set based on industry best practice and/or
historical evidence.
Method D: Indicators with insufficient data – For indicators where there is
no industry standard and insufficient historical evidence or where a target
may not be appropriate, no target has been proposed. Once more data
are available, a baseline and target will be set, if appropriate.

3
Attachment A identifies the proposed indicators and targets. Attachment
B compares the current (2015-16) and proposed (2016-17) indicators,
identifying the rationale for changes.
Relevant Factors The scorecard indicators are currently organized into 6 domains (shown
in Attachment B) that differ from the Strategic Directions included in the
2016-19 IHSP. Attachment A reorganizes the indicators in alignment with
the IHSP framework. Harmonizing scorecard domains with the IHSP
would help to reduce complexity in reporting and communications.
Recommendations or Options:
Beginning with the 2016-17 first quarter performance reports, it is
recommended that the LHIN Board approve:
1. Adoption of the indicators and targets in attachment A. 2. Reorganization of the indicator domains to align with the 2016-19
IHSP per attachment A
Board Resolution (if any): Be it resolved that the Champlain LHIN Board of directors approve the
indicators, targets and domains identified in attachment A for us in the
LHIN scorecard and performance reports.
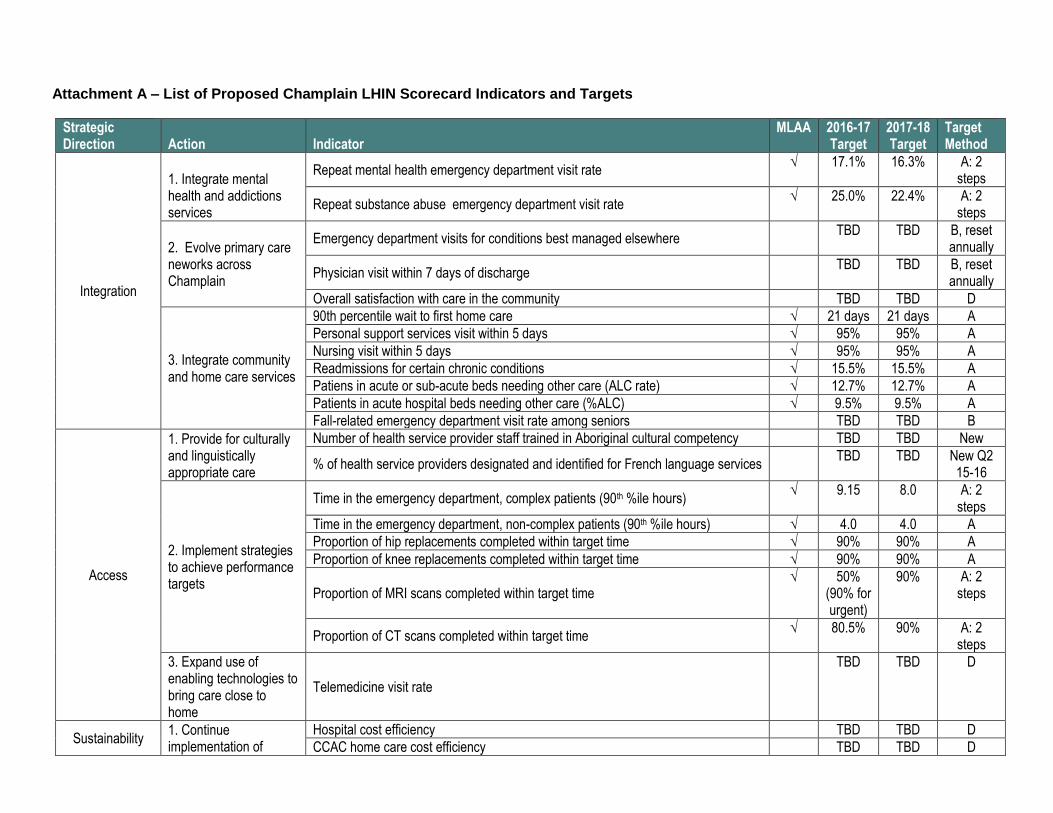
Attachment A – List of Proposed Champlain LHIN Scorecard Indicators and Targets
Strategic Direction Action Indicator
MLAA 2016-17 Target
2017-18 Target
Target Method
Integration
1. Integrate mental health and addictions services
Repeat mental health emergency department visit rate √ 17.1% 16.3% A: 2
steps
Repeat substance abuse emergency department visit rate √ 25.0% 22.4% A: 2
steps
2. Evolve primary care neworks across Champlain
Emergency department visits for conditions best managed elsewhere TBD TBD B, reset
annually
Physician visit within 7 days of discharge TBD TBD B, reset
annually
Overall satisfaction with care in the community TBD TBD D
3. Integrate community and home care services
90th percentile wait to first home care √ 21 days 21 days A
Personal support services visit within 5 days √ 95% 95% A
Nursing visit within 5 days √ 95% 95% A
Readmissions for certain chronic conditions √ 15.5% 15.5% A
Patiens in acute or sub-acute beds needing other care (ALC rate) √ 12.7% 12.7% A
Patients in acute hospital beds needing other care (%ALC) √ 9.5% 9.5% A
Fall-related emergency department visit rate among seniors TBD TBD B
Access
1. Provide for culturally and linguistically appropriate care
Number of health service provider staff trained in Aboriginal cultural competency TBD TBD New
% of health service providers designated and identified for French language services TBD TBD New Q2
15-16
2. Implement strategies to achieve performance targets
Time in the emergency department, complex patients (90th %ile hours) √ 9.15 8.0 A: 2
steps
Time in the emergency department, non-complex patients (90th %ile hours) √ 4.0 4.0 A
Proportion of hip replacements completed within target time √ 90% 90% A
Proportion of knee replacements completed within target time √ 90% 90% A
Proportion of MRI scans completed within target time √ 50%
(90% for urgent)
90% A: 2 steps
Proportion of CT scans completed within target time √ 80.5% 90% A: 2
steps
3. Expand use of enabling technologies to bring care close to home
Telemedicine visit rate
TBD TBD D
Sustainability 1. Continue implementation of
Hospital cost efficiency TBD TBD D
CCAC home care cost efficiency TBD TBD D
5
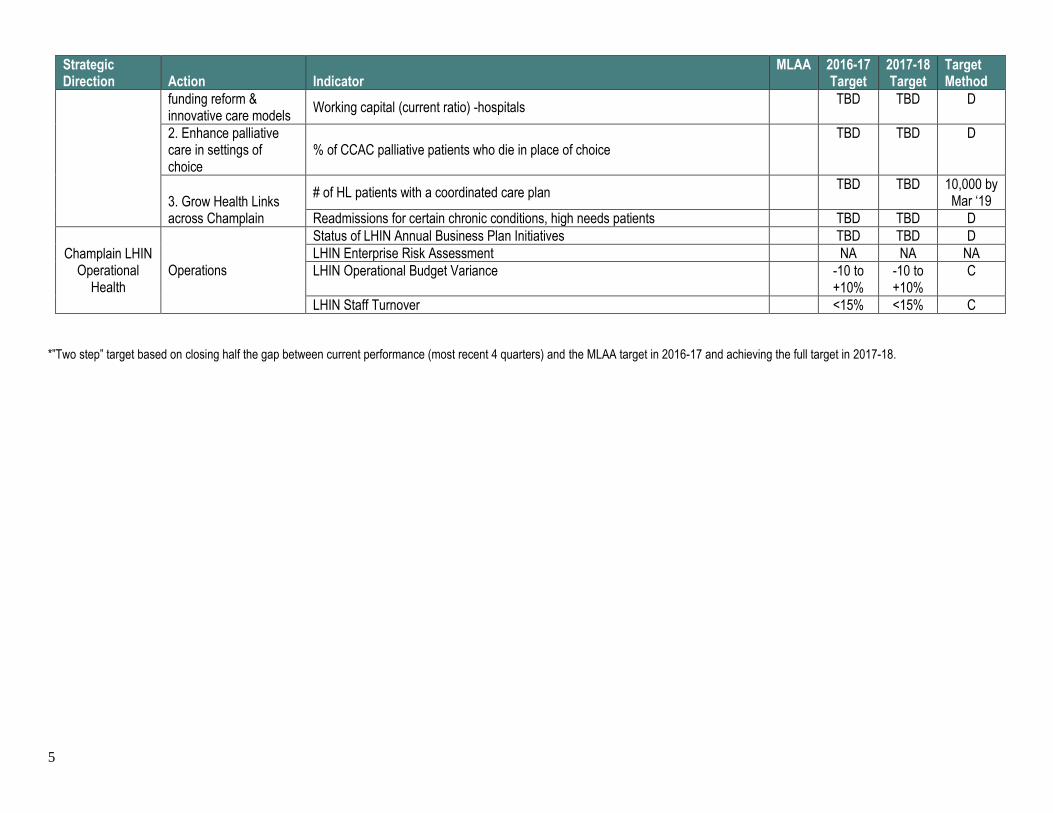
Strategic Direction Action Indicator
MLAA 2016-17 Target
2017-18 Target
Target Method
funding reform & innovative care models
Working capital (current ratio) -hospitals TBD TBD D
2. Enhance palliative care in settings of choice
% of CCAC palliative patients who die in place of choice TBD TBD D
3. Grow Health Links across Champlain
# of HL patients with a coordinated care plan TBD TBD 10,000 by
Mar ‘19
Readmissions for certain chronic conditions, high needs patients TBD TBD D
Champlain LHIN Operational
Health Operations
Status of LHIN Annual Business Plan Initiatives TBD TBD D
LHIN Enterprise Risk Assessment NA NA NA
LHIN Operational Budget Variance -10 to +10%
-10 to +10%
C
LHIN Staff Turnover <15% <15% C
*”Two step” target based on closing half the gap between current performance (most recent 4 quarters) and the MLAA target in 2016-17 and achieving the full target in 2017-18.
6
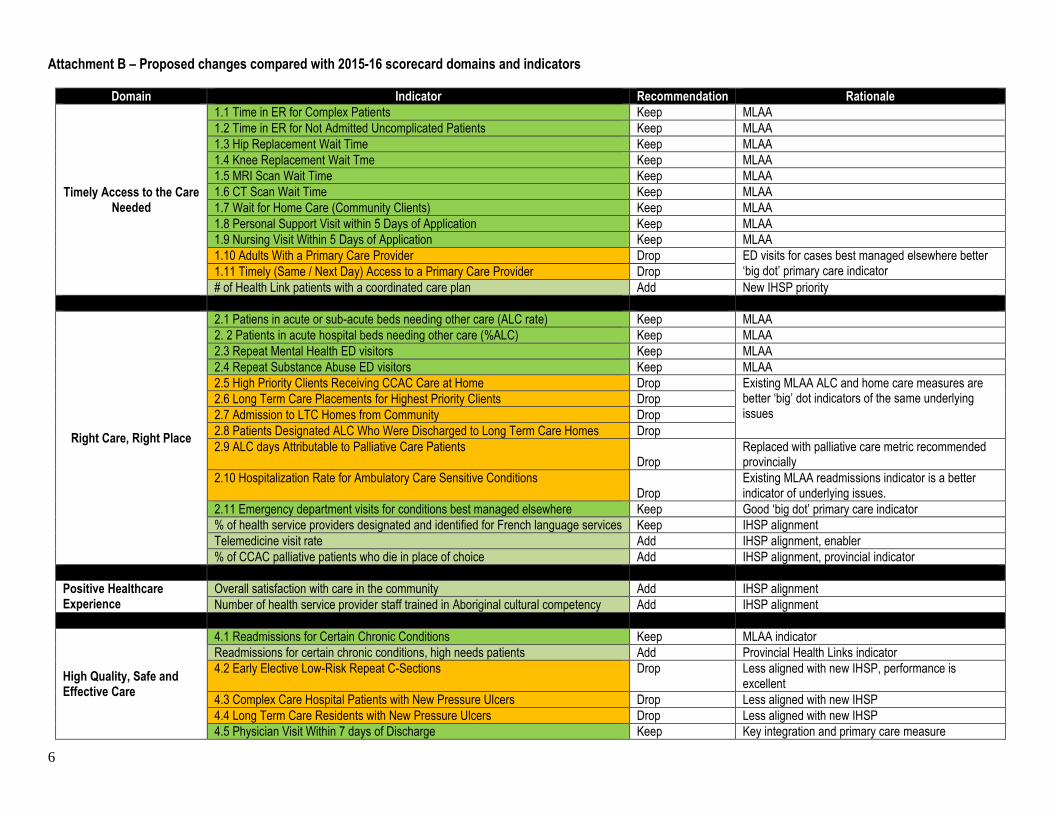
Attachment B – Proposed changes compared with 2015-16 scorecard domains and indicators
Domain Indicator Recommendation Rationale
Timely Access to the Care Needed
1.1 Time in ER for Complex Patients Keep MLAA
1.2 Time in ER for Not Admitted Uncomplicated Patients Keep MLAA
1.3 Hip Replacement Wait Time Keep MLAA
1.4 Knee Replacement Wait Tme Keep MLAA
1.5 MRI Scan Wait Time Keep MLAA
1.6 CT Scan Wait Time Keep MLAA
1.7 Wait for Home Care (Community Clients) Keep MLAA
1.8 Personal Support Visit within 5 Days of Application Keep MLAA
1.9 Nursing Visit Within 5 Days of Application Keep MLAA
1.10 Adults With a Primary Care Provider Drop ED visits for cases best managed elsewhere better ‘big dot’ primary care indicator 1.11 Timely (Same / Next Day) Access to a Primary Care Provider Drop
# of Health Link patients with a coordinated care plan Add New IHSP priority
Right Care, Right Place
2.1 Patiens in acute or sub-acute beds needing other care (ALC rate) Keep MLAA
2. 2 Patients in acute hospital beds needing other care (%ALC) Keep MLAA
2.3 Repeat Mental Health ED visitors Keep MLAA
2.4 Repeat Substance Abuse ED visitors Keep MLAA
2.5 High Priority Clients Receiving CCAC Care at Home Drop Existing MLAA ALC and home care measures are better ‘big’ dot indicators of the same underlying issues
2.6 Long Term Care Placements for Highest Priority Clients Drop
2.7 Admission to LTC Homes from Community Drop
2.8 Patients Designated ALC Who Were Discharged to Long Term Care Homes Drop
2.9 ALC days Attributable to Palliative Care Patients Drop
Replaced with palliative care metric recommended provincially
2.10 Hospitalization Rate for Ambulatory Care Sensitive Conditions Drop
Existing MLAA readmissions indicator is a better indicator of underlying issues.
2.11 Emergency department visits for conditions best managed elsewhere Keep Good ‘big dot’ primary care indicator
% of health service providers designated and identified for French language services Keep IHSP alignment
Telemedicine visit rate Add IHSP alignment, enabler
% of CCAC palliative patients who die in place of choice Add IHSP alignment, provincial indicator
Positive Healthcare Experience
Overall satisfaction with care in the community Add IHSP alignment
Number of health service provider staff trained in Aboriginal cultural competency Add IHSP alignment
High Quality, Safe and Effective Care
4.1 Readmissions for Certain Chronic Conditions Keep MLAA indicator
Readmissions for certain chronic conditions, high needs patients Add Provincial Health Links indicator
4.2 Early Elective Low-Risk Repeat C-Sections Drop Less aligned with new IHSP, performance is excellent
4.3 Complex Care Hospital Patients with New Pressure Ulcers Drop Less aligned with new IHSP
4.4 Long Term Care Residents with New Pressure Ulcers Drop Less aligned with new IHSP
4.5 Physician Visit Within 7 days of Discharge Keep Key integration and primary care measure
7
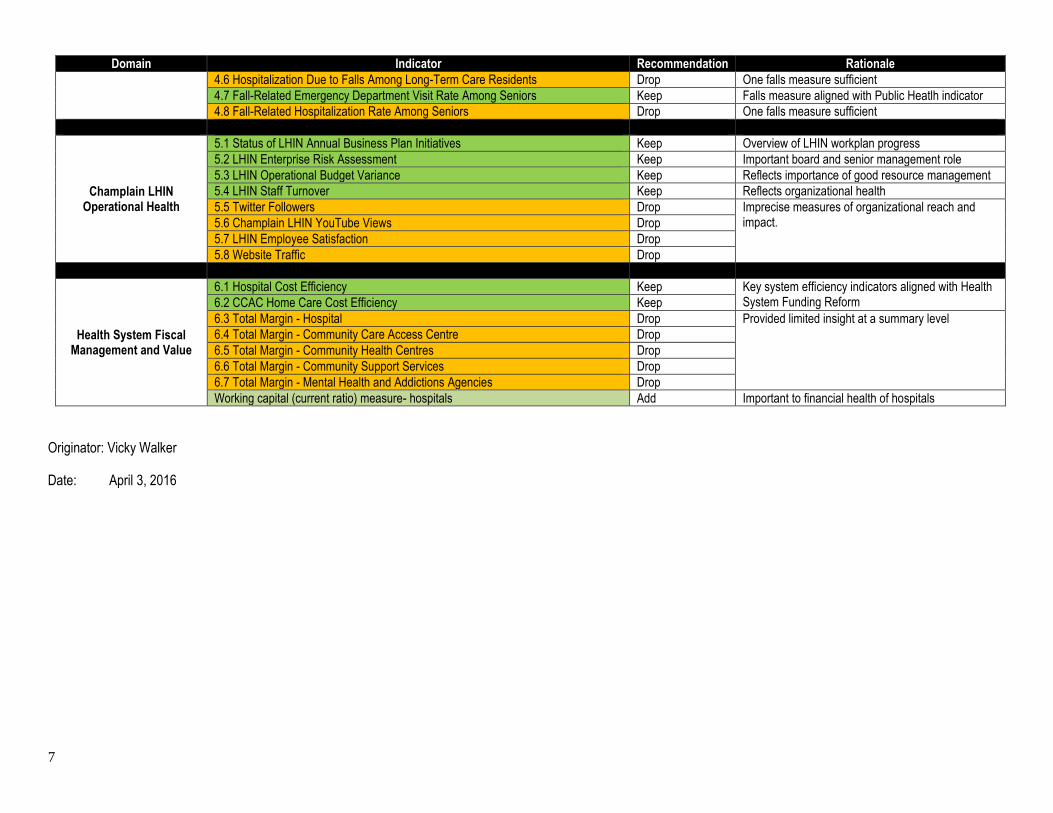
Domain Indicator Recommendation Rationale
4.6 Hospitalization Due to Falls Among Long-Term Care Residents Drop One falls measure sufficient
4.7 Fall-Related Emergency Department Visit Rate Among Seniors Keep Falls measure aligned with Public Heatlh indicator
4.8 Fall-Related Hospitalization Rate Among Seniors Drop One falls measure sufficient
Champlain LHIN Operational Health
5.1 Status of LHIN Annual Business Plan Initiatives Keep Overview of LHIN workplan progress
5.2 LHIN Enterprise Risk Assessment Keep Important board and senior management role
5.3 LHIN Operational Budget Variance Keep Reflects importance of good resource management
5.4 LHIN Staff Turnover Keep Reflects organizational health
5.5 Twitter Followers Drop Imprecise measures of organizational reach and impact. 5.6 Champlain LHIN YouTube Views Drop
5.7 LHIN Employee Satisfaction Drop
5.8 Website Traffic Drop
Health System Fiscal Management and Value
6.1 Hospital Cost Efficiency Keep Key system efficiency indicators aligned with Health System Funding Reform 6.2 CCAC Home Care Cost Efficiency Keep
6.3 Total Margin - Hospital Drop Provided limited insight at a summary level
6.4 Total Margin - Community Care Access Centre Drop
6.5 Total Margin - Community Health Centres Drop
6.6 Total Margin - Community Support Services Drop
6.7 Total Margin - Mental Health and Addictions Agencies Drop
Working capital (current ratio) measure- hospitals Add Important to financial health of hospitals
Originator: Vicky Walker
Date: April 3, 2016
8

2016-17 Health Service Provider
Service Accountability Agreements Update
• Long-Term Care Homes:
• 44 agreements for 60 Homes. 43 agreements fully executed.
• One with special wording with respect to insurance
• Community Sector:
• 96 of 97 agreements fully executed
• Two with special obligations to develop plans for 2016/17
• One with a commitment to evaluate its falls prevention
program
1
Update, continued
• Hospitals:
• 6-month amending agreements fully executed for 20 hospitals
• Three with total margin performance waivers to June 30, 2016
• For some hospitals, there are material differences between
budgeted revenue assumptions and recent funding
announcements which will require further examination and
development of mitigation strategies
• To date, no changes to clinical services have been submitted to
the LHIN
2
Queensway Carleton Hospital
Pre-Capital Submission for
Mental Health Department Redevelopment
Presented to the Champlain LHIN Board of Directors
April 27, 2016
Purpose
QCH submitted a Pre-Capital Planning Submission for the
redevelopment of the 24-bed Mental Health Department.
The purpose of this discussion is to obtain LHIN Board
endorsement of the pre-capital submission for the
proposed Mental Health Department redevelopment.
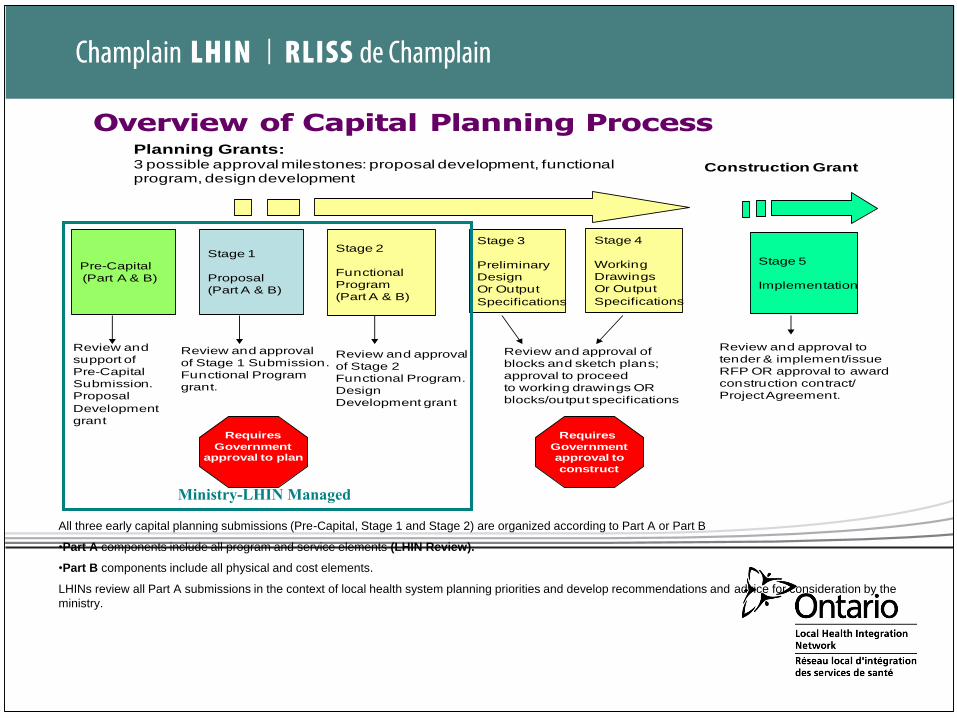
All three early capital planning submissions (Pre-Capital, Stage 1 and Stage 2) are organized according to Part A or Part B
•Part A components include all program and service elements (LHIN Review).
•Part B components include all physical and cost elements.
LHINs review all Part A submissions in the context of local health system planning priorities and develop recommendations and advice for consideration by the
ministry.
Overview of Capital Planning ProcessPlanning Grants:3 possible approval milestones: proposal development, functional program, design development
Construction Grant
Stage 1
Proposal
(Part A & B)
Stage 2
Functional
Program
(Part A & B)
Stage 3
Preliminary
Design
Or Output
Specifications
Stage 4
Working
Drawings
Or Output
Specifications
Stage 5
Implementation
Review and approval
of Stage 1 Submission.
Functional Program
grant.
Review and approval
of Stage 2
Functional Program.
Design
Development grant
Review and approval of
blocks and sketch plans;
approval to proceed
to working drawings OR
blocks/output specifications
Review and approval to
tender & implement/issue
RFP OR approval to award
construction contract/
Project Agreement.
Pre-Capital
(Part A & B)
Requires
Government approval to plan
Review and
support of
Pre-Capital
Submission.
Proposal
Development
grant
Requires
Governmentapproval to
construct
Ministry-LHIN Managed
The redevelopment will include:
• Renovating and expanding the existing 1976 era space;
• Moving the current beds (24) to the former Acute Care of the Elderly Unit;
• Addition of an Acute Day Hospital program (2,300 visits per year).
The Acute Day Hospital program will be funded from internal efficiencies
with no increase in hospital operating costs.
A potential requirement to increase the bed capacity is under review by
QCH and will be further articulated at a later stage of the process.
Total estimated cost is approximately $9.7 million.
Overview
Relevant Factors
Renewal and expansion of the QCH’s Mental Health infrastructure was
initiated in 2002 as part of a larger redevelopment project, however the mental
health renewal was deferred indefinitely when the project scope was reduced.
A 2015 Accreditation Canada Survey, a 2015 College of Physicians and
Surgeons of Ontario review and patient surveys have all identified the
requirement for physical improvements to the mental health infrastructure.
A 2015 internal review of the mental health program indicated that the
existing mental health facilities at QCH are in need of upgrading in order to
meet current or future demands for the delivery of contemporary mental
health services.
Relevant Factors
The plan will be aligned with the Champlain LHIN Integrated Health Service
Plan and regional mental health plan.
The plan is consistent with QCH’s Strategic and Master Redevelopment
Plans.
Letters of support for the initiative have been provided from health system
partners.
LHIN endorsement at the pre-capital stage indicates that there is sufficient
rationale to warrant further planning.
Proposed LHIN Board Motion
• Whereas the LHIN staff has reviewed the Queensway Carleton Hospital’s pre-
capital submission for the redevelopment of the Mental Health Department;
• Whereas the program and services elements of the pre-capital proposal are
aligned with the Champlain LHIN’s Integrated Health Services Plan and regional
mental health services;
• Whereas the Queensway Carleton Hospital will be required to ensure that its
mental health program is aligned with the plan for a regional in-patient mental
health program that will be developed over the course of 2016-17;
• Be it resolved that the Champlain LHIN Board of Directors endorses the
program and service elements outlined in the Queensway Carlton Hospital Pre-
Capital Submission for the redevelopment of its Mental Health Department.
7
1
Champlain LHIN Plan for Vision Care April 2016
2
Table of Contents
Page Number
Section A
Acknowledgements………………………………………………………………………………....4
Executive Summary…………………………………………………………………………………5
Introduction………………………………………………………………………………………….9
Champlain LHIN Vision Care Network…………………………………………………………….10
Section B
Current State Analysis for Ophthalmology Services…………………………………………....11
Overview of the Champlain LHIN……………………………………………………………………11
Demographic Analysis Highlights……………………………………………………………………12
Diabetes Prevalence…………………………………………………………………………….......15
Hub and Spoke Model……………………………………………………………………………….17
Hospitals Providing Ophthalmic Services in the Hub and Spoke Model…………………………….21
The Ottawa Hospital………………………………………………………………………22
Children’s Hospital of Eastern Ontario .…………………………………………………...24
Hôpital Montfort…………………………………………………………………………. 24
Winchester District Memorial Hospital …………………………………………………… 25
Pembroke Regional Hospital …………………………………………………………….25
Cornwall Community Hospital ……………………………………………………………25
Ophthalmology On-Call Services ……………………………………………………………….…. 26
Emergency Services ……………………………………………………….……………………… 26
Communication …………………………………………………………….……………………… 28
Strengths of the Current Hub and Spoke Model …………………………………………………… 28
Recommendation for Improvement of the Current Hub and Spoke Model………………………… 29
Overview of Community Based Vision Care Services in the Champlain LHIN…………………….. 30
Community Providers - Ophthalmologists ………………………………………………... 30
Community Providers - Optometrists……………………………………………………….30
Academic Program and Research………….………………………………………………….…… 31
Section C
Performance Measurement and Quality ………………………………………………………… 33
Ophthalmic Surgery in the Champlain LHIN ………………………………………………………. 33
Pediatric Ophthalmology…………………………………………………….……………………… 42
Performance Management and Best Practice……………………………………………………… 45
3
Cataract Procedure Workflow …………………………………………………………….…… 46
Pre-assessment process ……………………………………………………………….…… 46
Operating Room Efficiencies ……………………………………………………………….… 46
Anesthesia Model ……………………………………………………………….…….……47
Quality Indicators ……………………………………………………………….…….……… 48
Patient Satisfaction ….………………………………………………………………….……. 49
Section D
Future Planning of Surgical Services…………………………………………………………………… 50
Recommendations …………………………………………………………….……….……….……53
Section E
Stakeholder Engagement ……………………………………………………………….………… 55
Section F
Final Summary of Recommendations by Priority………………………………….……………. 61
Section G
Appendix ……………………………………………………………….……………….………….. 66
4
SECTION A
Acknowledgements
We would like to acknowledge and thank all stakeholders who have generously given their time and
expertise to ensure that we have a comprehensive Vision Plan for the Champlain Local Health Integration
Network (LHIN).
This plan was developed from valuable information and insights provided by ophthalmologists,
optometrists, health care administrators and members of the Champlain LHIN across the region. The
process has enhanced the collaborative relationships that exist in our region; with members committing to
a Regional Vision Care Network/Committee, which will continue the work to ensure access to quality
vision care services in our region.
Our Vision Plan was enhanced by the participation of our patients, community and family members.
Their valuable insights and recommendations have helped to prioritize and focus our plan.
We also extend our appreciation to Eric Partington and Vicky Walker, Champlain LHIN, who provided
valuable advice, technical support and guidance throughout the project. Rosemary Bickerton, Project
Manager, has provided exceptional leadership, research and support on this project.
We appreciate the opportunity to facilitate and support this important work.
Respectfully,
Dr. Steve Gilberg, Co-Chair Jeanette Despatie, Co-Chair
Chairman and Head, President and Chief Executive Officer
Department of Ophthalmology Cornwall Community Hospital
The Ottawa Hospital
5
Executive Summary
Champlain LHIN Vision Care Network Plan
In 2013, the Ministry of Health and Long-Term Care (MOHLTC) released “A Vision for Ontario:
Strategic Recommendations for Ophthalmology in Ontario” through the Provincial Vision Strategy Task
Force. The Champlain Local Health Integration Network (LHIN) Vision Care Network Committee arose
from recommendations to assess the current state and future needs of the delivery of eye care in our
region. In the spring of 2015, medical and administrative leads from each of the hospitals providing
ophthalmic care were brought together in a collegial and collaborative environment to acquire data,
discuss current status and needs, and look to the future for managing the growing population that we
serve.
In this document we describe the current model of delivery within our geographic region that provides
access to care for patients in their own communities while simultaneously being able to deliver complex
tertiary and quaternary care 24 hours per day, 7 days per week 365 days a year. A “hub and spoke” model
is described and demonstrates its effectiveness in meeting these goals.
Eye care is provided in the Champlain LHIN by ophthalmologists and optometrists in a collegial and
collaborative environment. Clinical care is provided both in private offices of eye care providers and
within hospitals such as The Ottawa Hospital, the academic center for ophthalmology in the region.
Hospitals providing ophthalmic care are well distributed geographically within the region and act as hubs
for those hospitals that do not provide eye care. The vast majority of ophthalmic surgery is performed in
hospital settings with significant support from the local populations and hospital administrations.
The Champlain LHIN has a population of over 1.3 million people and a slightly older demographic than
the rest of Ontario. It is unique in that it has a significant Francophone population and its northeastern
border is adjacent to the province of Quebec. Services are widely available in both official languages. A
significant number of Quebec patients seek care within our LHIN for all levels of ophthalmic care and
this cross provincial care adds additional complexity to calculating needs and assessing metrics such as
wait times for Ontario patients.
Several recommendations to address current challenges are found throughout the document and
summarized collectively in the last section and are also listed in order of priority in the chart at the end of
this Executive Summary. The Champlain LHIN has been recognized for many years as having long
surgical Wait 2 for pediatric strabismus surgery and Wait 1 for pediatric consultation and addressing these
two challenges has been identified universally as an immediate need by the committee. Despite several
measures to increase access by implementing even greater efficiencies, the recommendation to increase
pediatric ophthalmic surgical resources at the Children’s Hospital of Eastern Ontario in conjunction with
a much needed renovation of the ophthalmology clinic is essential. Both elements are essential in
addressing these challenges that have repercussions throughout the LHIN for providers of pediatric eye
care.
Members of the Champlain LHIN have worked collaboratively over the past 3 years to manage Wait 2
targets for cataract surgery. In 2011-12 additional Wait Time Strategy funding was given to reduce the
wait times to fund additional cataracts (approximately 1500 cases or 15%) which effectively managed
6
Wait 2. When the funding process changed to Quality Based Procedures (QBP), and the one time Wait
Time funding was removed, Wait Times have steadily risen above the 182 day target. It has become
evident to members of the committee that after re-analysis of LHIN data, an increase of 15% to the base
volume would bring us to an equilibrium that is sustainable with increases going forward based on
demographic data.
A recommendation that has provincial and national implications regards implementation of a fully
integrated functional electronic medical record (EMR) necessary to bring health care in Ontario into the
21st century. To evaluate quality and value metrics, data must be easily accessible for analysis with inputs
not only from hospitals but from community providers such as office based ophthalmologists and
optometrists. An effective EMR would provide a framework for colleagues in other medical disciplines
such as family medicine, endocrinology and diabetic services to monitor their patients. Several metrics
for quality are discussed throughout the document that can only be analyzed with an EMR and a
tremendous opportunity for “big data” analysis to drive policy is currently not available. A concerted
effort by the province to establish an effective and fully functional EMR is critical if we wish to meet
these expectations in health care delivery.
We wish to acknowledge the active engagement and interest expressed by all members of the Champlain
Vision Care Network Committee and the contributions made by stakeholders in the creation of this
document. The direction of the Champlain LHIN support team was appreciated and of tremendous value
in providing data and a framework for discussion. The formulation of this Plan was enhanced and
informed by the active participation of numerous stakeholders including much appreciated input from
patients and their families.
In conclusion, we feel we have accurately depicted the current status, immediate and future needs for the
provision of ophthalmic services in the Champlain LHIN. The Champlain LHIN historically has been
very effective in delivering most aspects of eye care services to the right patient, in the right place at the
right time however it was felt that the formal assembly of this committee further strengthened
relationships and provided a venue to continue to improve the patient experience. The current
membership of the committee has enthusiastically welcomed the opportunity to reconvene after formal
review of the document is completed to provide direction in advancing the quality of vision care services
in the Champlain LHIN.
Accountability of Priorities
The Champlain Vision Care Network Committee was tasked to describe the current and future state of
vision care services delivery in the Champlain LHIN and this document reflects the dedicated work of its
constituent members. We were able to identify shortfalls that currently exist within the service delivery
model and demographically derived shifts that will impact volume and quality of services in the future.
Some recommendations to improve quality can be driven by institutions across the region without great
operational or financial impact. The fiscal realities of health care provision in the province of Ontario
have led to increased efficiencies within Champlain LHIN. Despite these efforts there remain
shortcomings, many of which listed as recommendations that require additional funding for
implementation. Shifting of funds that currently exist within the Champlain LHIN either within
ophthalmology or external to ophthalmology would adversely affect the area from which the funds were
derived assuming internal efficiencies have already taken place. The committee members did not have
7
access or the expertise to redistribute funds that could potentially impact the delivery/quality of services
in those areas from which those funds would be derived. The derivation of this additional funding lies
beyond the scope of this committee but funding to support the demographically calculated volumes is an
essential component of fairly and transparently allocating funding. Discussions of where this funding
would arise requires continuing collaboration of the Ministry of Health and Long-Term Care and
representatives from provincial ophthalmology and in some recommendations, provincial optometric
bodies. There are also recommendations such as low vision care that require an even broader discussion at
the national level that is beyond the scope of this committee.
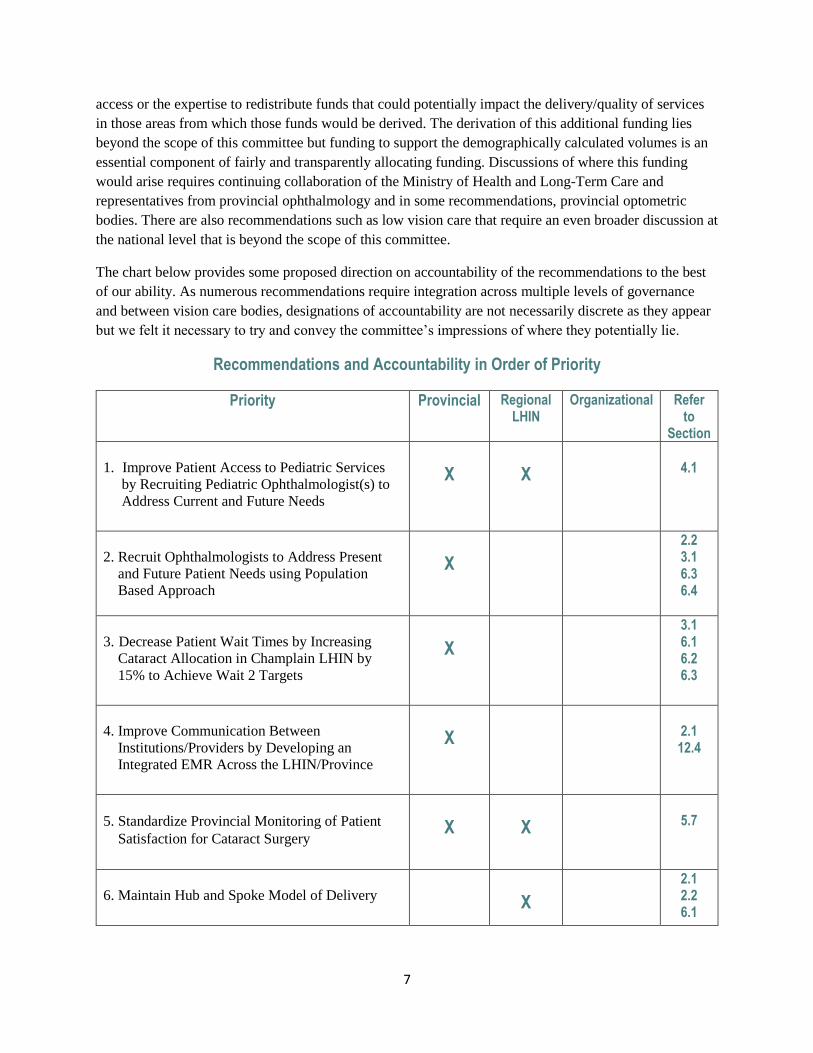
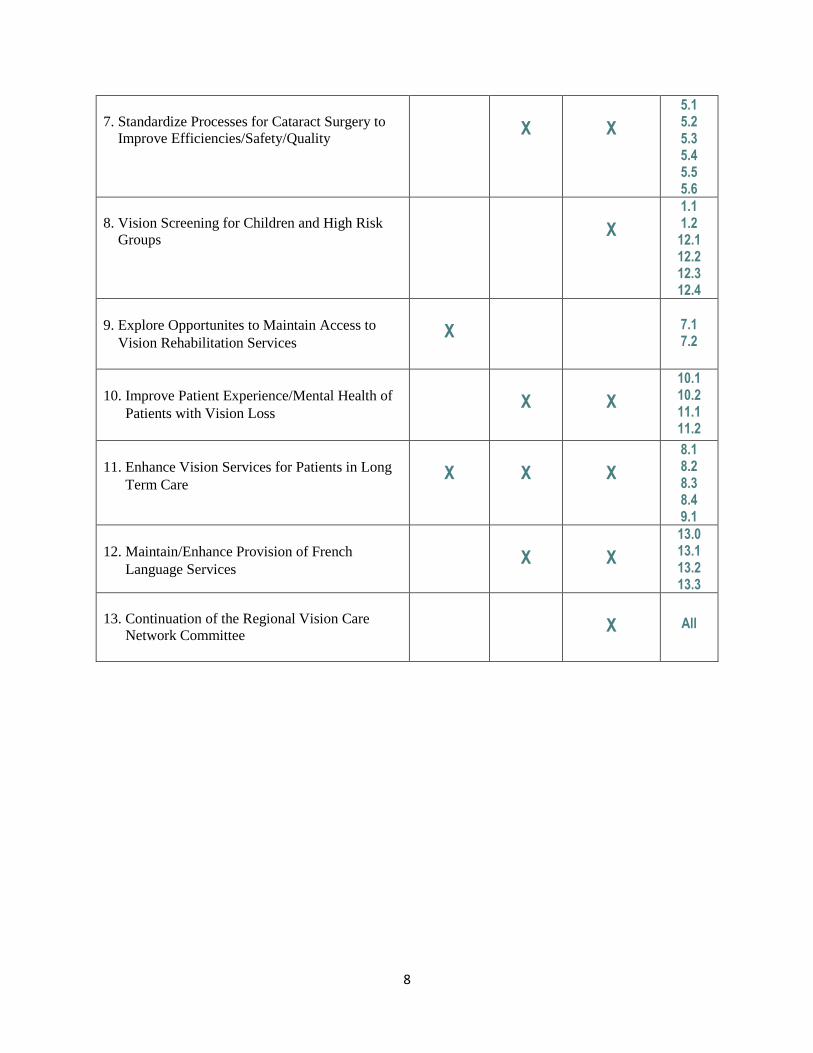
The chart below provides some proposed direction on accountability of the recommendations to the best
of our ability. As numerous recommendations require integration across multiple levels of governance
and between vision care bodies, designations of accountability are not necessarily discrete as they appear
but we felt it necessary to try and convey the committee’s impressions of where they potentially lie.
Recommendations and Accountability in Order of Priority
Priority Provincial Regional LHIN
Organizational Refer to
Section
1. Improve Patient Access to Pediatric Services
by Recruiting Pediatric Ophthalmologist(s) to
Address Current and Future Needs
X
X
4.1
2. Recruit Ophthalmologists to Address Present
and Future Patient Needs using Population
Based Approach
X
2.2 3.1 6.3 6.4
3. Decrease Patient Wait Times by Increasing
Cataract Allocation in Champlain LHIN by
15% to Achieve Wait 2 Targets
X
3.1 6.1 6.2 6.3
4. Improve Communication Between
Institutions/Providers by Developing an
Integrated EMR Across the LHIN/Province
X
2.1 12.4
5. Standardize Provincial Monitoring of Patient
Satisfaction for Cataract Surgery
X
X
5.7
6. Maintain Hub and Spoke Model of Delivery
X
2.1 2.2 6.1
8
7. Standardize Processes for Cataract Surgery to
Improve Efficiencies/Safety/Quality
X
X
5.1 5.2 5.3 5.4 5.5 5.6
8. Vision Screening for Children and High Risk
Groups
X
1.1 1.2 12.1 12.2 12.3 12.4
9. Explore Opportunites to Maintain Access to
Vision Rehabilitation Services
X
7.1 7.2
10. Improve Patient Experience/Mental Health of
Patients with Vision Loss
X
X
10.1 10.2 11.1 11.2
11. Enhance Vision Services for Patients in Long
Term Care
X
X
X
8.1 8.2 8.3 8.4 9.1
12. Maintain/Enhance Provision of French
Language Services
X
X
13.0 13.1 13.2 13.3
13. Continuation of the Regional Vision Care
Network Committee
X
All

9
Introduction
The Ministry of Health and Long-Term Care released A Vision for Ontario: Strategic Recommendations
for Ophthalmology in Ontario in 2013. This report recommended that Local Health Integration Networks
(LHIN) should develop vision plans describing how they will provide for the vision care needs of their
communities.1
The Provincial Vision Strategy Task Force conducted a comprehensive review of ophthalmology services
in Ontario identifying system issues and developing an evidence-based planning framework to enhance
patient-centered vision care. The Task Force developed strategies to “improve access to emergency and
scheduled surgical, medical and diagnostic ophthalmology services for all Ontarians, optimize quality,
cost efficiency and patient outcomes more specifically for ophthalmology surgery and identify
performance indicators for measuring local and provincial improvement in ophthalmology services”.2
In April 2015, the Champlain LHIN embarked on a review of the current state of vision care across the
region and developed recommendations to provide for current and future eye care needs of the people in
the Champlain LHIN. The review included an examination of current services, needs and issues as well
as projections for future needs.
1 The Provincial Vision Strategy Task Force. A Vision for Ontario Strategic Recommendations for
ophthalmology in Ontario. 2013 Ministry of Health and Long Term Care.
2 A Vision for Ontario Strategic Recommendations for ophthalmology in Ontario. P.13.
10
Champlain LHIN Vision Care Network
The Champlain LHIN Vision Care Network Committee was established to develop the local Champlain
LHIN Vision Plan based on the Provincial Vision Strategy Task Force Report and its findings. The Vision
Plan is to address current and future provision of pediatric and adult vision care services. Representatives
from across the LHIN included physician and administrative representation from all hospitals providing
vision care services including pediatric and adult services, local administrative representation from the
Provincial Vision Task force, senior administrators from The Ottawa Hospital (TOH), local
ophthalmologists and optometrists. LHIN members included the Senior Director of Health System
Performance and the Senior Performance Specialist. The Network Committee was co-chaired by the CEO
of Cornwall Community Hospital and the Chief of Ophthalmology, TOH.
See Appendix 1.0 for list Champlain Vision Care Network Committee Members
See Appendix 1.1 for Terms of Reference
To support the development of a regional plan for vision care services, the Champlain LHIN Vision Care
Network collected and analyzed data on the current state and anticipated future need of services. Other
data not available through existing data sources was obtained through the use of two on-line surveys. All
hospitals providing vision care services were surveyed including the Children’s Hospital of Eastern
Ontario (CHEO). The second survey included all private practice ophthalmologists and facilities
delivering vision care in the region. The results of these surveys are contained in the following sections of
the Champlain LHIN Vision Plan report. (See Appendix 2.0 and 2.1 for Survey Results)
Hospitals surveyed:
Cornwall Community Hospital (CCH)
Hôpital Montfort (HM)
Pembroke Regional Hospital (PRH)
Children’s Hospital of Eastern Ontario (CHEO)
The Ottawa Hospital (TOH)
Winchester District Memorial Hospital (WDMH)
See Appendix 1.2 for list of Private Practice/Facilities surveyed
In developing the LHIN Vision Plan, the Network engaged key stakeholders from the community.
Representatives from the Canadian National Institute of the Blind (CNIB), a patient from the blind
community, a family representative from pediatric services, a physician lead for Long Term Care, a
diabetes Advanced Practice Nurse, an Integration Specialist of diabetes for the Champlain LHIN, an
optometric representative, and hospital administrators attended a stakeholders meeting of the Vision
Network. Stakeholders provided their perspective on vision care services in our community. The Network
also requested Le Réseau (French Language Health Services Network of Eastern Ontario) to review our
draft document to ensure that French language services exist for patients seeking vision care services in
the Champlain LHIN.
See Appendix 1.3 for list of Stakeholders
11
Section B
CURRENT STATE ANALYSIS OF OPHTHALMOLOGY SERVICES
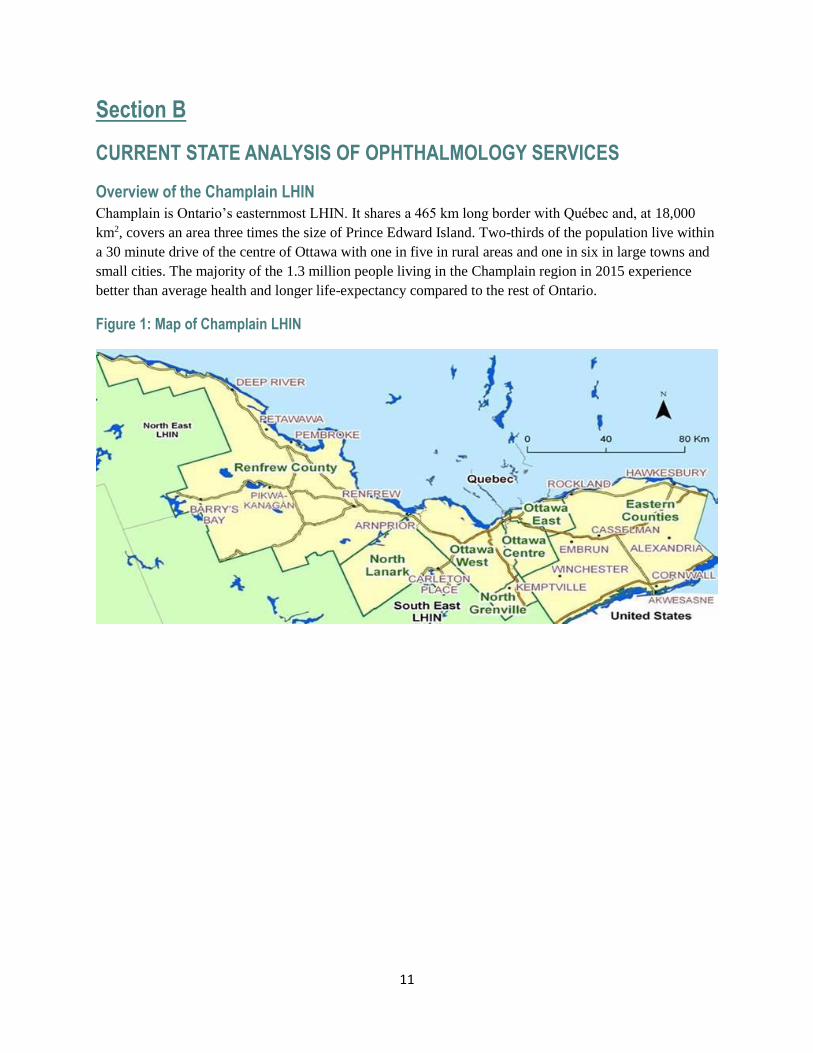
Overview of the Champlain LHIN
Champlain is Ontario’s easternmost LHIN. It shares a 465 km long border with Québec and, at 18,000
km2, covers an area three times the size of Prince Edward Island. Two-thirds of the population live within
a 30 minute drive of the centre of Ottawa with one in five in rural areas and one in six in large towns and
small cities. The majority of the 1.3 million people living in the Champlain region in 2015 experience
better than average health and longer life-expectancy compared to the rest of Ontario.
Figure 1: Map of Champlain LHIN
12
Demographic Analysis Highlights
• Champlain’s total population (2015): 1.3 million people - Approximately 10% of Ontario’s
population
• 65% live in the large urban centre of Ottawa; 20 % live in rural areas
• 19% of the population are Francophone
• Champlain is the Ontario LHIN with the most Francophone residents, i.e., 228,055
• 3.5% are Aboriginal, of which 22% live on reserves. Regions include two large reserves: 1)
Akwesasne (near Cornwall) and 2) Pikwàkanagàn (in Renfrew County)
• Canada’s largest urban Inuit population reside in Ottawa
• 18% of the population are visible minorities (24% Black, 17% South Asian, 17% Chinese) verses
Ontario of which 26% are visible minorities
• 19% of the population are immigrants versus Ontario of which 29% are immigrants
• Most common places of birth are United Kingdom, China, and African countries
• 22% of the population use a language other than English or French
15% speak Arabic, 13% Spanish, and 12% a Chinese language
• 16% of LHIN are seniors (aged 65+) versus 13.7% in Ontario
• Diabetes prevalence increases by approximately 5,000 people per year in Champlain, this would
translate to 128,461 Champlain residents 18+ with diabetes in 2017
By 2025, Champlain’s population is projected to grow from 1.3 to 1.5 million people (increase of 12%;
slightly higher than Ontario 11%)
• Proportion of seniors (65+) will increase from 15.9% to 20.7% (figure 2)
13
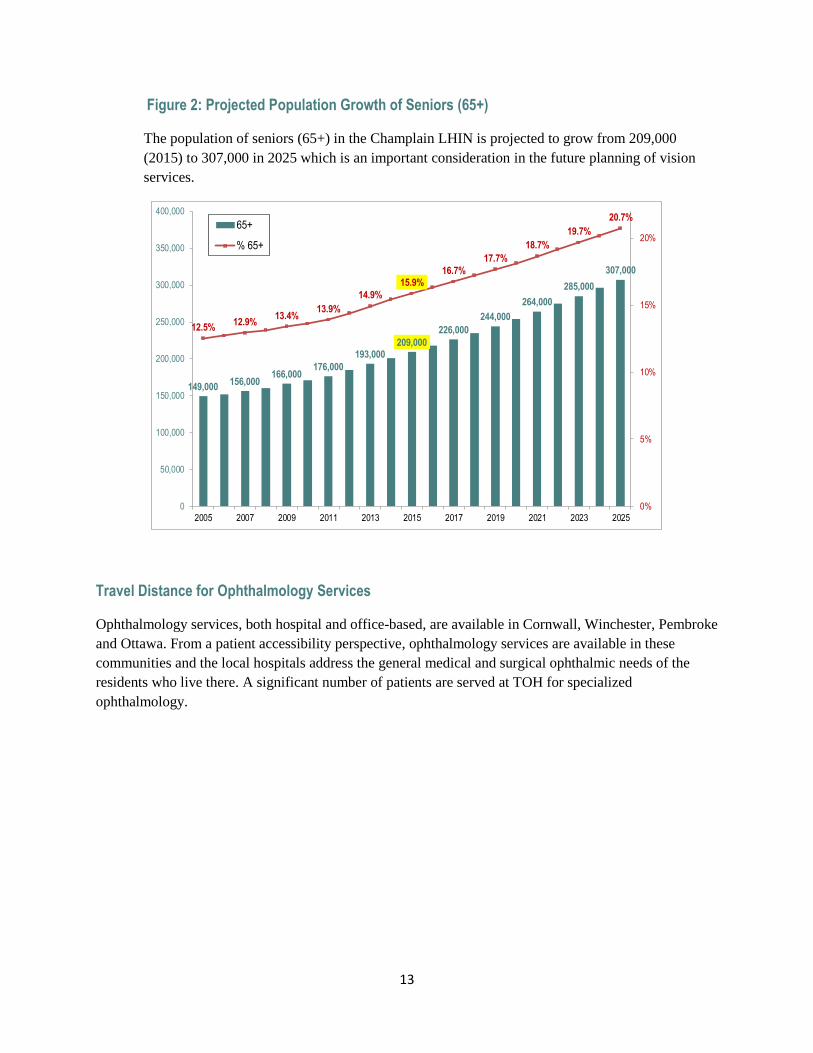
Figure 2: Projected Population Growth of Seniors (65+)
The population of seniors (65+) in the Champlain LHIN is projected to grow from 209,000
(2015) to 307,000 in 2025 which is an important consideration in the future planning of vision
services.
Travel Distance for Ophthalmology Services
Ophthalmology services, both hospital and office-based, are available in Cornwall, Winchester, Pembroke
and Ottawa. From a patient accessibility perspective, ophthalmology services are available in these
communities and the local hospitals address the general medical and surgical ophthalmic needs of the
residents who live there. A significant number of patients are served at TOH for specialized
ophthalmology.
149,000156,000
166,000176,000
193,000209,000
226,000
244,000
264,000
285,000
307,000
12.5%12.9%
13.4%13.9%
14.9%
15.9%16.7%
17.7%
18.7%
19.7%
20.7%
0%
5%
10%
15%
20%
0
50,000
100,000
150,000
200,000
250,000
300,000
350,000
400,000
2005 2007 2009 2011 2013 2015 2017 2019 2021 2023 2025
65+
% 65+

14
Figure 3: Distance Travelled for Cataract Surgery, Champlain LHIN, 2012-13
There is a small percent (6%) of patients that have to travel more than 75 kilometers to obtain cataract
surgery (figure 3). Generally patients are well served by the distribution of services within the Champlain
LHIN and there is no anticipated need for additional surgical sites in other communities.
There are three hospitals in the region where a significant portion of their patients are coming from
outside of their immediate area (figure 4). These hospitals are Pembroke, Winchester and Montfort. There
may be opportunities to treat some of the patients at Pembroke and Winchester closer to home. While the
Hôpital Montfort also sees a significant portion of patients that have another Ottawa hospital as their
closest hospital, this is of less concern because patients are still staying within the Ottawa area and may
be choosing Montfort because it is a Francophone hospital. Patients have not expressed a desire to have
ophthalmic services delivered closer to home and understand the need to attend centres of excellence for
specialized care.
52%
19%
8%
14%
6%
15km or less 16-30 km 31-45 km 46-75 km 76 km or more
15
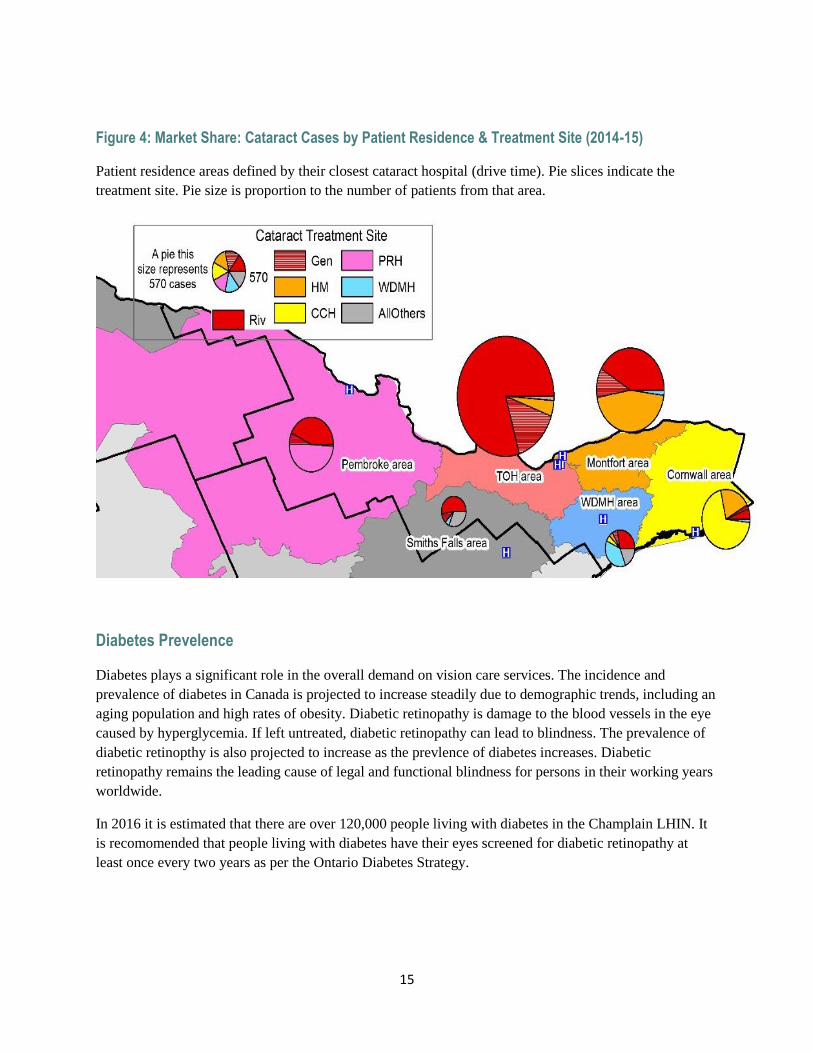
Figure 4: Market Share: Cataract Cases by Patient Residence & Treatment Site (2014-15)
Patient residence areas defined by their closest cataract hospital (drive time). Pie slices indicate the
treatment site. Pie size is proportion to the number of patients from that area.
Diabetes Prevelence
Diabetes plays a significant role in the overall demand on vision care services. The incidence and
prevalence of diabetes in Canada is projected to increase steadily due to demographic trends, including an
aging population and high rates of obesity. Diabetic retinopathy is damage to the blood vessels in the eye
caused by hyperglycemia. If left untreated, diabetic retinopathy can lead to blindness. The prevalence of
diabetic retinopthy is also projected to increase as the prevlence of diabetes increases. Diabetic
retinopathy remains the leading cause of legal and functional blindness for persons in their working years
worldwide.
In 2016 it is estimated that there are over 120,000 people living with diabetes in the Champlain LHIN. It
is recomomended that people living with diabetes have their eyes screened for diabetic retinopathy at
least once every two years as per the Ontario Diabetes Strategy.
16
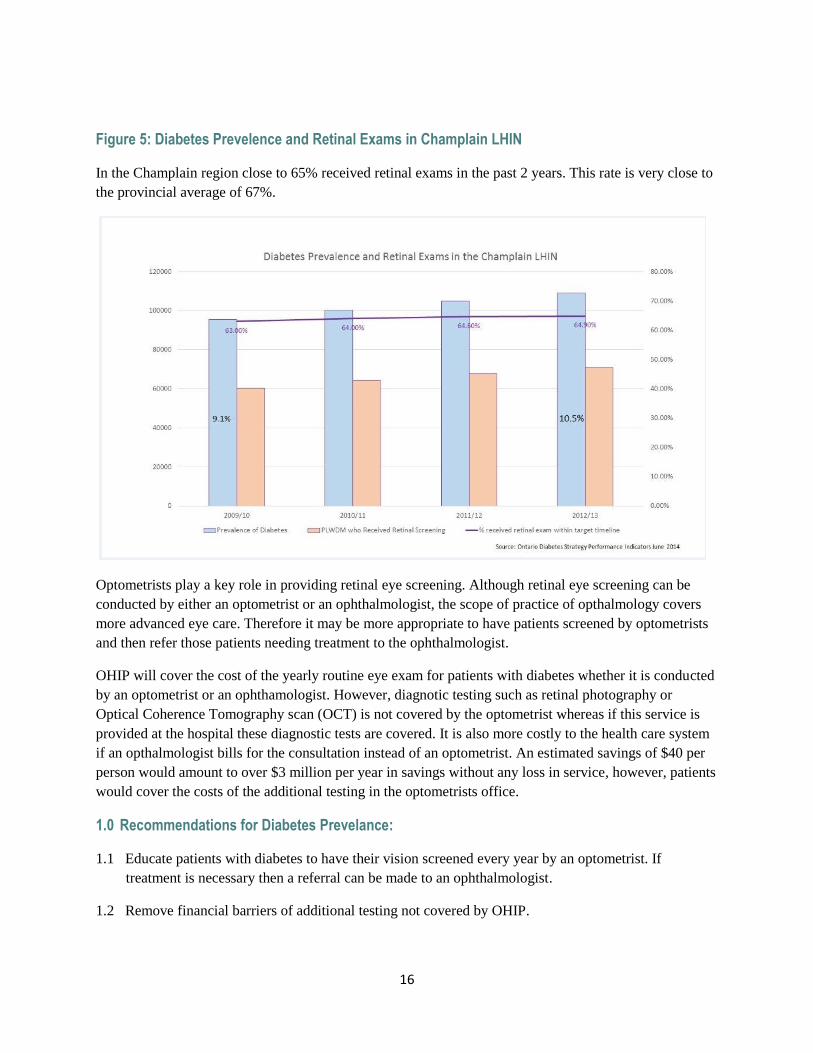
Figure 5: Diabetes Prevelence and Retinal Exams in Champlain LHIN
In the Champlain region close to 65% received retinal exams in the past 2 years. This rate is very close to
the provincial average of 67%.
Optometrists play a key role in providing retinal eye screening. Although retinal eye screening can be
conducted by either an optometrist or an ophthalmologist, the scope of practice of opthalmology covers
more advanced eye care. Therefore it may be more appropriate to have patients screened by optometrists
and then refer those patients needing treatment to the ophthalmologist.
OHIP will cover the cost of the yearly routine eye exam for patients with diabetes whether it is conducted
by an optometrist or an ophthamologist. However, diagnotic testing such as retinal photography or
Optical Coherence Tomography scan (OCT) is not covered by the optometrist whereas if this service is
provided at the hospital these diagnostic tests are covered. It is also more costly to the health care system
if an opthalmologist bills for the consultation instead of an optometrist. An estimated savings of $40 per
person would amount to over $3 million per year in savings without any loss in service, however, patients
would cover the costs of the additional testing in the optometrists office.
1.0 Recommendations for Diabetes Prevelance:
1.1 Educate patients with diabetes to have their vision screened every year by an optometrist. If
treatment is necessary then a referral can be made to an ophthalmologist.
1.2 Remove financial barriers of additional testing not covered by OHIP.
17
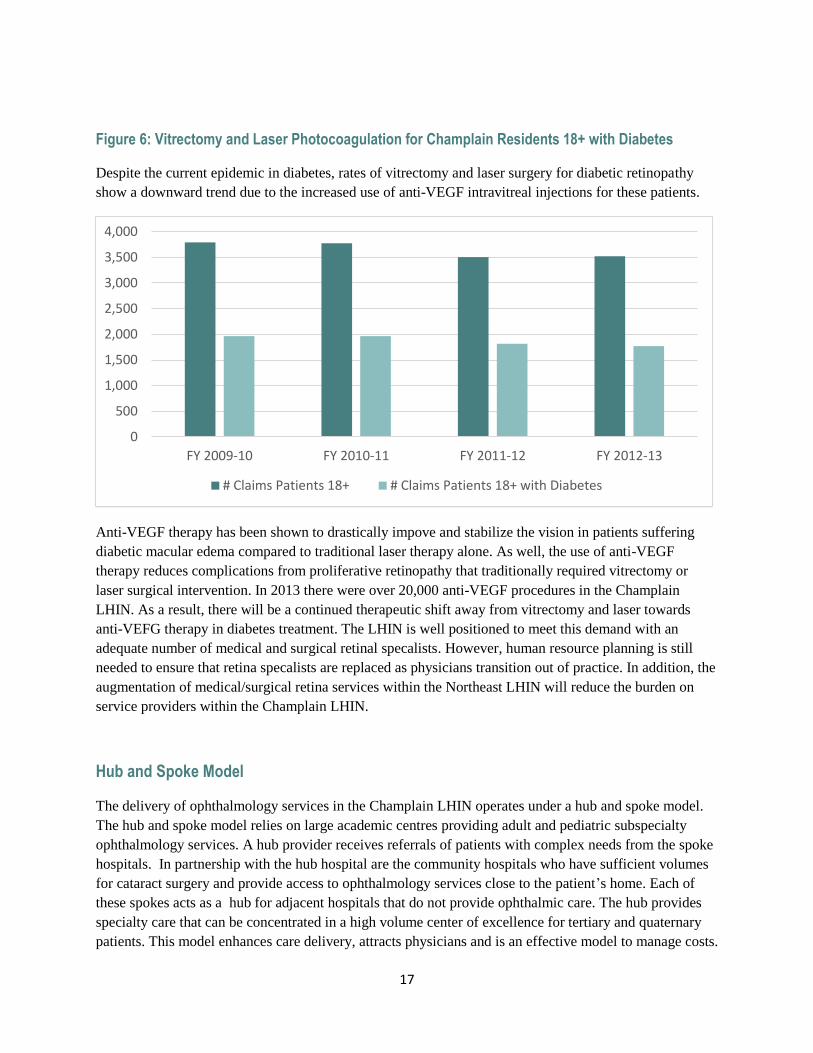
Figure 6: Vitrectomy and Laser Photocoagulation for Champlain Residents 18+ with Diabetes
Despite the current epidemic in diabetes, rates of vitrectomy and laser surgery for diabetic retinopathy
show a downward trend due to the increased use of anti-VEGF intravitreal injections for these patients.
Anti-VEGF therapy has been shown to drastically impove and stabilize the vision in patients suffering
diabetic macular edema compared to traditional laser therapy alone. As well, the use of anti-VEGF
therapy reduces complications from proliferative retinopathy that traditionally required vitrectomy or
laser surgical intervention. In 2013 there were over 20,000 anti-VEGF procedures in the Champlain
LHIN. As a result, there will be a continued therapeutic shift away from vitrectomy and laser towards
anti-VEFG therapy in diabetes treatment. The LHIN is well positioned to meet this demand with an
adequate number of medical and surgical retinal specalists. However, human resource planning is still
needed to ensure that retina specalists are replaced as physicians transition out of practice. In addition, the
augmentation of medical/surgical retina services within the Northeast LHIN will reduce the burden on
service providers within the Champlain LHIN.
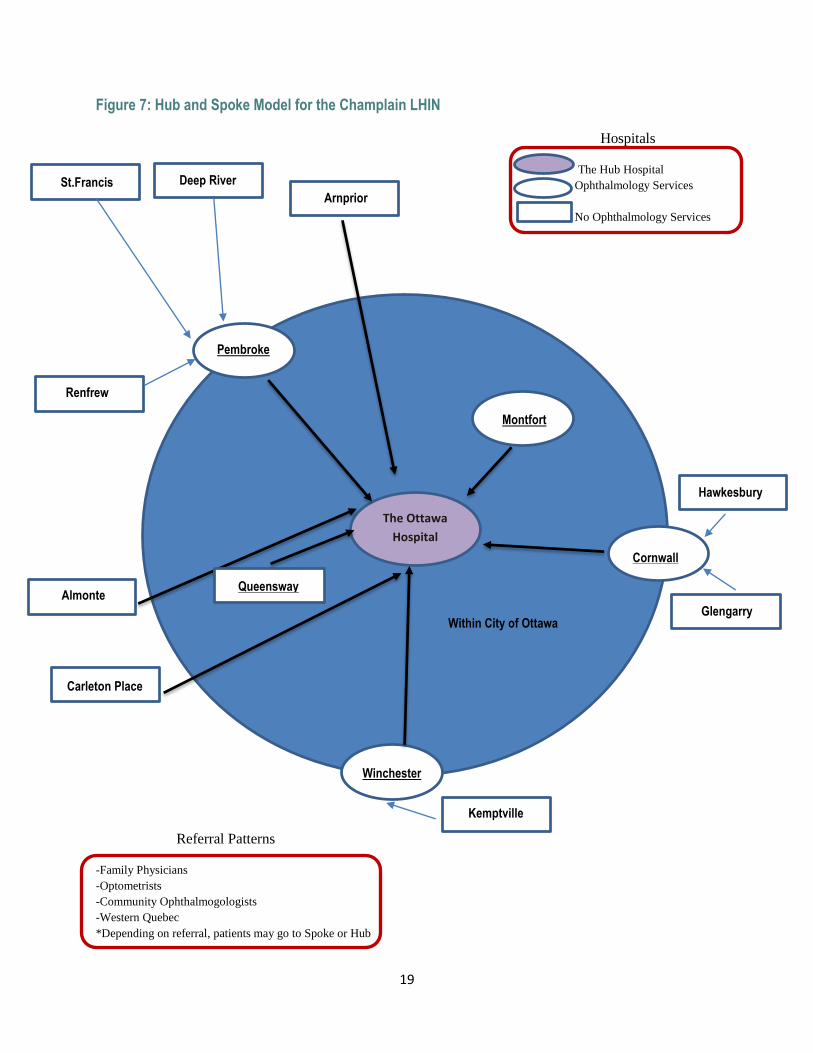
Hub and Spoke Model
The delivery of ophthalmology services in the Champlain LHIN operates under a hub and spoke model.
The hub and spoke model relies on large academic centres providing adult and pediatric subspecialty
ophthalmology services. A hub provider receives referrals of patients with complex needs from the spoke
hospitals. In partnership with the hub hospital are the community hospitals who have sufficient volumes
for cataract surgery and provide access to ophthalmology services close to the patient’s home. Each of
these spokes acts as a hub for adjacent hospitals that do not provide ophthalmic care. The hub provides
specialty care that can be concentrated in a high volume center of excellence for tertiary and quaternary
patients. This model enhances care delivery, attracts physicians and is an effective model to manage costs.
0
500
1,000
1,500
2,000
2,500
3,000
3,500
4,000
FY 2009-10 FY 2010-11 FY 2011-12 FY 2012-13
# Claims Patients 18+ # Claims Patients 18+ with Diabetes
18
The hub and spoke model in the Champlain LHIN is extremely successful. The advantages and key
components of this model are:
High volume dedicated cataract surgery facilities: by optimizing and standarizing the peri-operative
processes for routine cataract surgery, high volumes can be achieved ensuring high quality at low cost per
case.
Low volume facility: a separate operating room suite is used for complex cases, teaching and research.
Emergency services: ophthalmogists provide coverage for the hub and any emergencies that cannot be
dealt with by the rural hospitals. Coverage is 24 hours per day, 365 days per year.
Recruiting ophthalmologists: this model facilitates the process of recruiting ophthalmologists for the
community hospitals in the region. Smaller hospitals do not have the vast network and capabilites to
undertake effective recruitments of specialists. The opportunity to remain connected with the academic
centre is an important consideration for ophthalmologists working in the rural areas both for maintenance
of competency and remaining abreast of new developments in the field.
Maintenance of competence: the academic centres provide education, refresher practicums and
workshops on new clinical developments. Educational programs and patient teaching booklets are
available for all in the region.
Quality and safety management program: the academic centres have a number of programs for managing
quality and safety in ophthalmology that are available to the community hospitals.
Community hospitals: are the spokes in the hub and spoke model. They provide medium volume cataract
surgery to patients close to their home. The hub provides planning and assistance in recruiting
ophthalmologists, and quality and saftey systems. Many of the hub ophthalmologists operate in the rural
areas and provide standarized, quality care close to home for the patients. Local patients benefit from
convenient access and the assurance of quality. Complex cases are referred to the hub hospital.
19
Figure 7: Hub and Spoke Model for the Champlain LHIN
Hospitals
The Hub Hospital
Ophthalmology Services
No Ophthalmology Services
Referral Patterns
-Family Physicians
-Optometrists
-Community Ophthalmogologists
-Western Quebec
*Depending on referral, patients may go to Spoke or Hub
Montfort
Cornwall
Winchester
Pembroke
Kemptville
Hawkesbury
Glengarry Almonte
Carleton Place
St.Francis
Renfrew
Deep River Arnprior
The Ottawa
Hospital
Queensway
Within City of Ottawa
20
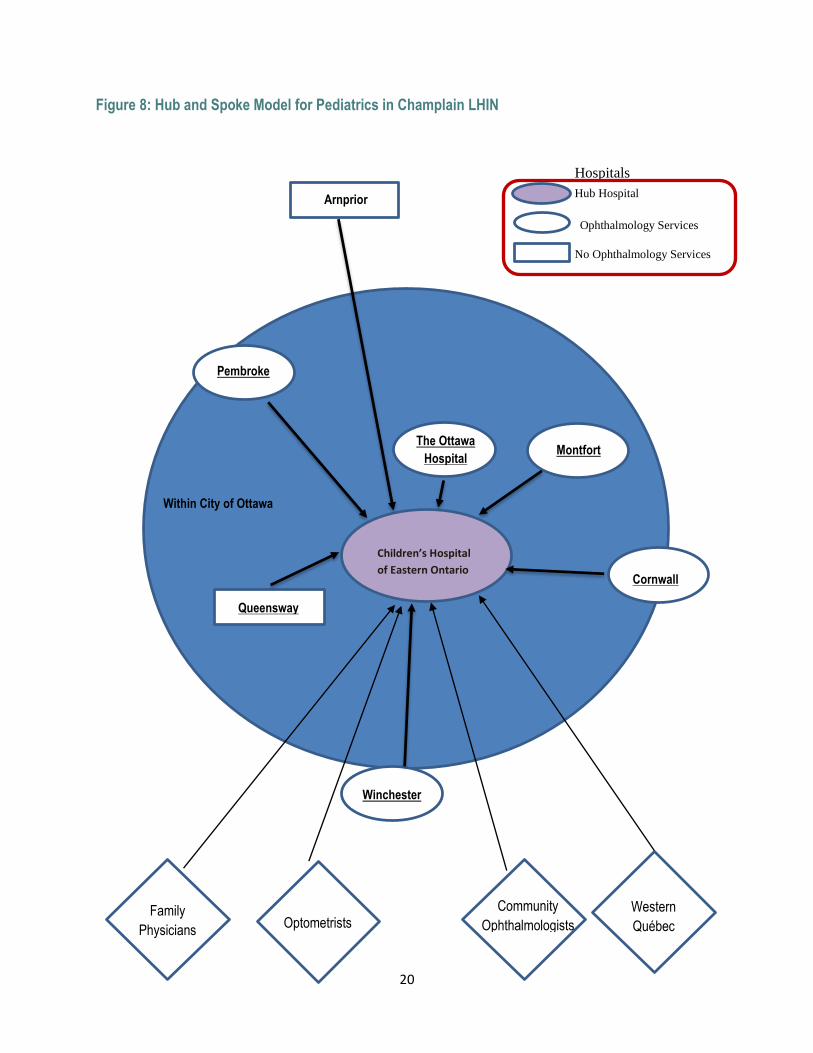
Figure 8: Hub and Spoke Model for Pediatrics in Champlain LHIN
Hospitals
Hub Hospital
Ophthalmology Services
No Ophthalmology Services
Montfort
Cornwall
Winchester
Pembroke
Arnprior
Children’s Hospital
of Eastern Ontario
Queensway
Within City of Ottawa
The Ottawa
Hospital
F Family
Physicians F
Optometrists F Community
Ophthalmologists
Western
Québec
21
Hospitals Providing Ophthalmic Services in the Hub and Spoke Model
The Champlain LHIN derives much of its success from the development of the hub and spoke model. As
one of the largest Academic Health Sciences Centres in Canada, The Ottawa Hospital (TOH) lies at the
centre of the adult hub of ophthalmic sercies. Ophthalmology services provided outside the hub, at the
spokes, are: 1) Hôpital Montfort (HM) (Ottawa), 2) Winchester District Memorial Hospital (WDRH)
3) Pembroke Regional Hospital (PRH) and 4) Cornwall Community Hospital (CCH). Each of these
hospitals has a long history of community support and is strongly engaged with their local populations.
Each of the spoke hospitals in turn act as a hub for smaller community hospitals that do not provide
ophthalmology services.
Although the Perth and Smiths Falls District Hospital (PSFDH) resides in the South East LHIN,
ophthalmologists from TOH provide surgical services on site and patients may elect to travel to Ottawa or
Kingston (South East LHIN) for additional care.
The Children’s Hospital of Eastern Ontario (CHEO) is the hub for all secondary, tertiary and quaternary
pediatric ophthalmology care in the Champlain LHIN. It is a major referral centre for pediatric
ophthalmology from Champlain optometrists, ophthalmologists, family physicians and emergency rooms.
As there is limited ophthalmology care for children in the North East LHIN and the Quebec Outaouais
regions, children from these areas are also referred to CHEO for specialized care in pediatric
ophthalmology. CHEO also provides all specialized pediatric ophthalmology care to children from
Iqaluit.
As the Champlain LHIN is in close proximity to the Province of Quebec, many of the hospitals within the
LHIN provide medical, surgical and emergency services to patients of that province. The city of Gatineau
(4th largest city in Quebec) lies directly across the Ottawa River from the City of Ottawa. Cataract surgery
for out-of-province (e.g., Quebec) patients, occurs at PRH, HM, CCH and at TOH (figure 11). The need
to provide subspecialty and emergency care for regional Quebec patients in Champlain LHIN Hospitals
derives from the lack of subspecialty presence in the Outaouais region. Montreal is the closest medical
centre capable of providing tertiary and quaternary ophthalmic care. The integration of Quebec
ophthalmology patients into the Champlain LHIN can lead to logistical challenges in calculating certain
metrics including wait time for patients of the Province of Ontario. Patients from the Province of Quebec
access services within the Champlain LHIN at varying degrees depending on the institution. At TOH
approximately 500 Quebec cataract surgeries are performed annually. There is a financial benefit to the
organization at present that permits this activity to continue. At the University of Ottawa Eye Institute
approximately 20 percent of patient visits are from Quebec.
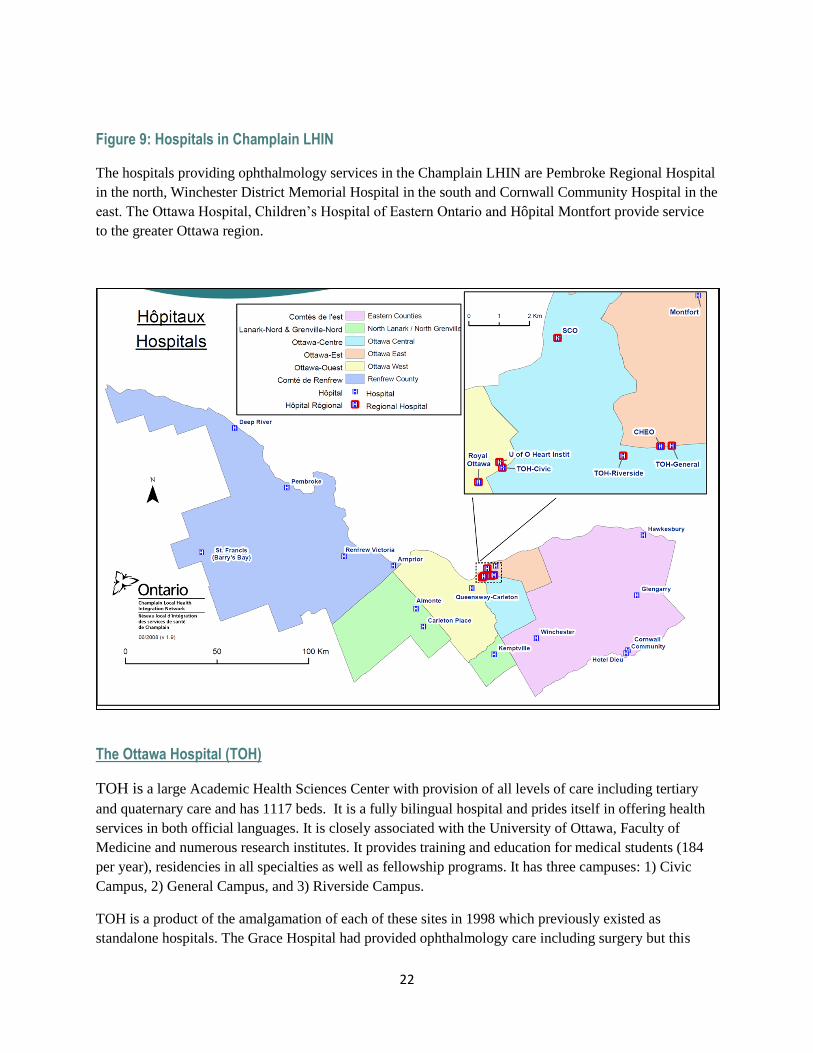
22
Figure 9: Hospitals in Champlain LHIN
The hospitals providing ophthalmology services in the Champlain LHIN are Pembroke Regional Hospital
in the north, Winchester District Memorial Hospital in the south and Cornwall Community Hospital in the
east. The Ottawa Hospital, Children’s Hospital of Eastern Ontario and Hôpital Montfort provide service
to the greater Ottawa region.
The Ottawa Hospital (TOH)
TOH is a large Academic Health Sciences Center with provision of all levels of care including tertiary
and quaternary care and has 1117 beds. It is a fully bilingual hospital and prides itself in offering health
services in both official languages. It is closely associated with the University of Ottawa, Faculty of
Medicine and numerous research institutes. It provides training and education for medical students (184
per year), residencies in all specialties as well as fellowship programs. It has three campuses: 1) Civic
Campus, 2) General Campus, and 3) Riverside Campus.
TOH is a product of the amalgamation of each of these sites in 1998 which previously existed as
standalone hospitals. The Grace Hospital had provided ophthalmology care including surgery but this
23
facility was closed in 1999. This activity was transferred to the Riverside Campus of TOH and renamed
the Riverside Eye Care Centre. The ophthalmology program at the Civic Campus was also transferred to
the Riverside Campus at the time of amalgamation. Both the Civic and General Campus have inpatient
activity and the Riverside Campus is strictly an outpatient facility.
TOH ophthalmology has approximately 89,000 outpatient visits per year on–site and performs 15,000
ophthalmic procedures, of which 11,000 are cataract surgeries making it the largest provider of cataract
surgery in Canada. Seventy per cent of the cataract allocation for the Champlain LHIN is carried out at
TOH. Unique to TOH is Ottawa’s proximity to Quebec. On average over 600 cataracts per year are from
out-of-province. The Department of Ophthalmology provides multidisciplinary support at TOH for
neurology, neurosurgery, trauma services, endocrinology, dermatology, oncology and rheumatology.
TOH offers cataract surgery and subspecialty care in a cohesive two site model with timely, cost effective
surgery ensuring quality of care. The hub and spoke model combines the flagship role of a large teaching
hospital and a medical school’s ophthalmology department in partnership with the local community
hospitals to provide access near to home for those located far from the hub. This model is considered the
best practice framework for regional networks for cataract surgery in Canada. By optimizing and
standardizing the entire peri-operative processes at TOH for routine cataract surgery, it has achieved high
quality at low cost. Historically, with incremental volumes funded through the Wait Time Strategy, TOH
has been able to ramp up surgical volume in the last 3 months of the fiscal year (Feb-April 1). This has
helped the Champlain LHIN and local providers meet cataract wait time targets. In the past year the need
to accelerate surgical volume at TOH has been more muted but is certainly challenging when allocated
cataract volumes are not known in a timely fashion to allow for accommodation of both physical and
manpower resources.
TOH is well known in the Champlain region for its leading position in teaching, research and clinical
services. TOH provides affiliated community hospitals with the same TOH standards of ophthalmology
services by sending TOH ophthalmologists to perform cataract surgery for patients in their home
community.
Civic Campus - This site is designated as the primary trauma center for TOH. The ophthalmology
program (clinics and operating room) were transferred at the time of amalgamation to the Riverside
Campus and ophthalmology is a consult service only at the Civic Campus. Some ophthalmology services
such as oculoplastic surgery and neuro-ophthalmology provide support as members of multidisciplinary
teams in neurosurgery, trauma and head and neck oncology at this campus. Dedicated ophthalmology
operating room suites and surgical staff do not exist at this site.
Riverside Campus: Eye Care Centre – At the time of amalgamation the Riverside Campus was
converted into an outpatient facility. Numerous outpatient clinics including ophthalmology provide
clinical services Monday to Friday. Surgical eye care is provided by 3 dedicated cataract operating rooms
and 1 retina room Monday to Friday. The Riverside staff physicians provide much of the inpatient
ophthalmic support for the Civic Campus. In-patients from the Civic Campus are either transferred to the
Riverside clinic or they are seen at the bedside at the Civic site if transport is difficult. The Eye Care
Centre, Riverside Campus is a high volume dedicated ophthalmic surgical unit performing approximately
80% of the total volume of cataract surgery at TOH in an efficient and safe environment. The Eye Care
Centre completed 8,557 (2014/15) cataracts including combined procedures, and an additional 1,400
24
subspecialty surgeries, 200 of these being retinal procedures. As well as being a high volume cataract
center, there are 8 refracting lanes, a minor procedure room and a full complement of diagnostic services
including retinal imaging and therapeutic lasers.
General Campus: Eye Institute - The University of Ottawa Eye Institute opened in 1992 and is the home
of 14 full time subspecialty ophthalmologists in retina vitreous surgery, uveitis, neuro-ophthalmology,
glaucoma, ophthalmic plastic and reconstructive surgery, adult strabismus, cornea and external disease
and ophthalmic pathology. The Eye Institute completed 1,900 cataracts including combined procedures,
and in addition another 1,600 subspecialty procedures. There are 26 refracting lanes, one minor procedure
operating room, and 2 dedicated ophthalmology operating rooms. In addition, one large ophthalmic
operating room is located as one of 17 main operating rooms one floor below the Eye Institute (3RD floor)
within the Critical Care Wing (2nd floor). The main operating room is utilized by ophthalmology Tuesday-
Friday and is available after hours and on weekends for emergency surgery. It is the only ophthalmology
operating room at TOH available after hours. The Eye Institute is home to the largest ophthalmic
diagnostic services in Canada. They provide a full range of diagnostic services in proximity to the clinics
and the operating rooms.
Children’s Hospital of Eastern Ontario (CHEO)
CHEO is an academic hospital affiliated with the University of Ottawa Medical School and the General
Campus of TOH. CHEO is the only specialized hospital serving the pediatric population in the Champlain
LHIN. It is a 167 bed affiliated facility providing all levels of care including tertiary and quaternary care.
There are two on-site pediatric ophthalmologists and one affiliated community ophthalmologist utilizing
operating room resources. Emergency access is 24 hours per day, 365 days per year with a call schedule
integrated into the TOH call schedule. All in-patient consults and emergency follow-ups are managed by
the onsite pediatric ophthalmologists. Two CHEO pediatric ophthalmologists are integrated into the TOH
adult strabismus program.
There are 6,300 outpatient pediatric ophthalmology visits at CHEO annually which includes 400 pediatric
strabismus cases, and close to 200 pediatric intraocular procedures. TOH based subspecialists in retina,
cornea, glaucoma and oculoplastic surgery also provide pediatric care at CHEO. Pediatric
ophthalmologists at CHEO provide urgent, emergent and elective care, both medical and surgical, to
children from the North East LHIN, as well as the Outaouais and Iqaluit, due to limited resources in these
regions.
The vast majority of pediatric ophthalmic services for the Champlain LHIN are centered at the CHEO.
Very few general ophthalmologists in the community provide primary and secondary pediatric eye care.
Hôpital Montfort (HM)
Hôpital Montfort is a 289 bed facility located within Ottawa. It is located in the east end of Ottawa
approximately 8 km from the Riverside and General campuses of TOH. HM is an academic facility of the
University of Ottawa, Faculty of Medicine for medical student and resident education mostly in the
Francophone stream. The HM has one ophthalmic operating room. They complete 2,000 cataracts
annually. There are 6 surgeons on staff all but one have a cross appointment to TOH. Patients are
followed in the offices; however, the HM does provide clinic space for retinal imaging and laser
25
procedures for retina and glaucoma as well as appropriate equipment to assess inpatient and emergency
referrals. Hôpital Montfort strongly supports the Francophone community of both the Ottawa region and
the Outaouais. The staff ophthalmologists have subspecialty training in glaucoma, medical retina and
cornea. They have an emergency call schedule partially integrated with the call schedule of TOH.
Winchester District Memorial Hospital (WDMH)
WDMH is a rural hospital affiliated with University of Ottawa, Faculty of Medicine with approximately
50 in-patient beds located 45 minutes south of Ottawa. Four ophthalmologists have surgical privileges
and provide in patient consultation services. Three of the 4 ophthalmologists have appointments to TOH.
Approximately 450 cataract surgeries are performed annually. The operating room does not have a fixed
ceiling mounted microscope but uses a portable version. A ceiling mounted microscope has been
requested. No formal call schedule for ophthalmology exists locally but call coverage is provided by
TOH.
Pembroke Regional Hospital (PRH)
PRH is located 150 km northwest of Ottawa. PRH is an affiliated teaching facility of the University of
Ottawa, Faculty of Medicine with approximately 140 in-patient beds. There are 2 ophthalmologists
residing within Pembroke that provide call coverage and one ophthalmologist performs cataract surgery.
In addition, two TOH surgeons perform cataract surgery (Hub and Spoke Model). PRH completes 650
cataracts annually on local residents. There is also an outreach program for oculoplastic surgery where
two TOH oculoplastic surgeons hold clinics 6-8 times annually.
Cornwall Community Hospital (CCH)
CCH is located 100 km southeast of Ottawa and is a 138 bed facility with academic affiliation with the
University of Ottawa. CCH currently has 2 ophthalmologists and are actively recruiting for a third in
2016. As well, one ophthalmologist who no longer performs surgery continues to provide medical care.
CCH performs approximately 1,200 cataract surgeries annually (with approximately 250 bilateral cataract
surgeries not funded by MOH). One of the CCH ophthalmologists runs a private surgical facility located
off site that performs cataract surgery, femtolaser cataract surgery and intravitreal injections. At the
private center 100 cataracts (OHIP or refractive) are performed annually. The ophthalmologists in
Cornwall see the full spectrum of patients in all age groups including the pediatric population. All
specialized care in pediatric ophthalmology is referred to the CHEO.
Perth and Smiths Falls District Hospital (PSFDH) – South East LHIN
It is important to note that PSFDH is in the South East LHIN. This historical relationship between TOH
and PSFDH has existed prior to the creation of the LHINS.
PSFDH is a two site (Perth and Smiths Falls) hospital with 85 beds located within the South East LHIN
located 78 km southwest of Ottawa. TOH surgeons travel to Smiths Fall to perform approximately 400
cataract surgeries at Smith Falls for local patients. Emergency coverage is shared with TOH and Kingston
within the South East LHIN.
26
Ophthalmology On-Call Services
Ophthalmology on-call services is varied across the constituent hospitals of the Champlain LHIN.
However, the successful integration of call services across the LHIN has promoted the right access, at the
right time to the right patient for many years in its current design as a hub and spoke model.
At the hub, TOH has an on-call schedule for both general ophthalmology and retina services. The other
subspecialties such as oculoplastics, cornea, glaucoma, neuro-ophthalmology and uveitis provide ad hoc
support which functions very well. The on-call staff is all surgeons. Medical ophthalmologists do not
provide on-call services. CHEO is integrated into the TOH after-hours call schedule providing cross
coverage for adult and pediatric ophthalmology. Many of the part time physicians of TOH also have
appointments at other hospitals (Montfort, Winchester, and Pembroke and Quebec hospitals in the
Outaouais region) and they are able to integrate coverage. The call schedule is updated and provided to
Locating at TOH so that all hospital emergency rooms can access coverage. TOH’s two campuses for
ophthalmology divide the greater Ottawa area and Champlain LHIN into two regions: 1) hospitals and
emergency rooms west of Bank Street are triaged by the Riverside Eye Care Centre, and 2) hospitals and
emergency rooms east of Bank Street are triaged by the University of Ottawa Eye Institute at the General
Campus. The retina service provides on-call services 365 days per year with 6 retina surgeons following a
weekly call schedule. Cross LHIN support for retina has been provided to the South East LHIN
(Kingston) when their retina surgeon is unavailable (approximately 6 weeks per year). Additionally as
there is no retina/vitreous support in the Northeast LHIN patients often travel to Ottawa for retinal care.
The spokes provide coverage as follows:
HM has a formal call schedule and many of its ophthalmic staff have cross appointments to TOH. When
possible their call schedule is integrated into the TOH call schedule framework.
WDMH does not have a call schedule but emergency patients are covered within TOH on-call.
PRH has two ophthalmologists that split on-call services equally 365 days per year.
CCH has two ophthalmologists with a third surgical ophthalmologist to be recruited in 2016. This new
recruit will enable almost complete on-call coverage. CCH provides ophthalmology on-call coverage to
Glengarry Memorial Hospital and Hawkesbury and District General Hospital. Although there is no formal
call integration with TOH, pragmatically any patient unable to access emergency medical services can
seek consultation with TOH 365 days of the year. Follow-up of these patients will occur in Cornwall once
service is accessible (usually with a few days at most).
CHEO has integrated call with TOH.
PSFDH (South East LHIN) at the present refer patients from their emergency room to TOH. This
legacy relationship is currently undergoing re-examination.
Emergency Services 24 hours a day, 7 days a week
The Champlain vision services are provided around a construct of the hub and spoke model. Lying at the
centre, both geographically and functionally are TOH and CHEO. TOH provides adult ophthalmology
27
care and CHEO provides pediatric ophthalmology care. Both are academic centres and able to provide all
levels of ophthalmic care in all subspecialties and provide emergent care to the population within this
LHIN, surrounding LHINs and adjacent regions of Quebec. The spoke hospitals (CCH and PRH) provide
on-call through varied approaches. WDMH does not have coverage but is integrated as is the MH into the
call schedule of TOH where the vast majority of surgeons at these sites have appointments at TOH. TOH
and CHEO have integrated call with an on-call surgeon and resident support 365 days a year. The staff
surgeons provide call on one week rotations. Emergency clinics with onsite staff surgeons, and supported
by residents, are run every day of the year in order to accept referrals from emergency rooms, family
physicians and optometrists. Retina emergency services are also provided 24 hours a day, 365 days a year
with an on-call retina surgeon and resident/fellow support. Six retina surgeons rotate call on a weekly
basis throughout the year. The yearly call schedule is distributed to TOH communications in the fall of
each year for the following calendar year. All emergency departments in the Champlain LHIN are trained
to know how to reach urgent ophthalmology services at their local hospital. All ophthalmologists know to
call On-call Telecommunications at TOH when a subspecialist is required.
At TOH, in-patients at the Civic and General Campuses are covered by the on-call staff physician in
conjunction with residents and fellows. The patients may be seen in the clinics or at the bedside
depending on patient needs and mobility profile. At CCH, MH and PRH, in-patients are attended to by
staff surgeons either at the bedside or in hospital based clinics.
The hub and spoke model in the Champlain LHIN achieves good access for rural areas with PRH to the
north, CCH to the east and WDMH to the south. The west encroaches upon PSFDH which is within the
South East LHIN.
Staff surgeons from TOH have clinics and surgery at some of the “spoke” hospitals to help support local
optometrists and ophthalmologists in smaller centers. PRH and WDMH follow this model. CCH does not
have TOH surgeons working at this site.
Telemedicine is utilized at the Riverside Eye Care Centre, TOH for the Pre-Assessment visit prior to
cataract surgery. The pre-assessment visits are provided via telemedicine to two rural hospitals.
Collaboration between the Renfrew Victoria Hospital and the Carleton Place and District Memorial
Hospital has made this service available. This service saves a commute to Ottawa for patients living in
outlying areas who are having cataract surgery.
E-consult services are provided by two CHEO pediatric ophthalmologists. An e-consult pilot project is
underway with other pediatric specialties at CHEO which is showing an increased volume of e-consult
requests over the past year. Overall early data suggests that 50% of consults can be managed or rerouted
to a more appropriate care provider without needing to engage the hospital.
Outside of the Champlain LHIN many ophthalmologists participate in the CNIB van program in Northern
Ontario. TOH has a contractual agreement with Nunavut to provide ophthalmic care. Dr. Rama Behki
travels to Iqaluit bi-annually with resident support for two, one-week clinics, in June and December.
TOH surgeons in Ottawa provide subspecialty support and surgery (at TOH) for referrals from Dr. Behki
for Nunavut patients.
28
Communication
Currently, communication between institutions and providers relies on email, fax or conventional mail to
deliver consult material to referring physicians. The electronic medical records (EMRs) of the hospitals
within the LHIN are varied and integration is minimal. Individual ophthalmologists and optometrists are
transitioning into EMR systems from various vendors but these records are also not integrated. Diagnostic
imaging systems at various hospitals do not allow access except in a limited scope. Duplication of
imaging studies often occurs as it expedites patient care but at the cost of efficiency and unnecessary
redundancy. TOH is at the early stages of implementing a new EMR system but other hospitals in the
LHIN may have already moved to a non-compatible system or wish to use an alternative system. This
presents a significant challenge to providing integrated health information systems across the LHIN. The
development of an OHIP billing code for e-consult is strongly recommended.
CHEO has an integrated EMR in many clinical and inpatient units. The rollout of the EPIC EMR for
ophthalmology has been postponed indefinitely, due to budgetary constraints imposed in the spring of
2015.
Individual providers do not share common health information systems/EMR either within the specialty of
ophthalmology or with other physicians. Many optometrists have migrated to EMR systems but there is
no integration between the various vision care providers.
Strengths of the Current Hub and Spoke Model
1. The hub and spoke model of delivery and integration of care has been very successful in
providing care to patients of the Champlain LHIN and has been seen as a model for other
jurisdictions. The central location of such services such as retina permits easy tracking of
complications such as endophthalmitis which are all referred to a single center of excellence.
All cases of endophthalmitis are tracked within the retina service and the infectious disease
department of the TOH so that patterns and triggers for possible intervention for process
management are able to be identified. Expertise with an academic hub permits 24 hours a day,
365 days a year access for all patients in the Champlain LHIN.
The ‘spoke hospitals’ play an important role in permitting access to care within reasonable
distances of a patient’s home within the Champlain LHIN. Primary, secondary and even some
tertiary care is safely provided. Some of the distances between Ottawa and the hospitals in
Pembroke and Cornwall can exceed 150km and travel, particularly in the severe winters
experienced within the LHIN can be reduced.
There has been strong local support for the hospitals with fundraising of the spoke hospitals and
there has been no expression of interest or recognized need in consolidation of services.
2. Integration of call schedule and provision of 365 emergency access. As outlined in the description
of the hospitals providing ophthalmic care, there is a strongly integrated call system in place that
can address patients’ needs at the local level or, if unavailable or requiring tertiary/quaternary

29
care, can be accessed 24 hours per day, 365 days per year at the TOH. The Champlain LHIN
provides access for complex and emergent cases when necessary to our bordering LHINs namely
the South East and North East LHINs. The Champlain LHIN is also unique in Ontario as it
provides significant support for Quebec patients in adjacent areas as needed.
3. Within the Champlain LHIN there is a diversity of subspecialty expertise. TOH General Campus
has 14 dedicated subspecialists covering retina, cornea and external disease, neuro-
ophthalmology, ophthalmic plastic and reconstructive surgery, uveitis, pediatrics, adult
strabismus, pathology, epidemiology and electrophysiology. Approximately half of the
community ophthalmologists of the TOH have subspecialty training including cornea, retina,
glaucoma, adult strabismus, low vision, ophthalmic plastic and reconstructive surgery, neuro-
ophthalmology, medical education and international ophthalmology.
2.0 Recommendations for Improvement of the Current Hub and Spoke Model
2.1 Improve communication between institutions and providers
Despite tremendous advances in technology over the past two decades a persistent deficiency in the health
care system remains at the core of its information systems. Providers both at the organization level and
individual provider (ophthalmologist, optometrist, family physician etc.) have not been able to harness the
modern day health delivery systems in North America. In some instances, work-arounds have been
cobbled together in an attempt to distribute information such as imaging studies amongst providers.
Often these modifications are tedious and not user friendly thereby leading to underutilization.
A fully integrated functional Electronic Medical Record (EMR) across the LHIN (provincially/nationally)
would improve patient care and more importantly communication between providers. This is critical if
outcomes are to be analyzed in detail for the delivery of health care. In ophthalmology, where
optometrists and ophthalmologists often work together to care for patients, communication flow in both
directions is essential. Co-management of cataract surgery patients by ophthalmologists and optometrists
exemplifies this challenge. In an effort to determine the value of publicly funded cataract surgery, an
outcome analysis is essential. However, systems are not in place that permit easy, rapid and reliable
sharing of preoperative and post-operative visual acuities. Manual recording and retrieval of this data is
arduous and impractical. The lack of a universal, fully functional EMR across the province hampers
outcome analysis of “big data” and thus reduces opportunities for population health and clinical research.
Family physicians would be better served by being able to view eye care data from both optometrists and
ophthalmologists particularly in the diabetic population.
A fully integrated functional EMR should be a high priority provincially and ideally nationally. Research
would also be enhanced as has been evidenced by the recent introduction of the IRIS Registry in the
United States where over a third of ophthalmologists pool data into this system so that national eye health
data (big data) can be collected and evaluated. Provincial leadership, guidance and support are required to
bring information systems into the 21st century in Ontario.
30
2.2 Recruit a retina vitreous surgeon in the North East LHIN
With the predicted demographic increase for ophthalmic services (figure 2) within the Champlain LHIN
and slow growth of health care expenditures, it would be appropriate for the North East LHIN to recruit a
retina/vitreous surgeon. This would reduce or eliminate the transfer of medical and surgical retina cases to
the Champlain LHIN. This recruitment would increase access and reduce travel distances/cost for patients
that currently come to the Champlain LHIN for care. Ideally, a retina vitreous surgeon should be recruited
to the Outaouais region but as this lies in another provincial jurisdiction (Quebec) no influence has been
successful to date.
Overview of Community Based Vision Care Services in the Champlain LHIN
Community Providers - Ophthalmologists
As part of the current state analysis of vision care in the Champlain LHIN, the community
ophthalmologists were surveyed using an on-line survey (see appendix 2.1 for survey results). Many of
the community practices are group practices therefore the survey went to the group practice verses the
individual. Twenty-four surveys were distributed and 19 responded to give a 79% response rate. There are
over 50 ophthalmologists with private office practices. The office practices provide comprehensive and
subspecialty services as well as refractive eye surgery and some diagnostics. The highlights of the survey
provided the following data:
Pediatrics ophthalmic care is provided by 10/19 office practices although many do not routinely
see children under the age of 12.
Most offices have a Wait 1 (from referral to seen in the office) of 1 month or less and some
offices identified a 1-4 month wait for routine patient referrals.
The volume of out-of-province patients served (e.g. Quebec) ranged from 5-10%, although two
offices reported 50%-70%.
Non-OHIP cataracts and clear lens extractions are performed in private surgical centres (2)
however the volumes are under 10 per month.
Coverage for on-call and emergency services is arranged with other physicians in the same office
and off-hours emergencies are directed to go to the closest emergency department.
Summary of comments/challenges of respondents:
1. Volumes and acuity levels of patients: increasing volumes of patients with complex issues due to
the aging population.
2. Limited access to the operating room which increases the Wait 2 time.
3. Funding reductions in diagnostic fees are not consistent with rising costs of office practices.
Community Providers - Optometrists
Within the LHIN and surrounding areas there are approximately 420 optometrists. Approximately 36%
offer services in both official languages. Optometrists are regulated health professionals in Ontario who
are trained to examine eyes, screen for changes such as diabetic retinopathy, prescribe corrective lenses

31
and can prescribe certain medications for the eye. OHIP coverage is available for those patients on social
assistance and for patients yonger than 20 and over 65 years of age. Patients of any age who have diabetes
or an eye disease qualify for insured eye examintions every year. However, the fees for diagnostic tests
such as photographs of the retina are not covered by OHIP which can be a disincentive to patients for
screening.
Academic Program and Research
TOH is a centre of excellence for medical education and training in ophthalmology within the Champlain
LHIN. The University of Ottawa provides a five year comprehensive training program in ophthalmology
which leads to eligibility to write the Royal College specialty ophthalmology examination. Following the
PGY-1 year, which is designed to give a broad-based clinical exposure, the residents start their four core
years of ophthalmology. All residents are sent for a two-month comprehensive basic science and
introductory to clinical/surgical skills course in Toronto upon completing the PGY-1 core rotations.
Throughout the four years, there is weekly dedicated formal lecture time and seminars which continue
through the academic year. The department sponsors an active visiting professor program attracting world-
class clinicians and scientists. A journal club is held periodically with both faculty and community
ophthalmologists participating. The curriculum, encompassing four years of core ophthalmology training,
has dedicated research time, electives and in-depth exposure to subspecialties. The resident's progress is
closely monitored in the clinics, operating room and teaching sessions and by practice oral examinations.
All residents write the OKAP exam in the spring of each year. Resident training sites include:
University of Ottawa Eye Institute, Ottawa Hospital - General Campus
Children's Hospital of Eastern Ontario
Riverside Eye Care Center, Ottawa Hospital - Riverside Campus
Baffin Program - Iqaluit, Nunavut
All TOH residents are actively engaged in ophthalmic research. Residents actively participate in a
research project each year and their results are presented at the annual departmental Research Day in
May. Residents are encouraged and supported when they present papers and posters at national and
international meetings.
The Department of Ophthalmology partnership at TOH provides financial and resource support for basic
science and clinical research which has been in place for two decades. The Department has recently
engaged with the University of Ottawa, Faculty of Medicine and the associated Research Institutes in
creating a partnership agreement which should further advance research endeavors by integrating
recruitment and cost sharing with recently acquired tenured positions made available by the University of
Ottawa Central.
The Department of Ophthalmology at TOH has weekly grand rounds throughout the academic year at the
General Campus. These rounds are video broadcasted to the Riverside Eye Care Center and webcast to
ophthalmologists at their homes or offices. Journal Club is held monthly during the academic year.
The Department of Ophthalmology of TOH, CHEO and members of the HM provide undergraduate
teaching for medical students in both the English and Francophone streams at the University of Ottawa

32
Medical School. Currently in the Francophone stream, optometrists are involved in teaching some
ophthalmic examination skills at the Montfort.
The Sally Letson Symposium (SLS) is the largest CME outside of the Canadian Ophthalmology Annual
meeting in Canada. This three-day educational symposium covers a specific subspecialty/topic every fall
with attendance of between 500-700 invitees including ophthalmologists, optometrists, residents, fellows,
nurses and ophthalmic technicians. This has been a great opportunity for ophthalmologists to acquire
CME credits and update their skills in clinical care. The SLS has been in existence for over 45 years and
is supported by the Canadian Ophthalmological Society.
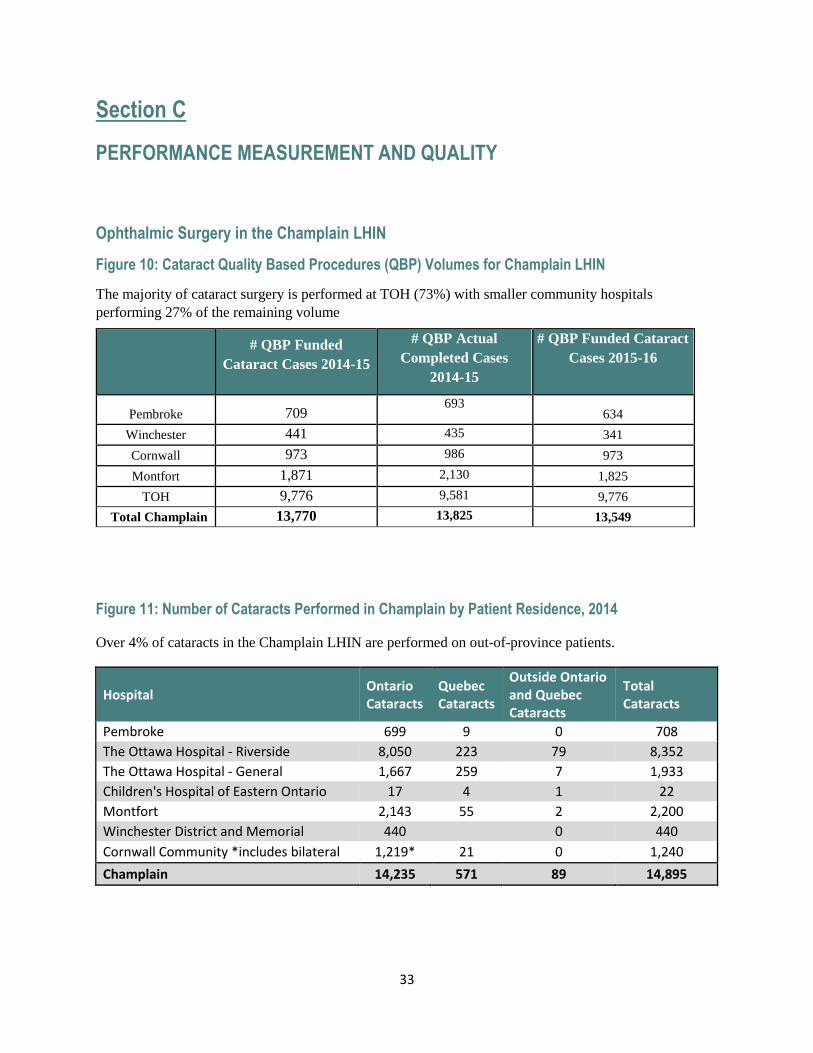
33
Section C
PERFORMANCE MEASUREMENT AND QUALITY
Ophthalmic Surgery in the Champlain LHIN
Figure 10: Cataract Quality Based Procedures (QBP) Volumes for Champlain LHIN
The majority of cataract surgery is performed at TOH (73%) with smaller community hospitals
performing 27% of the remaining volume
Figure 11: Number of Cataracts Performed in Champlain by Patient Residence, 2014
Over 4% of cataracts in the Champlain LHIN are performed on out-of-province patients.
Hospital Ontario Cataracts
Quebec Cataracts
Outside Ontario and Quebec Cataracts
Total Cataracts
Pembroke 699 9 0 708
The Ottawa Hospital - Riverside 8,050 223 79 8,352
The Ottawa Hospital - General 1,667 259 7 1,933
Children's Hospital of Eastern Ontario 17 4 1 22
Montfort 2,143 55 2 2,200
Winchester District and Memorial 440 0 440
Cornwall Community *includes bilateral 1,219* 21 0 1,240
Champlain 14,235 571 89 14,895
# QBP Funded
Cataract Cases 2014-15
# QBP Actual
Completed Cases
2014-15
# QBP Funded Cataract
Cases 2015-16
Pembroke 709 693
634
Winchester 441 435 341
Cornwall 973 986 973
Montfort 1,871 2,130 1,825
TOH 9,776 9,581 9,776
Total Champlain 13,770 13,825 13,549
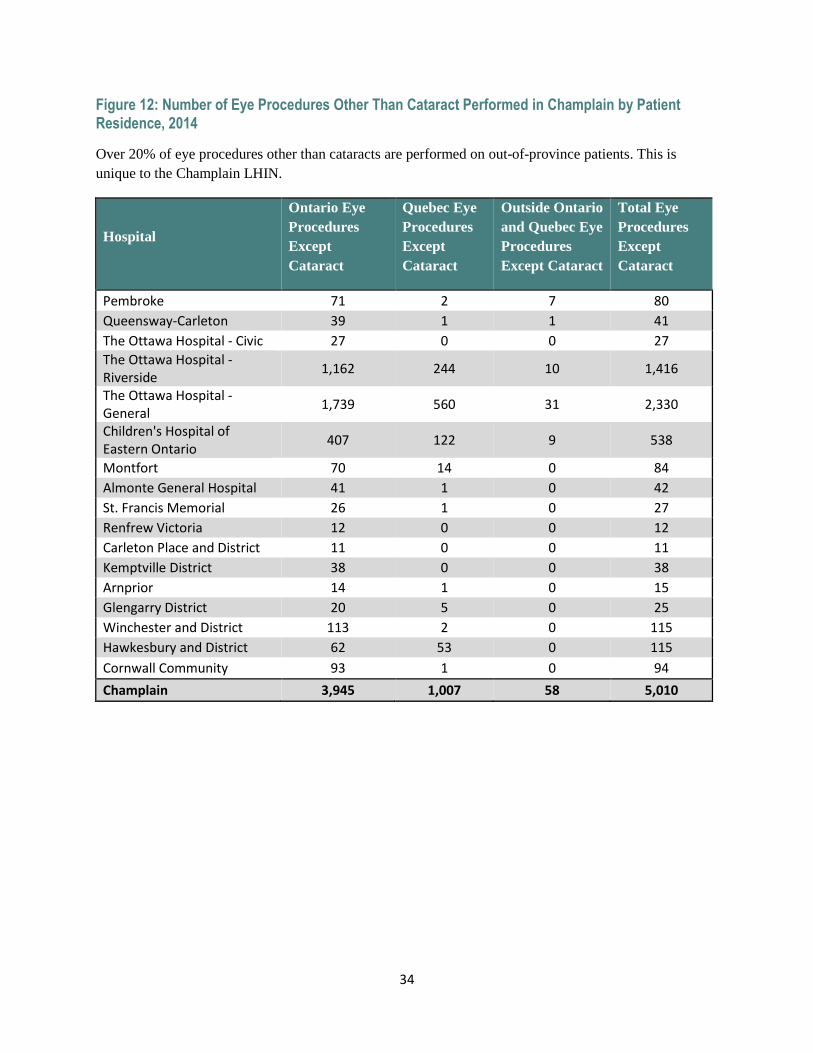
34
Figure 12: Number of Eye Procedures Other Than Cataract Performed in Champlain by Patient Residence, 2014
Over 20% of eye procedures other than cataracts are performed on out-of-province patients. This is
unique to the Champlain LHIN.
Hospital
Ontario Eye
Procedures
Except
Cataract
Quebec Eye
Procedures
Except
Cataract
Outside Ontario
and Quebec Eye
Procedures
Except Cataract
Total Eye
Procedures
Except
Cataract
Pembroke 71 2 7 80
Queensway-Carleton 39 1 1 41
The Ottawa Hospital - Civic 27 0 0 27
The Ottawa Hospital - Riverside
1,162 244 10 1,416
The Ottawa Hospital - General
1,739 560 31 2,330
Children's Hospital of Eastern Ontario
407 122 9 538
Montfort 70 14 0 84
Almonte General Hospital 41 1 0 42
St. Francis Memorial 26 1 0 27
Renfrew Victoria 12 0 0 12
Carleton Place and District 11 0 0 11
Kemptville District 38 0 0 38
Arnprior 14 1 0 15
Glengarry District 20 5 0 25
Winchester and District 113 2 0 115
Hawkesbury and District 62 53 0 115
Cornwall Community 93 1 0 94
Champlain 3,945 1,007 58 5,010
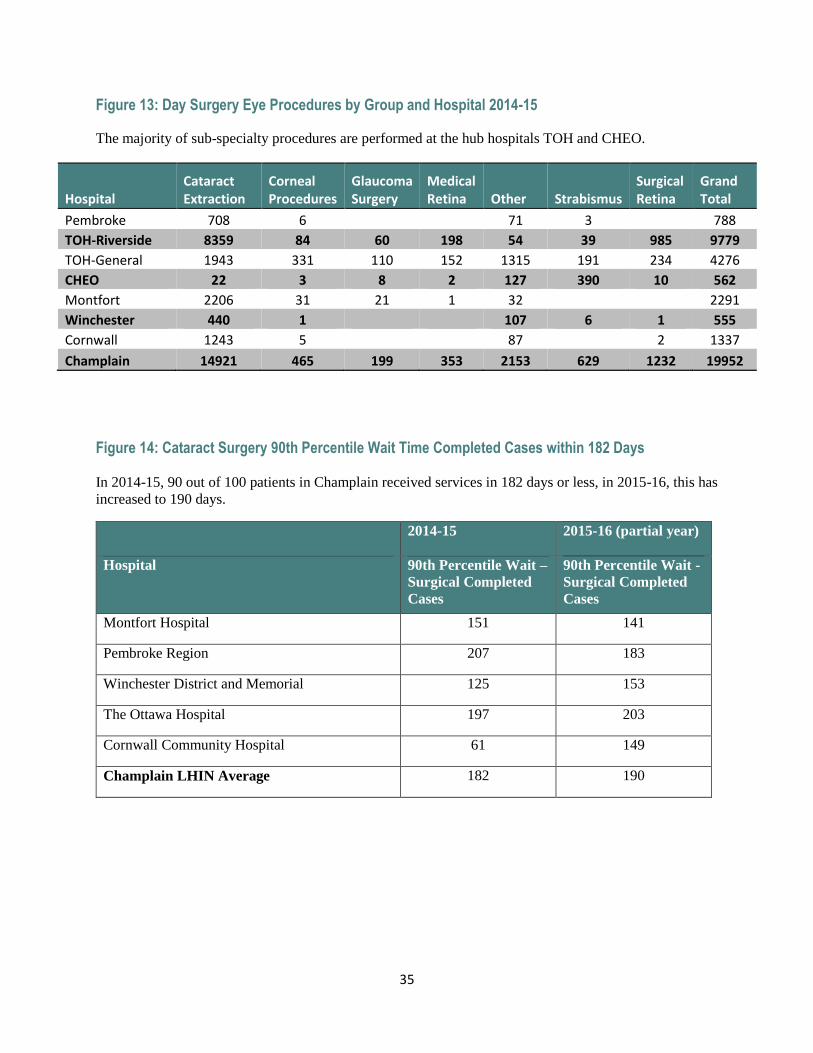
35
Figure 13: Day Surgery Eye Procedures by Group and Hospital 2014-15
The majority of sub-specialty procedures are performed at the hub hospitals TOH and CHEO.
Hospital Cataract Extraction
Corneal Procedures
Glaucoma Surgery
Medical Retina Other Strabismus
Surgical Retina
Grand Total
Pembroke 708 6 71 3 788
TOH-Riverside 8359 84 60 198 54 39 985 9779
TOH-General 1943 331 110 152 1315 191 234 4276
CHEO 22 3 8 2 127 390 10 562
Montfort 2206 31 21 1 32 2291
Winchester 440 1 107 6 1 555
Cornwall 1243 5 87 2 1337
Champlain 14921 465 199 353 2153 629 1232 19952
Figure 14: Cataract Surgery 90th Percentile Wait Time Completed Cases within 182 Days
In 2014-15, 90 out of 100 patients in Champlain received services in 182 days or less, in 2015-16, this has
increased to 190 days.
2014-15 2015-16 (partial year)
Hospital 90th Percentile Wait –
Surgical Completed
Cases
90th Percentile Wait -
Surgical Completed
Cases
Montfort Hospital 151 141
Pembroke Region 207 183
Winchester District and Memorial 125 153
The Ottawa Hospital 197 203
Cornwall Community Hospital 61 149
Champlain LHIN Average 182 190
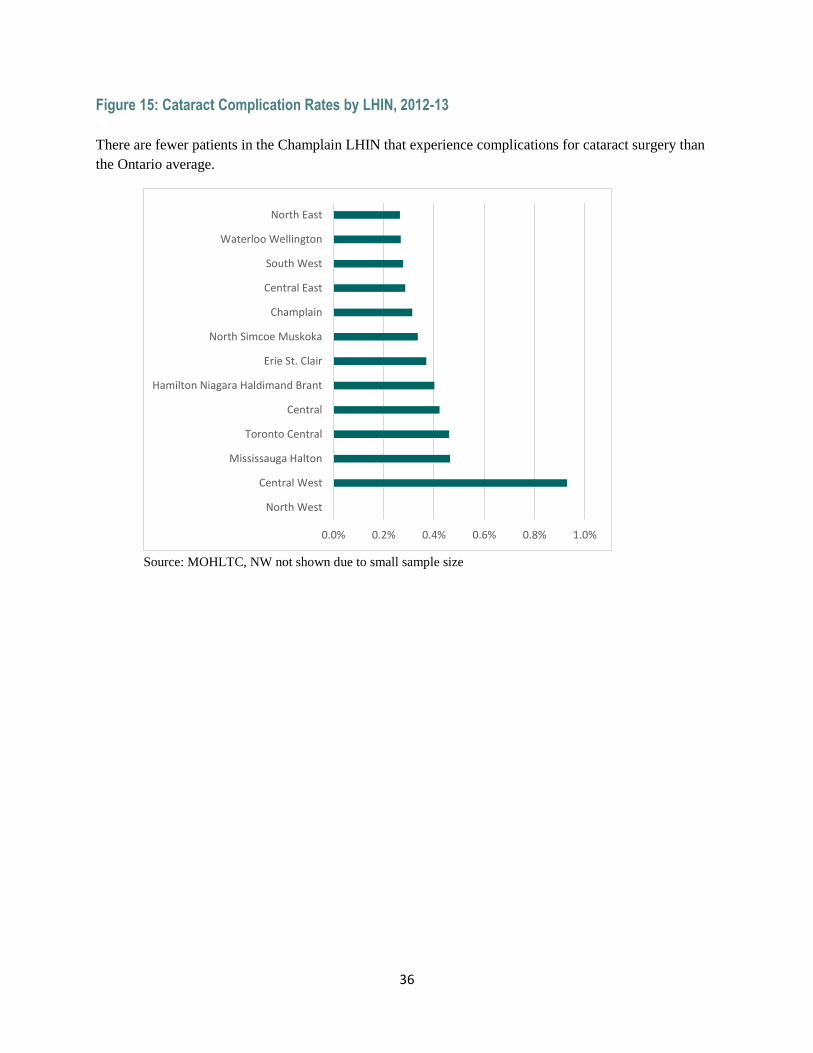
36
Figure 15: Cataract Complication Rates by LHIN, 2012-13
There are fewer patients in the Champlain LHIN that experience complications for cataract surgery than
the Ontario average.
Source: MOHLTC, NW not shown due to small sample size
0.0% 0.2% 0.4% 0.6% 0.8% 1.0%
North West
Central West
Mississauga Halton
Toronto Central
Central
Hamilton Niagara Haldimand Brant
Erie St. Clair
North Simcoe Muskoka
Champlain
Central East
South West
Waterloo Wellington
North East
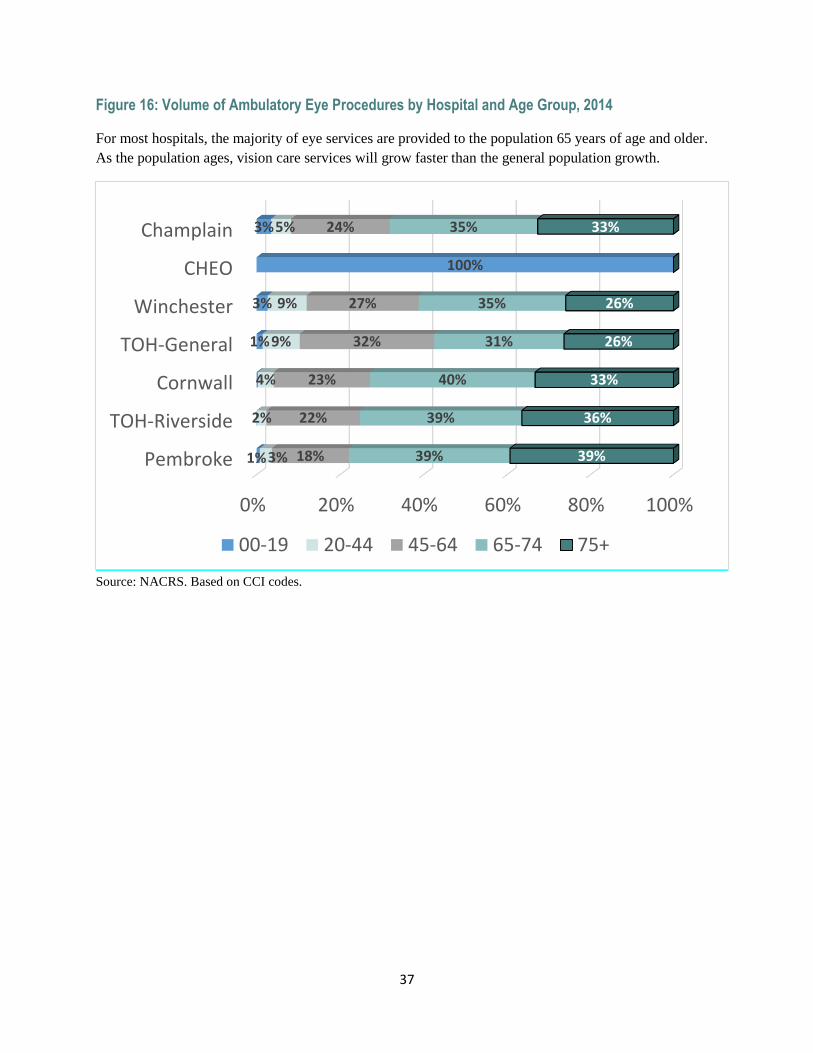
37
Figure 16: Volume of Ambulatory Eye Procedures by Hospital and Age Group, 2014
For most hospitals, the majority of eye services are provided to the population 65 years of age and older.
As the population ages, vision care services will grow faster than the general population growth.
Source: NACRS. Based on CCI codes.
0% 20% 40% 60% 80% 100%
Pembroke
TOH-Riverside
Cornwall
TOH-General
Winchester
CHEO
Champlain
1%
1%
3%
100%
3%
3%
2%
4%
9%
9%
5%
18%
22%
23%
32%
27%
24%
39%
39%
40%
31%
35%
35%
39%
36%
33%
26%
26%
33%
00-19 20-44 45-64 65-74 75+
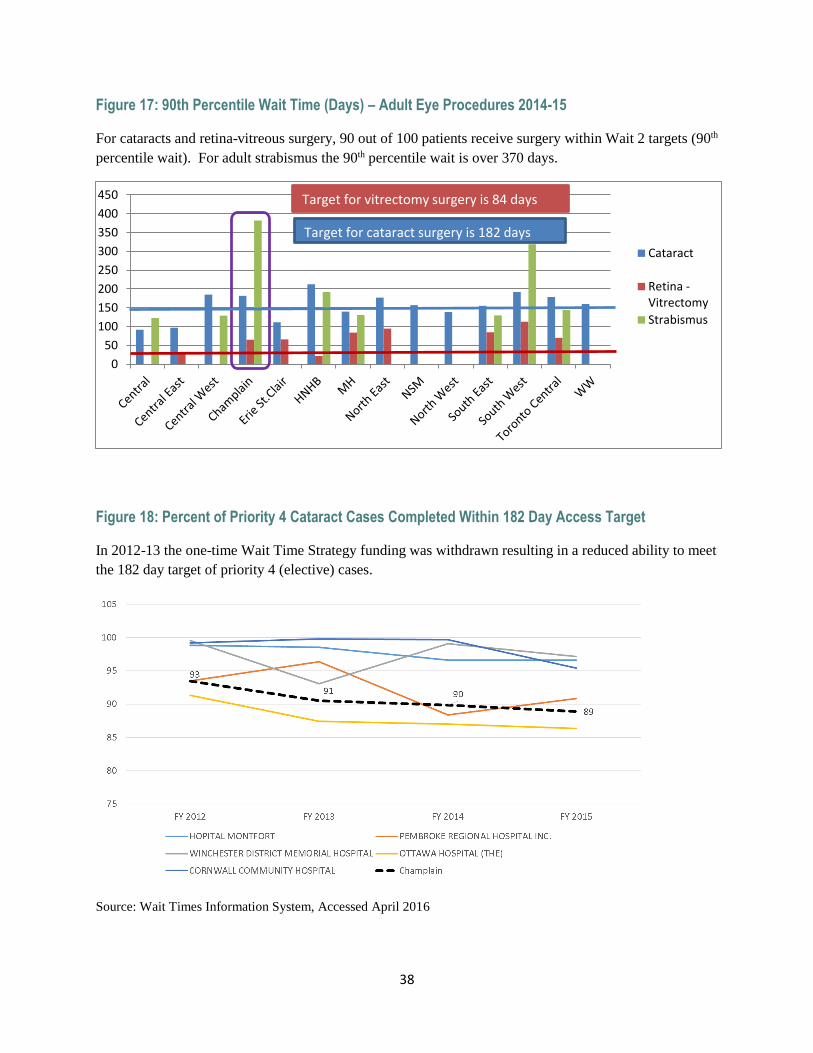
38
Figure 17: 90th Percentile Wait Time (Days) – Adult Eye Procedures 2014-15
For cataracts and retina-vitreous surgery, 90 out of 100 patients receive surgery within Wait 2 targets (90th
percentile wait). For adult strabismus the 90th percentile wait is over 370 days.
Figure 18: Percent of Priority 4 Cataract Cases Completed Within 182 Day Access Target
In 2012-13 the one-time Wait Time Strategy funding was withdrawn resulting in a reduced ability to meet
the 182 day target of priority 4 (elective) cases.
Source: Wait Times Information System, Accessed April 2016
0
50
100
150
200
250
300
350
400
450
Cataract
Retina -Vitrectomy
Strabismus
Target for cataract surgery is 182 days
Target for vitrectomy surgery is 84 days
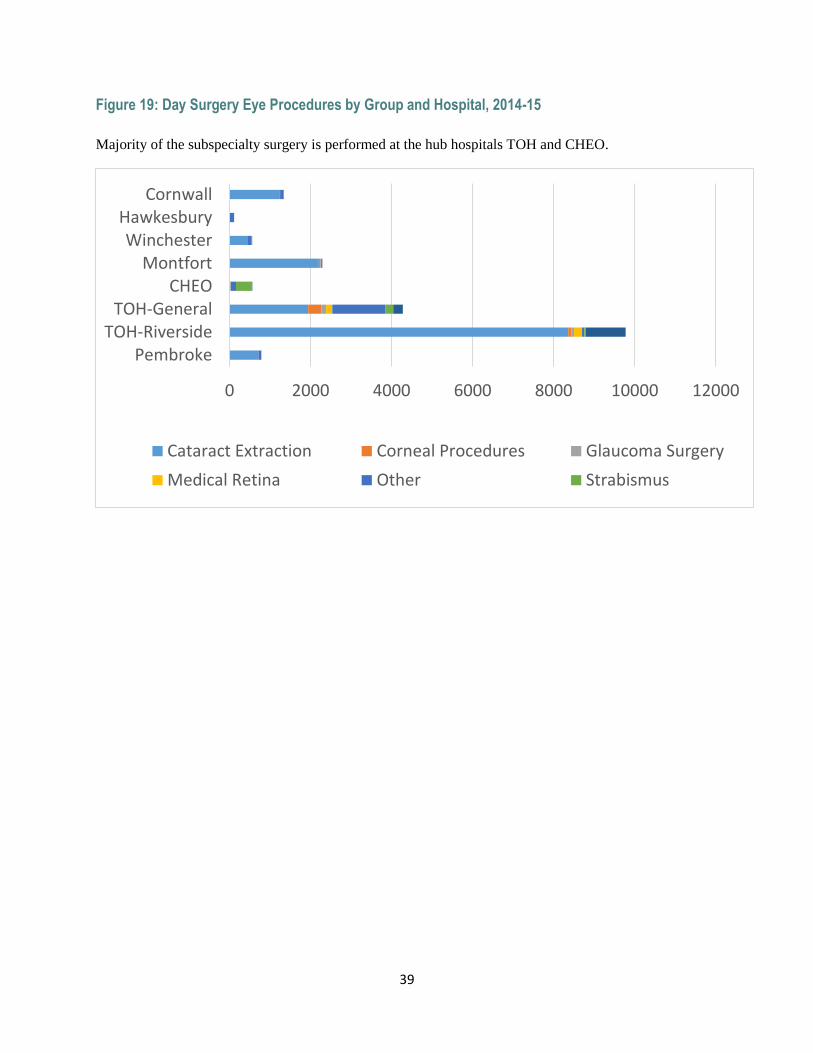
39
Figure 19: Day Surgery Eye Procedures by Group and Hospital, 2014-15
Majority of the subspecialty surgery is performed at the hub hospitals TOH and CHEO.
0 2000 4000 6000 8000 10000 12000
PembrokeTOH-Riverside
TOH-GeneralCHEO
MontfortWinchester
HawkesburyCornwall
Cataract Extraction Corneal Procedures Glaucoma Surgery
Medical Retina Other Strabismus
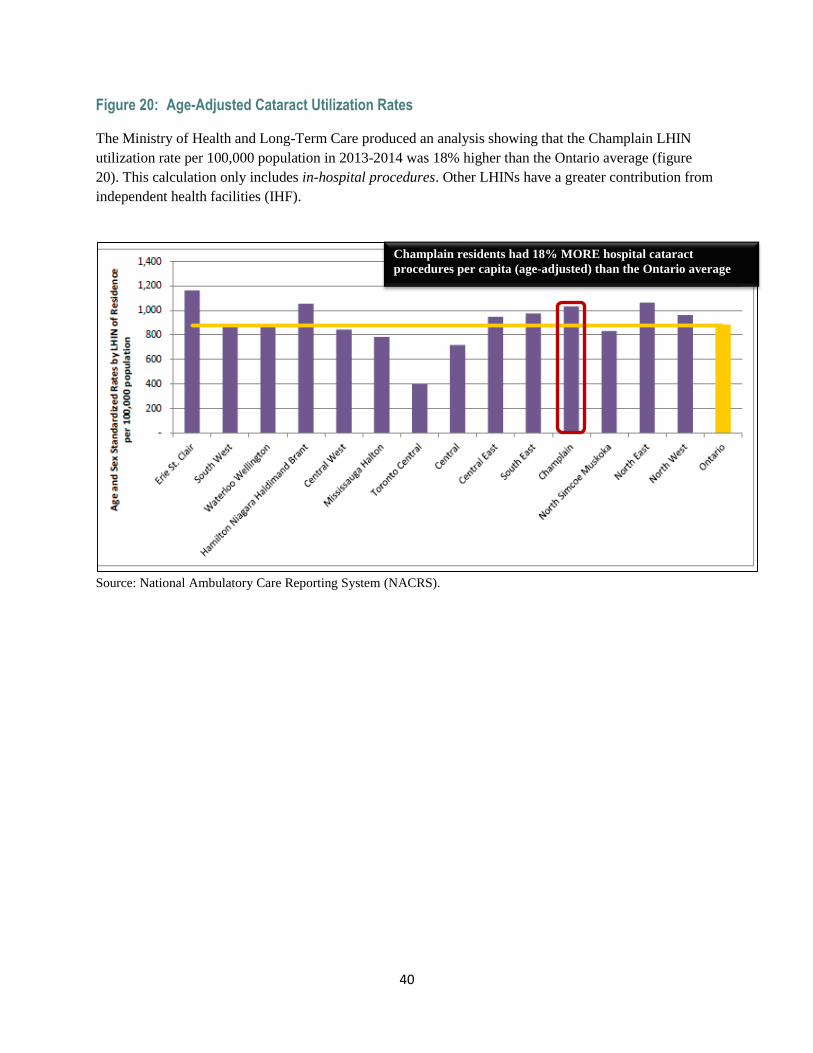
40
Figure 20: Age-Adjusted Cataract Utilization Rates
The Ministry of Health and Long-Term Care produced an analysis showing that the Champlain LHIN
utilization rate per 100,000 population in 2013-2014 was 18% higher than the Ontario average (figure
20). This calculation only includes in-hospital procedures. Other LHINs have a greater contribution from
independent health facilities (IHF).
Source: National Ambulatory Care Reporting System (NACRS).
Champlain residents had 18% MORE hospital cataract
procedures per capita (age-adjusted) than the Ontario average
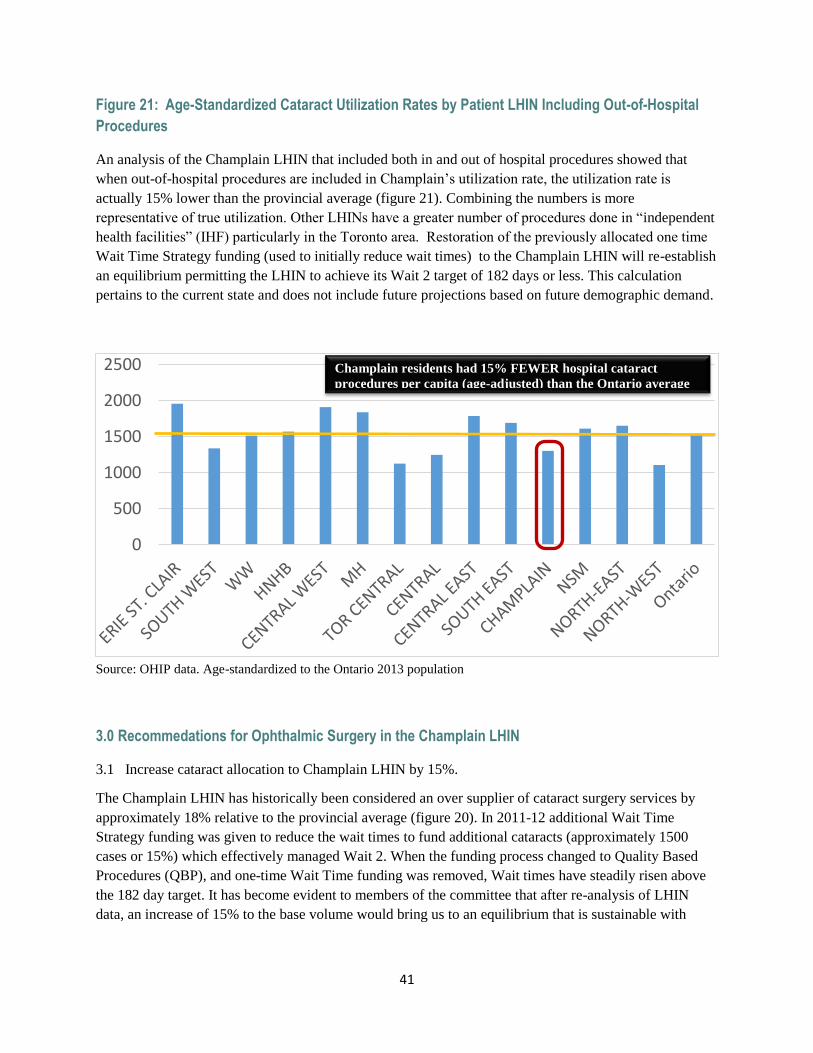
41
Figure 21: Age-Standardized Cataract Utilization Rates by Patient LHIN Including Out-of-Hospital
Procedures
An analysis of the Champlain LHIN that included both in and out of hospital procedures showed that
when out-of-hospital procedures are included in Champlain’s utilization rate, the utilization rate is
actually 15% lower than the provincial average (figure 21). Combining the numbers is more
representative of true utilization. Other LHINs have a greater number of procedures done in “independent
health facilities” (IHF) particularly in the Toronto area. Restoration of the previously allocated one time
Wait Time Strategy funding (used to initially reduce wait times) to the Champlain LHIN will re-establish
an equilibrium permitting the LHIN to achieve its Wait 2 target of 182 days or less. This calculation
pertains to the current state and does not include future projections based on future demographic demand.
Source: OHIP data. Age-standardized to the Ontario 2013 population
3.0 Recommedations for Ophthalmic Surgery in the Champlain LHIN
3.1 Increase cataract allocation to Champlain LHIN by 15%.
The Champlain LHIN has historically been considered an over supplier of cataract surgery services by
approximately 18% relative to the provincial average (figure 20). In 2011-12 additional Wait Time
Strategy funding was given to reduce the wait times to fund additional cataracts (approximately 1500
cases or 15%) which effectively managed Wait 2. When the funding process changed to Quality Based
Procedures (QBP), and one-time Wait Time funding was removed, Wait times have steadily risen above
the 182 day target. It has become evident to members of the committee that after re-analysis of LHIN
data, an increase of 15% to the base volume would bring us to an equilibrium that is sustainable with
0
500
1000
1500
2000
2500 Champlain residents had 15% FEWER hospital cataract
procedures per capita (age-adjusted) than the Ontario average
42
increases going forward based on demographic data. This calculation pertains to the current state and does
not include future projections based on future demographic demand.
The single queue model has been implemented in some clinical environments to reduce wait times with
patients being directed towards surgeons with the lowest wait times. At TOH orthopedic surgery has
found significant success utilizing this model. At TOH, the Eye Care Executive Committee reviews the
wait time data every two months and implements strategies to address challenges of outliers. The single
queue has been discussed within ophthalmology however currently it is felt that with an increased
allocation of 1500 cataract cases and additional resources going forward being based on demographic
projections that wait time targets will be easily achieved. In addition a cataract allocation model being
developed at TOH will have as a metric wait times with resources being directed towards those that
achieve their targets. We have also partially implemented restriction of inflow into individual practices to
manage wait times with some success. Providers have expressed concerns that the major issue with a
single queue model concerns the disruption of the patient/physician relationship. Many surgeons feel that
once they have engaged a patient it is their duty to continue to deliver care. By modifying inflow into
their practices the relationship is never established and thus cannot be disrupted. Overlying the single
queue model is a concern of patient choice. A single queue tends to commoditize the procedure and
surgeons within the Champlain LHIN are working towards alternative solutions as physician interest is
low in implementing the single queue.
Pediatric Ophthalmology
The vast majority of pediatric ophthalmic services for the Champlain LHIN are centered at the CHEO.
See Providers (page 23) for description of CHEO pediatric ophthalmology services. Over the last few
decades, there has been a shift in the pattern in the delivery of care by general ophthalmologists in the
provision of care to children in large urban centres such as Ottawa. With the opening of CHEO in 1974
and the creation of a center of excellence for pediatric ophthalmology, many ophthalmologists began
reducing or eliminating children from their practices as they took on a heavier burden with the needs of an
aging population.(e.g. cataract surgery). Family physicians and optometrists began referring directly to
pediatric ophthalmologists and this continues to this day. These changes in the practice patterns of general
ophthalmologists with regards to the pediatric population have led to exceedingly long Wait 1 and Wait 2.
The neighbouring Outaouais region has one of the highest birth rates in Quebec. Our Wait 1 and Wait 2
metrics are directly impacted by the number of Quebec patients waiting for ophthalmology care at CHEO.
These children and their families would otherwise have to travel to Montreal for secondary, tertiary and
quaternary pediatric ophthalmology care.
The Wait 1 for pediatric services in the Champlain LHIN is by far the longest in Ontario, approaching 18
months. Over the years, there have been some attempts made in Ottawa to encourage general
ophthalmologists to see children. However, the provincial Wait Time’s initiative for cataract surgery has
shifted the focus of ophthalmologists to providing cataract care, with the unintended consequence of
decreasing their ability to care for patients with other eye diseases, especially children, who present
specific challenges in their assessment. Ophthalmologists in Cornwall and Pembroke continue to see
pediatric patients.
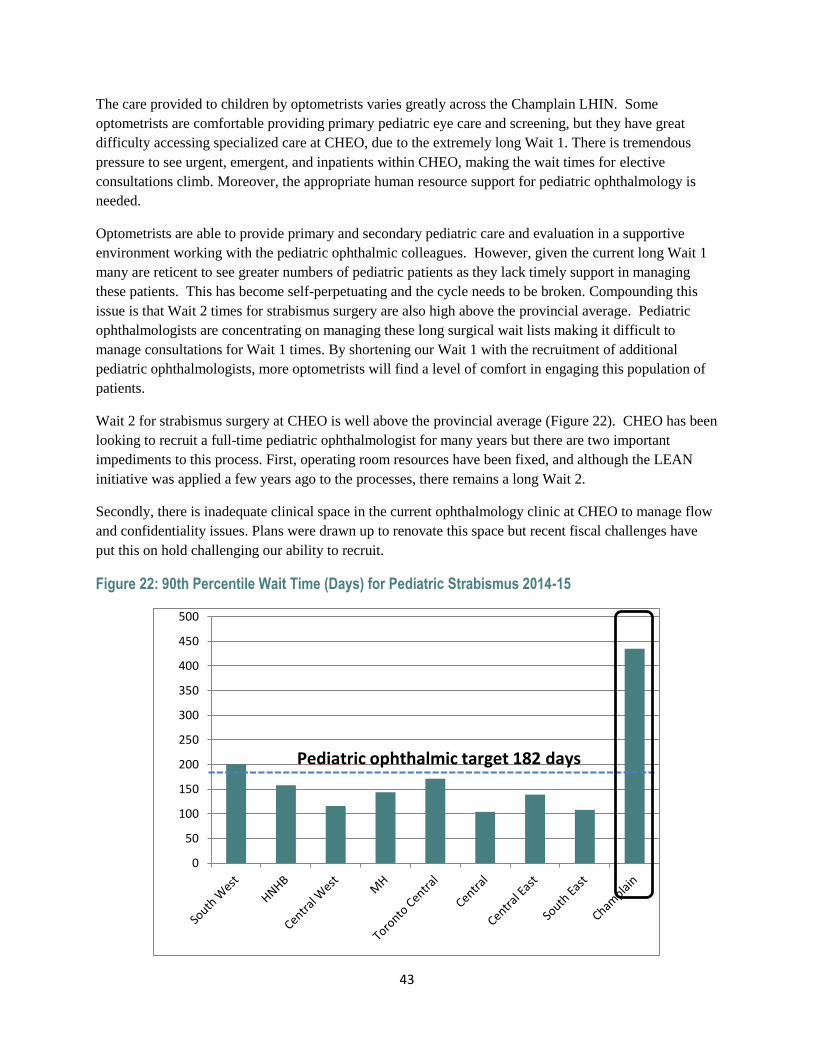
43
The care provided to children by optometrists varies greatly across the Champlain LHIN. Some
optometrists are comfortable providing primary pediatric eye care and screening, but they have great
difficulty accessing specialized care at CHEO, due to the extremely long Wait 1. There is tremendous
pressure to see urgent, emergent, and inpatients within CHEO, making the wait times for elective
consultations climb. Moreover, the appropriate human resource support for pediatric ophthalmology is
needed.
Optometrists are able to provide primary and secondary pediatric care and evaluation in a supportive
environment working with the pediatric ophthalmic colleagues. However, given the current long Wait 1
many are reticent to see greater numbers of pediatric patients as they lack timely support in managing
these patients. This has become self-perpetuating and the cycle needs to be broken. Compounding this
issue is that Wait 2 times for strabismus surgery are also high above the provincial average. Pediatric
ophthalmologists are concentrating on managing these long surgical wait lists making it difficult to
manage consultations for Wait 1 times. By shortening our Wait 1 with the recruitment of additional
pediatric ophthalmologists, more optometrists will find a level of comfort in engaging this population of
patients.
Wait 2 for strabismus surgery at CHEO is well above the provincial average (Figure 22). CHEO has been
looking to recruit a full-time pediatric ophthalmologist for many years but there are two important
impediments to this process. First, operating room resources have been fixed, and although the LEAN
initiative was applied a few years ago to the processes, there remains a long Wait 2.
Secondly, there is inadequate clinical space in the current ophthalmology clinic at CHEO to manage flow
and confidentiality issues. Plans were drawn up to renovate this space but recent fiscal challenges have
put this on hold challenging our ability to recruit.
Figure 22: 90th Percentile Wait Time (Days) for Pediatric Strabismus 2014-15
0
50
100
150
200
250
300
350
400
450
500
Pediatric ophthalmic target 182 days
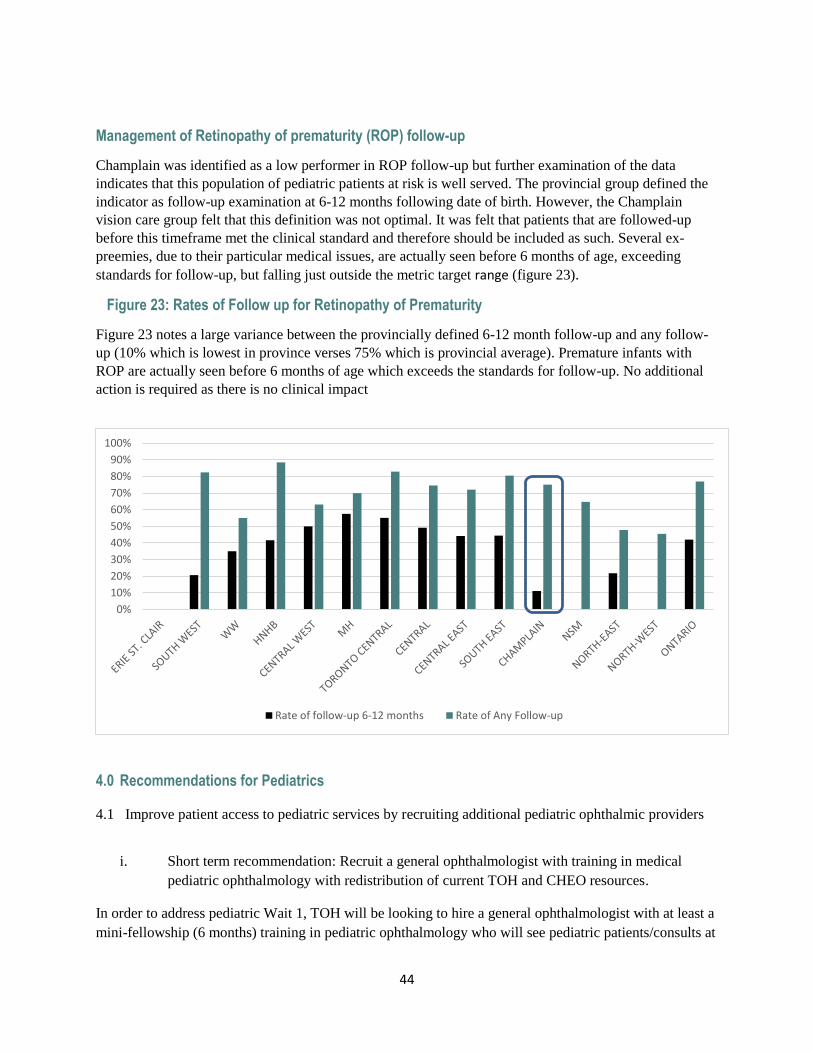
44
Management of Retinopathy of prematurity (ROP) follow-up
Champlain was identified as a low performer in ROP follow-up but further examination of the data
indicates that this population of pediatric patients at risk is well served. The provincial group defined the
indicator as follow-up examination at 6-12 months following date of birth. However, the Champlain
vision care group felt that this definition was not optimal. It was felt that patients that are followed-up
before this timeframe met the clinical standard and therefore should be included as such. Several ex-
preemies, due to their particular medical issues, are actually seen before 6 months of age, exceeding
standards for follow-up, but falling just outside the metric target range (figure 23).
Figure 23: Rates of Follow up for Retinopathy of Prematurity
Figure 23 notes a large variance between the provincially defined 6-12 month follow-up and any follow-
up (10% which is lowest in province verses 75% which is provincial average). Premature infants with
ROP are actually seen before 6 months of age which exceeds the standards for follow-up. No additional
action is required as there is no clinical impact
4.0 Recommendations for Pediatrics
4.1 Improve patient access to pediatric services by recruiting additional pediatric ophthalmic providers
i. Short term recommendation: Recruit a general ophthalmologist with training in medical
pediatric ophthalmology with redistribution of current TOH and CHEO resources.
In order to address pediatric Wait 1, TOH will be looking to hire a general ophthalmologist with at least a
mini-fellowship (6 months) training in pediatric ophthalmology who will see pediatric patients/consults at
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Rate of follow-up 6-12 months Rate of Any Follow-up
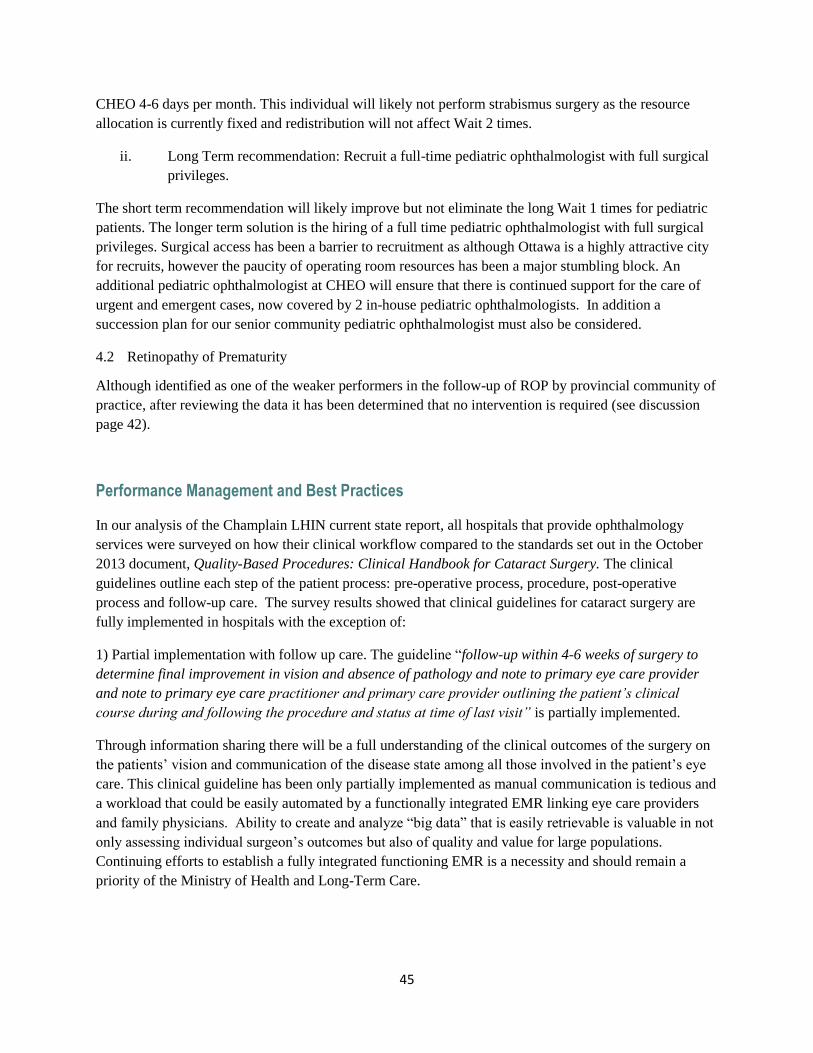
45
CHEO 4-6 days per month. This individual will likely not perform strabismus surgery as the resource
allocation is currently fixed and redistribution will not affect Wait 2 times.
ii. Long Term recommendation: Recruit a full-time pediatric ophthalmologist with full surgical
privileges.
The short term recommendation will likely improve but not eliminate the long Wait 1 times for pediatric
patients. The longer term solution is the hiring of a full time pediatric ophthalmologist with full surgical
privileges. Surgical access has been a barrier to recruitment as although Ottawa is a highly attractive city
for recruits, however the paucity of operating room resources has been a major stumbling block. An
additional pediatric ophthalmologist at CHEO will ensure that there is continued support for the care of
urgent and emergent cases, now covered by 2 in-house pediatric ophthalmologists. In addition a
succession plan for our senior community pediatric ophthalmologist must also be considered.
4.2 Retinopathy of Prematurity
Although identified as one of the weaker performers in the follow-up of ROP by provincial community of
practice, after reviewing the data it has been determined that no intervention is required (see discussion
page 42).
Performance Management and Best Practices
In our analysis of the Champlain LHIN current state report, all hospitals that provide ophthalmology
services were surveyed on how their clinical workflow compared to the standards set out in the October
2013 document, Quality-Based Procedures: Clinical Handbook for Cataract Surgery. The clinical
guidelines outline each step of the patient process: pre-operative process, procedure, post-operative
process and follow-up care. The survey results showed that clinical guidelines for cataract surgery are
fully implemented in hospitals with the exception of:
1) Partial implementation with follow up care. The guideline “follow-up within 4-6 weeks of surgery to
determine final improvement in vision and absence of pathology and note to primary eye care provider
and note to primary eye care practitioner and primary care provider outlining the patient’s clinical
course during and following the procedure and status at time of last visit” is partially implemented.
Through information sharing there will be a full understanding of the clinical outcomes of the surgery on
the patients’ vision and communication of the disease state among all those involved in the patient’s eye
care. This clinical guideline has been only partially implemented as manual communication is tedious and
a workload that could be easily automated by a functionally integrated EMR linking eye care providers
and family physicians. Ability to create and analyze “big data” that is easily retrievable is valuable in not
only assessing individual surgeon’s outcomes but also of quality and value for large populations.
Continuing efforts to establish a fully integrated functioning EMR is a necessity and should remain a
priority of the Ministry of Health and Long-Term Care.
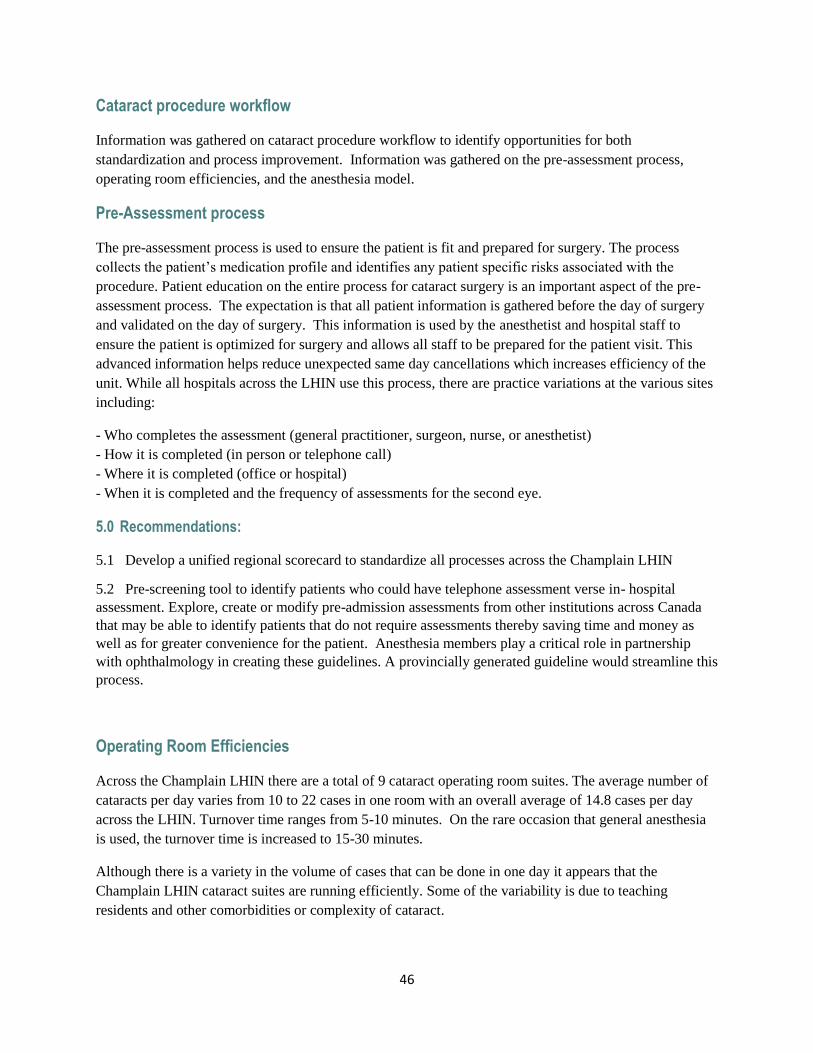
46
Cataract procedure workflow
Information was gathered on cataract procedure workflow to identify opportunities for both
standardization and process improvement. Information was gathered on the pre-assessment process,
operating room efficiencies, and the anesthesia model.
Pre-Assessment process
The pre-assessment process is used to ensure the patient is fit and prepared for surgery. The process
collects the patient’s medication profile and identifies any patient specific risks associated with the
procedure. Patient education on the entire process for cataract surgery is an important aspect of the pre-
assessment process. The expectation is that all patient information is gathered before the day of surgery
and validated on the day of surgery. This information is used by the anesthetist and hospital staff to
ensure the patient is optimized for surgery and allows all staff to be prepared for the patient visit. This
advanced information helps reduce unexpected same day cancellations which increases efficiency of the
unit. While all hospitals across the LHIN use this process, there are practice variations at the various sites
including:
- Who completes the assessment (general practitioner, surgeon, nurse, or anesthetist)
- How it is completed (in person or telephone call)
- Where it is completed (office or hospital)
- When it is completed and the frequency of assessments for the second eye.
5.0 Recommendations:
5.1 Develop a unified regional scorecard to standardize all processes across the Champlain LHIN
5.2 Pre-screening tool to identify patients who could have telephone assessment verse in- hospital
assessment. Explore, create or modify pre-admission assessments from other institutions across Canada
that may be able to identify patients that do not require assessments thereby saving time and money as
well as for greater convenience for the patient. Anesthesia members play a critical role in partnership
with ophthalmology in creating these guidelines. A provincially generated guideline would streamline this
process.
Operating Room Efficiencies
Across the Champlain LHIN there are a total of 9 cataract operating room suites. The average number of
cataracts per day varies from 10 to 22 cases in one room with an overall average of 14.8 cases per day
across the LHIN. Turnover time ranges from 5-10 minutes. On the rare occasion that general anesthesia
is used, the turnover time is increased to 15-30 minutes.
Although there is a variety in the volume of cases that can be done in one day it appears that the
Champlain LHIN cataract suites are running efficiently. Some of the variability is due to teaching
residents and other comorbidities or complexity of cataract.
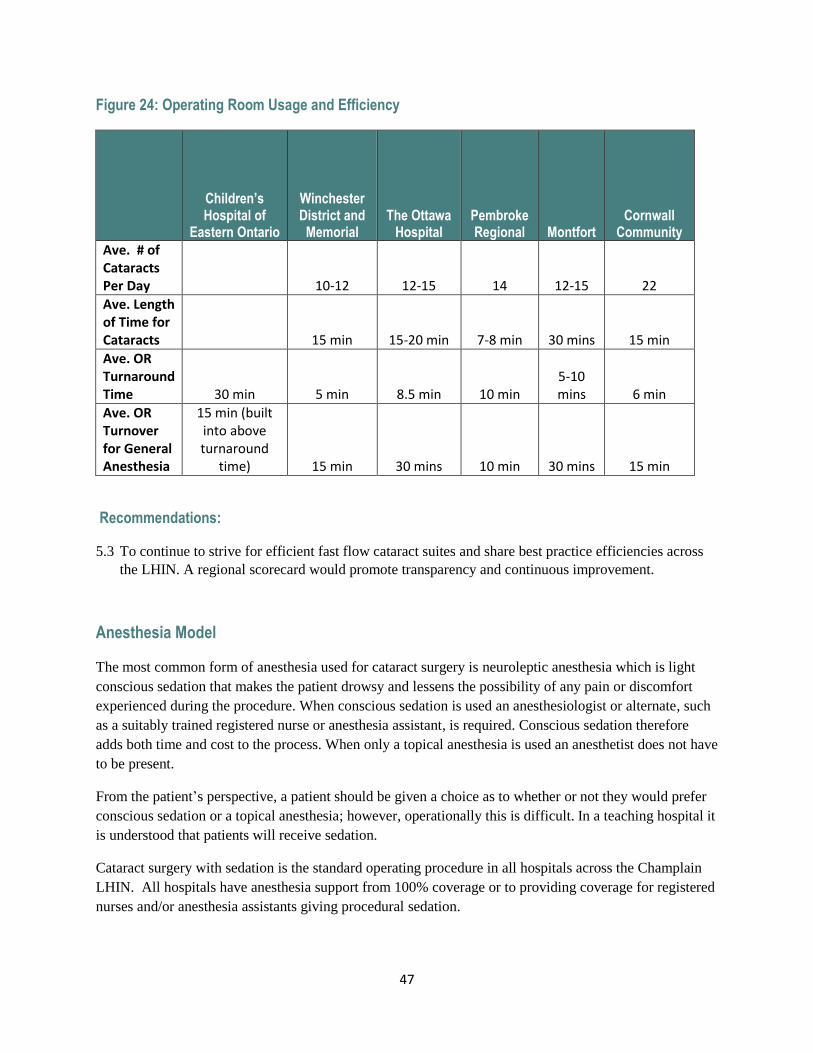
47
Figure 24: Operating Room Usage and Efficiency
Children’s Hospital of
Eastern Ontario
Winchester District and
Memorial The Ottawa
Hospital Pembroke Regional Montfort
Cornwall Community
Ave. # of Cataracts Per Day 10-12 12-15 14 12-15 22
Ave. Length of Time for Cataracts 15 min 15-20 min 7-8 min 30 mins 15 min
Ave. OR Turnaround Time 30 min 5 min 8.5 min 10 min
5-10 mins 6 min
Ave. OR Turnover for General Anesthesia
15 min (built into above turnaround
time) 15 min 30 mins 10 min 30 mins 15 min
Recommendations:
5.3 To continue to strive for efficient fast flow cataract suites and share best practice efficiencies across
the LHIN. A regional scorecard would promote transparency and continuous improvement.
Anesthesia Model
The most common form of anesthesia used for cataract surgery is neuroleptic anesthesia which is light
conscious sedation that makes the patient drowsy and lessens the possibility of any pain or discomfort
experienced during the procedure. When conscious sedation is used an anesthesiologist or alternate, such
as a suitably trained registered nurse or anesthesia assistant, is required. Conscious sedation therefore
adds both time and cost to the process. When only a topical anesthesia is used an anesthetist does not have
to be present.
From the patient’s perspective, a patient should be given a choice as to whether or not they would prefer
conscious sedation or a topical anesthesia; however, operationally this is difficult. In a teaching hospital it
is understood that patients will receive sedation.
Cataract surgery with sedation is the standard operating procedure in all hospitals across the Champlain
LHIN. All hospitals have anesthesia support from 100% coverage or to providing coverage for registered
nurses and/or anesthesia assistants giving procedural sedation.

48
Recommendations:
5.4 To ensure that in hospitals where sedation is the standard operating procedure, ophthalmologists are
able to not use sedation during cataract surgery when it is determined to be in the best interest of the
patient.
5.5 Ensure that when sedation is being used that the current Ontario Medical Association A Sedation
Standards for Uncomplicated Cataract Surgery under Topical Anesthesia are reviewed.
Quality Indicators
Cataract surgery is currently lacking a clinical outcome measure that is robust and applicable to all types
of cataract surgery. There are many indications for cataract surgery depending on the patients underlying
disease which makes measuring outcomes difficult.
Cataract complication rates for the Champlain LHIN in 2015 were 0.3% (figure 16). Rates of post-
operative endophthalmitis are tracked at TOH through the Department of Ophthalmology as well as
through the Department of Infection Control. With the integrated retina service at one site (TOH) all
cases of endophthalmitis within the Champlain LHIN are referred to the retina service for follow up and
treatment. This integrated system facilitates the tracking and reporting of endophthalmitis. The number of
endophthalmitis cases is reported and tracked by Infection Control at TOH who alert the department if
any clusters of endophthalmitis are apparent. This is critical in alerting leadership as to breaches or
inappropriate processes in place.
Systems vary for tracking capsular breakages or other complications across the LHIN. There is no formal
method in place. Most hospitals rely on physician feedback, self-reporting and patient complaints.
Capsular breakage rates at TOH are recorded and the data is used internally as a quality initiative. It also
is used to confirm that resident teaching is safe for patients.
TOH has the most rigorous reporting system for adverse events and patient safety in the LHIN. Data is
collected on return to operating room within 24 hours as well as compliance to the Surgical Safety Check
List and near misses. Near misses, where the surgical safety check captures an error, is used for teaching,
coaching and verification of the validity of the process.
At TOH the Department presents regularly to the Patient Safety and Quality Committee on the following:
- Endophthalmitis rate
- Toxic Anterior Segment Syndrome (TASS)
- Capsular Breakage Rates
- Surgical Safety Checklist
Recommendation:
5.6 Develop a unified regional scorecard to standardize all processes across the Champlain LHIN. This
will enable all stakeholders to know best clinical practices are being followed and outcomes are
reported. Sharing of best practices amongst constituent members of the LHIN is strongly encouraged

49
and provincial or national indicators should be standardized. The measurement of clinical
performance indicators will demonstrate that all providers of cataract surgery are offering quality
procedures with positive outcomes
Patient Satisfaction
Patient satisfaction data is collected in a variety of ways across the Champlain LHIN. There is not a
specific patient satisfaction survey for all to use after cataract surgery. Three of the hospitals use NRC
Picker for patient satisfaction scores. Other hospitals have informal processes such as patient comment
cards, rounding on patients and one hospital has a web site that provides the opportunity to patients to
send in a compliment or complaint.
The Patient Satisfaction Scorecard 2013-2014 for TOH for the Eye Care program was 71% excellent in
overall rating of care. TOH recently implemented post-op calls to cataract patients when possible
(approximately 50% of the time). Nurses in the day care unit will call the patients to ensure they
understand their instructions, have filled their eye drop prescription and ask them how their care was.
Patients and family have expressed their appreciation for this service.
Recommendation:
5.7 A standardized province-wide cataract surgery patient satisfaction survey.
See Proposed Cataract Patient Satisfaction Survey in Appendix 1.4
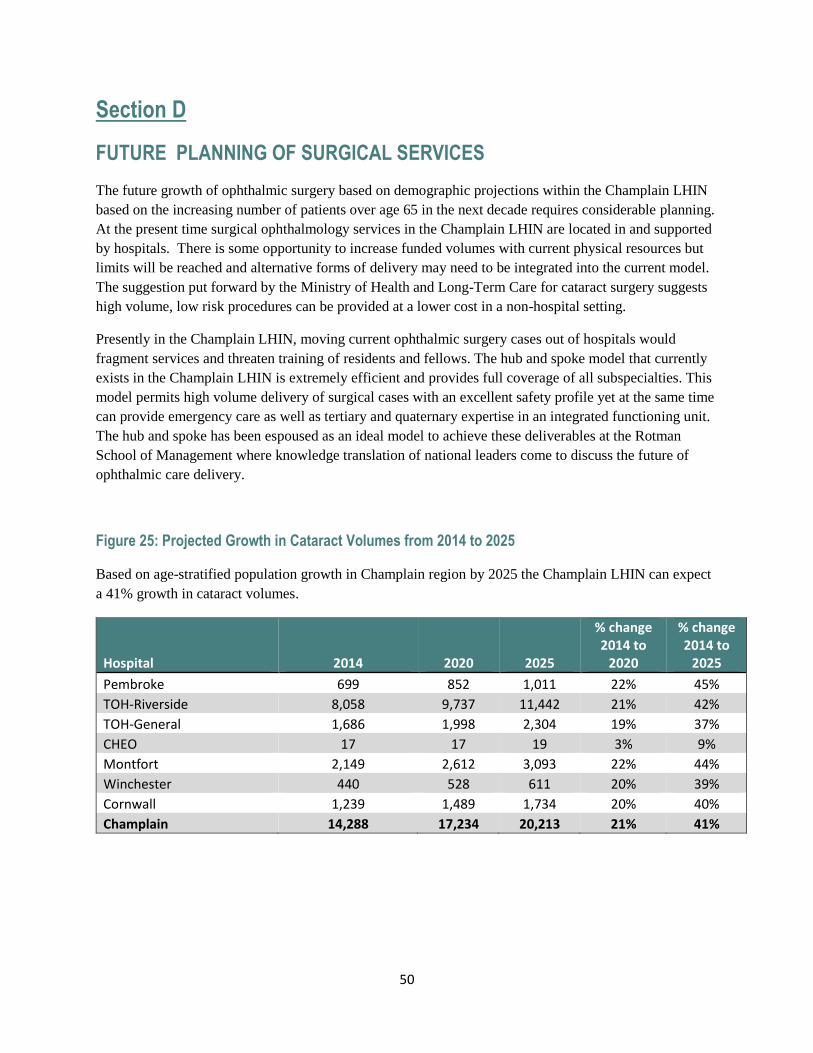
50
Section D
FUTURE PLANNING OF SURGICAL SERVICES
The future growth of ophthalmic surgery based on demographic projections within the Champlain LHIN
based on the increasing number of patients over age 65 in the next decade requires considerable planning.
At the present time surgical ophthalmology services in the Champlain LHIN are located in and supported
by hospitals. There is some opportunity to increase funded volumes with current physical resources but
limits will be reached and alternative forms of delivery may need to be integrated into the current model.
The suggestion put forward by the Ministry of Health and Long-Term Care for cataract surgery suggests
high volume, low risk procedures can be provided at a lower cost in a non-hospital setting.
Presently in the Champlain LHIN, moving current ophthalmic surgery cases out of hospitals would
fragment services and threaten training of residents and fellows. The hub and spoke model that currently
exists in the Champlain LHIN is extremely efficient and provides full coverage of all subspecialties. This
model permits high volume delivery of surgical cases with an excellent safety profile yet at the same time
can provide emergency care as well as tertiary and quaternary expertise in an integrated functioning unit.
The hub and spoke has been espoused as an ideal model to achieve these deliverables at the Rotman
School of Management where knowledge translation of national leaders come to discuss the future of
ophthalmic care delivery.
Figure 25: Projected Growth in Cataract Volumes from 2014 to 2025
Based on age-stratified population growth in Champlain region by 2025 the Champlain LHIN can expect
a 41% growth in cataract volumes.
Hospital 2014 2020 2025
% change 2014 to
2020
% change 2014 to
2025
Pembroke 699 852 1,011 22% 45%
TOH-Riverside 8,058 9,737 11,442 21% 42%
TOH-General 1,686 1,998 2,304 19% 37%
CHEO 17 17 19 3% 9%
Montfort 2,149 2,612 3,093 22% 44%
Winchester 440 528 611 20% 39%
Cornwall 1,239 1,489 1,734 20% 40%
Champlain 14,288 17,234 20,213 21% 41%
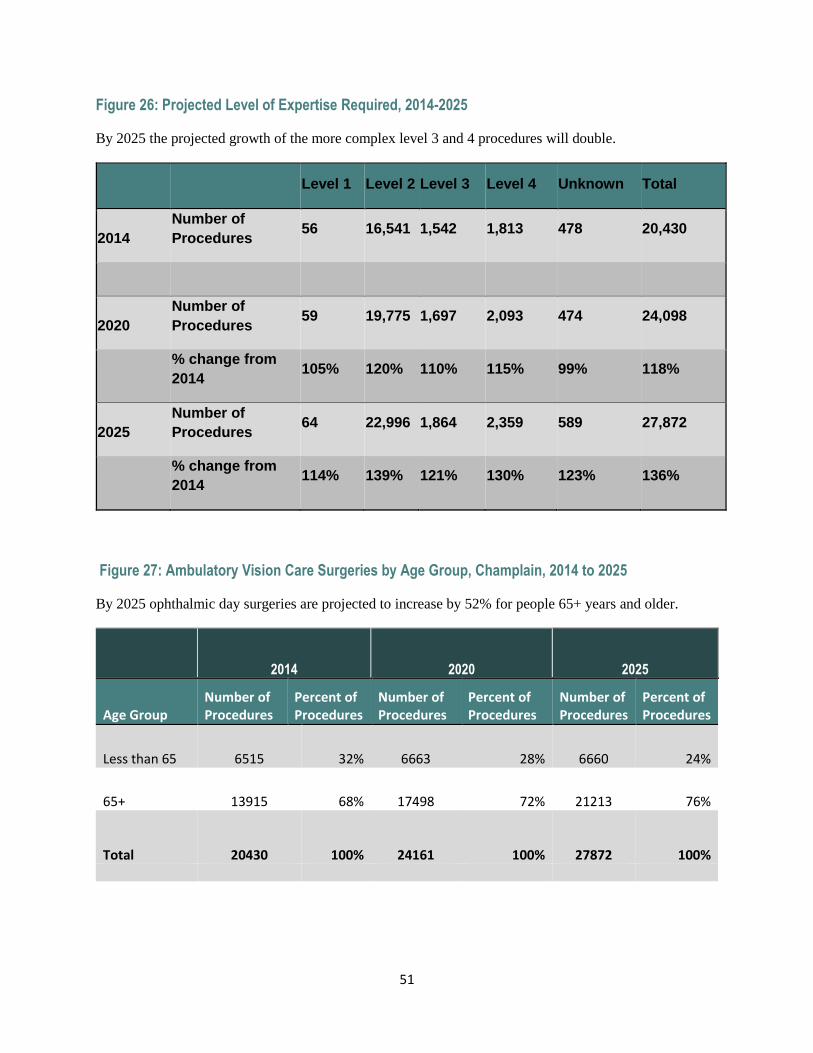
51
Figure 26: Projected Level of Expertise Required, 2014-2025
By 2025 the projected growth of the more complex level 3 and 4 procedures will double.
Level 1 Level 2 Level 3 Level 4 Unknown Total
2014
Number of
Procedures 56 16,541 1,542 1,813 478 20,430
2020
Number of
Procedures 59 19,775 1,697 2,093 474 24,098
% change from
2014 105% 120% 110% 115% 99% 118%
2025
Number of
Procedures 64 22,996 1,864 2,359 589 27,872
% change from
2014 114% 139% 121% 130% 123% 136%
Figure 27: Ambulatory Vision Care Surgeries by Age Group, Champlain, 2014 to 2025
By 2025 ophthalmic day surgeries are projected to increase by 52% for people 65+ years and older.
2014 2020 2025
Age Group Number of Procedures
Percent of Procedures
Number of Procedures
Percent of Procedures
Number of Procedures
Percent of Procedures
Less than 65 6515 32% 6663 28% 6660 24%
65+ 13915 68% 17498 72% 21213 76%
Total 20430 100% 24161 100% 27872 100%
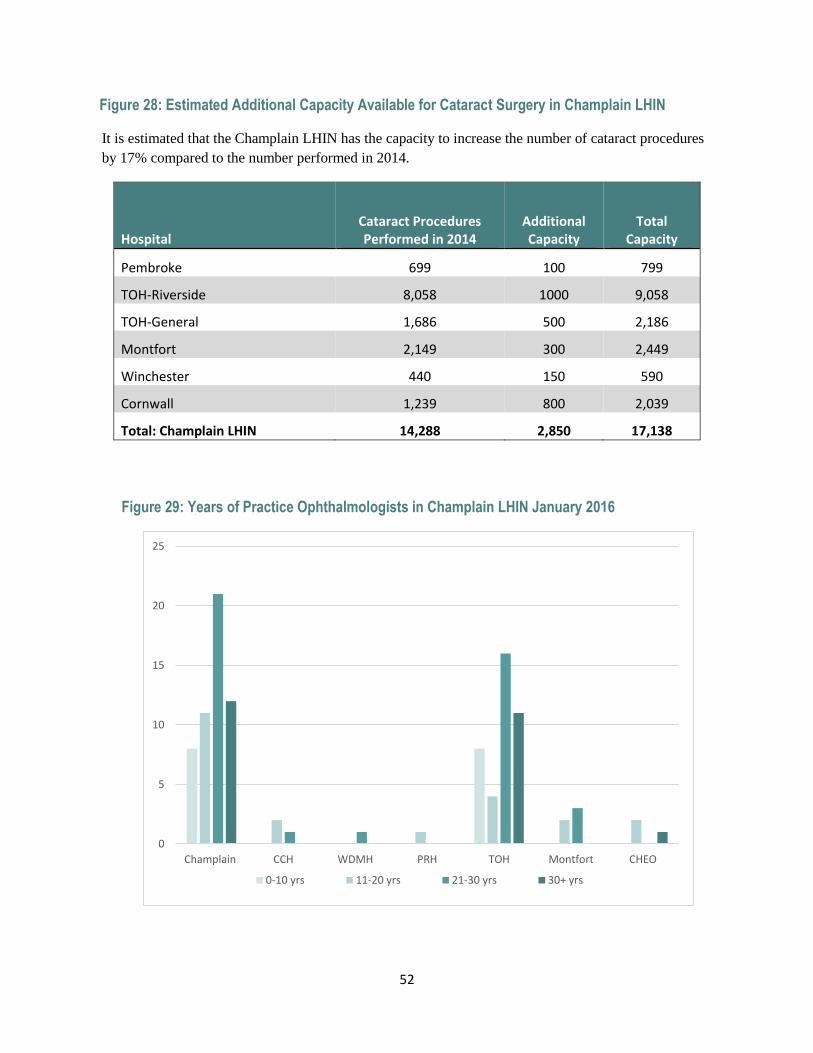
52
Figure 28: Estimated Additional Capacity Available for Cataract Surgery in Champlain LHIN
It is estimated that the Champlain LHIN has the capacity to increase the number of cataract procedures
by 17% compared to the number performed in 2014.
Hospital Cataract Procedures Performed in 2014
Additional Capacity
Total Capacity
Pembroke 699 100 799
TOH-Riverside 8,058 1000 9,058
TOH-General 1,686 500 2,186
Montfort 2,149 300 2,449
Winchester 440 150 590
Cornwall 1,239 800 2,039
Total: Champlain LHIN 14,288 2,850 17,138
Figure 29: Years of Practice Ophthalmologists in Champlain LHIN January 2016
0
5
10
15
20
25
Champlain CCH WDMH PRH TOH Montfort CHEO
0-10 yrs 11-20 yrs 21-30 yrs 30+ yrs
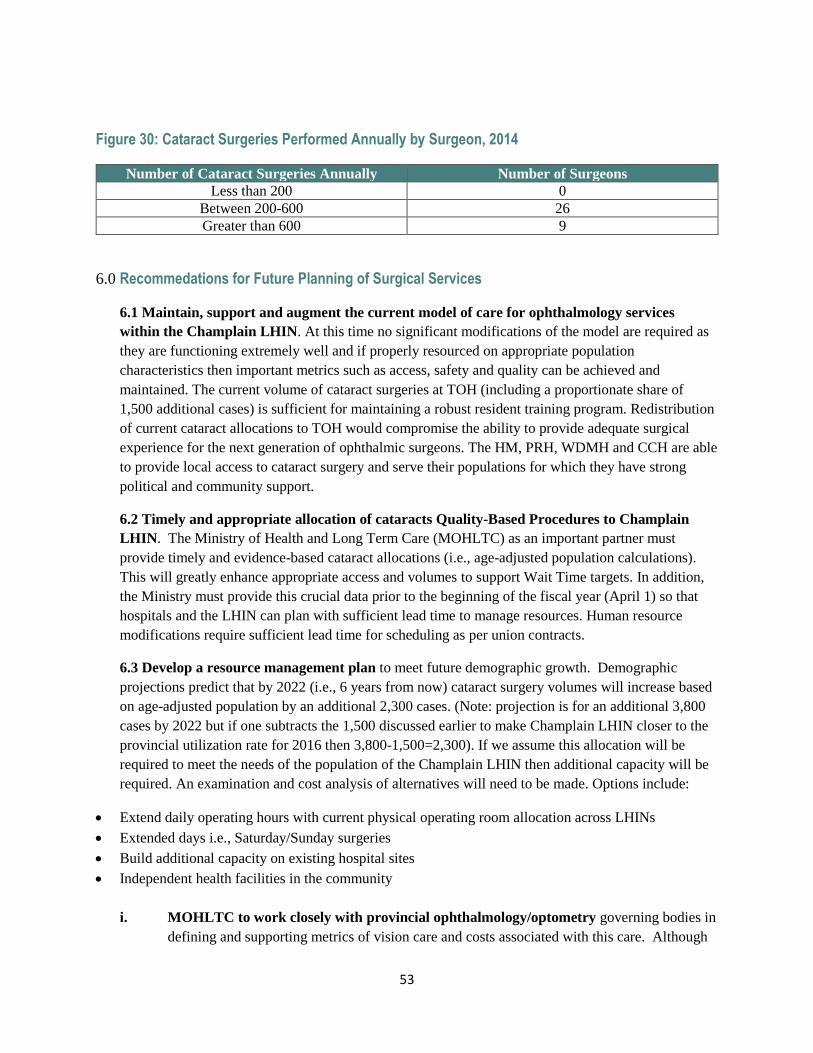
53
Figure 30: Cataract Surgeries Performed Annually by Surgeon, 2014
Number of Cataract Surgeries Annually Number of Surgeons
Less than 200 0
Between 200-600 26
Greater than 600 9
6.0 Recommedations for Future Planning of Surgical Services
6.1 Maintain, support and augment the current model of care for ophthalmology services
within the Champlain LHIN. At this time no significant modifications of the model are required as
they are functioning extremely well and if properly resourced on appropriate population
characteristics then important metrics such as access, safety and quality can be achieved and
maintained. The current volume of cataract surgeries at TOH (including a proportionate share of
1,500 additional cases) is sufficient for maintaining a robust resident training program. Redistribution
of current cataract allocations to TOH would compromise the ability to provide adequate surgical
experience for the next generation of ophthalmic surgeons. The HM, PRH, WDMH and CCH are able
to provide local access to cataract surgery and serve their populations for which they have strong
political and community support.
6.2 Timely and appropriate allocation of cataracts Quality-Based Procedures to Champlain
LHIN. The Ministry of Health and Long Term Care (MOHLTC) as an important partner must
provide timely and evidence-based cataract allocations (i.e., age-adjusted population calculations).
This will greatly enhance appropriate access and volumes to support Wait Time targets. In addition,
the Ministry must provide this crucial data prior to the beginning of the fiscal year (April 1) so that
hospitals and the LHIN can plan with sufficient lead time to manage resources. Human resource
modifications require sufficient lead time for scheduling as per union contracts.
6.3 Develop a resource management plan to meet future demographic growth. Demographic
projections predict that by 2022 (i.e., 6 years from now) cataract surgery volumes will increase based
on age-adjusted population by an additional 2,300 cases. (Note: projection is for an additional 3,800
cases by 2022 but if one subtracts the 1,500 discussed earlier to make Champlain LHIN closer to the
provincial utilization rate for 2016 then 3,800-1,500=2,300). If we assume this allocation will be
required to meet the needs of the population of the Champlain LHIN then additional capacity will be
required. An examination and cost analysis of alternatives will need to be made. Options include:
Extend daily operating hours with current physical operating room allocation across LHINs
Extended days i.e., Saturday/Sunday surgeries
Build additional capacity on existing hospital sites
Independent health facilities in the community
i. MOHLTC to work closely with provincial ophthalmology/optometry governing bodies in
defining and supporting metrics of vision care and costs associated with this care. Although
54
politically challenging the definition of a “medically necessary cataract” is critical in a world
with declining resources. The MOHLTC and ophthalmology/optometry governing bodies
need to define what services can be rendered with charges to the patient and guidelines to the
pricing to protect the public good. If future services are to be provided in the community such
as in an independent health facility then concrete guidelines are required to protect not only
the public from costs but also the physician and his/her employees from the burden of
transferring this financial risk from hospital to the community surgical environment. Stability
and predictability of facility funding is key so that surgeons can reliably predict success to
encourage potential transitions into an independent health facility model of care and preserve
the tenants of access, safety and quality.
6.4 Succession Planning: There are 12 ophthalmologists in the region that have more than 30 years of
experience. Hospitals should ensure that succession plans are established (figure 29).
i. Cataract Allocation Model: The Ontario Vision Strategy Task Force has recommended
guidelines of minimum 200 and maximum 600 cataracts per performed annually. The
minimum is to maintain surgical skill and the maximum to consider distribution to recent
graduates. These guidelines are difficult to achieve in the current environment however TOH
is embarking on development of an allocation policy based on academic and hospital metrics
that will shift resources based on these contributions. It presents an opportunity to manage
operating room resources to recruit surgeons in Ottawa (figure 30).
55
Section E
STAKEHOLDER ENGAGEMENT
Our Vision Care Network team identified key stakeholders for the development of the Champlain LHIN
Vision Plan. Our Vision Care Stakeholders included:
CNIB Regional Director of Ontario East
Long-Term Care Physician lead and The Mobile Eye Clinic
Parent representative from the Children’s Hospital of Eastern Ontario (CHEO)
Client/patient of the blind community
Diabetic program TOH, Advanced Practice Nurse
Integration Specialist on diabetes Champlain LHIN
Aboriginal Peoples
Réseau for providing French language services to patients
Neighbouring LHINs e.g. South East LHIN,
Vision screening for children in school environment
The stakeholders were invited to meet with our Vision Network Team to discuss and give their
perspective on the following questions.
1. What currently works really well regarding vision care services for patients and families?
2. Do you have any comments about access to vision care services e.g. timely access, linguistically
and culturally appropriate care?
3. What 2 top things would you suggest we do to improve our vision care services?
The stakeholders were welcomed and a discussion of the above questions ensued.
Canadian National Institute for the Blind (CNIB)
CNIB is a registered charity, passionately providing community-based support, knowledge and a national
voice to ensure Canadians who are blind or partially sighted have the confidence, skills and opportunities
to fully participate in life. (CNIB website)
CNIB is the primary provider and funder of rehabilitation therapy after loss of sight. Their present role in
rehabilitation therapies for the visually impaired is not sustainable through charity funding. CNIB
believes they can no longer support these important services under the charitable umbrella.
Path to Change CNIB’s bold new direction for 2014-2018 is their new Strategic Plan. The CNIB plan
calls upon provincial governments, LHINs and the medical community to provide rehabilitation services
for the visually impaired so that it will be the responsibility of our public health care system and not be
dependent on charity funding. The plan strongly supports that rehabilitation therapy for Canadians with
vision loss must be better integrated within the continuum of care in every province. CNIB will continue
56
to work as a charity and will focus on enhancing the quality of people’s lives through advocacy,
employment, literacy and accessibility.
Goals of CNIB 2014-2018
1. Integrate post-vision loss rehabilitation therapy into the continuum of care
2. Redefine CNIB’s role as a charity
7.0 Stakeholder Recommendations: CNIB
7.1 Recommend that the province create a low vision fee code for optometrists
7.2 Increase the services of the existing Low Vision clinics
Long-Term Care
Vision loss is often a low priority health component of the elderly. However, the financial impact of low
vision is staggering. Seniors with vision loss are 1.5 to 2 times more likely to fall which is a major
component that increases health care costs.
Patients in long-term care facilities are underserviced in vision services. The elderly are often difficult to
transport to vision clinics, are isolated and do not have family support to facilitate these appointments.
The wait time for vision services for residents in long term care is over 6 months. A comprehensive
ophthalmologist currently provides eye examinations one half day a month to patients from Élisabeth
Bruyère and St Vincent’s Hospital. The Élisabeth Bruyère Hospital is Ottawa’s largest provider of stroke
and geriatric inpatient rehabilitation and is Ottawa’s only palliative care hospital. St Vincent’s Hospital is
a continuing care hospital for patients with complex care needs.
This is an extremely valuable service that decreases the load of difficult patients attending hospital clinics
and ultimately reduces health care costs related to slips and falls caused by low vision.
8.0 Stakeholder Recommendations: Long-Term Care
8.1 Suggest incentives to have OHIP modify the fee code or use inpatient codes for these patients.
8.2 Suggest the University of Ottawa ophthalmology residents assist in these clinics once a month. This
provides excellent teaching experience and is tremendously beneficial to patients.
8.3 Equipment needs: wheel chair accessible slit lamp and OCT.
8.4 Eye care providers need to expand their efforts to provide vision preserving services within long-term
care facilities. This will reduce overall health care spending as it reduces the number of patients
coming to hospital clinics and decreases the number of patient falls.
Bruyère Continuing Care and The Mobile Eye Clinic
Bruyère is a leading care provider for the elderly in the Champlain region, helping them remain
independent and healthy. Through a pilot project in 2014, Bruyère has partnered with the Canadian
Council of the Blind in conjunction with Lions Club to improve vision health for seniors in the
Champlain region through a mobile eye clinic. The mobile eye clinic brings an optometrist to the senior’s
57
long term care facilities to perform OHIP covered eye exams to seniors. The mobile eye clinic has
partnered with the Ottawa-Carleton District School Board and provides eye exams to children 8 years of
age and up.
In the past 2 years the mobile eye clinic has assessed 674 seniors and 1447 children. Over 55% of seniors
had one or more ocular issues and 39% had updated prescriptions to improve their vision. Over 17% of
children had one or more vision issues and 14% were prescribed corrective glasses.
9.0 Stakeholder Recommendation: Mobile Eye Clinics for Seniors
9.1 Funding be provided to sustain this program for seniors as it aligns with the Champlain LHIN Slip
and Falls and Vision Plan
Patient/family representative from CHEO
A very engaged parent shared her perspective on her journey through the vision care system with her
child with vision loss. The parent was very supportive of the medical team at CHEO and appreciated their
medical expertise and the flexibility of appointments. The parent was extremely satisfied with access to
vision care services.
Areas for improvement were discussed and the parent felt there is a shortage of pediatric
ophthalmologists related to the long waiting time on appointment days. Wait times can be up to 3 hours
with young children. This must be improved. Ophthalmic equipment at CHEO is outdated and needs to be
replaced. The clinic has confidentiality/privacy issues due to the lack of space and soundproof walls. The
biggest concern was the lack of emotional support for parents and children with sight threatening disease
such as support groups to help families dealing with children suffering from sight threatening diseases.
10.0 Stakeholder Recommendations: Family Representative
10.1 Update equipment and facilities (to improve confidentiality) at CHEO.
10.2 Support group for parents and children with sight threatening diseases - local/provincial/national
virtual forums.
Client in the Blind Community
This very engaged sight impaired client of the blind community shared her perspective on vision services
in our community. The client was very satisfied with access to services and believes vision services
worked very well in comparison to other areas of health services.
The client stated that there are improvements to be made at facilities for sight impaired patients. There is
a lack of training and sensitivity by staff to assist blind patients to navigate in the clinic, lack of
instructional material in large print and lack of email services to notify patients of return appointments
instead of small appointment cards. There is a demonstrated need to provide more care for the emotional
and mental health aspect of vision loss.
58
11.0 Stakeholder Recommendations: Client in the Blind Communing
11.1 Training of health care staff to assist with the unique needs of vision impaired patients. Facilities
should use existing technology such as email to facilitate instructions and appointments.
11.2 Provide more support for the emotional and mental health issues that accompany vision loss.
Advanced Practice Nurse Diabetes and Integrated Specialist on Diabetes
These experts on diabetes shared their perspective on vision services for patients with diabetes. It was
noted that in the Champlain LHIN over 120,000 people have diabetes and this number is increasing.
Access to vision services is very good for patients with diabetes. Screening is done by optometrists or
ophthalmologists.
There are huge improvements that can be made using technology and tele-screening for retinopathy so
that imaging of the back of the eye can be sent remotely. Improvements in correspondence between the
ophthalmologist and the diabetes specialists need to be made as charts are difficult to read and follow-up
instructions may be unclear. Family physicians also need a consult note back from the eye specialist with
specific findings and directives (e.g. stable diabetes and follow-up in 1 year with laser). Additionally,
suggestions to improve eye care services included a comprehensive list of service providers for eye exams
and timely access to an ophthalmologist.
12.0 Stakeholder Recommendations: Vision Services for Patients with Diabetes
12.1 Increase the use of telemedicine for screening diabetic retinopathy
12.2 Improve correspondence between ophthalmologist, optometrist and GP and/or diabetes specialist.
12.3 Develop a comprehensive list of service providers for eye exams.
12.4 Implement an integrated EMR to facilitate communication between specialists, family practitioners,
optometrists. Ideally this should be a province/nationwide initiative.
Aboriginal Peoples
There are approximately 41,000 Aboriginal people in the Champlain region. This includes 31,000 off-
reserve (2011Census) and an extimated 10,000 living on the Mohawks of Akwesane reserve. The
National Household Survey of 2011 indicates that there are 10,300 First Nation people living in the
Champlain region, 6,400 Métis and approximately 710 Inuit. Ottawa is the city with the largest
concentration of Inuit beyond northern Canada.
Diabetes is one of the fastest growing diesases among the Aboriginal populations. This rapid increase in
diabetes has a tremendous impact on their health and and vison. Diabetes education and care is key for the
prevention and control of diabetic retinopathy leading to vision loss.
There are five centres dedicated to Aboriginal peoples in the Champlain LHIN that provide diabetes
education and care
Akausivik Inuti Family Health Team
Akwesasne Department of Health
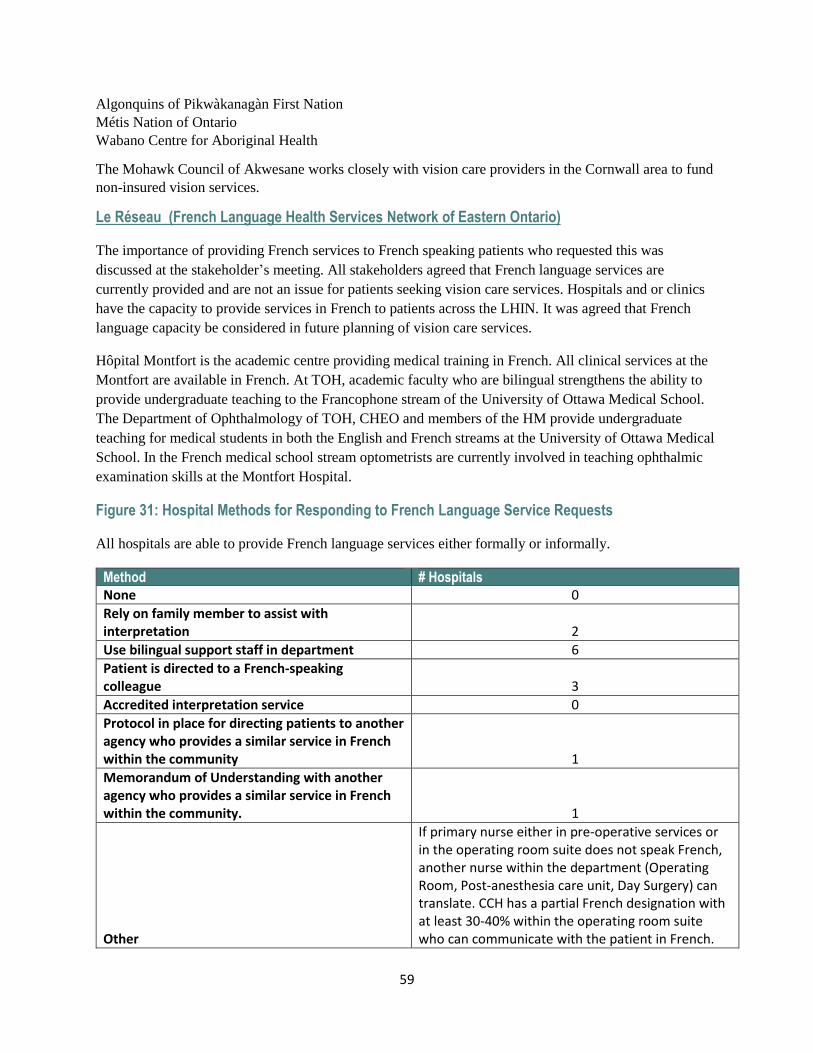
59
Algonquins of Pikwàkanagàn First Nation
Métis Nation of Ontario
Wabano Centre for Aboriginal Health
The Mohawk Council of Akwesane works closely with vision care providers in the Cornwall area to fund
non-insured vision services.
Le Réseau (French Language Health Services Network of Eastern Ontario)
The importance of providing French services to French speaking patients who requested this was
discussed at the stakeholder’s meeting. All stakeholders agreed that French language services are
currently provided and are not an issue for patients seeking vision care services. Hospitals and or clinics
have the capacity to provide services in French to patients across the LHIN. It was agreed that French
language capacity be considered in future planning of vision care services.
Hôpital Montfort is the academic centre providing medical training in French. All clinical services at the
Montfort are available in French. At TOH, academic faculty who are bilingual strengthens the ability to
provide undergraduate teaching to the Francophone stream of the University of Ottawa Medical School.
The Department of Ophthalmology of TOH, CHEO and members of the HM provide undergraduate
teaching for medical students in both the English and French streams at the University of Ottawa Medical
School. In the French medical school stream optometrists are currently involved in teaching ophthalmic
examination skills at the Montfort Hospital.
Figure 31: Hospital Methods for Responding to French Language Service Requests
All hospitals are able to provide French language services either formally or informally.
Method # Hospitals
None 0
Rely on family member to assist with interpretation 2
Use bilingual support staff in department 6
Patient is directed to a French-speaking colleague 3
Accredited interpretation service 0
Protocol in place for directing patients to another agency who provides a similar service in French within the community 1
Memorandum of Understanding with another agency who provides a similar service in French within the community. 1
Other
If primary nurse either in pre-operative services or in the operating room suite does not speak French, another nurse within the department (Operating Room, Post-anesthesia care unit, Day Surgery) can translate. CCH has a partial French designation with at least 30-40% within the operating room suite who can communicate with the patient in French.
60
13.0 Stakeholder Recommendations: Provision of French language Services
13.1 Capture the linguistic identity of all patients
13.2 French language capacity be considered in future planning of vision care services
13.3 Proactively offer French language services to patients whose linguistic identity is French
Vision screening for kindergarten children in Ottawa
A research project Let your Children See the Future is being piloted in Ottawa in the spring 2016
involving the vision screening of 500-1000 children in junior kindergarten. This pilot program is led by
researchers Dr. Daphne Maurer, McMaster University and Dr. Agnes Wong, The Hospital for Sick
Children in collaboration with the Ontario Association of Optometrists and The Eye See...Eye Learn®
program. The initial vision screening will be done by University of Ottawa Medical students with follow-
up in-school exams by The Eye See...Eye Learn® optometrists.
Eye See…Eye Learn® provides comprehensive eye exams by participating local optometrists to junior
kindergarten students across Ontario. If the child requires a pair of glasses, they will receive a
complimentary pair. The Eye See...Eye Learn® program was developed to raise awareness among parents
of the importance of having their children's eyes checked when starting school. Each year, thousands of
children start school without ever having had an eye exam.
This initiative illustrates a collaborative effort between optometrists, ophthalmologists and schools across
the LHIN.
Neighbouring LHINs
The Champlain LHIN has strong referral partnerships across neighbouring LHINs for pediatrics, some
subspecialties and level 4 (complex) procedures. Patients requiring specialty ophthalmology services
often need to cross LHIN boundaries to obtain theses services. Specialty centres in the Champlain LHIN
should consider the use of tele-ophthalmology and electronic medical records to reduce travel time for
follow-up visits as necessary.
Communication between the Chair of Ophthalmology in Ottawa and Kingston was initiated to more
accurately define the historical relationship of Perth and Smith Falls District Hospital which straddles
both the Champlain and South East LHIN (see page 26).

61
Section F
Final Summary of Recommendations by Priority
The Champlain LHIN Vision Care Plan provides an overview of ophthalmology services across the LHIN
and a view to the future needs of the population. These recommendations in collaboration with the
Provincial Vision Strategy Task Force will set the stage for quality improvements to improve vision care
services for the residents of the Champlain LHIN. These recommendations have been further categorized
and ranked in order of priority by the Vision Care Network Committee.
Priorty 1: Improve Patient Access to Pediatric Services by Recruiting Pediatric Ophthalmologist(s)
to Address Current and Future Needs (see Recommendation #4. 1)
Pediatric ophthalmologist with surgical privileges to improve access for children and eliminate decrease
the long Wait 1 for pediatrics to be located at CHEO. Additional operating room resources will need to be
created to address Wait 2 and completion of a planned but currently on hold renovation to the pediatric
eye clinic will be required to meet this recommendation.
Priority 2: Recruit Ophthalmologists to Address Future Patient Needs using Population Based
Approach (see Recommendations #2.2, 3.1, 6.3,6.4)
Using a population-based approach the future need of comprehensive and subspecialty ophthalmologists
demonstrates a growing need for recruitment and succession planning.
1. Comprehensive ophthalmologist with surgical privileges for the Cornwall area to increase
surgical staff from 2 to 3.
2. TOH to endeavor to recruit a community glaucoma specialist to manage increasing surgical
demands. Baseline distribution of 200 cataract cases from current allocation or anticipated
increased allotment (see Priority #3). Savings from within program should be allocated to the
base budget of the Department of Ophthalmology to provide additional glaucoma operating
room access.
In the short term TOH is planning to hire a general ophthalmologist with training (mini-fellowship) in
pediatric ophthalmology who will see pediatric patients/consults at CHEO 4-6 days per month. This will
help to reduce Wait 1. Local optometrists will likely as a result see increased number of children knowing
there is an additional pediatric ophthalmologist to refer to provide support (backstopping).
62
The long term plans are:
Succession planning for the most senior pediatric ophthalmologist as well as senior
comprehensive ophthalmologists.
It is recommended that the hub hospitals collaborate with community hospitals in future
recruitment. It is recommended that the Department of Ophthalmology at the University of
Ottawa/TOH take steps to provide community hospital and community ophthalmology
opportunities for its residents to broaden their experience. This could support future recruitment
in regions outside the city of Ottawa.
It is recommended that the Regional Vision Care Network committee initiate discussions with the
North East LHIN for recruitment of a retina-vitreous surgeon. This recruitment would increase
access and reduce travel distances and costs for patients that currently come to the Champlain
LHIN for specialized retinal care.
Priority 3: Decrease Patient Wait Times by Increasing Cataract Allocation in Champlain LHIN by
15% to Achieve Wait 2 Targets (see Recommendations #3.1, 6.1, 6.2, 6.3)
In 2012-13 the one-time Wait Time Strategy Funding was withdrawn resulting in a reduced ability to
meet the 182 day target of priority 4 cases. When the Wait Time funding ceased approximatly 1,500 cases
were cut which was a reduction of 15%. After 2013 there was an increase in Wait 2 despite increasing
operating room efficiencies (figure 18).
The Ministry of Health and Long-Term Care produced an analysis showing that the Champlain LHIN
utilization rate per 100,000 population was 18% higher than the Ontario average (figure 20). However, a
subsequent analysis by the Champlain LHIN that included both in and out of hospital procedures showed
the Champlain’s utilization rate is actually 15% lower than the provincial average. Combining the
numbers is more representative of true utilization from a patient’s perspective and not from site delivery.
Other LHINs have a greater number of procedures done in Independent Health Facilities (IHF)
particularly in the Toronto area. Restoration of the previously allocated one time Wait Time Strategy
Funding (used to initially reduce wait times) to the Champlain LHIN will re-establish an equilibrium
permitting the LHIN to achieve its Wait 2 target of 182 days or less. This calculation pertains to the
current state and does not include future projections based on future demographic demand.
An immediate 15% increase in cataract volume across the LHIN.
The newly formed Regional Vision Care Network committee and not the Ministry be responsible
for allocating the cataract volumes within the LHIN. This committee will have representation
from all hospitals and can proactively plan for the increased volume in a timely manner.
In addition to a base allocation that a year over year increase in cataract volumes is needed to
keep pace with the future population changes. Demographic demand dictates that an additional
2,500 cases will need to be performed by 2022 within the Champlain LHIN.
63
Priority 4: Improve Communication Between Institutions and Providers by Developing an Integrated
EMR across the LHIN/Province (see Recommendations #2.1, 12.4)
Communicating the clinical outcomes of cataract and all ophthalmology procedures is extremely
important from a quality of care perspective. It is recommended that a fully integrated functional EMR
across the LHIN (provincially/nationally) would improve patient care and more importantly
communication between providers immensely. Communicating outcomes is critical if post-op metrics are
to be analyzed. Optometrists and ophthalmologists work closely together to care for patients and
communication flow in both directions is essential. Family physicians, diabetic nurse specialists would be
better served by being able to view eye care data from both optometrists and ophthalmologists
particularly for patients with diabetes.
In the Short Term all ophthalmologists/optometrists should provide a note regarding diabetic
evaluations/treatments to the patient’s primary care physician and or specialist (i.e. diabetic specialist)
involved with the patient’s medical care.
In the long term a fully integrated functional EMR should be a high priority provincially and ideally
nationally.
Priorty 5: Standardize Provincial Monitoring of Patient Satisfaction for Cataract Surgery (see
Recommendations #5.7)
The patient experience, prior to, during and after cataract surgery is an important indicator of success. It is
recommended that the patient experience and their satisfaction levels be monitored. This information can
be used to improve processes and improve the experience from the patient’s point of view. It is
recommended that:
Patient satisfaction is monitored and used to improve the quality of care.
A standardized patient satisfaction survey be developed specifically for cataract surgery and be
used across the LHIN and across the province (see Appendix 1.4 for example of Draft Patient
Satisfaction Survey).
Prioity 6: Maintain Hub and Spoke Model of Delivery (see Recommendations #2.1,2.2 6.1)
It is recommended that the hub and spoke model for the delivery of ophthalmology care in the Champlain
LHIN continue. Delivery and integration of complex and subspecialty services through TOH and CHEO
at the hub has proved to be extremely successful. The spoke hospitals play an important role in permitting
access to care within reasonable distances of a patient’s home within the Champlain LHIN. Primary,
secondary and even some tertiary care is safely provided. The success of this model can be considered by
other LHINs within Ontario.
64
Priority 7: Standardize Processes for Cataract Surgery to Improve Efficiencies/Safety/Quality (see
Recommendations #5.1, 5.2, 5.3, 5.4, 5.6)
Standardizing the process for cataract surgery as effectively and efficiently as possible will ultimately
improve efficiencies and lower the cost per case. All hospitals need to strive for efficiencies that meet best
practices and ensure clinical guidelines are being followed. It is recommended that the newly formed
Regional Vision Care Committee is actively involved in standardization of processes across the LHIN.
Ideally the development of a regional scorecard would streamline these processes.
Pre-Assessments recommendations:
Establish best practice standards to ensure all patients have been screened prior to surgery.
Share practices across the LHIN on best practices for pre-assessments (e.g. screening tools,
second eye assessments, nurse verse GP assessments).
Operating room recommendation:
Share best practices across LHIN to improve efficiencies for all hospitals ensuring clinical
guidelines are followed e.g. number of cases per day, staff mix, turnover, standardization of trays
and processes for all surgeons.
Review sedation models with anesthesia to ensure patients are able to decide whether or not to
use sedation based on patient needs ensuring that the OMA Sedation Standards are followed.
Post procedure recommendation:
Sharing of best practices amongst constituent members of the LHIN is strongly encouraged and
provincial or National indicators should be standardized.
Priority 8: Vision Screening for Children and High Risk Groups (see Recommendations #1.1, 1.2, 12.1, 12.2,
12.3, 12.4)
There are high risk groups in the community that need to be screened and monitored to reduce the
complications of eye problems. Young children and people living with diabetes are high risk groups for
eye problems. Family physicians should strive to follow recommendations for eye exams for each of
their patients with diabetes and make appropriate referrals to an eye care provider. Educate patients with
diabetes to have their vision screened every year by an optometrist. If treatment is necessary then a
referral can be made to an ophthalmologist. As well, it is important to understand the needs of refugee and
immigrant populations and to educate providers and newcomers on accessing available resources and
services for vision care.
Remove financial barriers of additional testing not covered by OHIP
Communication of results of vision screening should be shared with the patient’s primary health
care provider.
Support vision screening projects for kindergarten children.
65
Priority 9: Explore Opportunites to Maintain Access to Vision Rehabilitation Services (see
Recommendations #7.1, 7.2)
In future planning of vision rehabilitation services it was brought to our attention that CNIB will no
longer provide low vision rehabilitation services using their charity funds. It was acknowledged that other
providers will need to increase service provision. It is recommended to:
Advise the province to create a low vision fee code for optometrists.
Increase the services of the existing low vision clinics.
Priority 10: Improve Patient Experience/Mental Health of Patients with Vision Loss (see
Recommendations #10.1,10.2,11.1, 11.2,)
Older adults are becoming a greater proportion of our population and will encounter vision loss
particularly from age related macular degeneration. Depression is associated with functional visual loss
and social isolation. Recognizing depression in the elderly and those particularly with vision loss will be
important in the years ahead. Collaborative work with family physicians in managing depression in
conjunction with eye care providers and particularly those with expertise in vision rehabilitation is
necessary. Education of support workers and rehabilitation training programs can enhance the wellness of
patients with significant visual impairment.
Provide information on support groups for patients and parents with children with sight
threatening diseases- locally/provincial/national virtual forums.
Provide more support for the emotional and mental health issues that accompany vision loss.
Ensure training of health care staff in eye care providers’ offices to deal with the unique needs of
vision impaired patients.
Update equipment and facilities (to improve confidentiality) at CHEO.
Priority 11: Enhance Vision Services for Patients in Long Term Care (see Recommendations #8.1, 8.2, 8.3,
8.4, 9.1)
Long-term care patients are a high risk group for vision loss and have difficulty accessing vision services
outside of their institution. Eye care providers need to expand their efforts to provide vision preserving
services within long-term care facilities. This will reduce overall health care spending as it reduces the
number of patients coming to hospital clinics and reduce the number of patient falls.
Suggest OHIP modify the fee code or use inpatient codes for these patients to incentivize this
activity.
Suggest the University of Ottawa ophthalmology residents assist in these clinics as they also
provide an excellent teaching experience and sensitize them to the needs of these services.
Funding for equipment needs such as wheel chair accessible slit lamp and OCT.
Eye care providers to expand their efforts to provide vision preserving services within long-term
care facilities
Funding to sustain Mobile Eye Clinics for long-term care programs as it aligns with the
Champlain LHIN Slip and Falls and Vision Plan.
66
Priority 12: Maintain/Enhance Provision of French Language Services (see Recommendations #13.0, 13.1,
13.2, 13.3)
It is recommended that in future planning of vision care services across the Champlain LHIN that French
language services are considered.
Capture the linguistic identify of all patients
Proactively offer French language services to patients whose linguistic identity is French.
Priority 13: Continuation of the Regional Vision Care Network Committee
It is recommended that the Regional Vision Care Network Committee will continue to meet with a
mandate to implement the finding and results of this project. Administrative and clinical membership will
come from throughout the region. Hospitals, ophthalmologists, and optometrists under the guidance of the
LHIN administrators should be represented. Its mandate should include:
Monitoring of performance metrics such as quality issues, practice standards and best practices
and providing expert advice across the Champlain LHIN in collaboration with the Provincial
Vision Strategy Task Force on the ophthalmology performance indicators identified in A Vision
for Ontario.
Guidance in the quality based procedure (QBP) allocation for the Champlain LHIN.
Monitoring of wait times across the LHIN of all hospitals and ophthalmologists to ensure access
is fair and equitable and to compare their performance to the provincial target and LHIN average.
If there is a significant inequity the committee should discuss other alternatives to reduce wait
times such as redistribution of inflow to individual providers.
Discussions with other LHINs for recruitment and for the improvement of services that are
overlapping between the LHINs.
Develop a resource plan for the financial impact of these recommendations
67
Section G
Appendix
1.0 Champlain Vision Care Network Committee Members
1.1 Terms of Reference
1.2 Private Practice/Facilities Surveyed
1.3 List of Stakeholders
1.4 Proposed Cataract Patient Satisfaction Survey
2.0 Hospital Survey Results
2.1 Community Survey Results

1900 City Park Drive, Suite 204 Ottawa, ON K1J 1A3 Tel 613.747.6784 • Fax 613.747.6519 Toll Free 1.866.902.5446 www.champlainlhin.on.ca
1900, promenade City Park, bureau 204 Ottawa, ON K1J 1A3 Téléphone : 613 747-6784 • Télécopieur : 613 747-6519 Sans frais : 1 866 902-5446 www.rlisschamplain.on.ca
Appendix 1.0 Champlain Vision Care Network Committee Members
1 Dr. Steven Gilberg – co-chair
Head, Department of Ophthalmology, The Ottawa Hospital
2 Jeanette Despatie – co-chair
CEO, Cornwall Community Hospital
3 Dr. Bernie Hurley Assistant Professor of Ophthalmology, The University of Ottawa
Vitreo-Retinal Surgeon, The Ottawa Hospital
4 Dr. Christine Suess Chief of Ophthalmology Service, Cornwall Community Hospital
5 Dr. Steven Poleski Chief, Ophthalmology Unit, Hôpital Montfort
6 Dr. Annick Fournier
Chief of Ophthalmology, CHEO
7 Tammy DeGiovanni
Director, Ambulatory Care, CHEO
8 Mario Bédard Clinical Director, Pharmacy & Eye Care Program, The Ottawa Hospital
9 Lucille Perreault Vice-President, Clinical Programs and Chief Nursing Executive, Hôpital Montfort
10 François Lemaire
Vice-President Patient Services - Acute Care and Chief Nursing Executive
Pembroke Regional Hospital
11 Dr. Ali Shoughary
Ophthalmologist Surgeon, Pembroke Regional Hospital
12 Dr. Walter Delpero
Ophthalmologist, Winchester District Memorial Hospital
13 Lynn Hall Senior Vice-President, Clinical Services / Chief Nursing Executive / Professional Practice
Leader, Winchester District Memorial Hospital
14 Dr. Thomas-A. Noël
McLeod Optometry Clinic
Project Manager: Rosemary Bickerton, The Ottawa Hospital
Champlain LHIN Representatives: Eric Partington, Elizabeth Woodbury, Vicky Walker
1
Appendix 1.1 Champlain LHIN Vision Care Network Terms of Reference
Background and Context In May of 2013, the Provincial Vision Strategy Task Force submitted its report Strategic
Recommendations for Ophthalmology in Ontario to the Ministry of Health and Long-Term Care. The
Task Force conducted a thorough review of Ophthalmology services in Ontario including an assessment
of the future patient needs. One of the recommendations in the report is that “each LHIN should develop a
Local Vision Plan describing how they will provide for the current state and future needs of their
communities, based on the Provincial Vision Strategy Task Force Report and its findings”. The
Champlain LHIN Vision Services Network has been struck to advise the LHIN on developing such a
regional vision plan.
Other relevant provincial strategies that will guide this work include the Excellent Care for All Act and
the introduction of health system funding reform (HSFR). The Excellent Care for All Act (ECFAA) was
passed in June 2010 and puts patients first by improving the quality and value of the patient experience
through the application of evidence-based health care. ECFAA positions Ontario to implement reforms
and develop the levers needed to mobilize the delivery of high quality, patient-centered care.
Four core principles underpin the vision of ECFAA:
1. Care is organized around the person to support their health.
2. Quality and its continuous improvement is a critical goal across the health system.
3. Quality of care is supported by the best evidence and standards of care.
4. Payment, policy and planning support quality and efficient use of resources.
In January 2012, Ontario’s Action Plan for Health Care expanded on the fourth principle and outlined the
need for health system funding reform (HSFR):
Today’s fiscal reality requires that we act now to make Ontario’s health care system sustainable;
We need to create a system that improves quality for patients as it delivers increased value for
taxpayers;
Evidence helps answer the question of how finite health care dollars should be allocated to best
serve patients;
Our entire patient care transformation will be successful only if our funding models reflect our
priorities;
Funding must follow the patient.
Purpose The purpose of the Champlain LHIN Vision Care Network is to:
Act as the principle advisor to the Champlain LHIN CEO regarding the organization and delivery
of vision care services in the Champlain LHIN;
Guide the development of the Champlain LHIN Vision Plan; and
Ensure timely and equitable patient access to high quality vision care across the Champlain
LHIN.
2
Note: While the scope of the planning is focused on those services delivered in hospitals, it is recognized
that community-based eye care services are a vital component of comprehensive, integrated vision care
services in the Champlain LHIN. Committee membership will incorporate this key role and input.
Responsibilities The Champlain LHIN Vision Care Network will have the following responsibilities:
Regional Planning
Recommend appropriate distribution of vision care services and resources to ensure access to
high quality, integrated care.
Direct regional initiatives related to Vision Care (e.g. Human Resource Planning, standardization
of processes or equipment and supplies, clinical and management best practices).
Incorporate Ministry of Health and Long- term Care directions and system funding changes as
they arise.
Ensure that regional planning examines the impact of services provided to residents of Quebec,
and other out of province jurisdictions and what these services mean for corresponding
Champlain utilization rates and resource impacts.
Ensure planning and service distribution is consistent with French language service designation.
Ensure planning and service distribution considers at risk patient populations (e.g. patients with
diabetes, aboriginal communities) and their needs.
Resource and Volume Allocation
Make recommendations to the LHIN on the principles that will guide resource allocation and
service distribution.
Make recommendations to the LHIN on annual QBP (Quality Based Procedure) and Wait Time
volume allocations and reallocations.
Performance Monitoring and Management
Monitor performance of vision care services by reviewing regional and provincial indicators,
quality measures and reports and identify strategies to improve performance.
Best Practices and Quality Improvement
Promote the establishment, use, and evaluation of best practice standards of care, guidelines and
operational processes.
Ensure the integration of QBP and similar Clinical Handbook recommendations.
Education, Research and Knowledge Mobilization
Promote evidence-based, standardized, regional ophthalmology education and knowledge
exchange activities, programs and research.
Ensure academic training requirements of ophthalmology service providers are met.
Communication and Stakeholder Engagement
Develop a communication plan for the network`s activities
3
Note: The Network will explore opportunities to engage patients and families for their input and
participation during the development of the Champlain LHIN Vision Plan.
Accountability The Champlain LHIN Vision Care Network reports to the Champlain LHIN CEO
Membership CEO Cornwall Hospital (co-chair)
Chief, Ophthalmology, Ottawa Hospital (co-chair)
Physician and administrative representation – all hospitals providing vision care services
Local Administration Representative from Provincial Vision Task Force - Senior VP and COO, Ottawa
Hospital
Local Physician Representative from Provincial Vision Task Force – University of Ottawa Eye Institute
Community optometry representative
Consultations as required Anesthesia
Emergency medicine
Family medicine
Nursing Management Representative – University of Ottawa Eye Institute
French Language Health Services Network of Eastern Ontario (Réseau)
LHIN support staff
Senior Director, Health System Performance
Director, Accountability
Director, System Performance and Analysis
Senior Performance Specialist
Meetings Monthly to establish Terms of Reference, network structure and workplan. Frequency can then be
reevaluated.
Agenda, Minutes and Materials
A package will be sent to Network members 3-5 business days in advance of a meeting. The
package will include the following:
Agenda
Minutes of previous meeting
Any related progress reports
Any other relevant documents considered important to the meeting
Minutes for the meeting will be taken by the Executive Assistant for the Senior Director, Health System
Performance.

4
Decision Making and Quorum Quorum is defined as 2/3 of voting members. Quorum is required to proceed with a network meeting.
A consensus decision-making model will be used by the Network whereby consensus is defined as the
willingness among all members to support a decision once it is made.
When consensus cannot be reached, the co-chairs can request a formal vote to arrive at a decision. A 2/3
majority is required for a motion to be carried.
Terms of Reference Review Terms of Reference will be reviewed annually and revised as needed.
Specifically, once the Champlain LHIN Vision Plan is developed, the nature and scope of an ongoing
committee structure should be reviewed, defined and established as required.
Appendix 1.2 Commmunity Providers
Pembroke offices:
Dr Ali Shoughary
Dr Canniff
Cornwall offices:
Dr Suess Dr Youssef Dr Guindon
Hawksbury office:
Dr Helena Mihalovits
Winchester office:
Dr Dennis Conrad
Ottawa offices:
Dr Agapitos Eye Associates: Drs MacInnis, Bastianelli, Britton, Marshall, Myles, Zabel LasikMD: Dr Myles and Dr Zabel Dr Lapointe, Dr Bhargava, and Dr Baryla iCareCentre: Dr Bhatti and Smith; Dr Bonn Retina Centre of Ottawa; Drs Lee, Tuli, Britton. Drs Chevrier, Harding and Morgan Dr Delpero Dr Desroches FOCUS EYE CENTRE; Drs Edmison, Menard, Cheung and Smith Drs Munro, Engel Dr Entwistle Dr Jordan Dr Konzuk, Teboul Dr Hector MacDonald “Revisage” Dr Poleski Dr Rock Dr Ross Dr Weston Dr Madeline Murphy

Appendix 1.3 List of Stakeholders
1. Mike Nicholson, Regional Director, ON East, CNIB
2. Leona Emberson (Client of the blind community)
3. Dr. Jim Farmer ( LTC perspective – St. Vincent’s Long-Term Care Hospital)
4. Candace Hay (CHEO family representative) 5. Filomena De Sousa (Advanced Practice Nurse Diabetes)
6. Leah Bartlett (LHIN Senior Integration Specialist)
7. The Mobile Eye Clinic ( Mel Doris, The Canadian Council of the Blind)
8. Dr. Daphne Maurer McMaster University (Researcher for vision screening for kindergarten
children in the school environment)
Appendix 1.4 Proposed cataract patient satisfaction survey
YOUR EXPERIENCE WITH CATARACT SURGERY
Thank you for completing this short questionnaire to help us improve the experience and
care you received.
As a patient who had a Cataract surgery, we would like to hear from you. There are no right or wrong answers.
We are interested in your honest feedback and comments.
All responses will be collected anonymously. No personal identifying information will be collected from you.
Your surgeon will NOT have access to the individual responses you provided in this survey.
Please note: Completion of this survey is completely voluntary.
If you have any questions about completing the questionnaire, please contact ________
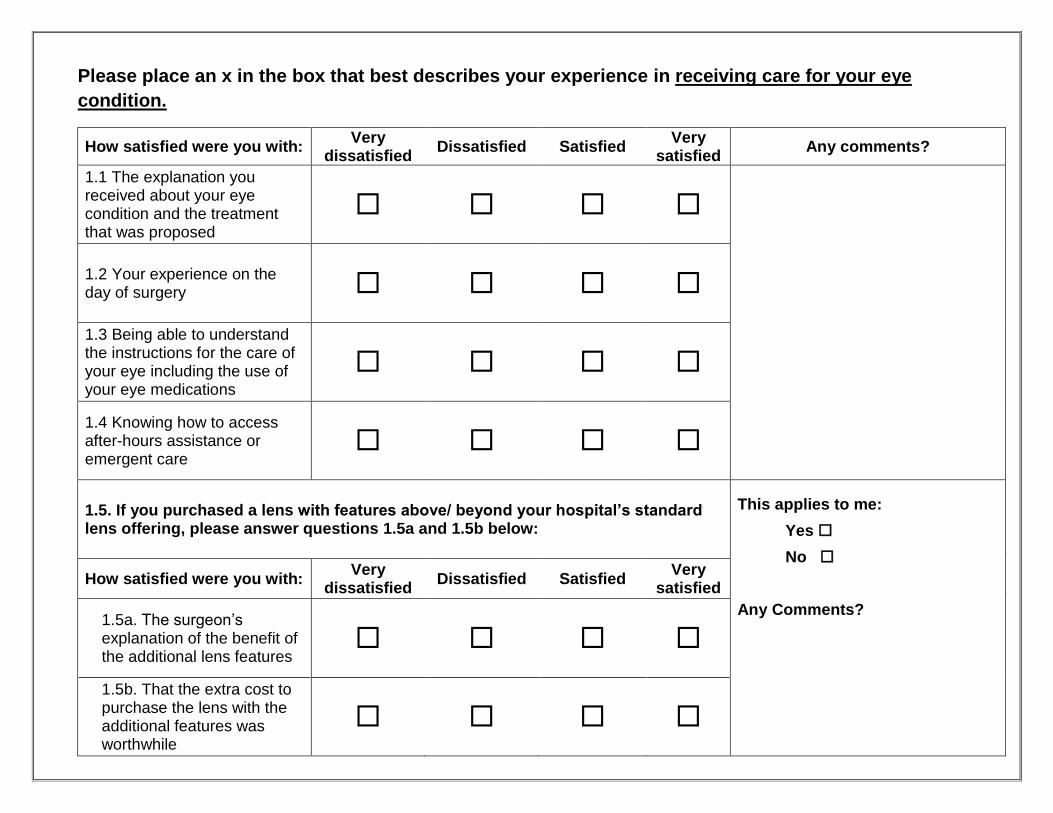
Please place an x in the box that best describes your experience in receiving care for your eye
condition.
How satisfied were you with: Very
dissatisfied Dissatisfied Satisfied
Very satisfied
Any comments?
1.1 The explanation you received about your eye condition and the treatment that was proposed
1.2 Your experience on the day of surgery
1.3 Being able to understand the instructions for the care of your eye including the use of your eye medications
1.4 Knowing how to access after-hours assistance or emergent care
1.5. If you purchased a lens with features above/ beyond your hospital’s standard lens offering, please answer questions 1.5a and 1.5b below:
This applies to me:
Yes
No
Any Comments?
How satisfied were you with: Very
dissatisfied Dissatisfied Satisfied
Very satisfied
1.5a. The surgeon’s explanation of the benefit of the additional lens features
1.5b. That the extra cost to purchase the lens with the additional features was worthwhile
Once again thank you for your input!
If you would like your operating surgeon to contact you, please provide your contact information
below:
Full name: ________________________
Telephone number: ________________
Email address:_____________________
Appendix 2.0
Vision Care Day Surgery
Hospital Survey Results
Prepared by Vicky Walker
Event Vision Care Planning Meeting
Date November 24, 2015
Objectives
• Provide an overview of the hospital survey results
• Provide additional information on current status and
projected future needs for vision care day surgery in
Champlain hospitals
• Identify next steps to support the Champlain Regional
Vision Planning Initiative
2
Methods
• All hospitals in the Champlain region that provide ophthalmology
services were surveyed in October/November 2015 over a 2 week
period
• 5 hospitals provide adult services; 1 provides paediatric services
• Response rate 100%
3
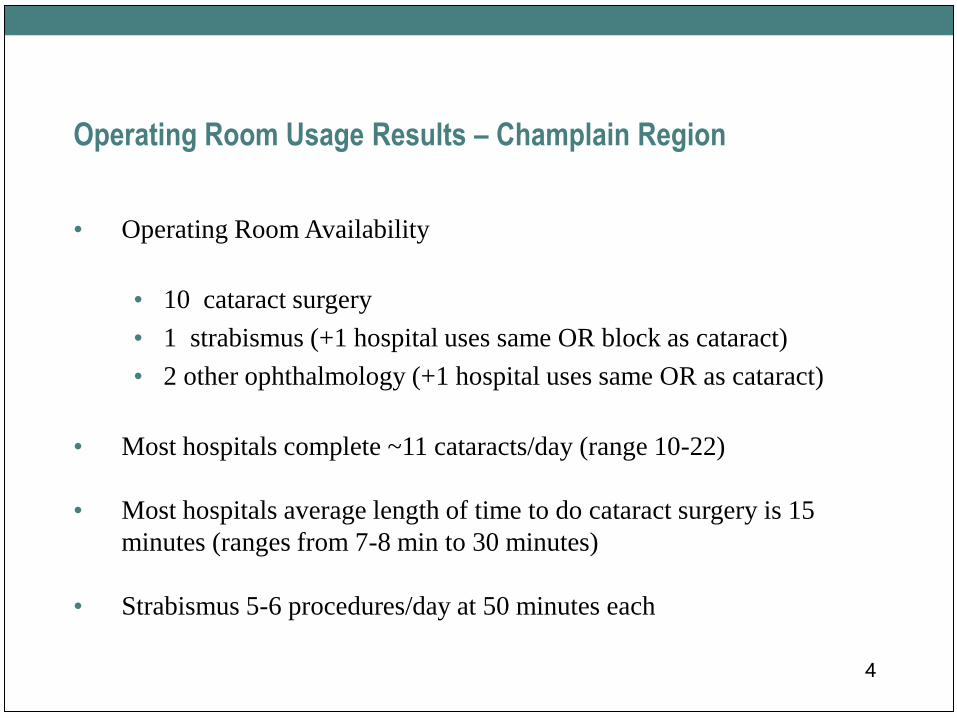
Operating Room Usage Results – Champlain Region
• Operating Room Availability
• 10 cataract surgery
• 1 strabismus (+1 hospital uses same OR block as cataract)
• 2 other ophthalmology (+1 hospital uses same OR as cataract)
• Most hospitals complete ~11 cataracts/day (range 10-22)
• Most hospitals average length of time to do cataract surgery is 15
minutes (ranges from 7-8 min to 30 minutes)
• Strabismus 5-6 procedures/day at 50 minutes each
4
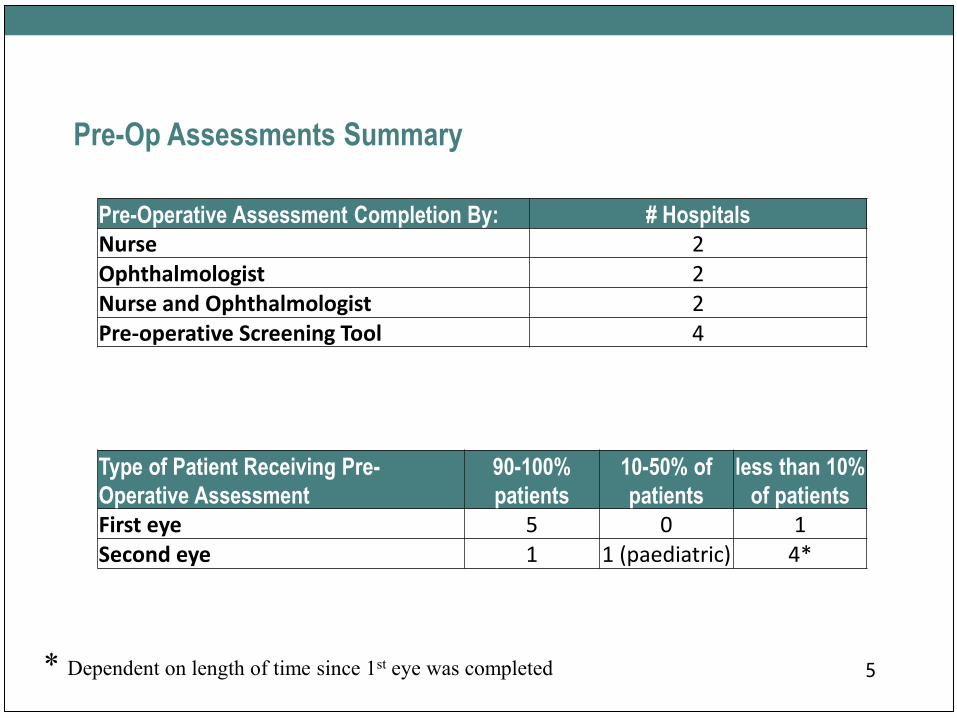
Pre-Op Assessments Summary
5
Type of Patient Receiving Pre-
Operative Assessment
90-100%
patients
10-50% of
patients
less than 10%
of patients
First eye 5 0 1Second eye 1 1 (paediatric) 4*
Pre-Operative Assessment Completion By: # Hospitals
Nurse 2Ophthalmologist 2Nurse and Ophthalmologist 2Pre-operative Screening Tool 4
* Dependent on length of time since 1st eye was completed
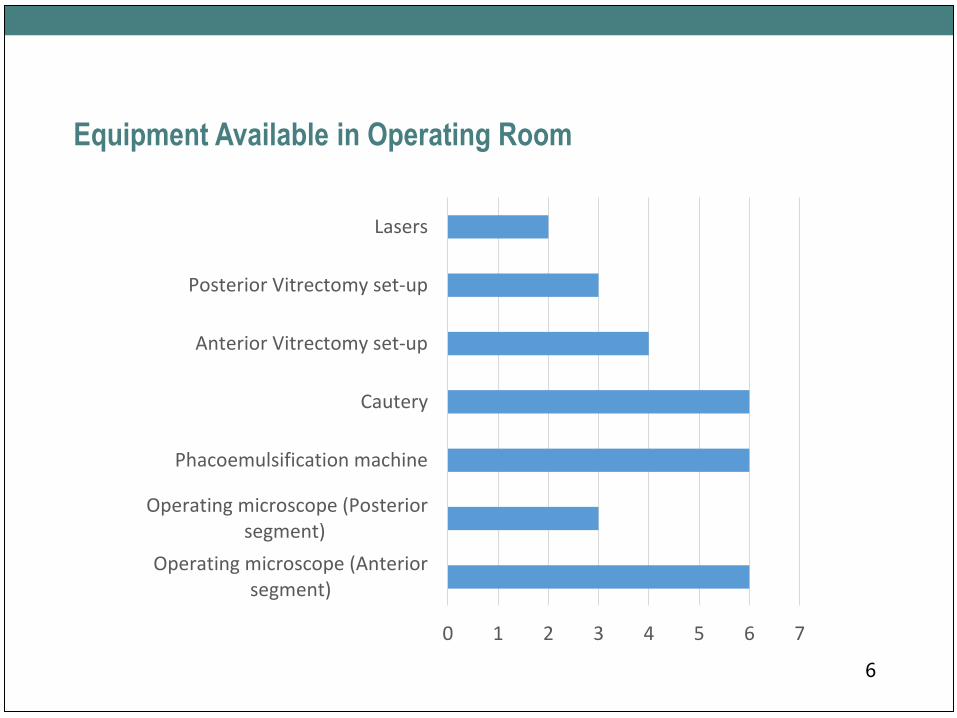
Equipment Available in Operating Room
6
0 1 2 3 4 5 6 7
Operating microscope (Anteriorsegment)
Operating microscope (Posteriorsegment)
Phacoemulsification machine
Cautery
Anterior Vitrectomy set-up
Posterior Vitrectomy set-up
Lasers
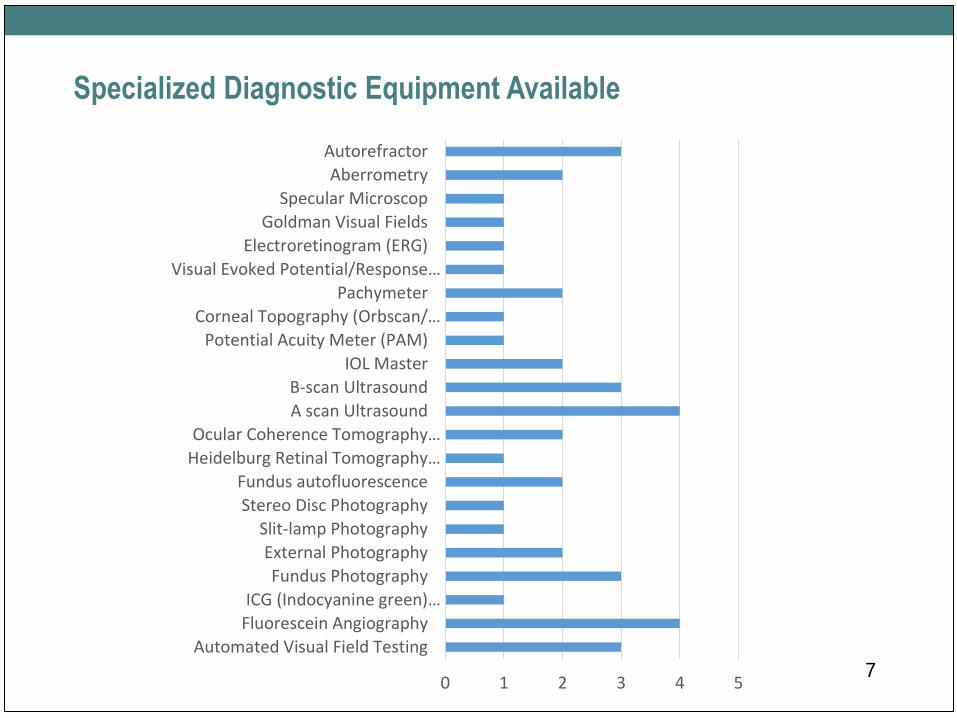
Specialized Diagnostic Equipment Available
70 1 2 3 4 5
Automated Visual Field Testing
Fluorescein Angiography
ICG (Indocyanine green)…
Fundus Photography
External Photography
Slit-lamp Photography
Stereo Disc Photography
Fundus autofluorescence
Heidelburg Retinal Tomography…
Ocular Coherence Tomography…
A scan Ultrasound
B-scan Ultrasound
IOL Master
Potential Acuity Meter (PAM)
Corneal Topography (Orbscan/…
Pachymeter
Visual Evoked Potential/Response…
Electroretinogram (ERG)
Goldman Visual Fields
Specular Microscop
Aberrometry
Autorefractor
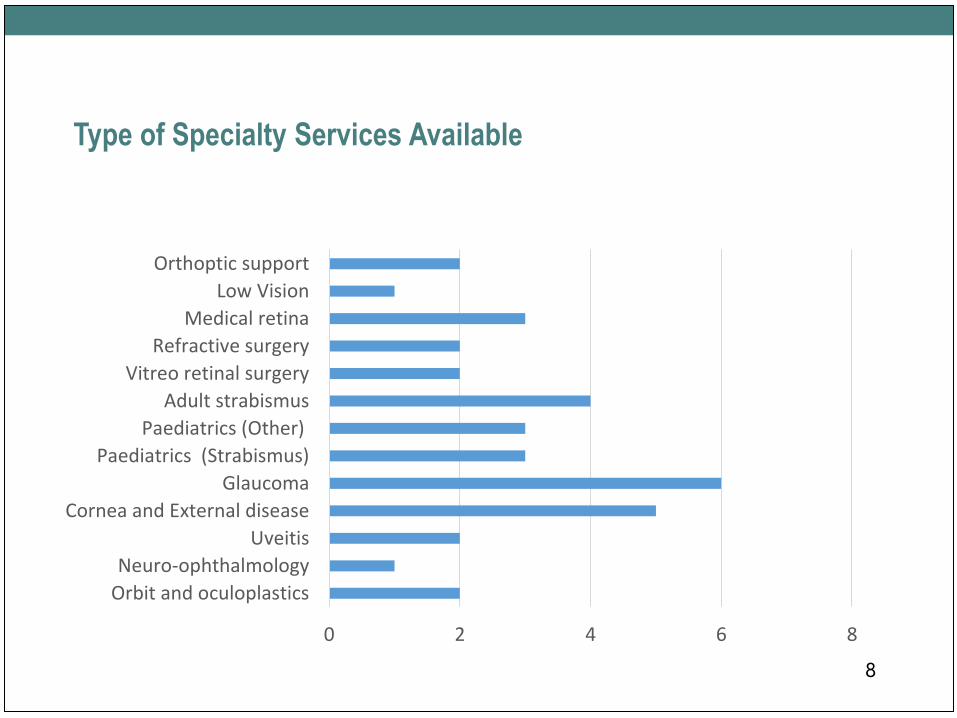
Type of Specialty Services Available
8
0 2 4 6 8
Orbit and oculoplastics
Neuro-ophthalmology
Uveitis
Cornea and External disease
Glaucoma
Paediatrics (Strabismus)
Paediatrics (Other)
Adult strabismus
Vitreo retinal surgery
Refractive surgery
Medical retina
Low Vision
Orthoptic support
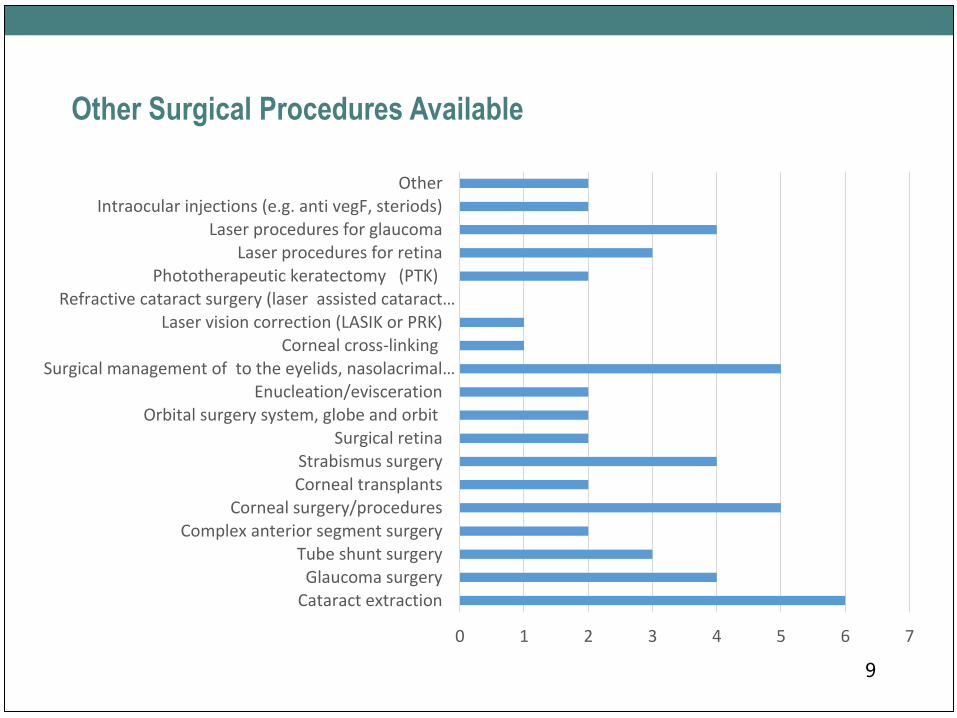
Other Surgical Procedures Available
9
0 1 2 3 4 5 6 7
Cataract extractionGlaucoma surgery
Tube shunt surgeryComplex anterior segment surgery
Corneal surgery/proceduresCorneal transplantsStrabismus surgery
Surgical retinaOrbital surgery system, globe and orbit
Enucleation/eviscerationSurgical management of to the eyelids, nasolacrimal…
Corneal cross-linking Laser vision correction (LASIK or PRK)
Refractive cataract surgery (laser assisted cataract…Phototherapeutic keratectomy (PTK)
Laser procedures for retinaLaser procedures for glaucoma
Intraocular injections (e.g. anti vegF, steriods)Other
Monitoring of Wait Times – Cataract Surgery
• Monthly volumes monitored reports to surgeons quarterly
• WTIS (4 hospitals)
• Monthly reports generated by WTIS coordinator and reviewed by Eye Care
Committee Work. Targeted a few physicians regarding management of office
workflow.
• Wait times are reviewed every 2 months to determine patients exceeding wait
time. Discussions with physician and office staff occur should data require a
more detailed discussion.
10
Monitoring of Strabismus Wait Times
• WTIS monitored for in and out of window. Reviewed monthly and
strategic time allocated however limited due to MD resources.
(CHEO)
• Not monitored for adult strabismus.
• WTIS and Eye Care Committee as per above. We will be hiring a
neuro-ophthalmologist to perform additional surgery for adult
strabismus. Resources will be reallocated to provide additional OR
time.
• Reviewed but not in the same detail as cataracts.
• N/A (2 hospitals)11
On-Call Arrangements
• Daytime call shared among physicians on-site. After hours on-call according to
Eye Institute (city-wide call) (CHEO)
• No on call at hospital, patients return to Ottawa if an issue, numbers left with
patients at discharge (WDMH)
• General ophthalmology call-coverage 24 hours, 365 days per year-emergency
weekend clinics. Retina call 24 hours 365 days per year. Ad hoc support for
oculoplastics, cornea, neurophthalmology, glaucoma (TOH)
• 2 physicians; 50% of call time each (PRH)
• Always one physician on call X 24hrs (HM)
• 80% Hospital On-Call Coverage (CCH)
12

Are there significant human resources gaps for physicians?
• Significant (paediatric)
• Although not within walls of TOH there is a clinical need for
additional pediatric ophthalmology support as Wait 1 and 2 are high.
Demographics may drive need for more physicians to perform
antiVegF injections.
• Yes, currently recruiting a 3rd ophthalmologist, letter of offer has
been submitted to the successful candidate, waiting for his answer.
Tentative start date for this new physician is April 2016. (Cornwall)
• No (3 hospitals)
13
• Evaluating skill mix in clinic but have gap to cover late day clinics.
• Most ophthalmic nurses have seniority and are near retirement. There
are challenges in hiring as many young nurses are looking for full
time positions that currently do not exist.
• No (4 hospitals)
14
Are there significant human resources gaps for nurses?
Participation in Medical Education/Training
• Significant involvement in training programs and CME training at all levels
(nursing, Ophthalmic technicians, undergraduate MD, Residency,
Fellowship)
• Rotating medical and nursing students do attend the O.R. on occasion
• Academic Health Sciences Center with training of undergraduate medical
students, ophthalmology residents, residents from other disciplines such as
emergency, family medicine, dermatology, plastic surgery. Fellowship
training in retina, cornea, oculoplastics and ophthalmic pathology. TOH has
partnered with University of Ottawa and trains ophthalmic medical
technologists for years 3 and 4. These students graduate with a BSc in
Ophthalmic Medical Technology.
• Medical students
• No (3 hospitals)15
How does the hospital support CME credits?
• Surgical rounds weekly, presentations at Pediatric Grand Rounds, funding
support for conferences.
• One dedicated CME day per month for all physicians and services, no grand
rounds from WDMH
• CME through sponsored events
• There are weekly Grand Rounds held on site and webcast to members
(physicians, nurses, techs) off the primary site. 2 large conference rooms for
Journal Club and Department meetings. Financial funds come from a
Department Practice Plan and TOHAMO AFP funding. Historically industry
funds provided support but to streamline this has been transferred to TOH
Foundation and is in early stages of implementation.
• Grand rounds (2 hospitals)
16
On Call Emergency Coverage
• 24/7 on-call coverage for consults and O.R.
• No ophthalmologists on call pts sent back to Ottawa if emergency, all other
service have on call coverage a percentage of the time
• Coverage is through the ED and TOH ophthalmology on call.
• Staff ophthalmologist and retina call schedule 24/7 365 days per year. 2-3
residents on call to support staff physician.
• To call or present to the emergency room - 24/7 coverage is available
• On call team of nurses for emergencies, ophthalmologist will use the clinics
during evening if needed
• 80% of HOC coverage by our ophthalmologists
17
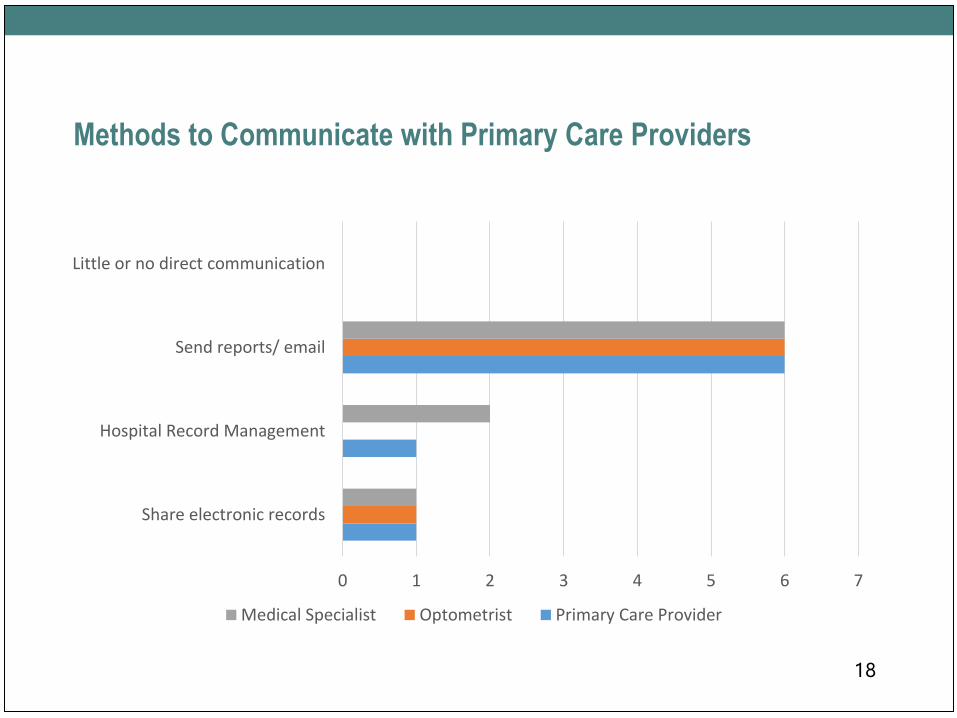
Methods to Communicate with Primary Care Providers
18
0 1 2 3 4 5 6 7
Share electronic records
Hospital Record Management
Send reports/ email
Little or no direct communication
Medical Specialist Optometrist Primary Care Provider
Interest in Regional Programs
• 5 hospitals interested in patient order sets
• 6 hospitals interested in regional program for QBPs
19

Non-Insured Services Provision and Fees
20
# Hospitals Surgeon's Fees
Hospital Admin
Fees
Specialty intraocular lenses 5 0 1X $75
Clear lens extraction for refractive purposes 0Laser assisted cataract surgery 0
Corneal cross-linking 1 $1500IOL master 2 1X$100 2X$100HRT 1 100
Refractive laser vision correction 1 $500 $1500
Cosmetic surgery (e.g. blepharoplasty) 1
Systems in Place to Track Quality Assurance Issues Such as
Postop Complications/Events
• Infection Prevention and Control monitoring, direct follow-up and care as required
• Complaints, surgical site infections
• None
• Full implementation of Surgical Safety Check List and near misses are recorded.
Endophthalmitis rates are tracked for entire Champlain LHIN as all are directed to
retina services at TOH. Each endophthalmitis case is reviewed as part of standing item
at Eye Care Executive meetings. Track posterior capsular breakage. Access Patient
Safety Learning System for patient incidents. Ophthalmic cases that return to the
operating room within 24 hours are reviewed monthly by Chief of Department.
• Physician feed back/ near miss event process, event review with disclosure
• Decision support repository
• Physician will self-report
21
Feedback From Patients
• Significant negative feedback from families and referring providers regarding
Wait 1.
• Positive feedback regarding wait time (3 hospitals)
• No complaints about cataract wait times. Patients with severe visual loss are
accommodated to obtain more rapid access either by the individual surgeon
reorganizing their OR list or sending to another surgeon. All consults are
triaged as to access for wait 1. However with the greater number of patients
seen at internal TOH clinics there have been complaints of excessive wait
(i.e. 2 hours or more) especially in clinics that are used to treat emergency
cases. These emergency cases are variable in number and thus scheduling can
be a challenge for previously booked patients.
• Always have heard positive feedback from patients about care received from
the surgeon and hospital care.
22
Summary of Key Issues and Challenges
• Wait times for initial consult, significant variation in Wait 2 between surgeons due to the
need for in-house (hospital and emergency) coverage
• Lean initiatives have shown staff to be working at maximal efficiency. Investment
required to increase throughput.
• Dated equipment (3 hospitals) - Capital costs curtailed and new equipment often requires
external fundraising. Fiscal reality limits our ability to remain at forefront of technology.
• OR capacity has not followed population growth. Most future growth will need to be
supported by eye care professionals in the community.
• OR access limits new ophthalmologists coming into the region.
• Staffing (2 hospitals) - Increasing financial pressures (cost per weighted case) and
increased efficiency goals are stressing OR capacity and wearing on nursing and physician
well being. Absenteeism places further stress on system as replacements not easily found.
• Decreased allocations lead to increased wait times (2 hospitals)
23*Additional details available in Appendix
Additional DataCurrent Status of Ophthalmology Services
in Champlain
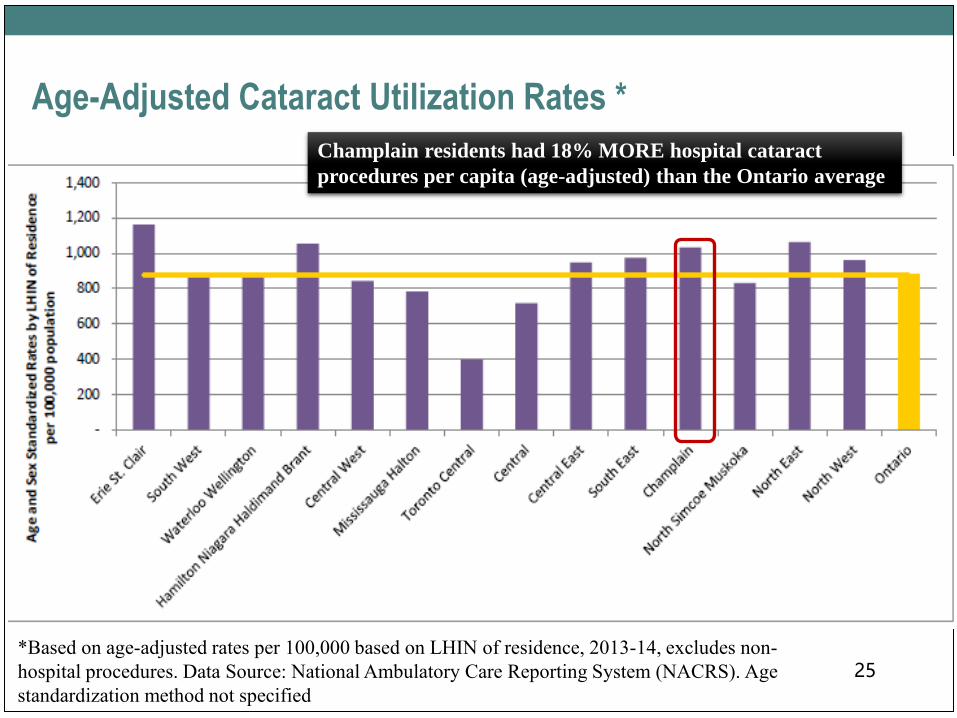
Age-Adjusted Cataract Utilization Rates *
25*Based on age-adjusted rates per 100,000 based on LHIN of residence, 2013-14, excludes non-
hospital procedures. Data Source: National Ambulatory Care Reporting System (NACRS). Age
standardization method not specified
Champlain residents had 18% MORE hospital cataract
procedures per capita (age-adjusted) than the Ontario average
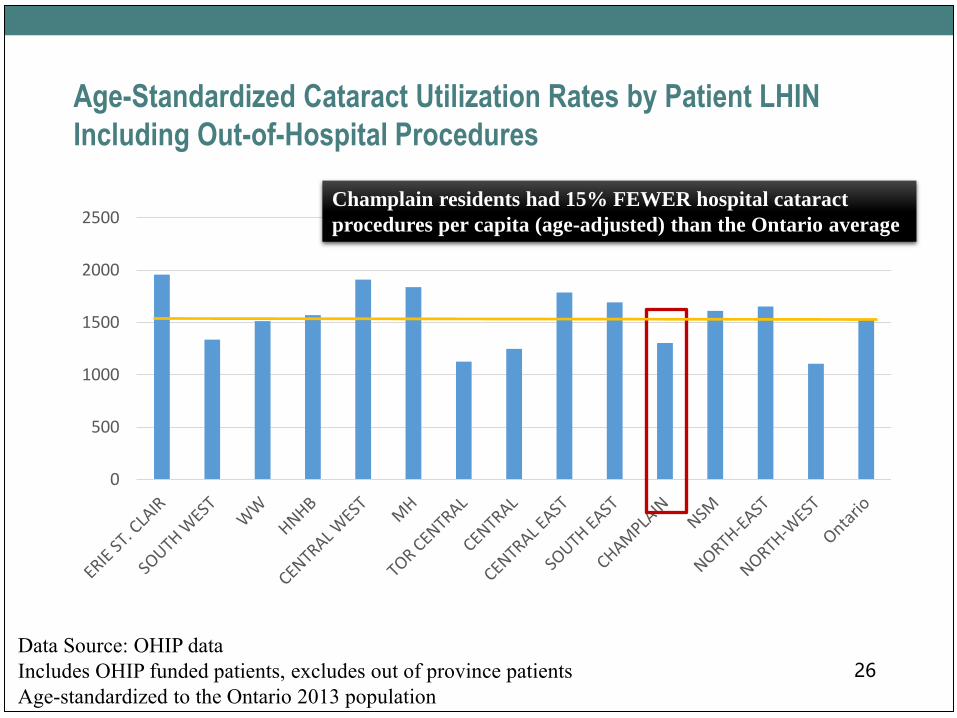
Age-Standardized Cataract Utilization Rates by Patient LHIN
Including Out-of-Hospital Procedures
26Data Source: OHIP data
Includes OHIP funded patients, excludes out of province patients
Age-standardized to the Ontario 2013 population
0
500
1000
1500
2000
2500Champlain residents had 15% FEWER hospital cataract
procedures per capita (age-adjusted) than the Ontario average
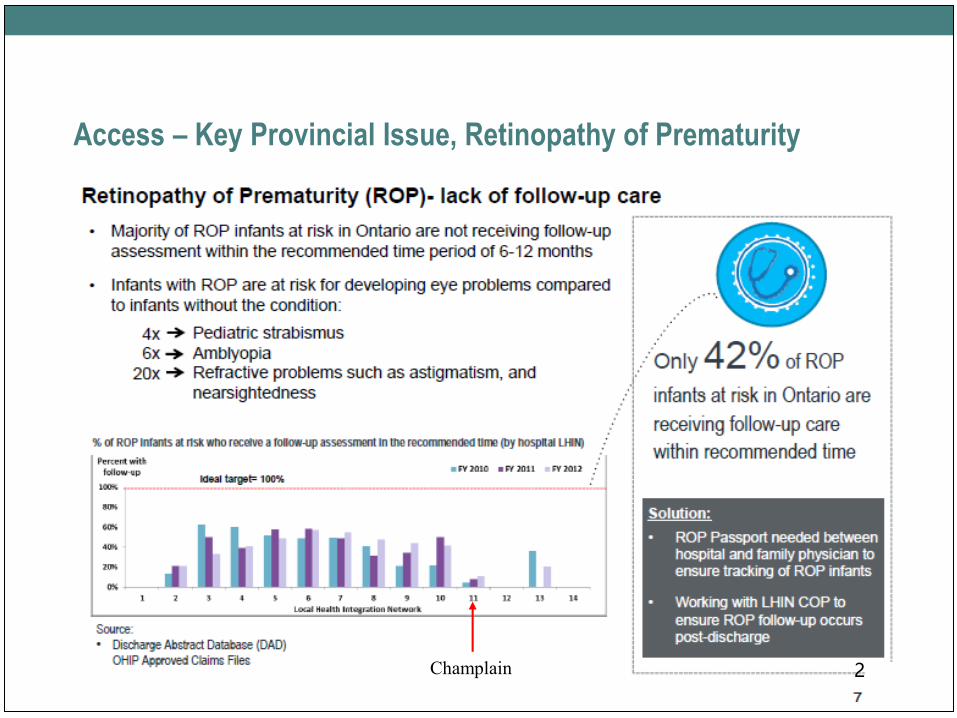
Access – Key Provincial Issue, Retinopathy of Prematurity
27Champlain
Retinopathy of Prematurity
• Bruce to provide
28
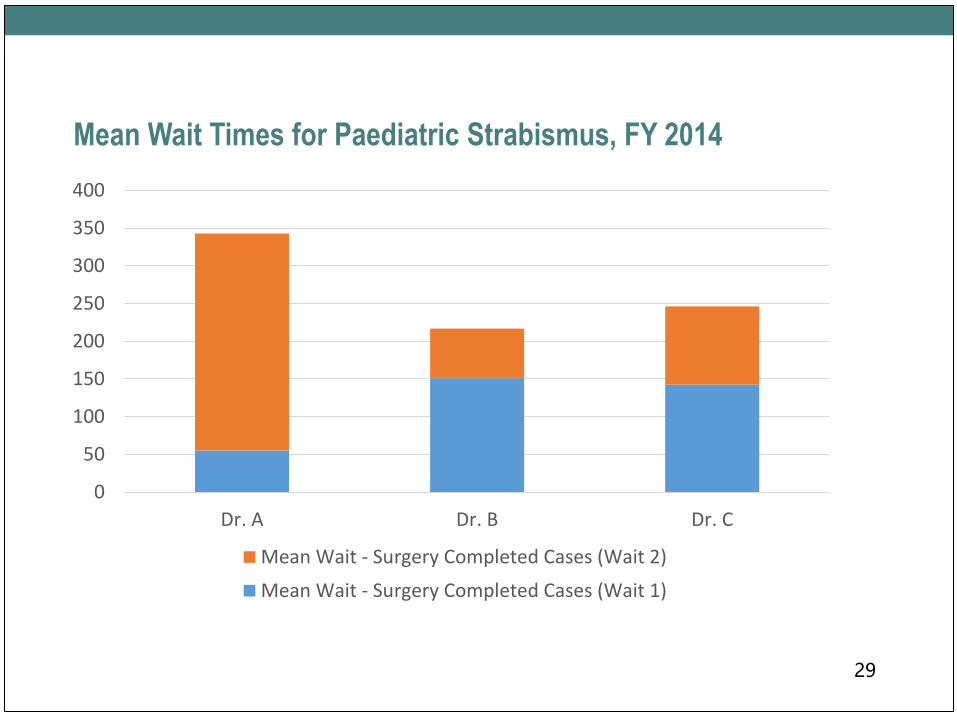
Mean Wait Times for Paediatric Strabismus, FY 2014
29
0
50
100
150
200
250
300
350
400
Dr. A Dr. B Dr. C
Mean Wait - Surgery Completed Cases (Wait 2)
Mean Wait - Surgery Completed Cases (Wait 1)
Diabetes Population Data
• Mitsi to provide
30
Discussion
• What do you see as the strengths, issues and gaps in the region?
• What do you consider to be the priorities for developing a vision plan
moving forward?
31
AppendixDetailed Survey Results
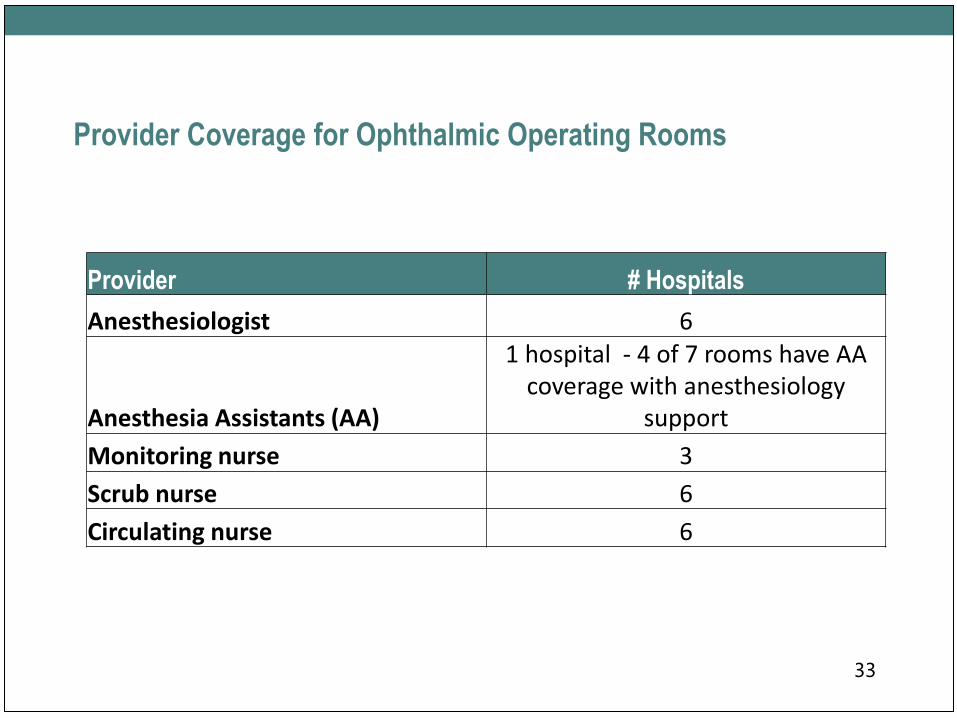
Provider Coverage for Ophthalmic Operating Rooms
Provider # Hospitals
Anesthesiologist 6
Anesthesia Assistants (AA)
1 hospital - 4 of 7 rooms have AA coverage with anesthesiology
support
Monitoring nurse 3
Scrub nurse 6
Circulating nurse 6
33
Pre-Op Assessments Detailed Results• Health History and allergy review completed in clinic. Determined if PAU visit required based on anaesthesia
screening tool. RPN and Anesthetist in Pre-op clinic all general and regional surgical patients are seen by a
nurse and an anesthetist at pre-op approx 2 weeks prior to OR date. All cataract pts have a physical assessment
done by GP prior to surgery to complete med rec and have a history and physical on the chart. Med rec and
allergy status is completed at time of pre-op clinic. All history and physicals are sent from the surgeon to
booking clerk at same time as the ebooking sheet is sent .
• All general and regional surgical patients are seen by a nurse and an anesthetist at pre-op approx 2 weeks prior
to OR date. All cataract pts have a physical assessment done by GP prior to surgery to complete med rec and
have a history and physical on the chart . Med rec and allergy status is completed at time of pre-op clinic. All
history and physicals are sent fro the surgeon to booking clerk at same time as the ebooking sheet is sent. Yes
all are assessed. All PAU done in house. Cataracts-nurse PAU for first eye. Other anterior segment surgeries-
nurse PAU. Main OR (retina, orbit, complex anterior segment requiring GA-screening tool by physician admin
assistant followed by nursing PAU assessment and anaesthesia consult if triggers hit on screening tool. Minor
OR-no PAU
• Yes all are assessed. All PAU done in house. Cataracts-nurse PAU for first eye. Other anterior segment
surgeries-nurse PAU. Main OR (retina, orbit, complex anterior segment requiring GA-screening tool by
physician admin assistant followed by nursing PAU assessment and anaesthesia consult if triggers hit on
screening tool. Minor OR-no PAU
• Yes, by the Pre-Operative Assessment Nurse
• Pre-operative assessment done by the ophthalmologist in the office prior to the day of surgery34
Monitoring of Wait Times – Cataract Surgery• WTIS monitored for in and out of window (some priority levels are impacted by the
lengthy Wait 1) (CHEO)
• Monthly volumes monitored reports to surgeons quarterly
• WTIS
• WTIS entry for all cataract procedures. Dedicated WTIS coordinator for TOH.
Monthly reports generated by WTIS coordinator and reviewed by Eye Care Committee
Work with coordinator to improve data input by repeated education of admin
assistants. Targeted a few physicians regarding management of office workflow.
• Wait times are reviewed every 2 months to determine patients exceeding wait time.
Discussions with physician and office staff occur should data require a more detailed
discussion.
• Wait Times Management System (Novari Access to Care)
35

Clinical Guidelines Implementation
• Clinical guidelines for cataract surgery are fully implemented at most
facilities with a couple of hospitals reporting a few areas where
guidelines are partially implemented
36
Mechanisms to Assess Patient Satisfaction
37
• NRC Picker (3 hospitals)
• Patient questionnaire
• Rounding in clinics
• Patient can call directly to speak to the OR Manager/Director. If
asked, contact information is provided. Web site provides any patients
with the opportunity to send an electronic complaint/compliment
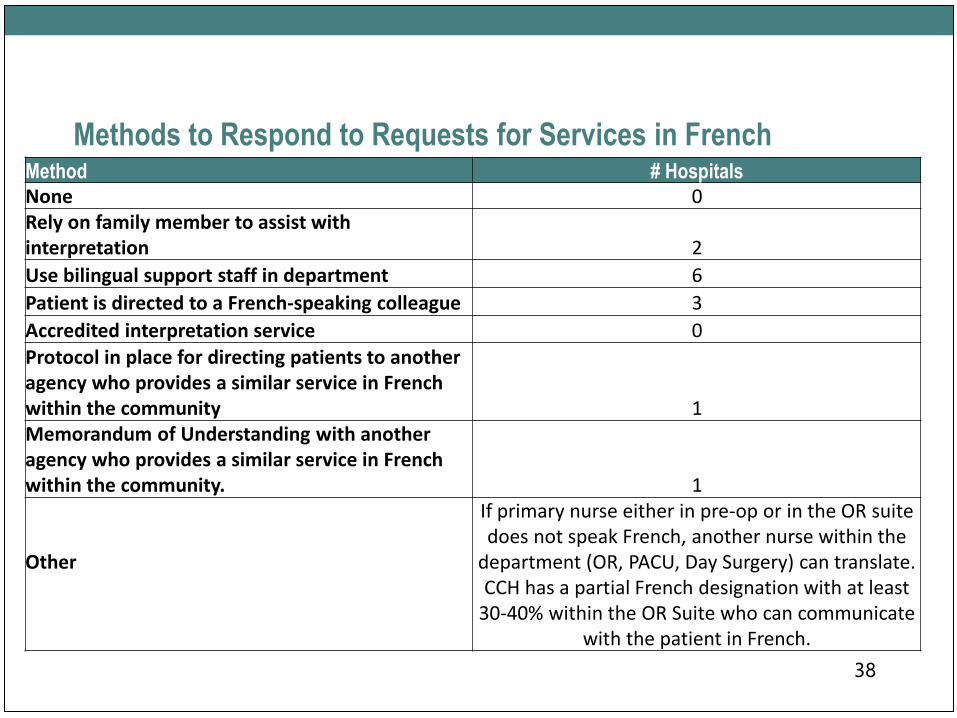
Methods to Respond to Requests for Services in FrenchMethod # HospitalsNone 0Rely on family member to assist with interpretation 2
Use bilingual support staff in department 6
Patient is directed to a French-speaking colleague 3
Accredited interpretation service 0
Protocol in place for directing patients to another agency who provides a similar service in French within the community 1Memorandum of Understanding with another agency who provides a similar service in French within the community. 1
Other
If primary nurse either in pre-op or in the OR suite does not speak French, another nurse within the
department (OR, PACU, Day Surgery) can translate. CCH has a partial French designation with at least
30-40% within the OR Suite who can communicate with the patient in French.
38
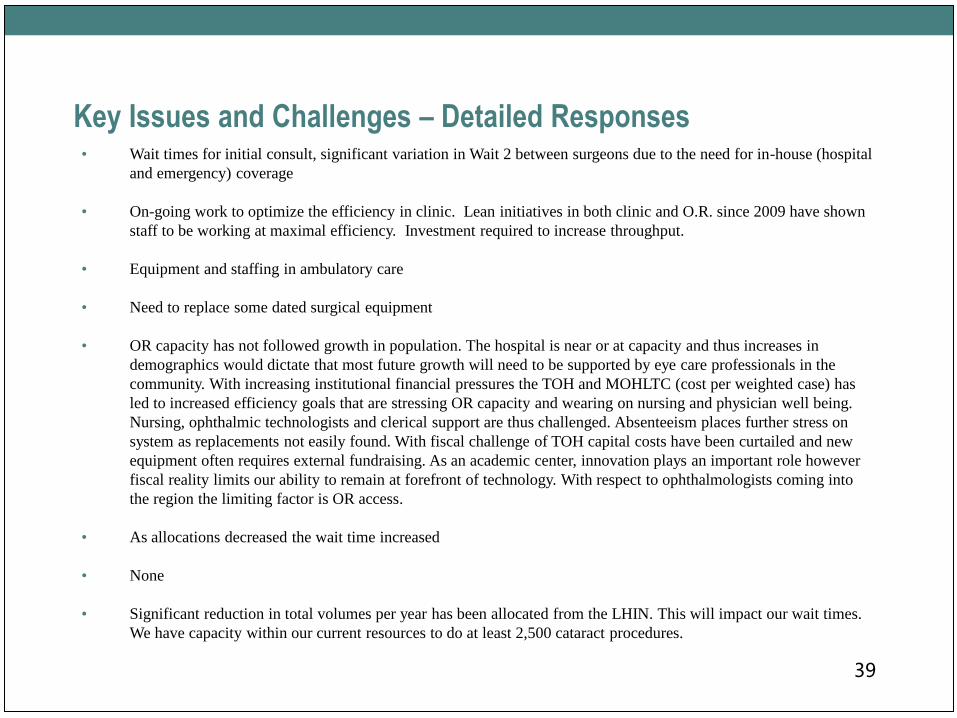
Key Issues and Challenges – Detailed Responses• Wait times for initial consult, significant variation in Wait 2 between surgeons due to the need for in-house (hospital
and emergency) coverage
• On-going work to optimize the efficiency in clinic. Lean initiatives in both clinic and O.R. since 2009 have shown
staff to be working at maximal efficiency. Investment required to increase throughput.
• Equipment and staffing in ambulatory care
• Need to replace some dated surgical equipment
• OR capacity has not followed growth in population. The hospital is near or at capacity and thus increases in
demographics would dictate that most future growth will need to be supported by eye care professionals in the
community. With increasing institutional financial pressures the TOH and MOHLTC (cost per weighted case) has
led to increased efficiency goals that are stressing OR capacity and wearing on nursing and physician well being.
Nursing, ophthalmic technologists and clerical support are thus challenged. Absenteeism places further stress on
system as replacements not easily found. With fiscal challenge of TOH capital costs have been curtailed and new
equipment often requires external fundraising. As an academic center, innovation plays an important role however
fiscal reality limits our ability to remain at forefront of technology. With respect to ophthalmologists coming into
the region the limiting factor is OR access.
• As allocations decreased the wait time increased
• None
• Significant reduction in total volumes per year has been allocated from the LHIN. This will impact our wait times.
We have capacity within our current resources to do at least 2,500 cataract procedures.
39
Vision Care
Community Survey Results
Prepared by Vicky Walker
Event Champlain Vision Care Network Meeting
Date January 12, 2016
Methods
• All community ophthalmology services providers in the Champlain
region were surveyed in October/November 2015 over a 4 week
period
• 19 respondents out of 24 surveys distributed
• 79% response rate
2
Does your facility/office meet the Out of Hospital Premises
(OHP) criteria as per the College of Physicians and Surgeons of
Ontario (CPSO)
3
• Level 1: Local anesthesia (1)
• Level 2: IV Sedation (3)
• Level 3: General Anesthesia (1)

Pediatric Services
4
• 9/19 offices treat paediatric patients of all
ages
• 1/19 offices treat paediatric patients older
than 12 years
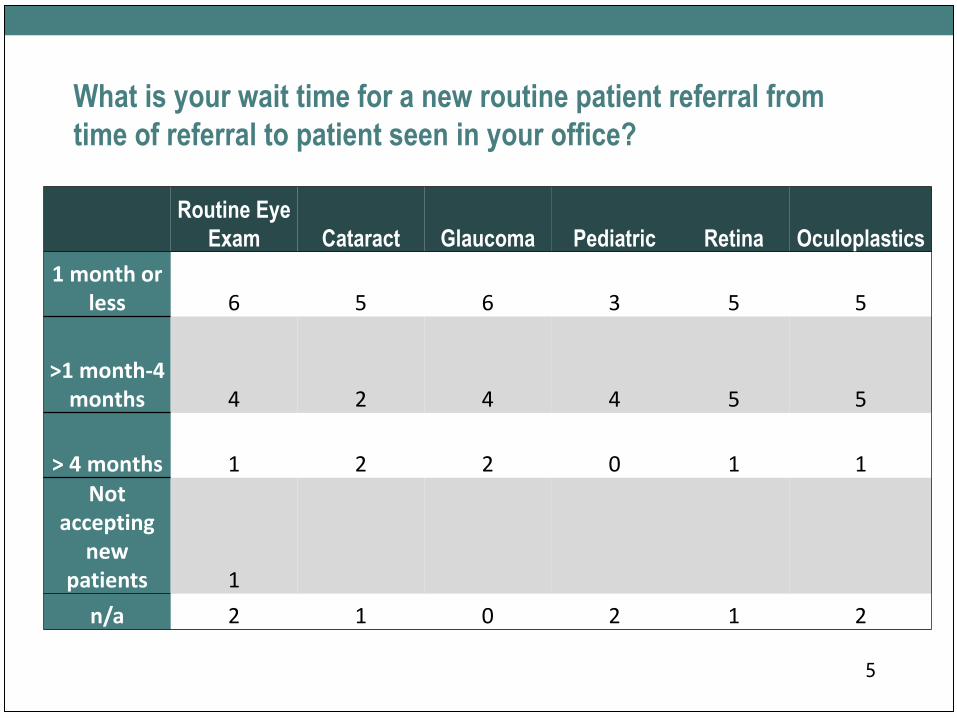
What is your wait time for a new routine patient referral from
time of referral to patient seen in your office?
5
Routine Eye
Exam Cataract Glaucoma Pediatric Retina Oculoplastics
1 month or less 6 5 6 3 5 5
>1 month-4 months 4 2 4 4 5 5
> 4 months 1 2 2 0 1 1Not
accepting new
patients 1
n/a 2 1 0 2 1 2

Surgical Procedures Available
6“Other includes: Lipiflow, dry eyes therapy; blepharoplasty upper and lower lids, brow
lift, lumps and bumps
0 1 2 3 4 5 6 7 8 9 10
Other
LRI Limbal Relaxing incisions
Intraocular injections anti vegF /steriods
Laser procedures for lens opacity PCO
Laser procedures for glaucoma
Laser procedures for retina tears, diabetic…
Phototherapeutic keratectomy ( PTK )
Refractive surgery - Refractive cataract surgery…
Refractive surgery - Laser vision correction…
Corneal cross-linking
Eyelids, nasolacrimal (trauma and non-trauma)…
Clear Lens Extraction, Phakic IOL
Cataract extraction
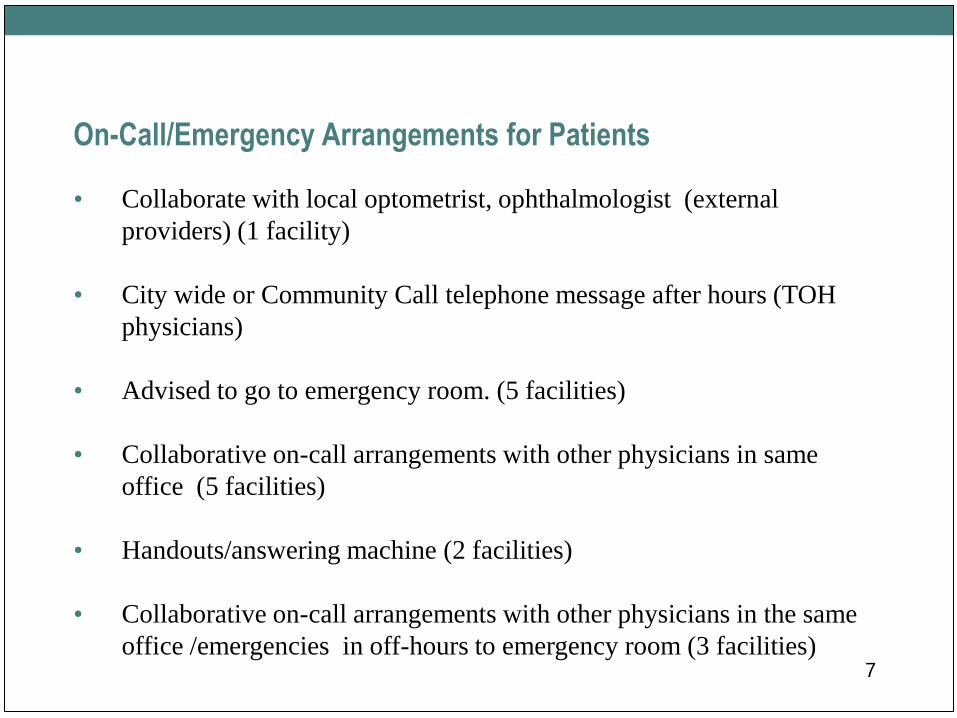
On-Call/Emergency Arrangements for Patients
• Collaborate with local optometrist, ophthalmologist (external
providers) (1 facility)
• City wide or Community Call telephone message after hours (TOH
physicians)
• Advised to go to emergency room. (5 facilities)
• Collaborative on-call arrangements with other physicians in same
office (5 facilities)
• Handouts/answering machine (2 facilities)
• Collaborative on-call arrangements with other physicians in the same
office /emergencies in off-hours to emergency room (3 facilities) 7
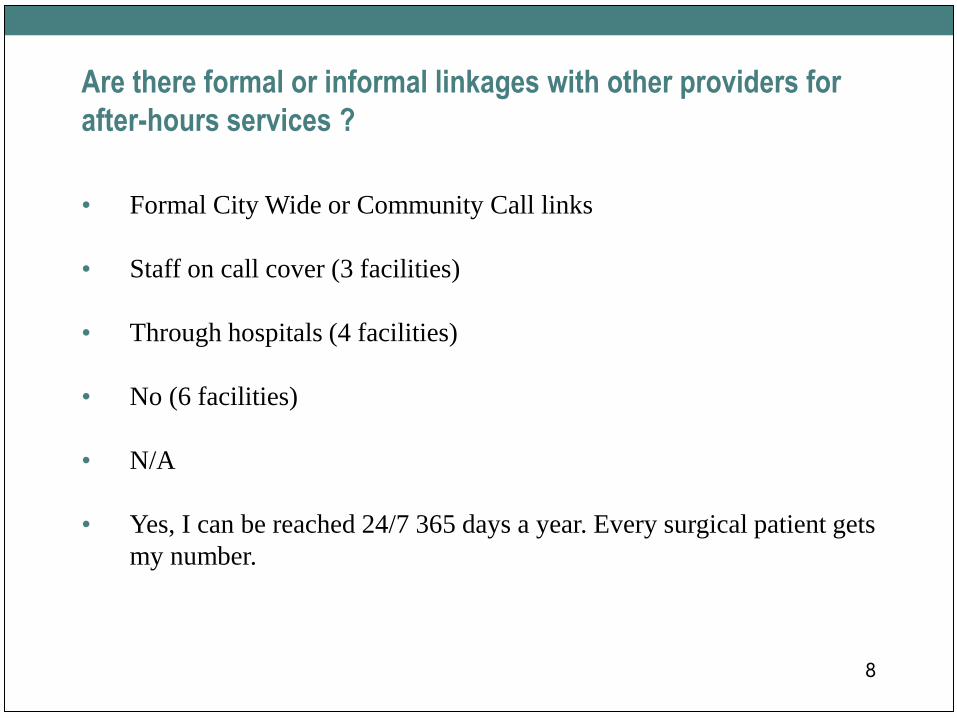
• Formal City Wide or Community Call links
• Staff on call cover (3 facilities)
• Through hospitals (4 facilities)
• No (6 facilities)
• N/A
• Yes, I can be reached 24/7 365 days a year. Every surgical patient gets
my number.
8
Are there formal or informal linkages with other providers for
after-hours services ?
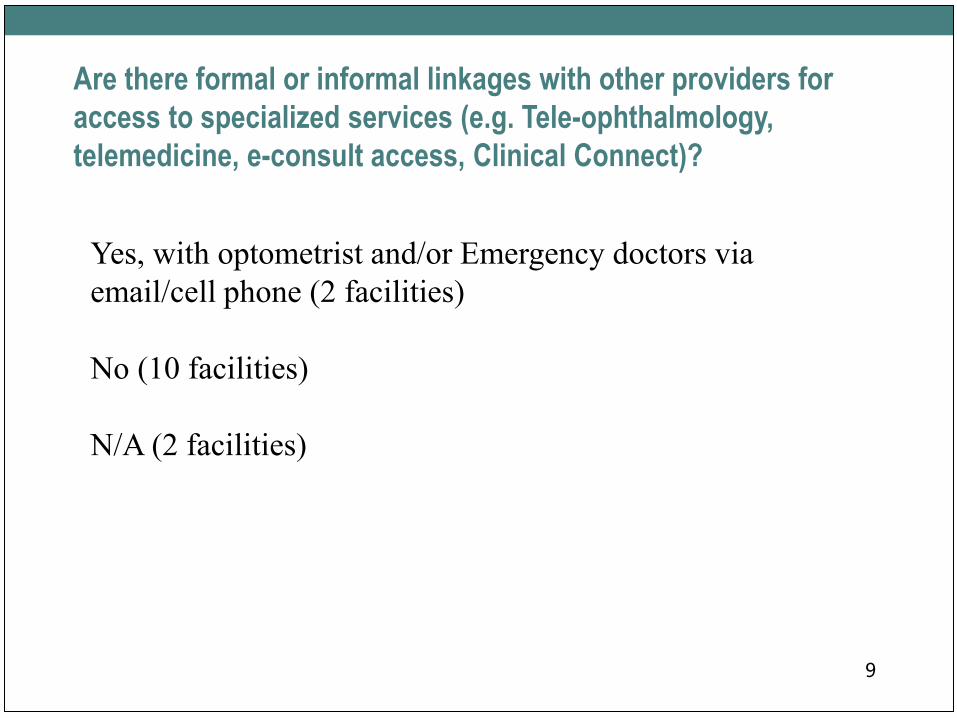
Are there formal or informal linkages with other providers for
access to specialized services (e.g. Tele-ophthalmology,
telemedicine, e-consult access, Clinical Connect)?
9
Yes, with optometrist and/or Emergency doctors via
email/cell phone (2 facilities)
No (10 facilities)
N/A (2 facilities)
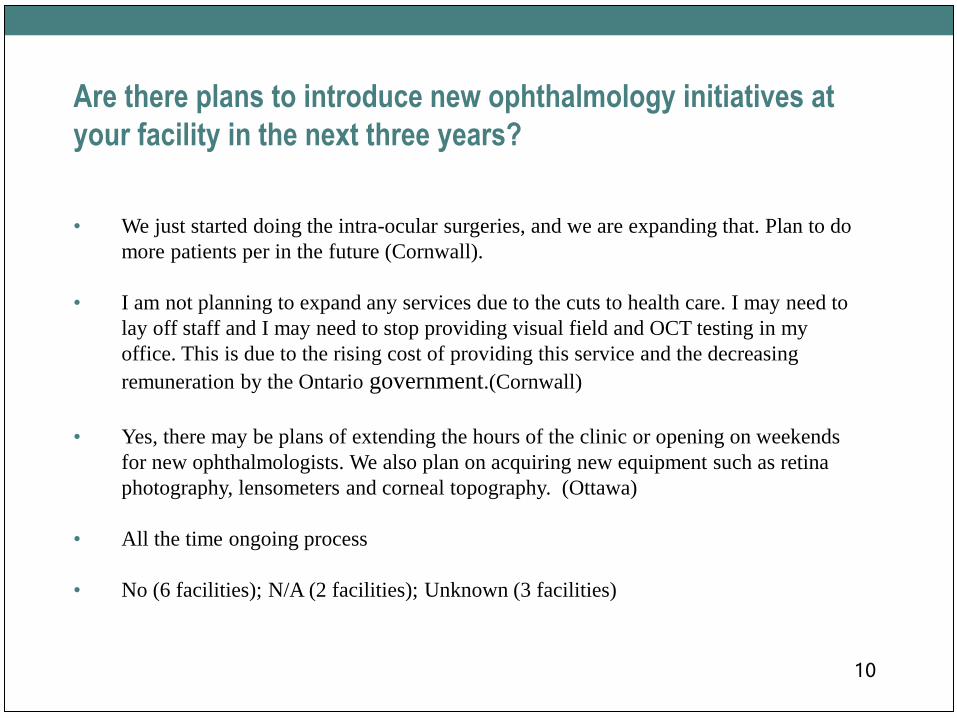
Are there plans to introduce new ophthalmology initiatives at
your facility in the next three years?
• We just started doing the intra-ocular surgeries, and we are expanding that. Plan to do
more patients per in the future (Cornwall).
• I am not planning to expand any services due to the cuts to health care. I may need to
lay off staff and I may need to stop providing visual field and OCT testing in my
office. This is due to the rising cost of providing this service and the decreasing
remuneration by the Ontario government.(Cornwall)
• Yes, there may be plans of extending the hours of the clinic or opening on weekends
for new ophthalmologists. We also plan on acquiring new equipment such as retina
photography, lensometers and corneal topography. (Ottawa)
• All the time ongoing process
• No (6 facilities); N/A (2 facilities); Unknown (3 facilities)
10
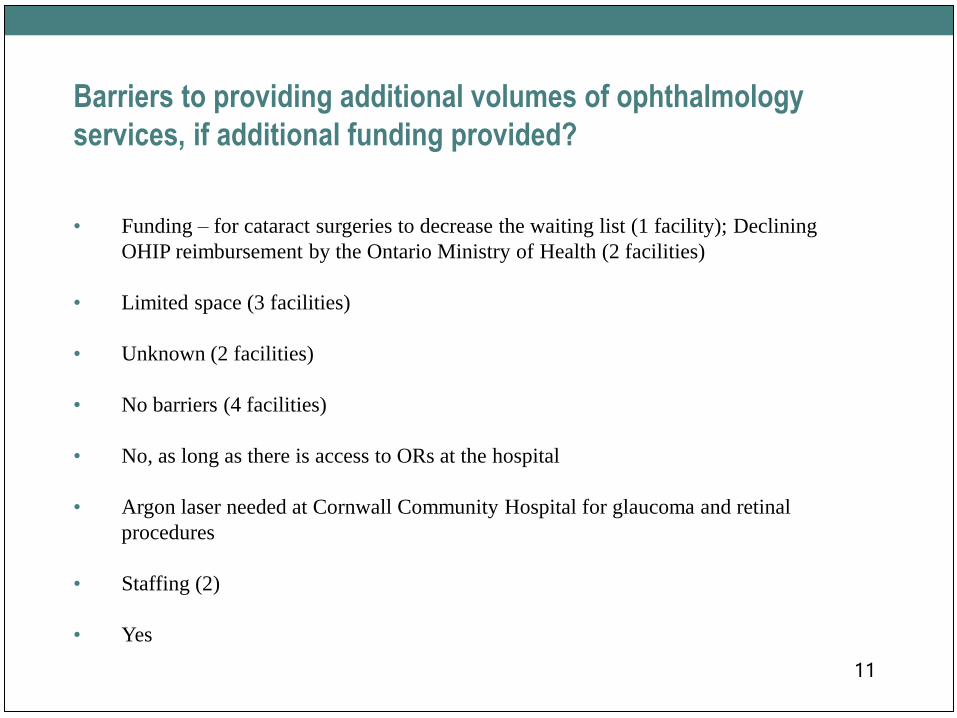
Barriers to providing additional volumes of ophthalmology
services, if additional funding provided?
• Funding – for cataract surgeries to decrease the waiting list (1 facility); Declining
OHIP reimbursement by the Ontario Ministry of Health (2 facilities)
• Limited space (3 facilities)
• Unknown (2 facilities)
• No barriers (4 facilities)
• No, as long as there is access to ORs at the hospital
• Argon laser needed at Cornwall Community Hospital for glaucoma and retinal
procedures
• Staffing (2)
• Yes
11
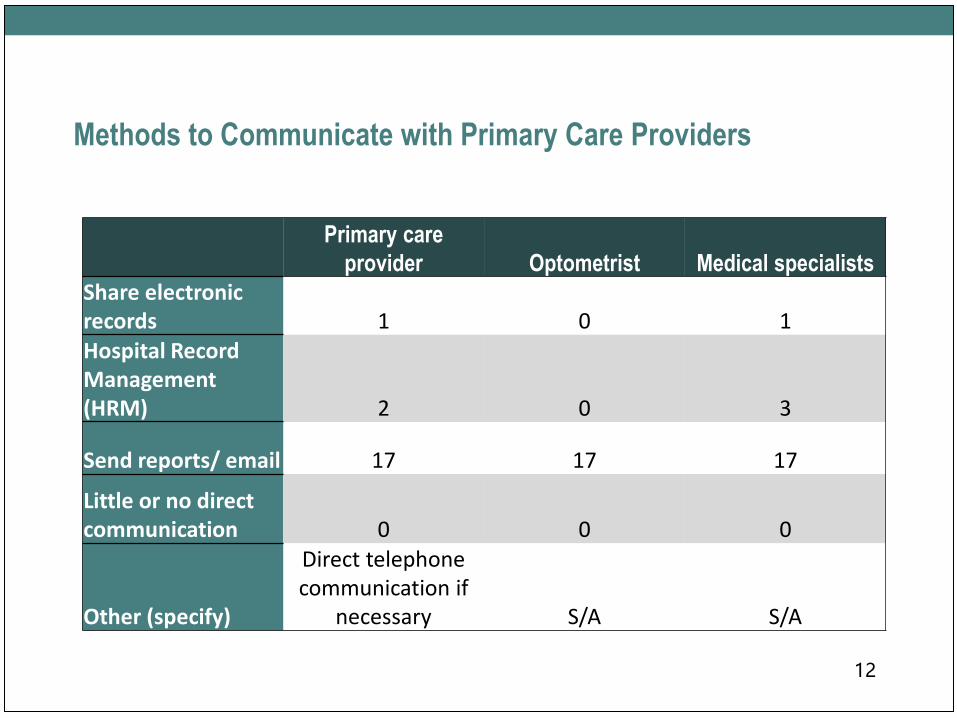
Methods to Communicate with Primary Care Providers
12
Primary care
provider Optometrist Medical specialists
Share electronic records 1 0 1Hospital Record Management (HRM) 2 0 3
Send reports/ email 17 17 17
Little or no direct communication 0 0 0
Other (specify)
Direct telephone communication if
necessary S/A S/A
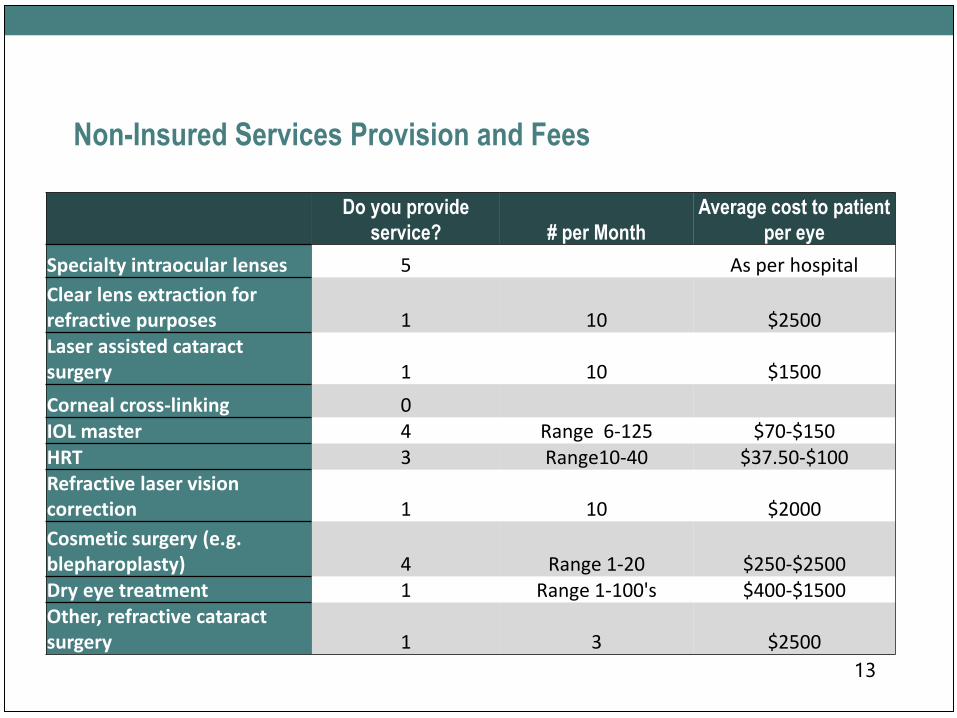
Non-Insured Services Provision and Fees
13
Do you provide
service? # per Month
Average cost to patient
per eye
Specialty intraocular lenses 5 As per hospital
Clear lens extraction for refractive purposes 1 10 $2500Laser assisted cataract surgery 1 10 $1500
Corneal cross-linking 0IOL master 4 Range 6-125 $70-$150HRT 3 Range10-40 $37.50-$100Refractive laser vision correction 1 10 $2000
Cosmetic surgery (e.g. blepharoplasty) 4 Range 1-20 $250-$2500Dry eye treatment 1 Range 1-100's $400-$1500Other, refractive cataract surgery 1 3 $2500
Methods to Obtain Feedback From Patients
• No (6 facilities)
• Informally asking the patient how are they doing after the procedures. (7
facilities)
• Yes via locked suggestion box in waiting room. (1 facility)
14
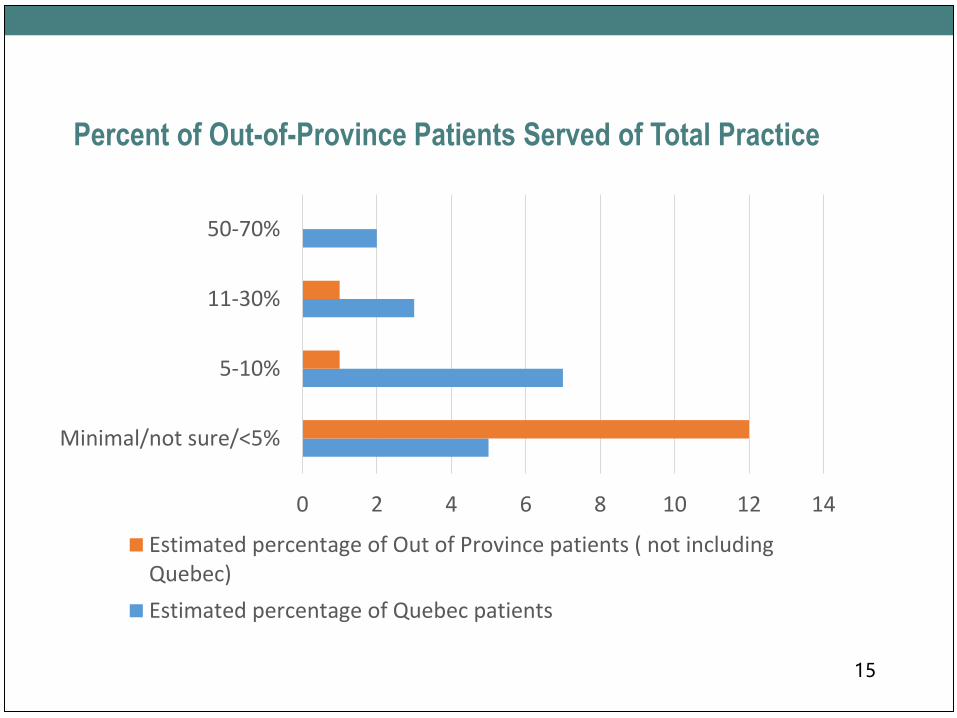
Percent of Out-of-Province Patients Served of Total Practice
15
0 2 4 6 8 10 12 14
Minimal/not sure/<5%
5-10%
11-30%
50-70%
Estimated percentage of Out of Province patients ( not includingQuebec)
Estimated percentage of Quebec patients
Summary of Key Issues and Challenges
• Funding (e.g. OHIP reduction in diagnostic fees) (4 facilities)
• Rising costs and no funding, could lead to closure in the future
• Wait times for surgical procedures and office consultations (4 facilities)
• Limited access to OR at the hospital (2 facilities)
• Ability to recruit ophthalmologists due to cuts in cataract volumes
• Meeting the ever growing needs of the community; Increasing complexity due to aging
population and therefore longer visits
• Limited space (2 facilities)
• Equipment deficiencies
• Purchase of an argon laser required (Cornwall Hospital)
• Equipment that accommodates patients in wheel chairs
16
Are there any initiatives underway to address the vision
screening and care needs of high risk population for patients
with diabetes to have regular retinopathy screening?
• Communication with diabetic clinic on regular basis.
• No (2 facilities)
• Patients are regularly evaluated for diabetes retinopathy (4 facilities)
• Yes
• n/a
17
Are there any initiatives underway to address the vision
screening and care needs of high risk population for vision
screening of children?
• No (3 facilities)
• We see them promptly
• N/A (3 facilities)
• I see all children whether referred or walk-ins
• We do not see children under the age of 12
18
Discussion
• What do you see as the strengths, issues and gaps in the region?
• What do you consider to be the priorities for developing a vision plan
moving forward?
19
Appendix
20
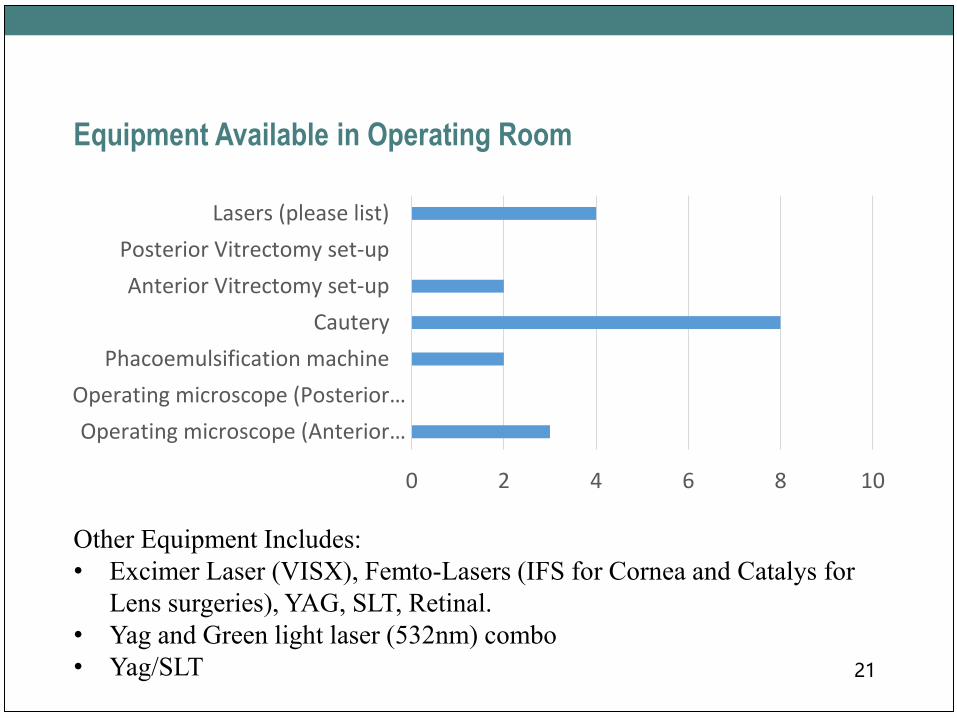
Equipment Available in Operating Room
21
0 2 4 6 8 10
Operating microscope (Anterior…
Operating microscope (Posterior…
Phacoemulsification machine
Cautery
Anterior Vitrectomy set-up
Posterior Vitrectomy set-up
Lasers (please list)
Other Equipment Includes:
• Excimer Laser (VISX), Femto-Lasers (IFS for Cornea and Catalys for
Lens surgeries), YAG, SLT, Retinal.
• Yag and Green light laser (532nm) combo
• Yag/SLT
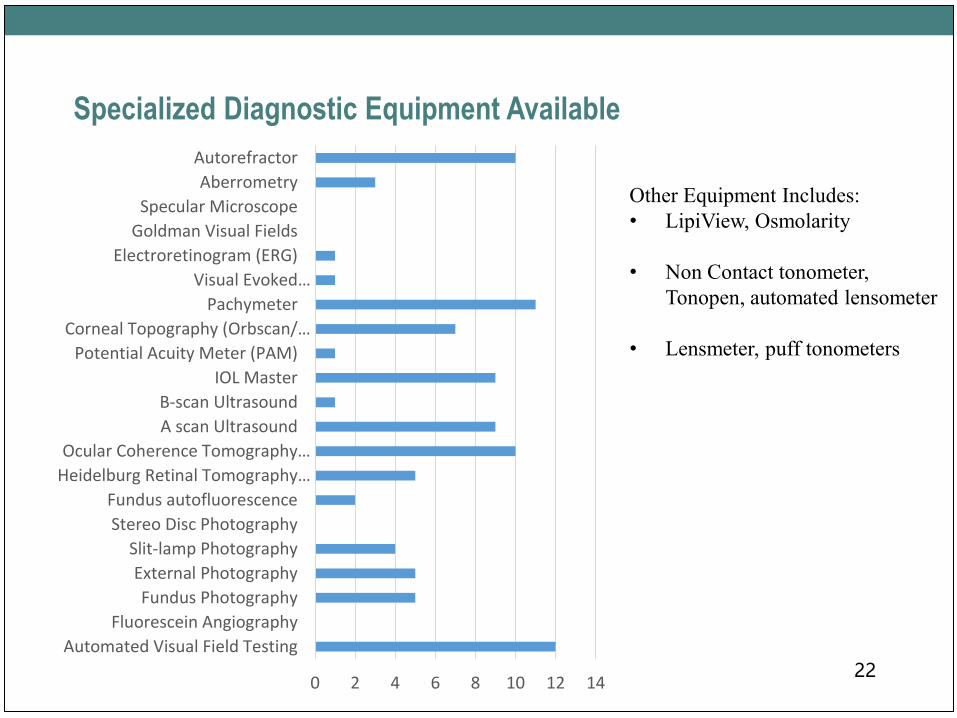
Specialized Diagnostic Equipment Available
22
Other Equipment Includes:
• LipiView, Osmolarity
• Non Contact tonometer,
Tonopen, automated lensometer
• Lensmeter, puff tonometers
0 2 4 6 8 10 12 14
Automated Visual Field Testing
Fluorescein Angiography
Fundus Photography
External Photography
Slit-lamp Photography
Stereo Disc Photography
Fundus autofluorescence
Heidelburg Retinal Tomography…
Ocular Coherence Tomography…
A scan Ultrasound
B-scan Ultrasound
IOL Master
Potential Acuity Meter (PAM)
Corneal Topography (Orbscan/…
Pachymeter
Visual Evoked…
Electroretinogram (ERG)
Goldman Visual Fields
Specular Microscope
Aberrometry
Autorefractor
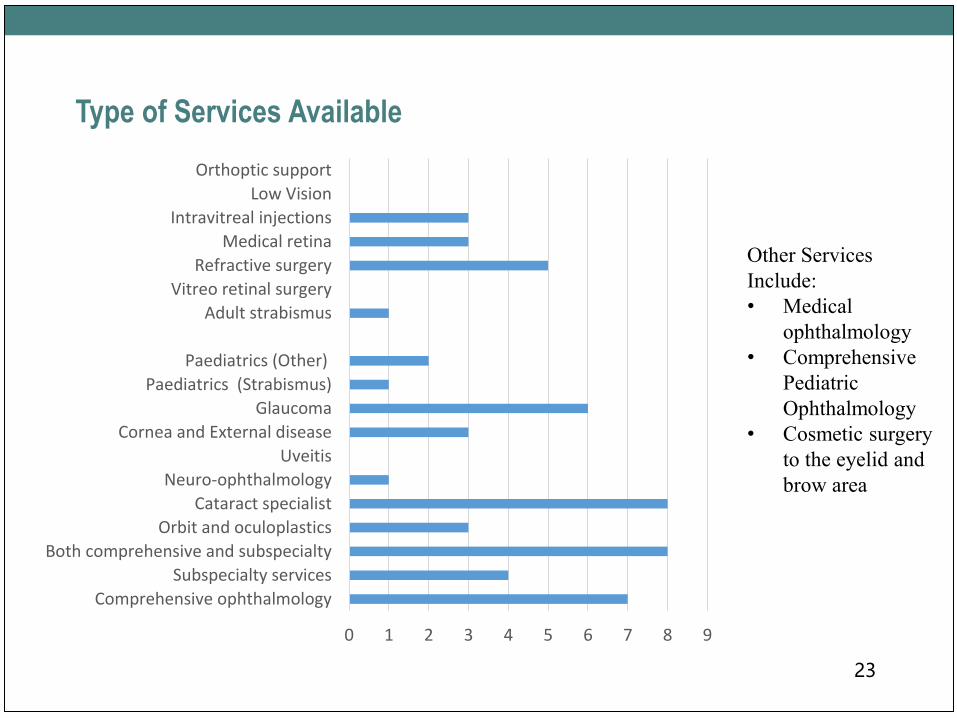
Type of Services Available
23
Other Services
Include:
• Medical
ophthalmology
• Comprehensive
Pediatric
Ophthalmology
• Cosmetic surgery
to the eyelid and
brow area
0 1 2 3 4 5 6 7 8 9
Comprehensive ophthalmology
Subspecialty services
Both comprehensive and subspecialty
Orbit and oculoplastics
Cataract specialist
Neuro-ophthalmology
Uveitis
Cornea and External disease
Glaucoma
Paediatrics (Strabismus)
Paediatrics (Other)
Adult strabismus
Vitreo retinal surgery
Refractive surgery
Medical retina
Intravitreal injections
Low Vision
Orthoptic support
Clinical Handbook Implementation- Surgery
• All organizations indicated that clinical best practices are fully
implemented with only 1 area noted where guidelines are partially
implemented at one organization.
24
Other Comments
• Need cataract surgery funding. We can provide an efficient, cost effective and high end service. We
will be able to cut the waiting list, and at the same time, save money for the MOHLTC.
• In 2012, I made the decision to become strictly an office-based medical ophthalmologist. The main
reason was due to the ever-increasing demands of the hospital regarding on-call duty. The
budgetary restrictions became an issue. If we are going to attract good ophthalmologists in this
province, the hospitals in smaller communities like Cornwall will need to be active participants.
• There is a GREAT need for more operating room time to keep up with our long wait lists in
paediatrics. I serve Ottawa, the Northern Ontario area, and 30% of my Practice is Quebec, Gatineau
and beyond
• There should be a medical directors from an OHP at the LHIN representing us in the Champlain
region as they have the most to offer in guiding the future of healthcare in an affordable manner.
25

68
Vision Care Services
Final Report and
Recommendations
Prepared by Dr. Steve Gilberg, Rosemary Bickerton
Event Board Meeting
Date April 27, 2016
Vision Plan Development Process
• A Vision Care Network was established in Spring 2015
• Data on volume, quality, efficiency, and wait times was extracted
from existing data sources
• 2 surveys (hospitals and community) were conducted
• Focus group of key stakeholders was held to solicit feedback on
quality of services and opportunities for improvement
2
Committee Membership
Thanks to all of our Committee members who participated:
3Project Manager: Rosemary Bickerton, The Ottawa Hospital
Champlain LHIN Representatives: Eric Partington, Elizabeth Woodbury, Vicky Walker
Dr. Steven Gilberg – co-chair Mario Bédard
Head, Department of Ophthalmology, The Ottawa HospitalClinical Director, Pharmacy & Eye Care Program, The Ottawa
Hospital
Jeanette Despatie – co-chair Lucille Perreault
CEO, Cornwall Community HospitalVice-President, Clinical Programs and Chief Nursing Executive,
Hôpital Montfort
Dr. Bernie Hurley François Lemaire
Assistant Professor of Ophthalmology, The University of Ottawa,
Vitreo-Retinal Surgeon, The Ottawa Hospital
Vice-President Patient Services - Acute Care and Chief Nursing
Executive, Pembroke Regional Hospital
Dr. Christine Suess Dr. Ali Shoughary
Chief of Ophthalmology Service, Cornwall Community Hospital Ophthalmologist Surgeon, Pembroke Regional Hospital
Dr. Steven Poleski Dr. Walter Delpero
Chief, Ophthalmology Unit, Hôpital Montfort Ophthalmologist, Winchester District Memorial Hospital
Dr. Annick Fournier Lynn Hall
Chief of Ophthalmology, CHEOSenior Vice-President, Clinical Services / Chief Nursing Executive /
Professional Practice Leader, Winchester District Memorial Hospital
Tammy DeGiovanni Dr. Thomas-A. Noël
Director, Ambulatory Care, CHEO McLeod Optometry Clinic

Pediatric Vision Care Patients - Sophie
• Sophie is a 3 years old patient who has been waiting for strabismus
surgery for over a year. The wait for surgery is stressful for the family
and has put her at risk for:
• Straight eye alignment
• Achieving normal vision
• Developing depth perception
• The sooner she receives surgery, the more likely she will achieve the
best possible vision
4
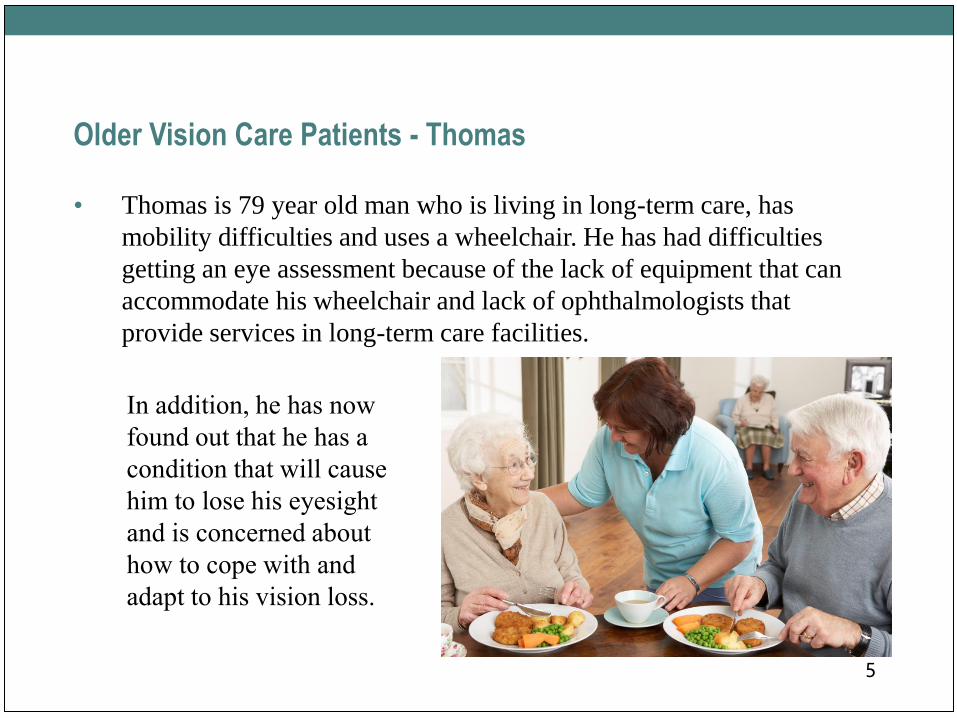
Older Vision Care Patients - Thomas
• Thomas is 79 year old man who is living in long-term care, has
mobility difficulties and uses a wheelchair. He has had difficulties
getting an eye assessment because of the lack of equipment that can
accommodate his wheelchair and lack of ophthalmologists that
provide services in long-term care facilities.
5
In addition, he has now
found out that he has a
condition that will cause
him to lose his eyesight
and is concerned about
how to cope with and
adapt to his vision loss.

Scope of Vision Care Services, 2014-15
6
Hospital Cataract Corneal
Glaucoma
Surgery
Medical
Retina Other Strabismus
Surgical
Retina
Grand
Total
Pembroke 708 6 71 3 788
TOH-
Riverside 8359 84 60 198 54 39 985 9779
TOH-General 1943 331 110 152 1315 191 234 4276
CHEO 22 3 8 2 127 390 10 562
Montfort 2206 31 21 1 32 2291
Winchester 440 1 107 6 1 555
Cornwall 1243 5 87 2 1337
Champlain 14921 465 199 353 2153 629 1232 19952
There were approximately 14,000 patients that required one
or more vision care procedures in 2014-15
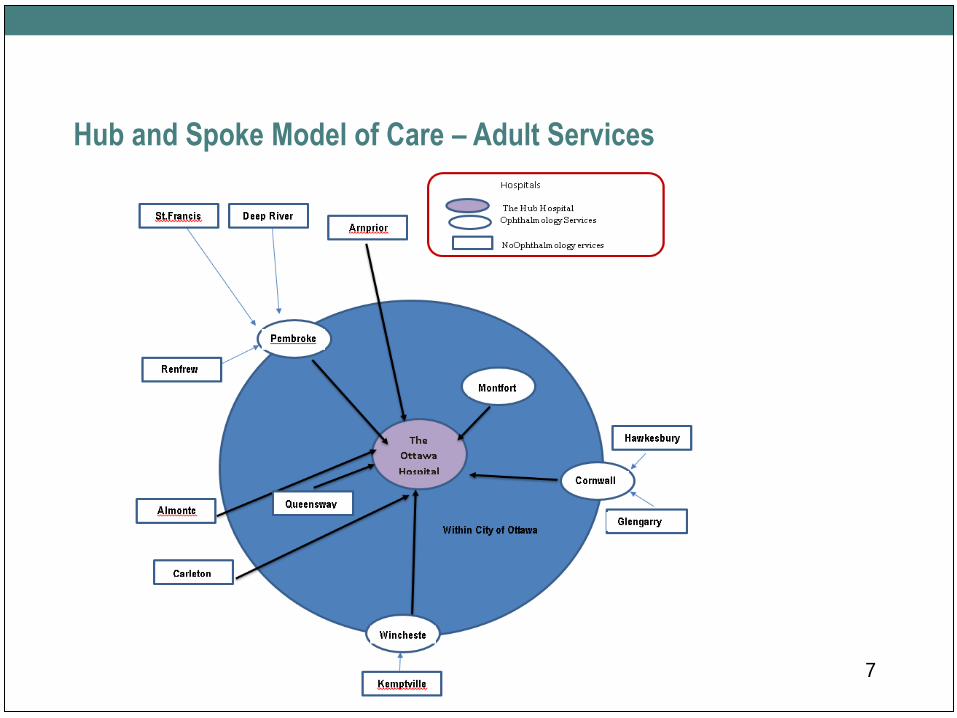
Hub and Spoke Model of Care – Adult Services
7
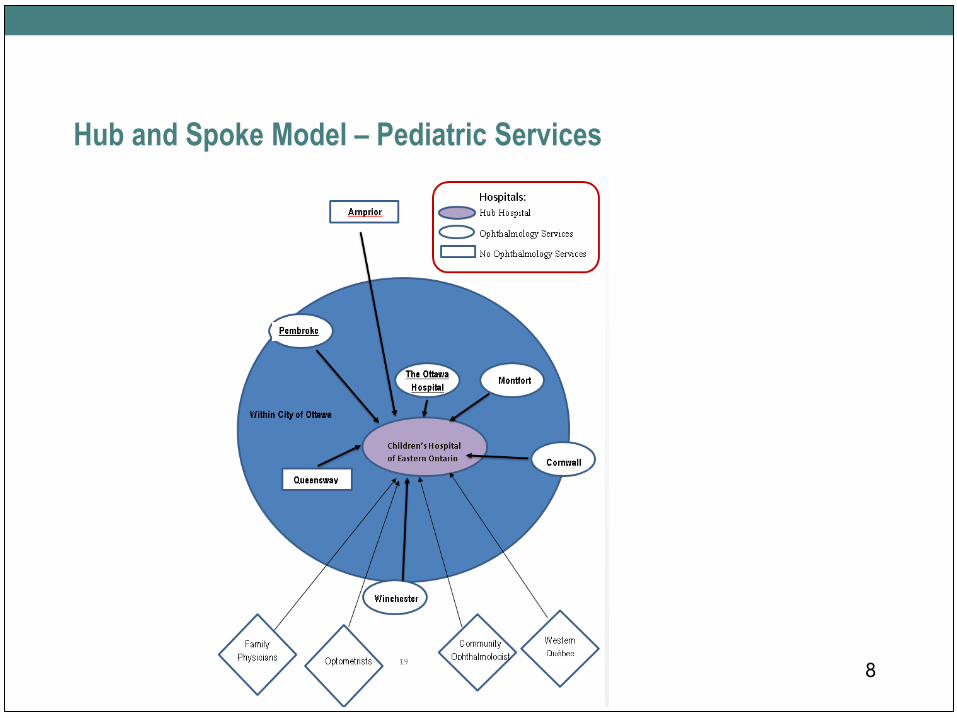
Hub and Spoke Model – Pediatric Services
8
Key Findings
• Current hub and spoke model of care in the region is working well
• Pediatric patients are underserved, wait times for pediatric and adult
strabismus well exceed targets and compare unfavourably with other
LHINs
• Patient waits for cataract surgery times have been slowly increasing
• Recruitment of ophthalmologists is needed to meet present and future
patient needs; and
• Enhanced sharing of patient information is needed to evaluate patient
outcomes and to support communications between hospitals and
community services for the provision of high quality care 9
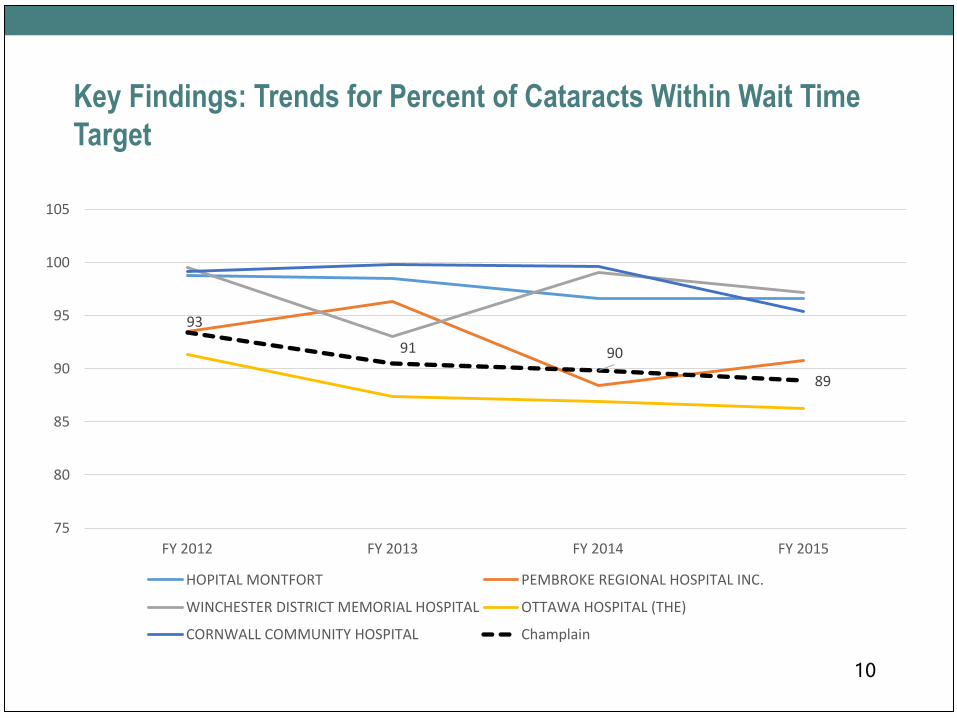
Key Findings: Trends for Percent of Cataracts Within Wait Time
Target
10
93
91 90
89
75
80
85
90
95
100
105
FY 2012 FY 2013 FY 2014 FY 2015
HOPITAL MONTFORT PEMBROKE REGIONAL HOSPITAL INC.
WINCHESTER DISTRICT MEMORIAL HOSPITAL OTTAWA HOSPITAL (THE)
CORNWALL COMMUNITY HOSPITAL Champlain

Key Findings: Quality
• Patient complication rates are low and compare favourably with other
LHINs
• Low rates of follow-up for patients at risk of retinopathy of
prematurity was identified as a concern at the provincial level, but
further analysis identified that no further action is required
• Screening for children and patients with diabetes could be enhanced
• A regional standardized scorecard would facilitate a better
understanding of quality, outcomes and patient satisfaction
11
Summary of Key Recommendations
• Improve patient access to paediatric services by recruiting pediatric
ophthalmologist(s) to address current and future patient needs
• Recruit ophthalmologists to address present and future patient needs using
population-based approach
• Decrease patient wait times by increasing cataract allocation in Champlain
LHIN by 15%
• Improve communication between institutions/providers by developing an
integrated EMR across the LHIN and province
• Standardize provincial monitoring of patient satisfaction for cataract surgery
• Maintain hub and spoke model of delivery
12
Key Recommendations - continued
• Standardize processes for cataract surgery to improve efficiencies /
safety / quality
• Enhance vision screening for children and high risk groups
• Explore opportunities to maintain access to vision rehabilitation
services for patients with vision loss
• Improve patient experience/mental health of patients with vision loss
• Enhance availability of vision services for patients in long term care
• Maintain/enhance provision of French language services
13
Next Steps
• Board Approval of Report
• Send to MOHLTC and Provincial Vision Care Task Group
• LHIN to evaluate scope, cost and human resource requirements of
recommendations pertaining to the LHIN and consider them for
integration into the LHIN’s annual business plan
• Regional Vision Care network to reconvene after formal review of
plan to provide advice on implementation of recommendations
14
Motion
• That the Board approve the Champlain LHIN Vision Care Plan
and requests that the plan be submitted to the Ministry of Health and
Long-Term Care for its consideration of the recommendations.
15
Health System Funding Reform2016-17 Updates
April 27, 2016
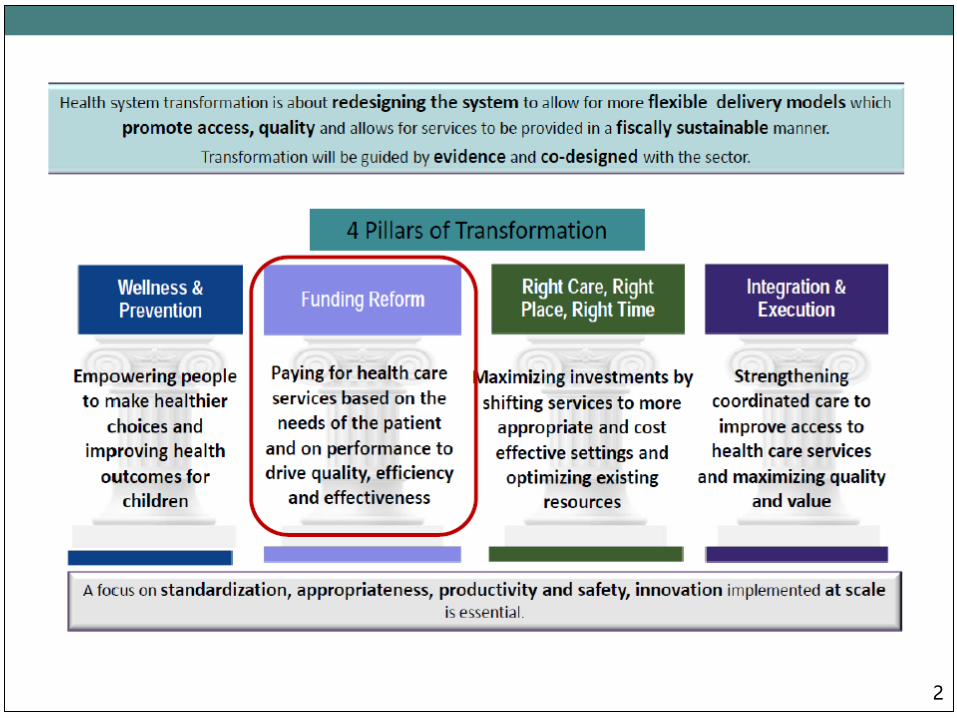
2
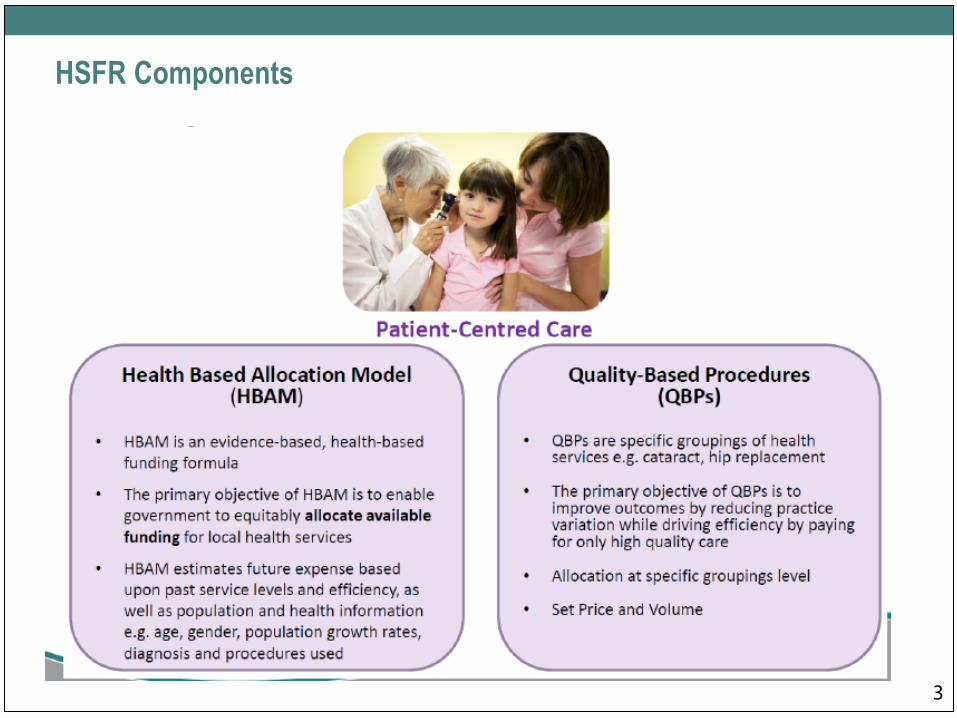
HSFR Components
3
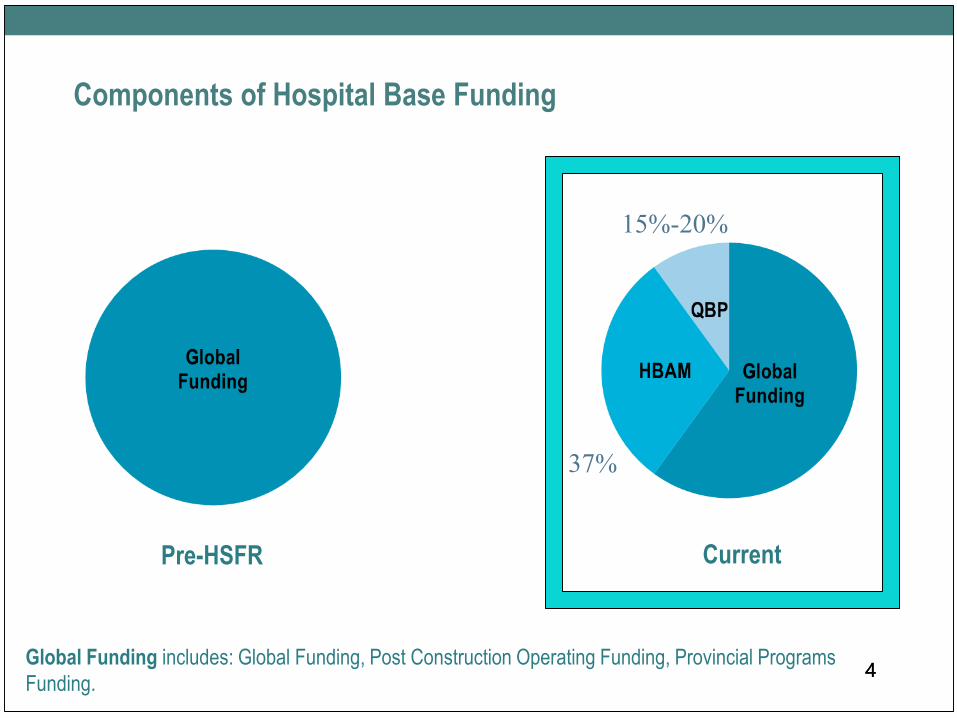
Components of Hospital Base Funding
44
Pre-HSFR Current
15%-20%
37%
Global Funding includes: Global Funding, Post Construction Operating Funding, Provincial Programs
Funding.
Small Hospitals
• Small hospitals continue to be excluded from
reallocation under the Health Based
Allocation Model (HBAM) and continue to
receive funding through the global budget
method
• Small Hospitals received an across the board
1% increase in base funding in 2016-2017.
Total of $ 897,500 in Champlain. Discussions
are in progress for 2017-18.
5
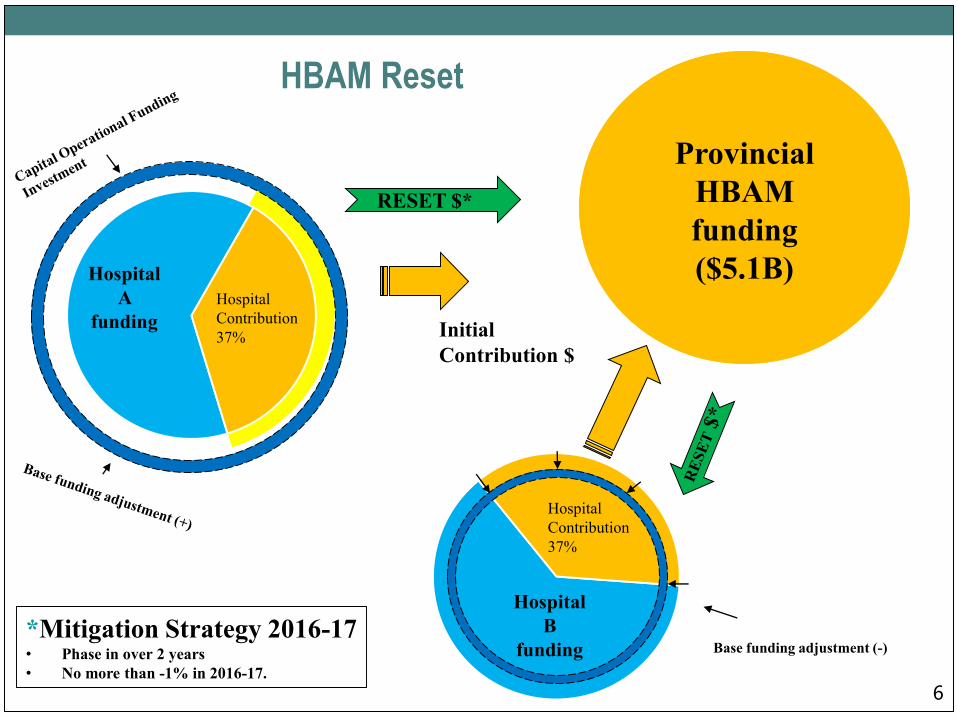
6
HBAM Reset
Hospital
Contribution
37%
Hospital
B
funding
Hospital
A
funding
Hospital
Contribution
37% Initial
Contribution $
Provincial
HBAM
funding
($5.1B)
Base funding adjustment (-)
RESET $*
*Mitigation Strategy 2016-17• Phase in over 2 years
• No more than -1% in 2016-17.
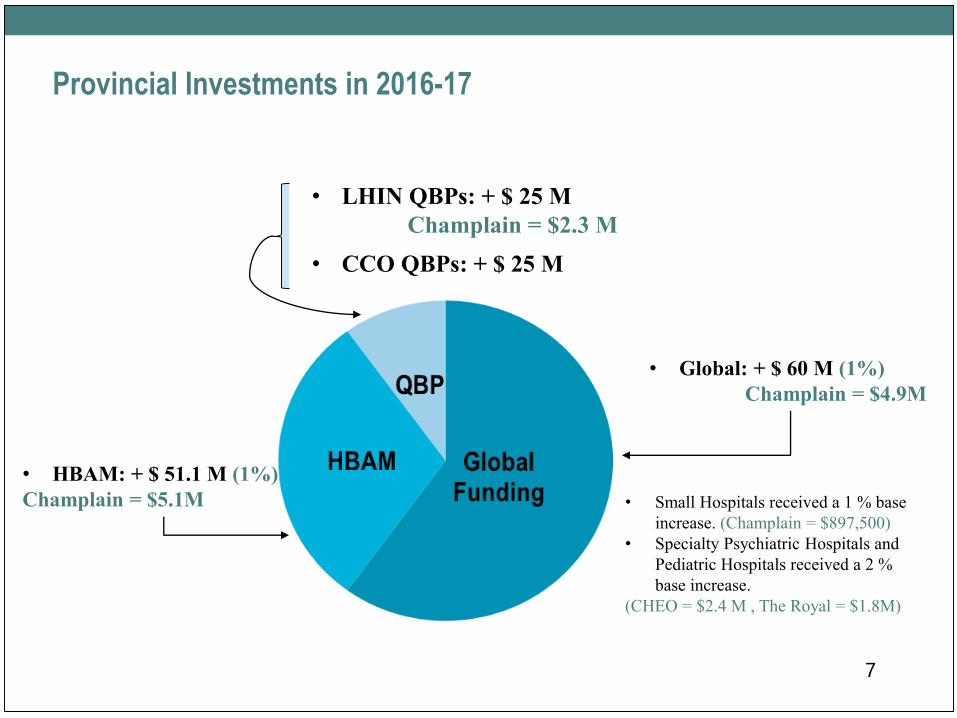
7
Provincial Investments in 2016-17
• LHIN QBPs: + $ 25 M
Champlain = $2.3 M
• CCO QBPs: + $ 25 M
• HBAM: + $ 51.1 M (1%)
Champlain = $5.1M
• Global: + $ 60 M (1%)
Champlain = $4.9M
• Small Hospitals received a 1 % base
increase. (Champlain = $897,500)
• Specialty Psychiatric Hospitals and
Pediatric Hospitals received a 2 %
base increase.
(CHEO = $2.4 M , The Royal = $1.8M)
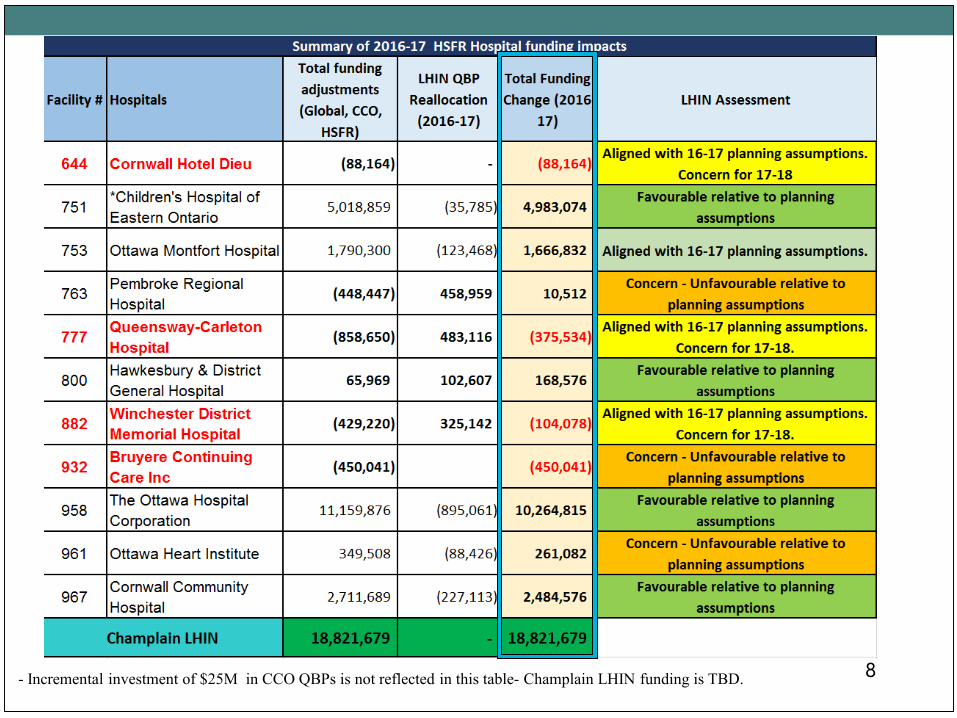
8- Incremental investment of $25M in CCO QBPs is not reflected in this table- Champlain LHIN funding is TBD.
9
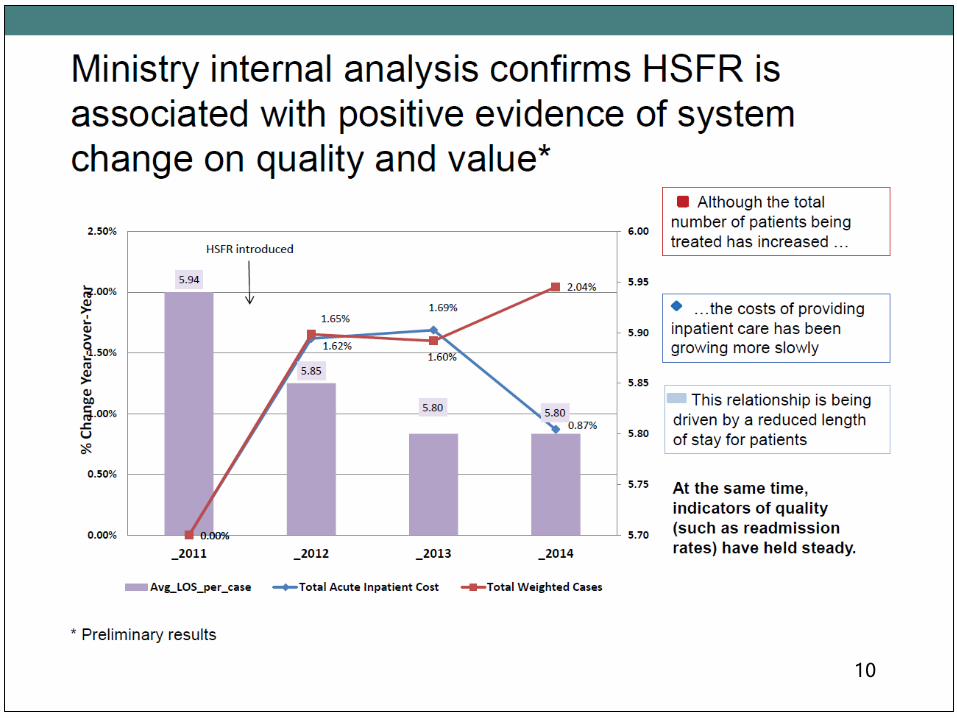
10
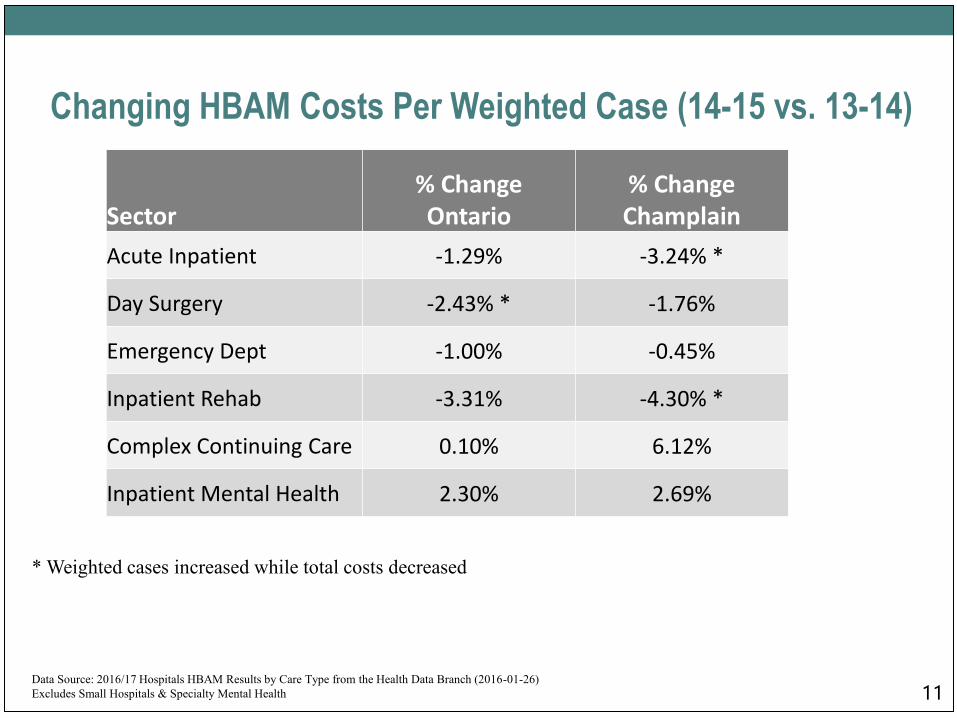
11
Changing HBAM Costs Per Weighted Case (14-15 vs. 13-14)
Sector% Change Ontario
% ChangeChamplain
Acute Inpatient -1.29% -3.24% *
Day Surgery -2.43% * -1.76%
Emergency Dept -1.00% -0.45%
Inpatient Rehab -3.31% -4.30% *
Complex Continuing Care 0.10% 6.12%
Inpatient Mental Health 2.30% 2.69%
* Weighted cases increased while total costs decreased
Data Source: 2016/17 Hospitals HBAM Results by Care Type from the Health Data Branch (2016-01-26)
Excludes Small Hospitals & Specialty Mental Health
Questions ?
12
1900 City Park Drive, Suite 204 Ottawa, ON K1J 1A3 Tel 613.747.6784 • Fax 613.747.6519 Toll Free 1.866.902.5446 www.champlainlhin.on.ca
1900, promenade City Park, bureau 204 Ottawa, ON K1J 1A3 Téléphone : 613 747-6784 • Télécopieur : 613 747-6519 Sans frais : 1 866 902-5446 www.rlisschamplain.on.ca
GOVERNANCE COMMITTEE
April 6, 2016- 3:00 p.m.
Champlain LHIN: Suite 204, Glassroom
1900 City Park Drive, Ottawa
M I N U T E S
In Attendance:
R. Reid (Committee Chair), JP Boisclair (Board Chair), A. Brewer, D. Somppi (via
teleconference), C. LeClerc, C. Martell
1. Call to order & Declaration & Conflict of Interest
The meeting is called to order at 3:00. D. Somppi declares a potential conflict of interest regarding
Pricewaterhouse Coopers.
2. Approval of Agenda
One amendment under item #8: One additional policy will be reviewed addressing social media.
There being no objection, the agenda is approved as amended.
Moved: Jean-Pierre Boisclair / Seconded: Alexa Brewer
All in favour
Carried
3. Consent Agenda:
Approval of Minutes: January 13, 2016 (attachment)
The minutes of January 13, 2016 are amended as follows:
Item 4.2 and 4.3: Correction: Jean-Pierre Boisclair proposes to review (remove to take)
Item 5.1: Remove second paragraph.
There being no objection, the item under the consent agenda is approved as amended.
Moves: David Somppi / Seconded: Alexa Brewer
All in favour
Carried
2
Business Arising from the Minutes:
There is no business arising from the minutes.
NEW BUSINESS
Board Management
4.1 Board Evaluation – Final Report and Next Steps
The final version of the board evaluation 2014-15 was received. There is no major change from
the draft presented in January. Jean-Pierre Boisclair and Randy Reid followed up with the
senior management team and hosted a productive meeting to address a few issues/responses
identified in the survey that differed from the Board’s responses. The practice of in-camera
sessions by the Board was one of the points that differed. A summary report tabulating all in-
camera sessions of the Board and Committees during fiscal year 2015-2016 was provided to the
group. It was felt that agenda items tabled during in-camera sessions were legitimate and that
no decision is taken during in-camera sessions. It was agreed that the new practice of
scheduling in-camera sessions at the beginning of Board meetings is preferable. It enables the
Chair to report in the public domain, when members of the public are present.
The management team and the Board are in agreement with the overall results of the evaluation.
The summary letter of the board’s evaluation results was sent to the Minister last week. It is
agreed that the Board’s evaluation report will not be posted on the website. Randy Reid will
provide a verbal summary during his report at the Board meeting on April 27, 2016 to be
captured in the Board meeting minutes.
4.2 Review Proposed Board Education/Retreat Program 2016-2017
The proposed program is reviewed and will start in May. After discussion it is agreed that the
capital planning topic will be removed from the schedule for this year as it is not an essential
component of the educational requirement for the Board. Another topic will be selected for the
November 2016 education (to be identified at a later date). The group agrees with the program
as amended. They also agree that it is an evergreen program that can be modified by the Chair
or CEO to fulfill the Board’s requirement. It is also agreed that more board retreats may be
added at any time to address the transformation agenda.
Cal Martell shares information regarding a possible upcoming education session on May 2,
2016 for the Champlain LHIN Board and management in Ottawa. This event may be of interest
and beneficial to the Board as it relates to Ethics in Health Care Governance. Details will be
shared with the Board.

3
4.3 Annual Review of Board Meeting Process
The documents shared for the review of board meetings will also be shared with the Board:
Attendance report – Board and committees: The report is satisfactory and the group has
no further comments.
In-camera session summary report: The in-camera meeting practice was discussed
earlier under the Board Evaluation Survey Results for 2014-2015 – see item 4.1. It is
agreed that the Chair will continue to share comments from in-camera sessions in the
public domain. When confidential items relate to difficulties experienced by service
providers, comments may be shared in the public domain by the Chair using a
constructive approach.
Logistical details regarding Board meetings: Based on results provided by members
surveyed, most of our logistical practice will continue as previously established.
Governance Committee Management
5.1 Review Work Plan 2015-16
The work plan was updated at the end of the fiscal year and previously shared with the Board as
part of the annual review. There is no further comments.
5.2 Review Work Plan 2016-17
The work plan and terms of reference were presented to the Board as part of the annual review.
The Governance committee terms of reference are considered evergreen and will be amended if
needed during the course of the present fiscal year to address the transformation agenda. If the
Governance Committee work plan becomes too full during the course of this year, a suggestion
is made that the Community Nominations Committee could help with new member’s
orientation as this committee is well versed in the board’s skills matrix.
5.3 Review Committee’ Performance Survey Results
Was previously distributed via email to committee members in March. All members were in
agreement with the results. Topics for proposed education sessions were added to the program
presented earlier for the current fiscal year.
5.4 Approve Committee’s Annual Report
This annual report was already shared with committee members via email and presented to the
Board as part of the annual review. There is no further comments.
4
Strategic Planning
6 There is no item to be tabled today under strategic planning.
Community Engagement
7 There is no item to be tabled today under community engagement.
Committee Oversight
8.1 Review and Approval of Policies
The group reviews each policy distributed and the following comments are noted:
Policy on Policies: Members are in agreement with the changes -- to have the committee with the expertise and
responsibility for specific policies to review and make recommendation for approval to the
board. The Governance Committee will retain the role of maintaining the inventory of policies
and establishing the timeframe for their review.
Disclosure of Wrongdoing (previously Fraud and Irregularities):
Members are in agreement with the changes -- This policy was created to clarify the intent of the
policy, which is the promotion of an ethical environment that allows for the reporting of any
wrongdoing. The policy content is based upon the Disclosure of Wrongdoing Directive. It
includes the essential elements of identifying and addressing any wrongdoing that has been
recognized. It is clarified that the policy is covered in the orientation process of new LHIN staff
member and that an annual reminder is sent every January to LHIN staff and LHIN Board to
promote the policy and process. ACTION: Darryl Gavard -- It is suggested to add a
reference and a link in the policy and in the annual reminder to the website of the Conflict
of Interest Commissioner for the province of Ontario.
Communications:
Members are in agreement with the changes -- This change was requested by the Board’s French
Language Services committee. The group agrees with the change and no further comments are
provided.
Occupational Health and Safety:
Members are in agreement with the changes -- Statements General Commitment and the Policy
Statement used to be separated and has been edited and combined into one document Policy
Statement. As representatives of the Organization and the Board, the signature of the Board
Chair and CEO are necessary to acknowledge the LHIN’s commitment to Health and Safety.
Governance Code of Conduct: Members are in agreement with the changes -- Minor changes were made to the format and
presentation of the policy. A change was made to the purpose of the policy to make it more
specific.
5
Social Media: This is a new policy. One minor correction is noted on page 6 and the reference to emerging
technologies should be replaced by existing and new technologies. A few other suggestions are
proposed and the policy will be amended. ACTION: Darryl Gavard/Sylvie Bleau.
Discussion follows regarding the application of the policy and examples/clarifications are
provided how the policy would be applied for staff and Board members. The policy is basically
alerting and asking LHIN Board and staff to be cautious, and when in doubt, to consult with
Communications staff before making a comment on social media.
When an education session is provided to LHIN staff on this issue, Board Members will
also be invited. ACTION: Darryl Gavard/Sylvie Bleau.
MOTION:
The Governance Committee recommends the Board approves the policies
mentioned above as amended.
Moved: Randy Reid / Seconded: Alexa Brewer
All in favour
Carried
ACTION S. Bleau: Bring Forward as an agenda item for future discussions of the
Governance Committee relating to the transformation agenda. Topic: The need to establish
mechanisms about ethical decision making (i.e. the need to put in place an independent ethics
officer).
Future Meetings
All meetings will be held from 3 to 5 p.m.:
June 8, 2016 - The group agrees to add this meeting to the approved meeting schedule.
ACTION: Sylvie Bleau will send a calendar invitation to committee
members.
September 7, 2016
November 9, 2016
January 11, 2017
March 1, 2017
There being no further business the meeting concludes 4:40 p.m.
Moved by David Somppi
Randy Reid, Committee Chair
6