apport des - endocardites aquitaine · apport des recommandations européennes gilbert habib...
TRANSCRIPT


Apport des
recommandations européennes
Gilbert HabibCardiology Department- La Timone Marseille - France
Bordeaux le 28 Juin 2011

Infective Endocarditis: a changing disease
new high-risk subgroups
changing microbiology
IVDAelderlyintracardiac devicesnosocomial diseases
changing microbiology
increasing incidence of staphylococcal IEnew microorganisms (Coxiella burnetii, Bartonella spp, Tropheryma whipplei)
more difficult to prevent
more difficult to diagnose
more difficult to treat



IE: new guidelines ESC 2009
1. prevention
2. diagnosis
3. treatment

IE: new guidelines ESC 2009
1. prevention
2. diagnosis
3. treatment

Case report 1




Incidence des bactériémies quotidiennes
Duval X, Leport C. Lancet Infect Dis 2008 ; 8 : 225-32
Adapted from Moreillon Med Mal Infect 2002 ; 32 : 605-12
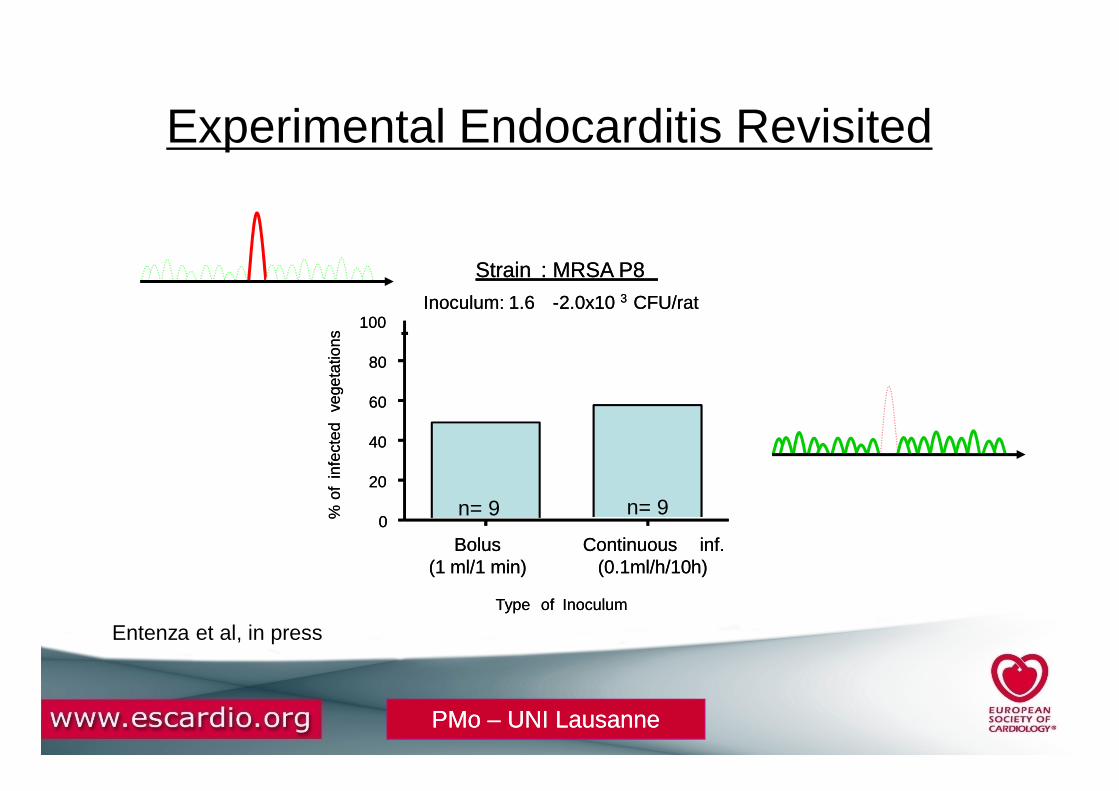
Strain : MRSA P8
Inoculum: 1.6 -2.0x10 3 CFU/rat
60
80
100ve
geta
tions
Strain : MRSA P8
Inoculum: 1.6 -2.0x10 3 CFU/rat
60
80
100ve
geta
tions
Experimental Endocarditis Revisited
Bolus(1 ml/1 min)
Continuous inf.(0.1ml/h/10h)
0
20
40
60
Type of Inoculum
% o
fin
fect
edve
geta
tions
n= 9
Bolus(1 ml/1 min)
Continuous inf.(0.1ml/h/10h)
0
20
40
60
Type of Inoculum
% o
fin
fect
edve
geta
tions
Entenza et al, in press
n= 9n= 9
PMo PMo –– UNI LausanneUNI Lausanne
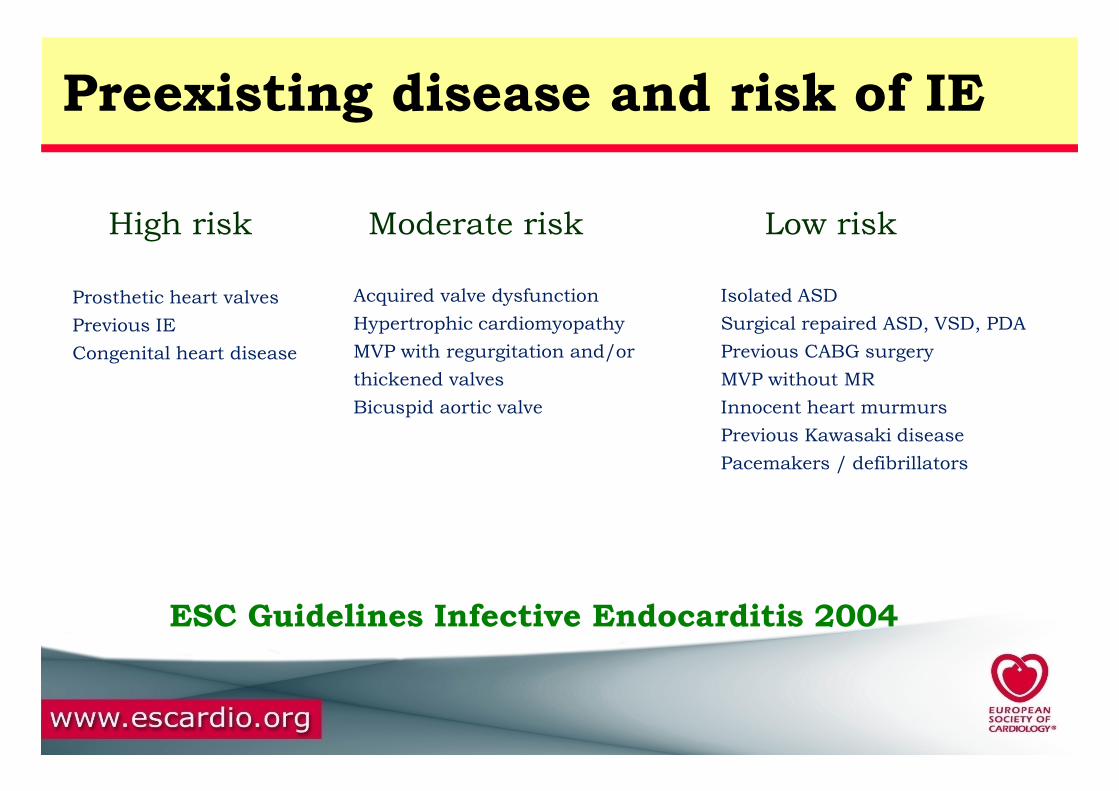
Preexisting disease and risk of IE
High risk Moderate risk Low risk
Acquired valve dysfunction
Hypertrophic cardiomyopathy
MVP with regurgitation and/or
thickened valves
Isolated ASD
Surgical repaired ASD, VSD, PDA
Previous CABG surgery
MVP without MR
Prosthetic heart valves
Previous IE
Congenital heart disease
Bicuspid aortic valve Innocent heart murmurs
Previous Kawasaki disease
Pacemakers / defibrillators
ESC Guidelines Infective Endocarditis 2004
Acquired valve dysfunction
Hypertrophic cardiomyopathy
MVP with regurgitation and/or
thickened valves
Isolated ASD
Surgical repaired ASD, VSD, PDA
Previous CABG surgery
MVP without MR
Prosthetic heart valves
Previous IE
Congenital heart disease
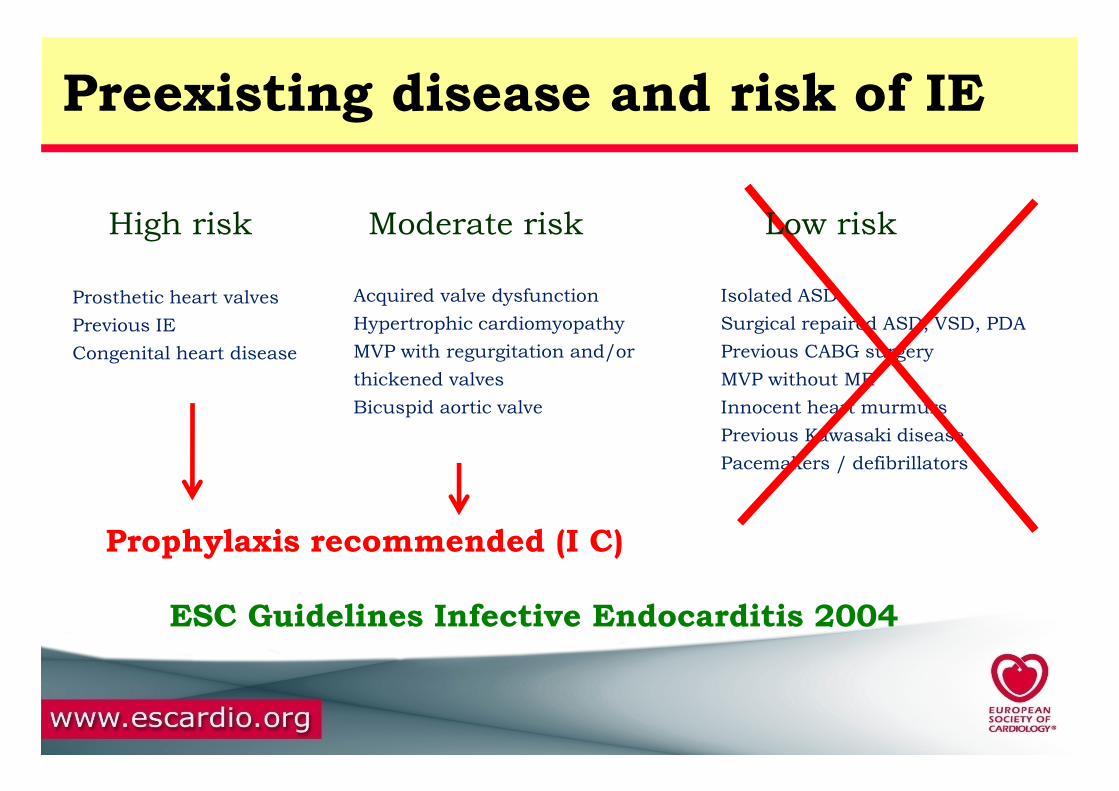
Preexisting disease and risk of IE
High risk Moderate risk Low risk
Bicuspid aortic valve Innocent heart murmurs
Previous Kawasaki disease
Pacemakers / defibrillators
Prophylaxis recommended (I C)
ESC Guidelines Infective Endocarditis 2004

Prosthetic heart valves
Previous IE
Congenital heart disease
Acquired valve dysfunction
Hypertrophic cardiomyopathy
MVP with regurgitation and/or
thickened valves
Isolated ASD
Surgical repaired ASD, VSD, PDA
Previous CABG surgery
MVP without MR
Preexisting disease and risk of IE
High risk Moderate risk Low risk
Bicuspid aortic valve Innocent heart murmurs
Previous Kawasaki disease
Pacemakers / defibrillators
Prophylaxis recommended (IIa C)
ESC Guidelines Infective Endocarditis 2009

Cardiac conditions at highest risk of IE

Procedures at highest risk of IE

IE prevention: main changes
1. The principle of antibiotic prophylaxis when performing procedures at risk
of IE in patients with predisposing cardiac conditions is maintained , but
2. Antibiotic prophylaxis must be limited to patients with the highest risk of
IE undergoing the highest risk dental procedures.
3. Good oral hygiene and regular dental review are more important than
antibiotic prophylaxis to reduce the risk of IE. antibiotic prophylaxis to reduce the risk of IE.
4. Aseptic measures are mandatory during venous catheter manipulation and
during any invasive procedures in order to reduce the rate of health care-
associated IE.
5. Whether the reduced use of prophylaxis is associated with a change in the
incidence of IE must be evaluated by prospective studies
IE prevention: main changes
1. The principle of antibiotic prophylaxis when performing procedures at risk
of IE in patients with predisposing cardiac conditions is maintained , but
2. Antibiotic prophylaxis must be limited to patients with the highest risk of
IE undergoing the highest risk dental procedures.
3. Good oral hygiene and regular dental review are more important than
antibiotic prophylaxis to reduce the risk of IE. antibiotic prophylaxis to reduce the risk of IE.
4. Aseptic measures are mandatory during venous catheter manipulation and
during any invasive procedures in order to reduce the rate of health care-
associated IE.
5. Whether the reduced use of prophylaxis is associated with a change in the
incidence of IE must be evaluated by prospective studies

Reco ESC 2010
Une bonne hygiène dentaire et un suivi dentaire régulier sont recommandés chez les patients à risque
Le piercing et les tatouages doivent être évités chez ces patients, surtout les piercings intéressant les muqueuses.patients, surtout les piercings intéressant les muqueuses.
Des mesures d’asepsie rigoureuse sont recommandées lors de la manipulation des cathéters ou durant toute procédure invasive, afin d’éviter les endocardites nosocomiales
1. simplification
2. réduction
CONCLUSIONS: LES ENJEUX
3. uniformisation
4. évaluation

IE: new guidelines ESC 2009
1. prevention
2. diagnosis
3. treatment

Case report 2

75 year-old woman, 2008: aortic bioprosthesis for aortic stenosis atrial flutter 2010december 2010: unexplained fever
History of the disease
Case report 2
no sign of CHFfever = 38°5aortic systolic murmur 2/6arterial pressure: 140 / 70 mmHgnormal neurological examination
Clinical examination



haemoglobin: 11 g / dlwhite blood cell count: 9,400 / mm3
sedimentation rate: 40 mmCRP = 35 mg/lcreatinin = 69 mg
Laboratory data
Case report
creatinin = 69 mg
Blood cultures / serologies:
negative

TEETEE

TEETEE
new episodes of unexplained fever
April 2011
no sign of CHFfever = 37°aortic systolic murmur 2/6
Clinical examination
4 months later
haemoglobin: 10 g / dlwhite blood cell count: 8,400 / mm3
sedimentation rate: 40 mmCRP = 12 mg/l
Laboratory data
negative
Blood cultures
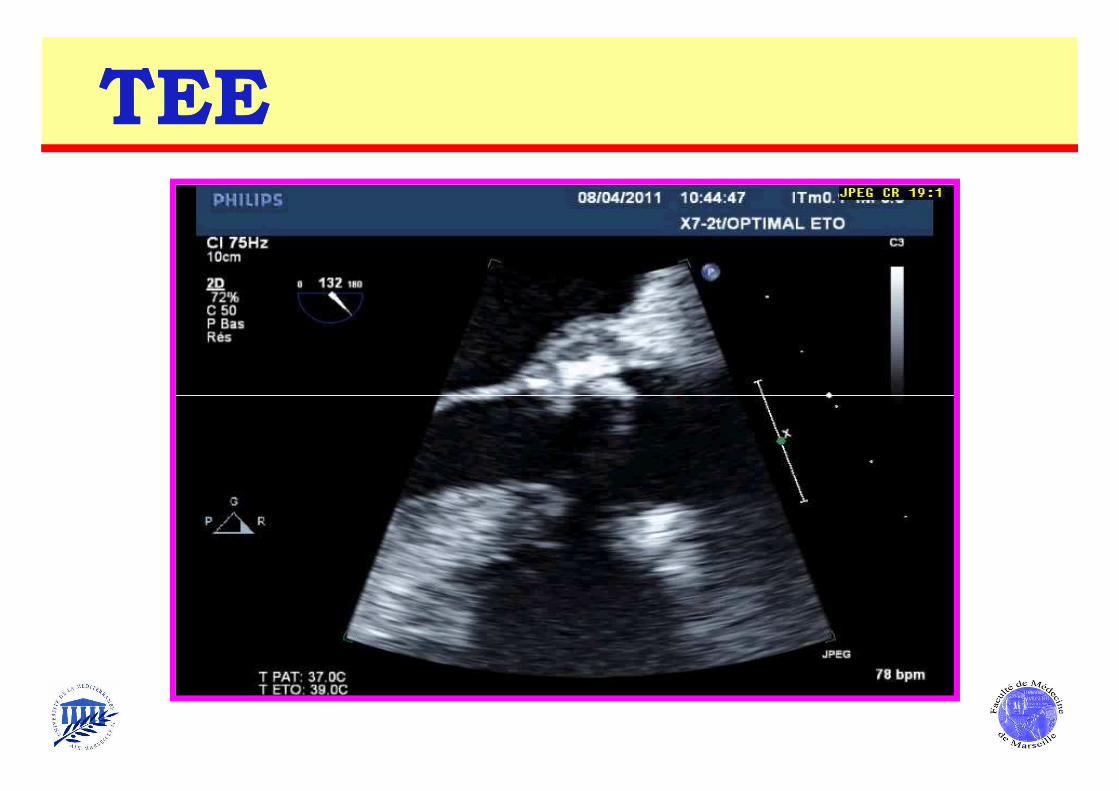
TEETEE

TEETEE

TEETEE
April 8, 2011December 20, 2010

TEETEE
April 8, 2011December 20, 2010
DecisionDecision
1. Consider infective endocarditis (BCNIE)
2. Initiate antibiotic therapy
Vancomycin: 6 weeksVancomycin: 6 weeks
Gentamycin: 2 weeks
3. Close follow-up, perform:
repeat TTE / TEE
TEP scan
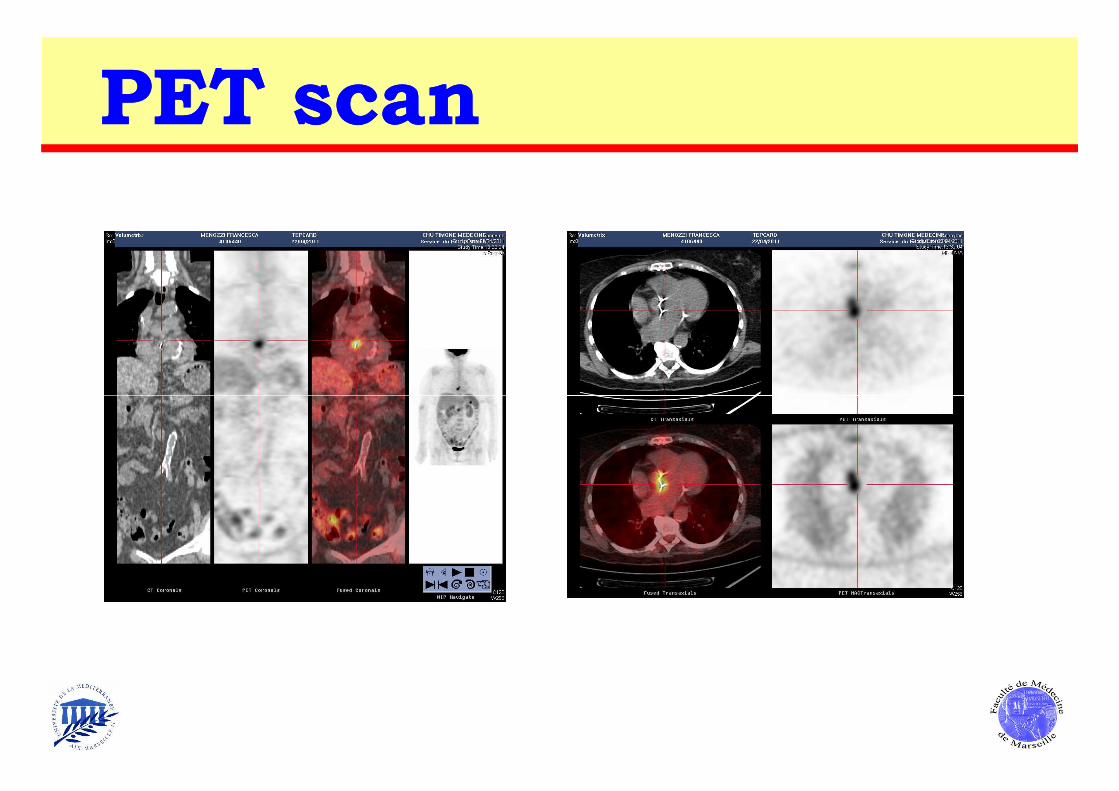
PET scan PET scan

FollowFollow--up up underunder therapytherapy
no fever
normal sedimentation rate, CRP, white blood cells
TTE: normally functioning bioprosthesis
blood cultures: negative
TEETEE

TEETEE

TEETEE

TEETEE
April 8, 2011 April 21, 2011

SurgerySurgery performedperformed on April 29, 2011on April 29, 2011
thickened aortic leaflets
small aortic vegetation
resection of infected tissues
bioprosthetic valve replacement
Surgical findings Surgical approach
posterior aortic root abscess
bioprosthetic valve replacement
Valve cultures
negative

SurgerySurgery performedperformed on April 29, 2011on April 29, 2011
PCR of the valve
identification of Bartonella henselae spp
Doxycycline 200 mg/d

The Duke echographic criteria Durack DT Am J Med 1994 ; 96 : 200-9
vegetation abscess new dehiscence
of prosthetic valve

*TEE is not mandatory in isolated right-sided native valve IE with good quality
TTE examination and unequivocal echocardiographic findings.
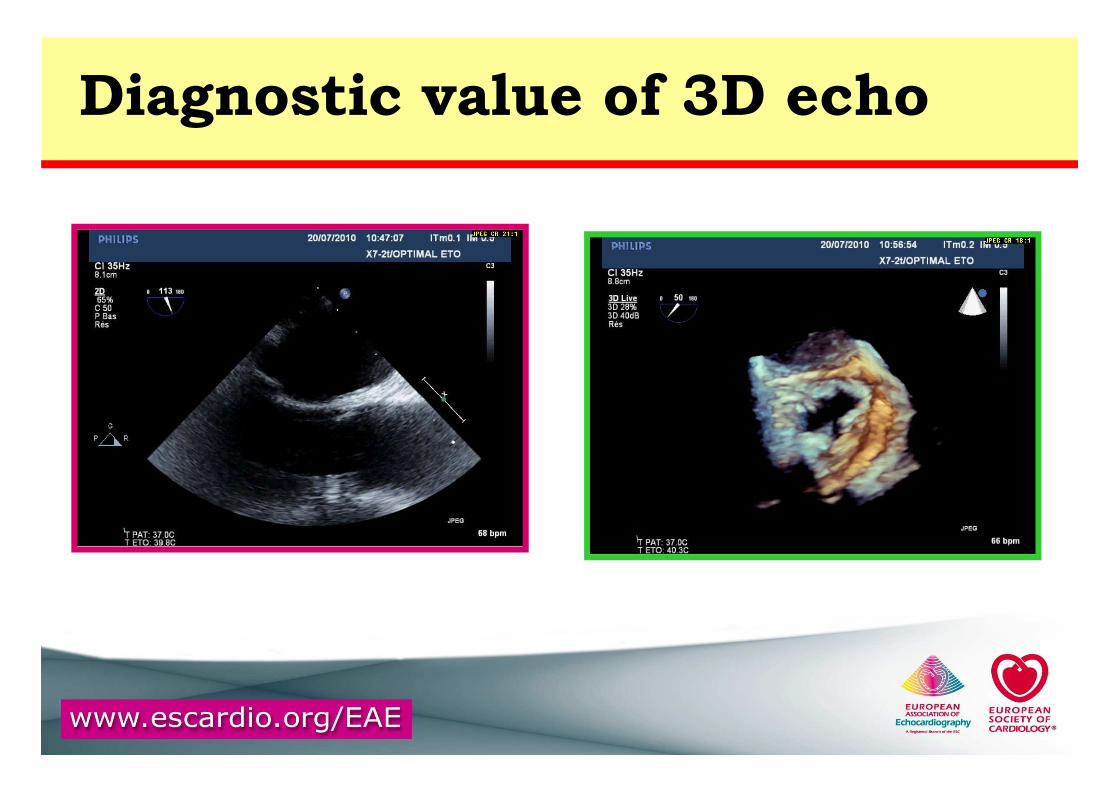
Diagnostic value of 3D echo

Aortic bioprosthetic abscess
October 6, 2009September 23, 2009

Recommendation 1: diagnosis1) TTE is recommended as the first imaging modality in suspected IE
2) TEE is recommended in patients with high clinical suspicion of IE and a
normal TTE
3) TEE should be considered in the majority of patients with suspected IE, even
in case with positive TTE
4) Repeat TTE/TEE within 7-10 days is recommended in case of initially
negative examination when clinical suspicion of IE remains high
5) TEE is not indicated in patients with good-quality negative TTE
and low clinical suspicion of IE

Role of echocardiography in IE

IE: new guidelines ESC 2009
1. prevention
2. diagnosis
3. treatment

Case report 3

52 year-old woman, march 2009 : fever and lombalgiadiagnosis of spondylitisno previous known cardiac diseasehospitalisation in the cardiology Department: June 4th, 2009
History of the disease
Case report
no sign of CHFfever = 38°5mitral systolic murmur 2/6arterial pressure: 120 / 70 mmHgnormal neurological examination
Clinical examination
haemoglobin: 8.5 g / dlwhite blood cell count: 11,000 / mm3
sedimentation rate: 60 mmCRP = 136 mg/lcreatinin = 60 mg
Laboratory data
Case report
creatinin = 60 mg
Blood cultures:
streptococcus bovis (group D)

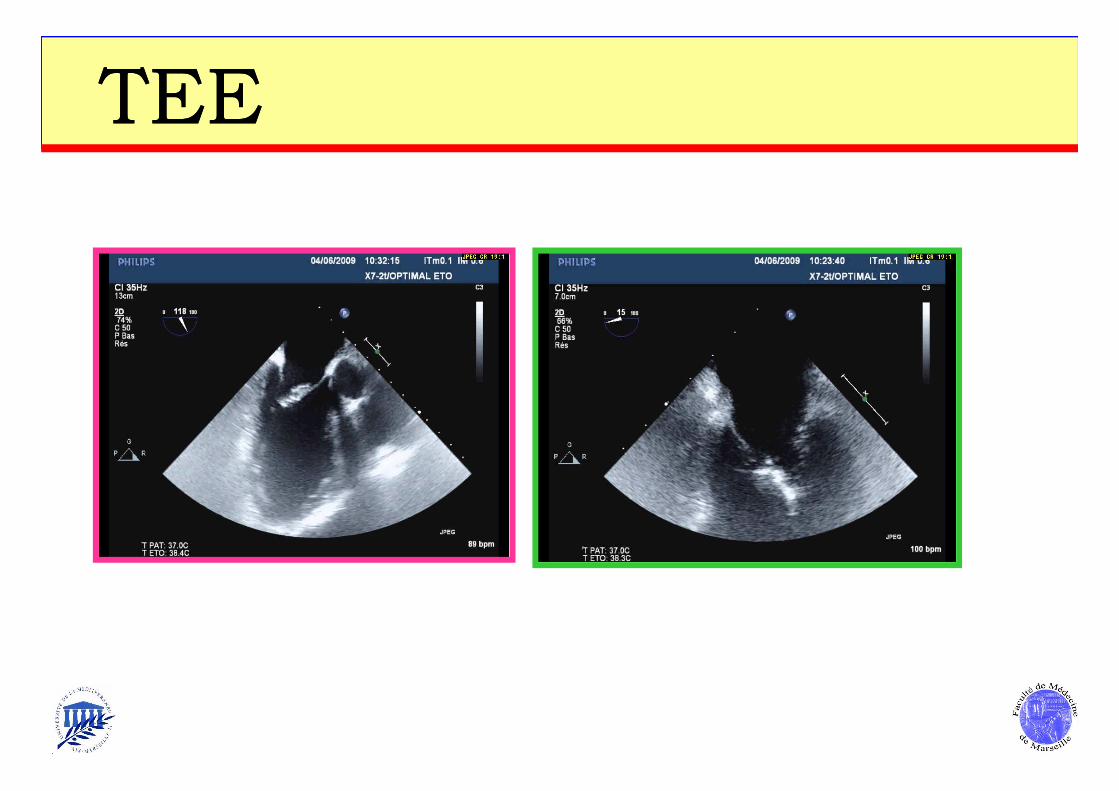
TEETEE

TEETEE
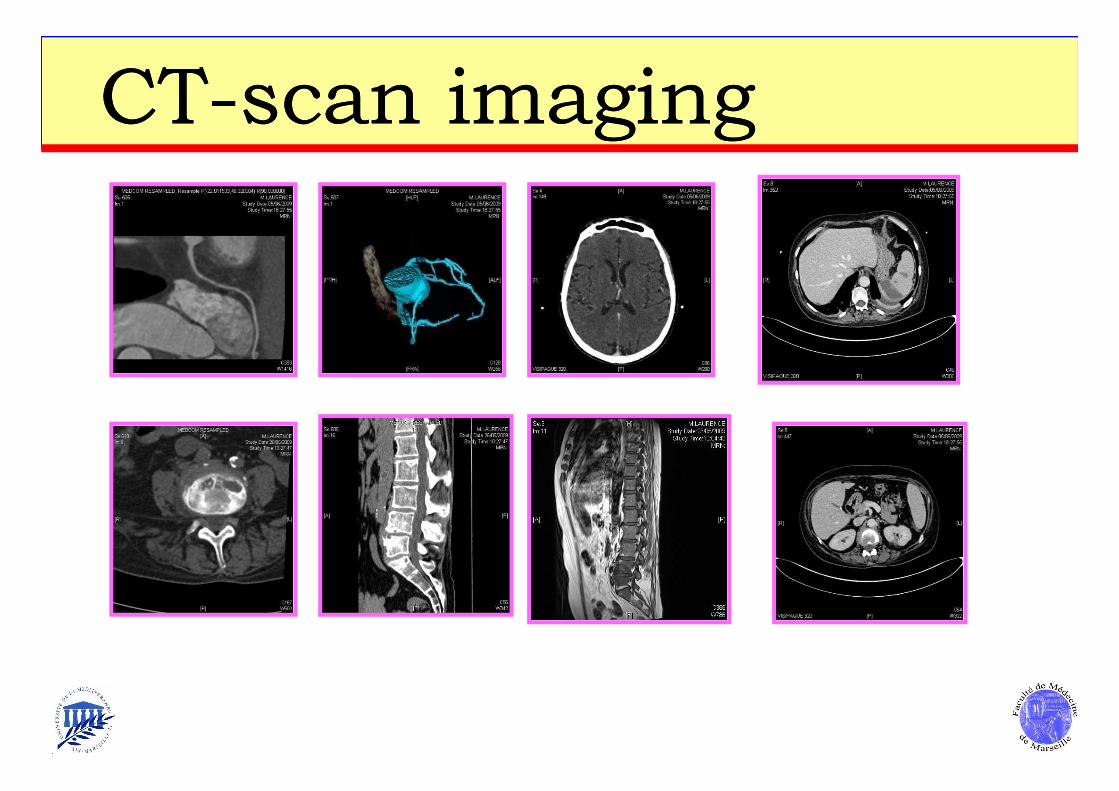
CTCT--scan scan imagingimaging

CTCT--scan scan imagingimaging

normal LV and RV function,
large (26 mm) mitral vegetation (A2)
probable A2 perforation
Patient case: summary
moderate mitral regurgitation: ERO = 28 mm²
no CHF
spondylitis, multiple emboli

1.1. Is early surgery necessary ?Is early surgery necessary ?
2.2. What is the optimal timing for surgery ?What is the optimal timing for surgery ?

1.1. Is early surgery necessary ?Is early surgery necessary ?
2.2. What is the optimal timing for surgery ?What is the optimal timing for surgery ?
60
80
100
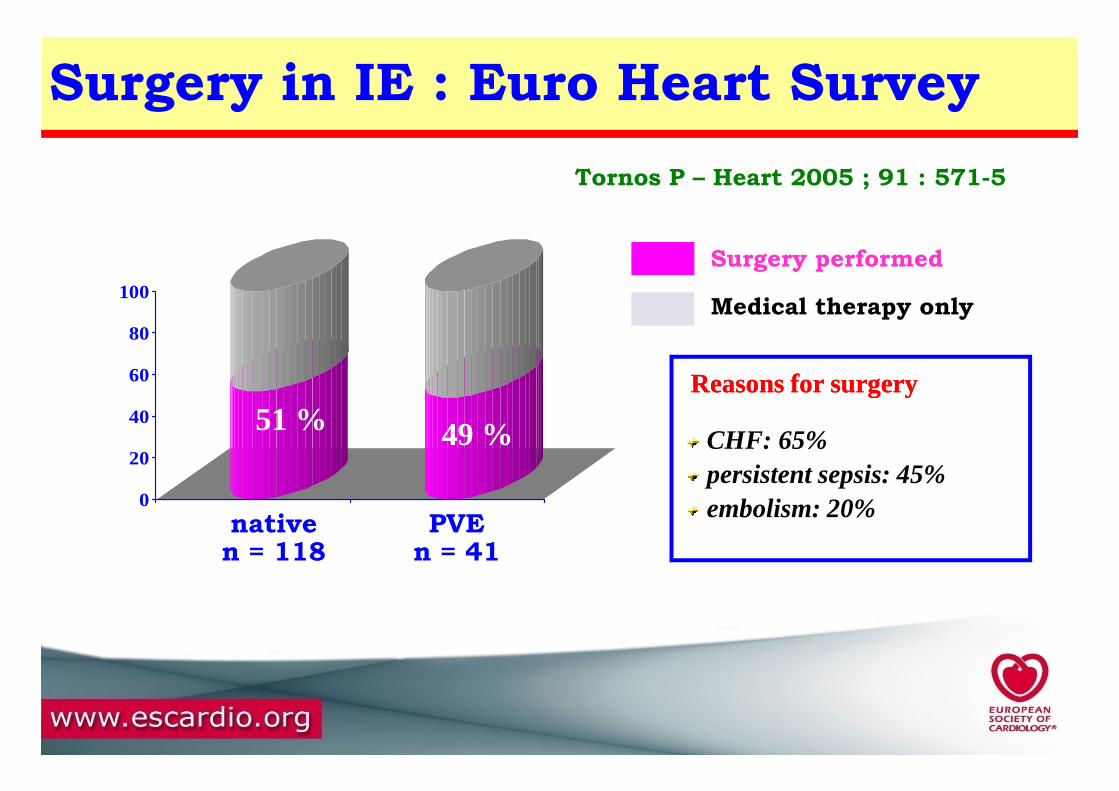
Surgery in IE : Euro Heart Survey
Tornos P – Heart 2005 ; 91 : 571-5
Reasons for surgeryReasons for surgery
Surgery performed
Medical therapy only
0
20
40
nativen = 118
PVEn = 41
51 % 49 % CHF: 65%persistent sepsis: 45%embolism: 20%
Reasons for surgeryReasons for surgery

New guidelines 2009: native IE

ERROR: ioerror
OFFENDING COMMAND: image
STACK: