aortic arch anomalies
TRANSCRIPT

Feb 27 2012 Voxelz©

Embryology
Diagnostic Approach
Aortic Arch
Anomalies
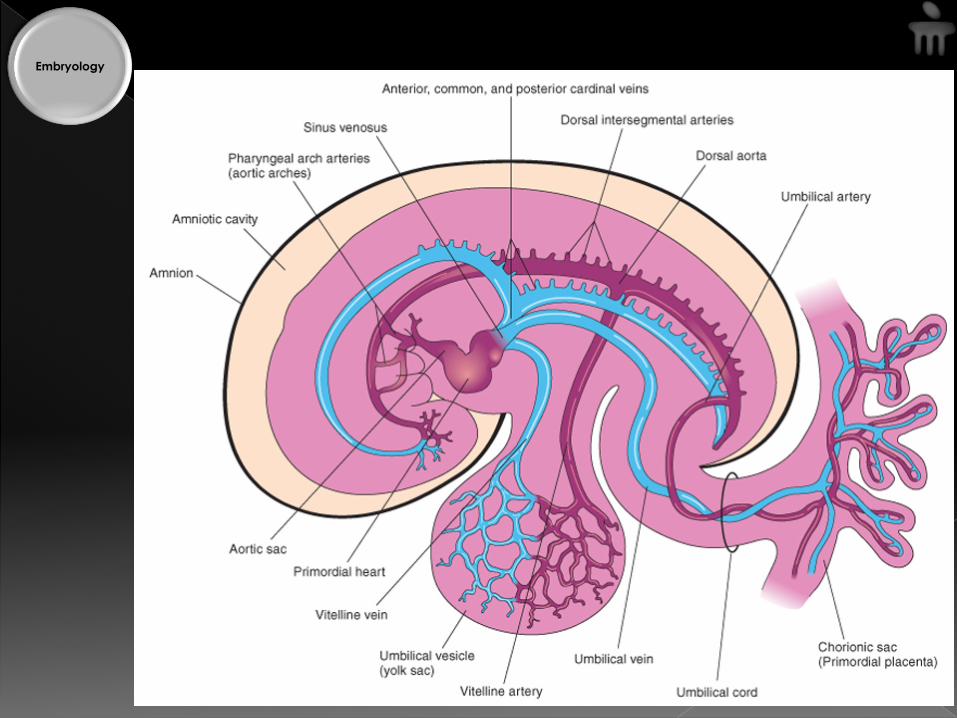
Embryology
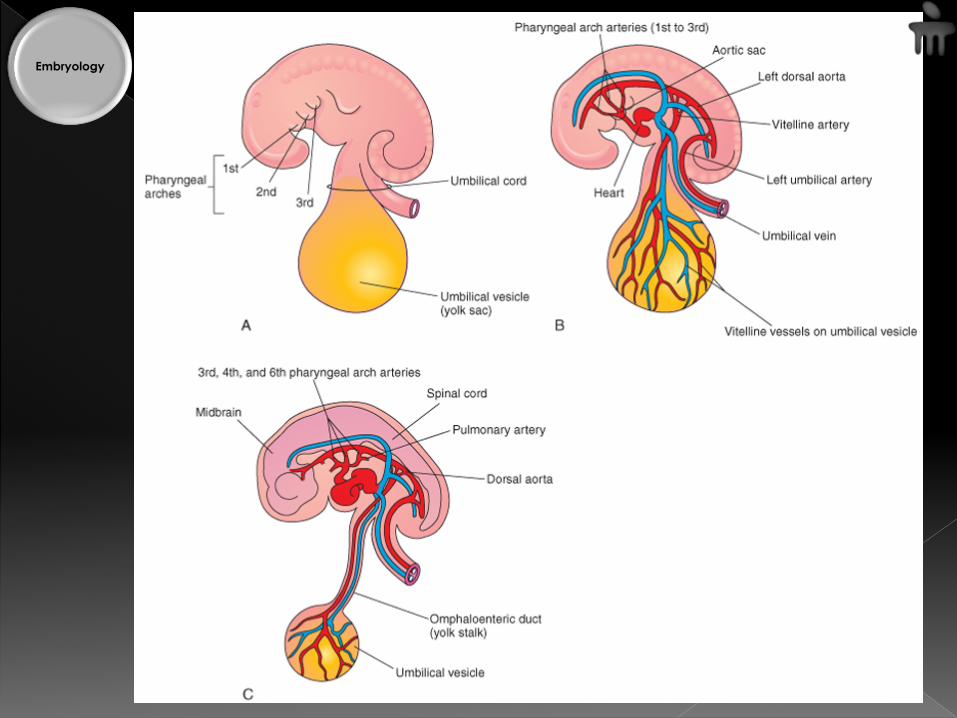
Embryology

Embryology
6 weeks 7 weeks
8 weeks 6 months
Embryology
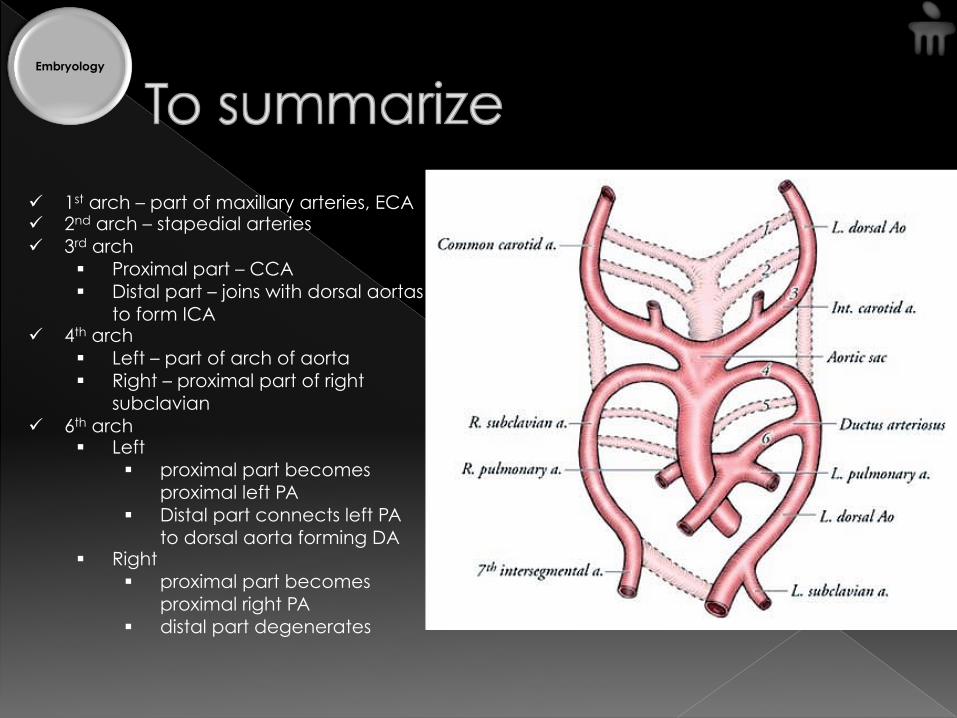
ü 1st arch – part of maxillary arteries, ECA ü 2nd arch – stapedial arteries ü 3rd arch
§ Proximal part – CCA § Distal part – joins with dorsal aortas
to form ICA ü 4th arch
§ Left – part of arch of aorta § Right – proximal part of right
subclavian ü 6th arch
§ Left § proximal part becomes
proximal left PA § Distal part connects left PA
to dorsal aorta forming DA § Right
§ proximal part becomes proximal right PA
§ distal part degenerates
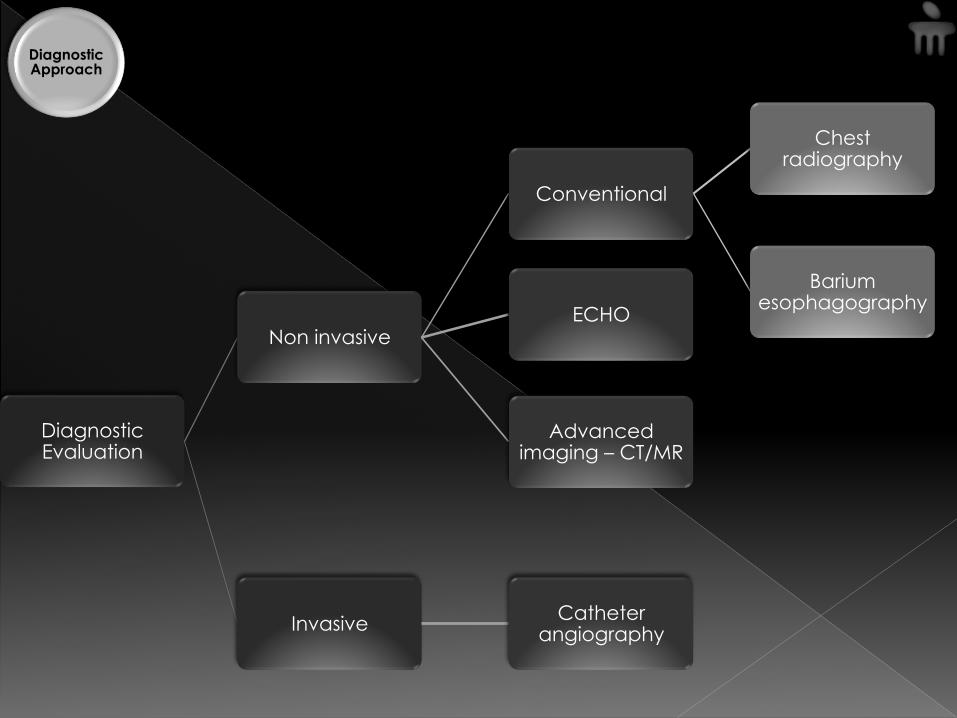
Diagnostic Evaluation
Non invasive
Conventional
Chest radiography
Barium esophagography
ECHO
Advanced imaging – CT/MR
Invasive Catheter angiography
Diagnostic Approach
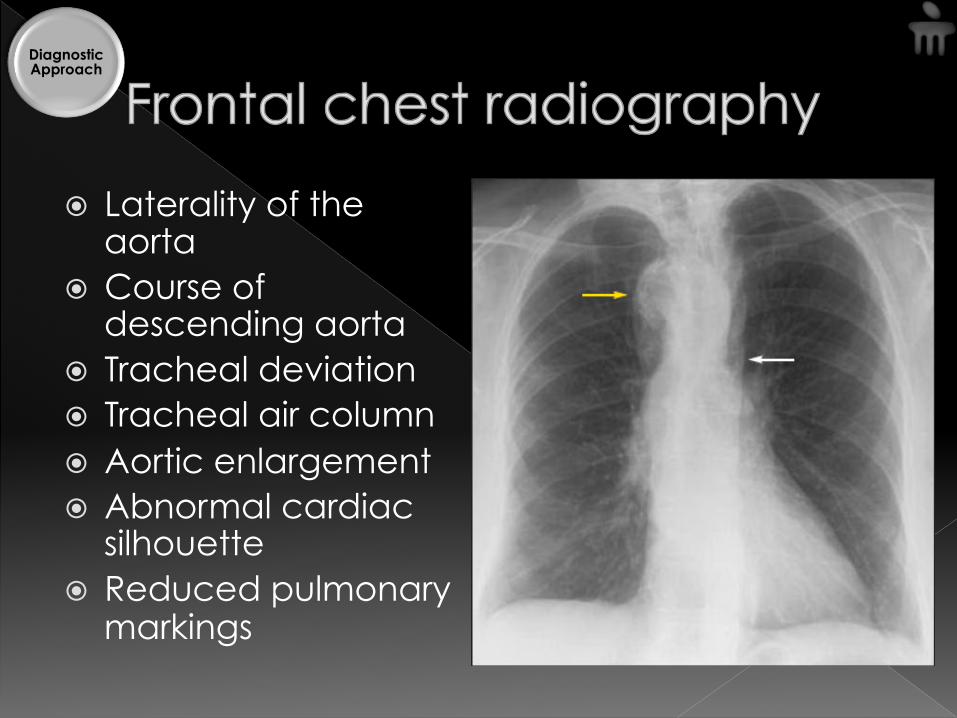
� Laterality of the aorta
� Course of descending aorta
� Tracheal deviation � Tracheal air column � Aortic enlargement � Abnormal cardiac
silhouette � Reduced pulmonary
markings
Diagnostic Approach
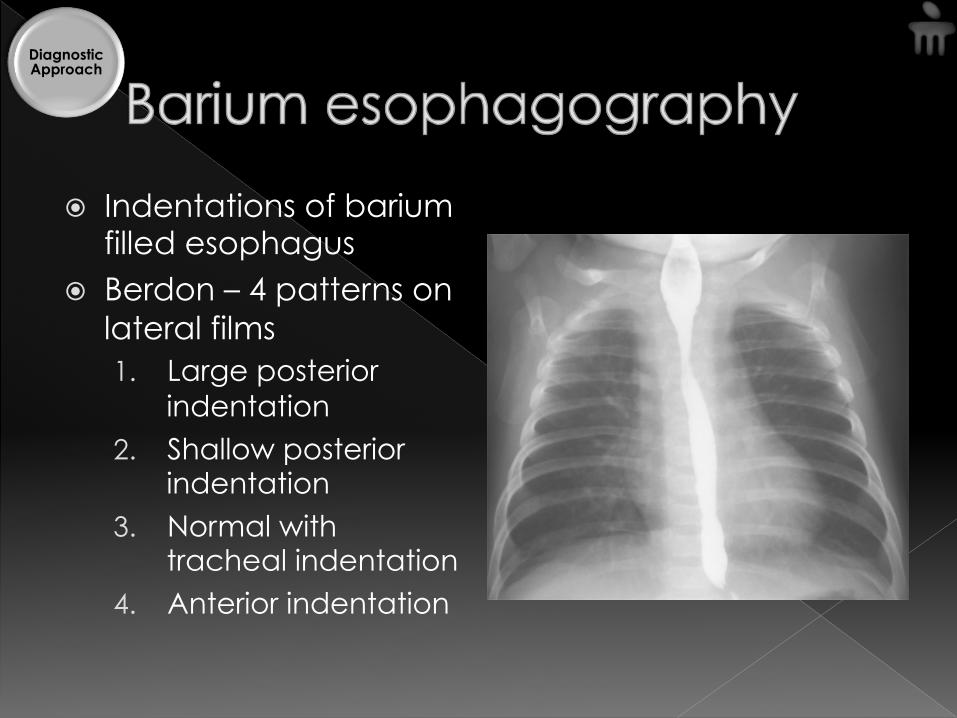
� Indentations of barium filled esophagus
� Berdon – 4 patterns on lateral films 1. Large posterior
indentation 2. Shallow posterior
indentation 3. Normal with
tracheal indentation 4. Anterior indentation
Diagnostic Approach
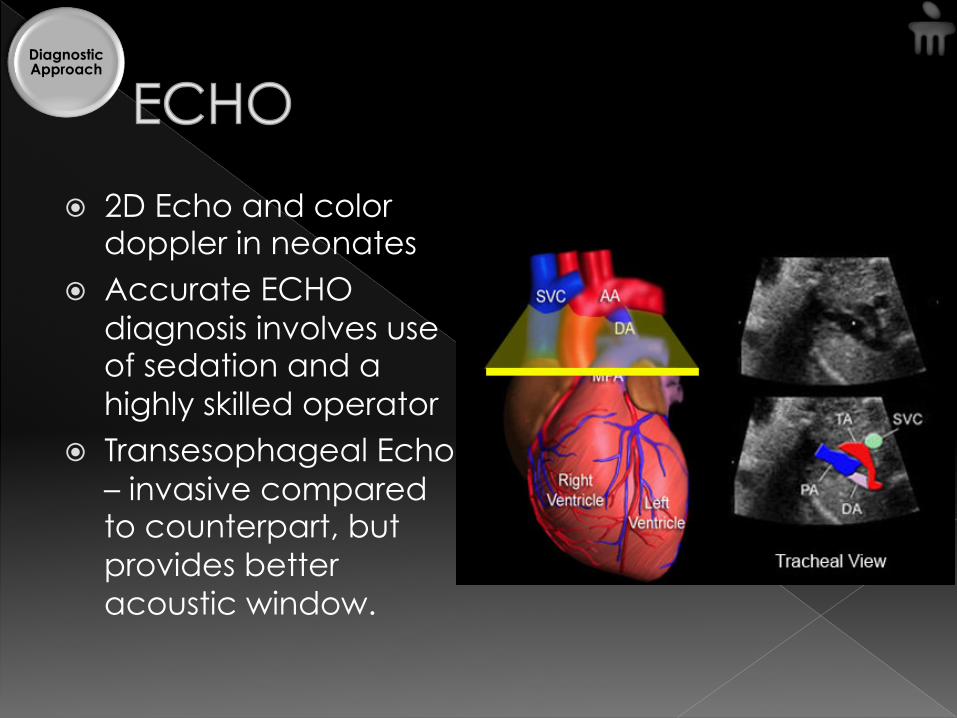
� 2D Echo and color doppler in neonates
� Accurate ECHO diagnosis involves use of sedation and a highly skilled operator
� Transesophageal Echo – invasive compared to counterpart, but provides better acoustic window.
Diagnostic Approach
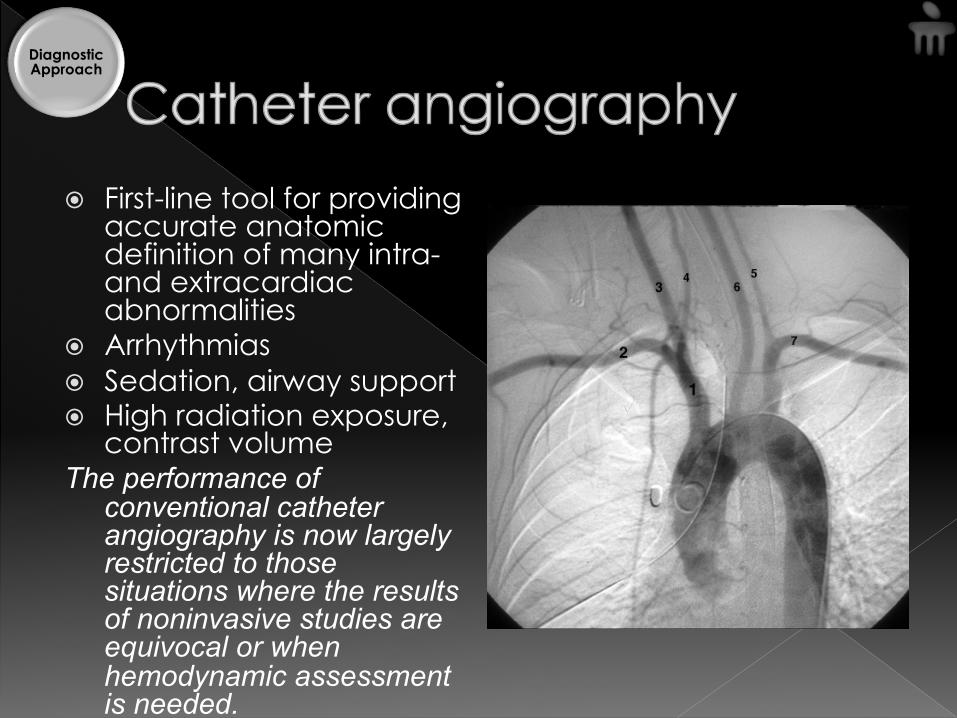
� First-line tool for providing accurate anatomic definition of many intra- and extracardiac abnormalities
� Arrhythmias � Sedation, airway support � High radiation exposure,
contrast volume The performance of
conventional catheter angiography is now largely restricted to those situations where the results of noninvasive studies are equivocal or when hemodynamic assessment is needed.
Diagnostic Approach
� >ECHO: unobscured by overlying air filled lung or bone
� > catheter angiography: separate structures superimposed on angiography › Shorter acquisition times, superior 3D
rendering greater range of coverage › Radiation dose of CTA is 2-3 times less
Diagnostic Approach
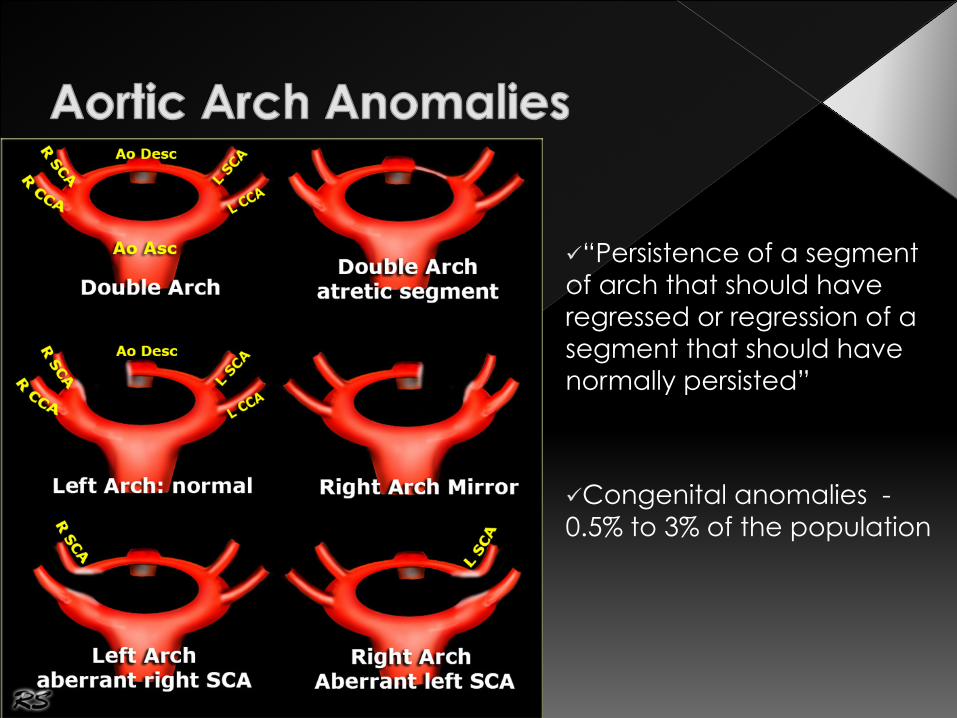
ü “Persistence of a segment of arch that should have regressed or regression of a segment that should have normally persisted”
ü Congenital anomalies - 0.5% to 3% of the population
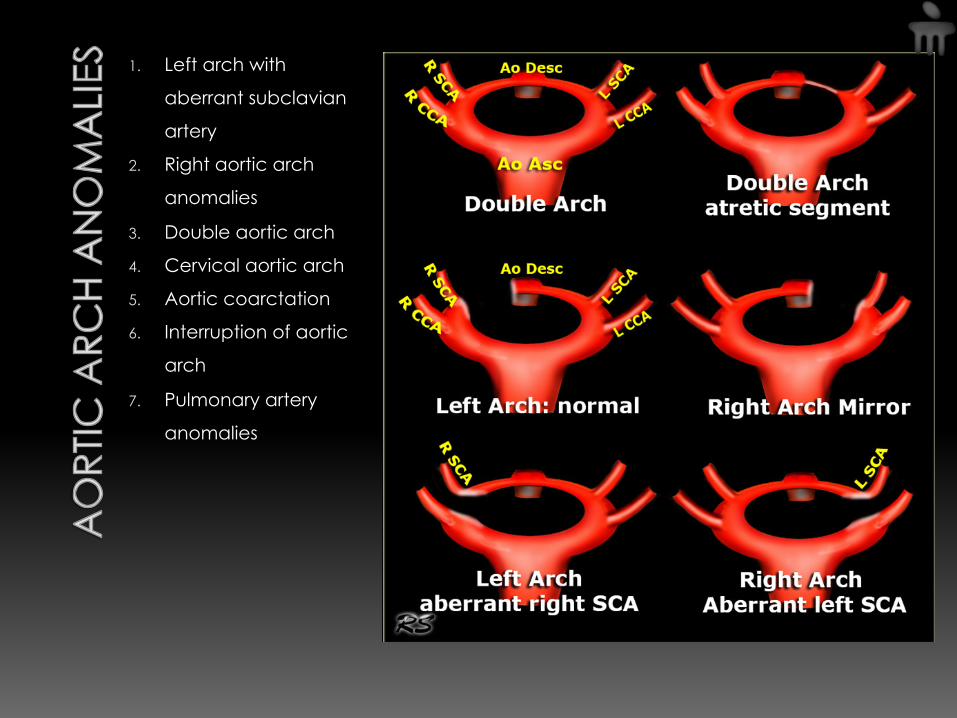
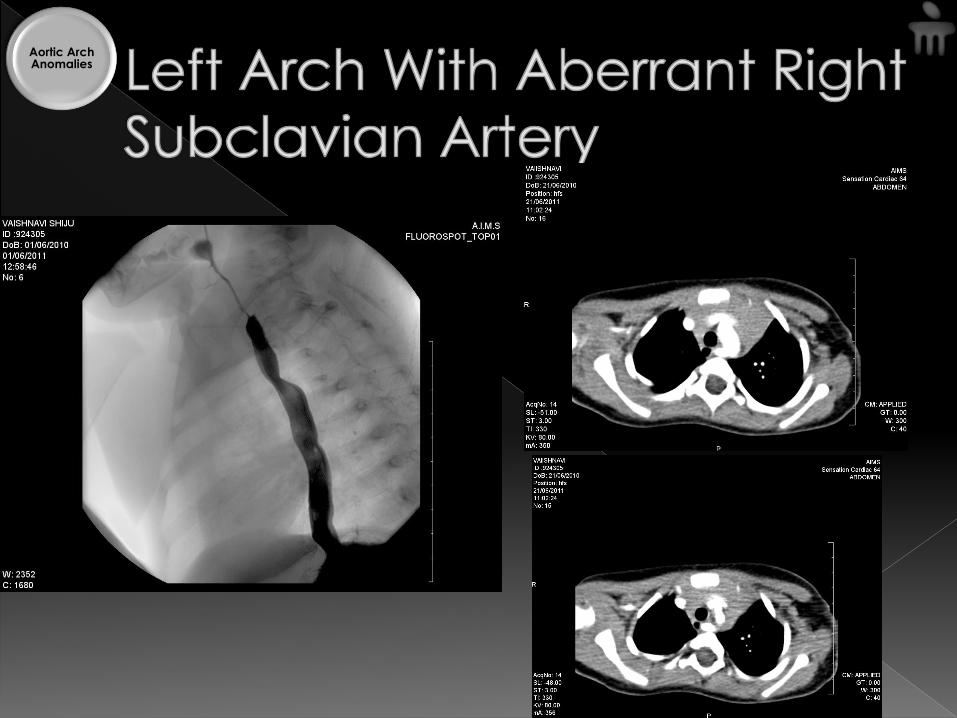
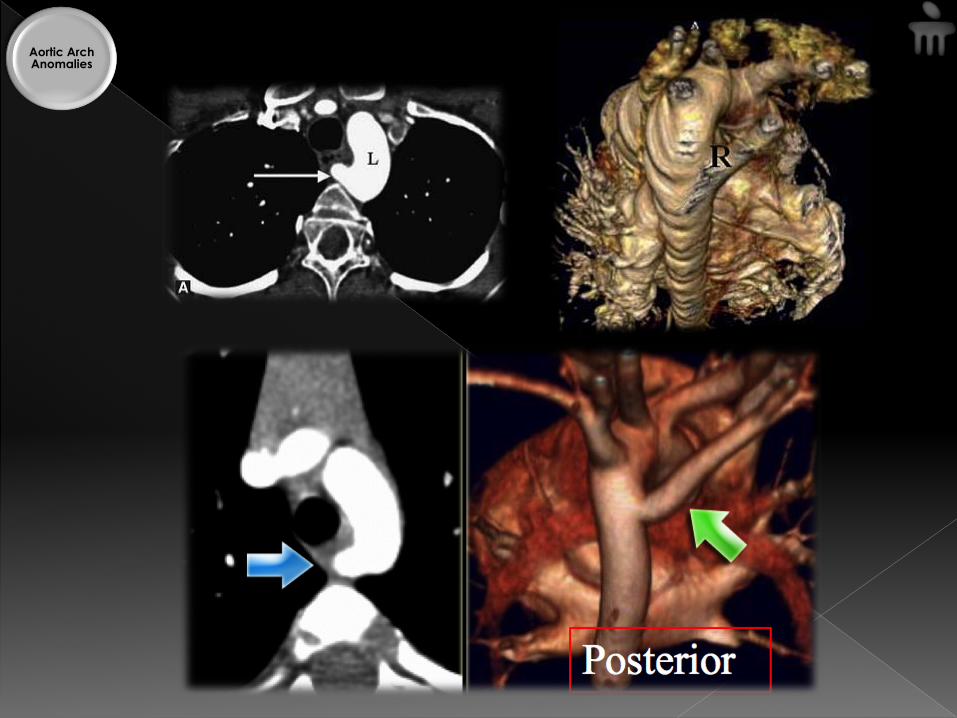
1. Left arch with
aberrant subclavian
artery
2. Right aortic arch
anomalies
3. Double aortic arch
4. Cervical aortic arch
5. Aortic coarctation
6. Interruption of aortic
arch
7. Pulmonary artery
anomalies
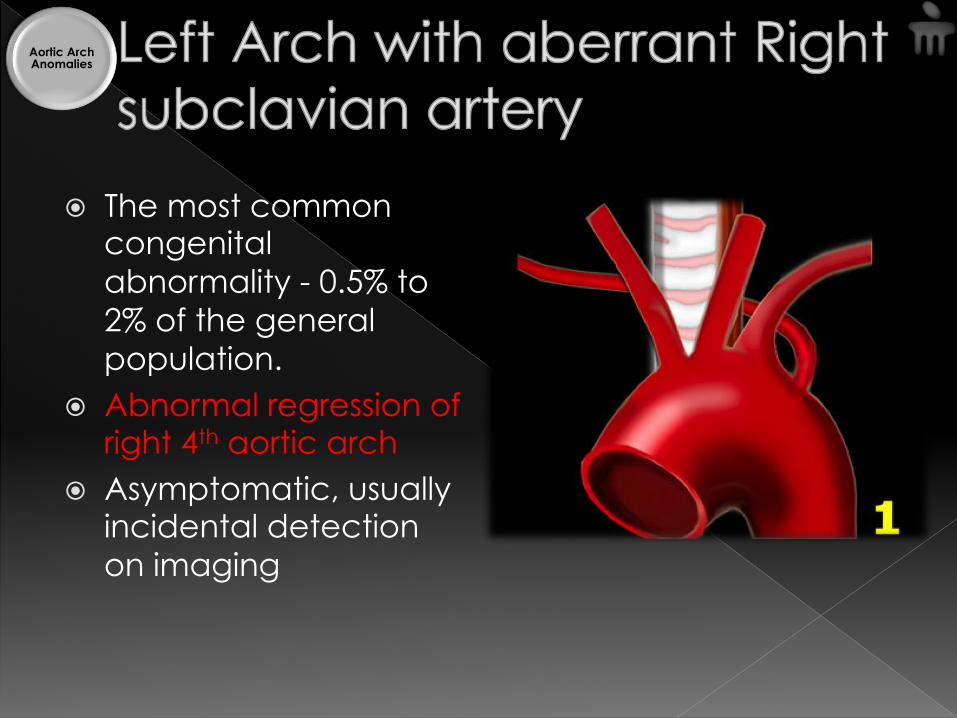
� The most common congenital abnormality - 0.5% to 2% of the general population.
� Abnormal regression of right 4th aortic arch
� Asymptomatic, usually incidental detection on imaging
Aortic Arch Anomalies
Aortic Arch Anomalies
Aortic Arch Anomalies

� 0.05% to 0.2% of the population � Two main types
1. The right arch with mirror image branching 2. The right arch with aberrant left subclavian
artery
Aortic Arch Anomalies
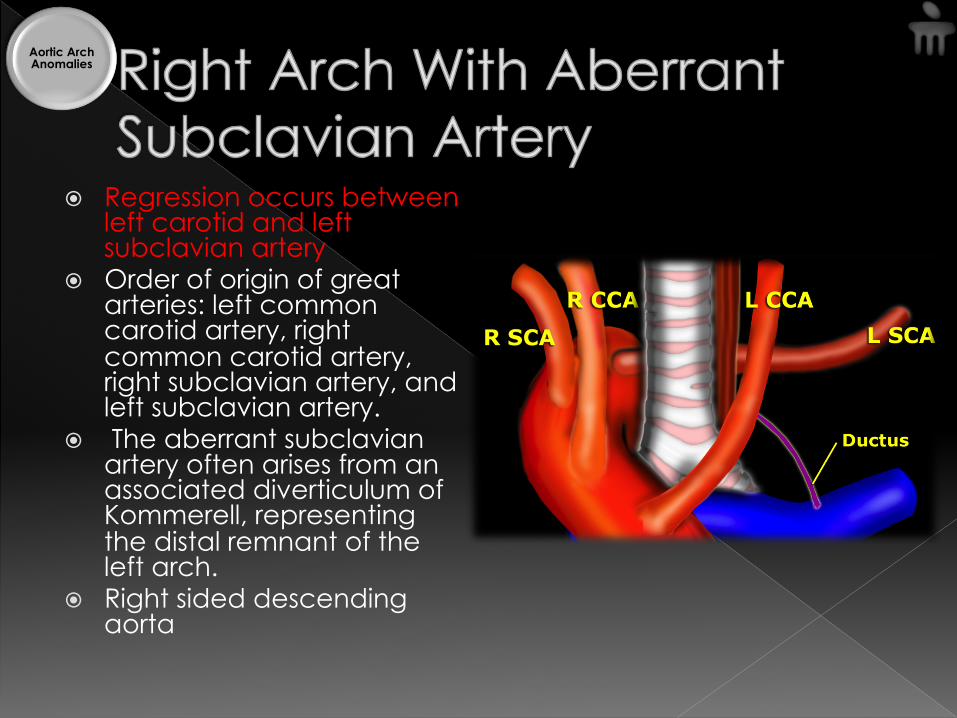
� Regression occurs between left carotid and left subclavian artery
� Order of origin of great arteries: left common carotid artery, right common carotid artery, right subclavian artery, and left subclavian artery.
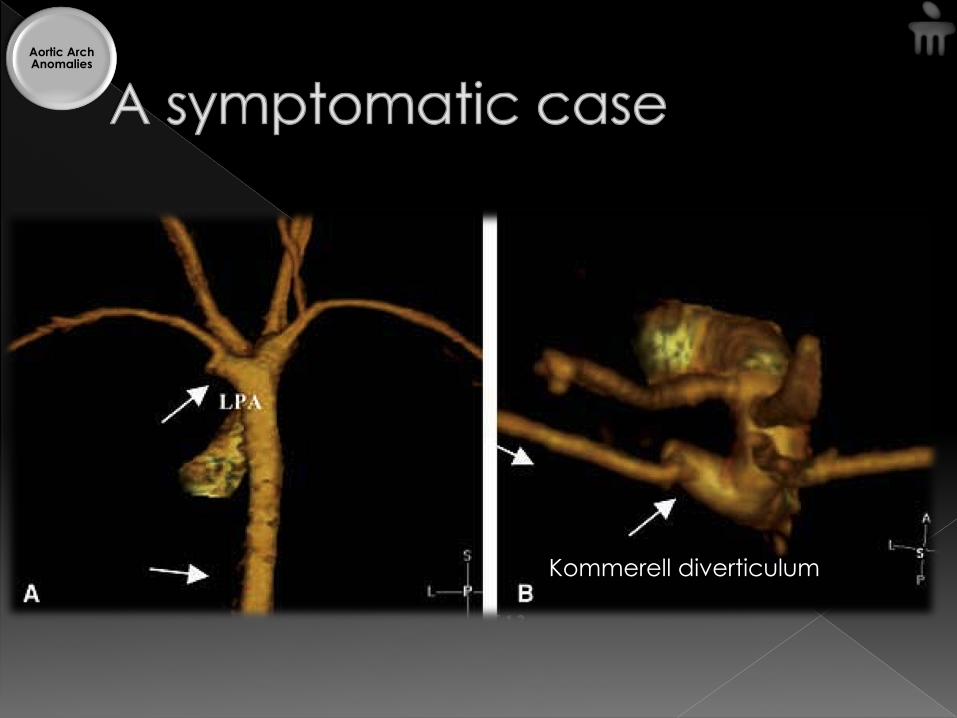
� The aberrant subclavian artery often arises from an associated diverticulum of Kommerell, representing the distal remnant of the left arch.
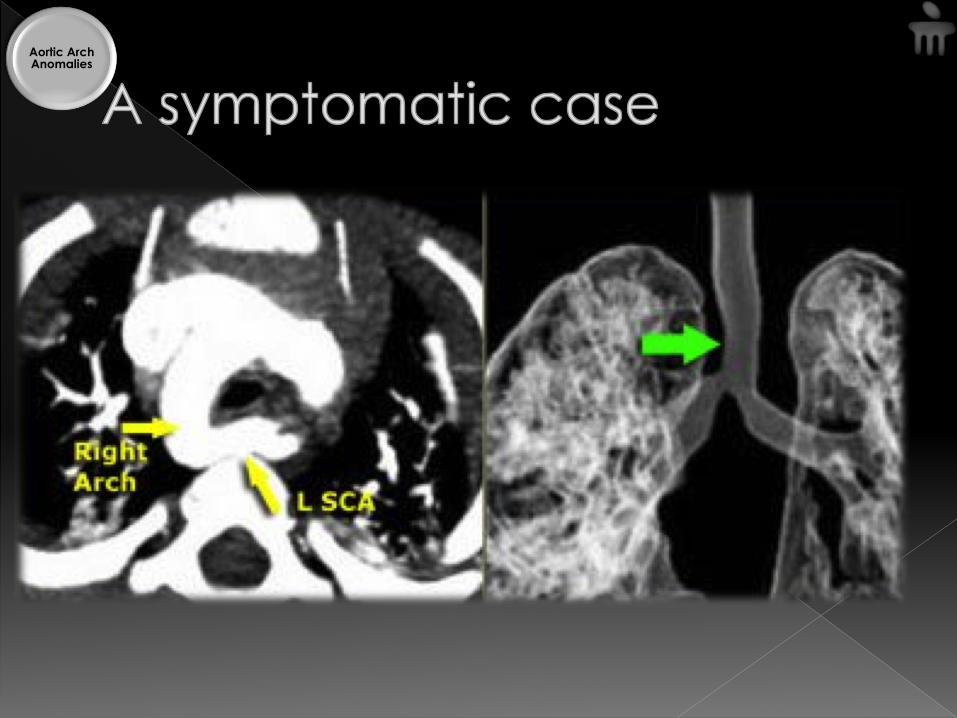
� Right sided descending aorta
Aortic Arch Anomalies
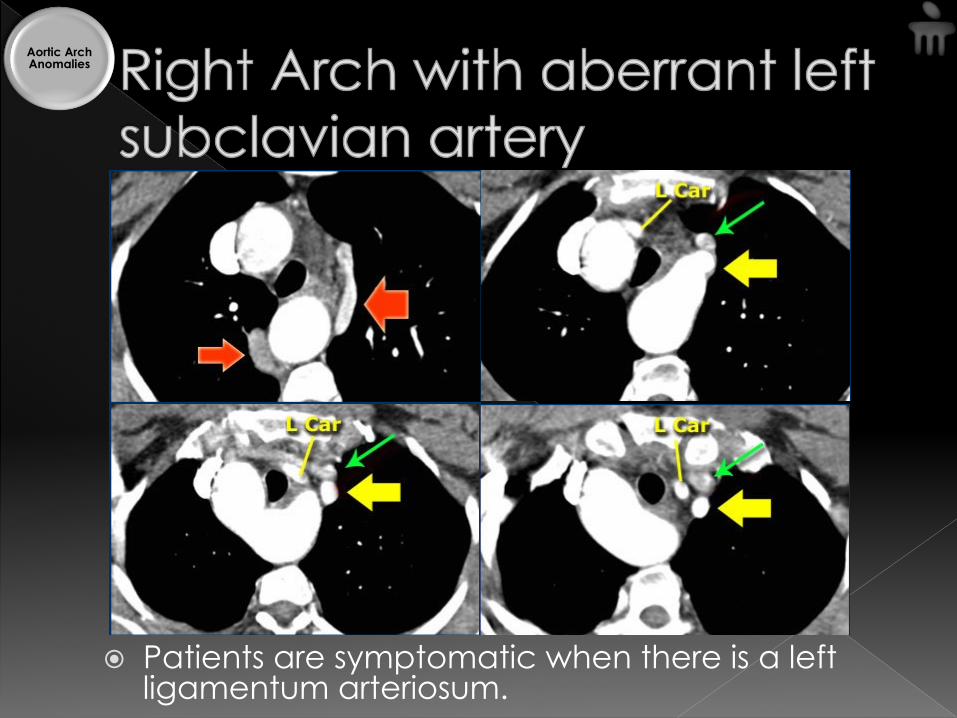
� Patients are symptomatic when there is a left ligamentum arteriosum.
Aortic Arch Anomalies

Vascular ring � Ascending aorta
anterior to trachea � Right arch to right
of trachea and esophagus
� Left subclavian artery or retroesophageal diverticulum posterior to esophagus
� DA or ligamentum arteriosum on the left
Aortic Arch Anomalies
Aortic Arch Anomalies
Aortic Arch Anomalies
Kommerell diverticulum
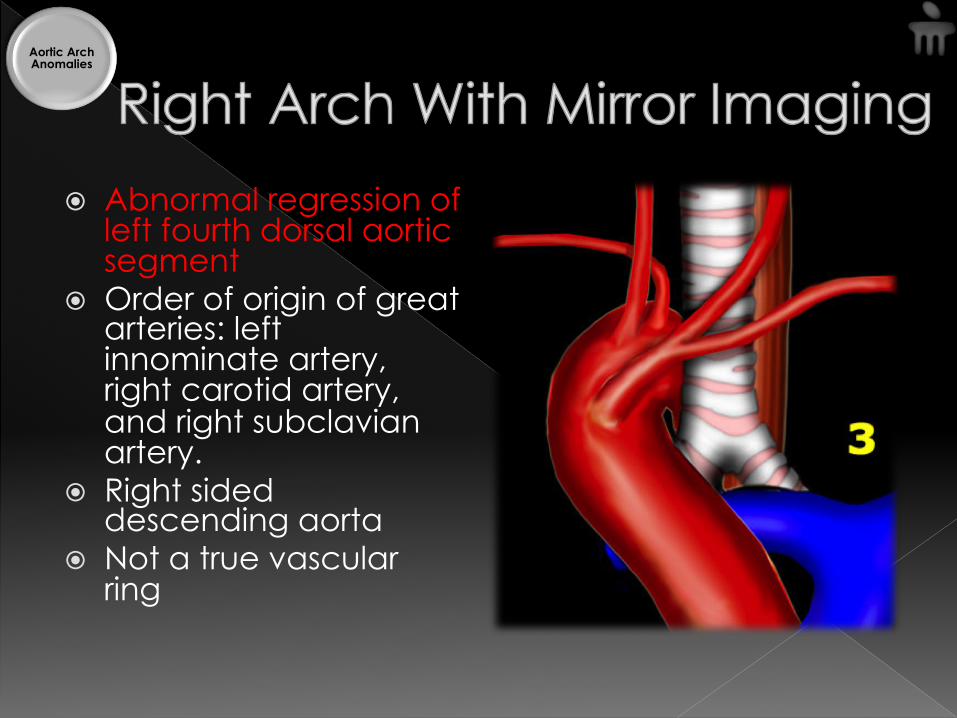
� Abnormal regression of left fourth dorsal aortic segment
� Order of origin of great arteries: left innominate artery, right carotid artery, and right subclavian artery.
� Right sided descending aorta
� Not a true vascular ring
Aortic Arch Anomalies

� Clinical attention because of associated cyanotic heart disease › Tetralogy of Fallot, truncus arteriosus, pulmonary artery atresia
with ventricular septal defect, tricuspid atresia, double outlet right ventricle, and transposition of the great arteries.
Aortic Arch Anomalies

� 0.05% to 3% of the population
� Failure of regression of right fourth dorsal arch
� Two aortic arches arising from a single ascending aorta.
� Each arch gives rise to its own subclavian and carotid arteries before uniting to form a single descending aorta, which is usually left-sided.
� Both limbs of the double arch are usually patent and functioning. The right limb is typically larger and more cephalad than the left arch
Aortic Arch Anomalies

� Patients with double arch are often symptomatic - symptoms of esophageal or tracheal compression.
� Double arch is usually diagnosed in childhood, although it can be discovered incidentally if the ring formed by the double arch is loose.
� Associated heart disease is rare.
Aortic Arch Anomalies
Aortic Arch Anomalies

� Four vessel sign � Right > Left � Vascular ring
Aortic Arch Anomalies

Aortic Arch Anomalies
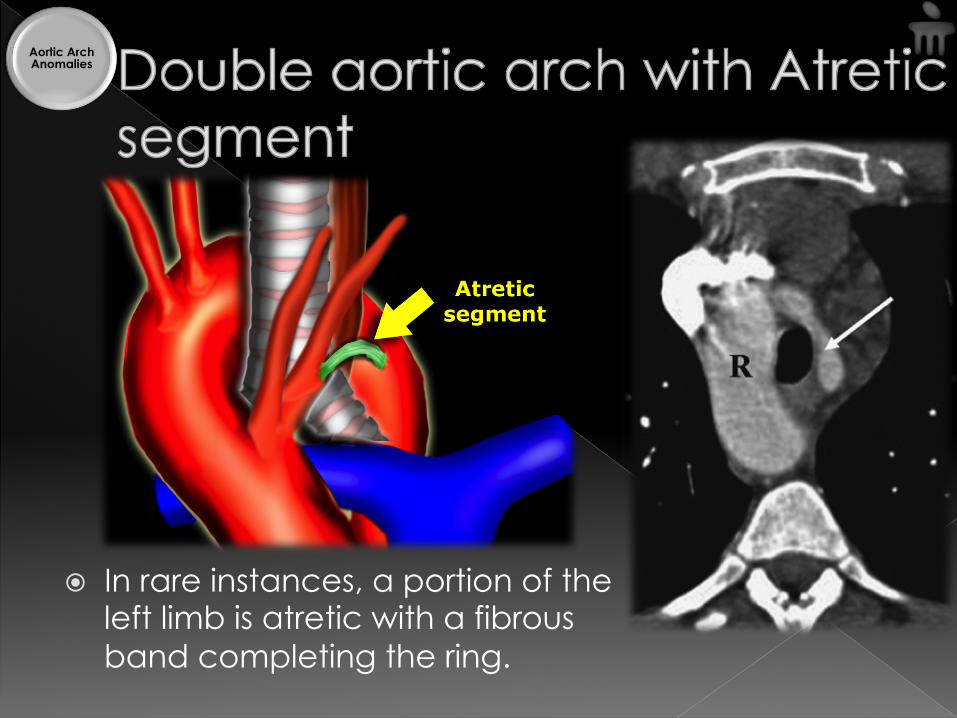
� In rare instances, a portion of the left limb is atretic with a fibrous band completing the ring.
Aortic Arch Anomalies

� A cervical aortic arch is a rare anomaly characterized by a high-riding elongated aortic arch
� Abnormal persistence of 2nd or 3rd primitive aortic arch
� Ascends into the neck, usually on the right.
Aortic Arch Anomalies
� Pulsatile mass in the neck � Compression of the mass produces
significant reduction in the pulse of the contralateral arm and leg
� Most patients are asymptomatic � Associated anomalies › absence of the innominate artery, origin of
the contralateral subclavian artery from the descending proximal aorta
Aortic Arch Anomalies
� 3.2 of 10,000 births, approx. 5% to 8% of all congenital cardiac disease.
� may present in the neonate or remain undetected well into adult life
� 80% - males, common in Turner’s syndrome
� 2 main types › Preductal (infantile) › Postductal (adult)
Aortic Arch Anomalies
� Degree of stenosis – variable › Asymmetric with a posterior shelf which is
preceded by some tapering of the aortic lumen
� Tubular hypoplasia in the arch – proximal/distal to origin of left subclavian
� Bicuspid aortic valve & cystic medial degeneration – dilated ascending aorta
� Post stenotic dilatation – abnormal elastic tissue in the media
Aortic Arch Anomalies
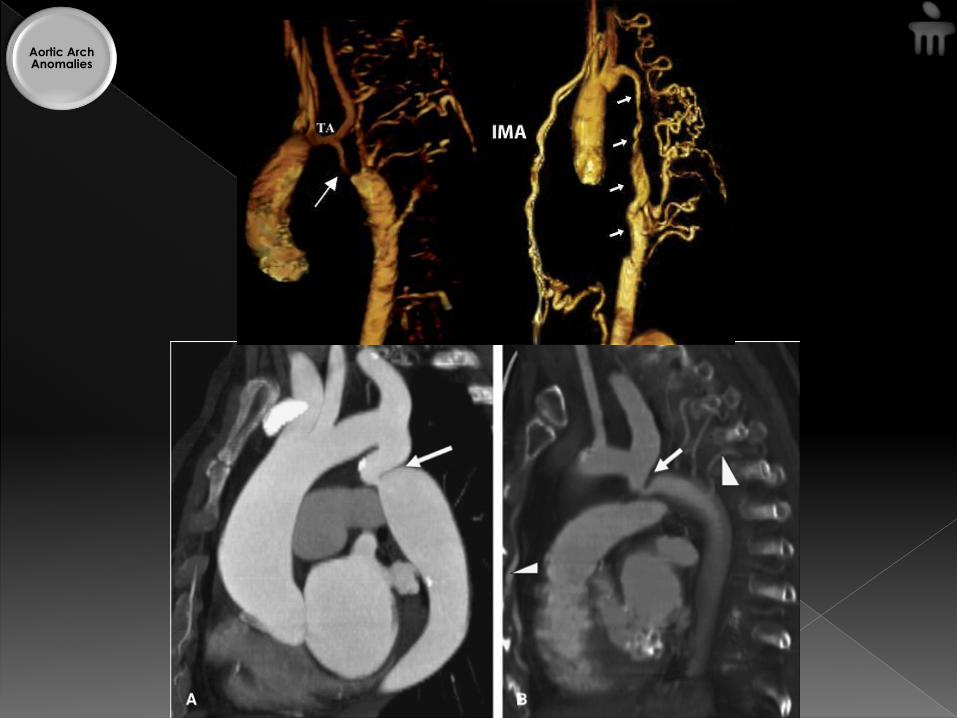
� Collateral circulation – in proportion to degree of stenosis. › Internal mammary arteries (via intercostal
arteries 3-9), inferior epigastric arteries, scapular & mediastinal arteries › Enlarged bilateral subclavian arteries › Rib notching
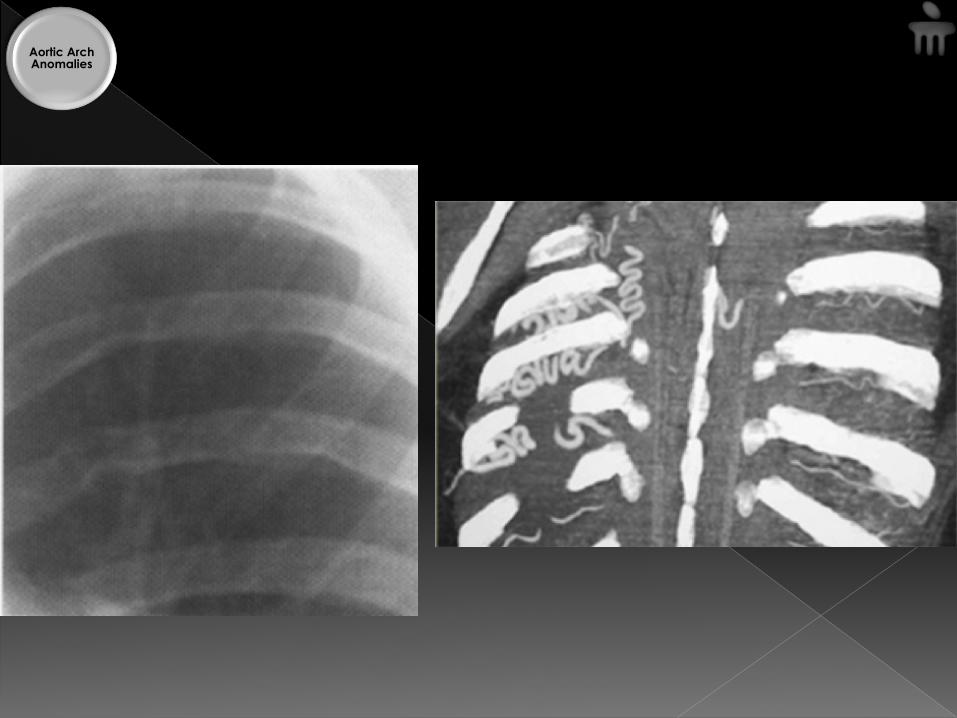
� Bilateral, asymmetric, inferior aspect of posterior third of the upper ribs
� Shallow or deep with a corticated margin
Aortic Arch Anomalies
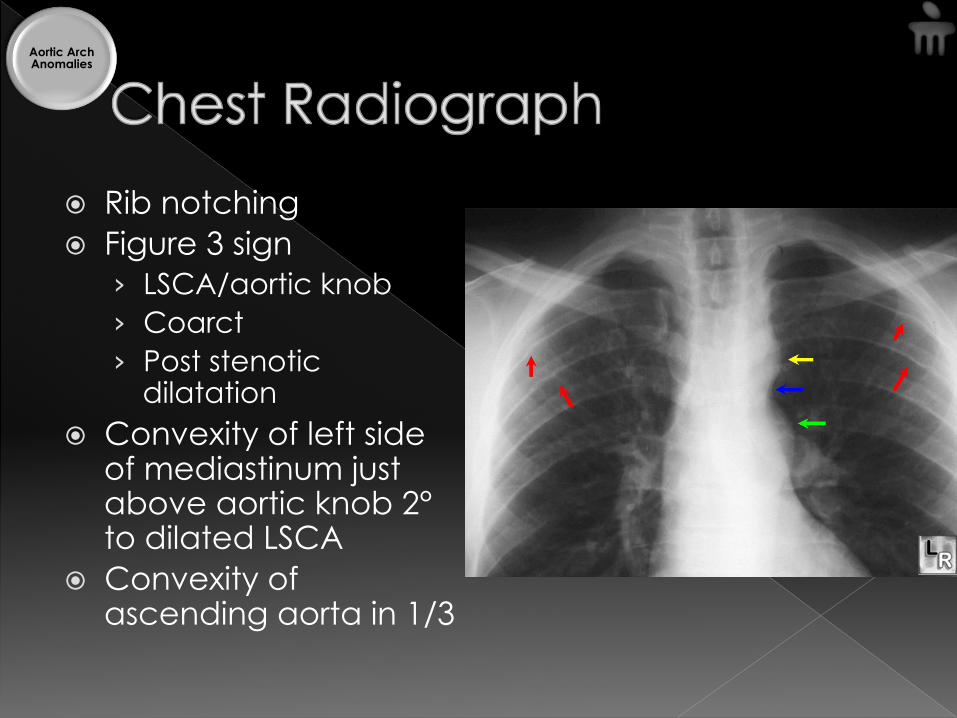
� Rib notching � Figure 3 sign › LSCA/aortic knob › Coarct › Post stenotic
dilatation � Convexity of left side
of mediastinum just above aortic knob 2° to dilated LSCA
� Convexity of ascending aorta in 1/3
Aortic Arch Anomalies
Aortic Arch Anomalies
Aortic Arch Anomalies
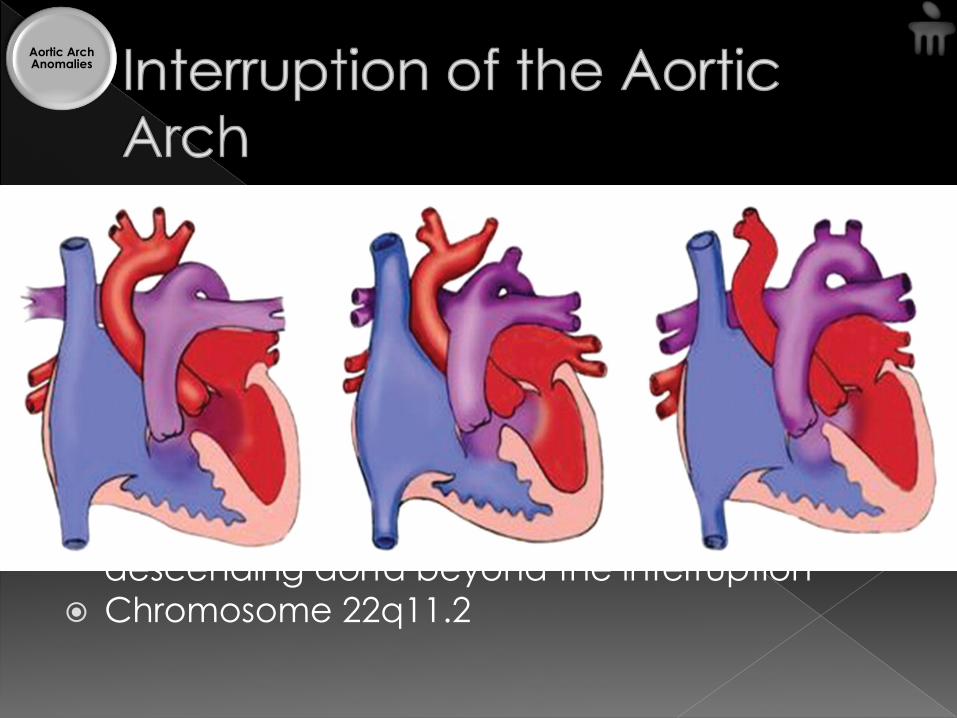
� 1.5% of cases of congenital heart disease (82). � Embryologically, this is related to regression of
portions of the arch on two sides. � Three basic types › Type A, interruption distal to the left subclavian artery › Type B (84%), interruption between the left common
carotid artery and the left subclavian artery › Type C, interruption between the brachiocephalic
trunk and the left carotid artery � A dilated patent ductus arteriosus supplies the
descending aorta beyond the interruption � Chromosome 22q11.2
Aortic Arch Anomalies

� Present early neonatal period with respiratory distress, cyanosis, and congestive heart failure.
� Congenital heart disease is usually present › ventricular septal defect, bicuspid aortic valve,
aortopulmonary window, truncus arteriosus, transposition of the great arteries, double-outlet right ventricle, and single ventricle › Type B interruption - associated with the
DiGeorge syndrome � Surgical repair - an end-to-end anastomosis
or by interposition of a conduit.
Aortic Arch Anomalies
� Common arterial trunk, also known as truncus arteriosus, persistent truncus arteriosus, and truncus arteriosus communis,
� Uncommon vascular lesion, 1-4% of all congenital heart disease.
� Failure of proximal division into the aorta and the pulmonary artery.
� Early presentation - neonatal period or infancy with cyanosis and congestive heart failure.
Aortic Arch Anomalies
� Classification › Type I - a common arterial trunk with confluent pulmonary arteries › Type II - a common arterial trunk with absence of one pulmonary artery › Type III - a common arterial trunk with interrupted aortic arch or severe coarctation.
Aortic Arch Anomalies
� One of the pulmonary arteries originates from the ascending aorta, while the other arises from the right ventricle.
� Affected patients usually present in the neonatal period or infancy with congestive heart failure secondary to a large left-to-right shunt
� The anomalous pulmonary artery, most commonly the right, usually arises from the posterior wall of the ascending aorta and enters the pulmonary hilus to supply the ipsilateral lung
� The left pulmonary artery arises from the right ventricle to supply its ipsilateral lung. Associated anomalies include patent ductus arterious and ventricular septal defect.
Aortic Arch Anomalies
� Persistence of the distal part of the sixth aortic arch
� Common lesion in pediatric patients, especially in those with hyaline membrane disease and severe congenital heart disease, particularly pulmonary atresia and hypoplastic left heart syndrome.
� Except for neonates, most patients with patent ductus arteriosus are asymptomatic, and the lesion is usually diagnosed by the discovery of a murmur
Aortic Arch Anomalies
� The diagnostic CT and MR finding is that of a small tubular structure connecting the descending proximal aorta with the distal main or proximal left pulmonary artery (105)
� The ductus may massively dilate in severe congenital heart disease, particularly when there are defects that cause large differences between aortic and pulmonary pressure, thus substantially increasing blood flow through the ductus. Treatment is either device closure or operative repair.
Aortic Arch Anomalies
1. Absence or proximal interruption
2. Pulmonary sling
Aortic Arch Anomalies
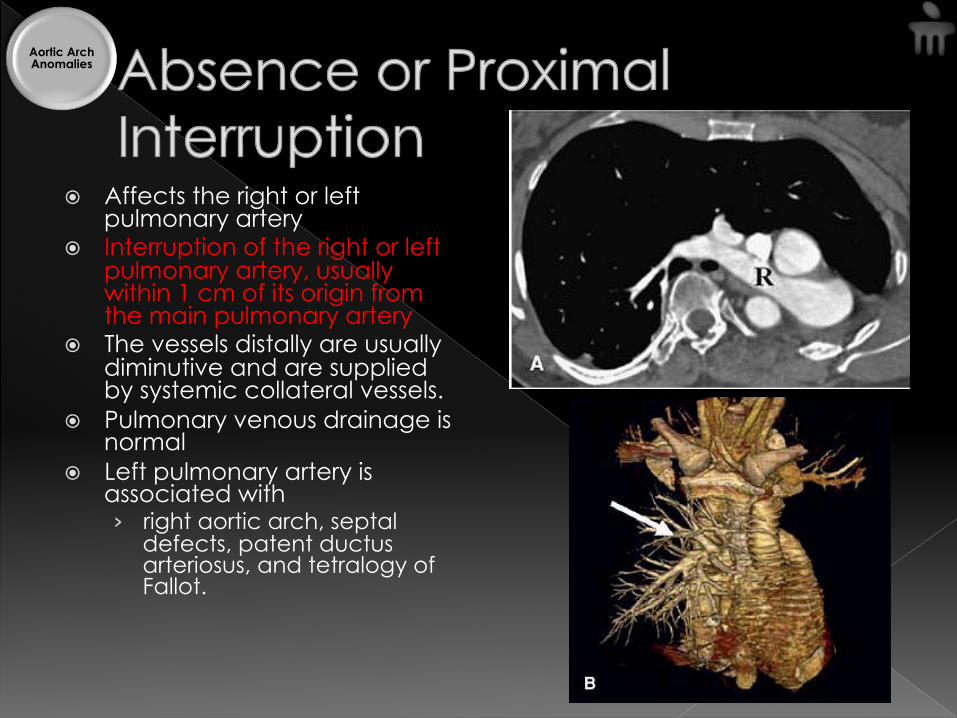
� Affects the right or left pulmonary artery
� Interruption of the right or left pulmonary artery, usually within 1 cm of its origin from the main pulmonary artery
� The vessels distally are usually diminutive and are supplied by systemic collateral vessels.
� Pulmonary venous drainage is normal
� Left pulmonary artery is associated with › right aortic arch, septal
defects, patent ductus arteriosus, and tetralogy of Fallot.
Aortic Arch Anomalies
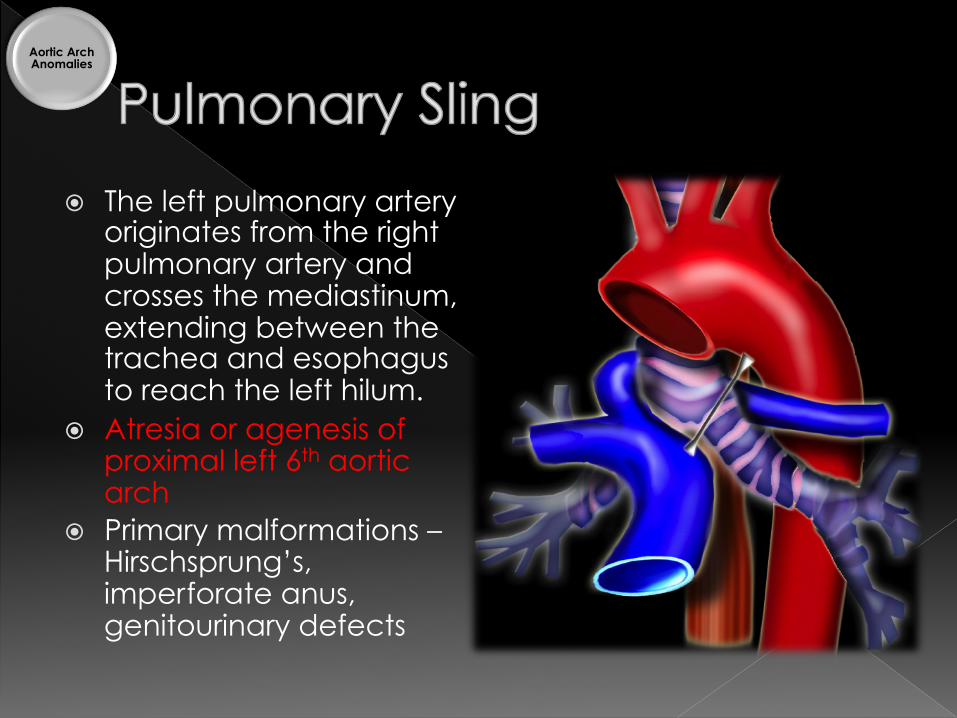
� The left pulmonary artery originates from the right pulmonary artery and crosses the mediastinum, extending between the trachea and esophagus to reach the left hilum.
� Atresia or agenesis of proximal left 6th aortic arch
� Primary malformations – Hirschsprung’s, imperforate anus, genitourinary defects
Aortic Arch Anomalies
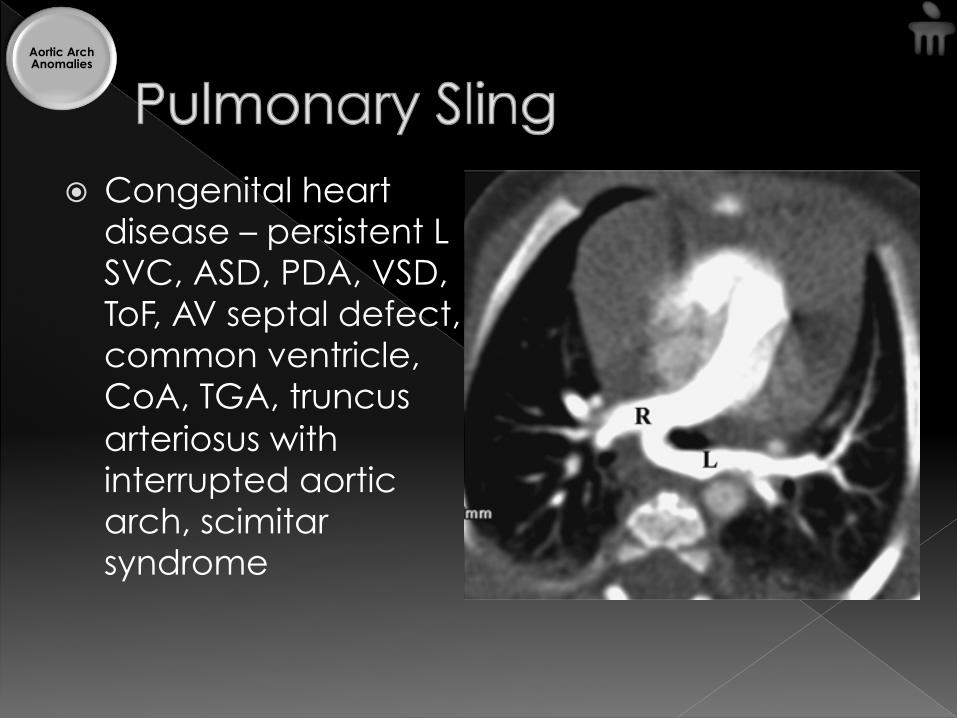
� Congenital heart disease – persistent L SVC, ASD, PDA, VSD, ToF, AV septal defect, common ventricle, CoA, TGA, truncus arteriosus with interrupted aortic arch, scimitar syndrome
Aortic Arch Anomalies
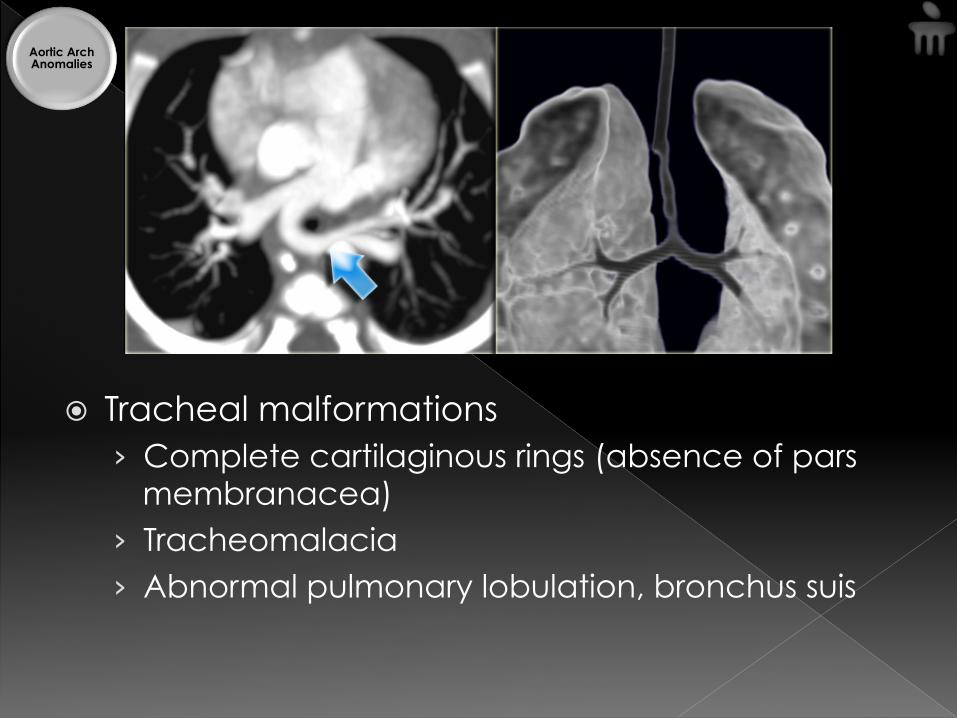
� Tracheal malformations › Complete cartilaginous rings (absence of pars
membranacea) › Tracheomalacia › Abnormal pulmonary lobulation, bronchus suis
Aortic Arch Anomalies
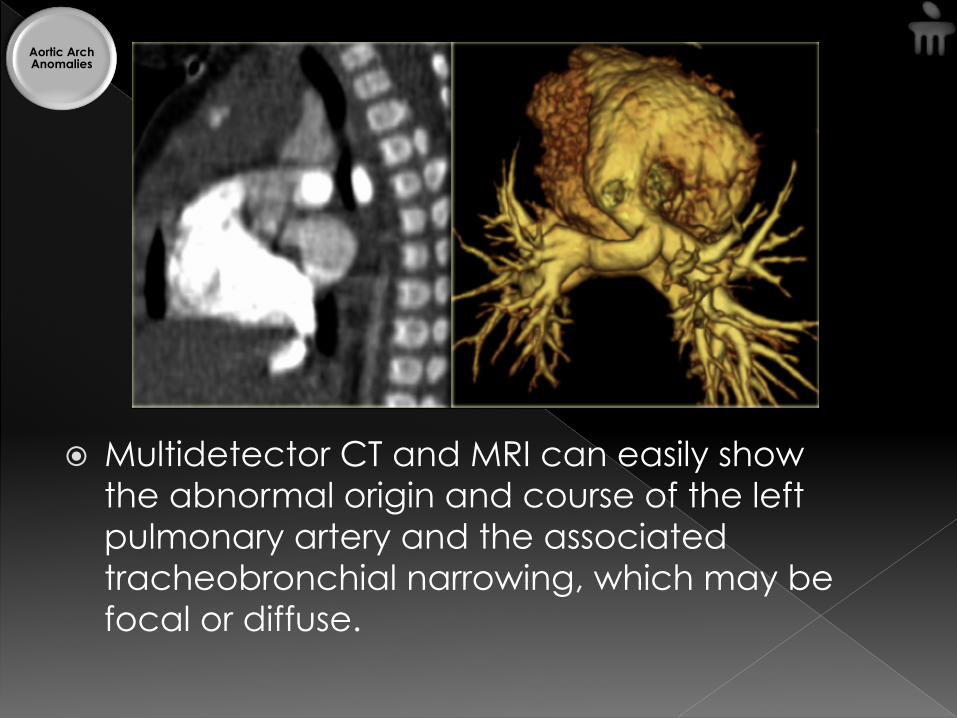
� Multidetector CT and MRI can easily show the abnormal origin and course of the left pulmonary artery and the associated tracheobronchial narrowing, which may be focal or diffuse.
Aortic Arch Anomalies

6-month old male who presents to the pediatric clinic with difficulty breathing. He has had similar episodes in the past. He has been diagnosed with asthma and has been treated with albuterol with only modest improvement. He has some nasal congestion, but no fever, vomiting or diarrhea. He feeds well and he has been gaining weight well.
� His past history is remarkable for multiple upper respiratory infections and wheezing during the past several months. He was born at term. His family history is significant for asthma in several relatives and his older siblings. He has three siblings who currently have colds.
Case

Examination � Pulse: 114 bpm � Resp rate: 39 pm � BP: 100/75 � He is alert, active, and in no distress. He is
not toxic. � URT - clear nasal mucus, normal TM's and a
clear pharynx with normal oral mucosa. � Heart regular without murmurs, but his
breath sounds are noisy so it is difficult to be sure. He has mild inspiratory and expiratory "wheezing".
� His lung fields demonstrate good aeration. He has no retractions. His abdomen is soft, non-tender and without organomegaly. His neurologic exam is unremarkable.
Case
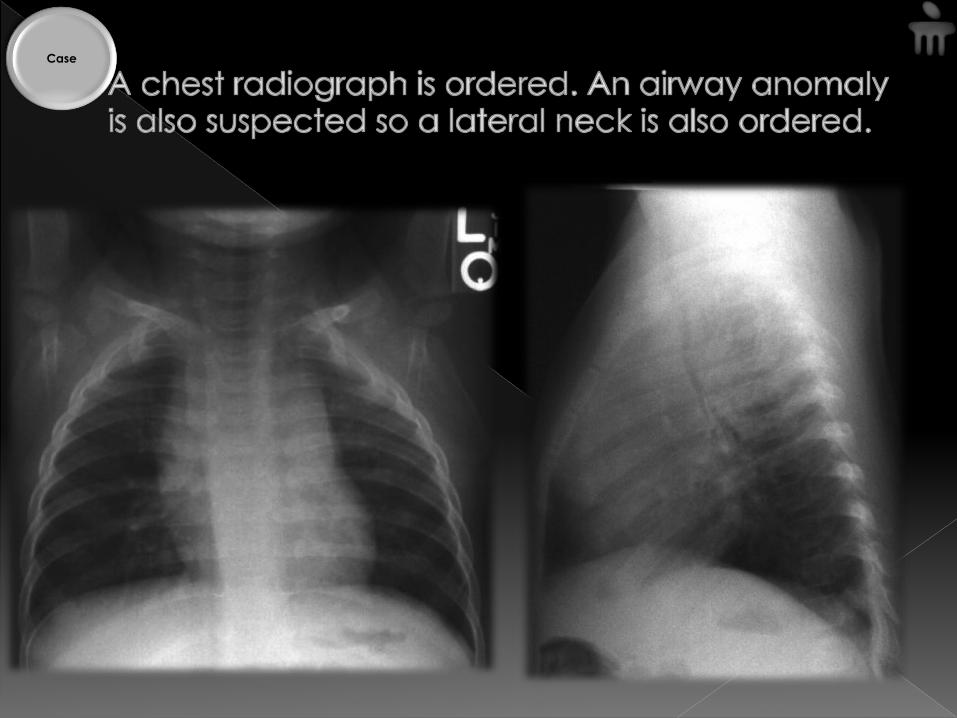
Case
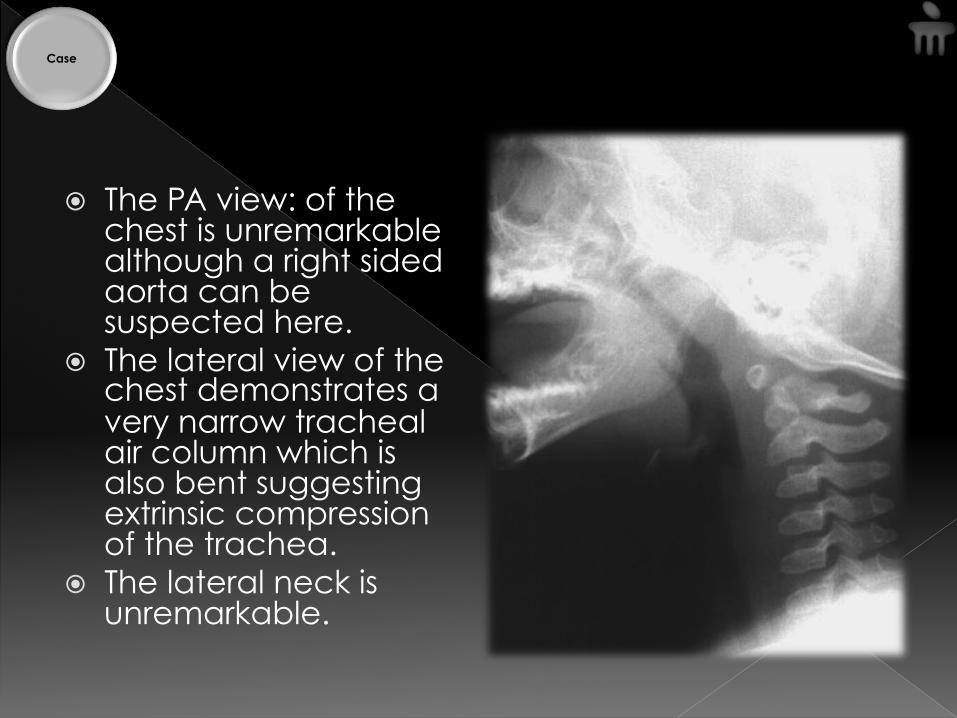
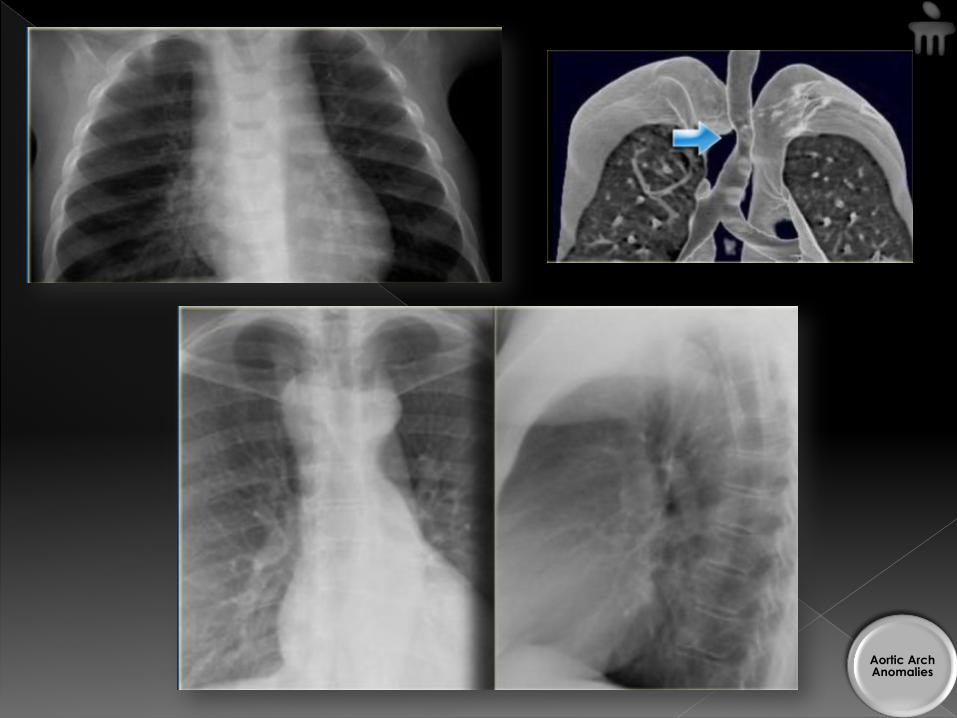
� The PA view: of the chest is unremarkable although a right sided aorta can be suspected here.
� The lateral view of the chest demonstrates a very narrow tracheal air column which is also bent suggesting extrinsic compression of the trachea.
� The lateral neck is unremarkable.
Case
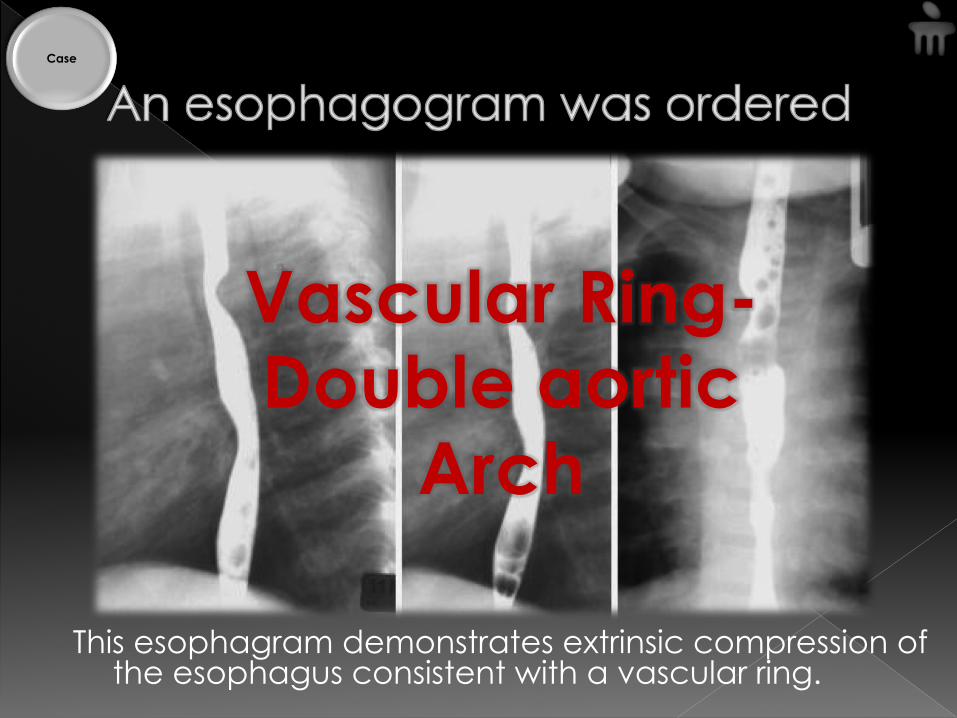
This esophagram demonstrates extrinsic compression of the esophagus consistent with a vascular ring.
Vascular Ring- Double aortic
Arch
Case

� A combination of chest radiography, barium study and ECHO more often than not helps identify the type of aortic arch anomaly in symptomatic patients.
� If the findings are equivocal, then CT/MR can be resorted to. (a catheter angiography only if necessitated)
� Surgical intervention – depends on severity of symptoms and the anomaly per se.
1. The Science and Practice of Pediatric Cardioliogy by
Williams and Wilkins
2. CT and MR Angiography - Comprehensive Vascular
Assessment by Geoffrey D. Rubin
3. Vascular Anomalies of Aorta, Pulmonary and Systemic
vessels by Marilyn J. Siegel and Robin Smithuis -
theRadiologyAssistant
4. Textbook of Radiology and Imaging by David Sutton
5. Grainger and Allison’s Diagnostic Radiology
Thank you J !