surgical treatment for aortic arch aneurysms
TRANSCRIPT

Lenox Hill Heart and VascularInstitute of New York
Surgical Treatment for AorticArch Aneurysms
Konstadinos A Plestis, MD
Associate Professor
Director of Aortic Surgery
Department of Thoracic and Cardiovascular Surgery
Lenox Hill Hospital, NY
Lenox Hill Heart and VascularInstitute of New York
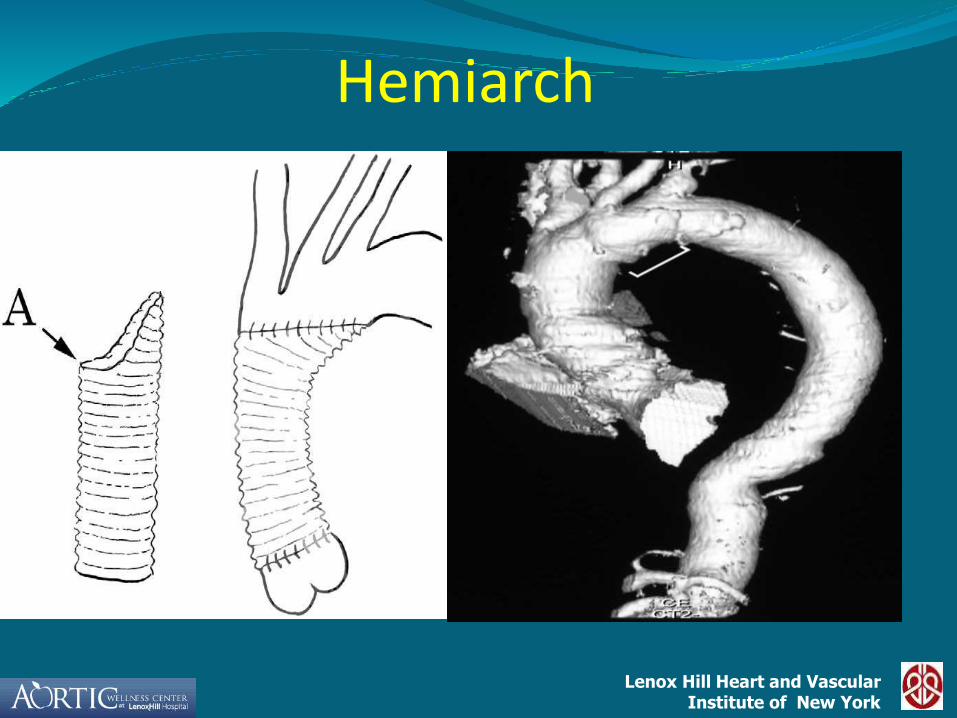
Hemiarch

Lenox Hill Heart and VascularInstitute of New York
Total Arch
Lenox Hill Heart and VascularInstitute of New York
Types of Cerebral Injuryduring Arch Surgery
Focal embolic
Diffuse ischemic
Lenox Hill Heart and VascularInstitute of New York
METHODS OF CEREBRAL PROTECTION
Deep hypothermic circulatory arrest HCA
Griepp 1975
Retrograde cerebral perfusion RCP
Ueda 1990, Takamoto 1992, Safi 1993
Antegrade cerebral perfusion ACP
Debakey 1957, Frist 1986, Bachet 1991, Kazui 1992
Lenox Hill Heart and VascularInstitute of New York
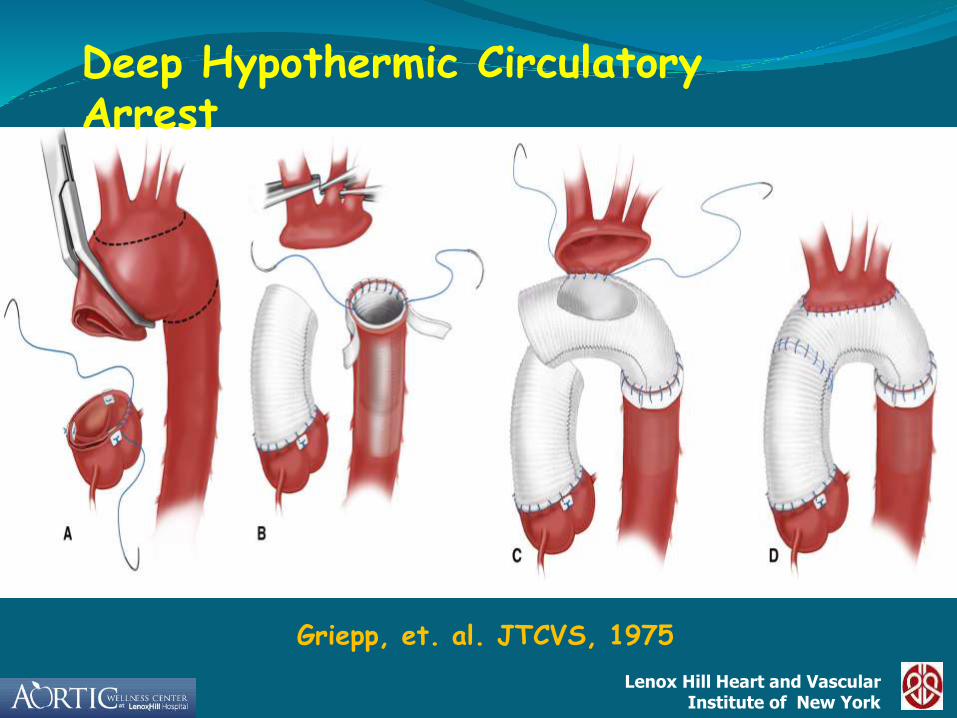
Griepp, et. al. JTCVS, 1975
Deep Hypothermic Circulatory Arrest
Lenox Hill Heart and VascularInstitute of New York
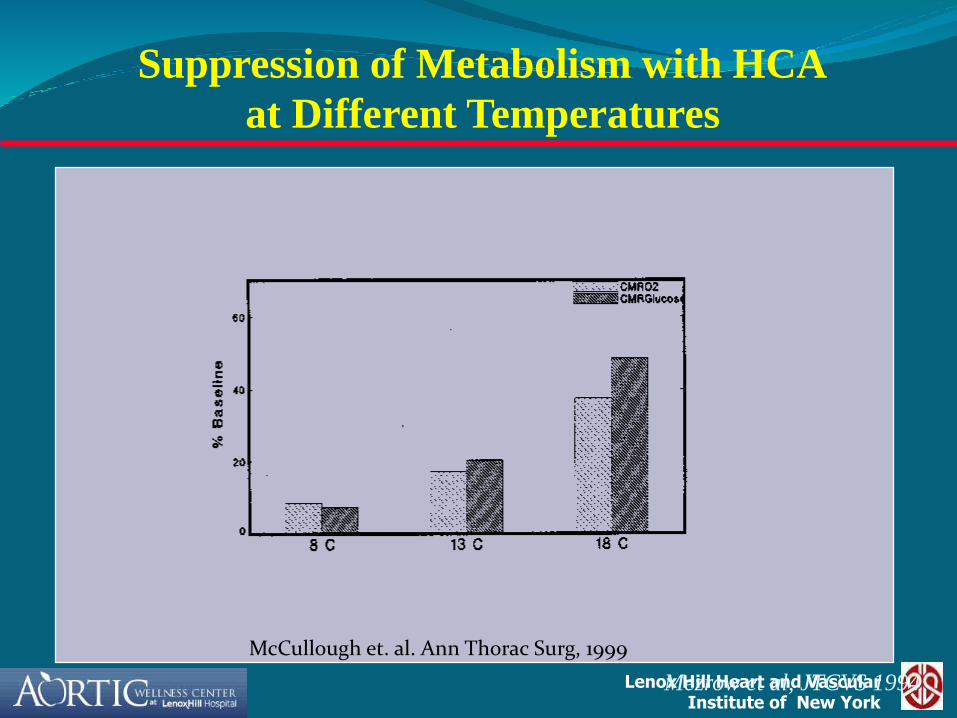
Suppression of Metabolism with HCA
at Different Temperatures
Mezrow et al, JTCVS 1994
McCullough et. al. Ann Thorac Surg, 1999

Lenox Hill Heart and VascularInstitute of New York
0
20
40
60
80
100
120
37 30 25 20 15 10
0
5
10
15
20
25
30
35
40
45
% CMRO2
SAFE HCA
Duration of HCAMin
% C
MR
O2
Temperature °C
Actual Q10 directly calculated in 37 Adult patients during DHCA
What is the LIMIT of “SAFE” HCA?
McCullough et. al. Ann Thorac Surg, 1999
Lenox Hill Heart and VascularInstitute of New York
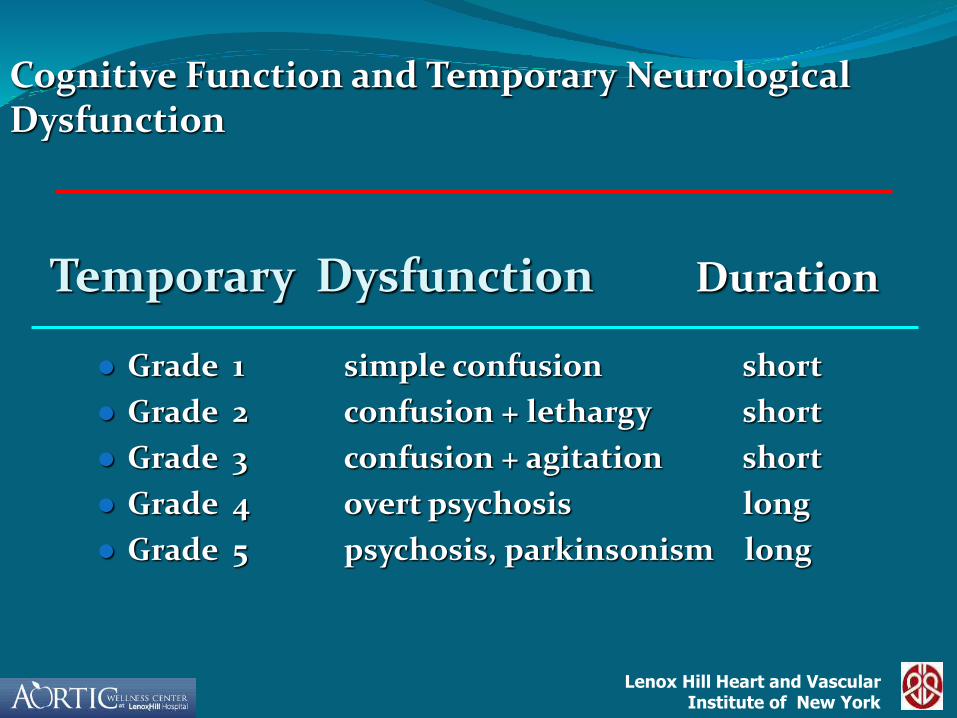
Temporary Dysfunction Duration
Grade 1 simple confusion short
Grade 2 confusion + lethargy short
Grade 3 confusion + agitation short
Grade 4 overt psychosis long
Grade 5 psychosis, parkinsonism long
Cognitive Function and Temporary Neurological Dysfunction
Lenox Hill Heart and VascularInstitute of New York
DHCA > 25 minutes
Advanced age
Neuropsychological impairment in fine motor and memory functions
Temporary Neurologic Dysfunction

Lenox Hill Heart and VascularInstitute of New York
Selective Antegrade Cerebral Perfusion

Lenox Hill Heart and VascularInstitute of New York
Neurological Outcome after Thoracic Aortic Surgery
Effect of Cerebral Protection Method on Stroke,
0
5
10
15
20
HCA HCA+ACP
Transient
Permanent
Stroke [%]
Transient
Permanent
Hagl et. al. JTCVS, 2001
Lenox Hill Heart and VascularInstitute of New York
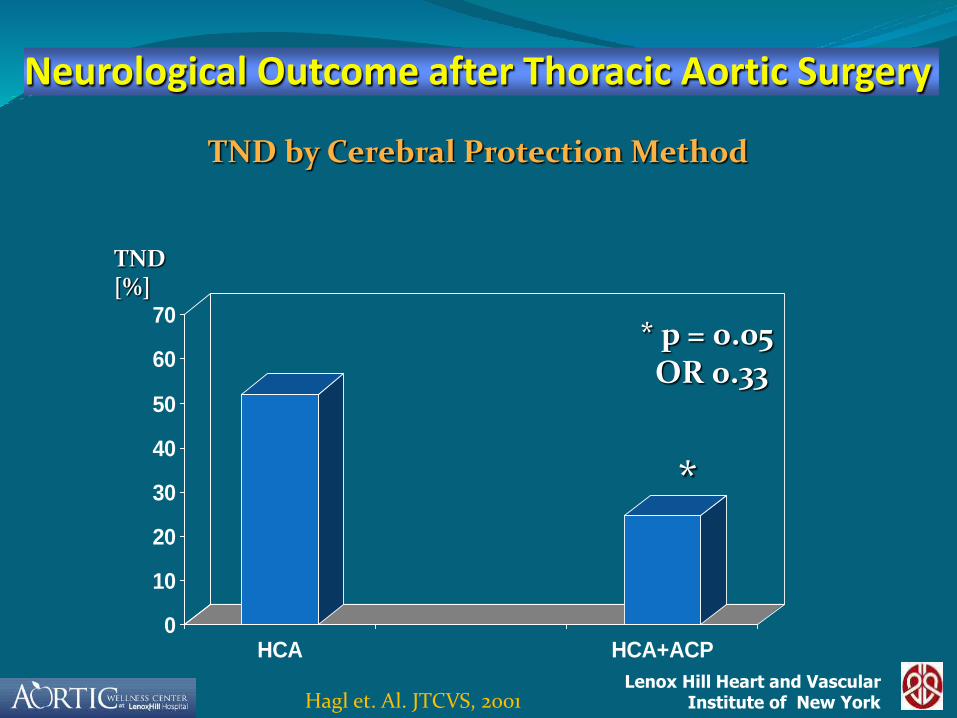
Neurological Outcome after Thoracic Aortic Surgery
TND by Cerebral Protection Method
0
10
20
30
40
50
60
70
HCA HCA+ACP
TND [%]
*
* p = 0.05OR 0.33
Hagl et. Al. JTCVS, 2001

Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York
Lenox Hill Heart and VascularInstitute of New York
Srategies to Minimize Cerebral Injury in Arch Surgery
Minimize particulate embolization
Axillary cannulation
Avoid manipulation of diseased vessels
Trifurcation graft
Aspirate cerebral vessels prior to resuming cerebral perfusion

Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York
• 22F – 26F
• wire-reinforced
• right angled
• flexible cannula
Lenox Hill Heart and VascularInstitute of New York
Pre-operative Aneurysm

Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York
Srategies to Minimize Cerebral Injuryduring Aortic Arch Surgery
Optimize implementation of HCA
Trifurcation graft (arch first technique)
EEG, SSEP
INVUS
Head packed in ice
Antegrade selective cerebral perfusion
Lenox Hill Heart and VascularInstitute of New York
OPTIMAL PARAMETERS FOR SELECTIVE CEREBRAL PERFUSION
Temperature: 10º-15ºC
Pressure: 50-70 torr
pH management: alpha stat
Hematocrit: 30%
Lenox Hill Heart and VascularInstitute of New York
Re-Operative Complex
Aortic Arch Repair
Konstadinos A Plestis, MDDirector, Aortic Surgery
Lenox Hill Hospital
Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York
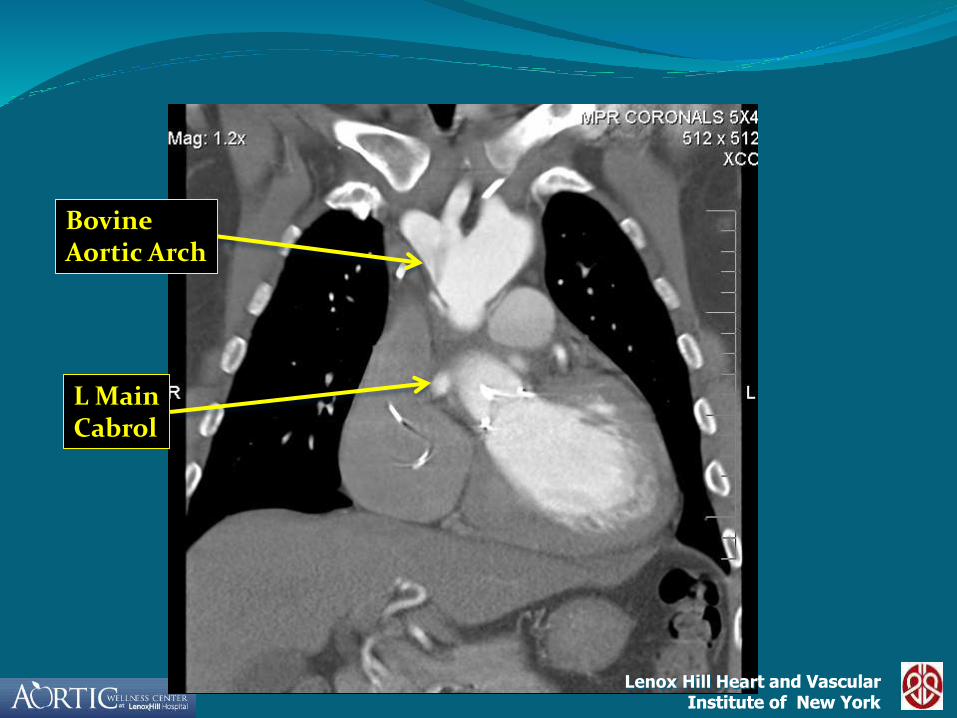
Case presentation 53 yr male
s/p AVR (bioprosthesis)- 2006
s/p Type A Aortic Dissection – 2007
Aortic Root Replacement
bioprosthetic composite valve graft
reimplantation of the right and left main coronary arteries (Cabrol)
Lenox Hill Heart and VascularInstitute of New York
Lenox Hill Heart and VascularInstitute of New York
BovineAortic Arch
L MainCabrol
Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York
True Lumen
False Lumen
Left Subclavian
RightCabrol Left Cabrol
Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York
True Lumen Thrombus
Lenox Hill Heart and VascularInstitute of New York
Lenox Hill Heart and VascularInstitute of New York
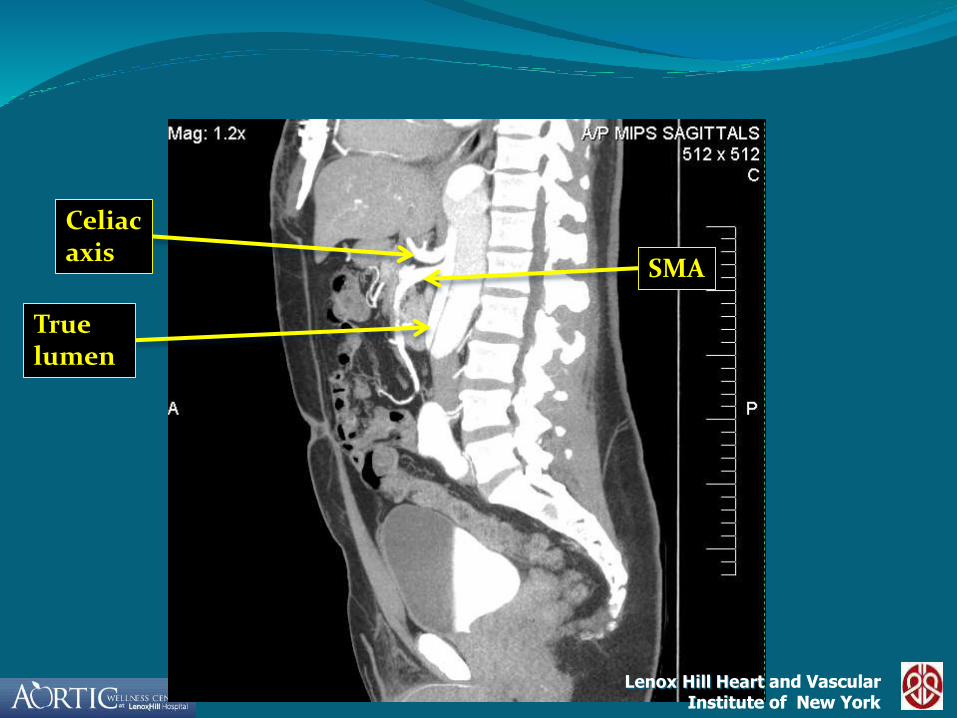
Celiacaxis
SMA
True lumen
Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York
• Right subclavian artery and right femoral vein cannulation
• Re-redo median sternotomy on bypass
• Deep Hypothermic Circulatory Arrest at 20° C
Lenox Hill Heart and VascularInstitute of New York
Lenox Hill Heart and VascularInstitute of New York
Surgical Strategy
• Trifurcation graft to innominate, left carotid and left subclavian arteries
• Antegrade selective cerebral perfusion
• Fenestration of the descending aorta
• Elephant trunk (Stage I)
Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York

Lenox Hill Heart and VascularInstitute of New York
• 66 yo Female
• S/P Right Nephrectomy
• Severe retrosternal chest pain

Lenox Hill Heart and VascularInstitute of New York
CT Angiogram:
Ascending: 8 cm Arch: 5.4 cm Descending: 8cm.
Abdominal: 11.7 cm.

Lenox Hill Heart and VascularInstitute of New York
Distal Arch

Lenox Hill Heart and VascularInstitute of New York
Ascending
Descending

Lenox Hill Heart and VascularInstitute of New York
Descending

Lenox Hill Heart and VascularInstitute of New York
Supraceliac Aorta

Lenox Hill Heart and VascularInstitute of New York
Abdominal Aorta

Lenox Hill Heart and VascularInstitute of New York
Ascending Aorta
Abdominal Aorta
Lenox Hill Heart and VascularInstitute of New York
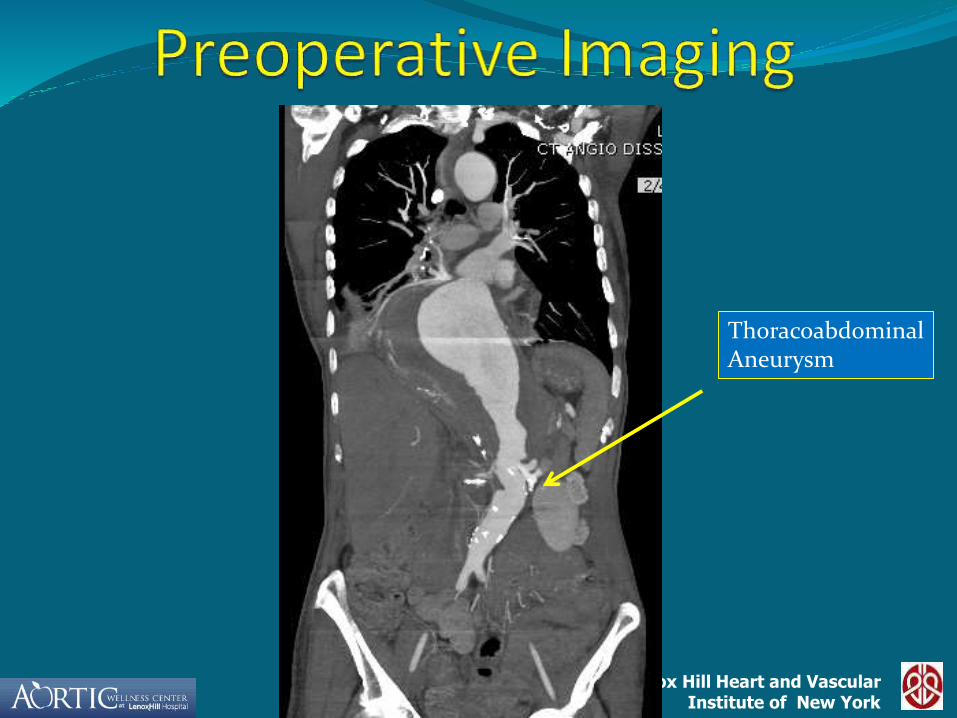
Thoracoabdominal Aneurysm

Lenox Hill Heart and VascularInstitute of New York
• Aortic Valve Repair
• Replacement of Ascending/ Arch Aorta
•(Stage I – Elephant Trunk)
• Reimplantation of Brachiocephalic, left Carotid
and left Subclavian
•(Trifurcation graft)
•DHCA, ACP, SSEP, EEG

Lenox Hill Heart and VascularInstitute of New York
Elephant Trunk

Lenox Hill Heart and VascularInstitute of New York
Elephant Trunk Graft
Lenox Hill Heart and VascularInstitute of New York
•Replacement of type I TAAA (stage II ET)
•Reimplantation of Celiac, SMA, Left Renal Artery
(trifurcation graft)
•Perfusion of Celiac, SMA, and Left Renal with cold blood
•DAP, CSF drainage, SSEP, MEP
Lenox Hill Heart and VascularInstitute of New York
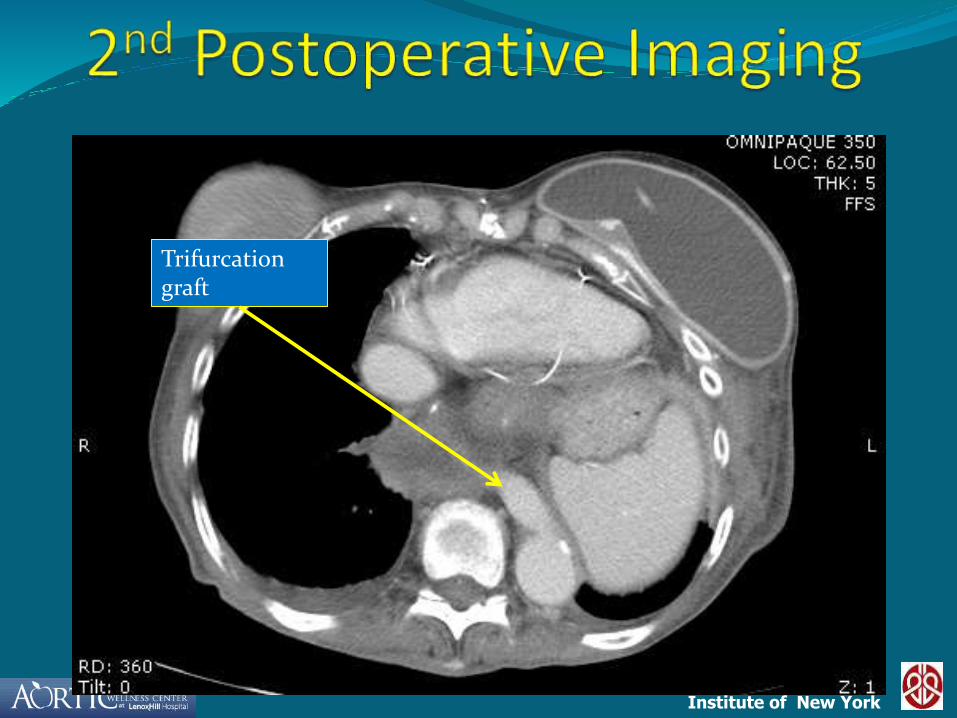
Trifurcation graft
Lenox Hill Heart and VascularInstitute of New York
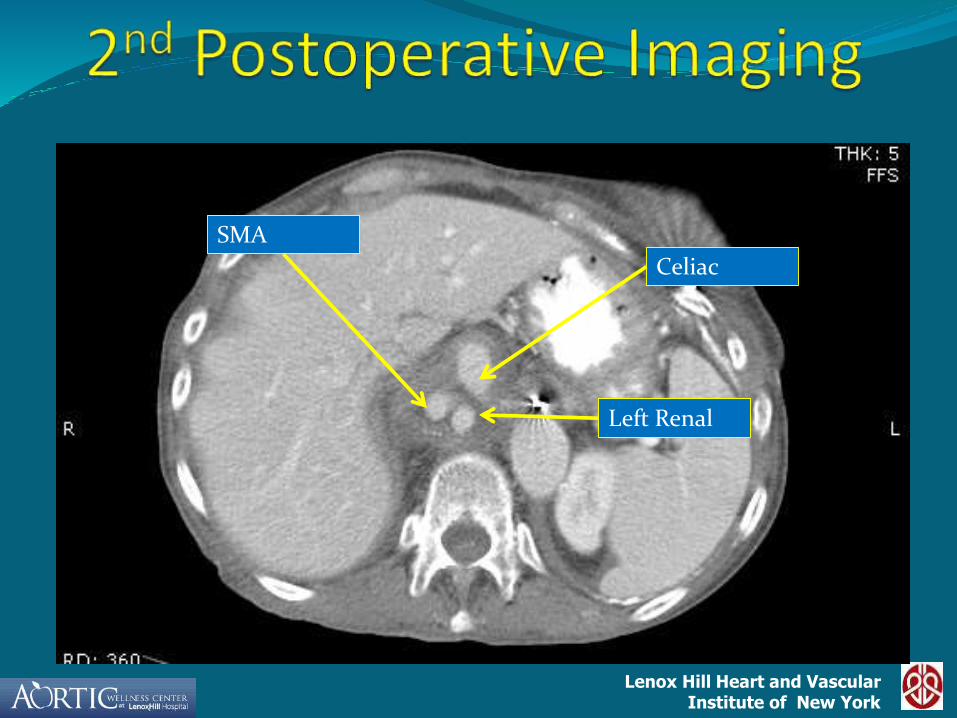
Celiac
SMA
Left Renal

Lenox Hill Heart and VascularInstitute of New York
Left renal
Lenox Hill Heart and VascularInstitute of New York
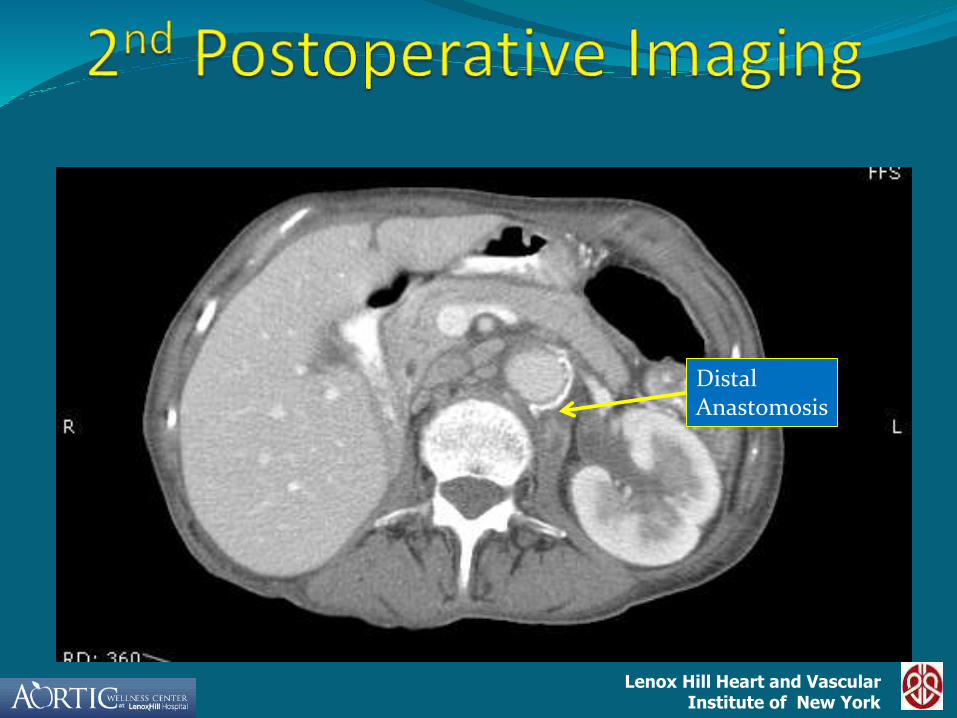
Distal Anastomosis

Lenox Hill Heart and VascularInstitute of New York
• 70 yo Female
• S/P Type A - Aortic dissection repair (‘96)
• Severe retrosternal chest pain

Lenox Hill Heart and VascularInstitute of New York
CT Angiogram:
Ascending Aorta = 5.0 cm.
Aortic Arch = 6.0 cm.
Descending Aorta = 3.4 cm.
Lenox Hill Heart and VascularInstitute of New York
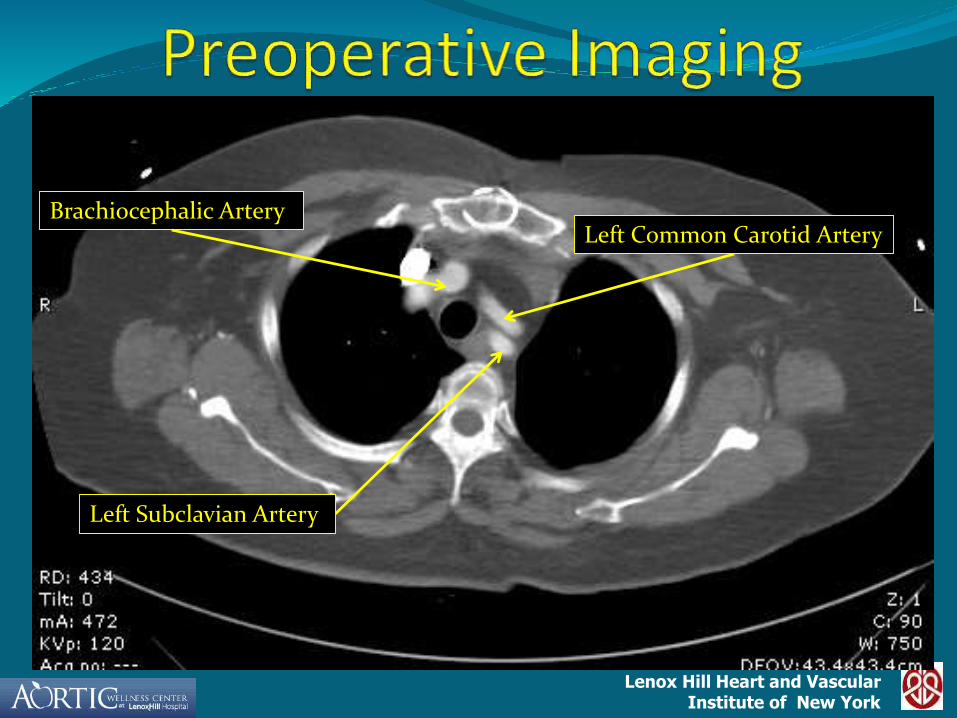
Brachiocephalic ArteryLeft Common Carotid Artery
Left Subclavian Artery

Lenox Hill Heart and VascularInstitute of New York
False Lumen of Dissection
Brachiocephalic Artery
Left Subclavian Artery
Left Common Carotid Artery
Lenox Hill Heart and VascularInstitute of New York
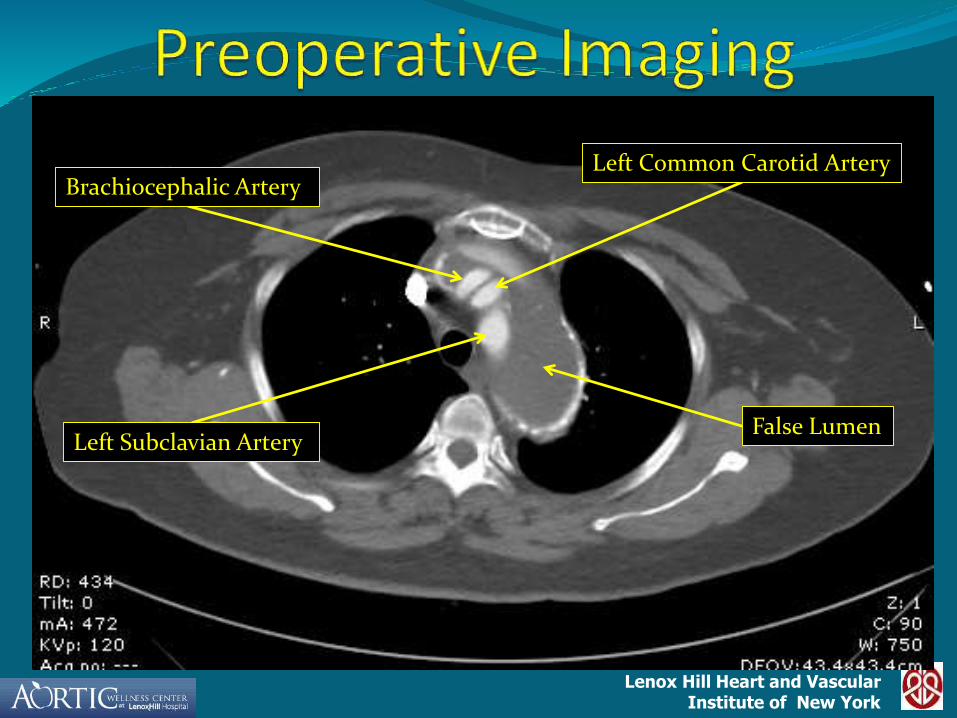
False Lumen
Brachiocephalic Artery
Left Subclavian Artery
Left Common Carotid Artery

Lenox Hill Heart and VascularInstitute of New York
False Lumen
True Lumen

Lenox Hill Heart and VascularInstitute of New York
False lumen
True Lumen
Lenox Hill Heart and VascularInstitute of New York
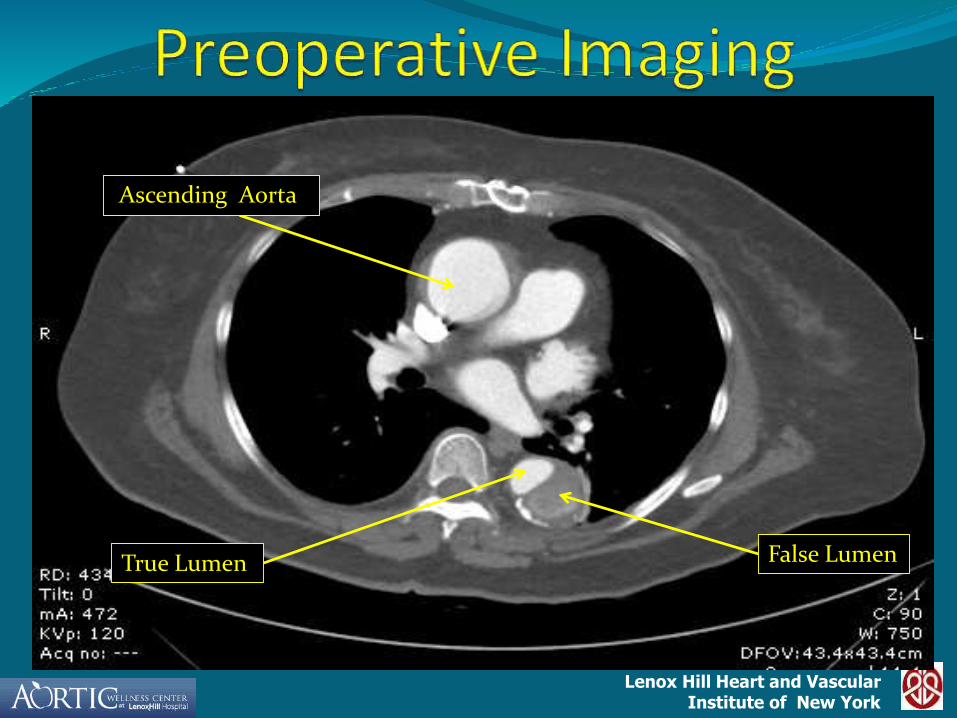
Ascending Aorta
False LumenTrue Lumen

Lenox Hill Heart and VascularInstitute of New York
False Lumen
True Lumen

Lenox Hill Heart and VascularInstitute of New York
True LumenFalse Lumen False Lumen
Lenox Hill Heart and VascularInstitute of New York
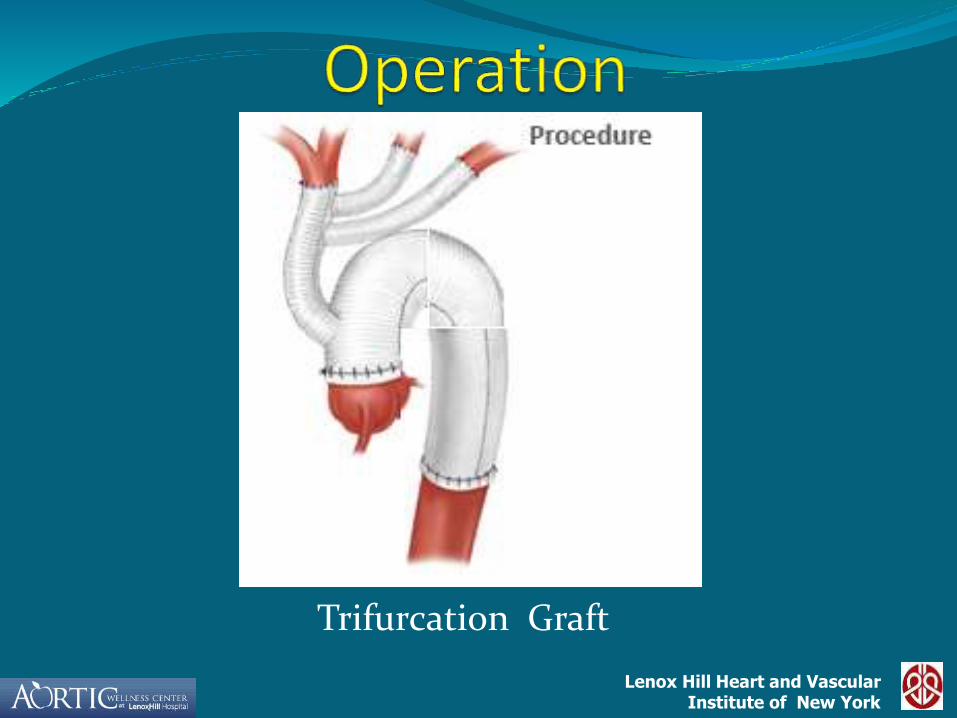
•Bilateral Anterior Thoracotomy
•Replacement of Ascending/ Arch/ Descending with a 22 mm Dacron graft.
•Reimplantation of Brachiochephalic, Left Carotid, Left Subclavian with a trifurcation graft.
•DHCA, ACP, EEG,SSEP
Lenox Hill Heart and VascularInstitute of New York
Trifurcation Graft
Lenox Hill Heart and VascularInstitute of New York
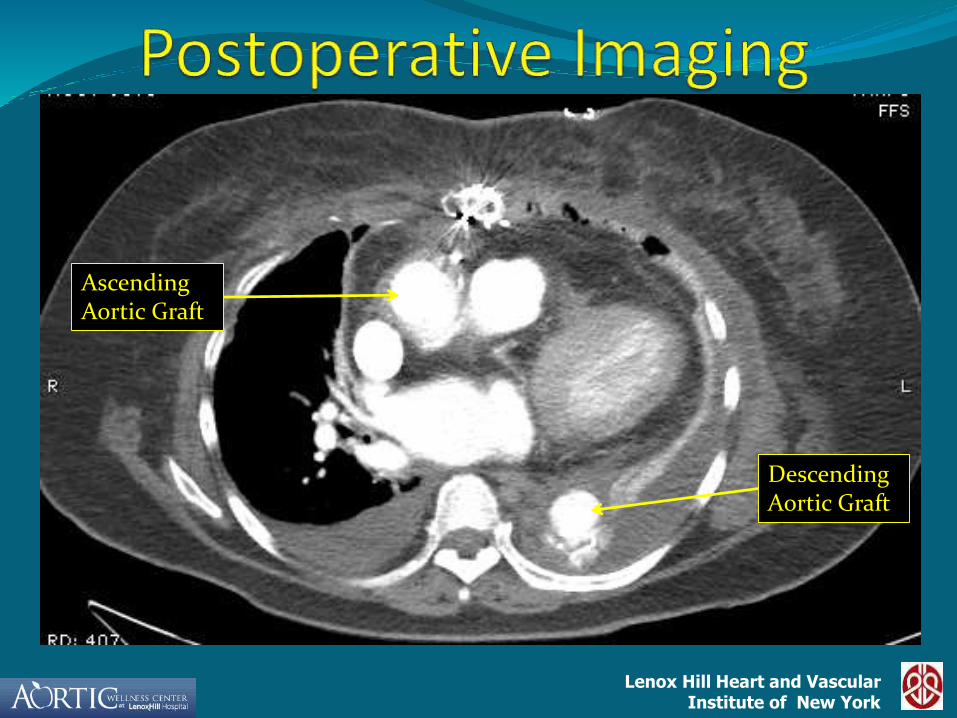
Descending Aortic Graft
Ascending Aortic Graft

Lenox Hill Heart and VascularInstitute of New York
Trifurcation
Lenox Hill Heart and VascularInstitute of New York
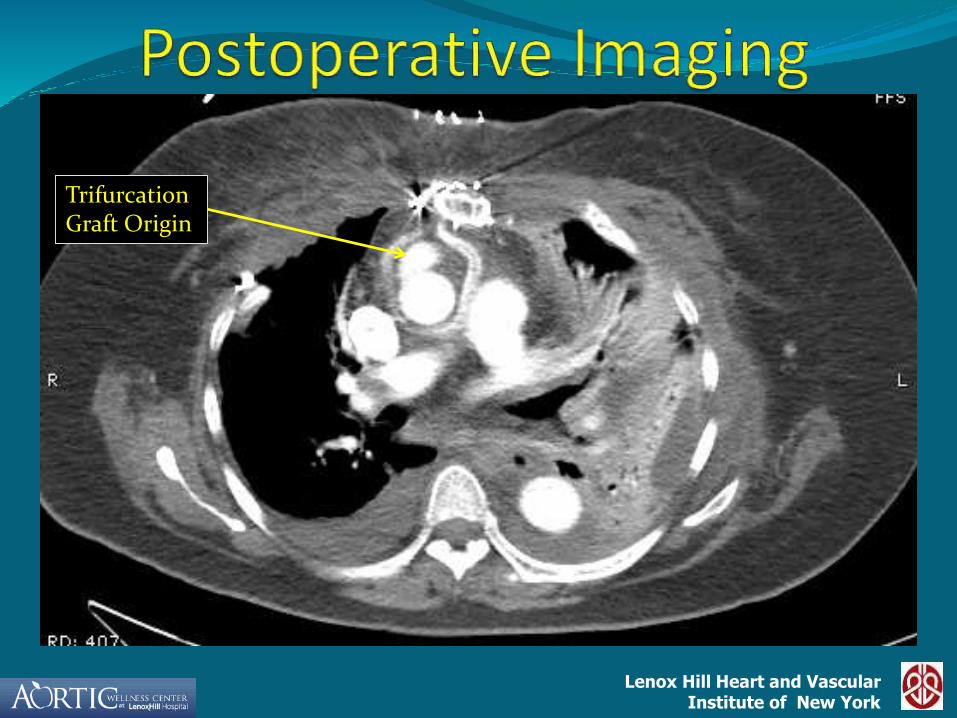
Trifurcation Graft Origin

Lenox Hill Heart and VascularInstitute of New York
Ascending Aortic Graft
Brachiocephalic branch of graft
Left Carotid
Lenox Hill Heart and VascularInstitute of New York
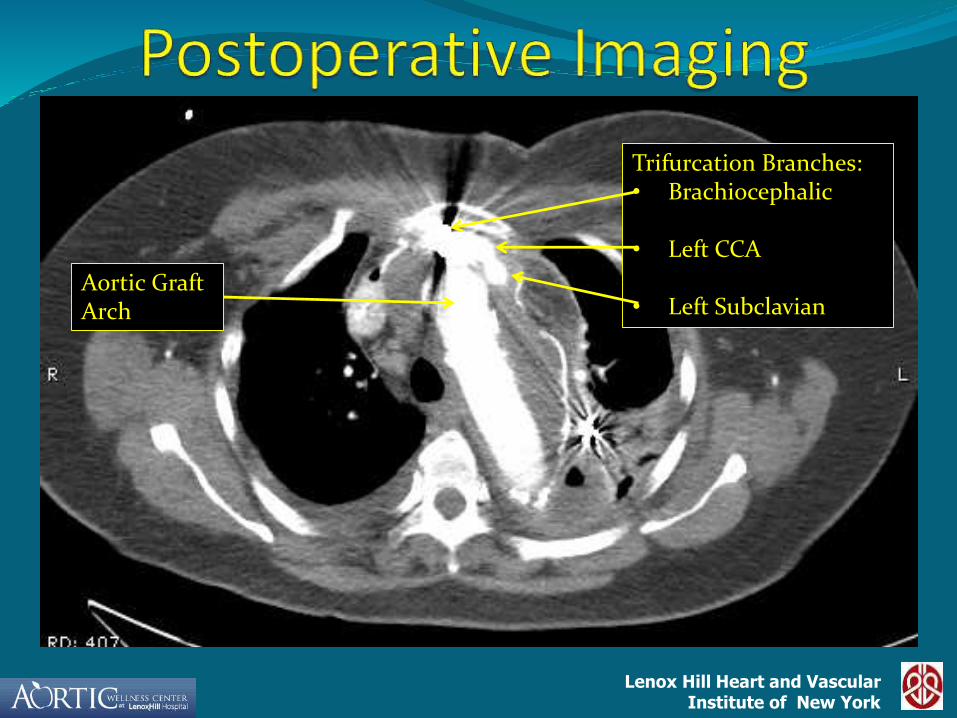
Aortic Graft Arch
Trifurcation Branches:• Brachiocephalic
• Left CCA
• Left Subclavian

Lenox Hill Heart and VascularInstitute of New York
False Lumen
Graft
Distal End of GraftGraft

Lenox Hill Heart and VascularInstitute of New York
Arch Replacement
9/05-9/11
N=157 Pts
Hemiarch 100
Total Arch 57
Lenox Hill Heart and VascularInstitute of New York
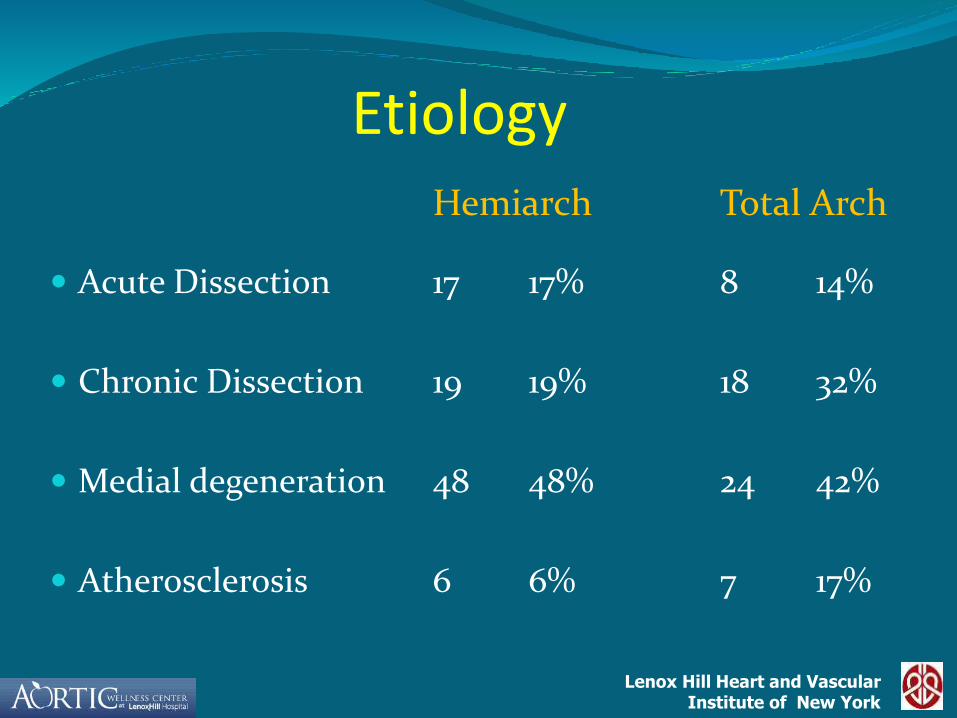
Etiology
Acute Dissection 17 17% 8 14%
Chronic Dissection 19 19% 18 32%
Medial degeneration 48 48% 24 42%
Atherosclerosis 6 6% 7 17%
Hemiarch Total Arch

Lenox Hill Heart and VascularInstitute of New York
Demographics
HTN 80 80% 47 82%
ASHD 1 9 19% 15 26%
COPD 24 24% 9 16%
Cerebrovascular 12 12% 10 18%
disease
Hemiarch Total Arch

Lenox Hill Heart and VascularInstitute of New York
Operative Variables
Root 57 57% 13 23%
Redo 33 33% 21 37%
Elective 60 60% 31 54%
Hemiarch Total Arch

Lenox Hill Heart and VascularInstitute of New York
Operative variables
Right Axillary 33 33% 50 88%
cannulation
RCP 44 44% 4 7%
ACP 15 15% 44 77%
Hemiarch Total Arch
Lenox Hill Heart and VascularInstitute of New York
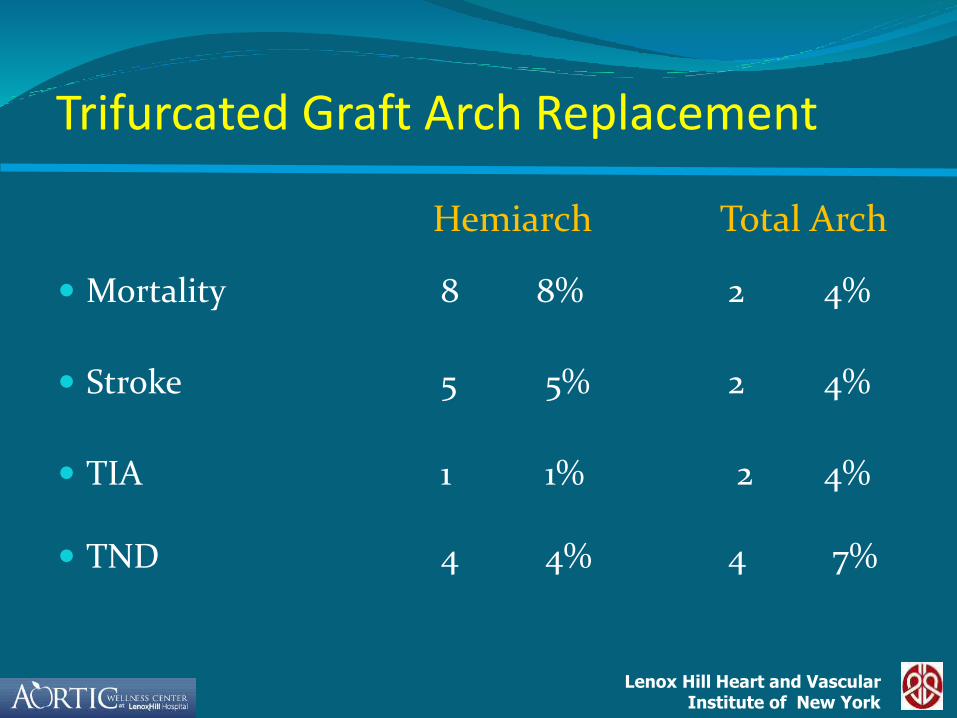
Trifurcated Graft Arch Replacement
Mortality 8 8% 2 4%
Stroke 5 5% 2 4%
TIA 1 1% 2 4%
TND 4 4% 4 7%
Hemiarch Total Arch
Lenox Hill Heart and VascularInstitute of New York
Conclusions
Total Aortic Arch replacement with the trifurcation graft has led to simplification of the technical aspects of the operation
The technique is very versatile and can be used in all the anatomical circumstances
The mortality and neurologic morbidity of arch replacement have improved significantly with the aid of antegrade and retrograde cerebral perfusion techniques
Lenox Hill Heart and VascularInstitute of New York
Thank you