antituberculosis drugs
DESCRIPTION
dTRANSCRIPT

BismillahirrohmaanirrohiimBismillahirrohmaanirrohiim
Asyhadu anlaa ilaaha illallohAsyhadu anlaa ilaaha illallohwa asyhadu anna Muhammadan rasuulullohwa asyhadu anna Muhammadan rasuululloh
Rodliitu billahi robbaaRodliitu billahi robbaawa bil-islaami diinaawa bil-islaami diinaawa bi Muhammadin nabiyyaw wa rosuulaawa bi Muhammadin nabiyyaw wa rosuulaa
Robbii zidni ‘ilmaaRobbii zidni ‘ilmaawarzuqnii fahmaawarzuqnii fahmaaAamiin....Aamiin....
Do’a belajar
CURRICULUM VITAECURRICULUM VITAE
Wiwik Kusumawati, Wiwik Kusumawati, MDMD, M, Master of Health aster of Health ScienceScience
Lecturer of Pharmacology (1996 to Lecturer of Pharmacology (1996 to nownow)) Lecturer of Medical Education (2004 to Lecturer of Medical Education (2004 to nownow)) Vice Dean for academic affair (2004 to 2007)Vice Dean for academic affair (2004 to 2007) Coordinator of Pharmacology Dept (1996 to Coordinator of Pharmacology Dept (1996 to
2002)2002) Coordinator of Medical Education Unit (2004 to Coordinator of Medical Education Unit (2004 to
2010)2010)
CURRICULUM VITAECURRICULUM VITAE PhD Cand. of Medical Education of PhD Cand. of Medical Education of Faculty of Faculty of
Medicine Gadjah Mada University, Yogyakarta Medicine Gadjah Mada University, Yogyakarta ((20072007 – – nownow))
Magister of Health Sciences from Faculty of Magister of Health Sciences from Faculty of Medicine of Gadjah Mada University, Medicine of Gadjah Mada University, Yogyakarta (1997 – 2000)Yogyakarta (1997 – 2000)
Medical Doctor from Faculty of Medicine of Medical Doctor from Faculty of Medicine of Airlangga University, Surabaya (1985 – 1991)Airlangga University, Surabaya (1985 – 1991)
General Practitioner (PTT doctor) at Ende, General Practitioner (PTT doctor) at Ende, Flores, NTT (1992Flores, NTT (1992 – – 1995)1995)

ANTITUBERCULOSIS ANTITUBERCULOSIS DRUGSDRUGSByBy
Wiwik KusumawatiWiwik Kusumawati

INTRODUCTIONINTRODUCTION
Tuberculosis InfectionTuberculosis Infection
??

INTRODUCTIONINTRODUCTION
Pulmonary tuberculosisPulmonary tuberculosis 7.5 to10.2 million new cases of tbc (WHO) 7.5 to10.2 million new cases of tbc (WHO) 2.5 to 3.5 million tuberculosis death2.5 to 3.5 million tuberculosis death Develop and developing countriesDevelop and developing countries Immunodeficiency virus (HIV) infectionImmunodeficiency virus (HIV) infection Up 80 % tbc px are HIV positiveUp 80 % tbc px are HIV positive 3.5 million, dual infection3.5 million, dual infection Reactivation – dormant infectionReactivation – dormant infection

INTRODUCTIONINTRODUCTION
Tbc infection in Indonesia?Tbc infection in Indonesia? PopulationPopulation Status of immunityStatus of immunity Status of economy Status of economy - nutrition - nutrition

CASE CASE
A A 554 years old man 4 years old man bring to the hospital with bring to the hospital with cough more than 3 weeks, cough more than 3 weeks, fever,fever, and and decreasing of appetitedecreasing of appetite after taking history and after taking history and conducting clinical examination, the doctor do conducting clinical examination, the doctor do laboratory test (sputum test). Laboratory result laboratory test (sputum test). Laboratory result revealed mycobactterium tbc positive and the revealed mycobactterium tbc positive and the doctor prescribe antituberculosis drugs.doctor prescribe antituberculosis drugs.

Pulmonary Pulmonary TTuberculosisuberculosis
Prompt diagnosis and effective treatmentPrompt diagnosis and effective treatment General symptomsGeneral symptoms
Weight loss, malaise, feversWeight loss, malaise, fevers
Respiratory symptomsRespiratory symptoms Cough, sputum and haemoptysisCough, sputum and haemoptysis

Resistance of M. Resistance of M. tuberculosis tuberculosis Spontaneous mutationSpontaneous mutation Improperly prescribed therapyImproperly prescribed therapy Erratic drug ingestionErratic drug ingestion Inadequate dosageInadequate dosage Incomplete therapyIncomplete therapy Lack of compliance by pxLack of compliance by px

Resistance of M. Resistance of M. tuberculosis tuberculosis MDR : INH and RifampicinMDR : INH and Rifampicin XDR : + Fluoroquinolone + 1 injection XDR : + Fluoroquinolone + 1 injection
drugdrug Primary Primary Secondary Secondary

Distribution of Primary MDRDistribution of Primary MDR

Distribution of Secondary Distribution of Secondary MDRMDR


MAJOR PROBLEM?MAJOR PROBLEM?
Compliance ?Compliance ?
DOT’SDOT’S
DIRECTLY OBSERVE THERAPYDIRECTLY OBSERVE THERAPY Five component of DOTSFive component of DOTS
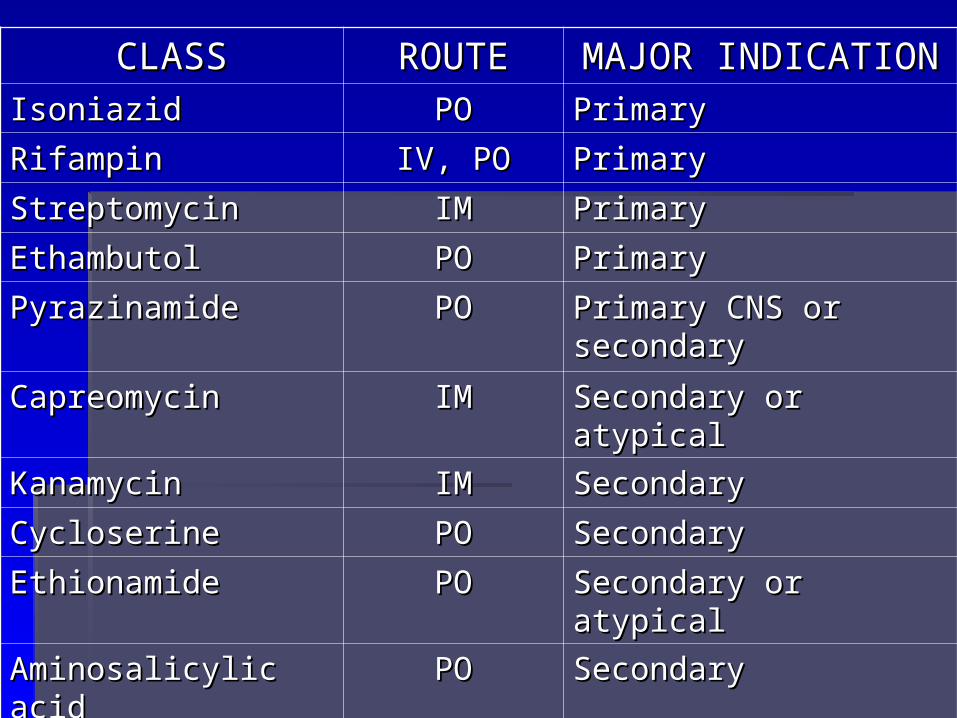
CLASSCLASS ROUTEROUTE MAJOR INDICATIONMAJOR INDICATION
IsoniazidIsoniazid POPO Primary Primary
RifampinRifampin IV, POIV, PO Primary Primary
StreptomycinStreptomycin IMIM Primary Primary
EthambutolEthambutol POPO Primary Primary
PyrazinamidePyrazinamide POPO Primary CNS or Primary CNS or secondary secondary
CapreomycinCapreomycin IMIM Secondary or atypicalSecondary or atypical
KanamycinKanamycin IMIM Secondary Secondary
CycloserineCycloserine POPO Secondary Secondary
EthionamideEthionamide POPO Secondary or atypical Secondary or atypical
Aminosalicylic acidAminosalicylic acid POPO Secondary Secondary
ClofazimineClofazimine POPO Atypical in HIV pxAtypical in HIV px
RifabutinRifabutin POPO Atypical in HIV pxAtypical in HIV px

DRUGSDRUGS
INH & RifampinINH & Rifampin Tuberculocidal for both extracellular intracellular Tuberculocidal for both extracellular intracellular
organismorganism Streptomycin Streptomycin
Tuberculocidal for extracellular organism onlyTuberculocidal for extracellular organism only Pyrazinamide Pyrazinamide
Tuberculocidal for intracellular organismTuberculocidal for intracellular organism Ethambutol, p-aminosalicylic acid & Ethambutol, p-aminosalicylic acid &
ethionamideethionamide Tuberculostatic Tuberculostatic
DRUGS (INH)DRUGS (INH)
Bactericidal – cell wall synthesisBactericidal – cell wall synthesis Combination Combination
Active infectionActive infection Secondary chemoprophylaxis Secondary chemoprophylaxis should be given with should be given with
2 or more effective drugs2 or more effective drugs
Should never be used as a single to treat Should never be used as a single to treat active tbcactive tbc
Single agent (monotherapy)Single agent (monotherapy) Primary chemoprophylaxisPrimary chemoprophylaxis
DRUGS (INH)DRUGS (INH) PO: well and rapidly absorbedPO: well and rapidly absorbed Peak concentration 1 to 2 hoursPeak concentration 1 to 2 hours The distribution is extensiveThe distribution is extensive 3 to 5 mg/kg/day – 20 mg/kg/day 3 to 5 mg/kg/day – 20 mg/kg/day Metabolism by acetylation and hydroxylation Metabolism by acetylation and hydroxylation
Slow acetylators (Scandinavia, North Africa) – Slow acetylators (Scandinavia, North Africa) – adverse effectsadverse effects
Rapid acetylators (Japan, Escimo) – Rapid acetylators (Japan, Escimo) – intermittent intermittent regimenregimen
No influence both the effect of therapy and side No influence both the effect of therapy and side effect if INH given everyday effect if INH given everyday
DRUGS (INH)DRUGS (INH)
Side effect Side effect Peripheral neuropathy – 10 mg/day of Peripheral neuropathy – 10 mg/day of
pyridoxine pyridoxine Induced hepatic injuryInduced hepatic injury
DRUGS (Rifampicine)DRUGS (Rifampicine)
A first-line bactericidal anti-tuberculosisA first-line bactericidal anti-tuberculosis Inhibits RNA-polymeraseInhibits RNA-polymerase Combination with pyrazinamide : “persisters” Combination with pyrazinamide : “persisters” PO, IVPO, IV PO : well and completely absorbtion (empty PO : well and completely absorbtion (empty
stomach)stomach) Peak concentration 2 to 4 hoursPeak concentration 2 to 4 hours Combination with INH not influence absorbtionCombination with INH not influence absorbtion

DRUGS (Rifampicine)DRUGS (Rifampicine)
Distribution is extensive, protein Distribution is extensive, protein (albumin) binding 80%(albumin) binding 80%
Red-brown colouration of body fluidRed-brown colouration of body fluid Metabolism deacetylation – active Metabolism deacetylation – active
metabolitemetabolite Excretion : biliary and renal (30%)Excretion : biliary and renal (30%) Resistant rifampicine – rifabutine Resistant rifampicine – rifabutine

DRUGS (Rifampicine)DRUGS (Rifampicine)
Dose 450 – 600 mg/day (adult); 10 – 20 mg/kg Dose 450 – 600 mg/day (adult); 10 – 20 mg/kg BW/day (children)BW/day (children)
Side effectSide effect Rash, fever, nausea, vomitingRash, fever, nausea, vomiting Flu like syndromeFlu like syndrome Hepatotoxic – hepatitis Hepatotoxic – hepatitis

DRUGS (Rifampicine)DRUGS (Rifampicine)
Enzyme hepatic inducer (increase metabolism Enzyme hepatic inducer (increase metabolism of oral contraception, corticosteroid, of oral contraception, corticosteroid, hypoglycemic agent, vitamine D)hypoglycemic agent, vitamine D)
PAS inhibits absorbtion of rifampicinePAS inhibits absorbtion of rifampicine Rifampicine + INH (slow acetlators) Rifampicine + INH (slow acetlators)

DRUGS (Pyrazinamide)DRUGS (Pyrazinamide)
Bactericidal to mycobacteria multiplying Bactericidal to mycobacteria multiplying intracellularly at low pH levelintracellularly at low pH level
The first 2 months of a treatment regimenThe first 2 months of a treatment regimen Reduce later relaps ratesReduce later relaps rates A shorter duration of therapyA shorter duration of therapy PO : well absorbedPO : well absorbed Penetrates well in CSFPenetrates well in CSF Nausea, flushing, arthralgia, Nausea, flushing, arthralgia, hepatotoxic hepatotoxic
reactionsreactions

STREPTOMYCINSTREPTOMYCIN
An aminoglycosideAn aminoglycoside Extracellular bacteria Extracellular bacteria Single drug – no effective Single drug – no effective Must be given by injection (IM)Must be given by injection (IM) Widely distributions – doesn’t cross well Widely distributions – doesn’t cross well
into CSFinto CSF 30 % protein binding 30 % protein binding 90 % drugs excreted via urine 90 % drugs excreted via urine

STREPTOMYCINSTREPTOMYCIN
Dose Dose 20 mg/kg BW – maximally 1 gram/day20 mg/kg BW – maximally 1 gram/day Side effectSide effect Neurotoxic and nephrotoxicNeurotoxic and nephrotoxic 8 cranial nerve damage, vestibular 8 cranial nerve damage, vestibular
toxicity, rashtoxicity, rash Caution Caution Pregnancy, elderly, renal disease, etcPregnancy, elderly, renal disease, etc

ETHAMBUTOLETHAMBUTOL
An essentially bacteriostaticAn essentially bacteriostatic Inhibits mycobacterial cell wall synthesisInhibits mycobacterial cell wall synthesis PO : well absorbed (75% to 80 %)PO : well absorbed (75% to 80 %) Doesn’t cross BBBDoesn’t cross BBB Excretion : unchanged in the urineExcretion : unchanged in the urine

ETHAMBUTOLETHAMBUTOL
Dose 15 mg/kg BW/dayDose 15 mg/kg BW/day Side effectSide effect Retrobulbar neuritis (bilateral)Retrobulbar neuritis (bilateral) Rash, fever, Increasing blood uric acid, Rash, fever, Increasing blood uric acid,
etcetc

INITIAL TREATMENTINITIAL TREATMENT
At least 3 drugsAt least 3 drugs INH, Rifampicin, PyrazinamideINH, Rifampicin, Pyrazinamide For at least 8 weeks – sensitivity For at least 8 weeks – sensitivity
establishedestablished

CONTINUATION CONTINUATION TREATMENTTREATMENT
Rifampicin and INHRifampicin and INH Further 4 monthsFurther 4 months 2HRZ/4HR – 6 months2HRZ/4HR – 6 months 2EHR/7HR – 9 month2EHR/7HR – 9 month Rifampicin not included : 18 months Rifampicin not included : 18 months

MONITORINGMONITORING
Monitoring adverse effect and efficacy of Monitoring adverse effect and efficacy of drugsdrugs
Monitoring up to 1 year after a regimen Monitoring up to 1 year after a regimen completely completely

CASE CASE
A A 444 years old 4 years old woman suffering from tbc woman suffering from tbc infection and also A type of hepatitis infection. infection and also A type of hepatitis infection. Health care provider give this patient Health care provider give this patient rifampicine, INH, pyrazinamide as rifampicine, INH, pyrazinamide as antituberculosis drugs for 2 months in intensive antituberculosis drugs for 2 months in intensive phasephase

SPECIFIC CONDITIONSPECIFIC CONDITION Treatment during pregnancyTreatment during pregnancy
INH, Ethambutol, Rifampicin (safely)INH, Ethambutol, Rifampicin (safely) INH, INH, PyrazinamidePyrazinamide, Rifampicin (poorly tolerated), Rifampicin (poorly tolerated) Ethionamide is contra indicationEthionamide is contra indication Streptomycin is best avoidedStreptomycin is best avoided
Treatment in renal diseaseTreatment in renal disease Rifampicin (normal dose)Rifampicin (normal dose) Other drugs (reduced dose)Other drugs (reduced dose) Pyrazinamide – precipitate gout Pyrazinamide – precipitate gout Streptomycin – if essentialStreptomycin – if essential Ethambutol is best avoided in renal failure (GFR 50 Ethambutol is best avoided in renal failure (GFR 50
ml/min or 3 L/h)ml/min or 3 L/h)

SPECIFIC CONDITIONSPECIFIC CONDITION Treatment in liver diseaseTreatment in liver disease
INH, rifampicin, ethionamide and pyrazinamide can INH, rifampicin, ethionamide and pyrazinamide can all be hapatotoxicall be hapatotoxic
Ethambutol, Streptomycin, INH Ethambutol, Streptomycin, INH Regular liver function monitoringRegular liver function monitoring
Treatment in childrenTreatment in children Standard initial regimen Standard initial regimen INH, rifampicin and pyrazinamideINH, rifampicin and pyrazinamide if 2 drugs regimen if 2 drugs regimen (INH and rifampicin) (INH and rifampicin) : 9 months: 9 months Ethambutol is best avoidedEthambutol is best avoided

RefferencesRefferences
Avery’s Drug Treatment 4Avery’s Drug Treatment 4thth edition edition (Trevor & Nicholas) : 1047 – 1054(Trevor & Nicholas) : 1047 – 1054
Clinical Pharmacology, Basic Principles Clinical Pharmacology, Basic Principles in Therapeutics (Melmon and Morelli’s) : in Therapeutics (Melmon and Morelli’s) : 711 – 712 711 – 712

SubhaanakallohummaSubhaanakallohummawabihamdikawabihamdikaasyhadu anlaa illaaha illa antaasyhadu anlaa illaaha illa antaastaghfiruka wa atuubu ilaikaastaghfiruka wa atuubu ilaika
Do’a penutup majelis