adverse reactions to antituberculosis agents
Upload: chulalongkorn-allergy-and-clinical-immunology-research-group
Post on 13-Dec-2014
4.076 views
DESCRIPTION
Adverse reactions to antituberculosis agentsTRANSCRIPT

Boonthorn14 Aug 2009

OutlineDefinitionEpidemiologyPrincipal of drug metabolismImmune system of the liverPathogenesisDiagnostic approachIn vitro testIn vivo test

Definition of drug allergic liver injuryDILI devided into :
Predictable (type A reaction ) or dose-dependent Effect of the reactive metabolites ( free radicals or reactive oxygen )
after phase I biotransformation
Unpredictable or idiosyncratic (type B reaction ) Immune idiosyncrasy (shortened delay on rechallenge )
eg. halothane Metabolic idiosyncrasy ( no decrease in delay on rechallenge)
eg. isoniazidType C reaction (chronic dose-time dependent exposure)Type D ( delayed ) reactionType E (withdrawal ) reaction Drug hypersensitivity. KARGER

DILI based on liver test abnormalitiesLiver injury deined by increase >2 times of ULN of ALT or
conjugated bilirubin or combined increase of AST,AP and total bilirubin
Acute hepatocellular injury (ALT>ULN or ALT/AP>5) Most common
Acute cholestatic liver injury (AP>2 times or ALT/AP<2)Acute cholestatic hepatitis (second most common ) resemble acute
biliary obstructionPure cholestasis : pruritis ,jaundiceMixed hepatocellular and cholestasis ( ALT/AP 2-5 )
frequently associated with immunoallergic manifestation
Drug hypersensitivity. KARGER

Epidemiology
Tubercle and Lung Disease

Tubercle and Lung Disease

Most common in first 9 weeks
Largely due to PZAMajority within 4 weeks
Tubercle and Lung Disease

MJAFI 2006; 62 : 45-49chronic HBV infection on ATT (9/24, 37.5%) patients given ATT who had no evidence of HBV infection (13/128,10.2%)
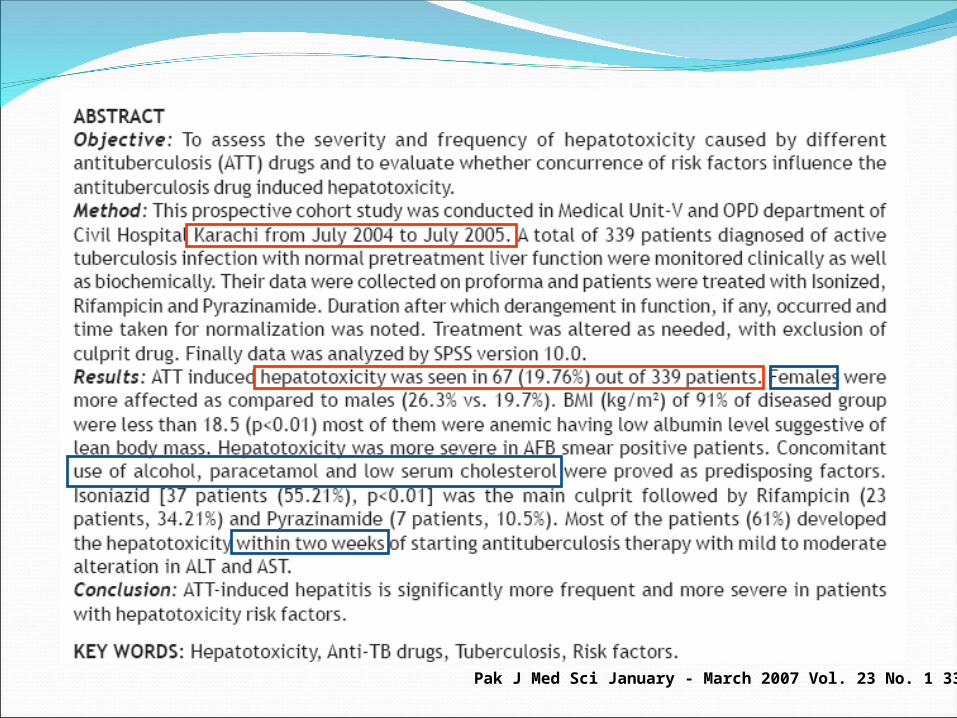
Pak J Med Sci January - March 2007 Vol. 23 No. 1 33-38
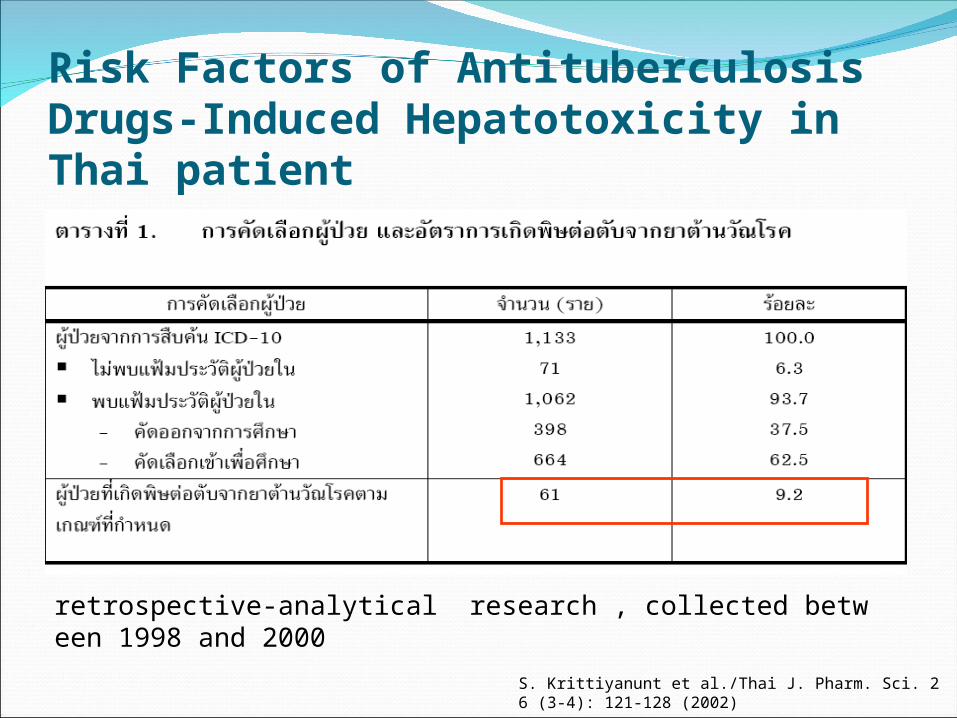
Risk Factors of Antituberculosis Drugs-Induced Hepatotoxicity in Thai patient
S. Krittiyanunt et al./Thai J. Pharm. Sci. 26 (3-4): 121-128 (2002)
retrospective-analytical research , collected between 1998 and 2000

S. Krittiyanunt et al./Thai J. Pharm. Sci. 26 (3-4): 121-128 (2002)
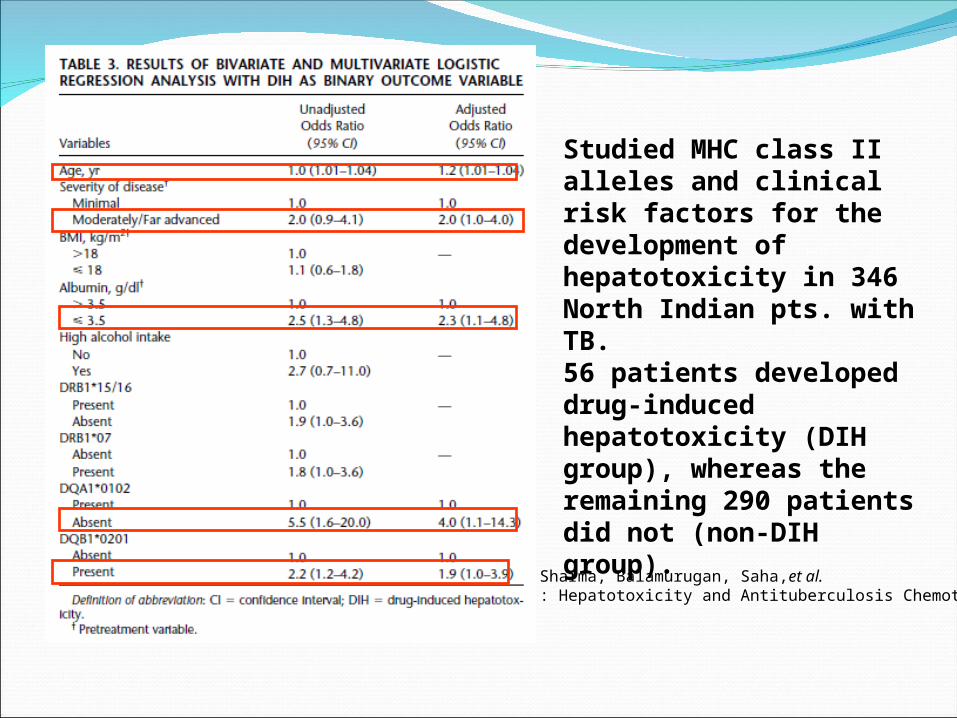
Studied MHC class II alleles and clinical risk factors for the development of hepatotoxicity in 346 North Indian pts. with TB. 56 patients developed drug-induced hepatotoxicity (DIHgroup), whereas the remaining 290 patients did not (non-DIHgroup).
Sharma, Balamurugan, Saha,et al.: Hepatotoxicity and Antituberculosis Chemotherapy

Breen, Miller, Gorsuch, et al
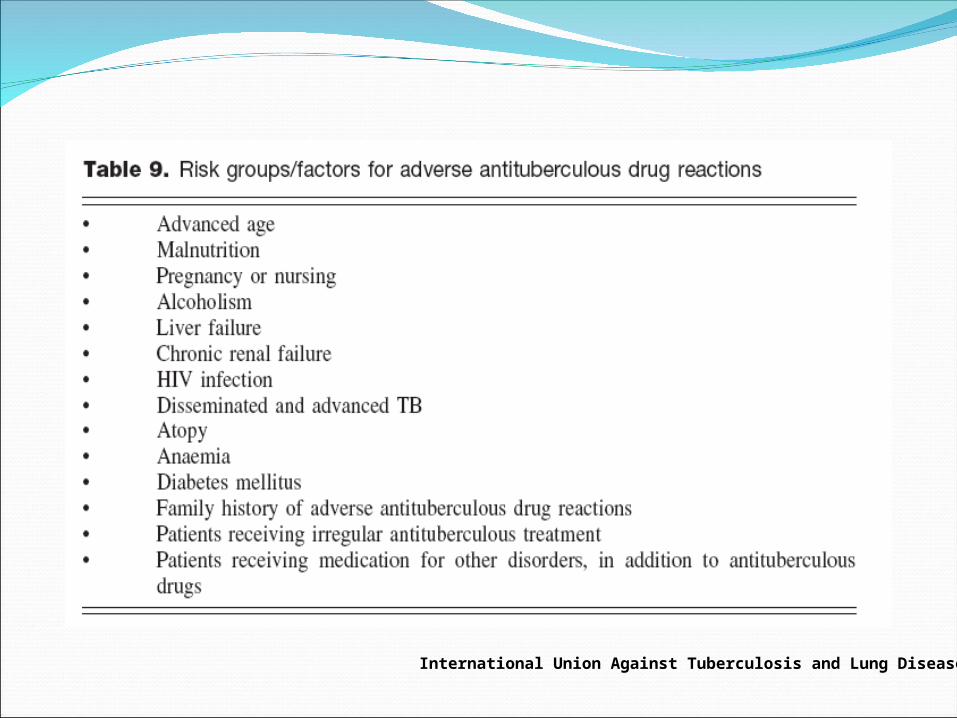
International Union Against Tuberculosis and Lung Disease 2003
1. Ageing. changes in drug metabolism and excretion2. Malnutrition. reduction in hepatocyte glutathione. little
neutralisation of the toxic metabolites originating from drug acetylation.hypoalbuminaemia , causes increase in the plasma free fraction of drugs, thus increasing the risk of drug-induced toxicity.
3. Pregnancy. fatty liver with hypoalbuminaemia 4. Liver or kidney dysfunction. Anti-TB drugs can cause
liver or kidney toxicity; consequently, special caution should be exercised when administering such substances to patients with impaired function of these organs
International Union Against Tuberculosis and Lung Disease 2003

.5. Treatment with other drugs. cytochrome P450 has been frequentlyassociated with production of hepatotoxic reactive metabolites6. Disseminated or advanced TB. consequence of malnutrition or liver deterioration attributable to the disease itself.7. Patients previously subjected to antituberculous therapy. increased risk of damage attributable to rifampicin, which in turn is associated with hypersensitivity reactions that lead to the release of immune complexes.8. Atopy. linked to the existence of other cases of adverseanti-TB drug reactions in family members; thus, the clinical history ofthe patient should be carefully evaluated before treatment is started.9. Sex. Women are at a comparatively greater risk of developing druginducedliver reactions. 10. HIV infection. risk of such reactions increases with the degree of hostimmunosuppression.
International Union Against Tuberculosis and Lung Disease 2003

Principle of drug metabolism
HEPATOLOGY, Vol. 37, No. 4, 2003 Journal compilation © 2006 Asian Pacific Society of Respirology

Drug-Induced Direct Hepatotoxicitydirect action of drug, or reactive metabolite of a
drug, against hepatocytes.Classically used to examine acetaminophenproduce centrilobular hepatic necrosis, which may
lead to acute liver failuremetabolite, N-acetylp-benzoquinoneimine (NAPQI)depletes glutathione and initiates covalent binding
to cellular proteinslead to the disruption of calcium homeostasis,
mitochondrial dysfunction, and oxidative stress and may eventually culminate in cellular damage and death.
The AAPS Journal 2006; 8 (1) Article 6

Immune system of liverKC play essential role in
phagocytosis and removal of pathogens produce cytokines and other mediators, including
prostanoids, nitric oxide, and reactive oxygen intermediatespromoting and regulating hepatic inflammationmodulating the phenotype of other cells in the liver eg. NK
and NKT cellsmajor population of antigen-presenting cells (APCs) within
the liverbalance between induction of immunity and tolerance
within the liverThe AAPS Journal 2006; 8 (1) Article 6
Immune system of liverNK and NKT cells
~50% of intrahepatic leukocytes.act as a fi rst line of defense against
pathogens and invading tumor cells Cytotoxic capacity against other cellsEnhanced by IL-12 and IL-18, produced by
activated KC.produce high levels of T helper (Th) 1 and Th2
cytokines upon stimulation (IFN- γ or IL-4 )The AAPS Journal 2006; 8 (1) Article 6

Immune system of liverAdaptive immune responses favor induction of immunological
tolerance rather than immunity. supported by (1) dietary antigens derived from the GI tract are tolerized in liver
(2) allogeneic liver organ transplants are accepted across MHC barriers
(3) preexposure to donor cells through the portal vein of recipient animals increased their acceptance of solid tissue allografts
(4) preexposure of soluble antigens via the portal vein leads to systemic immune tolerance
The AAPS Journal 2006; 8 (1) Article 6

Mechanisms for liver-induced toleranceapoptosis of activated T cells
elephant ’ s graveyard ” for activated T cells. Studies using T-cell receptor transgenic models have demonstrated that following antigen exposure, activated T cells undergo apoptosis after transient accumulation within the liver
immune deviation Th2 cytokine production is preferentially maintained LSEC are capable of selectively suppressing IFN- γ -
producing Th1 cells while promoting outgrowth of IL-4-expressing Th2 cells
active suppression of T cell activation Naïve T cells,normally encounter APCs in lymphoid tissues, could be
primed directly by LSEC and/or KC within the liverLSEC are presenting antigen to T cells, LSEC-activate d CD4 + or CD8
+ T cells fail to differentiate into Th1 cells or cytotoxic effector cellsThe AAPS Journal 2006; 8 (1) Article 6

Role of Innate Immunity in DILIIn acetaminophen overdose
NAPQI-induced hepatocyte damage lead to activation of innate immune cells stimulating hepatic infiltration of inflammatory cells.produce inflammatory
mediators, cytokines, chemokines, and ROSand RNS nitrogen species ,IFN-γ , Fas, or Fas ligand,causing liver damage
represent major source of hepatoprotective factors,in transgenic mice deficient in IL-10,IL-6, or COX-2 are more susceptible to liver injury
Depletion of NK and NKT cells protected mice from liver injury KC activation release TNF- α , IL-12 and IL-18 (activate
NK,NKT CELL) , IL-10 and IL-6 (protective role) Role of these cell remains controversial
The AAPS Journal 2006; 8 (1) Article 6

Mechanisms of Drug-Induced Liver Injury
The AAPS Journal 2006; 8 (1) Article 6

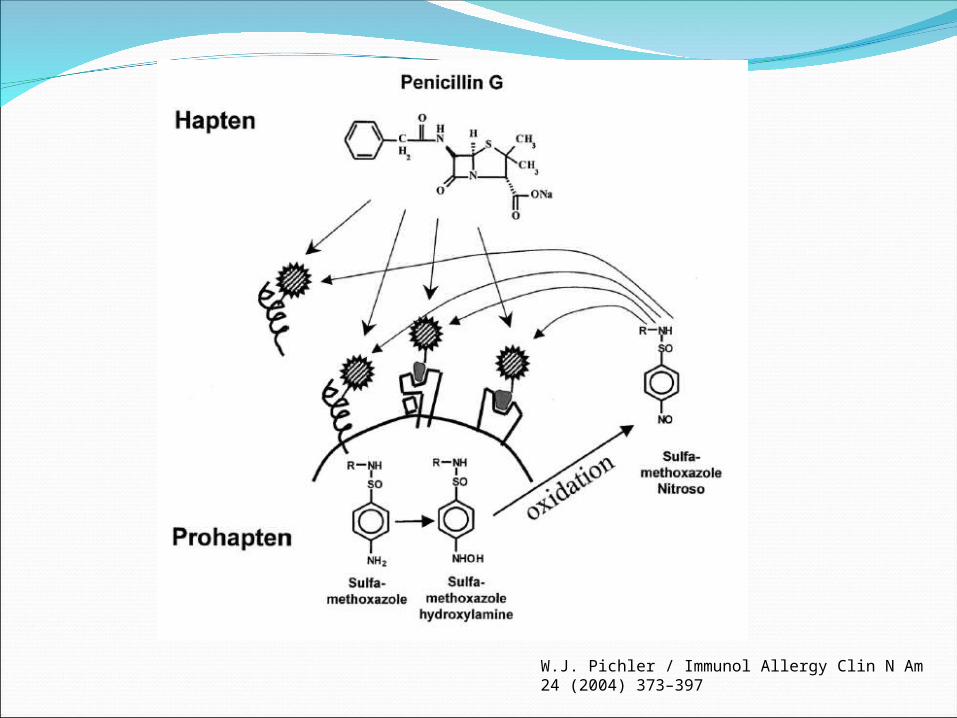
Role of Adaptive Immune Response in DILIhapten hypothesis
drugs, or metabolites , act as haptens and covalently bind to endogenous proteins to form immunogenic drug-protein adducts. elicit either antibody or cytotoxic T-cell responses
p-i conceptdrugs can bind to T-cell receptors, mimicking a
ligand and its receptor interaction, and cause T-cell activation in an MHC-dependent fashion
difficult to directly prove the pathogenic role of the adaptive immune system in DILI, because of the lack of animal models
W.J. Pichler / Immunol Allergy Clin N Am 24 (2004) 373–397

W.J. Pichler / Immunol Allergy Clin N Am 24 (2004) 373–397
p-i concept

DANGER HYPOTHESISimmune system does not directly differentiate
self and non-self, and it only responds to a foreign antigen if the antigen is associated with a danger signal
“immune system is more concerned with damage than with foreignness, and is called into action by alarm signals from injured tissues, rather than by the recognition of non-self”
driving force of the immune system is need to detect and protect against danger. Intracellular stress and cell death caused by a reactive metabolite are likely to be danger signals in DILI
Liver Immunology:Principles and Practice

Liver Immunology:Principles and Practice
model of the immune mechanisms of idiosyncraticDILI

Diagnosis:a practical approachDiagnosis:a practical approachStep 1:exclusion of other cause of liver injury
Serologies for viral and autoimmune hepatitisAbdominal ultrasonographyConfounders eg.hypotension,sepsis,heart failure,use of TPNConcomitant disease (affect outcome negatively )
eg.HIV,alcoholism,DM,obesityStep 2:identification of clinical signature
Clin Liver Dis 10 (2006) 207–217

Step 2:identification of clinical signaturePattern of liver test abnormality
hepatocellular jaundice : worst prognosis, >10% chanceof progressing to acute liver failure ,may result in liver transplantation or deathcholestatic pattern may present resembling acute biliary obstruction or chronically with jaundice or pruritus. usually resolve slowly after drug withdrawal
Clin Liver Dis 10 (2006) 207–217

Clin Liver Dis 10 (2006) 207–217

Latency periodshort (hours to days) : acetaminophenintermediate or delayed (1–8 wks):
sulindac,phenytoinlong (1–12 months): isoniazid , troglitazoneSome antibiotics (eg, amoxicillin/clavulanate,
erythromycin, and trovafloxacin) : symptoms and jaundice 3 to 4 weeks after cessation of therapy.
Clin Liver Dis 10 (2006) 207–217

Feature of immune hypersensitivityfevers, skin rash, and peripheral eosinophilia SJS and TENHematologic abn. Eg. granulocytopenia,
thrombocytopenia,or hemolytic anemia
Clin Liver Dis 10 (2006) 207–217

Course after drug withdrawal (dechallenge) cholestatic reactions tend to subside more slowl
y than hepatocellular reactions liver test abnormalities sometimes lasting for m
ore than a year Overall, in the nonfulminant situation, improve
ment after cessation can be viewed as consisten t with DILI.
Clin Liver Dis 10 (2006) 207–217

Recommendations for the use of ATT in cirrhosis
Meta analysis Incidence of clinical hepatitis : INH (0.6%),INH wihtout R (1.6%),rifam without INH (1.1%),INH with rifam (2.5%)British study :INH (0.3%),Rifam (1.4%),PZA (1.25%)Hepatitis per mo. :PZA>Rifam (3 times),>INH (5 times)
A meta-analysis. Chest 1991;99:465–71.Thorax 1994;45:403–8.

Role of liver test monitoring
Monitoring of ATT therapy (either isoniazid alone in patients older than 35 years or any regimen containing either isoniazid or pyrazinamide)
Role of steroids in the treatment of drug-induced liver injuryinsufficient data to support or refute use of steroids individu
ally for each casesevere hepatitis (jaundice and coagulopathy) do not improve
rapidly within 3 - 4 days after cessation of drug, and if concomitant features support allergy (rash, eosinophilia), trial of steroids (prednisone,40–60 mg) for 1 week followed by a rapid taper
Clin Liver Dis 10 (2006) 207–217

Lymphocytic Transformation test

DETECTION OF HYPERSENSITIVITY TO DRUGS BYLYMPHOCYTE CULTURES IN DRUG-INDUCEDALLERGIC HEPATITIS
antituberculosis drugs (streptomycin: 7,INH: 5, PAS: 3, ethionamide :2, rifampicin: 1)Positive responses : 15 cases ( MI test ) and 49 cases ( lymphocyte transformation ) Clinical symptoms : cutaneous eruption (60%), fever (69%) itching
(73%),eosinophilia (50%) were seen in more than half of the patients.
Gastroenterologia JaponicaVol. 10, No. 4.--1975--

Gastroenterologia JaponicaVol. 10, No. 4.--1975--

Lymphocyte transformation studies in drug hypersensitivity
CMA JOURNAL/MAY 5, 1979/VOL. 120
8 pts. with INH-induced hepatitis, liver biopsy (negative for HBsAg )and rapid resolution of jaundice,abnormal LFT upon withdrawal of the drug3 patients with MP rashes following INH therapy were assessed by LTT with INH. Substantial lymphocyte stimulation was demonstrated for 9/11 patients19 control subjects - 8 pts(INH without adverse effects ), 6 healthy individuals
and 5 patients who had recently discontinued isoniazid.

Diagnostic value of specific T cell reactivity todrugs in 95 cases of drug induced liver injury
Gut 1997; 41: 534–540

Gut 1997; 41: 534–540
25(26%) 53(56%)
clinical markers (rash,arthralgia,eosinophilia) absent about 70% pts. with demonstrable T cell
reactivity to drugs challenges

Drug lymphocyte stimulation test in diagnosis of adverse reactions to anti-tuberculosis drugsprospective study436 pts. with TB were admitted for treatment between January
2002 and August 2007DLST ,DPTtested drugs : INH, RIF,EMB,PZA69 (15.8%) had adverse drug reactions to anti-TB drugssensitivity of DLST was 14.9% for all drugs (INH: 14.3%,
RIF: 13.6%, EMB: 14.3%, PZA: 0%).DLST offers little contribution to the detection of causative
agents in patients with adverse anti-TB drug reactions
Suzuki Y., et al . Chest.

Lymphocyte transformation test for evaluation of adverse effects of anti TB drug15 pts. With INH and RIFControl 21pts. ( 7 exposed,14 never been exposed anti TB )4/15 of hepatotoxic only positive with RIF , 3/15 with INH8/15 negativeIn healthy control with previous contact :INH positive 2 , INH
+RIF 1Control without former contact : negativeLTT can be useful for identifying the drug responsible for
immunological side effects
Eur med res.1999 Feb 25 ;4(2) 67-71

Patch test

Hypersensitivity syndrome from isonizid34 yrs. Old woman with pulmonary TB Rx with INH,
RIF,PZA ,after 2 mo. Developed severe pruritic urticariform cutaneous eruption
PZA discontinued because RX completed1 wk later worsening
eruption,fever,icterus ,lymphadenopathy,hepatomegaly .eosinophilia (8%)ALT 1459,ANA neg,high LDH=> second line
1yr later LTT to INH,RIF,PZA negEpicutaneous test with 1%RIF in vaseline (neg),10%PZA in
alc.(neg),1% INH in NSS (strongly pos after 48,96hrs.) , 10 controls (neg)
Allergy S4 ,1999/1004-1013

Hypersensitivity syndrome from INH with positive patch test 68 yrs. Man in 1995 Dx :TB ,Rx:INH,RIF,PZA2 yrs. Later ,recurrent TB Rx:INH,RIF,EMB1 mo. Later develop fever, asthenia,facial
edema,pancytopenia,increase liver enz.=>stop anti TB10 d later he was asymptomaticPatch test with RIF,EMB,INH (50%pet)Positive(+++D2) only to INH ,10 healthy control (neg)DPT with RIF ,EMB were negative
Contact dermatitis. 2001,45,306
Delayed type hypersensitivity reaction to EMB and INH24 yrs, woman started with INH,RIF,EMB2 wks. Later itchy,desquamative,erythrematous,papular
rash5 d after drug withdrawal =>progressRx:topical fluticasone,oral cetrizine => improvedAfter subsided ,patch test were perform with
INH,RIF,EMB (crutch and moistened with water)Positive with EMB,INH at D310 healthy control were negative at D2,3
Contact dermatitis 2002:46:359

Rifampicin allergy confirmed by ID test,but with negative patch test45 yrs. Woman with peritoneal TBStart with INH,RIF,EMB,PZA 7.5 wks. Develop MP rash ,fever, chill , joint
pain=>stop drug => improvedPatch test with INH,RIF,EMB,PZA (30%pet)were
negSkin prick test with 1% INH and RIF,30% EMB
and PZA were negIDT 0.1% RIF 10mm.Reinstated with INH,EMB,PZA,strep=> no
eruption Contac dermatitis,2001.45.108

DRESS induced by ATT29 yrs. Female on celecoxib and
antituberculosis drug1 mo. Developed DRESSPatch test were positive for celecoxib and
EMB
J Korean Med Sci 2008; 23: 521-5

ConclusionDILI : type A or B , hepatocellular or
cholestatic Risk factor of ATT: age ,
sex ,malnutrition ,liver and kidney dysfunction , concomitant with HBV and HIV
Drug metabolism in liverTolerance VS immunityHapten, p-i concept , danger hypothesisDiagnostic approachInvtro and in vivo test