advancing the standard of care · advancing the standard of care: ... not as a substitute for...
TRANSCRIPT

Produced by
IN THIS ISSUE
ADVANCING THE STANDARD OF CARE:
Cardiovascular and Neurovascular Emergencies
ADVANCING THE STANDARD OF CARE:
Cardiovascular and Neurovascular Emergencies
EMCREG MonographFrom the ACEP 2006Sci nt fic s m lSatellite SymposiumOct ber 16 1 , 20 6
New Orleans, LA
EMCREG MonographFrom the ACEP 2006Scientific AssemblySatellite SymposiumOctober 16 & 17, 2006
New Orleans, LA

I n t e rna t i ona l
ADVANCING THESTANDARD OF CARE:
Cardiovascular andNeurovascular Emergencies
EMCREG MonographFrom the ACEP 2006Scientific AssemblySatellite Symposium
October 16 & 17, 2006New Orleans, LA
Edited by:W. Brian Gibler, MD
Professor & ChairmanDepartment of Emergency Medicine
University of CincinnatiCincinnati, OH, USA
President, EMCREG-International
Andra L. Blomkalns, MDAssistant Professor, Residency Program, Director
Vice Chairman-EducationDepartment of Emergency Medicine
University of CincinnatiCincinnati, OH, USA
Director, CME and Enduring MaterialsEMCREG-International
w w w . e m c r e g . o r g
Produced by EMCREG-International
[Emergency Medicine Cardiac Research and Education Group]

w w w . e m c r e g . o r gi
Andra L. Blomkalns, MDAssistant Professor, Residency Program, DirectorDepartment of Emergency MedicineUniversity of CincinnatiCincinnati, OHDirector, CME and Enduring MaterialsEMCREG-International
W. Brian Gibler, MDProfessor and ChairmanDepartment of Emergency MedicineUniversity of CincinnatiCincinnati, OHPresident, EMCREG-InternationalEMCREG-International
www.emcreg.org
December 2006
Dear Colleagues:
The Emergency Medicine Cardiac Research and Education Group (EMCREG) – International is pleased to present this monograph serving as the proceedings of our satellite symposium at the ACEP Scientific Assembly in New Orleans, Louisiana. Our symposia, now celebrating its 10th anniversary, took place on October 16 and 17, 2006. The faculty that presented at our symposia have prepared these pieces which cover topics of significant interest to clinicians caring for patients presenting emergently with cardiovascular or neurovascular diseases. This material can also be located at our www.emcreg.org web site in both downloadable hardcopy and web cast formats. All content is solely the work of the contributing author.
A number of important topics are covered in this monograph including management of non-ST-segment elevation and ST-segment elevation acute coronary syndrome (ACS), the CRUSADE Quality Improvement Initiative, decreasing time to treatment for ST-segment elevation myocardial infarction, direct thrombin inhibitors in ACS, acute decompensated heart failure care, the use of lactate as a marker for trauma and sepsis, point-of-care testing for cardiac biomarkers, the management of hypertension in acute neurovascular emergencies and advances in acute stroke care. For those interested in obtaining category 1 CME credit for reading this monograph, CME questions are available at the end of the document. We sincerely hope that you find this monograph interesting to read and its material helpful for your excellent care of patients with cardiovascular or neurovascular emergencies. We greatly appreciate your interest in EMCREG-International and your confidence in our symposia and enduring material pieces as a source of your continuing medical education.
EMCREG Educational MissionThe mission of EMCREG-International is to provide up-to-date, evidence based, and clinically useful educational materials to healthcare providers involved in the care of emergency conditions. We take great pride and effort to provide these materials free of commercial bias. While these educational endeavors are sponsored in part by industry, speaker or contributor influence or bias is carefully reviewed and strictly prohibited. Comments regarding any of our educational materials can be referred directly to Andra L. Blomkalns, MD, Director of CME and Enduring Materials at [email protected].
Sincerely,
Accreditation: The University of Cincinnati College of Medicine designates this educational activity for a maximum of 4 hours of Category 1 credit towards the AMA Physician’s Recognition Award. Each physician should claim only those hours that he/she actually spent on the educational activity. The University of Cincinnati is accredited by the Accreditation Council for Continuing Medical Education (ACCME) to support continuing medical education for physicians.
This educational monograph was supported in part by unrestricted educational grants from Abbott POC/i-STAT, Biosite, Bristol-Myers Squibb, PDL BioPharma, Sanofi-Aventis, Schering Plough, Scios, and The Medicines Company.
This document is to be used as a summary and clinical reference tool and NOT as a substitute for reading the valuable and original source documents. EMCREG will not be liable to you or anyone else for any decision made or action taken (or not taken) by you in reliance on these materials. This document does not replace individual physician clinical judgment.
Clinical judgment must guide each professional in weighing the benefits of treatment against the risk of toxicity. Doses, indications and methods of use for products referred to in this program are not necessarily the same as indicated in the package insert and may be derived from the professional literature or other clinical courses. Consult complete prescribing information before administering.
I n t e rna t i ona l

w w w . e m c r e g . o r gii
w w w . e m c r e g . o r gii
Contributing Authors
EMCREG MembersW. Brian Gibler, MD, PresidentUniversity of CincinnatiCincinnati, Ohio
V. Anantharaman, MDSingapore General HospitalSingapore
Tom P. Aufderheide, MDMedical College of WisconsinMilwaukee, Wisconsin
Roberto Bassan, MDPro-Cardiaco HospitalRio de Janeiro, Brazil
Andra L. Blomkalns, MDUniversity of CincinnatiCincinnati, Ohio
Gerald X. Brogan, MDNorth Shore University HospitalPlainview, New York
David F. M. Brown, MDMassachusetts General HospitalBoston, Massachusetts
Charles B. Cairns, MDDuke Clinical Research InstituteDurham, North Carolina
Douglas M. Char, MDWashington University School of MedicineSt. Louis, Missouri
Sean P. Collins, MDUniversity of CincinnatiCincinnati, Ohio
Herman H. Delooz, MDUniversity Hospital GasthuisbergLeuven, Belgium
Deborah S. Diercks, MDU.C. Davis Medical CenterSacramento, California
Gregory J. Fermann, MDUniversity of CincinnatiCincinnati, Ohio
Francis M. Fesmire, MDErlanger Medical CenterChattanooga, Tennessee
J. Lee Garvey, MDCarolinas Medical CenterCharlotte, North Carolina
Gary B. Green, MDJohns Hopkins Medical InstitutionsBaltimore, Maryland
Jin H. Han, MDVanderbilt University Medical CenterNashville, Tennessee
James W. Hoekstra, MDWake Forest UniversityWinston Salem, North Carolina
Judd E. Hollander, MDUniversity of PennsylvaniaPhiladelphia, Pennsylvania
Brian R. Holroyd, MDUniversity of Alberta HospitalsEdmonton, Alberta, Canada
Shingo Hori, MDKeio UniversityTokyo, Japan
Edward C. Jauch, MDUniversity of CincinnatiCincinnati, Ohio
Raymond E. Jackson, MDWilliam Beaumont HospitalRoyal Oak, Michigan
J. Douglas Kirk, MDU.C. Davis Medical CenterSacramento, California
Christopher J. Lindsell, PhDUniversity of CincinnatiCincinnati, Ohio
Chadwick V. Miller, MDWake Forest UniversityWinston Salem, North Carolina
Richard M. Nowak, MDHenry Ford HospitalDetroit, Michigan
Masatoshi Oba, MDFurukawa City HospitalJapan
Brian J. O’Neil, MDWilliam Beaumont HospitalRoyal Oak, Michigan
Joseph P. Ornato, MDMedical College of VirginiaRichmond, Virginia
Arthur M. Pancioli, MDUniversity of CincinnatiCincinnati, Ohio
W. Frank Peacock, MDThe Cleveland Clinic Cleveland, Ohio
Charles V. Pollack, MDUniversity of Pennsylvania HospitalPhiladelphia, Pennsylvania
Ivan C. Rokos, MDGeffen School of Medicine at UCLALos Angeles, California
Francios P. Sarasin, MDHospital CantonalGeneva, Switzerland
Harry Severance, MDUniversity of South FloridaTampa, Florida
Corey M. Slovis, MDVanderbilt University Medical CenterNashville, Tennessee
Richard L. Summers, MDUniversity of Mississippi Jackson, Mississippi
Brian R. Tiffany, MDMaricopa Medical CenterPhoenix, Arizona
James E. Weber, MDUniversity of MichiganFlint, Michigan
W. Brian Gibler, MDUniversity of CincinnatiCincinnati, Ohio
Andra L. Blomkalns, MDUniversity of CincinnatiCincinnati, Ohio
Robert H. Christenson, PhD, DABCC, FACBUniversity of Maryland Baltimore, Maryland
Deborah S. Diercks, MDU.C. Davis Medical CenterSacramento, California
Dorman Fawley, MHAHealth Alliance of Greater CincinnatiCincinnati, Ohio
James W. Hoekstra, MDWake Forest UniversityWinston Salem, North Carolina
Judd E. Hollander, MDUniversity of PennsylvaniaPhiladelphia, Pennsylvania
J. Douglas Kirk, MDU.C. Davis Medical CenterSacramento, California
E. Magnus Ohman, MD, FRCPI, FACCDuke University Medical CenterDurham, North Carolina
Arthur M. Pancioli, MDUniversity of CincinnatiCincinnati, Ohio
Charles V. Pollack, MDUniversity of Pennsylvania HospitalPhiladelphia, Pennsylvania
Brian A. Stettler, MDUniversity of CincinnatiCincinnati, Ohio

w w w . e m c r e g . o r giii
w w w . e m c r e g . o r giii
Disclosure of Faculty/Industry Relationships
In accordance with ACCME Standards for Commercial Support for Continuing Medical Education and the University of Cincinnati Office of Continuing Medical Education, faculty members have been asked to disclose any relationships they may have with commercial supporters of this CME activity or with companies providing drugs, medical equipment, etc, that may have relevance to the content of their presentations. Such disclosure is intended to provide participants with sufficient information to evaluate whether any given presentation has been influenced by the faculty’s relationship(s) or financial interests with said companies.
The following faculty have reported receiving honoraria and/or research support, either directly or indirectly, from the companies listed below.
Dr. Blomkalns Research and/or grant support: Abbott POC/i-STAT Consultant: PDL Biopharma, Inc. Speakers Bureau: Abbott POC/i-STAT Unrestricted educational grants to EMCREG-International from: Abbott POC/i-STAT; Biosite, Bristol Myers Squibb; Inovise; The Medicines Company;
PDL Biopharma; Sanofi-Aventis; Schering Plough, and Scios.
Dr. Christenson Research and/or grant support: Dade Behring, Biosite, Roche Diagnostics, and Response Biomedical
Advisory Board: Unipath and Response Biomedical Speakers Bureau: Dade Behring and Biosite
Dr. Diercks Advisory Board: Inovise and Astellas. Consultant: Sanofi-Aventis and The Medicines Company Speakers Bureau: Sanofi-Aventis
Mr. Fawley No disclosures
Dr. Gibler Research and/or grant support from Abbott POC/i-STAT. Unrestricted educational grants to EMCREG-International from:
Abbott POC/i-STAT; Biosite, Bristol Myers Squibb; Inovise; The Medicines Company; PDL Biopharma; Sanofi-Aventis; Schering Plough, and Scios.
Dr. Hoekstra Research and/or grant support: Schering-Plough and Biosite. Advisory Board: Sanofi-Aventis, Schering-Plough, and The Medicines Company Speakers Bureau: Sanofi-Aventis, Schering-Plough, and Bristol-Myers Squibb
Dr. Hollander Research and/or grant support: The Medicines Company and Glaxo Smith Kline Advisory Board: Schering-Plough, The Medicines Company Speakers Bureau: Sanofi-Aventis, Genentech and The Medicines Company
w w w . e m c r e g . o r giv
w w w . e m c r e g . o r giv
Dr. Kirk Research and/or grant support: PDL BioPharma, Sanofi-Aventis, Scios, Accumetrics, and Inovise
Consultant: Sanofi-Aventis, Schering-Plough, Biosite, PDL BioPharma, Scios, Accumetrics, and Inovise
Advisory Board: Sanofi-Aventis, Schering-Plough, PDL BioPharma, and Scios Speakers Bureau: Sanofi-Aventis, Schering-Plough, Scios and Biosite
Dr. Ohman Research and/or grant support: Bristol-Myers Squibb, Sanofi-Aventis, Schering-Plough, Millennium Pharmaceutical, and Eli Lilly
Dr. Pancioli Research and/or grant support: NIH funding from NINDS, PDL Bio Pharma Advisory Board: Astra Zeneca
Dr. Pollack Research and/or grant support: Glaxo Smith Kline Consultant: Sanofi-Aventis, and The Medicines Company Advisory Board: Sanofi-Aventis Speakers Bureau: Sanofi-Aventis
Dr. Stettler No relationships
Disclosure of Discussions off Off-Label and/or Investigational Uses of Drugs
Disclaimer: The opinions expressed during this educational activity are those of the faculty and do not necessarily represent the views of the University of Cincinnati College of Medicine or EMCREG - International. Participants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. Off-label Disclosure: Faculty members are required to inform the audience when they are discussing off-label, unapproved uses of devises and drugs. Physicians should consult full prescribing information before using any product mentioned in this program.
This educational monograph was supported in part by unrestricted educational grants from Abbott POC/i-STAT, Biosite, Bristol-Myers Squibb, PDL BioPharma, Sanofi-Aventis, Schering Plough, Scios, and The Medicines Company.
Copyright EMCREG-International, 2007w w w . e m c r e g . o r g
I n t e rna t i o na l

w w w . e m c r e g . o r gv
w w w . e m c r e g . o r gv
Table of ContentsManagement of non-ST-segment Elevation Acute Coronary Syndrome (NSTE-ACS) in the ED: State-of-the-Art Anti-platelet Management .............................1James W. Hoekstra, MD - Professor and Frederick Glass Chairman, Department of Emergency Medicine, Wake Forest University, Winston Salem, NC
Non-ST-segment Elevation Acute Coronary Syndrome: Optimal Anti-Coagulant Therapy for the Emergency Department ................................................................5Charles V. Pollack, Jr., MA, MD, FACEP - Chairman, Emergency Medicine, Pennsylvania Hospital, Professor of Emergency Medicine, University of Pennsylvania School of Medicine, Philadelphia, PA
CRUSADE Quality Improvement Initiative: Better Care for Patients with Unstable Angina and non-ST-segment Elevation Myocardial Infarction .......................11Deborah B. Diercks, MD - Associate Professor, Department of Emergency Medicine, University ofCalifornia, Davis, Medical Center, Sacramento, CA
ST-segment Elevation Myocardial Infarction (STEMI): Decreasing the Time to Treatment in the ED .......................................................17W. Brian Gibler, MD - Professor and Chairman; Department of Emergency Medicine, University of Cincinnati College of Medicine, Cincinnati, OH, President, EMCREG-International
Novel Anti-thrombotic Therapies for Acute Coronary Syndrome: Direct Thrombin Inhibitors ................................................................................23Judd E. Hollander, MD - Professor, Clinical Research Director, Department of Emergency Medicine,University of Pennsylvania School of Medicine, Philadelphia, PA
Management of ST-segment Elevation Myocardial Infarction in the ED: State-of-the-Art Anti-platelet and Anti-thrombotic Therapy ......................................28James W. Hoekstra, MD - Professor and Frederick Glass Chairman, Department of Emergency Medicine, Wake Forest University, Winston Salem, NC
Acute Decompensated Heart Failure: Novel Approaches to Classification and Treatment ...............................................33J. Douglas Kirk, MD - Associate Professor of Emergency Medicine and Vice Chair of Clinical Operations, Department of Emergency Medicine, University of California, Davis, Medical Center, Sacramento, CA
Lactate – A Marker for Sepsis and Trauma ..........................................................43Andra L. Blomkalns, MD - Assistant Professor; Vice Chairman-Education; Residency Program, Director, Department of Emergency Medicine, University of Cincinnati College of Medicine, Cincinnati, OH, Director of CME and Enduring Materials, EMCREG-International
Point-of-Care Testing for Cardiac Biomarkers in the ED: A Blueprint for Implementation ..........................................................................50W. Brian Gibler, MD - Professor and Chairman; Department of Emergency Medicine, University of Cincinnati College of Medicine, Cincinnati, OH, President, EMCREG-International
Hypertension Management in Acute Neurovascular Emergencies ...........................61Arthur M. Pancioli, MD - Vice Chairman of Research, Associate Professor, Department of Emergency Medicine, University of Cincinnati College of Medicine, Cincinnati, OH, Member, Greater Cincinnati/Northern Kentucky Stroke Team
Advances in Acute Stroke Care .........................................................................71Brian A. Stettler, MD - Assistant Professor, Department of Emergency Medicine, University of Cincinnati College of Medicine, Cincinnati, OH, Member, Greater Cincinnati/Northern Kentucky Stroke Team
Continuing Medical Education Questions ..............................................................80

1w w w . e m c r e g . o r g
MANAGEMENT OF NON-ST-SEGMENT ELEVATION ACUTE CORONARY SYNDROME (NSTE-ACS) IN THE ED: STATE-OF-THE-ART ANTI-PLATELET MANAGEMENT
Specifically, new clinical
trials data support the
use of higher doses of
clopidogrel and earlier
administration of GP
IIb/IIIa inhibitor therapy
in the management of
NSTE ACS.
MANAGEMENT OF NON-ST-SEGMENT ELEVATION ACUTE CORONARY SYNDROME (NSTE-ACS) IN THE ED: STATE-OF-THE-ART ANTI-PLATELET MANAGEMENT
James W. Hoekstra, MDProfessor and Frederick Glass Chairman, Department of Emergency Medicine
Wake Forest University, Winston Salem, NC
OBJECTIVES:1) Describe the ACC/AHA guidelines for the treatment of high risk non-ST-segment elevation
acute coronary syndromes.2) Describe the clinical trial evidence and rationale for the use of aspirin, clopidogrel, and GP
IIb/IIIa inhibitors in the treatment of high risk NSTE ACS.3) Describe the clinical trial data supporting the use of a 600mg loading dose of clopidogrel
in NSTE ACS.4) Review the clinical trial data supporting the early use of GP IIb/IIIa inhibitors upstream,
prior to coronary angiography, in high risk, troponin positive NSTE ACS patients.
INTRODUCTIONAlthough non-ST-segment elevation acute coronary syndromes (NSTE ACS) represent a well-recognized source of morbidity and mortality for patients with cardiovascular disease, evidence-based therapies shown to improve outcomes for NSTE ACS are frequently underutilized in appropriate patients, especially in the ED. The American College of Cardiology/American Heart Association (ACC/AHA) Guidelines for the Management of Unstable Angina/Non-ST-Elevation Myocardial Infarction1,2 were promulgated in an effort to standardize and optimize the evaluation, diagnosis, and management of patients with NSTE ACS and to provide physicians with a framework for clinical decision-making. These guidelines are somewhat outdated, however, having last been published in 2002, and may not reflect recent clinical trial evidence. Specifically, new clinical trials data support the use of higher doses of glycoprotein IIB/IIIA inhibitor (GPI) therapy in the management of NSTE ACS.
Whether or not these new developments will be included in the next rendition of the Guidelines, or into routine clinical care, remains to be seen. The intent of this NSTE ACS manuscript is to critically review some of these recent clinical trials involving the use of anti-platelet agents in NSTE ACS.
Anti-platelet Therapy in NSTE ACS:The pathophysiology of NSTE ACS is initiated by the endothelial rupture of an atherosclerotic coronary artery plaque. Plaque rupture leads to platelet aggregation, platelet activation, fibrin deposition, and downstream myocardial ischemia and necrosis. Therapies aimed at minimizing or reversing platelet and coagulation cascade activation are especially effective in NSTE ACS. Platelet inhibitors, including aspirin, clopidogrel, and GPI therapy have all been investigated in this group of patients with remarkable results.3-9 In high risk patients, the ACC/AHA Guidelines

2w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
2w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
recommend the early use of aspirin (160-325 mg po), clopidogrel (300 mg po), intravenous heparin or low molecular weight heparin (anti-thrombotic agents) and an intravenous GPI, initiated prior to an early percutaneous coronary intervention (PCI) approach (Figure 1).1 High risk patients are typically defined as having old age, ongoing chest pain, hemodynamic or rhythm instability, elevated cardiac biomarkers, or new ischemic electro-cardiographic (ECG) changes.
clopidogrel plus a GPI in low risk elective PCI patients.12 These data have led to the widespread use of a 600 mg loading dose of clopidogrel in the catheterization lab prior to PCI. Upstream use of the 600 mg loading dose in the emergency department (ED) or critical care unit (CCU) is not well defined, although pharmacokinetic and clinical data are very promising. Adaptation of the upstream dosing of clopidogrel in the ED appears to be limited more by the logistic complications of CABG-related bleeding than by issues of dose-response.
Figure 1. Class I recommended anti-platelet and anti-thrombin therapy in NSTE ACS, based on risk stratification to low, intermediate, and high risk for adverse outcomes. Reprinted with permission from Brauwald et al. J Am Coll Cardiol. 2000;36:970-1062.
Clopidogrel Dosing in High Risk NSTE ACS PatientsThe ACC/AHA Guidelines recommend that high risk NSTE ACS patients receive clopidogrel 300 mg po load, and 75 mg per day, in addition to aspirin therapy, beginning at patient presentation and continuing for at least one month, and up to one year post discharge from the hospital. The 300 mg loading dose provides approximately 40-60% platelet inhibition after achievement of steady state levels. Recent pharmacokinetic data have suggested that a 600 mg loading dose of clopidogrel, and 75 mg po bid, is associated with as high as 80% initial platelet inhibition.10 In the recently completed ARMYDA-2 trial, a loading dose of 600 mg of clopidogrel prior to PCI was associated with a 67% reduction (p=0.041) in death, MI, and urgent revascularization compared to the standard 300 mg loading dose (Figure 2).11 In ISAR-REACT-1, the loading dose of 600 mg of clopidogrel was found to be equivalent to
Figure 2. Results of the ARMYDA 2 Trial: Reduction in death, MI and target vessel revascularization with 600 mg clopidogrel loading dose versus the standard 300 mg dose. Reprinted with permission from Patti G, et al. Circulation. 2005;111:2099-2106.
Utilization of GPIs in Addition to Clopidogrel in High Risk NSTE ACSThe rather compelling data supporting the effectiveness of 600 mg loading doses of clopidogrel in PCI evaluate the utility of GPIs in addition to clopidogrel in high-risk NSTE ACS. The recently completed ISAR REACT-2 trial investigated whether a 600 mg loading dose of clopidogrel was as effective as 600 mg of clopidogrel plus the GPI abciximab in high risk patients undergoing PCI.13 The 2,022 high risk NSTE ACS patients in ISAR REACT-2 had either elevated troponin levels or ischemic ECG changes evident prior to PCI. Glycoprotein IIb/IIIa receptor blockers utilization in addition to clopidogrel administration resulted in a statistically significant reduction in death, MI, and urgent revascularization in

3w w w . e m c r e g . o r g
MANAGEMENT OF NON-ST-SEGMENT ELEVATION ACUTE CORONARY SYNDROME (NSTE-ACS) IN THE ED: STATE-OF-THE-ART ANTI-PLATELET MANAGEMENT
3w w w . e m c r e g . o r g
MANAGEMENT OF NON-ST-SEGMENT ELEVATION ACUTE CORONARY SYNDROME (NSTE-ACS) IN THE ED: STATE-OF-THE-ART ANTI-PLATELET MANAGEMENT
high risk patients (p=0.03) when compared to clopidogrel alone. This benefit was most notable in troponin positive patients (p=0.02) (Figure 3) and absent in troponin negative patients (p=0.98). The results of this trial underscore the need for GPIs, as an adjunct to PCI, in NSTE ACS patients who are high risk, and especially those who are troponin positive. Its applicability to ED or CCU GPI therapy upstream is limited, however, by the catheterization laboratory administration of these drugs in the original trial design.
Figure 3. Results of the ISAR REACT-2 trial: Reduction in ischemic outcomes in troponin-positive patients treated with clopidogrel plus GPI versus clopidogrel alone. Reprinted with permission form results presented at the ACC 2006, Kastrati A. et al. (Ref 13).
Figure 4. Benefits in ischemic outcome with GPI therapy before and after PCI: Results of a meta-analysis of GPI trials in NSTE ACS. Adapted with permission from Boersma E, et al. Circulation. 1999;100:2045-2048.
Early GPI Use in High Risk NSTE ACS: The ACUITY Timing Trial:A large body of evidence now supports the substantial clinical benefit of adjunctive platelet GPI utilization with PCI in the setting of NSTE ACS.3-5 A smaller but significant benefit with GP IIb/IIIa inhibitors is also discerned in the time period following initiation of treatment but prior to PCI (Figure 4),14,15 yet controversy still exists as to the benefits of upstream pre-catheterization GPI therapy. The recently completed ACUITY Timing trial attempted to address the effectiveness of early (in the ED or CCU) versus late (catheterization laboratory) initiation of GPI therapy in moderate and high risk NSTE ACS patients.16 Of the 9,207 patients in the ACUITY timing trial, 4,605
patients were treated with ED or CCU GPI versus 4,602 in the cardiac catheterization laboratory. Whereas the quadruple endpoint of death, MI, unplanned intervention, and bleeding was not different between groups, the upstream GPI group tended to have less ischemic events, and in those patients who underwent PCI, this difference was statistically significant (p=0.05) (Figure 5). The results of this trial favored an early GPI treatment strategy,
Figure 5. Results from the ACUITY timing trial: Net clinical outcome, ischemia and bleeding endpoints stratified by patient management strategy. Reprinted with permission form results presented at the ACC 2006, Stone GW. et al. (Ref 16).

4w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
but there were limitations to the trial which temper its conclusions. First, the patients involved in the ACUITY Timing trial were not truly high risk, with only 57% having troponin biomarker positivity, and therefore many may not have even been eligible to receive upstream GPI as indicated in the ACC/AHA guidelines. Second, the time from admission to cardiac catheterization was a median 19.7 hours, while the median early GPI treatment time was only 6.2 hours, limiting the applicability of these results to the ED. Finally, the ischemia benefit of ED or CCU GPI use was offset by an increase in bleeding in the cardiac catheterization laboratory, resulting in no net clinical benefit. Whereas the results of the ACUITY Timing Trial are intriguing, questions remain regarding the effectiveness of upstream GPI utilization. The much anticipated EARLY-ACS trial, which randomizes high risk NSTE ACS patients to ED versus cardiac catheterization laboratory eptifibatide, should provide a definitive answer to this important question.
SUMMARYThe ISAR REACT-2 trial and the ACUITY Timing trial are only two examples of the many recent clinical trials involving the care of patients with NSTE ACS using anti-platelet agents. Like many past studies, these recent trials answer some clinical questions, but raise others at the same time. Their results must be interpreted in regards to current practice, with emphasis on their applicability in the emergency setting. Lessons from these trials may change practice, or provide an improved evidence basis for current ED therapy for NSTE ACS. Emergency physicians should become aware of these trial results and other studies to provide optimal care for high-risk NSTE ACS patients.
REFERENCES1. Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA guidelines for the management
of patients with unstable angina and non-ST-segment elevation myocardial infarction: executive summary and recommendations: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Patients with Unstable Angina). Circulation. 2000;102:1193-1209. 2002 update posted at www.acc.org on March 15, 2002.
2. Pollack CV Jr, Roe MT, Peterson ED. 2002 update to the ACC/AHA guidelines for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction: implications for emergency department practice. Ann Emerg Med. 2003;41:355–369.
3. PURSUIT Trial Investigators. Inhibition of platelet glycoprotein IIb/IIIa with eptifibatide in patients with acute coronary syndromes. Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression Using Integrilin Therapy. N Engl J Med. 1998;339:436–443.
4. The PRISM-PLUS Investigators. Inhibition of the platelet glycoprotein IIb/IIIa receptor with tirofiban in unstable angina and non-Q-wave myocardial infarction. Platelet Receptor Inhibition in Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms. N Engl J Med. 1998;338:1488–1497.
5. Simoons ML; GUSTO IV-ACS Investigators. Effect of glycoprotein IIb/IIIa receptor blocker abciximab on outcome in patients with acute coronary syndromes without early coronary revascularization: the GUSTO IV-ACS randomized trial. Lancet. 2001;357:1915–1924.
6. Anti-platelet Trialists Collaboration: Collaborative overview of randomized trials of anti-platelet therapy. Br Med J 2002;324:71-86.
7. Peters RJG, Mehta SR, Fox KA, et al: Effects of aspirin dose when used alone or in combination with clopidogrel in patients with ACS. Circulation 2003;108:1682-1687.
8. CURE Study Investigators: Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med 2001;345:494-502.
9. Mehta S, Yusuf S, Peters R, et al: Effects of pretreatment with clopidogrel and aspirin followed by long term therapy in patients undergoing percutaneous coronary intervention: The PCI CURE Trial. Lancet 2001;358:527-533.
10. Müller I, Seyfarth M, Rudinger S, et al. Effect of a high loading dose of clopidogrel on platelet function in patients undergoing coronary stent placement. Heart. 2001;85:92-93.
11. Patti G, Colonna G, Pasceri V, et al. Randomized trial of high loading dose of clopidogrel for reduction of periprocedural myocardial infarction in patients undergoing coronary intervention: results from the ARMYDA-2 (Anti-platelet therapy for Reduction of MYocardial Damage during Angioplasty) study. Circulation. 2005;111:2099-2106.
12. Kastrati A, Mihilli J, Schuhen H, et al: The ISAR REACT trial: A clinical trial of abciximab in elective PCI after pretreatment with clopidogrel. N Engl J Med. 2004;350:232-238.
13. Kastrati A, Mehilli J, Neumann FJ, et al. Abciximab in patients with acute coronary syndromes undergoing percutaneous coronary intervention after clopidogrel pretreatment: the ISAR-REACT 2 randomized trial. JAMA. 2006;295:1531-1538.
14. Hoekstra J, Pollack C, Roe M, Peterson E, Brindis R, Harrington R, Christenson R, Smith S, Ohman M, Gibler WB. Improving the care of patients with acute coronary syndromes in the ED: the CRUSADE initiative. Acad Emerg Med 2002;9:1146-1155.
15. Boersma E, Harrington RA, Moliterno JH, et al: Platelet glycoprotein IIb/IIIa inhibitors in acute coronary syndromes: A meta-analysis of all major randomized clinical trials. Lancet 2002;359:189-198.
16. Stone GW, et al: The ACUITY Timing trial: Presented at the American College of Cardiology Scientific Session, Atlanta, GA, March, 2003.
Copyright EMCREG-International, 2007

5w w w . e m c r e g . o r g
NON-ST-SEGMENT ELEVATION ACUTE CORONARY SYNDROME: OPTIMAL ANTI-COAGULANT THERAPY FOR THE EMERGENCY DEPARTMENT
UFH has important
pharmacokinetic
limitations that
are related to its
nonspecific binding
to plasma proteins
and circulating
endothelial cells.
NON-ST-SEGMENT ELEVATION ACUTE CORONARY SYNDROME: OPTIMAL ANTI-COAGULANT THERAPY FOR THE EMERGENCY DEPARTMENT
Charles V. Pollack, Jr., M.A., M.D., FACEPChairman, Emergency Medicine, Pennsylvania Hospital
Professor of Emergency MedicineUniversity of Pennsylvania School of Medicine, Philadelphia, PA
OBJECTIVES:1. Discuss the options for anticoagulation for non-ST-segment elevation acute coronary
syndrome in the emergency department.2. Describe the differences among these options that may impact the choice of optimal
anticoagulation therapy in the emergency department when managing patients with non-ST-segment elevation acute coronary syndrome.
INTRODUCTIONSince the early 1990s, it has been understood that anti-thrombotic therapy—the combined use of aspirin and an anticoagulant—is foundation therapy for patients with unstable angina and non-ST-segment elevation acute coronary syndrome (NSTE ACS). Aspirin has remained as a foundation for therapy, but the optimal anticoagulant has been debated for the past decade in multiple comparative trials, large and small. Unfractionated heparin (UFH) has been the mainstay anticoagulant for ACS for many years, despite variable evidence for its efficacy and recognized concerns about its pharmacokinetics, pharmaco-dynamics, and bioavailability.
A review of the literature finds studies of UFH in NSTE ACS beginning as early as 1981.1 A placebo-controlled study performed by Theroux et al2 between 1986 and 1988 tested aspirin vs UFH (5,000 U IV bolus, followed by 1,000 U/hr infusion), demonstrating that UFH reduced the risk of myocardial infarction (MI) by 89% and the risk of recurrent refractory angina by 63%. An extension
of this study compared aspirin and UFH in patients with unstable angina. After treatment, MI (fatal or nonfatal) occurred nearly five times more frequently in patients who received aspirin than in patients who received UFH (p = 0.035).3 Conversely, in the Research Group in Instability in Coronary Artery Disease (RISC) trial, men with unstable angina or NSTEMI experienced significantly reduced risk of death or MI if they received aspirin, while treatment with UFH alone showed no benefit. Another group that was treated with the combination of aspirin and UFH had the lowest number of events during the initial 5 days.4 As this finding was assimilated with subsequent data, common practice gradually moved towards combination therapy with aspirin and UFH for ACS (Figure 1).
UFH has important pharmacokinetic limitations that are related to its nonspecific binding to plasma proteins and circulating endothelial cells. This “nonproductive” consumption of administered UFH results in both poor bioavailability and marked variability in

6w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
6w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
0
anticoagulant response among patients.5 The anticoagulant effect of UFH therefore requires monitoring with the activated partial thromboplastin time (aPTT), a test that is sensitive to the inhibitory effects of UFH on thrombin (factor IIa), factor Xa, and factor IXa. While such monitoring may be a nuisance in the ED, currently recommended weight-based dosing regimens for UFH require close follow-up to maintain the balance between necessary anticoagulation and the risk of bleeding. In the most recent ACC/AHA Guidelines,6 the recommended initial regimen is a bolus of 60 to 70 U/kg (maximum 5,000 U) followed by an infusion of 12-15 U/kg/h (maximum 1,000 U/h), targeting aPTT values between 60 and 80 seconds. In addition to body weight, metabolism of UFH is affected by patient age, smoking history, and the presence of diabetes mellitus.5 A rare but dangerous complication of UFH use is autoimmune heparin-induced thrombocytopenia (HIT), which may
paradoxically be complicated by acute thrombosis (HITT).7 Clinical suspicion of HIT or HITT mandates the immediate cessation of all heparin therapy, including that used to flush indwelling intravenous lines.
Alternatives to heparin currently approved for use in the ED for anticoagulation in NSTE ACS are the low molecular weight heparins (LMWH) enoxaparin and dalteparin. Direct thrombin inhibitors, like bivalirudin and synthetic pentasaccharide, have been studied in this setting but as yet are not approved for use by the United States Food and Drug Administration. LMWHs are manufactured through the chemical or enzymatic depolymerization of UFH (which has indirect activity against clotting factors IIa and Xa), yielding compounds with proportionately less anti-IIa activity and proportionately more anti-Xa activity. These drugs bind much less avidly to plasma proteins and endothelial cells than the parent compound, and have a dose-independent clearance with a longer half-life that results in more predictable and sustained anticoagulation with once or twice daily subcutaneous administration. This, coupled with the fact that LMWHs do not generally require laboratory monitoring of anti-thrombotic activity, make these agents particularly well suited for use in the ED.
In the FRagmin In unstable Coronary artery disease (FRIC) study, 1482 patients with UA/NSTEMI received open-label dalteparin (120 IU/kg SQ q12h) or UFH for 6 days.8 At day 6 and until day 45,
LMWHs are manufactured
through the chemical or
enzymatic depolymerization
of UFH (which has indirect
activity against clotting
factors IIa and Xa),
yielding compounds with
proportionately less anti-IIa
activity and proportionately
more anti-Xa activity.
Figure 1. Evidence for heparin use in acute coronary syndrome without ST-segment elevation.

77w w w . e m c r e g . o r g
NON-ST-SEGMENT ELEVATION ACUTE CORONARY SYNDROME: OPTIMAL ANTI-COAGULANT THERAPY FOR THE EMERGENCY DEPARTMENT
patients were randomized a second time to double-blind administration of dalteparin (120 IU/kg QD) or placebo. During the first part of the study, the risk of death, MI, or recurrent angina was not significantly increased with dalteparin (9.3% vs. 7.65%, p = 0.33), and the risk of death or MI was unaffected (3.9% vs. 3.6%, p = 0.8); death occurred more frequently with dalteparin (1.5% vs. 0.4% with UFH, p = 0.057). Between days 6 and 45, the rates of death, MI, and recurrence of angina were comparable between the dalteparin and placebo groups. Dalteparin was approved for use in the United States as an anticoagulant in NSTE ACS on the basis of this study.
In the latter half of the 1990s, two studies established the LMWH enoxaparin as being superior to UFH, at least in the medical management of NSTE ACS. This finding was underscored in the 2002 ACC/AHA guidelines for the management of unstable angina and NSTEMI, as enoxaparin became a IIa (level of evidence A) recommendation.6 The ESSENCE trial9 compared enoxaparin (1 mg/kg Q12h by subcutaneous administration) with standard UFH (5,000 U bolus), administered for 48 hours to 8 days (median duration in both groups of 2.6 days). With UFH, only 46% of patients reached the target aPTT within 12 to 24 h, reinforcing the lack of reliability of anticoagulation with this agent. The composite outcome of death, MI, or recurrent angina was reduced by 16.2% at 14 days with enoxaparin (19.8% UFH vs. 16.6% enoxaparin, p = 0.019) and by 19% at 30 days (23.3% vs. 19.8%, p = 0.017) (Figure 2). The single endpoint rates of death did not differ. One year follow-up of these patients demonstrated preservation of this difference between enoxaparin and UFH (Figure 3). A summary of clinical efficacy for four LMWHs and UFH is shown in Figure 4. The subsequent TIMI 11B trial10 randomized 3,910 patients with UA/NSTEMI to enoxaparin (30 mg IV initial bolus immediately followed by subcutaneous dosing of 1 mg per kg every 12 h) or UFH (70 U/kg bolus plus infusion of 15 U/kg/h titrated to a target aPTT 1.5 to 2.5 times control). The composite end point of death, MI, or need for an urgent revascularization was reduced at 8 days from 14.5% to 12.4% (p = 0.048) and at 43 days from 19.6%
Figure 3. ESSENCE one year follow-up data for death, MI, recurrent ischemia and coronary revascularization.
Figure 2. Comparison of the composite outcome of death, MI, or recurrent angina in the ESSENCE Trial.
to 17.3% (p = 0.048) with enoxaparin. The rates of death or MI were reduced from 6.9% to 5.7% (p = 0.114) at 14 days and from 8.9% to 7.9% (p = 0.276) at 43 days. The risk of minor bleeding was increased with enoxaparin (Figure 5).

8w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
8w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
A number of subsequent studies and registries were used to explore the potential role of enoxaparin in an interventional environment, as after 2000 the definitive management of NSTE ACS became increasingly based on angiography and revascularization. There were promising data from Collet et al,11 from the NICE registries,12 and from the interventional cohort of INTERACT.13 However, the optimal role for enoxaparin in the NSTE ACS patient being rapidly transitioned to the cardiac catheterization laboratory to be definitively investigated in the SYNERGY study.
Published in 2004, SYNERGY14 compared enoxaparin and UFH in 10,027 patients with NSTE ACS and high-risk features, 92% of whom underwent diagnostic coronary angiography. Patients were randomized to enoxaparin (1mg/kg SQ 12h) or UFH (60 U/kg bolus, then 12 U/kg/hr, adjusted to an aPTT of 50 to 70 seconds). Both groups had a median age of 68 (older than in previous trials), and 34% were women. On the index hospitalization, 47% underwent PCI, and 19% had bypass surgery; 57% received a glycoprotein IIb/IIIa receptor inhibitor, and 66% received clopidogrel. In this management setting, the two drugs were very similar in terms of ischemic efficacy. There were some bleeding concerns in the enoxaparin arm with increased TIMI major bleeding, although GUSTO severe bleeding and transfusion requirements were not different. Some of the excess bleeding has been attributed to off-protocol “switching” between enoxaparin and UFH. The major conclusion from the SYNERGY trial is that enoxaparin is as effective as heparin in contemporary ACS practice, while bleeding can be minimized with consistent anticoagulant therapy and no “switches.” Scrupulous attention to renal insufficiency as measured by creatinine clearance, particularly in older patients is necessary (Figure 6). Multiple subanalyses of this and other issues are expected from the SYNERGY investigators over the next several years.
Figure 4. Comparison of evaluating low molecular weight heparin versus unfractionated heparin (UFH).
Figure 5. Results of TIMI IIB comparing unfractionated heparin (UFH) versus enoxaparin.

99w w w . e m c r e g . o r g
NON-ST-SEGMENT ELEVATION ACUTE CORONARY SYNDROME: OPTIMAL ANTI-COAGULANT THERAPY FOR THE EMERGENCY DEPARTMENT
Emergency physicians
should be aware of
the importance of
balancing ischemic
risk and the
prevention of bleeding
complications which
occur after transition
of care of NSTE
ACS patients to the
cardiology service.
Emergency physicians should be aware of the importance of balancing ischemic risk and the prevention of bleeding complications which occur after transition of care of NSTE ACS patients to the cardiology service. Examination of the LMWH and UFH literature, as well as newer data for bivalirudin and pentasaccharide, it is apparent that there is no one optimal anticoagulation approach upstream of the catheterization laboratory. The choice of therapy in the ED should be based on a multidisciplinary institutional pathway and such specific factors for each patient as whether or not cardiac catheterization is planned and when the intervention will occur, age, renal function, baseline hematocrit, ischemic risk, and bleeding risk for the patient.
REFERENCES1. Telford AM, Wilson C: Trial of heparin versus atenolol in prevention of myocardial
infarction in intermediate coronary syndrome. Lancet 1981;1:1225-28.
2. Theroux P, Ouimet H, McCans J, et al: Aspirin, heparin, or both to treat acute unstable angina. N Engl J Med 1988;319:1105-11.
3. Theroux P, Waters D, Qiu S, McCans J, de Guise P, Juneau M: Aspirin versus heparin to prevent myocardial infarction during the acute phase of unstable angina. Circulation 1993;88:2045-8.
4. RISC Group: Risk of myocardial infarction and death during treatment with low dose aspirin and intravenous heparin in men with unstable coronary artery disease. Lancet 1990;336:827-30.
Figure 6. Primary efficacy outcome data from SYNERGY Trial comparing enoxaparin to unfractionated heparin (UFH)

10w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
5. Hirsh J, Warkentin TE, Raschke R, Granger C, Ohman EM, Dalen JE: Heparin and low-molecular-weight heparin: mechanisms of action, pharmacokinetics, dosing considerations, monitoring, efficacy, and safety. Chest 1998;114:489S-510S.
6. Braunwald E, Antman EM, Beasley JW, et al: ACC/AHA 2002 guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Unstable Angina). 2002. Available at: http://www.acc.org/clinical/guidelines/unstable/incorporated/index.htm.
7. Warkentin TE, Levine MN, Hirsh J, et al: Heparin-induced thrombocytopenia in patients treated with low-molecular-weight heparin or unfractionated heparin. N Engl J Med 1995;332:1330-5.
8. Klein W, Buchwald A, Hillis SE, et al: Comparison of low-molecular-weight heparin with unfractionated heparin acutely and with placebo for 6 weeks in the management of unstable coronary artery disease. FRagmin In unstable Coronary artery disease study (FRIC). Circulation 1997;96:61-68.
9. Cohen M, Demers C, Gurfinkel EP, et al, for the Efficacy and Safety of Subcutaneous Enoxaparin in Non-Q-Wave Coronary Events Study Group: A comparison of low-molecular-weight heparin with unfractionated heparin for unstable coronary artery disease. N Engl J Med 1997;337:447-52.
10. Antman EM, McCabe CH, Gurfinkel EP, et al: Enoxaparin prevents death and cardiac ischemic events in unstable angina/non-Q-wave myocardial infarction: results of the Thrombolysis In Myocardial Infarction (TIMI) 11B trial. Circulation 1999;100:1593-601.
11. Collet JP, Montalescot G, Lison L, et al : Percutaneous coronary intervention after subcutaneous enoxaparin pretreatment in patients with unstable angina pectoris. Circulation 2001;103:658-63.
12. Kereiakes DJ, Grines C, Fry E, et al: Enoxaparin and abciximab adjunctive pharmacotherapy during percutaneous coronary intervention. J Invasive Cardiol 2001;13:272-8.
13. Goodman S, Fitchett D, Armstrong PW, et al: Randomized evaluation of the safety and efficacy of enoxaparin versus unfractionated heparin in high-risk patients with non-ST-segment elevation acute coronary syndromes receiving the glycoprotein IIb/IIIa inhibitor eptifibatide. Circulation 2003;107:238-44.
14. Ferguson JJ, Califf R, Antman EM, et al: Enoxaparin vs unfractionated heparin in high-risk patients with non-ST-segment elevation acute coronary syndromes managed with an intended early invasive strategy: primary results of the SYNERGY randomized trial. JAMA 2004;292:45-54.
Copyright EMCREG-International, 2007

11w w w . e m c r e g . o r g
CRUSADE QUALITY IMPROVEMENT INITIATIVE: BETTER CARE FOR PATIENTS WITH UNSTABLE ANGINA AND NON-ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION CRUSADE QUALITY IMPROVEMENT INITIATIVE: BETTER CARE FOR PATIENTS WITH UNSTABLE ANGINA AND NON-ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION
Deborah B. Diercks, MDAssociate Professor, Department of Emergency Medicine
University of California, Davis, Medical Center, Sacramento, California
In 2002, the
American College of
Cardiology/American
Heart Association
disseminated expert
recommendations for
the management of
patients with
non-ST-segment
elevation myocardial
infarction ACS.
OBJECTIVES:1. Describe the CRUSADE quality improvement initiative.2. Using data from CRUSADE, describe the changes in acute care practice patterns that
have occurred during the last four years.3. Define potential areas of quality improvement directly related to emergency department
care for non-ST-segment elevation acute coronary syndrome.
INTRODUCTIONThe recognition and treatment of a patient with an acute coronary syndrome (ACS) are critical components of the evaluation of the patient with a complaint of chest pain by the emergency physician. Once a patient has been identified as having ACS, the treatment of these individuals traditionally has been based on local practices with generalized adoption of the use of aspirin and beta-blockers. In 2002, the American College of Cardiology/American Heart Association disseminated expert recommendations for the management of patients with non-ST-segment elevation myocardial infarction (NSTE) ACS.1 These recommendations encompass the entire course of care for a patient with NSTE ACS beginning in the pre-hospital setting.
Despite multiple iterations of these guidelines, routine adaptation into general clinical practice has not occurred. In an effort to stimulate better adherence to practice guidelines and improve the quality of care for patients with NSTE ACS, the CRUSADE (Can Rapid Risk Stratification of Unstable Angina
Patients Suppress ADverse Outcomes with Early Implementation of the ACC/AHA Guidelines) quality improvement
and educational initiative was developed. This program serves as an NSTE ACS registry and provides an innovative and multifaceted approach to the education of emergency physicians and cardiologists in the care of these patients. The CRUSADE quality improvement initiative is a multidisciplinary cooperative effort involving over 400
emergency departments (EDs) and medical centers across the United States. CRUSADE includes a registry of patients who meet diagnostic criteria for high-risk
NSTE ACS (positive cardiac markers, ST-segment depression, or transient ST-segment elevation). It was designed to characterize demographic patterns and risk stratification results. Embedded in this registry are mechanisms to measure the use of ED treatment modalities
including aspirin, heparin, beta-blockers, and platelet inhibitors as recommended in the ACC/AHA guidelines. Along with an education program, each participating institution is given a report of their own

12w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
12w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
The CRUSADE ACS
registry patient records
can be analyzed to
determine compliance
with ACC/AHA
guidelines for patients
with NSTE ACS.
treatment patterns. This initiative represents a truly innovative approach to improving care for ACS patients in the ED as well as on the cardiology service, recognizing that the care of patients with NSTE ACS is a continuum that begins in the ED and persists throughout the hospital course. This article describes the CRUSADE quality improvement initiative, its implications for the practicing emergency physician, and how to further identify areas for NSTE ACS care requiring improvement.
CRUSADE Quality Improvement InitiativeThe CRUSADE NSTE ACS registry includes patients who are prospectively identified in the ED as well as those who are retrospectively identified by discharge diagnosis
Practice PatternsThe CRUSADE quality improvement initiative is currently in its 5th year of data collection and education. As a result of this, the temporal changes in treatment patterns can be compared. When compared to clinical trials, patients enrolled in the CRUSADE quality improvement initiative are older, more often diabetic, female, have had a myocardial infarction, have a history of heart failure, and have undergone a PCI or CABG (Table 1).2-4 In addition, the in-hospital mortality rate (4.5%) is double that of clinical trials with similar entry criteria (Figure 1).2,3 This difference exhibited between patients enrolled in randomized clinical trials and those in the CRUSADE population has persisted over the last four years.4
Over the past 4 years there has been dramatic increase in the use of guideline recommended therapies.4 The increase in the use of acute medications includes a large increase in the percentage of patients receiving aspirin, beta-blockers, and heparin which are traditionally administered in the ED (Table 2). There has also been a decrease in the time from presentation to cardiac catheterization and coronary intervention. This accompanies a higher percentage of patients undergoing coronary catheterization (Table 3).
Although quality improvement initiatives are an integral part of the health care system, the success of these programs should be measured by their ability to change care coupled with evidence of improved outcome that accompanies this change. Using the CRUSADE registry, Peterson et al. showed that composite guideline adherence rates were significantly associated with in-hospital mortality. Observed mortality rates decreased from 6.31% in the hospitals with the lowest
or procedural logs. Patient inclusion criteria include 1) chest pain or anginal equivalent at rest, at least 10 minutes in duration and occurring less than 24 hours prior to presentation; 2) ischemic electrocardiogram
(ECG) changes (ST-segment depression or transient ST-segment elevation); or 3) elevated levels of biomarkers of myocardial necrosis (creatine kinase-MB or troponin) above baseline levels. Patients transferred into participating hospitals must arrive within 24 hours of their symptom onset to be eligible.
The CRUSADE ACS registry patient records can be analyzed to determine compliance with ACC/AHA guidelines for patients with NSTE ACS. The data points for acute therapy include treatment with aspirin, beta-blockers, heparin, glycoprotein IIb/IIIa inhibitors, as well as clopidogrel. Timing of therapies is documented in order to differentiate ED utilization from in-hospital downstream interventions. Contraindications for medication administration must be documented if not administered and the time frame identified for acute medication administration is 24 hours after ED presentation. Risk stratification criteria such as ECG and biomarker results are established for each patient. Patients are followed through their hospitalization course to determine outcomes.

13w w w . e m c r e g . o r g
CRUSADE QUALITY IMPROVEMENT INITIATIVE: BETTER CARE FOR PATIENTS WITH UNSTABLE ANGINA AND NON-ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION
13w w w . e m c r e g . o r g
CRUSADE QUALITY IMPROVEMENT INITIATIVE: BETTER CARE FOR PATIENTS WITH UNSTABLE ANGINA AND NON-ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION
2002 2006
Aspirin
Beta-blocker
Heparin
Glycoprotein IIb/IIIa inhibitor
90%
76%
83%
32%
96%
91%
87%
45%
Medication
0
1
2
3
4
5
6
PURSUIT1
(n = 9,461)PRISM-PLUS2
(n = 1,915)SYNERGY3
(n = 9,975)CRUSADE(n = 165,498)
1.8% 1.9%1.5%
4.5%
7-day mortality rate
In-hospitalmortality rate
Variable PURSUIT CURE SYNERGY CRUSADE(n = 9461) (n = 12,562) (n = 9975) (n = 165,498)
Mean age ± SD (yrs) 63 ± 11 63 ± 12 67 ± 11 67 ± 14
Female sex (%) 36 39 34 40
Diabetes mellitus (%) 23 23 29 33
Prior MI (%) 32 25 28 30
Prior CHF (%) 11 8 9 18
Prior PCI (%) 13 18* 20 21
Prior CABG (%) 12 18* 17 19
ST depression (%) 50 42 55 35
Table 1. Baseline characteristics for patients enrolled in three randomized clinical trials and CRUSADE.
Figure 1. In-hospital mortality rate in three randomized clinical trials versus CRUSADE. 1: The PURSUIT Trial Investigators, N Engl J; Med 1998; 2: The PRISM-PLUS Study Investigators, N Engl J Med 1998; 3: The Synergy Study JAMA 2004; 4: CRUSADE cumulative data: (through 12/31/2005)
Table 2. Acute treatment changes for therapies administered in the first 24 hours for patients with NSTE ACS. Adapted from National Data Reports (www.crusadeqi.com).
Cath
PCI
CABG
67%
36%
11%
% Hours(95% CI)
83%
63%
11%
32 (16,59)
28 (14,58)
86 (46,122)
23.3
21.6
68.6
% Hours(95% CI)
2002 2006ProcedureTable 3. Changes in time to procedure for patients with NSTE ACS. Adapted from National Data Reports (www.crusadeqi.com). PCI: percutaneous coronary intervention, CABG: coronary artery bypass grafting.

14w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
14w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
compliance rate to 4.15% for the highest compliance rate (P<.001) when the adherence scores were stratified into quartiles. After risk adjustment, every 10% increase in composite adherence at a hospital was associated with an analogous 10% decrease in its patients’ likelihood of in-hospital mortality (adjusted odds ratio, 0.90, 95% CI 0.84–0.97; P<.001) (Figure 2).5 Although these results were a composite of adherence to acute and chronic medications, similar trends were seen when acute medications were evaluated independently.
The trends noted in improved adherence coupled with the association of improved outcome are a credit to the effort of all the participants in the CRUSADE registry. These results show that collaboration, education, and continuous feedback with hospital administrators and health care providers can improve the care of patients with NSTE ACS.
Special PopulationsAlong with providing educational materials and regular feedback to the participating hospitals, the CRUSADE project has created a robust registry that
is being used to further the understanding of the management for patients with NSTE-ACS. Importantly, the CRUSADE registry has collected data points that enable analysis of parameters of clinical importance to the emergency physician. Manuscripts have addressed critical areas of disparity in acute treatment,6-12 outcomes associated with diagnostic tests performed in the ED settings,13-17 and potential areas where practice patterns can improve.18,19
Disparity in CareUsing the CRUSADE registry, differences in acute management of special populations have been analyzed. Blomkalns et al. evaluated the impact of gender on adhering to guideline-based treatment recommendations.7 Women were treated less aggressively than men in the administration of these acute medications - heparin, angiotensin-converting enzyme inhibitors, and glycoprotein IIb/IIIa inhibitors. In addition, women were less likely to undergo cardiac catheterization than men. Despite the difference in the acute treatment of women, there was no difference in the outcomes of death and re-infarction after adjustment for confounders.7 In a separate analysis, difference in the treatment by patient age was evaluated. It was reported that the use of anti-thrombin and anti-platelet drugs decreased as age increased. The rate of cardiac catheterization also decreased as age increased. These reductions in therapy use were associated with an increased rate of death and re-infarction with increasing age.6
The impact of patient race on ACS care was also evaluated. Data from
Although quality
improvement initiatives
are an integral part of
the health care system,
the success of these
programs should be
measured by their
ability to change care
coupled with evidence
of improved outcome
that accompanies
this change.
87% 90%
50%
66% 66%
17%
Aspirin Beta Blockers Heparin GP IIb-IIIa
Leading Centers
Lagging Centers
0%
20%
40%
60%
80%
100% 96%
85%
Figure 2. Comparison of guideline adherence for hospitals for acute medication use: Leading and lagging hospitals over first 24 hours.

15w w w . e m c r e g . o r g
CRUSADE QUALITY IMPROVEMENT INITIATIVE: BETTER CARE FOR PATIENTS WITH UNSTABLE ANGINA AND NON-ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION
15w w w . e m c r e g . o r g
CRUSADE QUALITY IMPROVEMENT INITIATIVE: BETTER CARE FOR PATIENTS WITH UNSTABLE ANGINA AND NON-ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION
CRUSADE have indicated that acute treatment varies by race.10,12 Black patients had a similar or higher likelihood than whites of receiving ACS treatments such as aspirin, beta-blockers, or ACE inhibitors but were significantly less likely to receive newer ACS therapies, including glycoprotein IIb/IIIa inhibitors and clopidogrel. Blacks were also less likely to receive cardiac catheterization or revascularization procedures. Despite difference in acute therapy there was no difference for in-hospital outcomes in black patients with NSTE ACS.10 Hispanics were noted to be managed more conservatively than whites. They were shown to undergo stress tests more frequently (13.0% vs 10.1%, P < .0001), and have less use of cardiac catheteri-zation within 48 hours (48.7% vs 55.5%, P < .0001).12 Clinical Practice In addition to evaluating treatment disparity by specific patient populations, data from the CRUSADE registry have been used to address pertinent clinical questions ranging from diagnosis of ACS to current treatment practice. In the clinical setting, it is difficult to interpret discrepant results between creatinine kinase-MB (CK-MB) and cardiac troponin (cTn) levels. Newby et al evaluated the risk of in-hospital mortality by troponin and CK-MB status.15 In-hospital mortality was 2.7% among CK-MB-/cTn- patients; 3.0%, CK-MB+/cTn-; 4.5%, CK-MB-/cTn+; and 5.9%, CK-MB+/cTn+. After adjustment for other presenting risk factors, in-hospital death was highest in patients who were troponin positive. The authors concluded that an elevated troponin level identifies patients at increased acute risk regardless of CK-MB status, but an isolated CK-MB+ status still has some prognostic value.15
Morphine has been traditionally used for the management of persistent pain in patients with cardiac related chest pain. Although never extensively studied, the use of morphine has become part of the standard therapy approach for patients with chest pain. In an analysis of the CRUSADE registry, morphine used either alone or in combination with nitroglycerin for patients presenting with NSTE ACS was associated with higher mortality even after risk adjustment and matching for propensity score for treatment. This analysis can not show a direct correlation
with adverse events, but raises concerns regarding the safety of using morphine for these patients and emphasizes the need for a randomized trial evaluating the use of morphine in the NSTE ACS population.14 Without data from a large observation registry such as CRUSADE it is doubtful that an association between morphine and in-hospital mortality would have been discovered.
Areas for ImprovementThe CRUSADE registry has also identified areas of clinical care that warrant further evaluation. Specifically, the registry has helped identify the process of care issues that are related to outcome in patients with NSTE ACS.18,19 While patients with NSTE ACS are typically admitted promptly after diagnosis, under conditions of ED or hospital overcrowding these patients may have prolonged ED stays. This can occur as the patient waits for transfer to an inpatient unit or to the cardiac catheterization laboratory. These patients continue to require ongoing evaluation and treatment. Under such conditions, it is possible for these patients to be less closely monitored or treated less aggressively as ED staff attention is diverted to the triage and treatment of new acute patients. Data from the CRUSADE registry suggest that patients who stay in the ED longer than usual for a given institution are less likely to receive guideline driven therapy for NSTE ACS and have worse in-hospital clinical outcomes than those patients who stay in the ED an the average length of stay.18
Another area of clinical importance is a potential for medication dosing errors in patients with NSTE ACS. The recommendations for acute treatment with anti-platelet and anti-thrombin drugs require specific dosing based on weight and creatinine clearance. The complexity of the dosing of these agents led to 42% of the patients receiving an excess dose of one of these drugs. Factors associated with excess dosing included older age, female sex, renal insufficiency, low body weight, diabetes mellitus, and congestive heart failure. Relative to those patients not administered excess dosages, patients with excess dosages of unfractionated heparin, low molecular weight heparin, and glycoprotein IIb/IIIa inhibitors tended toward higher risks for major bleeding (adjusted odds ratio [OR], 1.08; 95% confidence interval [CI], 0.94-1.26; OR, 1.39;

16w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
95% CI, 1.11-1.74; and OR, 1.36; 95% CI, 1.10-1.68; respectively). Mortality and length of stay were higher among those patients with excess drug doses. Both of these studies have identified areas that can be improved by focused education and protocol-driven care.19
SUMMARYThe CRUSADE quality improvement initiative has led to improve adherence to guideline recommended therapies. Through educational efforts, direct feedback, and a mechanism to foster collaboration between specialties at member hospitals, care for patients with NSTE ACS can be improved, with better outcomes. Data collected from this registry have also provided insight on the disparities of care and challenges to current practice patterns. Through the use of registries such as CRUSADE for NSTE ACS, consistent guideline-based therapies can be delivered for our patients with improved outcomes.
REFERENCES1. Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA 2002 guideline
update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction--summary article: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on the Management of Patients With Unstable Angina). J Am Coll Cardiol 2002;40(7):1366-74.
2. Ferguson JJ, Califf RM, Antman EM, et al. Enoxaparin vs unfractionated heparin in high-risk patients with non-ST-segment elevation acute coronary syndromes managed with an intended early invasive strategy: primary results of the SYNERGY randomized trial. Jama 2004;292(1):45-54.
3. Inhibition of platelet glycoprotein IIb/IIIa with eptifibatide in patients with acute coronary syndromes. The PURSUIT Trial Investigators. Platelet Glycoprotein IIb/IIIa in Unstable Angina: Receptor Suppression Using Integrilin Therapy. N Engl J Med 1998;339(7):436-43.
4. National Data Reports. www.crusadeqi.com.
5. Peterson ED, Roe MT, Mulgund J, et al. Association between hospital process performance and outcomes among patients with acute coronary syndromes. JAMA 2006;295(16):1912-20.
6. Alexander KP, Roe MT, Chen AY, et al. Evolution in cardiovascular care for elderly patients with non-ST-segment elevation acute coronary syndromes: results from the CRUSADE National Quality Improvement Initiative. J Am Coll Cardiol 2005;46(8):1479-87.
7. Blomkalns AL, Chen AY, Hochman JS, et al. Gender disparities in the diagnosis and treatment of non-ST-segment elevation acute coronary syndromes: large-scale observations from the CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse
Outcomes With Early Implementation of the American College of Cardiology/American Heart Association Guidelines) National Quality Improvement Initiative. J Am Coll Cardiol 2005;45(6):832-7.
8. Han JH, Chandra A, Mulgund J, et al. Chronic kidney disease in patients with non-ST-segment elevation acute coronary syndromes. Am J Med 2006;119(3):248-54.
9. Diercks DB, Roe MT, Mulgund J, et al. The obesity paradox in non-ST-segment elevation acute coronary syndromes: results from the Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the American College of Cardiology/American Heart Association Guidelines Quality Improvement Initiative. Am Heart J 2006;152(1):140-8.
10. Sonel AF, Good CB, Mulgund J, et al. Racial variations in treatment and outcomes of black and white patients with high-risk non-ST-elevation acute coronary syndromes: insights from CRUSADE (Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines). Circulation 2005;111(10):1225-32.
11. Brogan GX, Jr., Peterson ED, Mulgund J, et al. Treatment disparities in the care of patients with and without diabetes presenting with non-ST-segment elevation acute coronary syndromes. Diabetes Care 2006;29(1):9-14.
12. Cohen MG, Roe MT, Mulgund J, et al. Clinical characteristics, process of care, and outcomes of Hispanic patients presenting with non-ST-segment elevation acute coronary syndromes: results from Can Rapid risk stratification of Unstable angina patients Suppress ADverse outcomes with Early implementation of the ACC/AHA Guidelines (CRUSADE). Am Heart J 2006;152(1):110-7.
13. Diercks DB, Peacock WF, Hiestand BC, et al. Frequency and consequences of recording an electrocardiogram >10 minutes after arrival in an emergency department in non-ST-segment elevation acute coronary syndromes (from the CRUSADE Initiative). Am J Cardiol 2006;97(4):437-42.
14. Meine TJ, Roe MT, Chen AY, et al. Association of intravenous morphine use and outcomes in acute coronary syndromes: results from the CRUSADE Quality Improvement Initiative. Am Heart J 2005;149(6):1043-9.
15. Newby LK, Roe MT, Chen AY, et al. Frequency and clinical implications of discordant creatine kinase-MB and troponin measurements in acute coronary syndromes. J Am Coll Cardiol 2006;47(2):312-8.
16. Roe MT, Peterson ED, Li Y, et al. Relationship between risk stratification by cardiac troponin level and adherence to guidelines for non-ST-segment elevation acute coronary syndromes. Arch Intern Med 2005;165(16):1870-6.
17. Roe MT, Peterson ED, Pollack CV, Jr., et al. Influence of timing of troponin elevation on clinical outcomes and use of evidence-based therapies for patients with non-ST-segment elevation acute coronary syndromes. Ann Emerg Med 2005;45(4):355-62.
18. Diercks DB, Roe MT, Chen AY, et al. Prolonged emergency department stays are associated with worse guideline adherence and increased adverse events. American College of Emergency Physicians Scientific Assembly; 2006; New Orleans, LA; 2006. p. abstract.
19. Alexander KP, Chen AY, Roe MT, et al. Excess dosing of anti-platelet and anti-thrombin agents in the treatment of non-ST-segment elevation acute coronary syndromes. JAMA 2005;294(24):3108-16.
Copyright EMCREG-International, 2007

17w w w . e m c r e g . o r g
ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION (STEMI):DECREASING THE TIME TO TREATMENT IN THE ED
W. Brian Gibler, MDProfessor and Chairman; Department of Emergency Medicine,
University of Cincinnati College of Medicine, Cincinnati, Ohio, President, EMCREG-International
OBJECTIVES:1. Describe the role of fibrinolytic therapy in ST-segment elevation acute myocardial infarction
(STEMI).2. Review the impact of the 2004 ACC/AHA Guidelines for the treatment of STEMI on the
routine care of this disease process in the emergency department.3. Define the appropriate conditions for using fibrinolytic agents or percutaneous coronary
intervention in patients with STEMI.4. Describe the role of the entire team in the coordination and implementation of effective
care for STEMI patients.
INTRODUCTIONFor the last 2 decades, it has been well recognized that decreasing time to opening an occluded coronary artery in patients with ST-segment elevation myocardial infarction (STEMI) reduced mortality. Rapid reperfusion of ischemic myocardium improves left ventricular function, reduces infarct size, and ultimately increases patient survival. In the middle to late 1980’s, multiple large randomized trials began to demonstrate the efficacy of fibrinolytic therapy for treating STEMI. During the 1990’s, percutaneous coronary intervention (PCI), first through balloon angioplasty with evolution to routine stent placement, showed favorable comparison to fibrinolytic therapy in multiple trials, becoming the favored method for opening coronary arteries in STEMI patients at many institutions in the US that served as tertiary cardiac referral centers. Requirements for cardiothoracic surgery back-up for PCI limited the availability of interventional cardiology for STEMI to a relatively small number of hospitals. During the last 5 years there has been a resurgence of interest in defining the optimal approach to reperfusion therapy. In 2004, the American College of Cardiology/American Heart Association (ACC/AHA) Guidelines for the management of patients with ST-segment elevation
myocardial infarction recommended PCI as optimal therapy if the door to balloon opening time was 90 minutes or less from time of patient presentation to the emergency department (ED).1 If the delay in providing PCI was greater than 1 hour more than the 30 minute time period required to deliver intravenous fibrinolytics in the ED, fibrinolysis was considered the preferred reperfusion therapy. For patients presenting less than 3 hours after symptom onset, and there is no delay to an invasive strategy, there is no preference for either strategy (Figure 1).
FibrinolysisIn 1986, the GISSI, ISAM, AIMS, ISIS-2 and ASSET trials provided conclusive evidence in a randomized fashion versus placebo that streptokinase, streptokinase, anistreplase (APSAC), streptokinase, and tissue plasminogen activator respectively reduced mortality in patients with STEMI, typically within 6-12 hours after symptom onset.2-7 Beginning in the early 1990’s, study groups such as EMERAS and the LATE investigators began to explore treatment 6 hours or greater after symptom onset for STEMI patients.8,9 In 1994, the Fibrinolytic Therapy Trialist group performed a meta-analysis of all randomized
ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION (STEMI):DECREASING THE TIME TO TREATMENT IN THE ED

18w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
18w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
Figure 1. Assessment of reperfusion options. STEMI indicates ST-elevation myocardial infarction; PCI, percutaneous coronary intervention; ICH, intracranial hemorrhage. *Applies to fibrin-specific agents. Operator experience greater than a total of 75 primary PCI cases per year. Team experience greater than a total of 36 primary PCI cases per year. This calculation implies that the estimated delay to the implementation of the invasive strategy is greater than 1 hour vs initiation of fibrinolytic therapy immediately with a fibrin-specific agent. Adapted with permission from Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA Guidelines for the Management of Patients With ST-Elevation Myocardial Infarction—Executive Summary A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients With Acute Myocardial Infarction). J Am Coll Cardiol 2004;44:671–719.
The routine use of
PCI for patients with
STEMI, regardless of
whether the patient
presents primarily to an
interventional cardiology
center (PCI capable) or
is transferred from a
non-PCI capable center
to an interventional
center, has become
controversial.
fibrinolytic trials greater than 1000 patients showing that mortality benefit for patients receiving fibrinolysis was critically time-dependent. The greatest mortality benefit was noted in the first 3 hours after symptom onset, particularly in the first hour, with some statistical improvement in mortality seen up to 12 hours after symptom onset.10 For patients treated within 1 hour after symptom onset, there was an absolute mortality benefit of 39 lives saved per 1000 patients. If
treated between 2-3 hours after symptom onset, 30 lives were saved per 1000 patients and 21 lives were saved if patients were treated between 7-12 hours after symptoms began. Effectively, an absolute benefit reduction of 1.6 lives was realized for each hour of delay. Data from pre-hospital fibrinolytic trials indicate that the original Boersma curve demonstrating mortality benefit from fibrinolysis could actually be shifted 45-60 minutes to the right (Figure 2).11 These data are well

1919w w w . e m c r e g . o r g
ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION (STEMI):DECREASING THE TIME TO TREATMENT IN THE ED
Boersma’s original curveBoersma’s curve right shifted 45 minutesBoersma’s curve right shifted 60 minutes
Treatment delays (hours)0 1 2 3 4 5 6
140
120
100
80
60
40
20
0
Num
ber o
f extr
a liv
es sa
ved
per 1
000
treat
ed
Figure 2. Number of extra lives saved per 1000 patients treated with fibrinolytics at different time treatment delays from symptom onset. Adapted with permission from Terkelsen CJ, Lassen JF, Norgaard BL, et al. Are we underestimating the full potential of early thrombolytic treatment in patients with acute myocardial infarction? Heart 2003; 89:483-484.
summarized in an excellent recent publication evaluating indications for reperfusion therapy in patients with suspected MI.12 Current fibrinolytic agents such as rPA (reteplase) and TNK-tPA (tenecteplase) provide improved fibrin specificity combined with easier administration regimens compared to the original fibrinolytic agents, tPA (alteplase) and SK (streptokinase).13-17
Percutaneous Coronary InterventionFor patients presenting directly to a hospital with experienced acute interventional capabilities, PCI offers advantages including a higher TIMI-3 flow rate (greater than 95% compared to approximately 65% for fibrinolytic therapy) with a lower risk of intracranial hemorrhage. Bleeding at the site of skin/femoral artery penetration, typically in the groin, is greater for patients undergoing PCI though this bleeding can be controlled and usually is nonfatal. Finally, if time to balloon opening is 90 minutes or less after presentation, the advantages of greater TIMI-3 flow rate with less intracranial bleeding translates into improved mortality.18-20
In patients enrolled in the National Registry of Myocardial Infarction between June 1994 and March 1998, Cannon and colleagues found that multivariate-adjusted odds of mortality were increased over 40% when the door to balloon time was longer than 2 hours.21 Berger et al evaluated time or randomization to angioplasty during 4 time intervals from the GUSTO-IIb trial: <60, 61-75, 76-90, and >91 minutes for mortality. Each time interval had a 1.6-fold greater risk for death than the preceding time interval [95% confidence interval (CI), 1.13-2.26, P value = 0.008].22 Despite a Danish trial demonstrating favorable results for patients transferred from 24 community hospitals transferred to 5 invasive treatment centers,23 results from 4,278 transferred patients from the National Registry of Myocardial Infarction from January 1999 through December 2002 showed a median door to balloon time of 180 minutes, with only 4.2% treated within 90 minutes.24,25
Impact of Time to TreatmentOver the last 3 years, the routine use of PCI for patients with STEMI, regardless of whether the patient presents primarily to an interventional cardiology center (PCI capable) or is transferred from a non-PCI capable center to an interventional center, has become controversial.26 The additional time required to perform PCI, due to logistics, particularly for patients presenting “off hours” at an institution offering primary PCI for STEMI or to a non-PCI capable institution requiring transfer for PCI, may eliminate the advantages of PCI over intravenous fibrinolytics (Figures 3, 4, and 5).24-37 In these circumstances where the cardiac catheterization team is not “in house” at a PCI-capable center or for patients presenting to a non-PCI capable hospital, administration of fibrinolytic therapy may provide the best opportunity to gain coronary artery reperfusion within the first 2-3 hours after symptom onset. This represents the ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction optimal strategy of giving fibrinolytic therapy intravenously if the delay compared to door to balloon time for PCI exceeds 60 minutes.1

20w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
20w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
Figure 5. Mortality rates with primary PCI as a function of PCI-related time delay. Adapted with permission from Nallamothu BK, Bates ER. PCI versus fibrinolytic therapy in acute myocardial infarction: is timing (almost) everything? Am J Cardiol 2003; 92:824-826.
15
10
5
0
-50 20 40 60 80 100
P=0.006
Ab
solu
te R
isk
Dif
fere
nce
in D
eath
(%
)
PCI-Related Time Delay [(door-to-balloon time) - (door-to-needle time)]
������ ����� � ������ ���� �� ���������� ���������� ���� � �������� ���������������
������� � ������ ���
���� � ������ �����
��� ����� �� ������ ����� �� ���� ��� ��������� �� ��������� ���������� ������� ������
Developing Institutional Care PathwaysFor each institution, collaboration between emergency physicians, cardiologists, nursing, prehospital care providers, hospital administrators, and pharmacists for creation of a standardized approach to STEMI care is essential.37 This requires the routine use of pre-hospital electrocardiography, if available, to identify patients with STEMI in the pre-hospital setting before arrival at the hospital. Emergency physicians and nurses should have agreed upon standard order sets which include perfor-mance of a 12-lead electrocardiogram in 10 minutes or less and a uniform approach to ensuring that the STEMI patient receives appropriate adjunctive therapy including aspirin, beta-blockers, heparin/low molecular weight heparin, clopidogrel and glycoprotein IIb/IIIa receptor inhibitors as indicated. Cardiologists and emergency physicians must agree on the appropriate reperfusion therapy, either PCI or fibrinolytic therapy, based on a realistic time estimate of door to balloon opening versus administration of fibrinolytic therapy within 30 minutes after presentation as a standard. Establishing a standardized approach to data collection and continuous quality improvement processes
50
75
100
125
150
175
200
225
250
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
Min
utes
(M
edia
n)
233
Non-transfer-in
Transfer-in
Year of Discharge
113
162
99
DANAMI Transfer = 110 minutes
Figure 3. Median door-to-balloon times (minutes) for patients undergoing intervention from 1994-2004, by transfer status in the NRMI database. Adapted with permission from Nallamothu BK, Bates ER, Herrin J et al. Times to treatment in transfer patients undergoing primary percutaneous coronary intervention in the United States: National Registry of Myocardial Infarction (NRMI) ¾ analysis. Circulation 2005; 111:761-767.
05
1015202530354045
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004
Pe
rce
nt
of P
atie
nts
33.1%
41%
Year of Discharge
3.9% 5.4%
Non-transfer
Transfer
Figure 4. Door-to-balloon time ≤ 90 minutes by transfer status undergoing intervention from 1994-2004 in NRMI database. Adapted with permission from Nallamothu BK, Bates ER, Herrin J et al. Times to treatment in transfer patients undergoing primary percutaneous coronary intervention in the United States: National Registry of Myocardial Infarction (NRMI) 3/4 analysis. Circulation 2005; 111:761-767.

2121w w w . e m c r e g . o r g
ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION (STEMI):DECREASING THE TIME TO TREATMENT IN THE ED
is essential for evaluation of the system. Each institution should have regular meetings of its STEMI team to evaluate the significant data points for its STEMI patients including 1) time to receiving ECG (% 10 minutes of less), 2) administration of adjunctive therapy including aspirin, beta-blockers, heparin/low molecular weight heparin, clopidogrel, and glycoprotein IIb/IIIa receptor inhibitors, 3) door to administration of intravenous fibrinolytic therapy (% 30 minutes or less), and 4) door to balloon time for patients receiving primary PCI (% 90 minutes or less). Candid appraisal of these treatment approaches with discussion of outlying patients through a continuous quality improvement effort will ensure optimal care for an institution’s STEMI patients.38,39
Door to Balloon (D2B) InitiativeDuring the 206 American Heart Association meeting in Chicago (November, 2006), the American College of Cardiology announced the D2B (Door to Balloon) initiative.40 The ACC is challenging institutions to have greater than 75% of patients having a door to balloon time of less than 90 minutes. For this to be accomplished, it is imperative that the ED has efficient care plans for patients with STEMI that includes early 12-lead ECG acquisition so emergency physicians can call in the cardiac catheterization team for a rapid response including notification of the interventional cardiologist. Clearly this strategy will emphasize the importance of improving time to treatment by highlighting the 90 minute door to balloon goal on every STEMI patient. As importantly, for patients with STEMI that have no chance of receiving PCI close to the 90 minute standard, routine use of intravenous fibrinolytic therapy should be considered.
REFERENCES1. Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for
the management of patients with ST-elevation myocardial infarction: executive summary: a report of the ACC/AHA Task Force on Practice Guidelines (Committee to Revise the 1999 Guidelines on the Management of Patients with AMI). Circulation 2004; 110:1-49.
2. Gruppo Italiano per lo Studio della Streptochinasi nell’Infarto miocardico (GISSI). Effectiveness of intravenous thrombolytic treatment in acute myocardial infarction. Lancet 1986; 1:397-402.
3. Intravenous Streptokinase in Acute Myocardial Infarction (ISAM) Study Group. A prospective trial of intravenous streptokinase in acute myocardial infarction (ISAM). Mortality, morbidity, and infarct size at 21 days. N Engl J Med 1986; 314:1465-1471.
4. APSAC Intervention Mortality Study (AIMS) Trial Study Group. Effects of intravenous APSAC on mortality after AMI: preliminary report of a placebo-controlled clinical trial. Lancet 1988; 1:545-549.
5. Second International Study of Infarct Survival (ISIS-2) Collaborative Group. Randomised trial of intravenous streptokinase, oral aspirin, both, or neither among 17,187 cases of suspected acute myocardial infarction: ISIS-2. Lancet 1988; 2:349-360.
6. Wilcox RG, von der Lippe G, Olsson CG, et al. Anglo-Scandinavian Study of Early Thrombolysis (ASSET) Study Group. Trial of tissue plasminogen activator for mortality reduction in acute myocardial infarction. Lancet 1988; 2:525-530.
7. Third International Study of Infarct Survival (ISIS-3) Collaborative Group. ISIS-3: a randomised comparison of streptokinase vs tissue plasminogen activator vs anistreplase and of aspirin plus heparin vs aspirin alone among 41,299 cases of suspected acute myocardial infarction. Lancet 1992; 339:753-770.
8. Estudio Multicentrico Estreptoquinasa Republicas de America del Sur (EMERAS) Collaborative Group. Randomized trial of late thrombolysis in patients with suspected acute myocardial infarction. Lancet 1993; 342:767-772.
9. LATE Study Group. Late Assessment of Thrombolytic Efficacy (LATE) study with alteplase 6-24 hours after onset of acute myocardial infarction. Lancet 1993; 342:759-766.
10. Fibrinolytic Therapy Trialists (FTT) Collaborative Group. Indications for fibrinolytic therapy in suspected acute myocardial infarction: collaborative overview of early mortality and major morbidity results from all randomised trials of more than 1,000 patients. Lancet 1994; 343:311-322.
11. Terkelsen CJ, Lassen JF, Norgaard BL, et al. Are we underestimating the full potential of early thrombolytic treatment in patients with acute myocardial infarction? Heart 2003; 89:483-484.
12. Fesmire FM, Brady WJ, Han S, et al. Clinical Policy: Indications for Reperfusion Therapy in Emergency Department Patients with Suspected Acute Myocardial Infarction. Ann Emerg Med 2006; 48:358-371.
13. The GUSTO Investigators. An international randomized trial comparing four thrombolytic strategies for acute myocardial infarction. N Engl J Med 1993; 329:673-682.
14. Morrow DA, Antman EM, Sayah A, et al. Evaluation of the time saved by prehospital initiation of reteplase for ST-elevation myocardial infarction: results of the Early Retavase Thrombolysis in Myocardial Infarction (ER-TIMI) 19 Trial. J Am Coll Cardiol 2002; 40:71-77.

22w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
Copyright EMCREG-International, 2007
15. Topol EJ, for the GUSTO V Investigators: Reperfusion therapy for acute myocardial infarction with thrombolytic therapy and platelet glycoprotein IIb/IIIa inhibition: the GUSTO V randomised trial. Lancet 2001; 357:1905-1914.
16. Assessment of the Safety and Efficacy of a New Thrombolytic (ASSENT-2) Investigators. Single-bolus tenecteplase compared with front-loaded alteplase in acute myocardial infarction: the ASSENT-2 double-blind randomized trial. Lancet 1999; 354:716-722.
17. Boersma E, Maas AC, Deckers JW, et al. Early thrombolytic treatment in acute myocardial infarction: reappraisal of the golden hour. Lancet 1996; 348:771-775.
18. Rogers WJ, Dean LS, Moore PB, et al. Comparison of primary angioplasty versus thrombolytic therapy for acute myocardial infarction. Alabama Registry of Myocardial Ischemia Investigators. Am J Cardiol 1994; 74:111-118.
19. Tiefenbrunn AJ, Chandra NC, French WJ, et al. Clinical experience with primary percutaneous transluminal coronary angioplasty compared with alteplase (recombinant tissue-type plasminogen activator) in patients with acute myocardial infarction: a report from the Second National Registry of Myocardial Infarction (NRMI-2). J Am Coll Cardiol 1998; 31:1240-1245.
20. Rogers WJ, Canto JG, Barron HV, et al. Treatment and outcome of myocardial infarction in hospitals with and without invasive capability. Investigators in the National Registry of Myocardial Infarction. J Am Coll Cardiol 2000; 35:371-379.
21. Cannon CP, Gibson CM, Lambrew CT, et al. Relationship of symptom-onset-to-balloon time and door-to-balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA 2000; 283:2941-2947.
22. Berger PB, Ellis SG, Holmes DR, et al. Relationship between delay in performing direct coronary angioplasty and early clinical outcome in patients with acute myocardial infarction: results from the Global Use of Strategies to Open Occluded Arteries in Acute Coronary Syndromes (GUSTO-IIb) trial. Circulation 1999; 100:14-20.
23. Andersen HR, Nielsen TT, Rasmussen K, et al. DANAMI-2 Investigators. A comparison of coronary angioplasty with fibrinolytic therapy in acute myocardial infarction. N Engl J Med. 2003; 349:733-742.
24. Nallamothu BK, Bates ER, Herrin J et al. Times to treatment in transfer patients undergoing primary percutaneous coronary intervention in the United States: National Registry of Myocardial Infarction (NRMI) 3/4 analysis. Circulation 2005; 111:761-767.
25. Nallamothu BK, Bates ER. PCI versus fibrinolytic therapy in acute myocardial infarction: is timing (almost) everything? Am J Cardiol 2003; 92:824-826.
26. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised trials. Lancet 2003; 361:13-20.
27. Rawles JM. Quantification of the benefit of earlier thrombolytic therapy: five-year results of the Grampian Region Early Anistreplase Trial (GREAT). J Am Coll Cardiol 1997; 30:1181-1186.
28. Goldberg RJ, Mooradd M, Gurwitz JH et al. Impact of time to treatment with tissue plasminogen activator on morbidity and mortality following acute myocardial infarction (The second National Registry of Myocardial Infarction – NRMI). Am J Cardiol 1998;82:259-64.
29. De Luca G, Suryapranata H, Zijlstra F, et al. Symptom-onset-to balloon time and mortality in patients with acute myocardial infarction treated by primary angioplasty. J Am Coll Cardiol 2003; 42:991-997.
30. De Luca G, Suryapranata H, Ottervanger JP, et al. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: every minute of delay counts. Circulation 2004; 109:1223-1225.
31. Antoniucci D, Valenti R, Migliorini A, et al. Relation of time to treatment and mortality in patients with acute myocardial infarction undergoing primary coronary angioplasty. Am J Cardiol 2002; 89:1248-1252.
32. Brodie BR, Stuckey TD, Muncy DB, et al. Importance of time-to reperfusion in patients with acute myocardial infarction with and without cardiogenic shock treated with primary PCI. Am Heart J 2003; 145:708-715.
33. Juliard JM, Feldman LJ, Golmard JL, et al. Relation of mortality of primary angioplasty during acute myocardial infarction to door-to- Thrombolysis in Myocardial Infarction (TIMI) time. Am J Cardiol 2003; 91:1401-1405.
34. Betriu A, Masotti M. Comparison of mortality rates in acute myocardial infarction treated by PCI versus fibrinolysis. Am J Cardiol 2005; 95:100-101.
35. Grines C, Patel A, Zijlstra F et al. PCAT Collaborators. Percutaneous transluminal coronary angioplasty. Primary coronary angioplasty compared with intravenous thrombolytic therapy for acute myocardial infarction: six-month follow up and analysis of individual patient data from randomized trials. Am Heart J 2003; 145:47-57.
36. Widimsky P, Budesinsky T, Vorac D, et al. Long distance transport for primary angioplasty vs immediate thrombolysis in acute myocardial infarction. Final results of the randomized national multicentre trial – PRAGUE-2. Eur Heart J 2003; 24:94-104.
37. Kosowsky JM. Thrombolysis for ST-Elevation myocardial infarction in the emergency department. Crit Pathways in Cardiol 2006; 5:141-146.
38. Bradley EH, Herrin J, Wang W et al. Strategies for reducing door-to-balloon time in acute myocardial infarction. N Engl J Med 2006; 355:1-13.
39. Moscucci M, Eagle KA. Reducing the door-to-balloon time for myocardial infraction with ST-segment elevation. N Engl J Med 2006; 355:1-2.
40. Nissen SE. GAP-D2B: An Alliance for Quality. J Am Coll Cardiol 2006; 48:1911-1912.

23w w w . e m c r e g . o r g
NOVEL ANTI-THROMBOTIC THERAPIES FOR ACUTE CORONARY SYNDROME: DIRECT THROMBIN INHIBITORS
NOVEL ANTI-THROMBOTIC THERAPIES FOR ACUTE CORONARY SYNDROME: DIRECT THROMBIN INHIBITORS
Judd E. Hollander, MDProfessor, Clinical Research Director, Department of Emergency Medicine
University of Pennsylvania School of Medicine, Philadelphia, Pennsylvania
OBJECTIVES:1. Discuss the concept of net clinical benefit.
2. Describe the role of direct thrombin inhibitors in patients with non-ST-segment elevation acute coronary syndrome.
3. Discuss the role of the ACUITY study in determining the optimal anti-thrombin for use in ED patients with non-ST-segment elevation acute coronary syndrome.
INTRODUCTIONUnfractionated heparin (UFH), low molecular weight heparin (LMWH), thienopyridines (clopidogrel), and glycoprotein (GP) IIb/IIIa inhibitors are class I guideline recommendations from the most recent American College of Cardiology/American Heart Association (ACC/AHA) guidelines for the management of patients with non-ST-segment elevation acute coronary syndromes (ACS).1 The use of enoxaparin (a LMWH), rather than UFH, has decreased ischemic complications in patients with ACS who are treated conservatively.2,3 Reductions in both early and late composite of death and myocardial infarction (MI) are enhanced with early addition of clopidogrel4-6 and a GP IIb/IIIa inhibitor7-9 to unfractionated heparin (UFH) and aspirin in patients with ACS. Several trials10-12 have established early invasive management as the optimal treatment for patients with moderate-to high-risk ACS and the guidelines have endorsed this approach.1 An early invasive strategy consists of early initiation of
anti-thrombotic and anti-platelet therapy, angiographic assessment within 48 hours, followed by definitive therapy tailored to each patient’s coronary anatomy.
The ideal anti-thrombotic regimen for patients with ACS should facilitate an early invasive strategy (including percutaneous coronary intervention [PCI] or coronary artery bypass graft [CABG] surgery, if appropriate); should provide maximal protection from adverse ischemic events; should minimize the risk of hemorrhagic complications; enable more simplified (or emergency department [ED] friendly) treatment pathways; and should be cost-effective.
New considerations in trial design: Inclusion of Bleeding ParametersTraditionally, hard outcomes, such as death were considered the ideal outcome parameter for large scale clinical trials. However, improved treatment modalities have resulted in improved outcomes and a reduction in the frequency of death,
The ideal anti-thrombotic regimen for patients with ACS should facilitate an early invasive strategy
(including percutaneous coronary intervention or coronary artery
bypass graft surgery, if appropriate); should
provide maximal protection from adverse ischemic events; should minimize the risk of hemorrhagic
complications; enable more simplified (or ED friendly) treatment pathways; and should be cost-effective.

24w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
24
such that it is no longer practical as a sole outcome measurement, even in clinical trials with over 10,000 patients. The incremental improvement in mortality is too small to be detected, even with these large trials. Therefore, contemporary studies have used composite efficacy endpoints, comprised of patients that attain any of a combination of outcomes, typically, mortality, myocardial infarction and refractory ischemia (possibly defined by urgent target vessel revascularization). Recently, a new composite has been defined: net clinical benefit, which includes a triple composite efficacy parameter as well as major bleeding complications. The rationale is that short term bleeding complications are associated with worse long term outcomes.13 Likewise, the need for blood transfusions is associated with increased 30 day mortality even after adjustment for risk factors.14 It makes sense that the ideal anti-thrombotic therapy should minimize short term bleeding risk to optimize long term outcome.
Anti-thrombinsThrombin is the most potent natural platelet activator.15 Thrombin converts fibrinogen to fibrin, activates coagulation factors V and VIII, accelerates coagulation, stimulates its own generation, and interacts with endothelial cells to upregulate tissue factor.15-19 Thrombin is pivotal link in the process of tissue injury, coagulation, and the platelet response (Figure 1).
Unfractionated heparin, enoxaparin, and fondaparinux are considered indirect thrombin inhibitors because they require binding with circulating anti-thrombin III (an endogenous circulating alpha-globulin) to exert their anticoagulant affect. In contrast to UFH and LMWH, direct thrombin inhibitors interact with circulating and clot-bound thrombin.20
Bivalirudin, a direct thrombin inhibitor, binds specifically to thrombin at its active catalytic site and at the exosite-1 docking locus.21 Bivalirudin competitively inhibits thrombin with high affinity but is a short-acting agent, with a half-life of only 25 minutes (compared with 60 to 90 minutes with UFH).20,22 It does not require laboratory monitoring due to predictable linear pharmacokinetics.
New Clinical DataSince the publication of the 2002 AHA/ACC guidelines for the management of patients with NSTEMI, there have been 3 large pivotal trials regarding anti-thrombin therapy: SYNERGY, OASIS-5, and ACUITY.23-25 SYNERGY demonstrated that enoxaparin was non-inferior to UFH, with death and MI occurring in 14.0% (n = 696) and 14.5% (n = 722), respectively (hazard ratio 0.96; 95% CI = 0.86-1.06). There was a slight excess in bleeding in the enoxaparin group.23 In OASIS-5 (The Organization
Tissue factor
Plasma clottingcascade
Prothrombin
Thrombin
Fibrinogen Fibrin
Thrombus
Platelet aggregation
Platelet activation
Collagen
Thromboxane A2
ADP
AT
Aspirin
TiclopidineClopidogrel
Prasugrel (TIMI-38)Cangrelor (IV)
EptifibatideAbciximabTirofiban(GPI)
Bivalirudin
FactorXa
LMWHHeparin
Thrombolytics
Fondaparinux
AT
AT
Figure 1. The pivotal role of thrombin in the
process of tissue injury, coagulation, and the
platelet response. AT=anti-thrombin III
GPI=glycoprotein IIb/IIIa inhibitors

2525w w w . e m c r e g . o r g
NOVEL ANTI-THROMBOTIC THERAPIES FOR ACUTE CORONARY SYNDROME: DIRECT THROMBIN INHIBITORS
to Assess Strategies in Acute Ischemic Syndromes) fondaparinux (2.5mg SQ qd) was compared to enoxaparin (1 mg/kg SQ BID) in 20,078 unstable angina or NSTEMI patients with respect to a primary endpoint representing net clinical benefit.24 This net clinical endpoint was a composite of death, myocardial infarction, and refractory ischemia combined with major bleeding. OASIS-5 found no difference in the efficacy endpoint (fondaparinux, 5.8% versus enoxaparin, 5.9%), however the net clinical benefit outcome favored fondaparinux (hazard ratio, 0.81 (95% CI 0.74-0.90). This benefit was due to reduced major bleeding.
The Path to ACUITY: bivalirudinBivalirudin has been extensively investigated in patients undergoing PCI. In the Bivalirudin Angioplasty Trial,26,27 4312 patients receiving PCI were randomized to bivalirudin or UFH without GP IIb/IIIa inhibitor use. The bivalirudin-treated patients showed lower rates of ischemic events and hemorrhage.26-29 A 30% to 60% reduction in ischemic complications (P < .01) and 60% to 80% reduction in bleeding (P < .001) were noted in the 1006 unstable angina patients and the 741 patients following acute myocardial infarction. This trial predated the use of stents, GP IIb/IIIa inhibitors, and thienopyridines, and relatively high UFH doses were used in the control arm.
Since the publication
of the 2002 AHA/
ACC guidelines for
the management
of patients with
NSTEMI, there have
been 3 large pivotal
trials regarding
anti-thrombin therapy:
SYNERGY, OASIS-5,
and ACUITY.
A more contemporary study was performed in the Randomized Evaluation of PCI Linking Bivalirudin to Reduce Clinical Events (REPLACE)-2 trial.30 REPLACE-2 randomized 6010 patients undergoing stent implantation to UFH and planned GP IIb/IIIa inhibition versus bivalirudin and provisional GP IIb/IIIa inhibition (which was used in only 7.2% of patients). The 30-day composite net clinical benefit (death, MI, urgent repeat revascularization, and major bleeding) was similar between the two groups (10.0% with UFH + routine GP IIb/IIIa inhibition vs 9.2% with bivalirudin and provisional GP IIb/IIIa inhibition, P = .32), as was the rate of death, MI, and urgent revascularization (7.1% vs 7.6%, respectively, P = .40). Major bleeding was less common in the bivalirudin patients (4.1% vs 2.4%, P < .001).30 These studies demonstrated the utility of bivalirudin in the cardiac catheterization laboratory during angioplasty. It should be noted that the results were similar in the most ED relevant group: the 1340 REPLACE-2 patients who presented with ACS.
The Acute Catheterization and Urgent Intervention Triage strategY (ACUITY) trial was a large-scale, prospective, multicenter, randomized study designed to determine the optimal anticoagulation regimen in patients with moderate to high-risk ACS undergoing an early invasive strategy.25 In ACUITY, heparin (either UFH or enoxaparin) and bivalirudin, with or without an upstream GP IIb/IIIa inhibition, was compared to bivalirudin alone in high-risk NSTEMI ACS patients

26w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
26
Moderate-high risk
ACS
UFH orEnoxaparin+ GP IIb/IIIa
Bivalirudin+ GP IIb/IIIa
Bivalirudinalone
An
gio
gra
ph
y w
ith
in 7
2 h
ou
rs Medicalmanagement
PCI
CABG
R*
• Aspirin in all• Clopidogrel dosing and timing per local practice
Figure 2. ACUITY study design in high-risk NSTEMI ACS patients treated with a planned early interventional strategy.
treated with a planned early interventional strategy (Figure 2).25 An important secondary objective was to examine clinical outcomes after GP IIb/IIIa inhibition given upstream (before angiography) versus selective use of GP IIb/IIIa inhibition in patients undergoing PCI only.
The results of ACUITY, which were released at the American College of Cardiology Late Breaking Clinical Trials session in March of 2006, demonstrate the beneficial effects of bivalirudin on net clinical benefit (composite of death, AMI, urgent revascularization and major bleeding), predominantly due to reduction in major bleeding. The net clinical benefit endpoint favored bivalirudin monotherapy (10.1%) over heparin with or without upstream GP IIb/IIIa inhibition (11.7%), and bivalirudin with or without upstream GP IIb/IIIa inhibition (11.8%). The precise role of bivalirudin in the ED will be defined, as ACUITY is further analyzed to determine if ED administration is associated with improved outcomes.
The View From the Emergency DepartmentMost emergency physicians are primarily concerned with minimizing the risk of early adverse ischemic outcomes and are inherently less likely to be concerned about procedural complications. On the other hand, interventional cardiologists are also concerned about procedure complications and post-procedure bleeding. Therefore, it is not surprising that emergency physicians and cardiologists might choose different therapies given the same patient. The SYNERGY trial demonstrated that consistent therapy (not changing between UFH and LMWH in either direction) is associated with an improved outcome. The optimum anti-thrombin should enable a seamless transition from the ED to the cardiac catheterization laboratory. It should minimize pre-procedural ischemia and both peri- and post-procedural ischemic and bleeding outcomes, be easy to administer, require no monitoring, and be cost effective. The preliminary data from ACUITY suggest that bivalirudin has improved net clinical benefit. However, several questions remain unanswered: (1) Does
starting bivalirudin in the ED, when a patient may or may not receive cardiac catheterization, improve outcomes? (2) In patients who will receive an intervention, is there additional benefit to beginning upstream bivalirudin in the ED or should administration wait until catheterization? Further analysis of the ACUITY trial might help answer these and other questions, was well as determine whether patients benefit from having this therapy initiated in the ED.

2727w w w . e m c r e g . o r g
NOVEL ANTI-THROMBOTIC THERAPIES FOR ACUTE CORONARY SYNDROME: DIRECT THROMBIN INHIBITORS
REFERENCES
1. Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA 2002 guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Unstable Angina). 2002. Available at: http://www.acc.org/clinical/guidelines/unstable/incorporated/index.htm.
2. Cohen M, Demers C, Gurfinkel EP, et al., A comparison of low-molecular-weight heparin with unfractionated heparin for unstable coronary artery disease. N Engl J Med 1997;337:447–452.
3. Antman EM, McCabe CH, Gurfinkel EP, et al., Enoxaparin prevents death and cardiac ischemic events in unstable angina/non–Q-wave myocardial infarction. Circulation 1999;100:1593–1601.
4. Yusuf S, Zhao F, Mehta SR, et al., Effects of clopidogrel in addition to aspirin in patients with acute coronary syndromes without ST-segment elevation. N Engl J Med 2001;345:494–502.
5. Mehta SR, Yusuf S, Peters RJ, et al., Effects of pretreatment with clopidogrel and aspirin followed by long-term therapy in patients undergoing percutaneous coronary intervention. Lancet 2001;358:527–533.
6. Steinhubl SR, Berger PB, Mann JT, et al., Early and sustained dual oral anti-platelet therapy following percutaneous coronary intervention: a randomized controlled trial. JAMA 2002;288:2411–2420.
7. PRISM-PLUS Study Investigators, Inhibition of the platelet glycoprotein IIb/IIIa receptor with tirofiban in unstable angina and non–Q-wave myocardial infarction. N Engl J Med 1998;338:1488–1497.
8. PURSUIT Trial Investigators, Inhibition of platelet glycoprotein IIb/IIIa with eptifibatide in patients with acute coronary syndromes. N Engl J Med 1998;339:436–443.
9. Boersma E, Harrington RA, Moliterno DJ, et al., Platelet glycoprotein IIb/IIIa inhibitors in acute coronary syndromes: a meta-analysis of all major randomised clinical trials. Lancet 2002;359:189–198.
10. Cannon CP, Weintraub WS, Demopoulos LA, et al., Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med 2001;344:1879–1887.
11. FRISC II Investigators, Invasive compared with non-invasive treatment in unstable coronary-artery disease. Lancet 1999;354:708–715.
12. Fox KA, Poole-Wilson PA, Henderson RA, et al., Interventional versus conservative treatment for patients with unstable angina or non-ST-elevation myocardial infarction. Lancet 2002;360:743–751.
13. Rao SV, O’Grady K, Pieper K, et al. Impact of bleeding severity on clinical outcomes among patients with acute coronary syndromes. Am J Cardiol 2005;96:1200-6.
14. Rao SV, Jollis JG, Harrington RA, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes. JAMA 2004;292:1555-62.
15. Ashby CR, Daniel JL, Kunapuli SP and Smith JB, Platelet stimulatory and inhibitory receptors. In: R.W. Colman, Editor, Hemostasis and Thrombosis (4th edition.), Lippincott Williams & Wilkins, Philadelphia, Pa (2001), pp. 505–520.
16. Mann KG, Biochemistry and physiology of blood coagulation. Thromb Haemost 1999;82:165–174.
17. Brummel KE, Paradis SG, Butenas S, Mann KG, Thrombin functions during tissue factor–induced blood coagulation release and factor XIII activation. Blood 2002:100:148–152.
18. Monroe DM, Hoffman M, Roberts HR. Platelets and thrombin generation. Arterioscler Thromb Vasc Biol 2002;22:1381–1389.
19. Colman R, Clowes A, James G. Overview of hemostasis. In: R.W. Colman, Editor, Hemostasis and Thrombosis (4th edition.), Lippincott Williams & Wilkins, Philadelphia, PA (2001), pp. 3–16.
20. Eikelboom J, White H, Yusuf S. The evolving role of direct thrombin inhibitors in acute coronary syndromes. J Am Coll Cardiol 2003;41suppl:70S–78S.
21. Weitz JI, Bates ER. Direct thrombin inhibitors in cardiac disease. Cardiovasc Toxicol 2003;3:13–25.
22. Maraganore JM, Adelman BA. Hirulog: a direct thrombin inhibitor for management of acute coronary syndromes. Coron Artery Dis 1996;7:438–448.
23. Ferguson JJ, Califf RM, Antman EM, et al., Enoxaparin vs unfractionated heparin in high-risk patients with non-ST-segment elevation acute coronary syndromes managed with an intended early invasive strategy: primary results of the SYNERGY randomized trial. JAMA 2004;229:45–54.
24. The Fifth Organization to Assess Strategies in Acute Ischemic Syndromes Investigators (OASIS-5). Comparison of fondaparinux and enoxaparin in acute coronary syndromes. N Engl J Med., 2006;354(14), 1464-1476.
25. Stone GW, Bertrand M, Colombo A, et al. Acute Catheterization and Urgent Intervention Triage strategY (ACUITY) trial: Study design and rationale. American Heart Journal 2004;148:764-75.
26. Bittl JA, Chaitman BR, Feit F, et al., Bivalirudin versus heparin during coronary angioplasty for unstable or postinfarction angina. Am Heart J 2001;142:952–959.
27. Henry TD. Overcoming heparin limitations in high-risk percutaneous coronary intervention: the alternative strategy: replacing heparin with bivalirudin. J Invasive Cardiol 2002;(14 suppl B):19B–29B.
28. Bittl JA, Strony J, Brinker JA, et al., Treatment with bivalirudin (hirulog) as compared with heparin during coronary angioplasty for unstable or postinfarction angina. N Engl J Med 1995;333:764–769.
29. Bittl JA, Feit F. A randomized comparison of bivalirudin and heparin in patients undergoing coronary angioplasty for postinfarction angina. Am J Cardiol 1998;82: 43P–49P.
30. Lincoff AM, Bittl JA, Harrington RA, et al., Bivalirudin and provisional glycoprotein IIb/IIIa blockade compared with heparin and planned glycoprotein IIb/IIIa blockade during percutaneous coronary intervention. JAMA 2003;289:853–863.
Copyright EMCREG-International, 2007

28
MANAGEMENT OF ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION IN THE ED: STATE-OF-THE-ART ANTI-PLATELET AND ANTI-THROMBOTIC THERAPY
James W. Hoekstra, MDProfessor and Frederick Glass Chairman of Emergency Medicine
Wake Forest University Health Sciences, Winston Salem, NC
OBJECTIVES:1. Participants should understand the ACC/AHA guidelines for the treatment of ST-segment elevation myocardial
infarction (STEMI).2. Participants should understand the clinical trial evidence and rationale behind aspirin and clopidogrel use in the
treatment of STEMI.3. Participants should understand the clinical trial data supporting the use of enoxaparin in STEMI.4. Participants should understand the clinical trial data supporting the early use of glycoprotein IIb/IIIa inhibitors
upstream in the ED, prior to primary percutaneous intervention in STEMI.
INTRODUCTIONST-segment elevation myocardial infarction (STEMI) remains one of the most important disease entities treated by emergency physicians. When minutes count, and time is muscle, emergency physicians can have a crucial impact on patient morbidity and mortality by providing appropriate therapy in a time-efficient manner. The recently published American College of Cardiology/American Heart Association (ACC/AHA) Guidelines for the treatment of STEMI outline the recommendations for the emergency department (ED) management of STEMI, including anti-ischemic, anti-thrombotic, and fibrinolytic versus catheter-based reperfusion therapy (Table 1).1 These guidelines were promulgated in an effort to standardize and optimize the evaluation, diagnosis, and management of patients with STEMI and to provide physicians with a framework for clinical decision-making. They have become the cornerstone of many ED protocols for the treatment of STEMI which are crucial to providing efficient care in the ED and seamless transition for our patients
to the cardiac cardiac catheterization laboratory or coronary care unit (CCU). Within a few months after the ACC/AHA STEMI Guidelines publication, however, new clinical trials data were released and published which added significantly to our knowledge of the treatment of STEMI, confirmed some of the STEMI Guidelines recommendations, and provided valuable adjuncts to giving optimal care for STEMI in the emergency setting, beyond the Guidelines recommendations. Specifically, new clinical trials data support the use clopidogrel, enoxaparin, and earlier administration of GP IIb/IIIa inhibitor therapy in the management of STEMI. Whether or not these new developments will be adopted into the next version of the Guidelines, or into routine clinical care, remains to be seen. The intent of this paper is to critically review some of these recent clinical trials involving anti-platelet agent and anti-thrombin use in STEMI.
Anti-platelet Therapy in STEMIThe pathophysiology of STEMI is
The recently published American College of Cardiology/American
Heart Association (ACC/AHA) Guidelines
for the treatment of STEMI outline the
recommendations for the emergency department management of STEMI, including anti-ischemic, anti-thrombotic, and
fibrinolytic versus catheter-based
reperfusion therapy.
28w w w . e m c r e g . o r g

29w w w . e m c r e g . o r g
MANAGEMENT OF ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION IN THE ED: STATE-OF-THE-ART ANTI-PLATELET AND ANTI-THROMBOTIC THERAPY
initiated by the endothelial rupture of an atherosclerotic coronary artery plaque. Plaque rupture leads to platelet aggregation, platelet activation, fibrin deposition, and downstream myocardial ischemia and necrosis after complete coronary artery occlusion. Anti-platelet agents, including aspirin and glycoprotein IIb/IIIa receptor blockers (GPI) have all been investigated in this group of patients in large multicenter clinical trials, and these therapies have been incorporated as Class I recommendations in the ACC/AHA Guidelines.1 Specifically, aspirin 325 mg p.o. is indicated at patient presentation regardless of the reperfusion strategy, while GPIs are indicated in the cardiac catheterization laboratory as an adjunct to primary percutaneous intervention (PCI) as a reperfusion strategy.
Clopidogrel in STEMI: Results of the CLARITY and COMMIT TrialsClopidogrel is an oral anti-platelet agent that binds to platelets at the P
2Y
12 site, and
inhibits platelet activation through the ADP-mediated pathway. The ACC/AHA Guidelines for Non-ST-segment elevation ACS recommend that clopidogrel 300 mg p.o. loading dose, and 75 mg per day, be given at patient presentation and continued for at least a month and then up to a year post discharge from the hospital.2 The 2004 ACC/AHA STEMI Guideline recommendations do not, however, include clopidogrel therapy. The recently completed CLARITY trial investigated the effectiveness of a 300 mg loading dose of clopidogrel, in conjunction with fibrinolytic therapy, in the treatment of STEMI.3 The CLARITY trial randomized 3491 STEMI patients to
clopidogrel 300 mg load, and 75 mg per day versus placebo, initiated in the ED. The primary outcome of death, MI, and target vessel occlusion at angiography was reduced 36% (p=0.00000036) in the clopidogrel group (Figure 1), offset by only a 0.3% increase in bleeding. Death, MI and recurrent ischemia at 30 days were reduced 20% with clopidogrel (p=0.026). In the patients who went on to PCI after their initial fibrinolytic therapy, there was a 46% reduction in death, MI, and stroke in the patients treated with clopidogrel (p=0.008). These results were further supported by the COMMIT trial, which randomized almost 46,000 STEMI patients (recruited in Asia) who were treated with fibrinolytics or medical management, to 75 mg qd (no loading dose) of clopidogrel versus placebo.4 In the COMMIT trial, clopidogrel was associated with a 9% relative reduction in death, recurrent MI, and stroke (p=0.002) (Figure 2). The results of CLARITY and COMMIT are so strikingly supportive of the use of clopidogrel in the ED management of STEMI, with minimal side effects, that many practitioners have already added clopidogrel to their STEMI protocols.
Plaque rupture leads
to platelet aggregation,
platelet activation,
fibrin deposition, and
downstream myocardial
ischemia and necrosis
after complete coronary
artery occlusion.
AHA/ACC Guidelines Class I recommended ED pharmacologic and reperfusion therapy in STEMI.
• Targeted ED Protocol and Collaboration• O2, IV, monitor• Aspirin immediately (162-325 mg)• Nitrates, beta blockers (IV)• Heparin weight based dosing (60 U IV bolus and 12 U/kg/
hour infusion; maximum 4000 U total bolus/1000 U infusion)• Fibrinolytics in less than 30 minutes (esp if
chest pain <3 hours) • PCI less than 90 minutes if available• Treatment of Complications
Table 1.

30w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
30
Figure 1. Primary results of the CLARITY trial: Reduction in death, MI, and occluded infarct related artery with clopidogrel and fibrinolytic therapy initiated in the ED.
The results of CLARITY
and COMMIT are so
strikingly supportive of
the use of clopidogrel
in the ED management
of STEMI, with minimal
side effects, that
many practitioners
have already added
clopidogrel to their
STEMI protocols.
Figure 2. Results of the COMMIT trial. Reduction in ischemic outcomes in STEMI patients treated with clopidogrel.
Figure 3. Results of the EXTRACT TIMI-25 Trial: Comparison of enoxaparin to unfractionated heparin, in conjunction with fibrinolytic therapy, in STEMI
Enoxaparin versus Unfractionated Heparin in STEMIThe ACC/AHA STEMI Guidelines recommend the administration of unfractionated heparin in the ED, either in conjunction with fibrinolytic therapy or in preparation for primary PCI. These same guidelines give enoxaparin a
IIb recommendation as a substitute for heparin in conjunction with fibrinolytic therapy, in the absence of renal failure or age greater
than 75 years. The recently presented EXTRACT TIMI-25 trial compared enoxaparin (30mg IVP, and 1 mg/kg given subcutaneously) to unfractionated heparin (weight based dosing) in 20,478 patients treated with a variety of fibrinolytics for STEMI.5 The trial was a double-blind, double-dummy design, carried out mostly in Europe. The primary outcome of death and MI at 30 days was reduced 17% (p<0.0001) in patients treated with enoxaparin versus heparin (Figure 3). Bleeding was increased 2% in the enoxaparin treated patients, but the intracranial hemorrhage rate was not significantly different. The new dosing strategy of enoxaparin 0.75 mg subcutaneously in patients greater than 75 years old eliminated an increased risk of intracranial hemorrhage compared to heparin in that population. The results of the EXTRACT TIMI-25 PCI cohort were presented at the European Society of Cardiology in September, 2006.6 This subset analysis of EXTRACT analyzed PCI outcomes in 4676 EXTRACT patients who underwent PCI for a variety of indications in the 30 days post fibrinolytic therapy. In the enoxaparin treated patients, the primary outcome of death and MI
at 30 days was reduced 23% (p<0.001), with no increase in bleeding. Ischemic strokes were seen three times more often in the heparin treated

3131w w w . e m c r e g . o r g
MANAGEMENT OF ST-SEGMENT ELEVATION MYOCARDIAL INFARCTION IN THE ED: STATE-OF-THE-ART ANTI-PLATELET AND ANTI-THROMBOTIC THERAPY
patients (p=0.006). The results were consistent in those patients treated early in their hospitalization, on blinded study drug through treatment with PCI. It appears from EXTRACT that enoxaparin is preferable to unfractionated heparin in STEMI patients treated with fibrinolytic therapy, even if it is followed by PCI.
Facilitated PCI The ACC/AHA STEMI Guidelines give a Class I recommendation to primary PCI as a reperfusion strategy, as long as it can be accomplished expeditiously (<90 minutes door to balloon time) by experienced operators in high volume centers.1 Facilitated primary PCI, which involves the administration of pharmacologic reperfusion therapy prior to planned primary PCI, has been advocated as a method of enhancing the ease of primary PCI and/or preserving myocardial function while awaiting primary PCI. Half-dose fibrinolytics, full-dose fibrinolytics, or GPIs have all been used for facilitated PCI with variable results, mostly in small studies, subanalyses, or single-center reports.7-11 This approach of pre-PCI reperfusion therapy is of special interest to emergency physicians, who often find themselves feeling rather helpless, watching a patient infarct while awaiting activation of the cardiac catheterization laboratory for primary PCI or requiring transfer to a distant hospital offering PCI capability. The use of full-dose fibrinolytics for facilitated PCI has recently come under scrutiny with the results of the ASSENT 4 trial, which had to be prematurely terminated due to an increased in-hospital mortality (p=0.01) and an increased incidence of strokes in
patients treated with full-dose TNK prior to primary PCI.10 Fibrinolytic therapy prior to PCI also resulted in the increased ischemic complications of reinfarction and revascularization. Routine use of fibrinolytics prior to immediate PCI is presently being discouraged.
Early GPI Use in STEMI: The ED versus the Cardiac Catheterization LaboratoryGlycoprotein IIb/IIIa receptor blockers have been given a Class I recommendation for use as an adjunct to primary PCI in STEMI, based on a number of clinical trials, and years of experience.1 Utilization of GPIs in the ED, prior to planned primary PCI, has been less well investigated, despite data demonstrating fairly potent “fibrinolytic” activity with GPI therapy.11 A recent meta-analysis of 931 STEMI patients randomized to ED versus cardiac catheterization laboratory administration of abciximab prior to primary PCI demonstrated improved TIMI-2 or TIMI-3 flow in the infarct related artery with ED administration (OR 1.69, 95% CI
It appears from
EXTRACT that
enoxaparin is
preferable to
unfractionated heparin
in STEMI patients
treated with fibrinolytic
therapy, even if it is
followed by PCI.
1.28-1.22, p<0.001).12 Cutlip et al, in a single-center trial, showed that the early administration of eptifibatide was associated with a similar 43.4% increase in TIMI 2/3 flow at the time of primary PCI.13 Finally, this strategy was more rigorously evaluated in the TITAN TIMI 34 trial, in which 343 patients were randomized to eptifibatide in the ED versus cardiac catheterization laboratory.14 ED administration of eptifibatide was associated with higher TIMI-2/3 flow (p=0.08), greater levels of myocardial tissue perfusion (p=0.026), and higher full angiographic perfusion (p=0.059), with no significant increase in bleeding (Figure 4). Early administration of GPIs in the ED, while awaiting cardiac catheterization laboratory activation and primary PCI, appears to be a viable, effective, and safe alternative to providing no therapy for STEMI. Larger trials are needed to demonstrate more clinically significant benefits on mortality or morbidity with ED GPI administration in STEMI.

32w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
SUMMARYThe CLARITY, COMMIT, EXTRACT, and TITAN TIMI-34 trials are only four examples of the many recent clinical trials involving the care of patients with STEMI. It is important for clinicians to understand the data from these studies, as well as the potential clinical implications, to optimize care for these patients presenting with STEMI.
REFERENCES1. Antman EM, Anbe DT, Armstrong PW, et al: ACC/
AHA guidelines for the management of patients with ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association task force on practice guidelines: Committee to revise the 1999 guidelines for the management of patients with acute myocardial infarction. J Am Coll Cardiol. 2004;44(3):E1-E211.
2. Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA guidelines for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction: executive summary and recommendations: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Patients with Unstable Angina). Circulation 2000;102:1193-1209. 2002 update posted at www.acc.org on March 15, 2002.
Early administration
of GPIs in the ED,
while awaiting cardiac
catheterization
laboratory activation
and primary PCI,
appears to be a viable,
effective, and safe
alternative to providing
no therapy for STEMI.
3. Sabatine MS, Cannon CP, Gibson M, et al. Addition of clopidogrel to aspirin and fibrinolytic therapy for myocardial infarction with ST-segment elevation. N Engl J Med. 2005;352:1179-1189.
4. The COMMIT trial investigators: Addition of clopidogrel to aspirin in 45,852 patients with AMI: a randomized placebo controlled trial. Lancet 2005;366:1607-1621.
5. Antman EM, Morrow DA, McCabe CH, et al: Enoxaparin versus unfractionated heparin with fibrinolysis for ST-segment elevation MI (EXTRACT TIMI 25 trial). N Engl J Med 2006;354:1477-1488.
6. Gibson, et al: EXTRACT TIMI-25 PCI Cohort Study. Presented at the European Society Meeting, September, 2006.
7. Ross AM, Coyne KS, Reiner JS, et al: The PACT trial: A randomized trial comparing primary angioplasty with a strategy of short-acting thrombolysis and immediate planned percutaneous coronary angioplasty. Lancet 1988;1:197-203.
8. Simoons ML, Arnold AE, Betrui A, et al. Thrombolysis with TPA in AMI : No additional benefit from immediate percutaneous coronary angioplasty. Lancet 1988;1:197-203.
9. The TIMI Research Group: TIMI II A: Immediate versus delayed catheterization and angioplasty following thrombolytic therapy for AMI. JAMA 1988;260:2849-2858.
10. Van de Werf F, Ross A, Armstrong P, et al: Primary versus tenecteplase-facilitated PCI in patients with STEMI (the ASSENT-4 Trial). Lancet 2006;367(9510):569-578.
11. Gold HK, Gargedian HD, Dinsmore Re, et al: Restoration of coronary flow in myocardial infarction by intravenous chimeric 7E3 antibody without exogenous tissue plasminogen activators. Circulation 1997;95:1755-9.
12. Montalescot G, Borentain M, Payot L, et al: Early versus late administration of GP IIb/IIIa inhibitors in primary PCI for acute STEMI: A meta analysis. JAMA 2004;292362-366 .
13. Cutlip DE, Ricciardi MJ, Frederick SL, et al: Emergency room administration of eptifibatide before primary angioplasty for STEMI and its effects on coronary blood flow and procedure outcomes. Am J Cardiol 2001;88:62-64.
14. Gibson CM, Kirtane AJ, Murphy SA, et al. . Early initiation of eptifibatide in the emergency department before primary percutaneous coronary intervention for ST-segment elevation myocardial infarction: results of the Time to Integrilin Therapy in Acute Myocardial Infarction (TITAN)-TIMI 34 trial. Am Heart J. 2006 Oct;152(4):668-75.
Figure 4. Results from the TITAN TIMI-34 trial: Full angiographic reperfusion with ED versus catheterization laboratory initiated eptifibatide prior to primary PCI for STEMI.
Copyright EMCREG-International, 2007

33w w w . e m c r e g . o r g
ACUTE DECOMPENSATED HEART FAILURE: NOVEL APPROACHES TO CLASSIFICATION AND TREATMENT
OBJECTIVES:1. Discuss the new and complex pathophysiology of ADHF which consists of multiple types of
heart failure patients with various forms of acute decompensation.2. Discuss the categorization of ADHF patient types by clinical profile and hemodynamic
status and match them to specific therapies.
INTRODUCTIONAs the population ages, the prevalence of heart failure increases, as does the number of patients requiring hospitalization for acute decompensation.1 Between 1992 and 2001, emergency department (ED) visits for acute decompensated heart failure (ADHF) increased by almost 20% and accounted for 3% (10.8 million) of the more than 360 million ED visits made during the decade.2 Historically, these exacerbations were considered clinical manifestations of the downward spiral of congestive heart failure. These events depicted a pathophysiologic model characterized by systolic dysfunction and low cardiac output which resulted in volume overload and pulmonary congestion. The root cause was felt to be worsening underlying cardiac function, possibly due to dietary indiscretion or medication noncompliance or just progression of disease.3,4 As a result, intravenous diuretics were used to rapidly alleviate pulmonary congestion without clinical trial data to support long-term safety, efficacy, or beneficial outcome. In much the same way, vasodilators and inotropes eventually became elements of usual care.
Data from the ADHERE registry have challenged this simple model of ADHF and revealed a more complex and varied pathophysiologic entity-one that consists of multiple types of heart failure patients with various forms of acute decompensation.5 This new pathophysiologic concept has fostered changes in physicians’ views of therapeutic options and targets. Clinicians are now reconsidering how intravenous diuretics, vasodilators, and inotropes should be administered, which ADHF patients should get them, and the long-term morbidity and mortality implications of their decisions.
Although guidelines about the management of patients with heart failure have been previously disseminated, most pertain to chronic management.6 ADHF patient types have not been well characterized or matched with specific treatment strategies in prospective randomized studies. Despite the recent publication of new diagnosis and treatment guidelines,7 there are a lack of evidence and consensus-based treatment
Clinicians are now
reconsidering how
intravenous diuretics,
vasodilators, and
inotropes should be
administered, which
ADHF patients should get
them, and the long-term
morbidity and mortality
implications of their
decisions.
J. Douglas Kirk MD, FACEPAssociate Professor of Emergency Medicine and Vice Chair of Clinical Operations,
Department of Emergency Medicine, University of California, Davis, Medical CenterSacramento, California
ACUTE DECOMPENSATED HEART FAILURE: NOVEL APPROACHES TO CLASSIFICATION AND TREATMENT

34w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
34w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
algorithms that address the therapeutic needs of specific subsets of patients with ADHF suggested by databases such as ADHERE. It does appear however that patient risk stratification8 and initiation of aggressive treatment in the ED9 may limit potentially irreversible myocardial toxicity, especially in those with moderate to severe ADHF. This article will focus on therapeutic management, with particular emphasis on identifying ADHF patient types and matching them to specific treatment strategies. Management protocols and algorithms are provided which can be implemented in your institution.
MANAGEMENT ALGORITHMSThe algorithm depicted in Figure 1 provides guidance for the diagnostic and prognostic evaluation of the suspected ADHF patient, in addition to recommendations for therapeutic strategies and disposition decisions.10 Using typical historical, physical examination, and diagnostic test features, a clinical profile is defined, identifying patients in whom pulmonary congestion predominate the clinical presentation versus those with more of an element of hypoperfusion. Options for initial management of imminent respiratory failure and cardiogenic shock are described. Patients are then further divided based upon severity of illness (low, moderate, or critical severity) with recommendations for treatment and disposition provided for each group.
A minority of patients (~20%) will have mild exacerbations of ADHF (low severity) and the mainstay of therapy for them may be intravenous diuretics,
particularly if they have been noncompliant with diet or medications. Topical or sublingual nitrates may be warranted if moderate hypertension (systolic blood pressure 140-160 mmHg) is present or a history of diastolic dysfunction exists.
Most ADHF visits are of moderate severity (~70%) and typically require a longer duration of therapy which necessitates a hospital stay. More aggressive therapy with loop diuretics plus intravenous vasodilators is warranted, especially if significant hypertension is present. Preliminary data suggest these patients should be aggressively treated with intravenous vasodilators early in the ED course9 and a substantial number may be appropriate for observation unit management.11 The ideal choice of a specific vasodilator in these cases is contentious but both nitroglycerin and nesiritide are effective in symptomatic and hemodynamic improvement, however, their safety profiles remain controversial.12-14 Other factors, such as the need for titration with nitroglycerin which may require admission to an intensive care unit, and play a role in the choice of a specific agent. Using the guidelines to estimate severity from Figure 1, the majority of patients classified as moderate risk and those at low risk can all be managed in an ED observation unit.
Patients who are critically ill (~10%), with complications of respiratory fail-ure and/or cardiogenic shock are not surprisingly, the most difficult to manage. They typically require advanced airway support (endotracheal intubation or non- invasive ventilation) plus a complex
Using typical historical,
physical examination,
and diagnostic test
features, a clinical profile
is defined, identifying
patients in whom
pulmonary congestion
predominate the clinical
presentation versus
those with more of an
element of hypoperfusion.

35w w w . e m c r e g . o r g
ACUTE DECOMPENSATED HEART FAILURE: NOVEL APPROACHES TO CLASSIFICATION AND TREATMENT
35w w w . e m c r e g . o r g
ACUTE DECOMPENSATED HEART FAILURE: NOVEL APPROACHES TO CLASSIFICATION AND TREATMENT
combination of pharmaco-logical therapy (inotropes, diuretics, vasodilators), the choices of which depend upon the patient’s hemody-namic status. These patients are admitted to an intensive care unit and frequently re-quire pulmonary artery cath-eterization to guide therapy. Another algorithm with more patient specific treatment recommendations for management of ADHF in the ED was reported by DiDomenico et al15 and is described in Figure 2. The timeline for key elements of these guidelines is depicted in Figure 3 and provides clinicians with specific clinical targets that should be achieved during the ED or observation unit stay. In this strategy, treatment of ADHF is generally based on the presence or absence of volume overload and an assessment of the patient’s cardiac output. On the left side of Figure 2 [A, C, D, E, F], treatment recommendations are given for patients with ADHF experiencing signs and symptoms of volume overload, manifested by pulmonary congestion. One of the limitations of this algorithm is grouping all patients with pulmonary congestion together, regardless of the etiology.
Figure 1. Algorithm for the early stabilization of acute decompensated heart failure in the emergency department. ADHF, acute decompensated heart failure; BNP, B-type natriuretic peptide; BUN, blood urea nitrogen; CBC, complete blood count; Cr, creatinine; CXR, chest radiograph; ECG, electrocardiogram; ETT, endotracheal tube; ICU, intensive care unit; LVH, left ventricular hypertrophy; NIV, non-invasive ventilation; O2SAT, oxygen saturation; prn, as needed; SBP, systolic blood pressure; SL, sublingual. Adapted from Peacock WF, Allegra J, Ander D, et al. Management of acutely
decompensated heart failure in the emergency department. CHF 2003; 9(suppl 1):3-18

36w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
36w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
Assess response to initial therapy
Add additional therapy as needed
Initiate IV ADHF therapyDiuretic (mild-mod volume overload)
Diuretic + IV vasodilators (mod-sev volume overload)Inotrope (if low CO state)
Establish ADHFdiagnosis
Initial EDcontact
Reassess response to therapy
Add additional therapy as needed
Determine patient dispositionAdmit (ICU vs. observation unit vs. floor)
or discharge home
Transfer out of ED orObservation Unit
0 2 4 6 8 12 24
Time (hours) from initial ED physician evaluation
Figure 2. Acute decompensated heart failure treatment algorithm. ADHF, acute decompensated heart failure; AJR, abdominal jugular reflex; BiPAP, bi-level positive airway pressure; BNP, B-type natriuretic peptide; CI, cardiac index; CPAP, continuous positive airway pressure; DOE, dyspnea on exertion; HJR, hepatojugular reflex; JVD, jugular venous distention; PCWP, pulmonary capillary wedge pressure; PND, paroxysmal nocturnal dyspnea; SBP, systolic blood pressure; SCr, serum creatinine; SOB, shortness of breath; SVR, systemic vascular resistance. Adapted with permission from DiDomenico RJ, Park HY, Southworth MR, et al.. Guidelines for acute decompensated heart failure treatment. Ann Pharmacother. 2004;38:649-660.
Figure 3. Timeline for the management of acute decompensated heart failure in the emergency department/observation unit. ADHF, acute decompensated heart failure; CO, cardiac output; ED, emergency department; ICU, intensive care unit; mod-sev, moderate to severe. Adapted with permission from DiDomenico RJ, Park HY, Southworth MR, et al. Guidelines for acute decompensated heart failure treatment. Ann Pharmacother. 2004;38:649-660.

37w w w . e m c r e g . o r g
ACUTE DECOMPENSATED HEART FAILURE: NOVEL APPROACHES TO CLASSIFICATION AND TREATMENT
37w w w . e m c r e g . o r g
ACUTE DECOMPENSATED HEART FAILURE: NOVEL APPROACHES TO CLASSIFICATION AND TREATMENT
There is no consideration of the patient with severe hypertension and acute pulmonary edema, occasionally referred to as “vascular failure”3 whose primary therapy should be control of blood pressure with intravenous vasodilators. Nonetheless, it is quite helpful with general management principles.
The right side of the algorithm provides treatment recommendations for patients with signs and symptoms consistent with low cardiac output [B]. Inotropic support is recommended, with specific choice of therapy based upon the degree of hypotension and whether or not a beta-blocker is being used [G]. Patients may require vasopressor support if symptomatic hypotension develops. Patients with low cardiac output who fail to respond to inotropic therapy should be evaluated for the presence of very low cardiac output and may require additional aggressive management [J]. Typically, these patients require admission to an intensive care unit and may require the placement of a pulmonary artery catheter to more accurately assess their hemodynamic status. Patients with very low cardiac output who have sufficient systolic blood pressure (>90 mmHg) may benefit from the addition of intravenous diuretic therapy and/or intravenous vasodilators [F].
The major emphasis of this protocol is managing volume overload which is further divided into mild and moderate-severe groups. Patients with mild volume overload [C] are treated with intravenous diuretic therapy, typically loop diuretics [D]. Dosages for patients previously taking diuretics are guided by the total home daily dose, given as an intravenous bolus. Therapy for patients not taking oral diuretics at home is based upon renal function, and clinicians should exercise caution with diuretic therapy in patients with renal dysfunction to avoid further injury. Success of diuretic therapy is driven by urine output goals, and recommendations for repeat diuretic dosing are described in the algorithm. Again, caution should be exercised with extremely high doses of loop diuretics, because in addition to prerenal azotemia, electrolyte
abnormalities (hypokalemia/hypomagnesemia) are common and should be recognized and treated quickly. Standing orders for management of electrolyte disturbances can be quite helpful.
The authors recognized that patients with more severe volume overload are likely to have an inadequate response to intravenous diuretic therapy alone. In these patients the initial pharmacologic regimen should be more aggressive and include both an intravenous diuretic and vasodilator [F]. Nitroglycerin or nesiritide should be used to produce a more rapid response and more effectively relieve the signs and symptoms of congestion in these patients. Again, no specific recommendations are provided as to which vasodilator should be used, but the suggested starting dose of nitroglycerin (5-10 mcg/min) noted should be considerably higher. A corresponding physician order set was developed which can be modified accordingly to accommodate institutional variations in practice. These are a vital part of any management algorithm and are typically necessary to standardize the treatment of ADHF patients. ADHF Patient TypesOther methods of categorizing ADHF patient types have recently been described by a consensus panel of heart failure experts comprised of cardiologists, emergency physicians, hospitalists and pharmacists.16 These classifications are based more on hemodynamic characteristics rather than clinical symptom profile or severity of disease. While most EDs don’t have the luxury of obtaining hemodynamic parameters such as pulmonary capillary wedge pressure or cardiac output via invasive means, they do have a reliable and easily obtainable parameter—the patient’s blood pressure. Patients can be classified into normotensive, hypertensive, and hypotensive ADHF. The exact pathophysiology, clinical characteristics, and treatment options of each of these patient types has yet to be fully elucidated but some recommendations based upon expert consensus can be suggested.
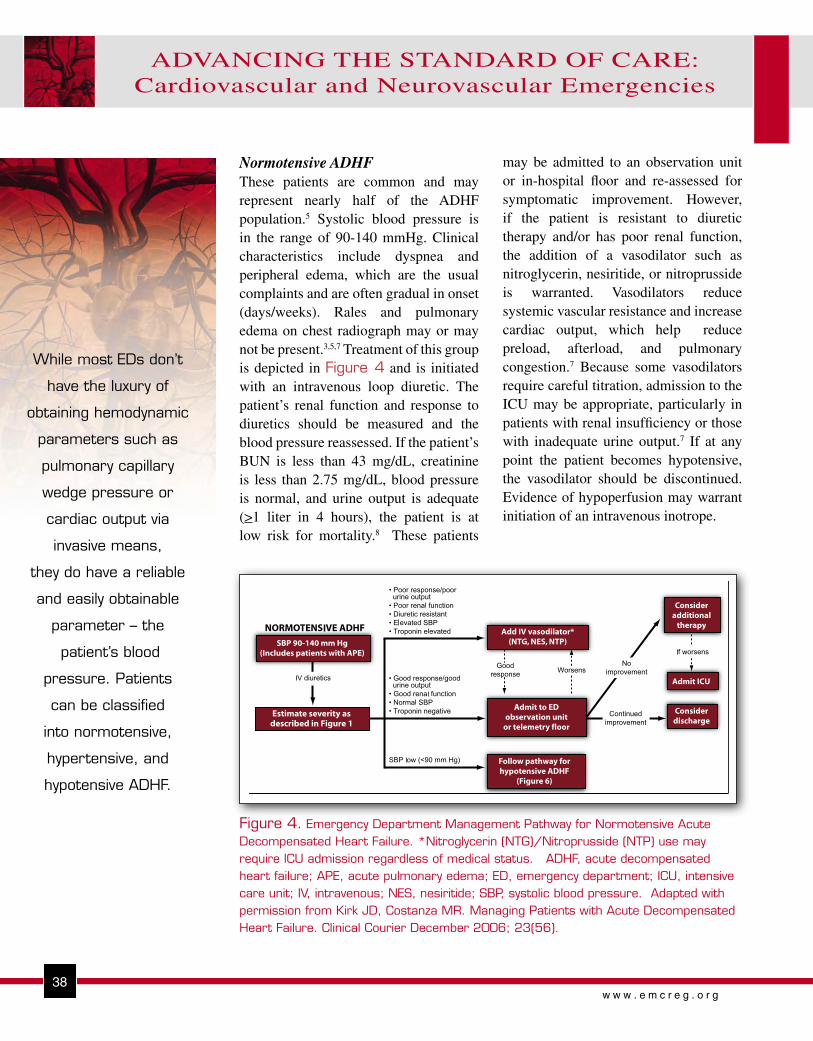
38w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
38w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
may be admitted to an observation unit or in-hospital floor and re-assessed for symptomatic improvement. However, if the patient is resistant to diuretic therapy and/or has poor renal function, the addition of a vasodilator such as nitroglycerin, nesiritide, or nitroprusside is warranted. Vasodilators reduce systemic vascular resistance and increase cardiac output, which help reduce preload, afterload, and pulmonary congestion.7 Because some vasodilators require careful titration, admission to the ICU may be appropriate, particularly in patients with renal insufficiency or those with inadequate urine output.7 If at any point the patient becomes hypotensive, the vasodilator should be discontinued. Evidence of hypoperfusion may warrant initiation of an intravenous inotrope.
While most EDs don’t
have the luxury of
obtaining hemodynamic
parameters such as
pulmonary capillary
wedge pressure or
cardiac output via
invasive means,
they do have a reliable
and easily obtainable
parameter – the
patient’s blood
pressure. Patients
can be classified
into normotensive,
hypertensive, and
hypotensive ADHF.
Normotensive ADHFThese patients are common and may represent nearly half of the ADHF population.5 Systolic blood pressure is in the range of 90-140 mmHg. Clinical characteristics include dyspnea and peripheral edema, which are the usual complaints and are often gradual in onset (days/weeks). Rales and pulmonary edema on chest radiograph may or may not be present.3,5,7 Treatment of this group is depicted in Figure 4 and is initiated with an intravenous loop diuretic. The patient’s renal function and response to diuretics should be measured and the blood pressure reassessed. If the patient’s BUN is less than 43 mg/dL, creatinine is less than 2.75 mg/dL, blood pressure is normal, and urine output is adequate (>1 liter in 4 hours), the patient is at low risk for mortality.8 These patients
Figure 4. Emergency Department Management Pathway for Normotensive Acute Decompensated Heart Failure. *Nitroglycerin (NTG)/Nitroprusside (NTP) use may require ICU admission regardless of medical status. ADHF, acute decompensated heart failure; APE, acute pulmonary edema; ED, emergency department; ICU, intensive care unit; IV, intravenous; NES, nesiritide; SBP, systolic blood pressure. Adapted with permission from Kirk JD, Costanza MR. Managing Patients with Acute Decompensated Heart Failure. Clinical Courier December 2006; 23(56).
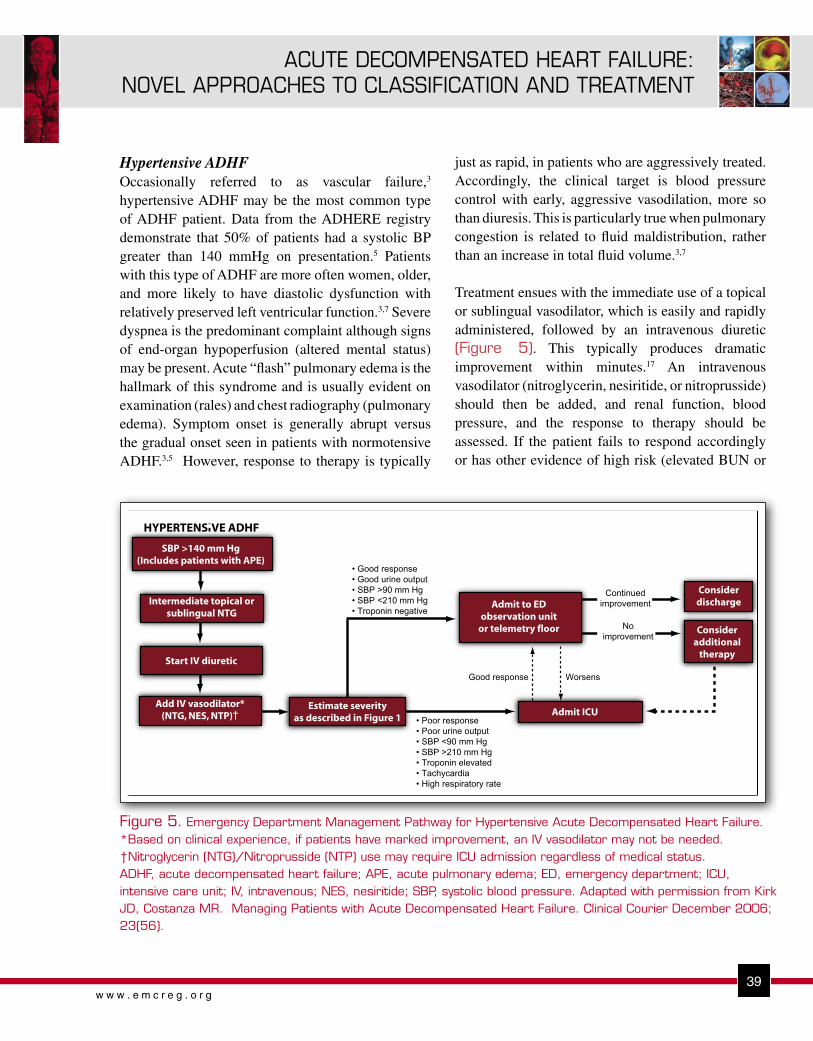
39w w w . e m c r e g . o r g
ACUTE DECOMPENSATED HEART FAILURE: NOVEL APPROACHES TO CLASSIFICATION AND TREATMENT
39w w w . e m c r e g . o r g
ACUTE DECOMPENSATED HEART FAILURE: NOVEL APPROACHES TO CLASSIFICATION AND TREATMENT
Figure 5. Emergency Department Management Pathway for Hypertensive Acute Decompensated Heart Failure. *Based on clinical experience, if patients have marked improvement, an IV vasodilator may not be needed. †Nitroglycerin (NTG)/Nitroprusside (NTP) use may require ICU admission regardless of medical status. ADHF, acute decompensated heart failure; APE, acute pulmonary edema; ED, emergency department; ICU, intensive care unit; IV, intravenous; NES, nesiritide; SBP, systolic blood pressure. Adapted with permission from Kirk JD, Costanza MR. Managing Patients with Acute Decompensated Heart Failure. Clinical Courier December 2006; 23(56).
just as rapid, in patients who are aggressively treated. Accordingly, the clinical target is blood pressure control with early, aggressive vasodilation, more so than diuresis. This is particularly true when pulmonary congestion is related to fluid maldistribution, rather than an increase in total fluid volume.3,7
Treatment ensues with the immediate use of a topical or sublingual vasodilator, which is easily and rapidly administered, followed by an intravenous diuretic (Figure 5). This typically produces dramatic improvement within minutes.17 An intravenous vasodilator (nitroglycerin, nesiritide, or nitroprusside) should then be added, and renal function, blood pressure, and the response to therapy should be assessed. If the patient fails to respond accordingly or has other evidence of high risk (elevated BUN or
Hypertensive ADHFOccasionally referred to as vascular failure,3 hypertensive ADHF may be the most common type of ADHF patient. Data from the ADHERE registry demonstrate that 50% of patients had a systolic BP greater than 140 mmHg on presentation.5 Patients with this type of ADHF are more often women, older, and more likely to have diastolic dysfunction with relatively preserved left ventricular function.3,7 Severe dyspnea is the predominant complaint although signs of end-organ hypoperfusion (altered mental status) may be present. Acute “flash” pulmonary edema is the hallmark of this syndrome and is usually evident on examination (rales) and chest radiography (pulmonary edema). Symptom onset is generally abrupt versus the gradual onset seen in patients with normotensive ADHF.3,5 However, response to therapy is typically

40w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
40w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
Figure 6. Emergency Department Management Pathway for Hypotensive Acute Decompensated Heart Failure. *If SBP ≥90 and no improvement; ADHF, acute decompensated heart failure; ED, emergency department; IV, intravenous; ICU, intensive care unit; NES, nesiritide; NTG, nitroglycerine; NTP, nitroprusside; SBP, systolic blood pressure. Adapted with permission from Adams KF, Kirk JD, Costanza MR. Managing Patients with Acute Decompensated Heart Failure. Kirk JD, Costanza MR. Managing Patients with Acute Decompensated Heart Failure. Clinical Courier December 2006; 23(56).
creatinine, hypotension)8, admission to the intensive care unit is recommended. If the patient responds adequately to initial therapy, admission to an observation unit or in-hospital floor is appropriate, unless ongoing titration of the vasodilator necessitates intensive care unit admission.
Hypotensive ADHFPatients typically present with evidence of end-organ hypoperfusion (altered mental status, cool extremities, poor urine output) in addition to pulmonary congestion.3,7 Patients with a systolic blood pressure <90 mmHg usually have low cardiac output, but can follow a continuum from cardiogenic shock to reasonably well compensated heart failure.7 Although this is the smallest subgroup of patients with ADHF, accounting for only 3% of the ADHERE population,5 it is associated with a disproportionately high in-
hospital mortality rate, approaching 30%.18 Admission to the intensive care unit is warranted and many of these patients require pulmonary artery catheterization to guide therapy. Typical hemodynamic parameters include elevated pulmonary capillary wedge pressure, decreased cardiac index and left ventricular ejection fraction, and advanced Killip class of III or IV.7
This group is the most challenging to manage, given the myriad clinical profiles, hemodynamic parameters, and complications of therapeutic agents (hypotension, myocardial injury, mortality risk). 12-14,19-21 Guidelines for therapy are likewise difficult to develop given these limitations (Figure 6). Inotropic therapy, which has been associated with poorer outcomes,19,20 does increase cardiac output and elevate blood pressure,4,7,22 and therefore may be appropriate in this critically ill population. If there are ongoing signs

41w w w . e m c r e g . o r g
ACUTE DECOMPENSATED HEART FAILURE: NOVEL APPROACHES TO CLASSIFICATION AND TREATMENT
41w w w . e m c r e g . o r g
ACUTE DECOMPENSATED HEART FAILURE: NOVEL APPROACHES TO CLASSIFICATION AND TREATMENT
of congestion, the addition of diuretic therapy may also be reasonable but is frequently curtailed due to hypotension. In some cases, vasodilator therapy may be appropriate if blood pressure increases and there are ongoing hemodynamic derangements such as high systemic vascular resistance, elevated pulmonary capillary wedge pressure, low cardiac index, or poor urine output.7,15
SUMMARYRecent data have challenged the historical model of ADHF and revealed a more complex and varied pathophysiologic entity-one that consists of multiple types of heart failure patients with various forms of acute decompensation. Clinicians and investigators are now reconsidering their therapeutic options. Which drugs should be administered to what type of patient, and most importantly, what are the safety implications are two considerations. Although there is a paucity of evidence-based treatment strategies for patients with ADHF, management protocols and algorithms categorized by clinical profile and hemodynamic status are helpful in identifying ADHF patient types and matching them to specific therapies. Utilizing such strategies should improve the consistency of emergent care and hopefully patient outcome.
REFERENCES1. Heart disease and stroke statistics—2003 update. Dallas: American
Heart Association, 2002.
2. Hugli O, Braun JE, Kim S, Pelletier AJ, Camargo CA Jr. United States emergency department visits for acute decompensated heart failure, 1992 to 2001. Am J Cardiol. 2005;96:1537-1542.
3. Gheorghiade M, De Luca L, Fonarow GC, et al. Pathophysiologic targets in the early phase of acute heart failure syndromes. Am J Cardiol. 2005;96(suppl 6A):11G-17G.
4. Cotter G, Moshkovitz Y, Milovanov O, et al. Acute heart failure: a novel approach to its pathogenesis and treatment. Eur J Heart Fail. 2002;4:227-234.
5. Adams KF Jr, Fonarow GC, Emerman CL, et al. Characteristics and outcomes of patients hospitalized for heart failure in the United States: rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE). Am Heart J. 2005;149:209-216.
6. Hunt SA, Baker DW, Chin MH, et al. ACC/AHA guidelines for the evaluation and management of chronic heart failure in the adult: executive summary. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to revise the 1995 Guidelines for the Evaluation and Management of Heart Failure). J Am Coll Cardiol. 2001;38:2101-2113.
7. Nieminen MS, Bohm M, Cowie MR, et al. Executive summary of the Guidelines on the Diagnosis and Treatment of Acute Heart Failure: The Task Force on Acute Heart Failure of the European Society of Cardiology. Eur Heart J. 2005;26:384-416.
8. Fonarow GC, Adams KF Jr, Abraham WT, et al. for the ADHERE Scientific Advisory Committee, Study Group, and Investigators. Risk stratification for in-hospital mortality in acutely decompensated heart failure: classification and regression tree analysis. JAMA. 2005;293:572-580.
9. Peacock WF, Emerman CL, Costanzo MR, et al. Early initiation of intravenous vasoactive therapy improves heart failure outcomes: an analysis from the ADHERE registry database. Ann Emerg Med 2003; 42(4):S26.
10. Peacock WF, Allegra J, Ander D, et al. Management of acutely decompensated heart failure in the emergency department. CHF. 2003; 9(suppl 1): 3-18.
11. Peacock WF IV, Holland R, Gyarmathy R, et al. Observation unit treatment of heart failure with nesiritide: results from the PROACTION trial. J Emerg Med. 2005;29:243-252.
12. Sackner-Bernstein JD, Kowalski M, Fox M, et al. Short-term risk of death after treatment with nesiritide for decompensated heart failure: a pooled analysis of randomized controlled trials. JAMA. 2005;293:1900-1905.
13. Abraham WT. Nesiritide and mortality risk: individual and pooled analyses of randomized controlled trials. Rev Cardiovasc Med. 2005;6:2.
14. Abraham WT, Adams KF, Fonarow GC, et al. In-hospital mortality in patients with acute decompensated heart failure requiring intravenous vasoactive medications: an analysis from the ADHERE registry. J Am Coll Cardiol. 2005; 46:57– 64.
15. DiDomenico RJ, Park HY, Southworth MR, et al. Guidelines for acute decompensated heart failure treatment. Ann Pharmacother. 2004;38:649-660.
16. Kirk JD, Costanza MR. Managing Patients with Acute Decompensated Heart Failure. Clinical Courier December 2006; 23(56).
17. Bussmann W, Schupp D. Effect of sublingual nitroglycerin in emergency treatment of severe pulmonary edema. Am J Cardiol 1978; 41:931-936.
18. Harjola VP, Ylikangas S, Siirila-Waris K. Type of acute heart failure significantly affects intensive care stay and in-hospital mortality. Presented at: Annual Scientific Sessions of the European Society of Cardiology; September 3-7, 2005; Stockholm, Sweden. Abstract P4076.
19. Cuffe MS, Califf RM, Adams KF Jr, et al. Short-term intravenous milrinone for acute exacerbation of chronic heart failure: a randomized controlled trial. JAMA. 2002;287:1541-1547.

42w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
20. O’Connor CM, Gattis WA, Uretsky BF, et al. Continuous intravenous dobutamine is associated with an increased risk of death in patients with advanced heart failure: insights from the Flolan International Randomized Survival Trial (FIRST). Am Heart J. 1999;138:78-86.
21. Gottlieb SS, Brater DC, Thomas I, et al. BG9719 (CVT-124), an A1 adenosine receptor antagonist, protects against the decline in renal function observed with diuretic therapy. Circulation. 2002 Mar 19;105(11):1348-53.
22. Felker GM, O'Connor CM. Inotropic therapy for heart failure: an evidence-based approach. Am Heart J. 2001;142:393-401.
Copyright EMCREG-International, 2007

43w w w . e m c r e g . o r g
LACTATE – A MARKER FOR SEPSIS AND TRAUMA
Rather than thinking
of lactate solely as a
byproduct of inadequate
blood perfusion, it may
be useful to consider
lactate as a marker
of strained cellular
metabolism.
LACTATE – A MARKER FOR SEPSIS AND TRAUMA
Andra L. Blomkalns, MDAssistant Professor; Vice Chairman-Education; Residency Program Director,
Department of Emergency Medicine, University of Cincinnati College of Medicine, Cincinnati, OH, Director of CME and Enduring Materials, EMCREG-International
OBJECTIVES:1) Describe the process by which lactate would become elevated for a given patient.2) List conditions which may cause elevated serum lactate other than trauma and sepsis.3) Explain the significance of “lactate clearance.” 4) Discuss the potential uses for lactate in the emergency department.
INTRODUCTIONIt seems that each month, our journals publish the findings of a new study which describes the use of a certain marker or set of markers for the diagnosis, prognosis, or treatment of some emergency medical condition. Manuscripts and symposia discussing marker clearance, marker change, marker panels, and point-of-care markers reside in every issue and every meeting. In this newsletter, lactate, a serum marker older than any cardiac marker cousin, assumes center stage in two of the most difficult and resource intensive emergency medicine conditions – sepsis and trauma. This EMCREG-International newsletter aims to familiarize the emergency physician with lactate and its potential use the emergency department (ED).
Lactic acid or lactate, as its name implies, was first isolated from sour milk in the 18th century. In 1918, scientists observed cases in which metabolic acidosis was associated with decreased blood flow and shock. In the 1970’s and 80’s, the seminal works of Huckabee and Cohen finally described the clinical syndrome
of lactic acidosis as we know it today.1,2 The clinical and physiologic condition of metabolic acidosis has been recognized for nearly a century, yet we are only now discovering new approaches for its diagnosis and treatment.
Biochemistry of Lactate: Production and Lactic AcidosisUnderstanding how lactate levels might be used in clinical practice requires an understanding of how the body produces and clears lactate. In a normal steady state with adequate tissue resources and oxygenation, more cellular energy can be extracted aerobically by means of the citric acid cycle and the electron-transport chain. In this case, cells convert pyruvate to acetyl CoA through oxidative decarboxylation.
In contrast, when the body experiences inadequate tissue perfusion, it undergoes anaerobic metabolism to create some energy, even in a small amount. In this case, pyruvate metabolizes to lactate
Pyruvate + NAD+ + CoA ‡ Acetyl CoA + CO2 + NADH
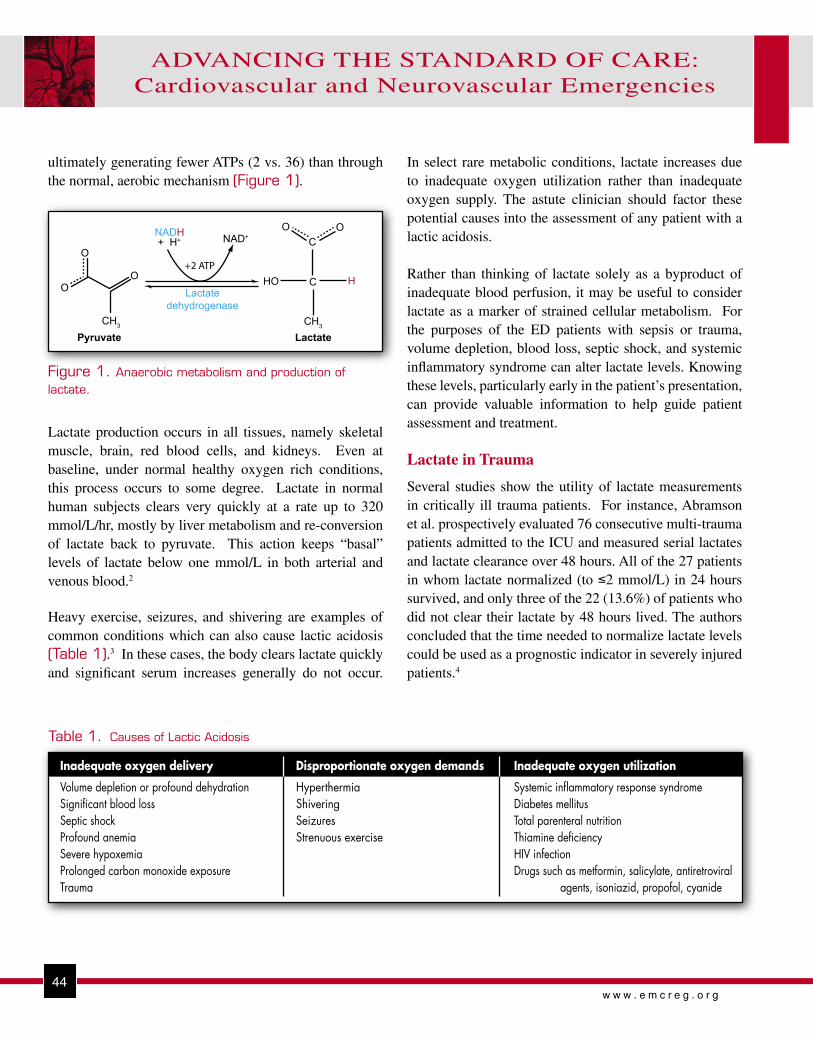
44w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
44w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
ultimately generating fewer ATPs (2 vs. 36) than through the normal, aerobic mechanism (Figure 1).
In select rare metabolic conditions, lactate increases due to inadequate oxygen utilization rather than inadequate oxygen supply. The astute clinician should factor these potential causes into the assessment of any patient with a lactic acidosis.
Rather than thinking of lactate solely as a byproduct of inadequate blood perfusion, it may be useful to consider lactate as a marker of strained cellular metabolism. For the purposes of the ED patients with sepsis or trauma, volume depletion, blood loss, septic shock, and systemic inflammatory syndrome can alter lactate levels. Knowing these levels, particularly early in the patient’s presentation, can provide valuable information to help guide patient assessment and treatment.
Lactate in Trauma
Several studies show the utility of lactate measurements in critically ill trauma patients. For instance, Abramson et al. prospectively evaluated 76 consecutive multi-trauma patients admitted to the ICU and measured serial lactates and lactate clearance over 48 hours. All of the 27 patients in whom lactate normalized (to ≤2 mmol/L) in 24 hours survived, and only three of the 22 (13.6%) of patients who did not clear their lactate by 48 hours lived. The authors concluded that the time needed to normalize lactate levels could be used as a prognostic indicator in severely injured patients.4
H
NADH+ H+ NAD+
O
O
O
CH3
O O
HO C
CH3
Lactatedehydrogenase
Pyruvate Lactate
C
+2 ATP
Table 1. Causes of Lactic Acidosis
Inadequate oxygen delivery
Volume depletion or profound dehydrationSignificant blood lossSeptic shockProfound anemiaSevere hypoxemiaProlonged carbon monoxide exposureTrauma
Disproportionate oxygen demands
HyperthermiaShiveringSeizuresStrenuous exercise
Inadequate oxygen utilization
Systemic inflammatory response syndromeDiabetes mellitusTotal parenteral nutritionThiamine deficiencyHIV infectionDrugs such as metformin, salicylate, antiretroviral
agents, isoniazid, propofol, cyanide
Lactate production occurs in all tissues, namely skeletal muscle, brain, red blood cells, and kidneys. Even at baseline, under normal healthy oxygen rich conditions, this process occurs to some degree. Lactate in normal human subjects clears very quickly at a rate up to 320 mmol/L/hr, mostly by liver metabolism and re-conversion of lactate back to pyruvate. This action keeps “basal” levels of lactate below one mmol/L in both arterial and venous blood.2
Heavy exercise, seizures, and shivering are examples of common conditions which can also cause lactic acidosis (Table 1).3 In these cases, the body clears lactate quickly and significant serum increases generally do not occur.
Figure 1. Anaerobic metabolism and production of lactate.

45w w w . e m c r e g . o r g
LACTATE – A MARKER FOR SEPSIS AND TRAUMA
45w w w . e m c r e g . o r g
LACTATE – A MARKER FOR SEPSIS AND TRAUMA
In his manuscript
on the importance
of 24-hour lactate
clearance, Dr. Blow
and colleagues
extend the critical
period of a “golden
hour” to a new
lactate driven adage
of the “silver day.”
Emergency physicians and emergency medical service providers pay much attention to the “golden hour” critical time period in trauma resuscitation. In his manuscript on the importance of 24-hour lactate clearance, Dr. Blow and colleagues extend the critical period of a “golden hour” to a new lactate driven adage of the “silver day.” This retrospective observational study followed by a prospective trial included trauma patients presenting to a Level I trauma center who survived greater than 24 hours and had an Injury Severity Score (ISS) greater than 20. Arrival and subsequent serial serum lactates were obtained and levels and time of lactate clearance measured. These patients (n=85) underwent aggressive resuscitation to clear lactate to a level less than 2.5 mmol/L and thereby treating what
the authors call “occult hypoperfusion.” Of the patients that corrected their lactate and occult hypoperfusion within 24 hours, all survived. The longer it took for lactate to clear, the higher the rate of multi-system organ failure and mortality. It was found that 43% of the patients died if lactate clearance took more than 24 hours (Figure 2).5
If one can conclude that lactate levels in trauma patients are prognostic and that rapid lactate normalization benefits trauma patients, then rapid assessment of lactate levels becomes desirable. To support this conclusion, Asimos et al. conducted a before-and-after study of implementation of a point-of-care testing platform for major trauma patients. Routine trauma labs included hemoglobin, sodium,
Figure 2. Morbidity and survival vs. time to correct occult hypoperfusion.5 Reprinted with permission from Blow et al. J Trauma 1999; 47:964-9.
100
80
60
40
20
00-6 Hours 7-12 Hours 13-24 Hours >24 Hours
100 100 100
0 0
169
21
43
57
36
50
= Survival= Multi-system organ failure= Respiratory complications
Mo
rbid
ity
and
Su
rviv
al (%
)
Time to correct occult hypoperfusion

46w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
46w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
glucose, potassium, chloride, blood urea nitrogen, pH, PCO2, PO2, HCO3, base deficit, and lactate. Only hemoglobin, glucose, blood gas, and lactate resulted in “emergency appropriate” management changes.6
Myths and Misconceptions Regarding Lactate Measurement in Trauma Patients
I. “You need to use arterial blood to measure lactate.”
Several studies find serial lactate measurements to be useful in trauma patient care. Initial ICU investigations used only arterial lactate and some of the more current literature does not indicate whether arterial or venous blood was used in the study population. Previous experience and clinical use of lactate in the ICU setting suggests that only arterial lactate is useful. Lavery et al. investigated this very issue and correlated the use of venous lactate and arterial lactate in triaged patients presenting to a trauma center. In this study, the authors sought to determine the correlation between arterial and venous lactate as well as determine if venous lactate could identify those patients with serious injuries.
As we know, the acquisition of specifically arterial lactate, despite its demonstrated utility, limits its usefulness in the undifferentiated patient population of the ED. Without an arterial line, arterial blood gas acquisition requires the special skills of a physician, nurse, or respiratory therapist. Patients find this procedure more painful and frequently refuse repeated attempts or serial sampling. Arterial punctures can also cause greater complications of bleeding, hematoma, and arterio-venous fistulas.
In this study, patients arriving to a trauma center (n=375) had both arterial and venous lactates performed within 10 minutes. Collected data included injury mechanism, demographics, admission vital signs, disposition, length of stay, hospital outcomes and injury severity score. The mean arterial lactate concentration was 3.11 mmol/L (SD 3.45, 95% CI 2.67-3.55) and the mean venous lactate concentration was 3.43 mmol/L (SD 3.41, 95% CI 2.96-3.90) demonstrating no significant differences between the two sources of blood lactate. The correlation between venous and arterial lactate levels was 0.94 (Figure 3).7
20
15
10
5
50 10 15 20
Venous lactate (mmol/L)
Arte
rial l
acta
te (m
mol
/L)
Figure 3. Scatter plot, regression line, and 95% confidence intervals for venous and arterial lactate. The equation for the line is y=0.076 + 0.889x.7 Reprinted with permission from Klein et al. Acta Med Austriaca 1976; 3:69-73.
47w w w . e m c r e g . o r g
LACTATE – A MARKER FOR SEPSIS AND TRAUMA
47w w w . e m c r e g . o r g
LACTATE – A MARKER FOR SEPSIS AND TRAUMA
Furthermore, an elevated venous lactate was associated with and correctly predicted moderate to severe injury as defined by the Abbreviated Injury Score (AIS). Lactate levels ≥ 2 mmol/L portended an increased risk of an ISS > 13, death, admission to the ICU, and length of stay great than 48 hours. It appears that both venous and arterial lactate can adequately predict injury severity and mortality, suggesting that either can be used in ED clinical practice.7
II. “I can use the anion gap and don’t need another lab test.”
A variety of laboratory parameters can help identify patients with severely compromised or strained metabolisms. Among these are the anion gap (AG), pH, and lactate levels. In a retrospective cohort study, Adams et al. included all ED patients over a seven month time period in whom a lactate level was measured for any reason. They considered an AG >12 abnormal and conducted sensitivity analyses of the AG for detecting the presence of a lactate >2.5 mmol/L. The AG was 52.8% sensitive, 81.0% specific with a negative predictive value of 89.7% for the prediction of lactic acidosis.8 While the three parameters of AG, pH, and lactate are related, they are not absolutely co-dependent. Critically-ill patients have impaired acid-base regulation and are thought to generate more unmeasured cations, such as magnesium and calcium, thereby affecting the AG. Furthermore, hypoalbuminemia affects the AG and is also prevalent in the ED population.8,9
From these studies, it appears that the AG cannot be considered a surrogate for lactate testing.
Lactate in Sepsis
In the United States alone, sepsis accounts for over 751,000 cases, 215,000 deaths, and 16.7 billion dollars in health care costs annually.10-12 With the more aggressive emphasis towards rapid discharges and outpatient surgeries, and the paucity of primary care, sepsis ranks as one of the higher prevalence, higher mortality, and more expensive conditions that an emergency physician will encounter. Recent emphasis on goal-directed resuscitation and new aggressive treatment adjuncts such as intensive insulin therapy, activated protein C, and steroid therapy stand to improve outcomes in this everyday emergency condition.12 Emergency physicians have an opportunity to make a significant impact in this challenging patient population.
Landmark studies in this area support the use of serum lactate in both the diagnostic and treatment phases for septic shock.11,13,14 Lactate levels are a critical parameter indicating sepsis induced hypoperfusion and triggering guideline driven early goal directed therapy (EGDT) in the Surviving Sepsis Campaign.15 In a multivariate analysis of over 20 hemodynamic (i.e. pulmonary artery pressures, total blood volume index) and regional variables of organ dysfunction (i.e. mucosal-arterial PCO2, gastric intramucosal pH), lactate was the only ED attainable parameter that was predictive of outcome.13 While previous resuscitation literature may have given the notion that directed care of septic shock patients required invasive measurements such as pulmonary artery pressures, oxygen delivery index, and systemic vascular resistance, more recent
Both venous and
arterial lactate can
adequately predict
injury severity and
mortality, suggesting
that either can be
used in ED clinical
practice.

48w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
48w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
investigations support testing more easily acquired in the ED such as mean arterial pressures (MAP), central venous pressures (CVP), and lactate levels.11,13
It also appears that lactate screening may prove beneficial even in normotensive, hemodynamically stable patients. Shapiro et al. in a study with 1,278 patients with infection, demonstrated that increasing lactate levels were associated with increased mortality. Lactate levels less than 2.5 mmol/L were associated with a 4.9% mortality rate compared to patients with lactate levels ≥ 4 mmol/L who had an in-hospital mortality of 28.4%. A lactate concentration ≥ 4 mmol/L was 36% (95% CI 27-45%) sensitive and 92% (95% CI 90-93%) specific for any death (Figure 4).12
Just as in the trauma population, serial lactate measurements and attention to lactate clearance or “lac-time” may provide additive information useful in the treatment and prognosis of the individual patient. For instance, Bakker et al. found that while initial
blood lactates did not differ between survivors and non-survivors in patients with septic shock, survivors had a significant decrease in lactate levels and lower “lac-times.”16 Levraut et al. used a novel method of determining lactate clearance by infusing exogenous lactate and measuring clearance as well as basal lactate production. An increase in blood lactate of ≥ 0.6 mmol/L 60 minutes after the start time of lactate infusion was 53% sensitive and 90% specific and was associated with an odds ratio of 14.2 (p=0.042) for 28-day mortality.17 Nguyen et al. examined a cohort of 111 ED and ICU patients with severe sepsis and septic shock. In this study, lactate clearance was defined as the percentage lactate decrease over the initial six hour ED evaluation and treatment period (Figure 5). All patients were followed for 72 hours and received protocol-driven early goal directed therapy EGDT. Multivariate logistic regression analysis of statistically significant univariate variables showed an inverse relationship with mortality - the higher the lactate clearance, the lower the mortality. In fact,
Lactate
Mor
talit
y R
ate
30.0%
25.0%
20.0%
15.0%
10.0%
5.0%
0.0%
4.9%1.5%
9.0%
4.5%
28.4%
25d in-hospitalmortalityDeath within 3d
0-2.4 2.5-3.9 4.0
22.4% Figure 4. Lactate as a predictor of mortality.12 Reprinted with permission from Shapiro et al. Ann Emerg Med. 2005; 45:524-28.
Figure 5. Definition of lactate clearance.18

49w w w . e m c r e g . o r g
LACTATE – A MARKER FOR SEPSIS AND TRAUMA
49w w w . e m c r e g . o r g
LACTATE – A MARKER FOR SEPSIS AND TRAUMA
mortality was reduced approximately 11% for each 10% increase in lactate clearance. Patients with a lactate clearance >10% had a greater improvement in Acute Physiology And Chronic Health Evaluation (APACHE) II scores and lower 60-day mortality.18 These findings suggest an important role for serial sampling and lactate clearance as a prognostic indicator.
SUMMARYUsing lactate as an indicator of impaired metabolism in trauma and sepsis patients may help emergency caregivers further diagnosis, risk stratify, and treat patients in the ED. Serial lactate measurements over the early diagnostic and treatment period can assist in monitoring treatment progress. Mainstream adaptation to the diverse ED environment will require further ED-based studies and observation of lactate utility in routine care of critically-ill and injured patients.
REFERENCES1. Cohen RD, Woods HF. Lactic acidosis revisited. Diabetes.
1983;32(2):181-191.
2. Huckabee WE. Abnormal resting blood lactate. I. The significance of hyperlactatemia in hospitalized patients. Am J Med. 1961;30:840-848.
3. Fall PJ, Szerlip HM. Lactic acidosis: from sour milk to septic shock. J Intensive Care Med. 2005;20(5):255-271.
4. Abramson D, Scalea TM, Hitchcock R, Trooskin SZ, Henry SM, Greenspan J. Lactate clearance and survival following injury. J Trauma. 1993;35(4):584-588; discussion 588-589.
5. Blow O, Magliore L, Claridge JA, Butler K, Young JS. The golden hour and the silver day: detection and correction of occult hypoperfusion within 24 hours improves outcome from major trauma. J Trauma. 1999;47(5):964-969.
6. Asimos AW, Gibbs MA, Marx JA, et al. Value of point-of-care blood testing in emergent trauma management. J Trauma. 2000;48(6):1101-1108.
7. Lavery RF, Livingston DH, Tortella BJ, Sambol JT, Slomovitz BM, Siegel JH. The utility of venous lactate to triage injured patients in the trauma center. J Am Coll Surg. 2000;190(6):656-664.
8. Adams BD, Bonzani TA, Hunter CJ. The anion gap does not accurately screen for lactic acidosis in emergency department patients. Emerg Med J. 2006;23(3):179-182.
9. Story DA, Poustie S, Bellomo R. Estimating unmeasured anions in critically ill patients: anion-gap, base-deficit, and strong-ion-gap. Anaesthesia. 2002;57(11):1109-1114.
10. Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29(7):1303-1310.
11. Rivers E, Nguyen B, Havstad S, et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med. 2001;345(19):1368-1377.
12. Shapiro NI, Howell MD, Talmor D, et al. Serum lactate as a predictor of mortality in emergency department patients with infection. Ann Emerg Med. 2005;45(5):524-528.
13. Poeze M, Solberg BC, Greve JW, Ramsay G. Monitoring global volume-related hemodynamic or regional variables after initial resuscitation: What is a better predictor of outcome in critically ill septic patients? Crit Care Med. 2005;33(11):2494-2500.
14. Varpula M, Tallgren M, Saukkonen K, Voipio-Pulkki LM, Pettila V. Hemodynamic variables related to outcome in septic shock. Intensive Care Med. 2005;31(8):1066-1071.
15. Dellinger RP, Carlet JM, Masur H, et al. Surviving Sepsis Campaign guidelines for management of severe sepsis and septic shock. Crit Care Med. 2004;32(3):858-873.
16. Bakker J, Gris P, Coffernils M, Kahn RJ, Vincent JL. Serial blood lactate levels can predict the development of multiple organ failure following septic shock. Am J Surg. 1996;171(2):221-226.
17. Levraut J, Ichai C, Petit I, Ciebiera JP, Perus O, Grimaud D. Low exogenous lactate clearance as an early predictor of mortality in normolactatemic critically ill septic patients. Crit Care Med. 2003;31(3):705-710.
18. Nguyen HB, Rivers EP, Knoblich BP, et al. Early lactate clearance is associated with improved outcome in severe sepsis and septic shock. Crit Care Med. 2004;32(8):1637-1642.
Copyright EMCREG-International, 2007

POINT-OF-CARE TESTING FOR CARDIAC BIOMARKERS IN THE ED:A BLUEPRINT FOR IMPLEMENTATION
W. Brian Gibler, MDProfessor and Chairman; Department of Emergency Medicine,
University of Cincinnati College of Medicine, Cincinnati, Ohio, President, EMCREG-International
OBJECTIVES:• To discuss the multiple factors present in the current emergency department (ED)
environment responsible for the growth of point-of-care (POC) testing for cardiac biomarkers.
• To describe the hospital administrator, laboratorian, and clinician stakeholders involved with evaluation, implementation and maintenance of a successful POC testing program for cardiac biomarkers in the ED.
• To describe recent POC testing trials for cardiac biomarkers in the ED.• To describe the strengths and limitations of POC testing in the ED environment.
INTRODUCTIONEmergency Department EnvironmentMultiple factors in the emergency department (ED) care environment have influenced the growth of point-of-care (POC) testing in the United States. In 2006, approximately 115,000,000 patients will visit EDs in the United States and over 5.2 million of these individuals will have possible acute coronary syndrome (ACS) requiring complex evaluations by the emergency physician including physical examination, electrocardiography, and cardiac biomarker testing.
1,2 This large
number of patients with potentially life-threatening ACS require diagnostic work-ups in EDs that are “overcrowded” due to the substantial variety of illnesses and injuries that can stress emergency human and material resources, and inundate hospital in-patient beds. To improve risk stratification and optimize use of in-patient beds for patients at significant risk for ACS and its complications, routine
in-patient stays for chest pain have now been replaced by evaluations in the ED or adjacent chest pain observation unit. Patient expectations for emergency diagnosis of potentially life-threatening conditions such as ACS include not only high quality accurate and knowledgeable care by the emergency physician, but also treatment that is efficient and rapid. Additionally, there has been a significant increase in time dependent therapies for patients with ACS. Patient demands for efficient care and the development and implementation of evidence-based approaches to therapy such as the 2002 ACC/AHA Unstable Angina/Non-ST-segment Elevation Myocardial Infarction Guidelines have increased the need for rapid testing for cardiac biomarkers through a reduction in laboratory test turn-around-time (TAT).3
Point-of-care (POC) testing is a response to process challenges in the central
The 2002 ACC/AHA
Unstable Angina/Non-
ST-segment Elevation
Myocardial Infarction
Guidelines have increased
the need for rapid testing
for cardiac biomarkers
through a reduction in
laboratory test turn-
around-time.
50w w w . e m c r e g . o r g

51w w w . e m c r e g . o r g
POINT-OF-CARE TESTING FOR CARDIAC BIOMARKERS IN THE ED:A BLUEPRINT FOR IMPLEMENTATION
laboratory that is responsible for an ever-increasing number of sophisticated diagnostic tests for a variety of different conditions throughout the hospital. Central laboratory processing of blood samples from the ED includes the delivery of the blood specimen, centrifugation and clot extraction if serum testing is required, and up to 20 minutes of assay time for the large automated immunoassay analyzers. Prior to this laboratory “analytical time”, the pre-analytical time in the ED includes writing the order for blood work, drawing the sample by the nurse or patient care technician, correctly labeling the test tube for laboratory identification and laboratory information system processing, and either walking the sample to the lab from the ED or pneumatic tube transfer. For patients in the ED that receive serial cardiac biomarker sampling for evaluation of possible ACS, demands for a rapid return of laboratory information return to the clinician have clearly increased. These demands from the ED have translated to increased volume of testing and the need to “turnaround” cardiac biomarker blood tests quickly from the central laboratory of the hospital. Point-of-care testing has proved effective for multiple disease processes in addition to ACS. For patients with heart failure, B-type natriuretic peptide (BNP) has a remarkable ability to risk stratify patients with heart failure presenting to the ED, identifying patients likely to have complications. In patients with possible toxic ingestions, POC testing for toxic substances can decrease the time required for diagnosis in the emergency setting. For patients with possible hypoglycemia, POC testing for blood glucose has been a mainstay for the last decade.
The results of cardiac biomarker tests such as myoglobin, creatine kinase-MB (CK-MB) and troponin are critical for risk stratification, initiating anti-platelet and anti-thrombotic therapy, admission decisions, and for patients without evidence of myocardial necrosis or ischemia, providing the impetus for release from the ED to home. Ideally, laboratory results would return to the clinician virtually instantaneously, as all of the previously described decisions are based, to a large extent, on the results of the cardiac biomarker testing from serial samples obtained in the ED. Point-of-care testing, often called “near patient testing,” occurs where patient care is rendered at the bedside, such as in the emergency setting. It serves to provide a rapid return of information to the clinician. The interval from the point that blood is drawn from the patient, to the moment the emergency physician receives the test result, has been termed the “vein to brain” interval. Optimal laboratory testing for patients with possible ACS should make this time period as short as possible.
As previously noted, consensus guidelines published by the American College of Cardiology and the American Heart Association for the diagnosis and treatment of non-ST-segment elevation ACS recommend that cardiac markers should be made available to the clinician within 30-60 minutes from the time of ED presentation.
3 As many EDs and
central laboratories are unable to meet this recommendation using traditional processes through the laboratory, POC testing has to be considered as an operational necessity for evaluating these patients.
The results of cardiac
biomarker tests
such as myoglobin,
creatine kinase-MB
(CK-MB) and troponin
are critical for risk
stratification, initiating
anti-platelet and anti-
thrombotic therapy,
admission decisions,
and for patients without
evidence of myocardial
necrosis or ischemia,
providing the impetus
for release from the
ED to home.

52w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
52w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
POC Cardiac Marker Assay Performance The most commonly used markers in cardiac risk stratification are CKMB, cardiac troponin (Tn) I or T, brain natriuretic peptide (BNP) and myoglobin. Other markers such as high-sensitivity CRP (hsCRP), myeloperoxidase, and D-dimer are also available.
4-11
The measurement of the cardiac troponins is the major focus for POC testing in patients presenting with potential ACS to the ED as this cardiac biomarker has substantial research basis to support its use in risk stratification for these patients. In a trial of 248 total patients using a POC test for TnI, Apple and colleagues evaluated the antibody specificity, detection limit, imprecision, linearity, assay specificity, sample type stability, interferences and reference limit determination. The detection limit for the POC assay was found to be 0.02 ng/L with a 99th percentile reference limit of 0.08 ng/L. This study demonstrated that the POC assay accurately detected TnI and was appropriate for use in a bedside environment for the evaluation and risk assessment of patients with possible ACS.
12
In the Chest Pain Evaluation by Creatine Kinase-MB, Myoglobin, and Troponin I (CHECKMATE) trial, “time to positivity” between POC testing and central laboratory were compared in the risk stratification of non-ST-segment elevation chest pain patients by Newby and colleagues. The primary outcome of this trial was the relation of marker status to 30-day death and myocardial infarction. Three markers strategies were compared: (1) POC myoglobin, CKMB, and TnI, (2) POC CKMB and TnI, and (3) local laboratory. This study found that time to positivity was decreased in both POC marker strategies (2.5 hours and 2.8 hours, respectively) when compared to the local central laboratory (3.4 hours). Outcome data of 30-day death or infarction showed that POC marker strategies better identified patients at risk for adverse outcomes than the local central laboratory (positive 18.8% and 21.9% versus 13.6%). The authors concluded that POC multimarker determination provided faster and better risk stratification for this patient population.
13
In another evaluation by Wu et al, CK-MB and TnI whole blood POC assays were evaluated in a multi-center trial in 185 patients suspected of ACS compared to 180 healthy subjects.
14 Clinical sensitivity and specificity for acute
myocardial infarction (AMI) were determined using the redefined guidelines from the ESC/ACC.
15 The authors
concluded that for 39 AMI and 67 non-AMI patients, the clinical sensitivity, specificity, and diagnostic efficiency of the POC tests were similar to the predicate assays and this bedside testing was an acceptable alternative to automated central laboratory instruments. Total imprecision ranged from 7.2% to 11.4% for TnI over the range of 0.22 to 5 ng/mL and 4.8% to 8.6% for CKMB at 7, 14, and 25 ng/mL.
14
In another trial conducted by McCord et al. evaluating 817 consecutive ED patients presenting with symptoms consistent with ACS, serial determinations of myoglobin, TnI, and CKMB at 0, 1.5, 3, and 9 hours were obtained using POC testing. Sensitivity and negative predictive value were compared for both the multimarker POC approach and the central laboratory strategy. This study found that sensitivity and negative predictive value for myoglobin and TnI by 90 minutes after patient presentation was 96.9% and 99.6%, respectively. CKMB measurements did not add to this evaluation. Additionally, laboratory result reporting was on average 57 minutes faster with the POC assay.
16
Renal failure patients also represent a particularly challenging population for cardiac biomarker assessment. False positive tests complicate the assessment and diagnosis in this high-risk group. Point-of-care testing has been successfully evaluated in these patients as well. Using the same patient population as the previously mentioned study by McCullough et al, patients were divided into five groups based on their renal function. Two independent cardiologists determined the diagnosis of AMI. Troponin I was found to be the most consistent cardiac biomarker across all patient groups without significant false positive results.
17

53w w w . e m c r e g . o r g
POINT-OF-CARE TESTING FOR CARDIAC BIOMARKERS IN THE ED:A BLUEPRINT FOR IMPLEMENTATION
53w w w . e m c r e g . o r g
POINT-OF-CARE TESTING FOR CARDIAC BIOMARKERS IN THE ED:A BLUEPRINT FOR IMPLEMENTATION
In a study by Hollander et al. of patients presenting to the ED with potential ACS, the addition of BNP to the standard myocardial necrosis markers TnI, CK-MB, and myoglobin, improved detection of adverse cardiovascular outcomes observed when the cardiac biomarkers were obtained on ED arrival. The sensitivity for detecting a 30 day adverse outcome was 63% (95% CI 53-73%), specificity was 65% (95% CI 61-70%), negative predictive value 93% (95% CI 90-96%) and positive predictive value 20% (95% CI 14-26%). Using a mathematical model for integrating the results of the four cardiac biomarkers myoglobin, CK-MB, TnI, and BNP, called the multimarker index (MMX) improved the performance for detection of AMI on the initial sample compared to using the individual results of the same four cardiac biomarkers with the usual test thresholds. Table 1 shows the Area Under the Curve (AUC) for the MMX relative to the individual cardiac biomarkers at the time of ED presentation.
18,19 If the
reader wishes to have more information regarding the actual commercial assays use in these cited studies, please read the original references for each trial.
Economic Assessment ofPoint-of-Care TestingAs medicine is under constant scrutiny to provide quality medical care with reduced costs, implementation of additional laboratory services will understandably be called into question. Is POC testing cost effective? This question is central for all parties involved with implementation of such a program. Benefits of POC testing
generally fall into the major categories of consumer demand, medical care, as well as time and resource management. The ultimate goal clearly is high quality, cost-effective, and efficient health care.
Both physicians and patients demand rapid cardiac biomarker results provided by POC testing. Physicians understandably want accessible and rapid results for the diagnosis and care of their patients. Patients and their insurers want rapid and accurate diagnosis and treatment for their conditions which is cost-effective. In a world where internet, fast food, instant replay, e-mail, digital audio, cell phones, and pagers have become routine – does it not seem reasonable that laboratory results in acute care environments would return faster today than 10 years ago? At least from the patient’s perspective, the immediate return of medical information has become an expectation and a source of dissatisfaction if a delay in diagnosis occurs.
Benefits of POC testing
generally fall into the
major categories of
consumer demand,
medical care, as well
as time and resource
management. The
ultimate goal is clearly
high quality, cost-
effective, and efficient
health care.
MARKER AUC 95% CI
MMX 0.98 .97-.98
CK-MB 0.91 .90-.92
TnI 0.94 .93-.96
Myoglobin 0.78 .76-.81
BNP 0.85 .83-.88
Table 1: Comparison of area under the curve (AUC) for the multimarker index relative to individual markers at the time of ED presentation. Greater areas under the curve represent greater diagnostic accuracy.

54w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
54w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
For time sensitive high morbidity medical conditions that are frequently encountered in the ED, rapid and improved turn-around time (TAT) for laboratory tests intuitively translates into improved medical care. If POC testing can improve the ability to diagnose efficiently, more effectively utilize medical treatment, improve pharmaceutical consumption, and decrease lengths of stay in the ED, the OR, the ICU, and the hospital, improve resource utilization, then certainly an economic benefit has to be realized. These inter-
related parameters, however, can be extremely difficult to quantify. Just as in the implementation of any new intervention, the ultimate test for POC testing will be to determine its effect on these outcomes. Showing improvement of outcomes is difficult but will be imperative in the ultimate judgment of POC testing.
Most notably, the cost/benefit analysis is not as basic as simply comparing the cost of the lab result in the POC and central laboratory environments. This has traditionally been called “cost-centered analysis.” Labor and reagent costs are not the only considerations. The focus
of POC testing should be medical care and systems costs, not the very isolated cost of the test itself. The viewpoint of a global evaluation of the entire cost of a health care episode with an outcomes-oriented approach is imperative. Even with the efforts of trying to find an answer to this question, very little is understood regarding what POC testing actually accomplishes in terms of benefits and outcomes.
In one evaluation, Blick used cardiac biomarkers myoglobin, CK-MB, TnI, and BNP determined by a POC platform compared to central laboratory testing.
Improvements in clinical outcome, operations, and economic benefits were realized when efficient protocols for ACS and heart failure were combined with ED POC testing. Length of stay (LOS) in the ED was reduced from approximately 15 hours to 8 hours for evaluation of patients with possible non-ST-segment elevation AMI. Combining 0 and 2 hour POC testing in an ED chest pain unit, the time to discharge of patients was reduced from 3.6 to 2.3 hours. For in-patient heart failure patients, LOS was reduced from 5.2 to 3.2 days, saving approximately $1,000 per patient.
20
Another study by Apple et al. noted substantial decrease in charges associated with POC testing using cardiac biomarkers. In this trial using POC TnI, a trend for substantial reduction in patient charges was seen when 271 patients in the central laboratory evaluation portion of the trial were compared to 274 patients evaluated using POC TnI testing. These decreased charges were noted in room, pharmacy, laboratory, non-cardiac procedures, and cardiac procedures.
21
The Time IssueDecreased TAT is the central issue in POC testing. Lee-Lewandrowski et al. showed an 84.5% reduction in TAT using a qualitative POC TnI assay which translated into a LOS reduction from 386 to 338 minutes.
22 Likewise, Caragher
et al, showed a TAT reduction of 55% compared to the central laboratory using the quantitative POC assays for TnI, CKMB, and myoglobin.
23
Point-of-care assays can perform tests faster. While it is intuitive that a test performed at the bedside in 10 minutes would take less time than a test that has traditionally required 60 minutes, these studies illustrate that TAT can be decreased (with POC testing) in the acute patient setting due to the significant impact of minimizing pre-analytical preparation of the specimen and central laboratory handling.
TAT can be decreased
in the acute patient
setting (with POC
testing) due to the
significant impact of
minimizing pre-analytical
preparation of the
specimen and central
laboratory handling.

55w w w . e m c r e g . o r g
POINT-OF-CARE TESTING FOR CARDIAC BIOMARKERS IN THE ED:A BLUEPRINT FOR IMPLEMENTATION
55w w w . e m c r e g . o r g
POINT-OF-CARE TESTING FOR CARDIAC BIOMARKERS IN THE ED:A BLUEPRINT FOR IMPLEMENTATION
Figure 1: Collection time to test results in patients
presenting with chest pain, shortness of breath or
acute coronary syndrome.
In a pilot trial conducted at two tertiary care institutions comparing POC testing for TnI to an historical central laboratory-based approach, POC testing substantially reduced the collection time for the blood specimen to test results obtained by the emergency physician by 51% for 3759 patients in the historical central laboratory control group and 3626 patients in the trial group for the busy community hospital and 60% for the major urban teaching hospital. Point-of-care testing used a multiple test approach with myoglobin, CK-MB, TnI and BNP for patients with chest pain, shortness of breath and possible ACS (Figure 1). This reduction TAT resulted in a substantial decrease in LOS for both patients receiving a single marker draw, often subsequently discharged from the ED, and also for admitted patients (Figures 2 and 3). 24
Does this decrease in laboratory TAT matter? The analysis of POC testing is only as robust as the clinical assumption that fast diagnosis and treatment is better for patients. From numerous studies we know that early intervention and medical treatment is beneficial
for patients with non-ST-segment elevation ACS.2,3,25
A reduction in ED LOS is also a critical factor for potential implementation of a POC system. Singer et al. demonstrated a reduced ED LOS of 68 minutes for potential ACS patients after implementation of a POC cardiac marker system.
26 The success and
benefits of POC testing clearly require that action be taken on the results obtained (Figure 4).
Stakeholders Required for Implementing POC Testing in the EDTo successfully implement POC testing in the ED, it is essential to recognize and involve the various stakeholders for cardiac biomarker testing from the beginning. Multiple viewpoints have recently been published which describe aspects of the implementation process for POC testing.
27-32 The
stakeholders from an institution should meet and discuss the available publications on POC testing which will include information from the Emergency Medicine, Cardiology, Laboratory Medicine, and Hospital Administration literature such as provided in this Newsletter. A meeting of these

56w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
56w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
Figure 2: Emergency department length-of-stay for patients presenting with chest pain, shortness of breath or acute coronary syndrome with one set of markers drawn.
Figure 3: Emergency department length-of-stay for for admitted patients presenting with chest pain, shortness of breath or acute coronary syndrome and one set of ma-rkers drawn.
Community Hospital Center Urban Teaching Center18
Community Hospital Center Urban Teaching Center

57w w w . e m c r e g . o r g
POINT-OF-CARE TESTING FOR CARDIAC BIOMARKERS IN THE ED:A BLUEPRINT FOR IMPLEMENTATION
57w w w . e m c r e g . o r g
POINT-OF-CARE TESTING FOR CARDIAC BIOMARKERS IN THE ED:A BLUEPRINT FOR IMPLEMENTATION
TIME
ClinicalQuestion
Test Result Action PatientOutcome
"POC testing has value only if caregivers take action on the result."
Figure 4: Model for Point-of-Care
Testing
individuals from a variety of disciplines will allow a consensus to be developed for moving forward and an understanding of the possible impediments to successful implementation of POC testing.
Emergency Physicians and CardiologistsTypically the emergency physician first recognizes that a more expeditious TAT for cardiac biomarkers is necessary for patients in the ED. Based on the 2002 ACC/AHA Guidelines for Non-ST-segment elevation ACS, cardiologists also are willing to support this initiative. It is important for the clinicians to emphasize the necessity for improving TAT to decrease the time required for diagnosis of myocardial necrosis which can reduce time for both admission and discharge disposition decisions. In addition, a positive troponin result indicates patients at high risk for ischemic complications which drives the use of anti-thrombotic therapy such as heparin, low molecular heparin and bivalirudin as well as anti-platelet agents including clopidogrel and glycoprotein IIb/IIIa inhibitors. In addition, at many institutions, a positive troponin level will serve as evidence for the need to admit a patient to an intensive care unit versus a step-down unit or monitored bed.
LaboratoriansClinical chemists and pathologists should be integrally involved in the evaluation and implementation of POC for the emergency setting. It is usually necessary for these specialists to provide
a baseline evaluation of the POC test to be used in the ED. Often, a pilot trial will provide the necessary TAT and test result data required to analyze the practicality of a POC program. Suggested measures to evaluate a pilot trial’s outcome include TAT, test assay accuracy (sensitivity, specificity, positive and negative predictive value), costs for care including admitted patients and patients released from the ED, and care outcomes including time to admission, time to release, time to receiving therapy in the ED, time to the cardiac catheterization laboratory, and also clinical outcomes such as revascularization, repeat myocardial infarction in-hospital, and death. It should be recognized and anticipated, that true clinical outcome differences (revascularization, repeat myocardial infarction in-hospital, and death) will be difficult to achieve in comparing POC testing to standard central laboratory testing due to the small number of patients in each group. Time data and cost calculations, however, should be very important in demonstrating differences despite small numbers of patients.
Pre-POC test TATs should be calculated and then compared to post-POC test TATs to establish the difference between these two approaches. After implementation of POC testing as a standard approach, monitoring these data will continuously improve the process of cardiac biomarker testing in an ED. All laboratory testing within the hospital requires compliance with the Clinical Laboratory

58w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
58w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
Improvement Amendment (CLIA) of 1988 which provides standards of quality to ensure accuracy of the results. Point-of-care tests are compared by laboratorians to the central laboratory version of the same cardiac biomarker assay to ensure that the assays provide the accurate test result information needed to make clinical decisions appropriately. In addition, POC tests currently being marketed are sufficiently straightforward such that individuals such as nurses and patient care assistants, not highly trained laboratory technicians, can perform the assays and achieve high quality accurate results. The laboratory’s involvement in routine checks of the POC equipment and assays, as well as routine checks of the test accuracy as well as proper patient identification are essential. In addition, laboratorians should require an electronic connection between the POC device in the ED and the laboratory information system. Not only does this ensure that POC test results performed in the ED become part of the medical record for patient care purposes, appropriate billing for these important tests can be performed. The acceptance of POC test results are also improved when results are available from the electronic medical record as all other central laboratory results are provided. An excellent relationship with strong collaboration between the clinicians and laboratorians is therefore essential for implementation of a POC program in a particular hospital setting.
Hospital AdministratorsUsually POC tests are, per unit, more expensive than tests run on “batch” central laboratory analyzers. Hospital administrators should therefore be involved in this POC implementation process from the beginning, including financial officers from the hospital, to demonstrate validity of cost savings and process improvement. Clinical effectiveness and six sigma process experts can help design the hospital pilot trial and subsequent long term implementation of POC testing in a fashion which maximizes the beneficial effects of the program to minimize costs and maximize efficiency. It is helpful for hospital
administrators to feel comfortable with the cost savings achieved globally in their hospital despite the fact that an individual POC test may be 3-4 times more expensive than the central laboratory mass analyzer version of the test. In absolute terms, however, the cost of the individual POC test usually is minimal in comparison to the costs of significant disposition decisions such as admission to a step-down bed or monitored bed versus an intensive care bed, or improving ED throughput which decreases ED walk-outs.
Strengths and LimitationsIt is important to note that POC testing supplements testing from the central laboratory. Some environments benefit more and are more conducive to POC testing. While the need for more rapid results is clear, the already burdened ED environment is challenging for non-laboratory personnel such as nurses or patient care assistants required to perform rapid and high quality tests. Ideally, the hospital laboratorian will be supportive of the POC testing initiative at an institution and provide expertise on the technical evaluation of the POC assay compared to the currently used central laboratory assay as well as help with implementation and analysis of the new bedside laboratory tests performed in the ED. These individuals are specially trained in quality control and assurance for laboratory testing and can assist in the complex implementation of POC systems (Table 2). From previous studies, it is clear that POC assays for cardiac biomarkers are effective in the emergency setting for evaluation ACS. The ACC and AHA recommend the cardiac specific troponins for the triage and treatment of patients with potential ACS. As even the most minor of elevations of troponin portend increased risk, how accurate does a POC test have to be to be useful clinically? Trials such as TACTICS TIMI-18 have shown that patients with troponin levels above the 99th cutoff percentile but below the 10% CV value are at increased risk.
33
Other studies and reviews have documented the value of POC testing for cardiac biomarkers in the emergency setting and for risk stratification.
34-40 It is
important for emergency physicians to understand
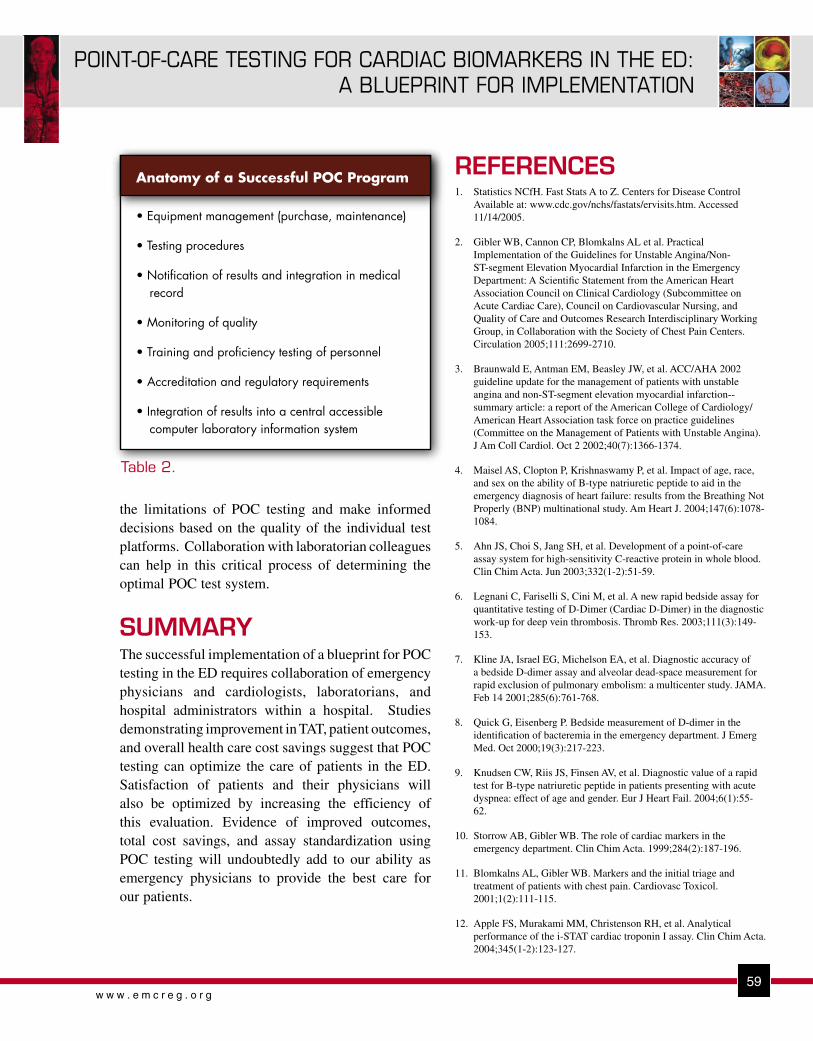
59w w w . e m c r e g . o r g
POINT-OF-CARE TESTING FOR CARDIAC BIOMARKERS IN THE ED:A BLUEPRINT FOR IMPLEMENTATION
59w w w . e m c r e g . o r g
POINT-OF-CARE TESTING FOR CARDIAC BIOMARKERS IN THE ED:A BLUEPRINT FOR IMPLEMENTATION
the limitations of POC testing and make informed decisions based on the quality of the individual test platforms. Collaboration with laboratorian colleagues can help in this critical process of determining the optimal POC test system.
SUMMARYThe successful implementation of a blueprint for POC testing in the ED requires collaboration of emergency physicians and cardiologists, laboratorians, and hospital administrators within a hospital. Studies demonstrating improvement in TAT, patient outcomes, and overall health care cost savings suggest that POC testing can optimize the care of patients in the ED. Satisfaction of patients and their physicians will also be optimized by increasing the efficiency of this evaluation. Evidence of improved outcomes, total cost savings, and assay standardization using POC testing will undoubtedly add to our ability as emergency physicians to provide the best care for our patients.
REFERENCES1. Statistics NCfH. Fast Stats A to Z. Centers for Disease Control
Available at: www.cdc.gov/nchs/fastats/ervisits.htm. Accessed 11/14/2005.
2. Gibler WB, Cannon CP, Blomkalns AL et al. Practical Implementation of the Guidelines for Unstable Angina/Non-ST-segment Elevation Myocardial Infarction in the Emergency Department: A Scientific Statement from the American Heart Association Council on Clinical Cardiology (Subcommittee on Acute Cardiac Care), Council on Cardiovascular Nursing, and Quality of Care and Outcomes Research Interdisciplinary Working Group, in Collaboration with the Society of Chest Pain Centers. Circulation 2005;111:2699-2710.
3. Braunwald E, Antman EM, Beasley JW, et al. ACC/AHA 2002 guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction--summary article: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on the Management of Patients with Unstable Angina). J Am Coll Cardiol. Oct 2 2002;40(7):1366-1374.
4. Maisel AS, Clopton P, Krishnaswamy P, et al. Impact of age, race, and sex on the ability of B-type natriuretic peptide to aid in the emergency diagnosis of heart failure: results from the Breathing Not Properly (BNP) multinational study. Am Heart J. 2004;147(6):1078-1084.
5. Ahn JS, Choi S, Jang SH, et al. Development of a point-of-care assay system for high-sensitivity C-reactive protein in whole blood. Clin Chim Acta. Jun 2003;332(1-2):51-59.
6. Legnani C, Fariselli S, Cini M, et al. A new rapid bedside assay for quantitative testing of D-Dimer (Cardiac D-Dimer) in the diagnostic work-up for deep vein thrombosis. Thromb Res. 2003;111(3):149-153.
7. Kline JA, Israel EG, Michelson EA, et al. Diagnostic accuracy of a bedside D-dimer assay and alveolar dead-space measurement for rapid exclusion of pulmonary embolism: a multicenter study. JAMA. Feb 14 2001;285(6):761-768.
8. Quick G, Eisenberg P. Bedside measurement of D-dimer in the identification of bacteremia in the emergency department. J Emerg Med. Oct 2000;19(3):217-223.
9. Knudsen CW, Riis JS, Finsen AV, et al. Diagnostic value of a rapid test for B-type natriuretic peptide in patients presenting with acute dyspnea: effect of age and gender. Eur J Heart Fail. 2004;6(1):55-62.
10. Storrow AB, Gibler WB. The role of cardiac markers in the emergency department. Clin Chim Acta. 1999;284(2):187-196.
11. Blomkalns AL, Gibler WB. Markers and the initial triage and treatment of patients with chest pain. Cardiovasc Toxicol. 2001;1(2):111-115.
12. Apple FS, Murakami MM, Christenson RH, et al. Analytical performance of the i-STAT cardiac troponin I assay. Clin Chim Acta. 2004;345(1-2):123-127.
Table 2.
Anatomy of a Successful POC Program
• Equipment management (purchase, maintenance)
• Testing procedures
• Notification of results and integration in medical record
• Monitoring of quality
• Training and proficiency testing of personnel
• Accreditation and regulatory requirements
• Integration of results into a central accessible computer laboratory information system

60w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
13. Newby LK, Storrow AB, Gibler WB, et al. Bedside multimarker testing for risk stratification in chest pain units: The chest pain evaluation by creatine kinase-MB, myoglobin, and troponin I (CHECKMATE) study. Circulation. 10 2001;103(14):1832-1837.
14. Wu AH, Smith A, Christenson RH, et al. Evaluation of a point-of-care assay for cardiac markers for patients suspected of acute myocardial infarction. Clin Chim Acta. 16 2004;346(2):211-219.
15. Myocardial infarction redefined--a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. Eur Heart J. 2000;21(18):1502-1513.
16. McCord J, Nowak RM, McCullough PA, et al. Ninety-minute exclusion of acute myocardial infarction by use of quantitative point-of-care testing of myoglobin and troponin I. Circulation. 2001;104(13):1483-1488.
17. McCullough PA, Nowak RM, Foreback C, et al. Performance of multiple cardiac biomarkers measured in the emergency department in patients with chronic kidney disease and chest pain. Acad Emerg Med. 2002;9(12):1389-1396.
18. Hollander JE, Sease KL, Robey JL. The addition of B-type natriuretic peptide to markers of myocardial injury improves sensitivity for immediate detection of 30-day advers outcomes. Acad. Emerg. Med. 2005; 12 (5 suppl .1) 33. Abs.
19. Hollander JE, Peacock WF, Shofer FS, et al. A cardiac multimarker index performs better than standard markers to diagnose acute myocardial infarction. Acad. Emerg. Med. 2005; 12(5 suppl. 1) :33. Abs.
20. Blick KE. Economics of Point-of-Care (POC) testing for cardiac markers and B-Natriuretic Peptide (BNP). Point of Care 2005;4:11-14.
21. Apple FS, Chung AY, Kogut ME et al. Decreased patient charges following implementation of point-of-care cardiac troponin monitoring in acute coronary syndrome patients in a community hospital cardiology unit. Clinica Chimica Acta 2006. Available online March 6, 2006.
22. Lee-Lewandrowski E, Corboy D, Lewandrowski K, et al. Implementation of a point-of-care satellite laboratory in the emergency department of an academic medical center. Impact on test turnaround time and patient emergency department length of stay. Arch Pathol Lab Med. 2003;127(4):456-460.
23. Caragher TE, Fernandez BB, Jacobs FL, et al. Evaluation of quantitative cardiac biomarker point-of-care testing in the emergency department. J Emerg Med. 2002;22(1):1-7.
24. Gibler WB and Rohlfing R. Unpublished POC trial data. 2006.
25. Cannon CP, Weintraub WS, Demopoulos LA, et al. Comparison of early invasive and conservative strategies in patients with unstable coronary syndromes treated with the glycoprotein IIb/IIIa inhibitor tirofiban. N Engl J Med. 2001;344(25):1879-1887.
26. Singer AJ, Ardise J, Gulla J, et al. Point-of-care testing reduces length of stay in emergency department chest pain patients. Ann Emerg Med. 2005;45(6):587-591.
27. Sieck S. The evolution of a new standard of hospital care: Paradigm shift to the emergency department and the role of point-of-care testing. Point Care J Near-Patient Testing Technol 2006;5:2-4.
28. Christenson RH. Insights into development of the National Academy of Clinical Biochemistry laboratory medicine practice guidelines for point-of-care testing for biomarkers of cardiac injury. Point Care J Near-Patient Testing Technol 2006; 5:13-18.
29. Wu AHB. Point-of-care testing for conventional cardiac markers. Point Care J Near-Patient Testing Technol 2006; 5:20-24.
30. Apple FS. Point-of-care cardiuac troponin T: Process improvements for detection of acute myocardial infarction. Point Care J Near-Patient Testing Technol 2006; 5:25-27.
31. Martinez A, Januzzi JL. Novel markers for the evaluation of patients with suspected ischemic heart disease. Point Care J Near-Patient Testing Technol 2006; 5:28-37.
32. Sluss PM. Cardiac markers:current technologies for their measurement at points of care. Point Care J Near-Patient Testing Technol 2006; 5:38-46.
33. Morrow DA, Cannon CP, Rifai N, et al. Ability of minor elevations of troponins I and T to predict benefit from an early invasive strategy in patients with unstable angina and non-ST elevation myocardial infarction: results from a randomized trial. JAMA. 2001;286(19):2405-2412.
34. Agewall S. Evaluation of point-of-care test systems using the new definition of myocardial infarction. Clin Biochem. 2003;36(1):27-30.
35. Apple FS, Murakami MM, Jesse RL, et al. Near-bedside whole-blood cardiac troponin I assay for risk assessment of patients with acute coronary syndromes. Clin Chem. 2002;48(10):1784-1787.
36. Apple FS, Wu AHB, Mair J, et al. Future Biomarkers for the detection of ischemia and risk stratification in acute coronary syndrome. Clin Chem 2005; 51:810-824.
37. Kost GJ, Tran NK. Point-of-care testing and cardiac biomarkers: The standard of care and vision for chest pain centers. Cardiol Clin 2005; 467-490.
38. Amos A and Newby LK. Using biomarkers to assess risk and consider treatment strategies in non-ST-segment elevation acute coronary syndromes. Current Cardiol Reports 2005; 7:263-269.
39. Di Serio FD, Amodio G, Varraso L et al. Integration between point-of-care markers in an emergency/cardiology department and the central laboratory: methodological and preliminary clinical evaluation. Clin Chem Lab Med 2005; 43: 202-209.
40. Ordonez-Llanos J, Santalo-Bel M, Merce-Muntanola J et al. Risk stratification of chest pain patients by poit-of-care cardiac troponin T and myoglobin measured in the emergency department. Clin Chim Acta 2006; 365:93-97.
Copyright EMCREG-International, 2007

61w w w . e m c r e g . o r g
HYPERTENSION MANAGEMENT IN ACUTE NEUROVASCULAR EMERGENCIES
OBJECTIVES:1. Describe the rationale for lowering blood pressure in hypertensive neurovascular
emergencies.2. Describe the potential harm in lowering blood pressure in hypertensive neurovascular
emergencies.3. Define the agents of choice in managing hypertensive neurovascular emergencies.
INTRODUCTIONManagement of blood pressure in the setting of neurovascular emergencies is of considerable concern to emergency physicians. It is an area of medicine with remarkably little clinical trial data from which to derive evidence-based treatment approaches. Thus, clinicians must rely on an understanding of the underlying pathophysiology and the mechanism of action of therapeutic agents to drive treatment decisions.
When treating patients with neuro-vascular emergencies and hypertension, two competing concerns must be balanced. The first is the concern that acutely elevated blood pressure can lead to injury in multiple vascular beds, including hemorrhage in the brain and elsewhere. The second is the concern that reduction of blood pressure can compromise tissue with marginal perfusion. Factors that must be considered in deciding whether to lower the patient’s blood pressure, and if so to what degree, include 1) the type of neurovascular emergency, 2) the level of hypertension, 3) the patient’s
Factors that must be
considered in deciding
whether to lower the
patient’s blood pressure,
and if so to what
degree, include 1) the
type of neurovascular
emergency, 2) the level
of hypertension, 3) the
patient’s past blood
pressure history, and 4)
the perceived condition of
the patient’s native
autoregulatory system.
past blood pressure history, and 4) the perceived condition of the patient’s native autoregulatory system.
The three types of neurovascular emergencies that will be considered here are acute ischemic stroke, intracerebral hemorrhage and subarachnoid hemorrhage. While all falling into the category of neurovascular emergencies, the underlying pathologies differ considerably as will the blood pressure management decisions required to treat them.
PathophysiologyBefore addressing the individual neurovascular emergencies, some underlying principles must be outlined. First, neuronal tissue has a very high metabolic demand and therefore it requires continuous high volume blood flow. Normal blood flow to the human cerebral cortex averages 50ml of blood flow / 100 grams of brain tissue / minute (expressed as: ml/100 g/min).1 At levels of perfusion less than 20 ml/100 g/min, neuronal cell membranes become impaired with resulting neurological
Arthur M. Pancioli, MD Vice Chairman of Research, Associate Professor, Department of Emergency Medicine,
University of Cincinnati College of Medicine, Cincinnati, OH, Member, Greater Cincinnati/Northern Kentucky Stroke Team
HYPERTENSION MANAGEMENT IN ACUTE NEUROVASCULAR EMERGENCIES
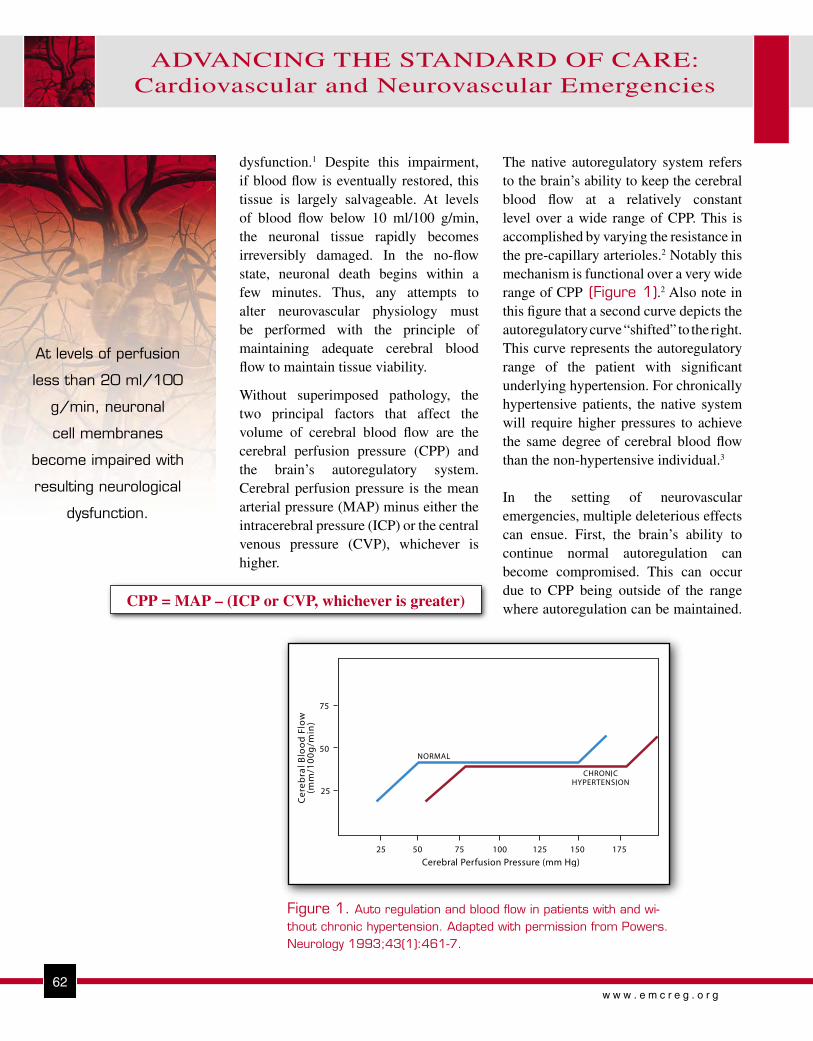
62w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
Figure 1. Auto regulation and blood flow in patients with and wi-thout chronic hypertension. Adapted with permission from Powers. Neurology 1993;43(1):461-7.
dysfunction.1 Despite this impairment, if blood flow is eventually restored, this tissue is largely salvageable. At levels of blood flow below 10 ml/100 g/min, the neuronal tissue rapidly becomes irreversibly damaged. In the no-flow state, neuronal death begins within a few minutes. Thus, any attempts to alter neurovascular physiology must be performed with the principle of maintaining adequate cerebral blood flow to maintain tissue viability.
Without superimposed pathology, the two principal factors that affect the volume of cerebral blood flow are the cerebral perfusion pressure (CPP) and the brain’s autoregulatory system. Cerebral perfusion pressure is the mean arterial pressure (MAP) minus either the intracerebral pressure (ICP) or the central venous pressure (CVP), whichever is higher.
The native autoregulatory system refers to the brain’s ability to keep the cerebral blood flow at a relatively constant level over a wide range of CPP. This is accomplished by varying the resistance in the pre-capillary arterioles.2 Notably this mechanism is functional over a very wide range of CPP (Figure 1).2 Also note in this figure that a second curve depicts the autoregulatory curve “shifted” to the right. This curve represents the autoregulatory range of the patient with significant underlying hypertension. For chronically hypertensive patients, the native system will require higher pressures to achieve the same degree of cerebral blood flow than the non-hypertensive individual.3
In the setting of neurovascular emergencies, multiple deleterious effects can ensue. First, the brain’s ability to continue normal autoregulation can become compromised. This can occur due to CPP being outside of the range where autoregulation can be maintained.
At levels of perfusion
less than 20 ml/100
g/min, neuronal
cell membranes
become impaired with
resulting neurological
dysfunction.
CPP = MAP – (ICP or CVP, whichever is greater)
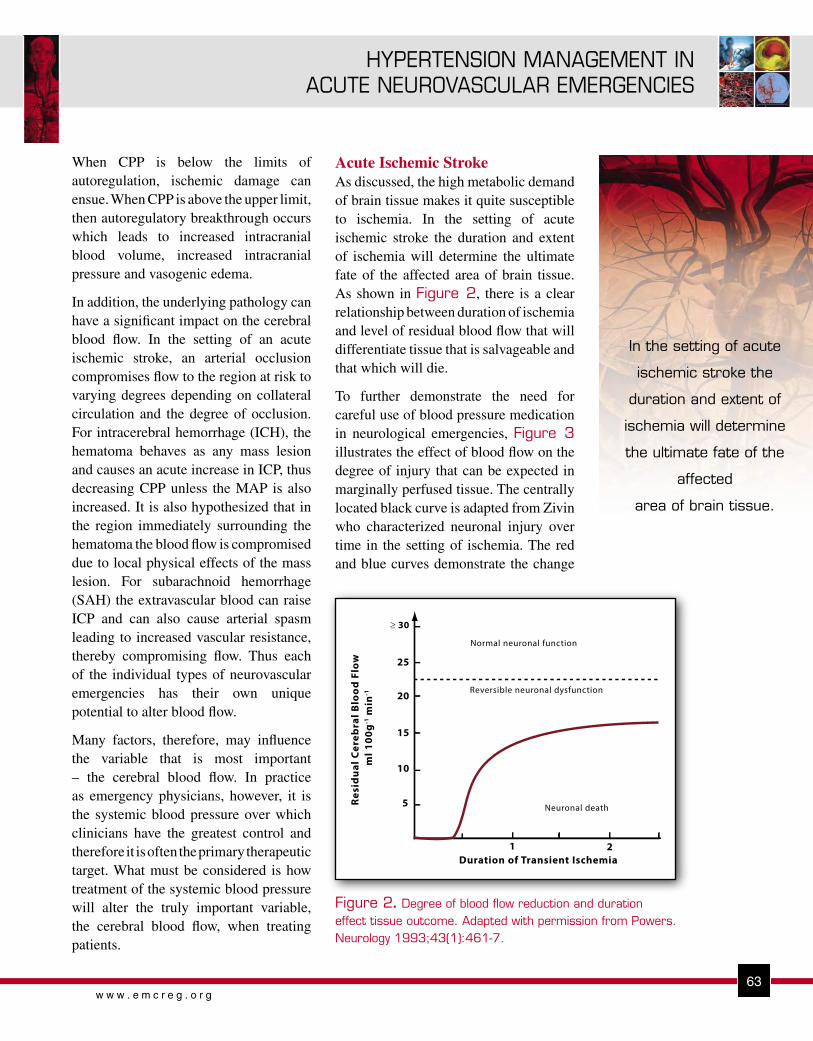
6363w w w . e m c r e g . o r g
HYPERTENSION MANAGEMENT IN ACUTE NEUROVASCULAR EMERGENCIES
When CPP is below the limits of autoregulation, ischemic damage can ensue. When CPP is above the upper limit, then autoregulatory breakthrough occurs which leads to increased intracranial blood volume, increased intracranial pressure and vasogenic edema.
In addition, the underlying pathology can have a significant impact on the cerebral blood flow. In the setting of an acute ischemic stroke, an arterial occlusion compromises flow to the region at risk to varying degrees depending on collateral circulation and the degree of occlusion. For intracerebral hemorrhage (ICH), the hematoma behaves as any mass lesion and causes an acute increase in ICP, thus decreasing CPP unless the MAP is also increased. It is also hypothesized that in the region immediately surrounding the hematoma the blood flow is compromised due to local physical effects of the mass lesion. For subarachnoid hemorrhage (SAH) the extravascular blood can raise ICP and can also cause arterial spasm leading to increased vascular resistance, thereby compromising flow. Thus each of the individual types of neurovascular emergencies has their own unique potential to alter blood flow.
Many factors, therefore, may influence the variable that is most important – the cerebral blood flow. In practice as emergency physicians, however, it is the systemic blood pressure over which clinicians have the greatest control and therefore it is often the primary therapeutic target. What must be considered is how treatment of the systemic blood pressure will alter the truly important variable, the cerebral blood flow, when treating patients.
Acute Ischemic StrokeAs discussed, the high metabolic demand of brain tissue makes it quite susceptible to ischemia. In the setting of acute ischemic stroke the duration and extent of ischemia will determine the ultimate fate of the affected area of brain tissue. As shown in Figure 2, there is a clear relationship between duration of ischemia and level of residual blood flow that will differentiate tissue that is salvageable and that which will die.
To further demonstrate the need for careful use of blood pressure medication in neurological emergencies, Figure 3 illustrates the effect of blood flow on the degree of injury that can be expected in marginally perfused tissue. The centrally located black curve is adapted from Zivin who characterized neuronal injury over time in the setting of ischemia. The red and blue curves demonstrate the change
In the setting of acute
ischemic stroke the
duration and extent of
ischemia will determine
the ultimate fate of the
affected
area of brain tissue.
30
25
20
15
10
5
21Duration of Transient Ischemia
Res
idu
al C
ereb
ral B
loo
d F
low
ml 1
00g
-1 m
in-1
Normal neuronal function
Reversible neuronal dysfunction
Neuronal death
Figure 2. Degree of blood flow reduction and duration effect tissue outcome. Adapted with permission from Powers. Neurology 1993;43(1):461-7.
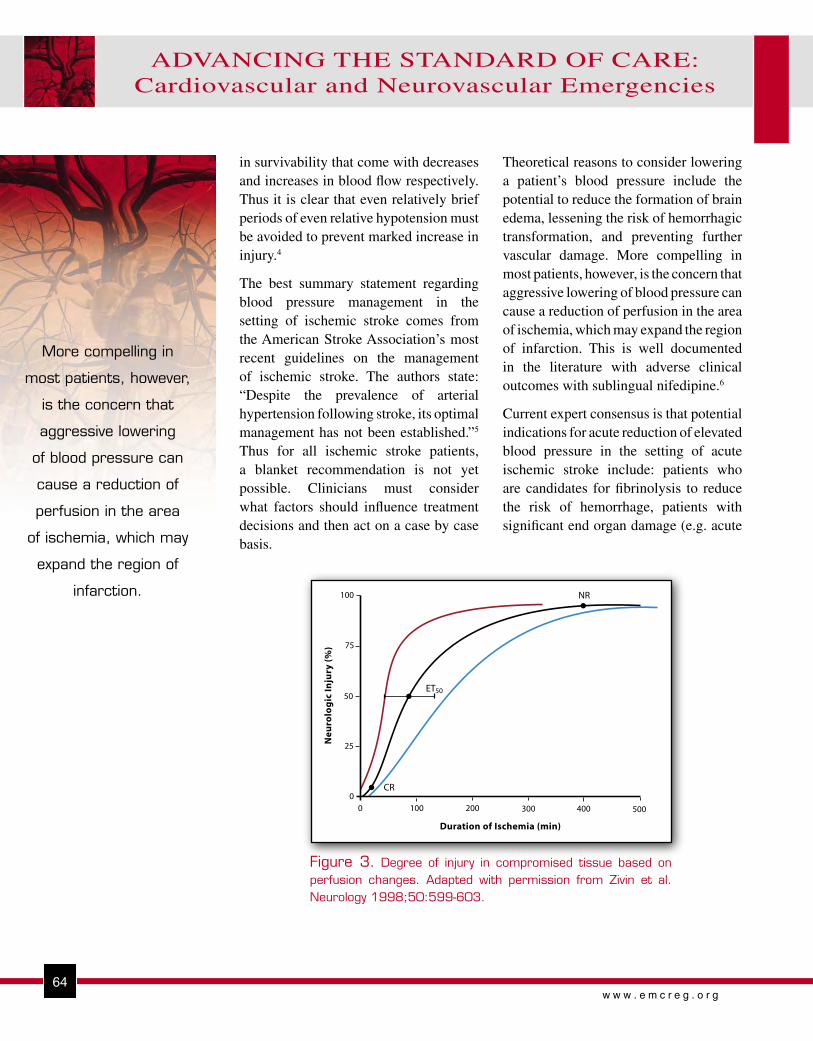
64w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
in survivability that come with decreases and increases in blood flow respectively. Thus it is clear that even relatively brief periods of even relative hypotension must be avoided to prevent marked increase in injury.4
The best summary statement regarding blood pressure management in the setting of ischemic stroke comes from the American Stroke Association’s most recent guidelines on the management of ischemic stroke. The authors state: “Despite the prevalence of arterial hypertension following stroke, its optimal management has not been established.”5 Thus for all ischemic stroke patients, a blanket recommendation is not yet possible. Clinicians must consider what factors should influence treatment decisions and then act on a case by case basis.
Theoretical reasons to consider lowering a patient’s blood pressure include the potential to reduce the formation of brain edema, lessening the risk of hemorrhagic transformation, and preventing further vascular damage. More compelling in most patients, however, is the concern that aggressive lowering of blood pressure can cause a reduction of perfusion in the area of ischemia, which may expand the region of infarction. This is well documented in the literature with adverse clinical outcomes with sublingual nifedipine.6
Current expert consensus is that potential indications for acute reduction of elevated blood pressure in the setting of acute ischemic stroke include: patients who are candidates for fibrinolysis to reduce the risk of hemorrhage, patients with significant end organ damage (e.g. acute
NR
ET
CR
100
75
50
25
00 100 200 300 400 500
Duration of Ischemia (min)
Ne
uro
log
ic In
jury
(%
)
50
Figure 3. Degree of injury in compromised tissue based on perfusion changes. Adapted with permission from Zivin et al. Neurology 1998;50:599-603.
More compelling in
most patients, however,
is the concern that
aggressive lowering
of blood pressure can
cause a reduction of
perfusion in the area
of ischemia, which may
expand the region of
infarction.

6565w w w . e m c r e g . o r g
HYPERTENSION MANAGEMENT IN ACUTE NEUROVASCULAR EMERGENCIES
myocardial infarction, aortic dissection, hypertensive encephalopathy, acute renal failure, acute pulmonary edema, etc.), or patients with extremes of blood pressure (systolic above 220 or diastolic above 120).5
The clearest indication for blood pressure lowering in the setting of acute ischemic stroke is in patients who are candidates for fibrinolytic therapy. In this population, elevated blood pressure significantly increases the risk of intracerebral hemorrhage. Fibrinolytic therapy should not be given to patients who have a systolic blood pressure >185 mm Hg or a diastolic blood pressure >110 mm Hg at the time of treatment.5,7 Often stroke patients arrive with very elevated blood pressure, but it may fall within these parameters after a few minutes without specific therapy. If not, guidelines for fibrinolytic therapy allow for treatment of the blood pressure with relatively modest measures, including intravenous labetalol boluses, enalaprilat and some centers are now using nicardipine infusion. However, very aggressive interventions to lower blood pressure should not be used, so if the above measures are not effective in achieving the blood pressure targets, then fibrinolytic therapy is contraindicated. If the patient is treated with a fibrinolytic, the blood pressure must be maintained <180/105 for the next 24 hours, using any or all of the agents described below.7
If the decision is made to treat the elevated blood pressure of a patient with acute ischemic stroke, then lowering the blood pressure should be performed cautiously. The agent of choice should be easily titratable to avoid erratic or precipitous declines in blood pressure and ideally would have minimal vasodilatory effect on the cerebral vessels to avoid increasing ICP. Agents with such properties include: nicardipine, labetalol, esmolol and enalaprilat. These agents are potentially useful in all of the hypertensive, neurovascular emergencies and are detailed later in this newsletter.
Intracerebral HemorrhageMultiple studies of ICH document an association between elevated blood pressure at presentation and poor outcomes.8-10 Data are mixed as to whether there is a relationship between elevated blood pressure at
presentation and subsequent hematoma growth.11 Further, studies have demonstrated that hematoma growth in ICH is a significant marker for worse outcomes.11 Thus, clinicians could immediately conclude that if blood pressure is reduced, poor outcomes can be decreased either by reducing hemorrhage growth or through other factors.
While this makes intuitive sense and may well be correct, the science to prove this hypothesis is sparse. Controversy remains as studies report conflicting conclusions. As an example, one prospective series studying hematoma growth did not find a relationship between presenting hemodynamic variables and hematoma growth.12 Also, while lowering elevated blood pressure may seem to be a logical treatment, one study found that the more rapid the decline in MAP over the first 24 hours, the higher the mortality.13 Thus if the choice is made to lower blood pressure, it must be performed with extreme caution.
The final concern that has existed in the medical literature is that an area around the hematoma exists where cerebral blood flow is reduced. If this were true, then lowering the blood pressure would increase any ischemic damage in the peri-hematomal tissue. To date, however, both positron emission tomography and magnetic resonance imaging studies have not documented this phenomenon and in fact peri-hematomal autoregulation appears to be generally intact.14,15 Thus, this theoretical concern may not have merit and blood pressure lowering, for this purpose, is likely to be safe.
Clinicians currently have guidelines from expert consensus panels that recommend that for a patient with ICH and a history of hypertension, the MAP should be maintained less than 130 mmHg. Some clinicians, including the authors of this manuscript, believe this target may be too high, and typically aim for a MAP less than 110 mmHg in practice. For patients who have undergone craniotomy, the MAP should be maintained under 100 mmHg. In all cases, MAP should be maintained above 90 mmHg, and the CPP should be maintained above 70 mmHg.16 Physicians should also realize that pain control may significantly reduce blood pressure in these patients.

66w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
66
Subarachnoid HemorrhageAneurysmal SAH is the one type of neurovascular emergency of which clinicians should absolutely treat elevated blood pressure. Patients with aneurysmal SAH, who do not receive definitive treatment for their aneurysm, have a risk of rebleeding of 20% at 2 weeks and 30% at one month.17 While there is little evidence that uncontrolled blood pressure increases that risk, the potential is all too logical. Clearly, extremes of blood pressure at admission (MAP> 130 or <70 mmHg) have been associated with poor outcomes.18 One study reports a linear relationship between early rebleeding and increasing SBP above 160 mmHg.19 Currently, most physicians caring for aneurysmal SAH treat elevated blood pressure when the patients MAP is above 130 and try to maintain the SBP below 160 mmHg. Prior to treatment with any antihypertensive agent, pain control and sedation should be considered followed by a careful reassessment of blood pressure. Agents such as fentanyl for conscious patients and propofol for patients who are intubated are excellent options. Once the decision is made to therapeutically lower blood pressure, agents that are titratable, and for SAH specifically have minimal cardiovascular side
effects, such as esmolol, labetalol and nicardipine, are currently the best options.
The AgentsAs previously described there are four agents that reduce blood pressure in a titratable fashion and do not lead to increases in intracranial pressure. These are nicardipine, labetalol, esmolol and enalaprilat (Table 1). Each of these drugs works by different mechanisms and therefore may be of benefit to different patients.
NicardipineNicardipine is a calcium ion influx inhibitor (slow channel blocker or calcium channel blocker). Nicardipine inhibits the transmembrane influx of calcium ions into cardiac muscle and smooth muscle without changing serum calcium concentrations. The contractile processes of cardiac muscle and vascular smooth muscle are dependent upon the movement of extracellular calcium ions into these cells through specific ion channels. The effects of nicardipine are more selective for vascular smooth muscle than cardiac muscle. Thus, nicardipine produces a dose-dependent decrease in systemic vascular resistance.
Table 1. Titratable agents for hypertensive cerebrovascular emergencies
���� ��������� ���� �����
�����������������
����������� ������ ��� ���� ���� �������� ���� ��������������������
��������� ��� ��� ������������� ����� �� ����� ���� �������� �� ������ �� ��� ��� �������������� ��������
������� ������������� ��� ����� ������ ��� ��������� �����������������
����������� ��� ��������� ����� �� ������ ���� ����� ��������� �� ����� � �

6767w w w . e m c r e g . o r g
HYPERTENSION MANAGEMENT IN ACUTE NEUROVASCULAR EMERGENCIES
Nicardipine has been shown to be as effective as sodium nitroprusside in controlling blood pressure, but requires fewer dose titrations and does not increase ICP. It has therefore supplanted sodium nitroprusside as a treatment for acute neurovascular emergencies.
Dosage is individualized based on the severity of the patient’s hypertension and the goals for therapy. For gradual reduction in blood pressure, initiate therapy 5.0 mg/hr. If desired blood pressure reduction is not achieved at this dose, the infusion rate may be increased by 2.5 mg/hr every 15 minutes up to a maximum of 15.0 mg/hr, until desired blood pressure reduction is achieved. For more rapid blood pressure reduction, initiate therapy at 5.0 mg/hr then the infusion rate may be increased by 2.5 mg/hr every 5 minutes up to a maximum of 15.0 mg/hr, until desired blood pressure reduction is achieved. Following achievement of the blood pressure goal, the infusion rate should be decreased to 3 mg/hr. For maintenance, the rate of infusion should be adjusted as needed to achieve the desired response.
Nicardipine is contraindicated in patients with advanced aortic stenosis because part of the therapeutic effect of nicardipine is secondary to reduced afterload. Reduction of diastolic pressure in these patients may worsen rather than improve myocardial oxygen balance.20
LabetalolLabetalol is an adrenergic receptor blocking agent that has both selective α1 - and nonselective β-adrenergic receptor blocking actions in a single drug. In humans, the ratios of α- to β-blockade have been estimated to be approximately 1:3 and 1:7 following oral and intravenous administration, respectively. Labetalol produces dose-related falls in blood pressure without reflex tachycardia and without significant reduction in heart rate, presumably through a mixture of its α-blocking and β-blocking effects.
For hypertensive emergencies labetalol is given as either repeated intravenous boluses or as a continuous
infusion. For repeat bolus dosing, labetalol injection should begin with a 10-20 mg dose (which corresponds to 0.125-0.25 mg/kg for an 80-kg patient) by IV injection over a 2-minute period. While much of the packaging of the agent lists 20 mg as the initial dose, many clinicians begin with a 10 mg dose to ensure safety of bolus therapy before proceeding to a 20 mg dose. Immediately before the injection and at 5 and 10 minutes after injection, supine blood pressure should be measured to evaluate response. Additional injections of 40 or 80 mg can be given at 10-minute intervals until a desired supine blood pressure is achieved or a total of 300 mg of labetalol has been injected. The maximum effect usually occurs within 5 minutes after each injection. A continuous infusion can also be given at 2 mg/min and titrated. The half-life of labetalol is 5 to 8 hours. In the ED, initial bolus therapy followed by infusion may be required.
Labetalol is contraindicated in bronchial asthma, overt cardiac failure, greater than first degree heart block, cardiogenic shock, severe bradycardia, and other conditions associated with severe and prolonged hypotension.21
EsmololEsmolol is a b1-selective (cardioselective) adrenergic receptor blocking agent with rapid onset, a very short duration of action, and no significant intrinsic sympathomimetic or membrane stabilizing activity at therapeutic dosages. Its elimination half-life after intravenous infusion is approximately 9 minutes. Esmolol inhibits the b1 receptors located chiefly in cardiac muscle, but this preferential effect is not absolute and at higher doses it begins to inhibit b2 receptors located chiefly in the bronchial and vascular musculature.
An initial loading dose of 0.5 milligrams/kg (500 micrograms/kg) infused over a minute duration followed by a maintenance infusion of 0.05 milligrams/kg/min (50 micrograms/kg/min) for the next 4 minutes is recommended. After the 4 minutes of initial maintenance infusion (total treatment

68w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
68
duration being 5 minutes), depending upon the desired response, the maintenance infusion may be continued at 0.05 mg/kg/min or increased step-wise to a maximum of 0.2 mg/kg/min with each step being maintained for 4 or more minutes.
Esmolol is contraindicated in patients with sinus bradycardia, heart block greater than first degree, cardiogenic shock or overt heart failure.22
EnalaprilatEnalaprilat, an angiotensin-converting enzyme (ACE) inhibitor when administered intravenously, is the active metabolite of the orally administered pro-drug, enalapril maleate. Enalaprilat intravenous results in the reduction of both supine and standing systolic and diastolic blood pressure. The onset of action usually occurs within fifteen minutes of administration with the maximum effect occurring within one to four hours. The duration of hemodynamic effects appears to be dose-related. Enalaprilat is indicated for the treatment of hypertension when oral therapy is not practical.
The dose in hypertension is 1.25 mg every six hours administered intravenously over a five minute period. A clinical response is usually seen within 15 minutes. Peak effects after the first dose may not occur for up to four hours after dosing. The peak effects of the second and subsequent doses may exceed those of the first.
Enalaprilat is contraindicated in patients with a history of angioedema related to previous treatment with an angiotensin converting enzyme inhibitor and in patients with hereditary or idiopathic angioedema. As with all vasodilators, enalapril should be given with caution to patients with obstruction in the outflow tract of the left ventricle.23
Why Not Sodium Nitroprusside?Sodium nitroprusside is used frequently in many EDs for rapid titratable blood pressure control in severely hypertensive patients. Sodium nitroprusside is a potent vascular smooth muscle relaxant, which
makes this drug very attractive in the facilitation of blood pressure reduction. It is exactly this property, however, which makes the drug potentially less attractive for cases of hypertensive neurological emergencies. Of great concern in this setting is the significant potential for this agent to not only reduce systemic blood pressure via relaxation of vascular smooth muscle, but also to cause significant increases in intracranial pressure due to dilatation of intracranial vasculature via the same mechanism. This increase is nicely illustrated in Figure 4 adapted from Anile
Figure 4. Changes in intracranial pressure with nitroprusside therapy. MICP = mean intracranial pressure. Adapted with permission from Anile et al. Acta Neurochir 1981;58:203-211.

6969w w w . e m c r e g . o r g
HYPERTENSION MANAGEMENT IN ACUTE NEUROVASCULAR EMERGENCIES
et al. in which preoperative neurosurgical patients with intraventricular catheters were treated with sodium nitroprusside for blood pressure reduction. The observed increase in intracranial pressure in 9 out of 10 patients was both rapid and concerning. Notably, after an initial period of steady incremental increase in intracranial pressure, there does appear to be a phenomenon of return toward pre-treatment intracranial blood pressures. In the majority of cases, however the ICP did not return to normal and, in fact, in some cases remained markedly elevated. Thus, with multiple other powerful, titratable agents available for blood pressure control in the setting of neurovascular emergencies, the use of sodium nitroprusside is generally not recommended. 24-27
SUMMARYBlood pressure management in acute neurovascular emergencies has potential for therapeutic benefit as well as the potential to cause harm if not performed with great care. The indications for management are as yet not clearly defined and the exact degree of management is highly dependent on the individual patient and their pathology. Fortunately, highly effective and easily titratable agents exist for use with these complicated patients.
REFERENCES1. Baron JC. Perfusion thresholds in human cerebral ischemia:
Historical perspective and therapeutic implications. Cerebrovasc Dis. 2001;11 Suppl 1:2-8
2. Powers WJ. Acute hypertension after stroke: The scientific basis for treatment decisions. Neurology. 1993;43:461-467
3. Paulson OB, Waldemar G, Schmidt JF, Strandgaard S. Cerebral circulation under normal and pathologic conditions. Am J Cardiol. 1989;63:2C-5C
4. Zivin JA. Factors determining the therapeutic window for stroke. Neurology. 1998;50:599-603
5. Adams HP, Jr., Adams RJ, Brott T, del Zoppo GJ, Furlan A, Goldstein LB, Grubb RL, Higashida R, Kidwell C, Kwiatkowski TG, Marler JR, Hademenos GJ. Guidelines for the early management of patients with ischemic stroke: A scientific statement from the stroke council of the American Stroke Association. Stroke. 2003;34:1056-1083
6. Grossman E, Messerli FH, Grodzicki T, Kowey P. Should a moratorium be placed on sublingual nifedipine capsules given for hypertensive emergencies and pseudoemergencies? JAMA. 1996;276:1328-1331
7. Brott T, Lu M, Kothari R, Fagan SC, Frankel M, Grotta JC, Broderick J, Kwiatkowski T, Lewandowski C, Haley EC, Marler JR, Tilley BC. Hypertension and its treatment in the NINDS rt-PA stroke trial. Stroke. 1998;29:1504-1509
8. Fogelholm R, Avikainen S, Murros K. Prognostic value and determinants of first-day mean arterial pressure in spontaneous supratentorial intracerebral hemorrhage. Stroke. 1997;28:1396-1400
9. Hemphill JC, 3rd, Bonovich DC, Besmertis L, Manley GT, Johnston SC. The ICH score: A simple, reliable grading scale for intracerebral hemorrhage. Stroke. 2001;32:891-897
10. Qureshi AI, Bliwise DL, Bliwise NG, Akbar MS, Uzen G, Frankel MR. Rate of 24-hour blood pressure decline and mortality after spontaneous intracerebral hemorrhage: A retrospective analysis with a random effects regression model. Crit Care Med. 1999;27:480-485
11. Broderick JP, Adams HP, Jr., Barsan W, Feinberg W, Feldmann E, Grotta J, Kase C, Krieger D, Mayberg M, Tilley B, Zabramski JM, Zuccarello M. Guidelines for the management of spontaneous intracerebral hemorrhage: A statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke. 1999;30:905-915
12. Jauch EC, Lindsell CJ, Adeoye O, Khoury J, Barsan W, Broderick J, Pancioli A, Brott T. Lack of evidence for an association between hemodynamic variables and hematoma growth in spontaneous intracerebral hemorrhage. Stroke. 2006;37:2061-2065
13. Becker KJ, Baxter AB, Bybee HM, Tirschwell DL, Abouelsaad T, Cohen WA. Extravasation of radiographic contrast is an independent predictor of death in primary intracerebral hemorrhage. Stroke. 1999;30:2025-2032
14. Powers WJ, Zazulia AR, Videen TO, Adams RE, Yundt KD, Aiyagari V, Grubb RL, Jr., Diringer MN. Autoregulation of cerebral blood flow surrounding acute (6 to 22 hours) intracerebral hemorrhage. Neurology. 2001;57:18-24
15. Bullock RM, Chesnut R, Clifton GL, al. e. Management and prognosis of severe traumatic brain injury, part 1. Guidelines for the management of severe traumatic brain injury. J Neurotrauma. 2000;17:451-553
16. Schellinger PD, Fiebach JB, Hoffmann K, Becker K, Orakcioglu B, Kollmar R, Juttler E, Schramm P, Schwab S, Sartor K, Hacke W. Stroke MRI in intracerebral hemorrhage: Is there a perihemorrhagic penumbra? Stroke. 2003;34:1674-1679
17. Ohkuma H, Tsurutani H, Suzuki S. Incidence and significance of early aneurysmal rebleeding before neurosurgical or neurological management. Stroke. 2001;32:1176-1180
18. Treggiari MM, Walder B, Suter PM, Romand JA. Systematic review of the prevention of delayed ischemic neurological deficits with hypertension, hypervolemia, and hemodilution therapy following subarachnoid hemorrhage. J Neurosurg. 2003;98:978-984

70w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
Copyright EMCREG-International, 2007
19. Wijdicks EFM. Aneurysmal subarachnoid hemorrhage. The clinical practice of critical care neurology. Oxford, UH: Oxford University Press; 2003.
20. PDL BioPharma, Inc. Nicardipine hydrochloride. 2006; http://www.cardeneiv.info/Cardene_Full_PI.pdf
21. Prometheus Laboratories. Labetalol HCl. 2003; http://www.prometheuslabs.com/pi/TrandateInj.pdf
22. Drugs.Com. Esmolol hydrochloride. 2006: MicromedexTM and MultumTM; http://www.drugs.com/pdr/ESMOLOL_HYDROCHLORIDE.html
23. Drugs.Com. Enalapril. 2006: MicromedexTM and MultumTM; http://www.drugs.com/cons/Enalapril_Systemic.html
24. Anile C, Zanghi F, Bracali A, Maira G, Rossi GF. Sodium nitroprusside and intracranial pressure. Acta Neurochir (Wien). 1981;58:203-211
25. Candia GJ, Heros RC, Lavyne MH, Zervas NT, Nelson CN. Effect of intravenous sodium nitroprusside on cerebral blood flow and intracranial pressure. Neurosurgery. 1978;3:50-53
26. Griswold WR, Reznik V, Mendoza SA. Nitroprusside-induced intracranial hypertension. JAMA. 1981;246:2679-2680
27. Turner JM, Powell D, Gibson RM, McDowall DG. Intracranial pressure changes in neurosurgical patients during hypotension induced with sodium nitroprusside or trimetaphan. Br J Anaesth. 1977;49:419-425

71w w w . e m c r e g . o r g
ADVANCES IN ACUTE STROKE CARE
The narrow time
windows from symptom
onset to treatment,
the relative lack of
knowledge about
stroke by the public,
and a lack of variety of
treatments for patients
not considered eligible
for rt-PA, reduces
the overall rate of
treatment for acute
stroke.
ADVANCES IN ACUTE STROKE CARE
OBJECTIVES:1. Discuss the use of advanced diagnostic imaging in stroke.2. Discuss the use of new therapies in ischemic stroke.3. Discuss a novel medical treatment for hemorrhagic stroke.
advanced in recent years to not only be able to assess the cerebral tissue damaged from a stroke, but also include the ability to assess for arterial occlusion as well as estimate the amount of brain tissue at risk during stroke in order to confirm a diagnosis and guide potential therapy.
One method of confirming the diagnosis of ischemic stroke and assessing the extent of the arterial blockage is through computed tomography angiography (CTA). For patients with ischemic stroke, CTA takes advantage of the widespread availability of CT scanners in EDs to allow a non-invasive look at the cerebral vasculature to assess for stenosis or occlusion. The technique uses standard spiral CT scanners with a 50 CC contrast bolus. The axial cuts, or source images, are then reformatted into a three-dimensional projection that allows visualization of the circle of Willis as well as proximal portions of the middle cerebral artery (MCA), anterior cerebral artery (ACA) and vertebrobasilar system. The entire process typically adds 10-15 minutes to the standard non-contrasted CT imaging.
INTRODUCTIONRecent years have brought many advances in both the diagnosis and treatment of acute stroke, with many technologies still undergoing testing in clinical trials. Unfortunately, despite this progress, stroke remains the third leading cause of death in the United States and the leading cause of disability. The narrow time windows from symptom onset to treatment, the relative lack of knowledge about stroke by the public, and a lack of variety of treatments for patients not considered eligible for recombinant tissue plasminogen activator (rt-PA) reduces the overall rate of treatment for acute stroke. This review will address some recent and emerging technologies for the diagnosis and treatment of acute stroke that may change the way this devastating disease is approached in the emergency department (ED).
Stroke DiagnosticsFor the past twenty years, diagnostics in the setting of acute stroke have classically consisted of a fingerstick blood sugar and non-contrast computed tomography (CT) of the head. Both CT and magnetic resonance imaging (MRI) technology have
Brian A. Stettler, MDAssistant Professor, Department of Emergency Medicine, University of Cincinnati College of Medicine
Member, Greater Cincinnati/Northern Kentucky Stroke TeamCincinnati, Ohio

72w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
72w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
The advantages of CTA include its speed and availability as well as its ability to assess for occlusion of the cerebral vessels that could affect treatment algorithms. Lev et al1 used CTA in 44 consecutive patients who presented within six hours of onset of symptoms to assess for occlusion of a cerebral vessel prior to angiographic correlation with diagnostic angiography. The study was designed to assess the feasibility that CTA could be used as a screening tool to decide when to proceed on to intra-arterial (IA) fibrinolysis. Of 224 vessels studied with diagnostic angiography after CTA, the sensitivity of CTA for large-vessel occlusion was 98.4% with a specificity of 98.1% and overall accuracy of 98.2%. They concluded that CTA is highly accurate in the detection of large vessel occlusion and may be valuable for the triage of patients to intra-arterial thrombolysis.
Another study performed by Verro et al2 evaluated 54 consecutive patients presenting with symptoms of ischemia with non-contrasted CT followed by CTA of the circle of Willis. The study was used to select patients who did not meet standard National Institute of Neurological Disorders and Stroke (NINDS) IV fibrinolysis criteria for digital subtraction angiography (DSA) and potential IA fibrinolysis. The authors concluded that CTA provides an accurate assessment of occlusion in the acute setting and may be used to screen candidates for aggressive treatment who might otherwise not receive standard IV therapy due to exclusion. It is important to remember, however, that even in the absence of documented occlusion on
CTA, a candidate for IV fibrinolysis should still be treated, as reversal of the neurologic deficit can still be achieved by opening a small-vessel occlusion not visualized on CTA. In fact, Verro et al suggested in a separate study that CTA did lead to more conservative management and lower rates of treatment compared to decisions made blinded to CTA results.3
The goal in the use of rt-PA for fibrinolysis of an acute ischemic stroke is to salvage the maximum amount of neuronal tissue that has not yet infarcted. It has been shown that in acute arterial occlusion there is a central core of brain that infarcts within minutes due to complete loss of blood flow and a larger area of ischemic brain which remains alive but functions abnormally due to loss of normal oxygen supply, termed the ischemic penumbra. The presence or absence of an ischemic penumbra seems to correlate with the prognosis for recovery after fibrinolysis.4,5 A lack of ischemic, but not yet infracted tissue reflects poorly on the chance of recovery after treatment. The gold standard for evaluation of the ischemic penumbra is investigation by MRI. Magnetic resonance imaging allows generation of images that show the area of decreased blood flow in the brain as well as the area of infarcted tissue, allowing a simple assessment of whether there still exists living tissue receiving inadequate blood flow that may benefit from fibrinolysis, also known as a diffusion-perfusion mismatch. Magnetic resonance angiography (MRA) functions in a fashion very similar to CTA, showing vessel anatomy, including cervical vessels and the circle of Willis.
It is important to
remember, however,
that even in the
absence of documented
occlusion on CTA,
a candidate for IV
fibrinolysis should still
be treated, as reversal
of the neurologic deficit
can still be achieved by
opening a small-vessel
occlusion not visualized
on CTA.

73w w w . e m c r e g . o r g
ADVANCES IN ACUTE STROKE CARE
73w w w . e m c r e g . o r g
ADVANCES IN ACUTE STROKE CARE
Diffusion-weighted MRI involves a technique that displays a hyperintense, or white, signal which represents tissue which is largely unsalvageable and irreversibly damaged. While conventional MRI or non-contrasted CT takes up to six hours to demonstrate changes of ischemia, diffusion-weighted imaging (DWI) will document these changes within minutes from onset of ischemia. Perfusion-weighted MRI uses MRI to track a bolus of gadolinium through the brain. Both cerebral blood volume (CBV) and the time it takes for the gadolinium to pass through the brain can be assessed, allowing cerebral blood flow (CBF) to be indirectly imaged. A decrease in CBF reflects the area of tissue which is underperfused, encompassing both the infarct core and the penumbra. Comparison of the DWI to the PWI allows the clinician to subtract the DWI hyperintense signal from the abnormal signal on PWI to ascertain whether there is still tissue which is alive but underperfused. This is the target area of tissue for reperfusion. A matched area of DWI and PWI signal abnormality suggests little benefit to fibrinolysis, as the infarct is completed.
Studies involving MRI in the hyperacute time period are small but encouraging. Parsons et al4 performed a study utilizing DWI/PWI in acute stroke of less than 6 hours duration. The study involved 19 patients treated within 6 hours with IV rt-PA matched with 21 historical controls. All patients underwent DWI/PWI, but they were given fibrinolysis based on standardized protocols and not by selection with MRI. The study showed that when patients were
analyzed by group as either treated or not treated, there was a trend towards benefit with treatment, but no significant difference between the groups. However, when only patients with a DWI/PWI mismatch were analyzed, there was a significant improvement in both outcome National Institute of Health Stroke Scale (NIHSS ) (Mean 5.3 points, 95% CI 1.0 – 11.7 points, p < 0.01) and functional independence by modified Rankin scale (mRS) (χ2 =4.6, p = 0.03) in the treated patients. Despite the small numbers in this study, it suggests that more benefit may be gained by treating patients with a DWI/PWI mismatch on MRI. When assessing an acute stroke, typical MRI protocols in the hyperacute time period add only 20 minutes to overall treatment time.
Cerebral perfusion CT also allows the differentiation of ischemic from infarcted tissue. In perfusion CT (PCT), a bolus of contrast is given IV and the attenuation of the brain parenchyma is then measured, with the thought that as the contrast passes through the parenchyma, the attenuation of the brain tissue will increase. Further, in the case of arterial occlusion, the increase in attenuation will be delayed or lost altogether in tissue that has decreased blood supply, allowing CT to identify tissue at risk of infarct or already infarcted. Tracking the contrast bolus in the parenchyma gives measures of CBF and CBV. Reduced perfusion with preserved or increased CBV is thought to represent areas of ischemia, while reduced perfusion coupled with reduced CBV is thought to represent already infarcted tissue. This allows the ultimate goal of determination of the ischemic penumbra by CT.
The presence or
absence of an ischemic
penumbra seems to
correlate with the
prognosis for recovery
after fibrinolysis.

74w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
74w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
Studies of the diagnostic capability of CT perfusion have generally included small numbers of patients, but appear promising in comparison with MRI. Wintermark et al6 evaluated 22 patients upon presentation to the ED with perfusion CT and then compared these images to delayed DWI MRI and found that the area of perfusion deficit on initial CT strongly correlated with the final DWI abnormality in patients without vessel recanalization (n= 8, correlation coefficient 0.958). The study further found that in those with arterial recanalization, the final infarct on the DWI was smaller than the area of total ischemia on initial CT, but larger than the area of initial infarct on CT, which they interpreted to show accurate CT depiction of the penumbra with some recovery after clot lysis (n=13). Ultimately, the authors concluded that PCT gives an accurate estimate of the area of ischemia and infarct, in comparison with MRI.
Another study by Schramm et al7 compared perfusion CT with perfusion-weighted MRI (PWI) and DWI to determine correlation between the two studies for area of perfusion and diffusion defects. In this study, 22 patients underwent both CT and MRI within six hours of onset of acute neurologic deficit. This study found no significant difference between perfusion CT lesion volume and PWI or CT perfusion evidence of infarction and DWI. This suggests good reproducibility between PCT and MRI for evaluation of the ischemic penumbra, although this will need to be confirmed with larger studies. The perfusion CT averaged approximately 10 minutes to complete and can be performed on most spiral CT scanners with the addition of imaging
software, making it more accessible to most EDs in real-time. At this point, most centers still require a non-contrast CT as the gold standard to rule out hemorrhage prior to treatment with rt-PA, therefore the coupling of standard non-contrast CT imaging with advanced CT diagnostics makes practical sense.
The ideal patient for acute multimodal imaging is the patient who arrives with prolonged duration of symptoms in which advanced imaging may document salvageable brain or in the patient with an atypical presentation in which the diagnosis of stroke is in question. In both of these instances, the advanced diagnostic imaging may help to guide therapy. Ongoing studies to evaluate the utility of DWI/PWI mismatch in patients with a prolonged time from symptom onset include DIAS II (Desmoteplase in Acute Ischemic Stroke II) which utilizes MRI to randomize patients to treatment with desmoteplase, a novel fibrinolytic, in the time frame from 3-9 hours from symptom onset. Only patients with a significant mismatch on imaging are entered, as they are thought to have salvageable brain. A preceding trial, DEDAS (Dose Escalation of Desmoteplase for Acute Ischemic Stroke) did show clinical benefit in the target population when treated with fibrinolytic at the prolonged time period.8 A second study, EPITHET (Echoplanar Imaging Thrombolysis Evaluation Trial) also evaluates the use of MRI in the setting of prolonged time from symptom onset and is currently ongoing. This trial uses standard-dose rt-PA 3-6 hours from symptom onset in patients with significant DWI/PWI mismatch. Further studies are still needed, but in a patient with an
The ideal patient for
acute multimodal
imaging is the patient
who arrives with
prolonged duration of
symptoms in which
advanced imaging may
document salvageable
brain or in the patient
with an atypical
presentation in which
the diagnosis of stroke
is in question.

75w w w . e m c r e g . o r g
ADVANCES IN ACUTE STROKE CARE
75w w w . e m c r e g . o r g
ADVANCES IN ACUTE STROKE CARE
obvious proximal vessel occlusion and significant mismatch, a discussion of risks and benefits with the patient and family may favor treatment despite increased risk of hemorrhage beyond three hours. This patient may also be guided towards IA therapy if this is available at the treating institution or referral center.
A final diagnostic tool that is still in the research stage is that of serum biomarkers. While a unique marker of cell death, such as troponin for the myocardium, has not yet been identified, there is ongoing work that suggests that a combination of serum markers may have sufficient sensitivity and specificity to be useful in the clinical arena. This biomarker panel would be ideal if it demonstrates a quick and accurate confirmatory test for cerebral ischemia while ruling out other causes of weakness.
Acute Therapies in Ischemic StrokeThere are many novel therapies for the treatment of ischemic stroke developed or advanced within the past few years, some of which are still undergoing evaluation in clinical research trials and some of which have entered clinical practice. These therapies include IA therapy with medications or mechanical devices for clot dissolution and removal, combined drug therapy, transcranial Doppler, novel fibrinolytic agents, and drugs designed to protect ischemic tissue from oxidative damage. A novel drug therapy for hemorrhagic stroke that may help decrease the size and resultant damage of intracerebral hemorrhage is also currently undergoing clinical testing.
One of the therapies with the longest clinical track record that is still undergoing evaluation is IA therapy for acute ischemic stroke. The theoretical basis for this therapy is that a drug or a mechanical device delivered directly to the sight of an arterial occlusion may be better at achieving recanalization of the vessel and recovery of ischemic brain tissue. Therapy delivered IA has been around for more than a decade and has previously included pro-urokinase
or rt-PA delivered directly or in close proximity to the thrombus by microcatheter. The treatment window for drug delivery typically extends out to six hours in this setting and sometimes beyond that time depending on the clinical picture and presence or absence of an ischemic penumbra.
Two clinical trials already completed using drug delivery via the IA route of administration include the IMS (Interventional Management of Stroke) trial9 using t-PA, and the PROACT II (Prolyse in Acute Cerebral Thromboembolism II) trial, which utilized pro-urokinase as a thrombolytic.10 Both of these trials used extended time windows of seven and eight hours from symptom onset, respectively, for the completion of the IA procedure. The IMS protocol called for a novel approach, instituting a reduced dose of IV rt-PA in patients with an NIHSS >10 presenting within three hours of symptom onset. All patients in IMS then went to angiography and also received IA rt-PA if they were found to have a large-vessel occlusion. This protocol allowed early initiation of therapy in the ED, but still takes advantage of directed fibrinolytic via the IA route. There was no randomization and all patients were treated, with the NINDS trial used as historical controls for comparison. The 80 subjects treated in IMS had a better clinical outcome by all endpoints than the placebo-treated patients in the NINDS trial11 and a similar outcome to the IV rt-PA treated historical controls from NINDS. Symptomatic hemorrhage rates were also similar to IV rt-PA at 6.3%.
The subjects in PROACT II were randomized to IA pro-urokinase plus heparin during angiography or a 4-hour infusion of heparin alone. The 121 subjects treated with IA pro-urokinase were more likely to have a mRS of 2 or less at 90 days than the 59 controls (p= 0.04) despite an increased risk of symptomatic intracerebral hemorrhage (10% vs 2% for controls, p=0.06). There was no difference in overall mortality in PROACT II between treated patients (25%) and controls (27%) despite the increased incidence of hemorrhage.

76w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
76w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
From these data, many questions remain unanswered. As IMS used combined intravenous rt-PA initiated within three hours and IA rt-PA, but had similar outcomes to the treated patients in the NINDS trial, it remains to be proven whether IV/IA or IV therapy alone is superior within three hours of symptom onset. This question is currently being studied in the ongoing IMS III trial, which randomizes patients to either IV rt-PA therapy or combined IV/IA within three hours of symptom onset.
Another IA therapy currently under study is the use of mechanical devices. The MR RESCUE (MR and Recanalization of Stroke Clots Using Embolectomy) trial randomizes patients based on the presence of a DWI/PWI difference to either best medical treatment or IA therapy with the MERCI retriever, a mechanical device designed to remove thrombus from proximal cerebral vessels without chemical agents. Study patients can be treated out to eight hours from symptom onset and are still eligible for treatment even if systemically anticoagulated with heparin or coumadin, as opposed to traditional treatment with IV rt-PA. Initial experience with this device has been fairly positive, as reported in the MERCI trial.12 The device did show a statistically significant ability to achieve recanalization at 46 % vs 18% of historical controls (p < 0.0001), although the long-term clinical benefit is more debatable. Only 28% of patients treated with the device achieved a mRS of 2 or less and the mortality was 44% at 90 days in treated patients. While both of these outcomes are substantially worse than previous benchmarks, the strokes
treated in MERCI were more severe, as measured by the NIHSS, than previous trials. Further, many of the treated patients were ineligible for other therapies, such as fibrinolytic, and the mechanical device offered the only possibility of therapy for their severe deficit. The addition of advanced diagnostic imaging in MR RESCUE may help define which group of patients will benefit from this novel therapy.
Another recent advance in acute stroke care comes with the testing of combined therapy in the early stages of acute ischemic stroke. There are several ongoing clinical trials that are testing the combination of a fibrinolytic agent with the addition of a glycoprotein IIb/IIIa inhibitor. The combination of these agents in previous cardiac trials has shown decreased rates of post-infarction complications, such as reinfarction and death.13,14
This is most likely due to increased recanalization and maintenance of vessel patency by attacking both the fibrin meshwork of the clot and disassociating the platelets from the thrombus as well. One trial that is currently ongoing, the CLEAR trial (Combined Approach to Lysis Utilizing Eptifibatide and rt-PA in Acute Ischemic Stroke) randomizes patients to treatment with standard rt-PA or low-dose rt-PA and eptifibatide within three hours of symptom onset. Goals of this trial are to assess both the efficacy of the combined approach to see if there is increased rate of recovery from stroke, but also to see if combined therapy at lower doses is safer than standard rt-PA, with lower rates of symptomatic intracranial hemorrhage (sICH).
… it remains to be
proven whether
IV/IA or IV therapy
alone is superior
within three hours of
symptom onset.

77w w w . e m c r e g . o r g
ADVANCES IN ACUTE STROKE CARE
77w w w . e m c r e g . o r g
ADVANCES IN ACUTE STROKE CARE
A second ongoing clinical trial using combined therapy incorporates many of the aspects already discussed. ROSIE (Reperfusion of stroke Safety study Imaging Evaluation) uses MRI to document a DWI/PWI mismatch and then randomizes those patients with a mismatch who present within 24 hours of stroke symptom onset to a combination of reteplase (rt-PA) plus abciximab or abciximab alone. Both of these trials are using lower doses of the fibrinolytic agent than the typical cardiac dose and are following patients for evidence of hemorrhage and clinical outcome. While the tissue of the heart and the brain are not similar, it is hoped that the combined therapies will show better, safer recanalization of cerebral vessels compared to the standard therapy of rt-PA.
A final therapy to be discussed for acute ischemic stroke treatment is that of transcranial Doppler ultrasound (TCD). Transcranial Doppler ultrasound uses high energy ultrasound to penetrate the skull for monitoring of vasospasm or occlusion of the large cerebral vessels such as the MCA or basilar artery. It was postulated that the energy of TCD, in the presence of a thrombus treated with rt-PA, may also speed recanalization of the target vessel. Alexandrov et al reported on TCD therapy in combination with rt-PA in 126 patients, 63 randomized to TCD therapy plus rt-PA and 63 treated with IV rt-PA only. TCD did show effectiveness in arterial recanalization of the MCA, although the effects on clinical outcome were minimal.15 All patients presented within three hours of symptom onset, received rt-PA at standard dosing, and
had a middle cerebral artery occlusion as documented by TCD and clinical symptoms. Complete recanalization of the target vessel that was sustained at two hours occurred in the TCD-treated group in 24 of 63 patients and in 8 of 63 controls (p = 0.002) There was no difference in sICH or death in the groups, but the clinical improvement in the TCD-treated group was not significantly better than the control group. While these data are encouraging, more work is required to determine if there is a select group of patients upon which this therapy should be instituted. Further, the therapy is technically difficult to achieve in the ED, as most hospitals do not have anyone trained in the use of TCD available on call and there is no standardized device for delivering this therapy which is very operator-dependent.
One of the therapies long sought in the realm of acute stroke care is that of a neuroprotectant. It is thought that part of the damage to the brain in the setting of ischemic stroke occurs due to the formation of free radicals within the brain tissue after arterial occlusion and subsequent reperfusion. The hope for this elusive neuroprotectant drug is that it would have few side effects and be easily administered to salvage ischemic brain from damage by these free radicals, both before and after fibrinolytic therapy, as well as in patients otherwise ineligible for treatment. There have been many examples of successful agents in laboratory animals and bench research, but until recently there have been no reported successes in human clinical trials. The SAINT trial (Stroke-Acute Ischemic NXY Treatment Trial) reported
While the tissue of
the heart and the
brain are not similar,
it is hoped that the
combined therapies
will show better,
safer recanalization
of cerebral vessels
compared to the
standard therapy
of rt-PA.

78w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
78w w w . e m c r e g . o r g
ADVANCING THE STANDARD OF CARE:Cardiovascular and Neurovascular Emergencies
on the use of an agent labeled NXY-059 in 1722 patients with acute ischemic stroke that presented within six hours of symptom onset.16 Patients were randomized to an infusion of NXY-059 over a 72 hour period versus placebo. NXY-059 did show a very modest clinical benefit in the modified Rankin scale at 90 days as compared to placebo. This effect was lost, however, in looking at NIHSS and Barthel index, as there was no difference at 90 days in these outcome scales between study patients and controls. Interestingly, in a post-hoc analysis, it was found that in patients treated with rt-PA in the trial, there was a significantly lower rate of sICH in patients treated with NXY-059 versus placebo (2.5% vs 6.4% respectively, p = 0.036). While this is yet unconfirmed, this suggests that there may be some protective effect against hemorrhagic transformation in patients treated with fibrinolytic agents, raising the possibility of using these agents in combination with NXY-059 in the future. The SAINT II trial is currently ongoing to further investigate the clinical efficacy of NXY-059 as a neuroprotectant and confirm or dispute previous results. Given the cost associated with the agent, it would be difficult for the health care system to support the drug in all ischemic strokes unless a more brisk clinical effect is seen in follow-up trials. Regardless, the search for an effective and well-tolerated neuroprotectant agent continues.
Acute Therapies in Hemorrhagic StrokeThere have been few effective therapies in the setting of hemorrhagic stroke, and
particularly intra-cerebral hemorrhage (ICH), and this disease process is associated with a very high morbidity and mortality. While work continues on the issues surrounding optimal blood pressure and glucose management after ICH, one therapy for ICH has shown some promise in a recent trial.
Previous work has shown that 26% of patients with ICH will have growth of the size of the hemorrhage within the first few hours and that this is significantly associated with clinical worsening.17 A recent trial by Mayer et al reported on the use of recombinant Factor VIIa (rFVIIa) in the setting of ICH.18 In this trial, 399 patients were randomized to placebo or escalating doses of rFVIIa given by IV bolus. Subjects presented to the ED within 3 hours of symptom onset and IV treatment had to be complete by four hours. Clinical outcomes were assessed at 90 days. There was a significant improvement in all clinical outcomes, including mRS, Barthel index, and Glascow outcome scale in patients treated with rFVIIa as opposed to placebo. There was a small increase in non-fatal thromboembolic events in the treated patients, but overall mortality was significantly reduced by the study drug (29% vs 18% placebo, p = 0.02). The FAST (Recombinant Factor VIIa in Acute Intracerebral Haemorrhage) trial is currently ongoing to confirm the results of this dose-finding trial. If the results are confirmed, this will represent the first proven drug therapy for ICH in the hyperacute time period.
There was a significant
improvement in all
clinical outcomes,
including mRS, Barthel
index, and Glascow
outcome scale in
patients treated with
rFVIIa as opposed to
placebo.

79w w w . e m c r e g . o r g
ADVANCES IN ACUTE STROKE CARE
79w w w . e m c r e g . o r g
ADVANCES IN ACUTE STROKE CARE
SUMMARYIn conclusion, a great many advances have occurred in the treatment of acute stroke in recent years. Both diagnostics and therapeutics have improved, with many encouraging trials ongoing to answer questions that remain about combined therapies, as well as extending the time window to treatment. The future will see the evolution of many of these therapies into clinical practice to advance the options available for care of the patient who presents to the ED with acute stroke.
REFERENCES1. Lev MH, Farkas J, Rodriguez VR, et al. CT
Angiography in the rapid triage of patients with hyperacute stroke to intraarterial thrombolysis: Accuracy in the detection of large vessel thrombus. J Comput Assist Tomogr 2001;25(4):520-8.
2. Verro P, Tanenbaum LN, Borden NM, Sen S, Eshkar N. CT Angiography in acute ischemic stroke: Preliminary results. Stroke 2002;33(1):276-8.
3. Verro P, Tanenbaum LN, Borden N, Eshkar N, Sen S. Clinical application of CT angiography in acute ischemic stroke. Clinical Neurology and Neurosurgery; In Press.
4. Parsons MW, Barber PA, Chalk J, et al. Diffusion- and perfusion-weighted MRI response to thrombolysis in stroke. Ann Neurol 2002;51(1):28-37.
5. Singer OC, du Mesnil de Rochemont R, Foerch C, et al. Early functional recovery and the fate of the diffusion/perfusion mismatch in patients with proximal middle cerebral artery occlusion. Cerebrovasc Dis 2004;17(1):13-20.
6. Wintermark M RM, Thiran JP, Maeder P, Chalaron M, Schnyder P, Bogousslavsky J, Meuli R. Prognostic accuracy of cerebral blood flow measurement by perfusion computed tomography, at the time of emergency room admission, in acute stroke patients. Ann Neurol 2002;51(4):417-32.
Both diagnostics and
therapeutics have
improved, with many
encouraging trials
ongoing to answer
questions that remain
about combined
therapies, as well as
extending the time
window to treatment.
7. Schramm P, Schellinger PD, Klotz E, et al. Comparison of perfusion computed tomography and computed tomography angiography source images with perfusion-weighted imaging and diffusion-weighted imaging in patients with acute stroke of less than 6 hours‘ duration. Stroke 2004;35(7):1652-8.
8. Furlan AJ, Eyding D, Albers GW, et al. Dose escalation of desmoteplase for acute ischemic stroke (dedas): evidence of safety and efficacy 3 to 9 hours after stroke onset. Stroke 2006;37(5):1227-31.
9. The IMS Study Investigators. Combined intravenous and intra-arterial recanalization for acute ischemic stroke: the interventional management of stroke study. Stroke 2004;35(4):904-11.
10. Furlan A, Higashida R, Wechsler L, et al. Intra-arterial pro-urokinase for acute ischemic stroke: the PROACT II study: a randomized controlled trial. JAMA 1999;282(21):2003-11.
11. The National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 1995;333(24):1581-8.
12. Smith WS, Sung G, Starkman S, et al. Safety and efficacy of mechanical embolectomy in acute ischemic stroke: results of the MERCI trial. Stroke 2005;36(7):1432-8.
13. Antman EM, Giugliano RP, Gibson CM, et al. Abciximab facilitates the rate and extent of thrombolysis : results of the thrombolysis in myocardial infarction (TIMI) 14 trial. Circulation 1999;99(21):2720-32.
14. The PURSUIT Trial Investigators. Inhibition of platelet glycoprotein IIb/IIIa with eptifibatide in patients with acute coronary syndromes. N Engl J Med 1998;339(7):436-43.
15. Alexandrov AV, Molina CA, Grotta JC, et al. Ultrasound-enhanced systemic thrombolysis for acute ischemic stroke. N Engl J Med 2004;351(21):2170-8.
16. Lees KR, Zivin JA, Ashwood T, et al. NXY-059 for acute ischemic stroke. N Engl J Med 2006;354(6):588-600.
17. Brott T, Broderick J, Kothari R, et al. Early hemorrhage growth in patients with intracerebral hemorrhage. Stroke 1997;28(1):1-5.
18. Mayer SA, Brun NC, Begtrup K, et al. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med 2005;352(8):777-85.
Copyright EMCREG-International, 2007

81w w w . e m c r e g . o r g
Continuing Medical Education Post-TestBased on the information presented in this monograph, please choose one correct response for each of the following questions or statements. Record your answers on the answer sheet on page 89. To receive Category I credit, complete the post-test and record your responses on the answer sheet. Mail in the return envelope no later than February 1, 2008. A passing grade of 80% is needed to receive credit. A certificate will be sent to you upon your successful completion of this post-test.
Management of non-ST-segment Elevation Acute Coronary Syndrome (NSTE-ACS) in the ED: State-of-the-Art Anti-platelet Management
1. Which of the following anti-platelet drugs is indicated in the emergency department management of high risk NSTE-ACS?
a) Clopidogrel b) Glycoprotein IIb/IIIa inhibitors c) Aspirin d) All of the above
2. Based on the ARMYDA-2 trial, what are the effects of increasing the loading dose of clopidogrel to 600 mg prior to PCI?
a) Increase in bleeding complications b) Reduction in death, MI, and target vessel
revascularization c) Increase in CABG related bleeding d) Reduction in bleeding complications.
3. According to the ISAR REACT-2 trial, which group of high risk NSTE-ACS patients received the most benefit from the addition of a GP IIb/IIIa inhibitor during PCI?
a) Troponin negative patients b) Troponin positive patients c) ECG ST segment depression patients d) All of the above
4. According to the ACUITY Timing trial results, which of the following patients received the most benefit in ischemic endpoint reduction with upstream GP IIb/IIIa inhibition?
a) CABG patients b) Medical management patients c) PCI patients d) All of the above
Non-ST-segment Elevation Acute Coronary Syndrome: Optimal Anti-Coagulant Therapy for the Emergency Department
5) For patients with NSTE ACS presenting to the ED, which of the following represent guideline-indicated therapy?
a) Heparin b) Low molecular weight heparin c) Both A and B d) Neither A and B 6) Low molecular weight heparin is prepared through
fractionation of the parent compound, heparin. a) True b) False 7) In the ESSENCE and TIMI IIB trials, enoxaparin
reduced the composite end points of death, MI, or recurrent angina/need for urgent revascularization compare to heparin. a) True b) False
8) In the SYNERGY trial, which of the following patients experienced increased risk of bleeding?
a) Elderly patients b) Patients with renal insufficency c) Patients experiencing “switching” between
unfractionated heparin and enoxaparin d) All of the above

82w w w . e m c r e g . o r g
82
Continuing Medical Education Post-Test (cont.)
CRUSADE Quality Improvement Initiative: Better Care for Patients with Unstable Angina and non-ST-segment Elevation Myocardial Infarction
9) The CRUSADE initiative includes the following types of patients:a) Only those with ST-segment elevation
myocardial infarction.b) All chest pain patients admitted to the hospitalc) Only chest pain patients admitted when a
myocardial infarctiond) Patients with a Non-ST-segment elevation
myocardial infarction and ST-segment depression, as well as cardiac biomarker positivity.
10) The CRUSADE initiative has the following
objectives:a) To determine compliance with AHA/ACC
guidelines for the management of these patients in the acute setting and time of discharge
b) To educate physicians about the AHA/ACC guidelines for NSTEMI ACS
c) To provide quality improvement toolsd) All of the above
11) The CRUSADE initiative has been used to evaluate
the following subjects except:a) Disparities in care based on genderb) Direct comparison of pharmacologic agents in a
prospective, randomized fashionc) Cardiac biomarker discrepancies
d) Disparities in care based on race
ST-segment Elevation Myocardial Infarction (STEMI): Decreasing the Time to Treatment in the ED
12) For patients presenting to the emergency department with STEMI, the ideal maximum door-to-needle time for infusion of fibrinolytic therapy is 30 minutes while the maximum door-to-balloon inflation time for percutaneous coronary intervention (PCI) is 90 minutes.
a) True b) False
13) Myocardial muscle salvage for patients with STEMI, based on trials of fibrinolytic therapy, occurs up to the following time after symptom onset:
a) 4 hours d) 16 hours b) 8 hours e) 20 hours c) 12 hours
14) Based on National Registry of Myocardial Infarction data for patients undergoing PCI for STEMI from 1994 through 1998, the advantage for mechanical intervention decreases substantially how many minutes after presentation to the ED:
a) 30 minutes c) 90 minutes b) 60 minutes d) 120 minutes
15) For patients being transferred from one hospital to another hospital for PCI, what percentage of patients typically receive a door-to-balloon time of 90 minutes or less at the receiving hospital?
a) 5% d) 20% b) 10% e) 30% c) 15%
16) In the D2B program instituted by the American College of Cardiology in November 2006, emergency physicians are responsible for activating the cardiac catheterization team to decrease the door-to-balloon time for patients presenting with STEMI.
a) True b) False
Novel Anti-thrombotic Therapies for Acute Coronary Syndrome: Direct Thrombin Inhibitors
17) New landmark studies in patients with acute coronary syndromes have focused on which of the following in the primary outcome:
a) Death b) Acute myocardial infarction c) Urgent revascularization d) Bleeding complications e) All of the above including both efficacy and
safety parameters f) 1, 2, 3 as the efficacy parameters

8383w w w . e m c r e g . o r g
18) Bivalirudin monotherapy was associated with reduction in ischemic endpoints
a) True b) False
19) Use of glycoprotein IIb/IIIa receptor antagonists was associated with an increase in bleeding endpoints, whether it was used with heparin or bivalirudin
a) True b) False 20) Bivalirudin monotherapy (without concurrent
glycoprotein 2b/3a receptor antagonists) was associated with reduction in bleeding endpoints, as well as an improvement in net clinical benefit.
a) True b) False
Management of ST-segment Elevation Myocardial Infarction in the ED: State-of-the-Art Anti-platelet and Anti-thrombotic Therapy
21) Which of the following anti-platelet drugs is NOT presently recommended by the ACC/AHA Guidelines for the emergency department management of STEMI?
a) Clopidogrel b) Glycoprotein IIb/IIIa inhibitors c) Aspirin d) None of the above
22) Based on the CLARITY trial, what are the effects of adding clopidogrel 300 mg to aspirin and fibrinolytic therapy in the ED treatment of STEMI?
a) Increase in intracranial hemorrhage b) Reduction in death, MI, and occluded artery
at angiogram c) Increase in PCI-related mortality d) Reduction in bleeding complications.
23) According to the ASSENT-4 Trial, the routine utilization of fibrinolytic therapy prior to immediate primary PCI results in:
a) Increased intracerebral complications b) Increased mortality c) Worse ischemic outcomes d) All of the above
Continuing Medical Education Post-Test (cont.)
24) According to the TITAN TIMI-34 trial, utilization of GPI’s for facilitated primary PCI results in:
a) Increase angiographic reperfusion at angiogram b) Increased tissue perfusion at angiogram c) No significant increase in bleeding d) All of the above
Acute Decompensated Heart Failure: Novel Approaches to Classification and treatment
25) When used for ADHF, IV nitroglycerin provides the following:
a) Reduces mortality b) Improves symptoms of congestion c) Neither d) Both 26) All patients with ADHF should receive IV
vasoldilators and IV diuretics: a) True b) False
27) Most patients with acute “flash” pulmonary edema have: a) Diastolic dysfuctionb) Systolic dysfuctionc) Severe hypertensiond) Hypotensione) a and cf) b and d
28) The majority of ADHF patients require admission to the ICU:
a) True b) False
Lactate - A Marker for Sepsis and Trauma
29) Lactate is a product of anaerobic metabolism. a) True b) False
30) Seizures can cause a transient elevation in serum lactate.
a) True b) False

84w w w . e m c r e g . o r g
84
31) Stable or increasing serum lactate levels are associated with improved mortality in septic patients.
a) True b) False
32) Lactate is cleared by the liver, kidney, brain, and red blood cells.
a) True b) False
Point-of-Care Testing for Cardiac Biomarkers in the ED: Blueprint for Implementation
33) Factors which have increased the growth of point-of-care (POC) testing for cardiac biomarkers in the United States include all of the following except:a) Large volume of patients presenting to
emergency departments each year causing “overcrowding”.
b) Guidelines for non-ST-segment elevation acute coronary syndrome published in 2002.
c) The low cost of the POC test compared to the central laboratory assay.
d) Decreased complexity of performing the POC test compared to using an assay performed on a central laboratory analyzer.
34) Cardiac biomarkers which are commonly used for POC testing in the emergency department include all of the following except:a) Myosin heavy chainb) Myoglobinc) CK-MBd) Troponine) BNP (brain natriuretic peptide)
35) POC testing for cardiac biomarkers in the emergency department can be used for risk stratification and to identify patients with ACS for treatment with anti-thrombotic and anti-platelet agents
a) True b) False
Continuing Medical Education Post-Test (cont.)
36) From the laboratory perspective, usual turn-around time (TAT) for cardiac biomarker testing includes pre-analytical time which occurs in the emergency department and the actual analysis of the specimen and reporting of the results back to the emergency physician.
a) True b) False
37) Stakeholders for the implementation of a POC testing program in an emergency department should include:a) Laboratoriansb) Cliniciansc) Hospital administratorsd) All of the above
Advances in Acute Stroke Care
38) CT perfusion is designed to show areas of: a) ischemia b) infarction c) both d) neither
39) MRA and CTA are both capable of documenting proximal cerebral vessel occlusion.
a) True b) False
40) Intra-arterial mechanical embolectomy devices have been shown to:
a) Improve rate of recanalization b) Improve mortality c) Improve long-term outcomes
41) Recombinant Factor VIIa has been shown to: a) Decrease hemorrhage volume b) Improve mortality c) Improve long-term outcomes d) All of the above

8585w w w . e m c r e g . o r g
EVALUATION QUESTIONNAIREOn a scale of 1 to 5, with 1 being highly satisfied and 5 being highly dissatisfied, please rate this program with respect to: Highly satisfied Highly dissatisfied
Overall quality of material: 1 2 3 4 5Content of monograph: 1 2 3 4 5Other similar CME programs: 1 2 3 4 5How well course objectives were met: 1 2 3 4 5
What topics would be of interest to you for future CME
programs?
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
Was there commercial or promotional bias in this
monograph? ❑ YES ❑ NO If YES, please explain:
_____________________________________________
_____________________________________________
_____________________________________________
_____________________________________________
How long did it take for you to complete this monograph?
_____________________________________________
_____________________________________________
Name (Please print clearly): ______________________
_____________________________________________
Degree: ______________________________________
_____________________________________________
Specialty: _____________________________________
Academic Affiliation (if applicable): _______________
_____________________________________________
_____________________________________________
Address: _____________________________________
_____________________________________________
City: ______________State: ___ Zip Code:_________
Telephone Number: ( ) ______________________
After you have read the monograph, carefully record your answers by circling the appropriate letter for each question and complete the evaluation questionnaire.
Mail the answer sheet to:
Office of Continuing Medical Education University of Cincinnati College of Medicine PO Box 670567 Cincinnati OH 45267-0567
CME expiration date February 1, 2008.
Continuing Medical Education Post-Test Answer Form and Evaluation
ACEP 2006 Scientific Assembly EMCREG Symposia
1. a b c d
2. a b c d
3. a b c d
4. a b c d
5. a b c d
6. a b
7. a b
8. a b c d
9. a b c d
10. a b c d
11. a b c d
12. a b
13. a b c d e
14. a b c d
15. a b c d e
16. a b
17. a b c d e f
18. a b
19. a b
20. a b
21. a b c d
22. a b c d
23. a b c d
24. a b c d
25. a b c d
26. a b
27. a b c d e f
28. a b
29. a b
30. a b
31. a b
32. a b
33. a b c d
34. a b c d e
35. a b
36. a b
37. a b c d
38. a b c d
39. a b
40. a b c
41. a b c d

Produced by
© 2006 EMCREG-International
www.emcreg.org
Produced by
AD
VA
NC
ING
TH
E ST
AN
DA
RD
OF C
AR
E: C
ardiovascular and Neurovascular E
mergencies - O
CT
OB
ER
2006
E
MC
RE
G-International
P r inted in the USA
This educational monograph was supported in part by
unrestricted educational grants from Abbott POC/i-STAT,
Biosite, Bristol-Myers Squibb, PDL BioPharma, Sanofi-Aventis,
Schering Plough, Scios, and The Medicines Company.
IN THIS ISSUE
ADVANCING THE STANDARD OF CARE:
Cardiovascular and Neurovascular Emergencies
ADVANCING THE STANDARD OF CARE:
Cardiovascular and Neurovascular Emergencies
EMCREG MonographFrom the ACEP 2006Scientific AssemblySatellite SymposiumOctober 16 & 17, 2006
New Orleans, LA
EMCREG MonographFrom the ACEP 2006Scientific AssemblySatellite SymposiumOctober 16 & 17, 2006
New Orleans, LA