a century of health services development in birmingham - tim jones
TRANSCRIPT
“We build on a noble heritage".
A century of health services development in Birmingham in the context of the broader political and
social environment
Where did it all begin? • Metchley Roman Fort is on
the same site as the QE.
• Originally a Roman staging
post on Icknield Street to
protect communication
routes.
• Archaeological evidence
shows sporadic use but there
is some evidence of a
medical function.
Hospitals in Birmingham
• Hospitals mainly providers to the poor pre 1914.
• Voluntary Hospitals & Municipal Hospitals.
• In Birmingham a number of charitable hospitals:
General 1770 [rebuilt 1897], Queens 1841,
Orthopaedic 1817, eye 1823, The Earl 1843,
Dental 1858, Children’s 1862, Women’s 1871 &
Skin 1881.
• Main Municipal Hospitals at Selly Oak and
Dudley Road.

Social Change • Doubling of population
between 1881 and 1921.
• Industrialisation and the motor
car led to an increase in
accidents (50,000 accidents
by 1920).
• Resources diverted to
munitions during the war
leading to overcrowding.
• Societal change brought about
by the war led to greater use
of hospitals by the middle
classes.
Date Population
1087 100
1546 2,300
1700 15,000
1801 73,670
1881 401,000
1921 922,000
1931 1,002,000
1951 1,100,000
2011 1,074,000

Medical Advances • Aseptic techniques and
antiseptics led to Golden age of
surgery between 1900-20.
• Roentengen’s work on x-rays
published in 1896.
• Development of specialist
diagnostics & discovery during
wartime.
• Antibiotics & Insulin.
• “The second quarter of the 20th
Century was the Golden Age of
Medicine “ Stanley Barnes

Municipal Hospitals • Workhouses were
transforming into Hospitals.
• At Selly Oak, a separate
infirmary was built in 1897 at
a cost of £52,000.
• Dudley Road was upgraded
for military use during the
war.
• Being Municipally funded the
hospitals were better placed
to access new technologies.
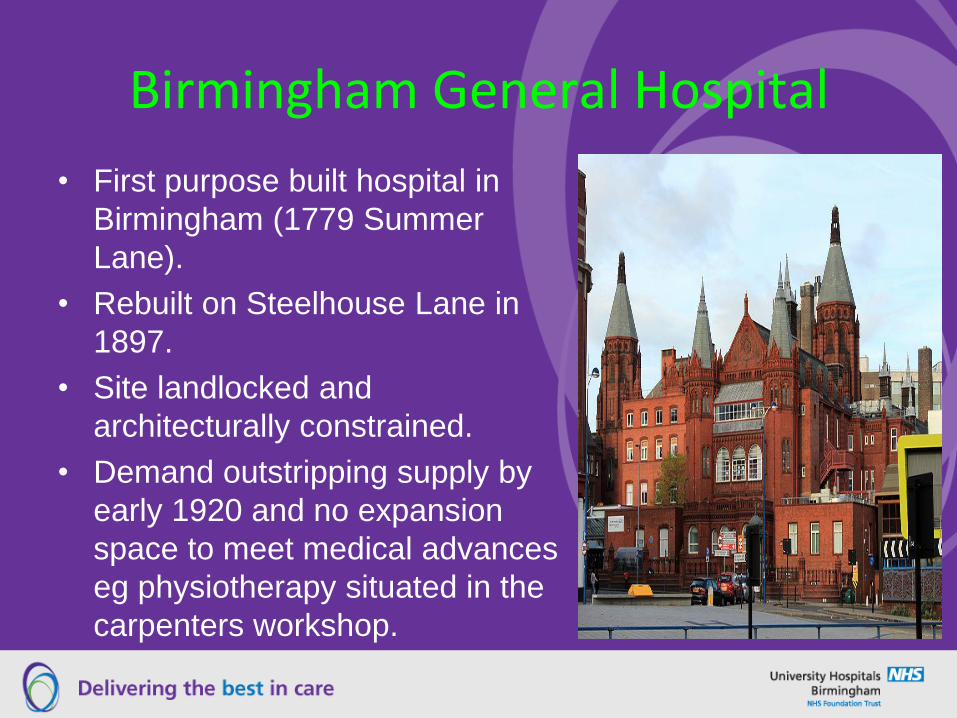
Birmingham General Hospital
• First purpose built hospital in
Birmingham (1779 Summer
Lane).
• Rebuilt on Steelhouse Lane in
1897.
• Site landlocked and
architecturally constrained.
• Demand outstripping supply by
early 1920 and no expansion
space to meet medical advances
eg physiotherapy situated in the
carpenters workshop.
Birmingham Queen’s Hospital • Opened in 1841 & named
after Queen Victoria.
• Built mainly for clinical
instruction.
• Opened with approximately
100 beds.
• Extended in 1868
(outpatients) and a nurses
home added in 1887.
• Further expansion in 1908
and in 1925.

Birmingham Medical School • Initially established in 1828 to remove young men from
the “distractions and allurements of the Metropolis”.
• The School of Medicine was situated near the Town Hall
in Queen’s College and could accommodate the
teaching but not the clinical experience.
• To meet the clinical aspects of medical education Sands
Cox a lecturer in anatomy established the first hospital to
support medical training at the Queen’s Hospital.
• The General Hospital established a rival school to attract
apprentices known as the Sydenham School.
• The 2 schools were merged in 1868 and became the
Faculty of Medicine on the establishment of the
University in 1900.
Post War Birmingham Health Economy
• Voluntary Hospitals charitable donations
dwindled during the war and post war years.
• Cost of care also rising due to medical
advances and growing demand.
• Nationally Voluntary Hospitals running into
debt but were too big to be allowed to fail.
• Government made half a million pounds
available to support voluntary hospitals.
• To access the funds Voluntary Hospitals had to
join and abide by the decisions of the Local
Voluntary Hospitals Committees.
General Hospital Response made by the Medical Committee
Medical Committee reported to the Management Board in
December 1922:
• An additional 130 beds
• Purpose built x-ray facility-double the size and triple the
equipment
• 4 new operating theatres
• 50% increase in Casualty and Observation ward
• 50% increase in outpatients.
• Increase in Physiotherapy space.
• New departments of bio-chemistry and clinical
pathology

The Board’s response?
• Established “THE EXTENSION
COMMITTEE”.
• First meeting Jan 1923.
• Reported in October 1925.
• All requests for additional beds to be
presented to the Local Voluntary
Hospitals Committee.
• LVHC recommended:
“That no decision be taken on the proposal to extend the bed accommodation in the centre of
the city until full enquiry has been made through the Ministry of Health and other
available sources as to the comparative cost and efficiency of general hospital extension in open
suburban areas compared with extension on the central site”.
“The work of an irresponsible body of men who had no
interest in the General Hospital”.
Board Member

Consequences of LVHC Decision • All further expansion of the
Queen’s and General Hospital
delayed / stopped.
• No public appeal for funds without
LVHC sanction.
• Main opposition to the General
Extension came from Alderman
WA Cadbury.
• Cadbury vision to create a 100
acre suburban site to provide for
Birmingham’s population for the
next 50 years.

Grant Robertson Committee Established • Invited the General & Queen’s
Hospital to consider a scheme
to consider a new Hospital
Centre adjacent to the new
University.
• The invitation was accepted by
both organisations
[unthinkable 5 years before
due to the animosity between
the 2 organisations].
• Steering Committee to be
chaired by Mr Charles Grant
Robinson Principal of the
University.
Birmingham Hospitals
Centre
Birmingham General Hospital
University of Birmingham
Queen’s Hospital

Grant Robertson Report Reported within 6 months in 1926 and unanimously
approved at the Hospitals Council in October 1926:
1. New Centre established adjacent to UoB site.
2. General & Queen’s amalgamated as quickly as
possible [achieved in 1933].
3. The amalgamated institution would have access to
1,200 beds.
4. New Hospital should have a minimum of 750 beds.
Work began on planning the new Medical Centre
sponsored by Alderman Cadbury who bought and
donated the site in 1926 and funded visits to medical
centres across Europe and an early rejection of the
traditional pavilion system.
1926 -31 • Executive Board established in 1927 but progress was
slow with no infrastructure to support the scheme and its
members fulfilling full time roles at their home
institutions.
• Had to resolve a legal issue with the Board of Trade as
to how the 2 legal entities could transfer a £1m asset to
a legal entity which did not exist.
• After an initial influx of funds bringing in nearly £500,000
the number and value of charitable donations dwindled.
• A decision was made to scale back the bed numbers
from 750 to 500 but maintain the ancillary services and
design in expansion space.
Controversy & Challenge –”A Birmingham Medical Man” Nov 1931
• Concern that the new
centre would mean the loss
of medical students &
status.
• Financial pressure due to
rising costs and poor
economic outlook
(Municipal Albatross).
• Birmingham had increased
by 879 beds since 1925.
Birmingham Hospitals Centre
Finance
Capacity
Identity
Battle lines are drawn – The Midland Institute Meeting – Jan 4th 1932
• Controversy came to a head at a public meeting
held in the Midland Institute.
• Opponents to the scheme included several
senior clinicians, the Municipal Medical Officer
and the Chancellor of the Exchequer.
• Supporters included the Subscribers to the fund,
The Hospitals Committee, The Hospitals
Saturday Fund and the Dunlop Rubber
Company.
• The supporters won the day by a relatively small
majority of 42.

Finally work begins
• Construction began in
1933 by The United
Birmingham Hospitals.
• Foundation stone laid by
the Prince of Wales 1934.
• Donations increased to
£1,158m to cover the initial
building cost.
• Construction and
commissioning completed
on the 1st of March 1938
and named after the
Queen.
Underlying planning principles in the late 1920’s:
• To maximise efficiency the Hospital Centre
to accommodate medical students and
faculty with appropriate specialisms in one
place.
• Optimum bed occupancy to be 85%.
• Optimal flexibility in bed use through a
combination of ward / room sizes ranging
from single rooms to 16 bed.
• Novel design and innovation in
heating/ventilation.
• Advanced activity modelling.
1940’s & 50’s • The QE immediately put
under pressure during the
war and increased from
540 to 750 beds.
• 1948 NHS established
and UBH transferred to
NHS.
• 1950 School of Nursing
opened.
• Nurse staffing 75 female
and 1 male [nursing
supported mainly by
students approx 500].

1960 to 1990 • 1968 Womens Hospital opened.
• First Computer used at QE in the
late 1960’s.
• Cardiac Pacemakers part of great
medical advances such as CT
Scanning, ultrasound and nuclear
imaging.
• MRI and renal dialysis
• First Liver Transplant in 1982 [now
the largest programme in the world.
• Ill fated Ackers Plan.

The brink of a 3rd IR driven by electronic communication
• Steam, Petrol &
Electronic.
• Medical technology
incrementally advancing.
• Digital technology is
providing the disruptive
change for transformative
change.
• Potentially offers a route
to balance supply &
demand.
Jeremy Rifkin 2011
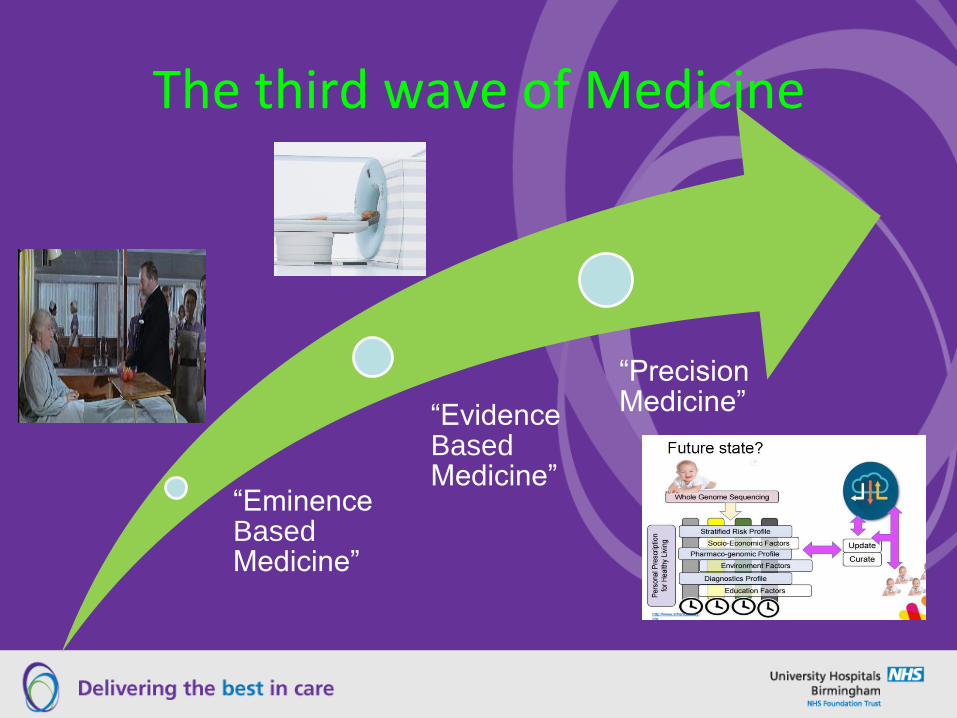
The third wave of Medicine
“Eminence Based Medicine”
“Evidence Based Medicine”
“Precision Medicine”
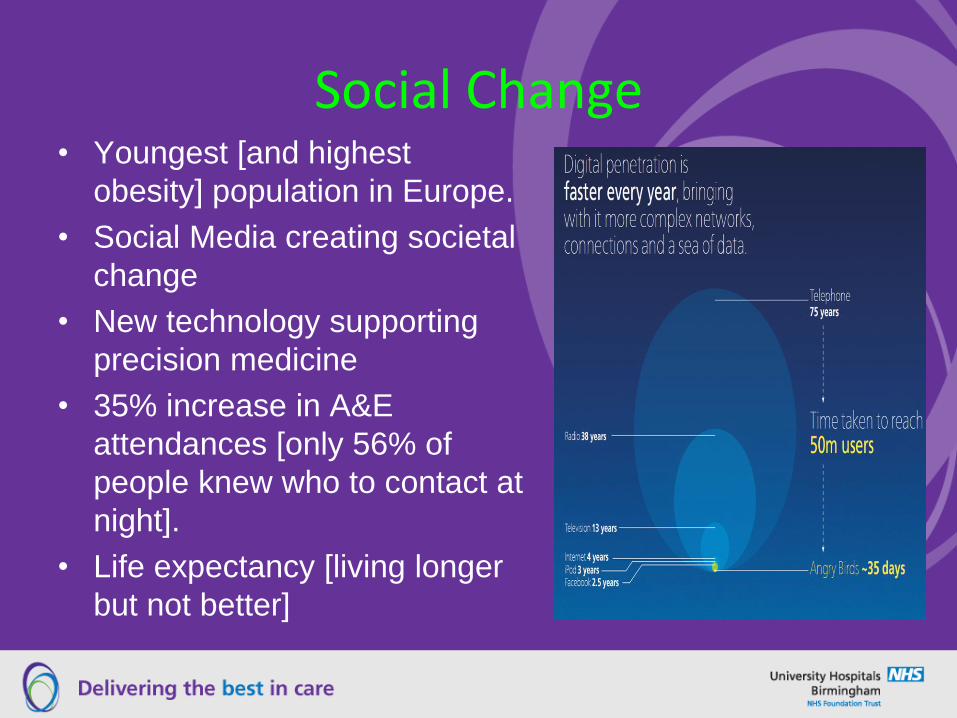
Social Change • Youngest [and highest
obesity] population in Europe.
• Social Media creating societal
change
• New technology supporting
precision medicine
• 35% increase in A&E
attendances [only 56% of
people knew who to contact at
night].
• Life expectancy [living longer
but not better]

Origins of the new QE
• Financial crisis in South
Birmingham HA led to
drastic reductions in service.
• Selly Oak & QE merged,
Accident Hospital closed in
1995.
• Smethwick Neurosurgical
Hospital closed 1996.
• Birmingham General closed
in 1997.

Urgent need for renewal
• £100m+ repair costs
• Two sites
• New technology
• Infection prevention
• New clinical needs
Key drivers
• Improve patient care
• Meet rising patient expectations
• Improve efficiency
• Complexity of Medicine
• Education and training

Planning started in 1999
• 21 Short Life Working Groups.
• Over 2000 Clinical Staff
involved in planning process.
• Detailed activity modelling.
• Invitation to Tender 2002.
• Preferred Bidder selected in
2003.
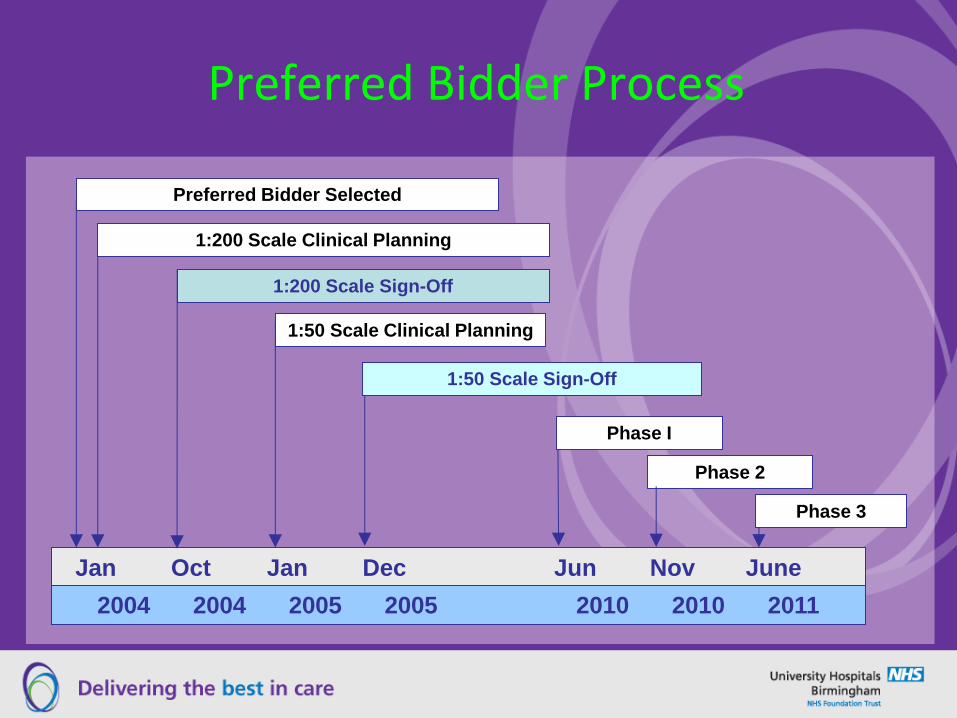
Preferred Bidder Process
Jan Oct Jan Dec Jun Nov June
2004 2004 2005 2005 2010 2010 2011
Preferred Bidder Selected
1:200 Scale Clinical Planning
1:200 Scale Sign-Off
1:50 Scale Clinical Planning
1:50 Scale Sign-Off
Phase I
Phase 3
Phase 2
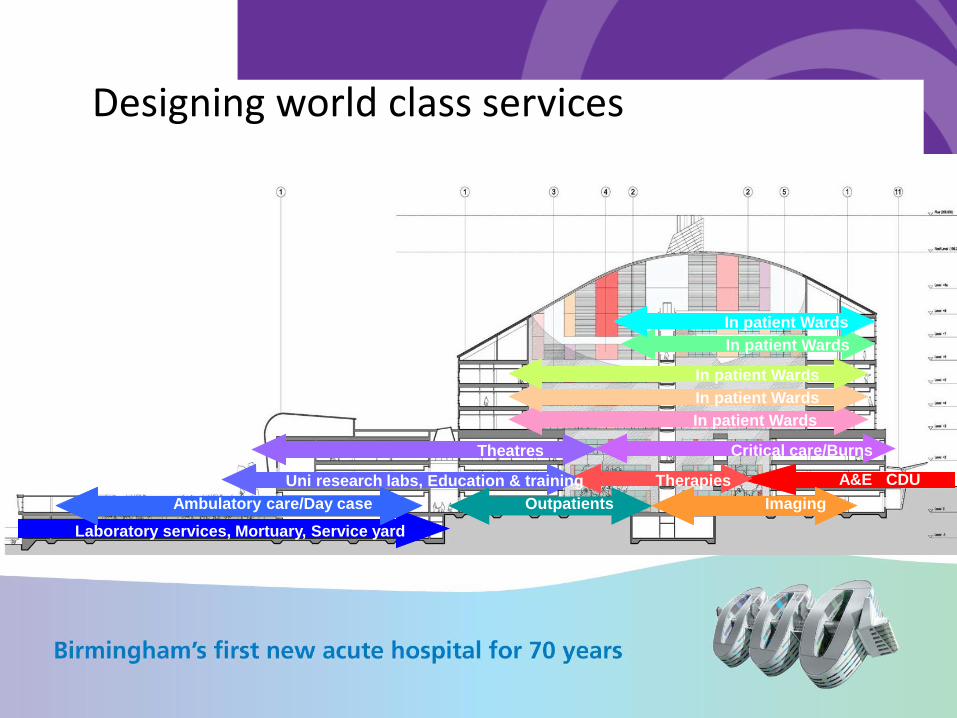
A&E CDU
Outpatients
Laboratory services, Mortuary, Service yard
Ambulatory care/Day case Imaging
Therapies Uni research labs, Education & training
Theatres Critical care/Burns
In patient Wards
In patient Wards
In patient Wards
In patient Wards
In patient Wards
Designing world class services

Beds in New Hospital - 1233
Bed Type: Current New Hospital Difference: Current
& Future
> 23 hrs (inc PPU) 1035 899
(inc. 36 growth)
-136
Assessment Trolleys +
Recliners
10 32 + 22
Critical Care 86 100
(inc. 14 growth)
+ 14
< 23 hrs
Beds and trolleys
64 64 0
< 23 hrs
Recliners
12 61 + 49
Dialysis Recliners 37
41 + 4
Decant Ward 0 36 + 36
TOTALS 1244 1233 - 11

Clinical Strategies to deliver new models
of care
• Reduction in avLOS (eg Increase preadmission: tight
control of LOS: new ways of working (RATS)
• “On Demand” Diagnostics (Front door = 4hrs: inpatients
24hrs MAX for diagnostics& intervention
• Reduction in beds days lost: (delayed discharge: HAIs)
• Activity conversion to ambulatory / short stay
• 7 day working
• ICT development to support new ways of working - eg
ELOS: “real-time” digital data retrieval & entry

Major Challenges
• Achieving “fit”.
• Paperless Hospital
• Clinical Aggregations.
• Managing the front door.
• Maintaining Quality

Another Intervention by No11
• Chancellor of Exchequer
again argues QE should
be delayed.
• Gordon Brown against
PFI.
• Borrowing to Capital ratio
changed by PFU.
• BoD approves the
World’s most expensive
hole in the Ground.
• PFU undertakes review.
Approval is achieved • Road to Affordability project
achieves new PFI ratio.
• 3 wards shelled & other
compromises made (oncology)
• WM SHA and SB’ham PCT approve
scheme.
• PFU agree revised finance model.
• Opposition to single site scheme
wanes following PFU approval.
• Sandwell & West Birmingham
announce 2010 project.




• 44% single rooms
• Integrated services
• Co-location of specialties
• Latest technology
• Leading edge care
• Great visitor facilities


Critical Care Unit

Theatres
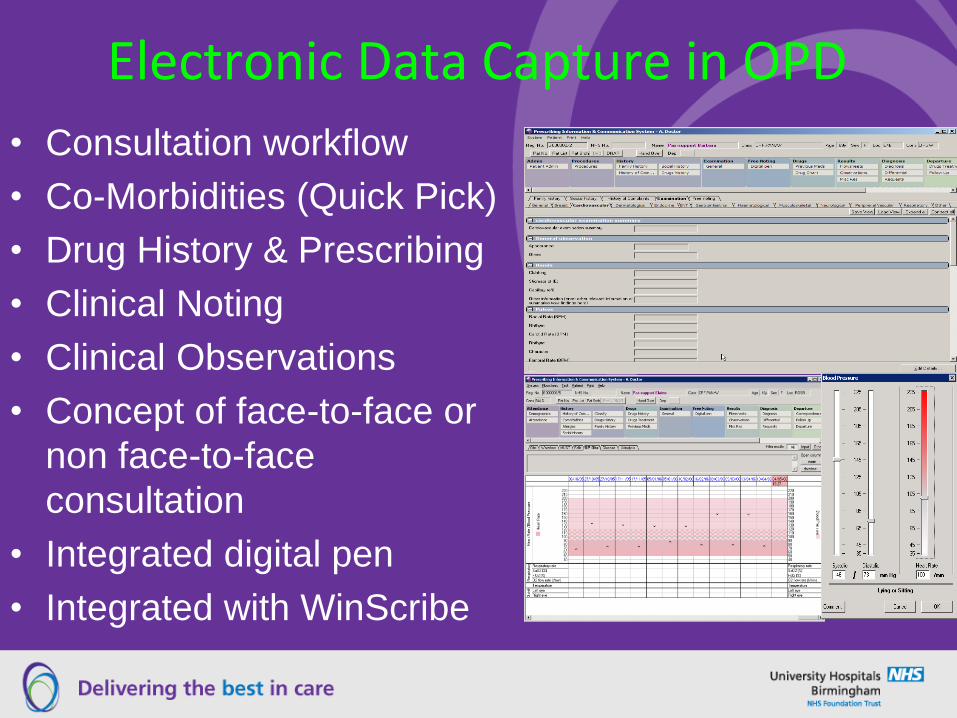
Electronic Data Capture in OPD
• Consultation workflow
• Co-Morbidities (Quick Pick)
• Drug History & Prescribing
• Clinical Noting
• Clinical Observations
• Concept of face-to-face or
non face-to-face
consultation
• Integrated digital pen
• Integrated with WinScribe

Facilitates a Journey from this -
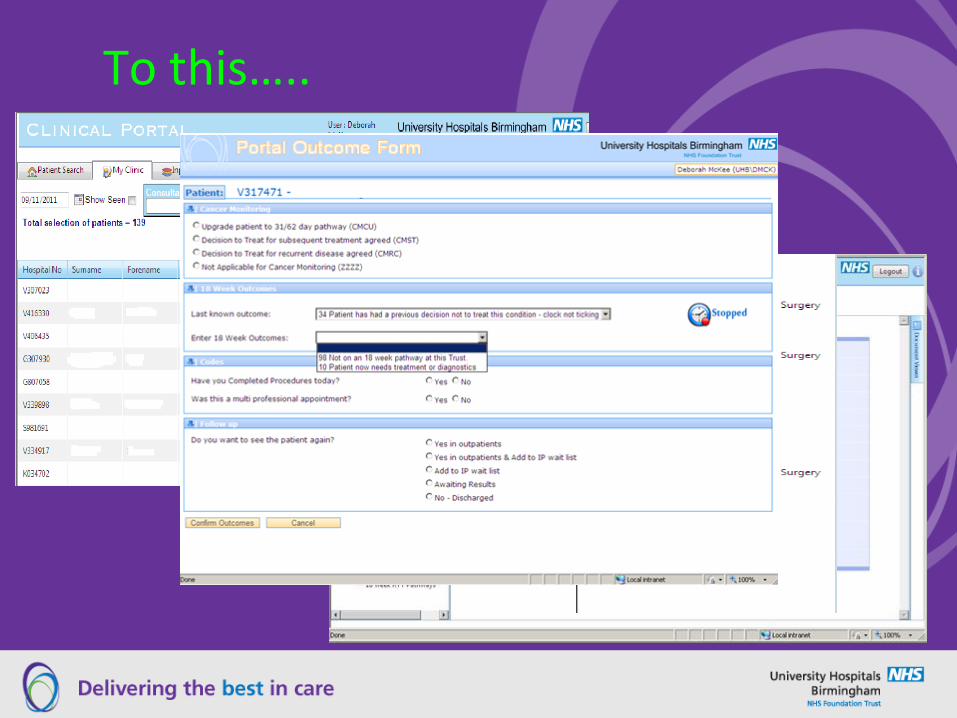
To this…..

And this…

Comparison of the 2 QE’s Old QE
• Controversial
• 12 years from inception to
occupation.
• 540 beds
• 7 Theatres
• State of the art labs &
imaging.
• Structural change –LVHC
• Plans for Children’s
Hospital
• Leveraging benefit from
campus
New QE
• Controversial
• 12 years from inception to
full occupation.
• 1,213 beds [c 1,400 beds]
• 32 Theatres
• 3T MRI, 5 MRI, 6 CT and
automated labs.
• STP & Devo
• Plans for Children's
Hospital
• Leveraging benefit from
campus

The Future
• Devolution agenda
• Ageing and morbidity
• Big Data pro’s and con’s
• Birmingham Metropolitan Hospital
• Precision or Personal Medicine
• Will the wealthy return to care in
their own homes?
Questions?