8. rectum and anal canal (49 ).pptx
TRANSCRIPT

Learning Objectives
Describe the anatomy of the rectum and anatomical relationships and peritoneal coverings.
Explain the anatomy of the anal canal and the functional anatomy of the anal sphincters and their innervation.
Describe the blood supply and lymphatic drainage of the rectum and anal canal and portal-systemic venous anastomosis.
Rectum & Anal Canal

Rectum 5 in. (13 cm) long.
Begins in front of the third sacral vertebra as a continuation of the sigmoid colon.
Passes downward, following the curve of the sacrum and coccyx
Ends in front of the tip of the coccyx by piercing the pelvic diaphragm and becoming continuous with the anal canal.
Lower part of the rectum is dilated to form the rectal ampulla.
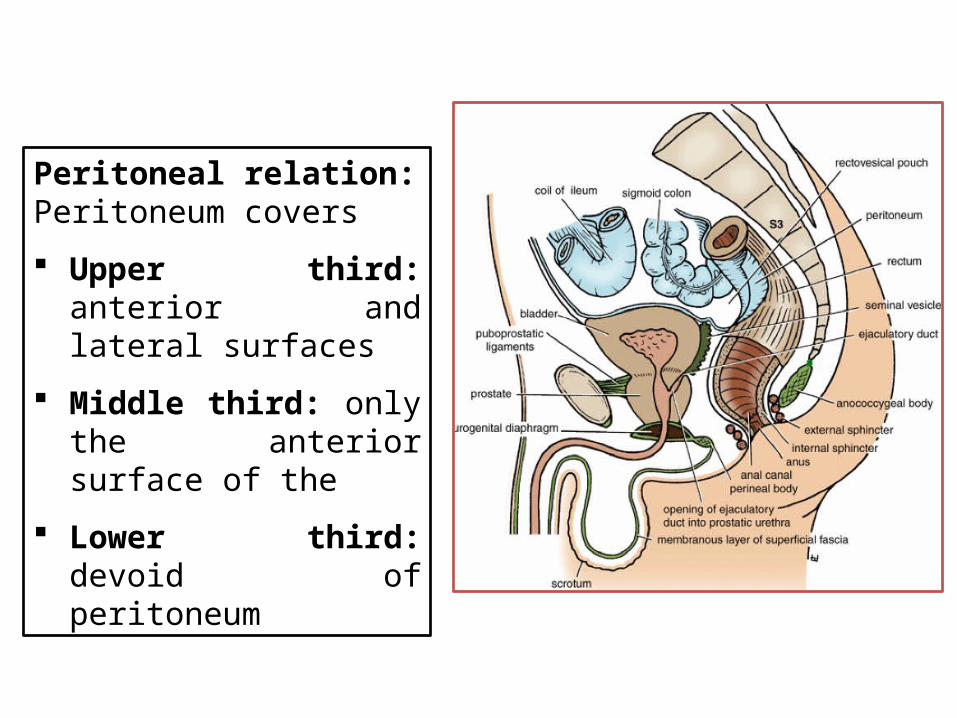
Peritoneal relation:Peritoneum covers
Upper third: anterior and lateral surfaces
Middle third: only the anterior surface of the
Lower third: devoid of peritoneum

Rectum: Anterior Relation:In the male: Upper two thirds: Sigmoid colon Coils of ileum Lower third: Posterior surface of the bladder Vas deferens Seminal vesicles on each side Prostate
In the female: Upper two thirds : Sigmoid colon Coils of ileumLower third: Devoid of peritoneum Posterior surface of the vagina

RelationsPosteriorly: Sacrum and coccyx Piriformis Coccygeus Levatores ani muscles Sacral plexus Sympathetic trunks
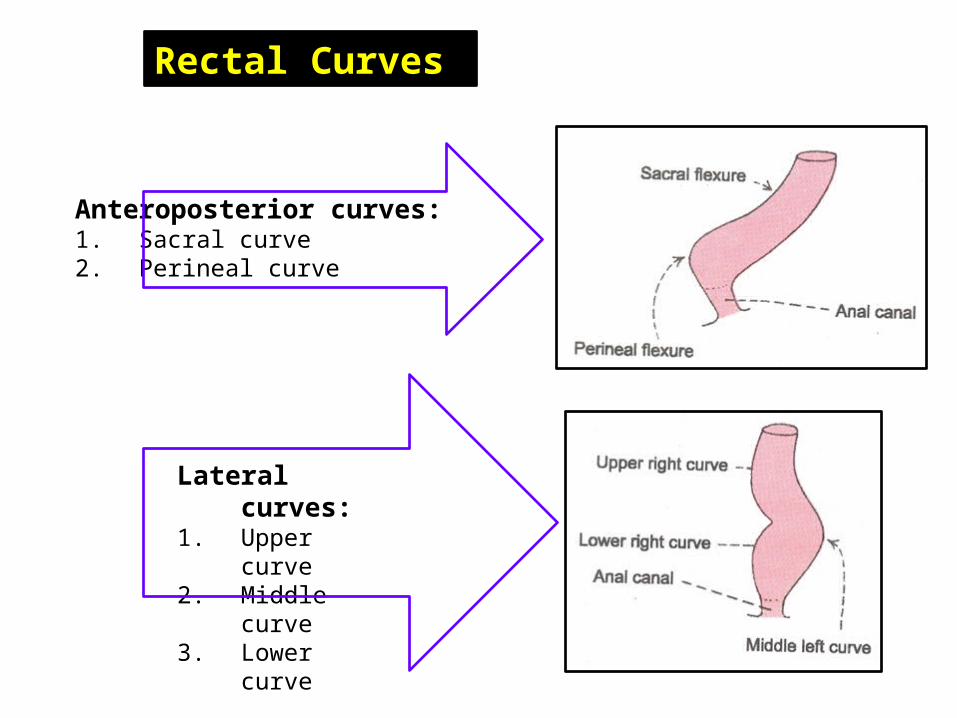
Lateral curves:1. Upper curve2. Middle curve3. Lower curve
Anteroposterior curves:1. Sacral curve2. Perineal curve
Rectal Curves

Mucosal Folds Crescentic transverse
mucosal folds of the rectum must also be borne in mind when passing an instrument into the rectum.
These folds serve to support the weight of the feces and to prevent excessive distention of the rectal ampulla.

Rectal Curves and Mucosal FoldsAnteroposterior flexure: follows the curvature of the sacrum and coccyx.
Lateral flexures: must be remembered when one is passing a sigmoidoscope to avoid causing the patient unnecessary discomfort.
(a) A metal proctoscope and two different-sized metal Lloyd-Davies rigid sigmoidoscopes – small (diameter 20 mm). Since theadvent of greater awareness of transmitted infection, disposable proctoscopesand sigmoidoscopes (b) have replaced the re-usable metal types.
A B

Arteries Superior rectal artery: direct
continuation of the inferior mesenteric artery and the chief artery supplying the mucous membrane.
Middle rectal artery: branch of the internal iliac artery, distributed mainly to the muscular coat.
Inferior rectal artery: branch of the internal pudendal artery. Anastomoses with the middle rectal artery at the anorectal junction.

Veins
Superior rectal vein: tributary of the portal circulation and drains into the inferior mesenteric vein.
Middle and inferior rectal veins drain into the internal iliac and internal pudendal veins, respectively.

Lymph Drainage The lymph vessels of the rectum drain first into the
pararectal nodes and then into inferior mesenteric nodes.
Lymph vessels from the lower part of the rectum follow the middle rectal artery to the internal iliac nodes.

Innervation of the Rectum Sympathetic supply: from the lumbar spinal cord,
conveyed via lumbar splanchnic nerves
Parasympathetic supply: from the S2-S4 spinal cord level, passing via the pelvic splanchnic nerves and the left and right inferior hypogastric plexuses to the rectal (pelvic) plexus.
All visceral afferent fibers follow the parasympathetic fibers retrogradely to the S2-S4 spinal sensory ganglia.
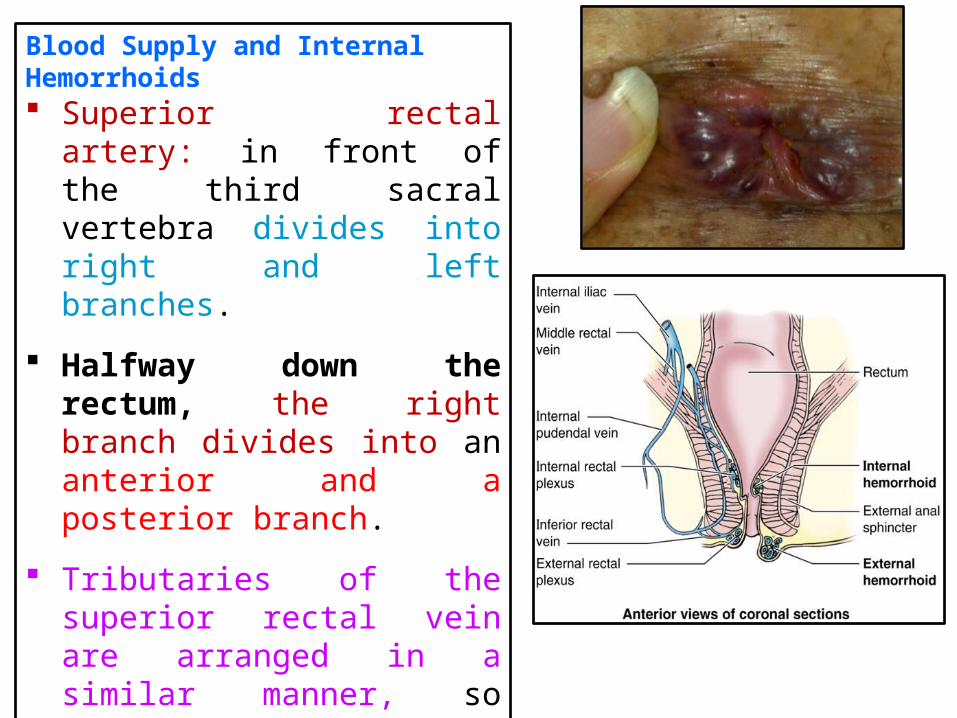
Blood Supply and Internal Hemorrhoids Superior rectal artery: in front of
the third sacral vertebra divides into right and left branches.
Halfway down the rectum, the right branch divides into an anterior and a posterior branch.
Tributaries of the superior rectal vein are arranged in a similar manner, so that internal hemorrhoids are arranged in three groups: two on the right side of the lower rectum and anal canal and one on the left.

Prolapse of the Rectum Damage to the levator ani muscles as the
result of childbirth and poor muscle tone in the aged are important contributing factors.
A complete rectal prolapse may be regarded as a sliding hernia through the pelvic diaphragm.
Partial prolapse: rectal mucous membrane and submucous coat protrude for a short distance outside the anus .
Complete prolapse: whole thickness of the rectal wall protrudes through the anus.

Cancer of the Rectum First, spread locally in the lymphatics around the circumference
of the bowel. Later, spreads upward and laterally along the lymph vessels, following the superior rectal and middle rectal arteries.
Venous spread occurs late, and because the superior rectal vein is a tributary of the portal vein, the liver is a common site for secondary deposits.
Posterior penetration involves the sacral plexus and can cause severe intractable pain down the leg in the distribution of the sciatic nerve.
Lateral penetration may involve the ureter.
Anterior penetration: Male: may involve the prostate, seminal vesicles, or bladder. Female: may involve the vagina and uterus.

Rectal Examination
Anal canal is about 1.5 in. (4 cm) long so that the pulp of the index finger can easily feel the mucous membrane lining the lower end of the rectum.
Many structures related to the anteroinferior part of the rectum may be palpated through its walls:
Prostate and seminal glands in males and cervix in females.
Sacrum and coccyx, ischial spines and tuberosities in both sexes
Enlarged internal iliac lymph nodes, pathological thickening of the ureters
Rectovesical pouch in the male or the rectouterine pouch in the female

Rectal Examination The internal aspect of the rectum can
be examined with a proctoscope, and biopsies of lesions may be taken through this instrument.
During insertion of a sigmoidoscope, the curvatures of the rectum and its acute flexion at the rectosigmoid junction have to be kept in mind so that the patient does not undergo unnecessary discomfort.
The operator must also know that the transverse rectal folds, which provide useful landmarks for the procedure, may temporarily impede passage of these instruments.
(a) A metal proctoscope and two different-sized metal Lloyd-Davies rigid sigmoidoscopes – small (diameter 20 mm). Since theadvent of greater awareness of transmitted infection, disposable proctoscopesand sigmoidoscopes (b) have replaced the re-usable metal types.
A
B

Resection of the Rectum Performed in the plane of
the rectovesical septum (a fascial septum extending superiorly from the perineal body)
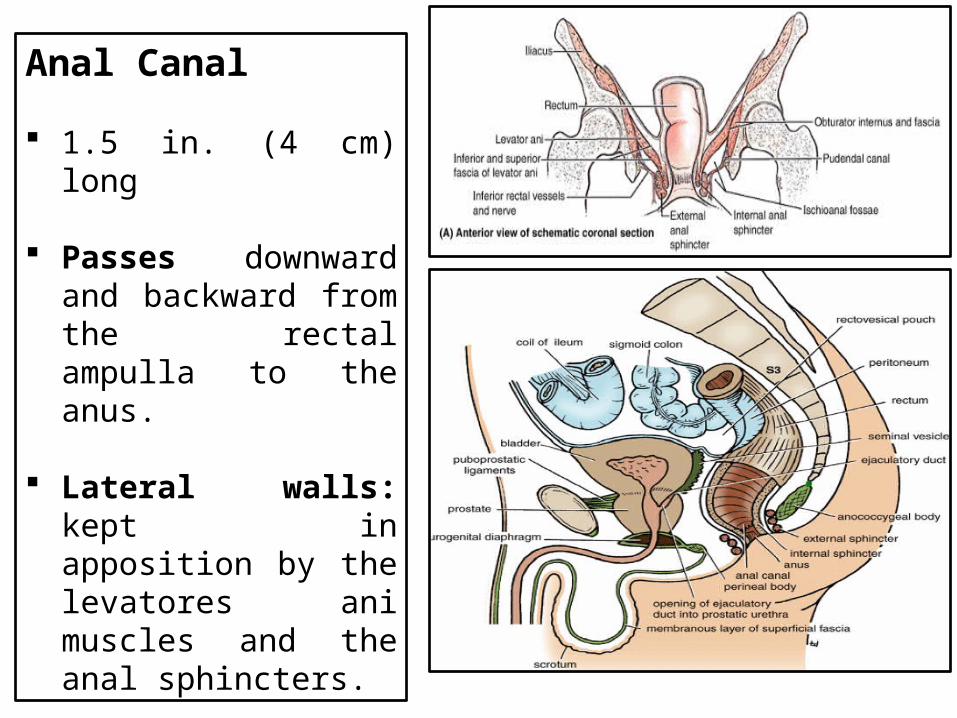
Anal Canal
1.5 in. (4 cm) long
Passes downward and backward from the rectal ampulla to the anus.
Lateral walls: kept in apposition by the levatores ani muscles and the anal sphincters.

Anterior Relation: Male: Perineal body, Urogenital diaphragm, Membranous part of the urethra, Bulb of the penis.
Female:Perineal body,Urogenital diaphragmLower part of the vagina.

Relations
Posteriorly: The anococcygeal body, which is a mass of fibrous tissue lying between the anal canal and the coccyx.
Laterally: The fat-filled ischiorectal fossae.

Mucous membrane of the upper half of the anal canal derived from hindgut entoderm . lined by columnar epithelium. thrown into vertical folds called anal columns, joined together at
their lower ends by small semilunar folds called anal valves (remains of proctodeal membrane).
Mucous membrane of the lower half of the anal canal Derived from ectoderm of the proctodeum. Lined by stratified squamous epithelium, which gradually merges at the
anus with the perianal epidermis . No anal columns .

The pectinate line indicates the level where the upper half of the anal canal joins the lower half

Mucous membrane of the upper half of the anal canal: Arterial supply form hindgut artery, the superior rectal artery, a
branch of the inferior mesenteric artery .
Mucous membrane of the lower half of the anal canal: Arterial supply from the inferior rectal artery, a branch of the
internal pudendal artery.

Mucous membrane of the upper half of the anal canal: Venous drainage by the superior rectal vein, a tributary of the
inferior mesenteric vein, and the portal vein.
Mucous membrane of the lower half of the anal canal: Venous drainage by the inferior rectal vein, a tributary of the
internal pudendal vein, which drains into the internal iliac vein.

Mucous membrane of the upper half of the anal canal: Lymphatic drainage: upward along the superior rectal artery to
the pararectal nodes and then eventually to the inferior mesenteric nodes.
Mucous membrane of the lower half of the anal canal: Lymph drainage: downward to the medial group of superficial
inguinal nodes.

Mucous membrane of the upper half of the anal canal: Nerve supply: same as that for the rectal mucosa and is derived
from the autonomic hypogastric plexuses. Sensitive only to stretch .
Mucous membrane of the lower half of the anal canal: Nerve supply: from the somatic inferior rectal nerve sensitive to pain, temperature, touch, and pressure

Anal Sphincters: Involuntary internal
sphincter and voluntary external sphincter.
Internal sphincter: Formed from a thickening of
the smooth muscle of the circular coat at the upper end of the anal canal.
Enclosed by a sheath of striped muscle that forms the voluntary external sphincter.

External sphincter can be divided into three parts: Subcutaneous part:
encircles the lower end of the anal canal and has no bony attachments.
Superficial part: attached to the coccyx behind and the perineal body in front.
Deep part: encircles the upper end of the anal canal and has no bony attachments.

Cancer and the Lymph Drainage of the Anal Canal
Upper half of the mucous membrane of the anal canal: drained upward to lymph nodes along the course of the superior rectal artery.
Lower half of the mucous membrane: drained downward to the medial group of superficial inguinal nodes.
Many patients have thought they had an inguinal hernia, and the physician has found a cancer of the lower half of the anal canal, with secondary deposits in the inguinal lymph nodes.

Anal Sphincter Nerve Block and Anesthetizing the Perianal Skin By blocking the branches of the inferior rectal nerve and the perineal branch of
the fourth sacral nerve
Procedure : A long needle attached to a syringe filled with anesthetic solution is inserted
through the cutaneous wheal into the sphincter muscles along the posterior and lateral surfaces of the anal canal. The procedure is repeated on the opposite side.
The purpose of the finger in the anal canal is to guide the needle and to prevent penetration of the anal mucous membrane.

Perianal Abscesses
Produced by fecal trauma to the anal mucosa .
Infection may gain entrance to the submucosa through a small mucosal lesion
Abscess may complicate an anal fissure or the infection of an anal mucosal gland.

Perianal Abscesses abscess may be localized to the
submucosa, submucous abscess. May occur beneath the perianal skin,
subcutaneous abscess. May be found in the space between
the ampulla of the rectum and the upper surface of the levator ani, pelvirectal abscess.
May occupy the ischiorectal fossa, ischiorectal abscess.
Perianal AbscessesLarge ischiorectal abscesses sometimes extend posteriorly around the side of the anal canal to invade the ischiorectal fossa of the opposite side (horseshoe abscess).

Anal fistulae: opens at one end at the lumen of the anal canal or lower rectum and at the other end on the skin surface close to the anus. (If the abscess opens onto only
one surface, known as a sinus.)
High-level fistulae: Rare Run from the rectum to the
perianal skin Located above the anorectal ring Fecal material constantly soils the
clothes. Low-level fistulae: occur below the level of the
anorectal ring.
Tearing downward of the anal valve to form an anal fissure.

Anal Fissure Develops due to Injury of the anal
valves and may get infected by the secondary infection
Extremely painful
occurs: most commonly, in the midline posteriorly
Caused: by the lack of support provided by the superficial part of the external sphincter in these areas
Lower half of the fissure, very sensitive as being supplied by the inferior rectal nerve
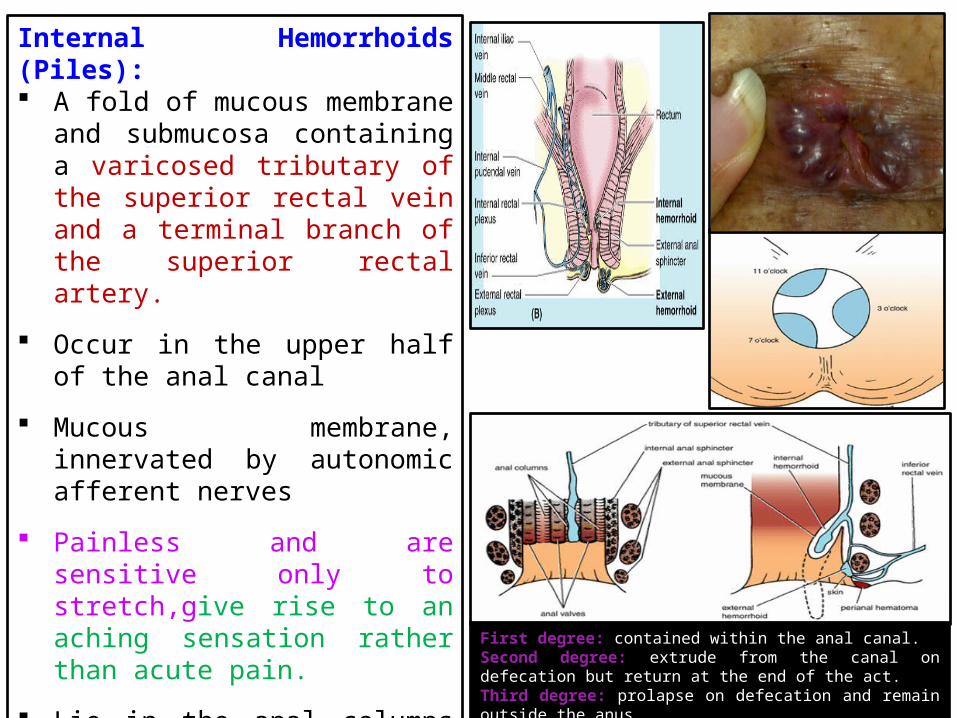
Internal Hemorrhoids (Piles): A fold of mucous membrane and
submucosa containing a varicosed tributary of the superior rectal vein and a terminal branch of the superior rectal artery.
Occur in the upper half of the anal canal
Mucous membrane, innervated by autonomic afferent nerves
Painless and are sensitive only to stretch,give rise to an aching sensation rather than acute pain.
Lie in the anal columns at the 3, 7, and 11-o'clock positions when the patient is viewed in the lithotomy position First degree: contained within the anal canal.
Second degree: extrude from the canal on defecation but return at the end of the act. Third degree: prolapse on defecation and remain outside the anus.

External Hemorrhoids: Varicosities of the tributaries
of the inferior rectal (hemorrhoidal) vein.
Covered by mucous membrane of the lower half of the anal canal or the skin
Innervated by the inferior rectal nerves.
Sensitive to pain, temperature, touch, and pressure
Tend to be painful.

Thank you